Embed Size (px)
Citation preview
January12015thruDecember312015
Plan Benefit Descriptions
Portsmouth Public Schools
Medical Reimbursement
Dependent/Child Care Reimbursement
Short Term Disability Insurance
Life Insurance
Cancer and Specified Disease Insurance
Heart/Stroke Insurance
Accident Insurance
Critical Illness Insurance
Vision Insurance
Retirement Solutions
Do not discard this booklet.
Keep for future reference.


TABLE OF CONTENTS What is a Section 125 Plan? Page 1 (This section will explain the following topics) **How does it work? **Who is eligible to participate? **How do I enroll? **What benefits are available under the plan to be pre taxed?
Benefit Brochures First Financial Debit Card Page 8 Short Term Disability Page 19 Life Insurance Page 28 Cancer Insurance Page 55 Heart/Stroke Insurance Page 65 Critical Illness Insurance Page 69 Accident Insurance Page 74 Vision Page 82 Retirement Solutions Page 83 What are the costs of the benefits? Page 89 Portsmouth Public Schools has adopted a Section 125 Flexible Benefit Plan for all eligible employees. The purpose of this booklet is to provide you with a brief description of the Plan and the benefits available to you under the Plan. In the event that a conflict develops between this booklet and the terms of the Plan, the latter instrument must control since it is the legal instrument which actually constitutes the Plan. Although the employer currently intends to continue all of the benefits described in this booklet, the employer reserves the right to amend, reduce or terminate any of these benefits at any time.

WHAT IS A SECTION 125 FLEXIBLE BENEFIT PLAN? A Section 125 Flexible Benefit Plan allows you, the employee to spend benefit dollars for benefits that you choose to meet your needs. The benefits from which you may choose are listed later in this booklet. The benefits that you elect under the Plan are paid for with benefit dollars made available to you by your employer or through a salary reduction agreement with your employer. Salary reduction means that you are able to use "pre-tax" dollars to pay for certain benefits that you may have previously paid for with "after-tax" dollars. HOW CAN THIS PLAN HELP YOU? By implementing this Plan, your employer is helping you reduce your taxes and increase your spendable income. The cost saving advantage of the Plan is simple. Any benefit costs or insurance premiums you pay under the plan are paid on a pre-tax basis. The example below illustrates the advantage of the Section 125 Plan in comparison with a situation without the benefits of a Plan. The bottom line is that you may have more dollars available to you for the purchase of other benefits you may need or available to you as increased take-home pay. WITHOUT SECTION 125 WITH SECTION 125 Average Monthly Salary $2,000 Less Estimated Federal Withholding (20%)
-400 $1,600 Less Insurance Premium(s) -200 Net Take-Home Pay $1,400 Less Out-of-Pocket "Flex" Expenses -50 Spendable Income $1,350
Average Monthly Salary $2,000 Less Qualified Insurance Premium(s) -200 Less Out-of-Pocket "Flex" Expenses -50 Taxable Income $1,750 Less Estimated Federal Withholding (20%) -350 Net Take-Home Pay/Spendable $1,400 Income
1
WHAT BENEFITS ARE AVAILABLE? The following benefits are available to you under the plan to be pre taxed: Expense Reimbursement Accounts: Medical Expense Reimbursement Dependent Care Expense Reimbursement Insurance Benefits:
Cancer, Critical Illness, Heart/Stroke, Accident, Vision, Disability* and Life* * Coverage available outside Section 125 only * If maternity benefits are provided: Group health plans and health insurance issuers offering group insurance coverage generally, under federal law, may not restrict benefits for any hospital length of stay in connection with childbirth for the mother or newborn child to less than 48 hours following a normal vaginal delivery, or less than 96 hours following a caesarian section, or require that a provider obtain authorization from the plan or the insurance issuer for prescribing a length of stay not in excess of the above periods. WHO CAN PARTICIPATE IN THE PLAN? If you are a contract employee and work at least 20 hours per week, you are eligible for supplemental benefits, 20 hours for annuities. HOW MUCH DOES IT COST TO PARTICIPATE? There is no charge to participate in the Flex Accounts and no charge for the Debit Card. Rates for
Supplemental Benefits both pre and post tax, are in the back of this booklet.
2

HOW DO I ENROLL IN THE PLAN? During the enrollment period, there will be group meetings scheduled for all employees to attend. These meetings will allow you the opportunity to hear a presentation concerning how the Plan works and information on the benefits available. Following the meeting, you will have the opportunity to visit with a representative from FFGA on a one-on-one basis concerning your individual needs. At this meeting, you will again have the opportunity to ask questions and you will complete an election form. This election form must be completed and signed by each employee, whether or not you wish to elect to participate in the benefit portion of the Plan. This is when you decide to waive all elections offered, elect new products and deductions or continue current deductions with no changes. CAN I STAY IN THE PLAN IF I AM ABSENT ON A FAMILY MEDICAL LEAVE? If you are absent from work on a leave of absence covered by the Family Medical Leave Act (FMLA) for periods totaling 12 weeks during the plan year, you are entitled to maintain the coverage you have under the Plan during your absence. Of course, you must pay the premiums for the coverage during your absence using one of the following methods: Prepayment: Under the prepayment option, you may (at your option) increase your salary reduction in an amount sufficient to cover the premiums that will come due during the FMLA leave. Pay-as-you-go: With the pay-as-you-go option, you continue to pay premiums on a regular basis through the FMLA leave. If you continue to receive your salary while you are gone, the premiums will be paid with pre-tax money as if you had not taken the leave. On the other hand, if your FMLA leave is unpaid and you choose this option, you will have to reimburse the Plan at regular intervals from your after-tax funds for the premiums that come due during the leave. The language above regarding the two payment methods assumes that both the prepayment and the pay-as-you-go methods are offered under the Plan.
CAN I STAY IN THE PLAN IF I LEAVE OR RETIRE?
If you leave Portsmouth Public Schools for any reason, you may take these products with you. You may pay for these in many different ways such as monthly bank draft, quarterly, semi annually or annually. Dental, Vision and Health are also available for continuation under COBRA guidelines.
3

PREMIUM CONVERSION The following insurance products may be purchased under the Section 125 Flexible Benefit Plan with the premiums paid on a pre-tax basis:
Health, Cancer, Heart/Stroke, Accident, Critical Illness, Hospital Protection, Dental and Vision
Enrolling in any of these benefits on the election form does not enroll you in the insurance product itself. In most cases, an insurance application to the company issuing the insurance product must also be completed. EXPENSE REIMBURSEMENT ACCOUNTS The following expense reimbursement accounts are available under the Section 125 Flexible Benefit Plan with your contributions to the account paid on a pre-tax basis:
Dependent Care Expense Reimbursement Medical Expense Reimbursement
IMPORTANT GUIDELINES FOR ENROLLMENT IN REIMBURSEMENT ACCOUNTS 1. Be sure that the amount set aside is conservative – amounts not used for qualified
expenses cannot be carried over or returned to you. 2. You cannot be reimbursed for these expenses from any other source. 3. All expenses to be reimbursed must be incurred in the plan year in which your
contributions are made. 4. Expenses reimbursed under the Plan may not be used when calculating your medical
expense deduction or the dependent care tax credit. 5. You have a 90-day grace period at the end of the plan year to request reimbursement of
expenses you incurred during the plan year. 6. You should consult with your tax advisor concerning participation in the reimbursement
accounts.
4

MEDICAL EXPENSE REIMBURSEMENT ACCOUNTS
The Medical Expense Reimbursement Account can benefit you if you have any predictable out-of-pocket medical, dental or vision care expenses. Only expenses incurred for you or your dependents during the plan year may be reimbursed. For the Medical Expense Reimbursement Account, you will only be allowed to change your benefit election due to termination of your employment. HOW MUCH IS AVAILABLE FOR REIMBURSEMENT? The total amount of a qualified expense is available for reimbursement upon receipt of a voucher and original bill or receipt. The amount of the reimbursement, however, will not exceed the total contribution for the plan year less any reimbursements paid to date. Total reimbursements for the plan year will not exceed the contribution amount for the plan year. IS THERE A CONTRIBUTION LIMIT?
Maximum amount available under the Medical Expense Reimbursement Account is $2500 per plan year.
DEPENDENT CARE REIMBURSEMENT
WHAT IS THE MAXIMUM I CAN CONTRIBUTE? In most cases, you may contribute up to $5,000 per year; however, that amount may be reduced if: 1. If you are married and file a separate tax return, the maximum contribution is
$2,500. 2. If you or your spouse earns less than $5,000 a year, the maximum contribution is
equal to the lesser income amount.
WHAT IS AVAILABLE FOR REIMBURSEMENT? Upon receipt of the voucher and acknowledgement form, you will be reimbursed for the expense you claimed up to the amount you have in your account. If your voucher is for an amount in excess of the amount in your account, the balance of the expense will be carried forward to future months as additional payments are received for your account.
5

TAX CREDIT ALTERNATIVE You should be aware that you may be able to take a federal tax credit on the amount you pay for dependent care expenses instead of participating in the dependent care expense reimbursement account. You cannot claim the tax credit for expenses that have been reimbursed through the plan. Please consult you tax advisor to determine which plan may be most advantageous to you. IMPORTANT TAX INFORMATION Regardless of whether you participate in the dependent day care plan under Section 125 or claim the credit on you income tax, you must provide the IRS with the name, address and taxpayer identification number (TIN) of your dependent day care provider(s) by completing Schedule 2 of Form 1040A or Form 2441 and attaching it to you annual income tax return. Failure to provide this information to the IRS could result in loss of the pre-tax exemption for your dependent day care expenses.
6

First Financial Group of America EMPLOYEE EXPENSE WORKSHEET EMPLOYER: NAME OF EMPLOYEE: SOCIAL SECURITY #:_____________________________DATE OF BIRTH:_____________ MARITAL STATUS: ________________ NUMBER OF DEPENDENTS:________________ ESTIMATED USE ONLY I.OUT-OF-POCKET MEDICAL EXPENSES: ANNUAL COST ELECTION Type of Expense $ Health insurance Deductibles Doctor Office Visits Over the Counter Medications Physicals Prescription Drugs Dental Costs (check-ups, cleaning, fillings) Orthodontia Costs (braces, exams, etc.) Vision & Eye Care (glasses, contacts) Surgery Other Health Related Expenses Specify TOTAL AVERAGE MONTHLY EXPENSE (divide total by 12 or number of months being paid if less than 12) II. DEPENDENT OR CHILD CARE EXPENSES: Child Care Expenses $ Other Employment Related DDC Costs TOTAL: _______ AVERAGE MONTHLY EXPENSE (divide total by 12 or number of months being paid if less than 12) This is a worksheet only and does not obligate you in any way. If you decide to participate in either of the expense reimbursement accounts or in both of them, there may be a monthly administration fee to be payroll deducted. Remember that you should review you tax situation carefully as to the tax advantage of the dependent care tax credit compared with participation in the dependent care expense reimbursement portion of the Section 125 Flexible Benefit Plan.
7
SECTION 125 FLEXIBLE BENEFITS PLAN
PARTICIPANT GUIDELINES FOR SPENDING ACCOUNTS- Medical Expense Reimbursement
- Dependent Care Reimbursement
PREPARED BY:
First Financial Administrators, Inc.
For your Employer’s Plan
8

WE ARE COMMITTEDFirst Financial Administrators, Inc. is dedicated to providing excellent
service to our customers and are delighted to serve as your cafeteria
plan service provider. Our role is to process your requests for
reimbursement according to the plan designed by your employer.
» There are two types of Flexible Spending Accounts (FSAs):
The first is unreimbursed medical (URM) and the second is
dependent day care (DDC).
» Your participation in an FSA program allows a portion of your
salary to be redirected to provide reimbursement for these
types of expenses on a tax-exempt basis.
» At the beginning of each plan year, you elect a specific dollar
amount for each FSA you wish to participate.
» Participation in one or both FSAs can save you money by
reducing your taxable income. This is because taxes will be
calculated after the elected amount is deducted from your salary.
» If applicable, your taxable income will be reduced for Social
Security purposes; therefore, there may be a corresponding
reduction In Social Security benefits.
» Once you have elected your annual amount, you cannot change
your election unless you experience a change in family status.
See Election Irrevocability
» To ensure that you are aware of your account balance at all
times, we send a new explanation of benefits with each claim
that is paid. The explanation of benefits will provide you with
information regarding your account balance, claims paid to
date, and claims pending.
» We send notifications 45 days prior to the end of the plan year. The notification reflects your current available balance. You can view account information by logging into our secure website.
Section 125 Flexible Spending AccountFirst Financial Administrators, Inc.
FILING A CLAIMBefore submitting your claim, make sure you have had
the service(s).
TO FILE YOUR CLAIM
1. Complete a claim form, and be sure to sign and date it.
2. Attach a legible receipt(s) from the service provided or an EOB (Explanation Of Benefits) showing:
» A description of the service or a list of supplies furnished.
» The charge(s) for each service.
» The date(s) of service.
» The name of the person(s) receiving the service.
» The amount you are responsible for.
3. For convenient direct deposit, complete the AutomaticDeposit Agreement form.
Or use your FFA Benefits Card
REQUESTING SERVICES (Toll-free)For Inquires: 1-866-853-3539
For Claim Forms: www.ffga.com
To Submit Claims by Fax: 1-800-298-7785
9

ELECTION IRREVOCABILITYYou may not make changes before the beginning of the next plan
year unless there is a qualified change in status (as permitted by
your plan) that affects Eligibility.
Qualified changes in status may include:
» Change in employee’s legal marital status
» Change in number of tax dependents
» Change in employment status that affects eligibility
» Dependent satisfies or ceases to satisfy eligibility requirements
» Change in residence that affects eligibility
» Judgment, decree, or court order dictating provision of coverage
» Entitlement of Medicare or Medicaid (URM only)
» Change in cost of the benefit (DDC only)
• Addition or elimination of benefit option
• Change in coverage of spouse or dependent under his/her employer’s plan
• Significant curtailment of coverage
If a change in status occurs, you may make changes consistent with
the qualifying event or as otherwise defined by your plan document.
See your plan Sponsor for further details about making changes.
Dollar Limits
Unreimbursed Medical Account:
Your plan sponsor determines the maximum benefit that may
be elected. Please see your employer for the maximum benefit
amount allowed under your plan.
Note: Due to Healthcare Reform, all URM Accounts will have an annual maximum of
$2,500 starting January 1, 2013.
Dependent Daycare Account:
This reimbursement (when aggregated with all other dependent
care reimbursements during the same calendar year) may not
exceed the least of the following:
» $5,000, or
» $2,500, if married but filing separate tax returns
Use-it-or-lose-it-Rule
Money remaining in your FSA account(s) will not be returned to
you at the end of the plan year. Any amount remaining after the
end of the runoff or grace period, if your employer offers one, will
be forfeited. Because of the use-it-or-lose-it rule, it is important
for you to carefully estimate your out-of-pocket URM and DDC
expenses for the upcoming plan year.
TERMINATION OF EMPLOYMENTURM Account:
Your salary redirections will end; however, you may still file claims
for dates of service that were incurred within your employment
period. You have 90 days after termination to submit a claim.
DDC Account:
If you have not received reimbursement for all contributions
made to your DDC account upon termination, you have 90 days
after the end of the plan year to submit a claim.
COBRA
COBRA does not apply to DDC. However, it may apply to your
URM account and allow you to continue participation in your URM,
thus allowing you to receive reimbursement for medical expenses
incurred after your employment termination if:
» The plan sponsor is subject to COBRA, and
» When you terminate employment and you have contributed
more for URM than you have received in URM benefits.
Note: Under COBRA you must elect coverage within 60 days and continue to submit
contributions to your employer to continue coverage under your URM account for the
current year.
General IRS Rules & InformationThe following rules apply to both URM and DDC FSAs
10

UNREIMBURSED MEDICAL FSAAlmost every person has a number of necessary and
predictable expenses that are not paid by their insurance
plans. You can save money by putting that amount directly
into your Unreimbursed Medical FSA. The FSA will help you
pay for these predictable expenses with your pre-tax dollars.
Please be aware of change in tax law – Beginning Jan. 1,
2011, money from flexible spending accounts will no longer be
available to pay for most over-the-counter drugs and medicines
without a doctor’s prescription.
ELIGIBLE EXPENSESWith the FSA, you can pay out-of-pocket health care expenses for yourself, your spouse and
all of your eligibile dependents for health, dental, and vision care expenses. The services must
be incurred while you are actively participating in the FSA plan. The eligible expenses may
be reimbursed regardless of whether you, your spouse or dependents are covered by your
employer’s medical, dental, or health plan.
Expenses for medical care will be limited to expenses incurred primarily for the prevention or
improvement of a physical or mental defect or illness. An expense that is merely beneficial to your
general health is not an eligible expense. It must be an expense to treat an existing medical condition.
INELIGIBLE EXPENSESSome expenses that you incur during your plan year may not be eligible for reimbursement
under current IRS regulations.
» EXPENSES NOT YET INCURRED - Expenses that have been paid, but not yet incurred
(i.e. Prepayment of service), cannot be reimbursed until the service is rendered. Expenses don’t
necessarily have to be PAID, but merely incurred.
» PREMIUMS FOR INSURANCE - Premiums and payments to insurance policies are not eligible
for reimbursement.
» EXPENSES PAID BY ANOTHER PLAN OR THIRD PARTY - Expenses that have already been
paid by an insurance company or other reimbursement through your FSA plan.
» EXPENSES INCURRED AFTER TERMINATION/SEPARATION FROM YOUR EMPLOYER -
If you are no longer participating in the FSA plan through your employer (termination, resignation, etc)
any claims incurred after your participation ends are not eligible for reimbursement.
COMMON ELIGIBLE EXPENSES
» Co-Payments
» Co-Insurance
» Deductibles
» Over-the Counter Drugs
(with physician’s prescription)
» Dental Treatment
» Orthodontia
» Lab Fees
» X-Rays
» Vision Expenses
» Lasik Surgery
» Physical Therapy
» Chiropractor Services
» Acupuncture
» Eye Contact Solution
» Eye Drops
COMMON INELIGIBLE EXPENSES
» Cosmetic Surgery
» Teeth Whitening
» Veneers
» Botox
» Non Prescribed Vitamins
and Supplements
» Toiletries
» Medical Insurance Premiums
» Health Club Membership Fees
General IRS Rules & Information
11

» Acupuncture» Alcohol and drug rehabilitation
expenses» Ambulance» Anesthetist» Artificial limbs and teeth» Birth control pills» Blood donor (expense)» Chiropodist» Chiropractor» Christian Science Practitioners» Certain corrective surgery» Contact lens solution
and cleaner» Co-payment for health
insurance» Dental care and dentures» Drugs and medical supplies» Examinations» Eye exam, eyeglasses,
and contacts» Gynecologist
» Hearing aids and batteries» Home health care» Hospital and skilled nursing
facility expenses» Laboratory fees» Lip-reading lessons» Midwife» Nursing care» Obstetrical expense» Oculist» Operations and related
treatments» Optometrist» Orthodontist**» Osteopath» Outpatient clinic» Over-the-Counter Medications
(with physician’s prescription) » Pediatrician» Physician» Podiatrist» Practical nurse
» Prescription drugs» Psychiatrist» Psychologist» Rental or purchase of medical
equipment, including special equipment for use by handicapped persons
» Sanitarium» Stop Smoking Programs
and Drugs» Support or corrective devices» Surgery» Therapy» Transportation expenses» Weight Loss for Obesity*» X-ray
» Dancing or swimming lessons» Medications purchased
outside US» Expenses reimbursed under
any health plan or other source» Health Club Dues» Face creams, moisturizers, etc.» Hair removal treatments/waxes» Vacation» Cosmetic Surgery» Teeth Whitening» Vitamins taken for overall
health» OTC Medications not for
Medical Care» Toothpaste/Toothbrushes» Mouth washes, oral
anesthetics, etc.
EXAMPLES OF ELIGIBLE MEDICAL CARE EXPENSESThe following lists are examples of the types of expenses that
may or may not be reimbursed. These lists are not intended to
be complete, as other expenses may also be eligible or ineligible
under federal tax law or under employer’s plan. To be eligible
under an FSA URM account, the medical expense(s) must be
incurred for medical care that is not reimbursed from any other
source. Medical care means the drug or service is needed to
treat a medical condition. First Financial Administrators, Inc. may
request additional information from you to substantiate that an
expense is for health care.
ELIGIBLE MEDICAL EXPENSES INELIGIBLE EXPENSES
General IRS Rules & Information
* This service requires a letter of medical necessity with a diagnosis from the referring physician.** Requires an active orthodontia contract be on file.
12

DEPENDENT CARE FSAThe Dependent Care FSA allows you to pay for day care
expenses for your qualified dependent/child with pre-tax dollars
while you (and your spouse) are working, seeking employment,
or attending school as a full-time student for at least 5 months
during the year.
ELIGIBILITY REQUIREMENTSEligible dependents must be claimed as an exemption on your tax
return. These dependents can include step-children, grandchildren,
adopted children, or foster children. In a divorce situation, you must
have custody of the child in order for the child to be considered
an eligible dependent. Under IRS regulations, eligible dependents
are further defined as: under the age of 13, and/or physically or
mentally unable to care for themselves, such as a disabled spouse,
disabled child, or elderly parents that live with you.
ELIGIBLE EXPENSESEligible dependent care expenses are those expenses you
must pay for the care of a dependent so that you and your
spouse can work. The care may be provided in your home or
at a licensed center outside of your home. If the care is in your
home, the service cannot be provided by another child of yours
under the age of 19, by your spouse, or by your dependents.
INELIGIBLE EXPENSESOnly those dependents care expenses that enable you and
your spouse to work are eligible. Some expenses that you incur
during your plan year may not be eligible for reimbursement
under current IRS regulations
» Educational Costs
» Weekends/Evening-out babysitting
» Transportation, books, clothing, food, activities,
entertainment, and registration fees are ineligible if these
expenses are shown separately on your bill
COMMON ELIGIBLE EXPENSES
» Day Camps
» Before/After School Care
» Babysitters/Day Care Centers
» Au Pair
» Nanny
» Nursery School
COMMON INELIGIBLE EXPENSES
» Registration Fees
» Care for child while not working
» Kindergarten
» Food/Activity expenses if
separate from cost of care
» Care provided by anyone
under age 19
» Pre-School
» Books and Supplies
» Field Trips
General IRS Rules & InformationThe following rules apply to both URM and DDC FSAs
13

THE REIMBURSEMENT PROCESSREIMBURSEMENTS- The healthcare/medical FSAs are pre-funded; therefore, you are eligible to receive reimbursement up to
your elected annual contribution from the beginning of your FSA plan year. The healthcare/medical FSA funds that are reimbursed
to you will be recovered as your deductions are taken from your paycheck throughout the plan year. Dependent Care FSAs are
NOT pre-funded; therefore, you will only receive reimbursement up to your year-to-date contributions from payroll deductions.
The remainder of the reimbursement request is paid when additional funds are received from payroll deductions.
PAYMENT METHOD CHOICE- For Unreimbursed Medical expenses
you may pay with your FFA Benefits Flex Card at the time you incur the
expense, or pay the provider out-of-pocket and file a manual (paper)
claim to receive a reimbursement. The FFA Benefits Flex Card is only
available for Healthcare/Medical FSAs.
MANUAL CLAIMS-To obtain reimbursement from your FSA, you must
complete a manual claim form and attach all itemized receipts from the
service provider. Cancelled checks, bankcard/credit card receipts, and
credit card statements are NOT acceptable forms of documentation.
The receipt must come from the service provider or the Explanation of
Benefits from your medical health carrier and must include the following
information:
» Patient name
» Date of service incurred
» Provider / Merchant name
» Amount of your out-of-pocket charge incurred
» Type of service incurred
» Must include prescription number
REMEMBER-You must sign and date all claim forms.
FFGA recommends submitting an Explanation of Benefits (EOB)
from your insurance company, if available.
CLAIMS PROCESSING AND PAYMENTSAll claim reimbursements are handled with strict adherence to IRS adjudication and reporting regulations.
Claims are processed daily, and our turn around time upon receipt is 3-5 business days and during peak
periods (December-March) 5-10 business days. Your reimbursement check will be mailed to your home
address on file. You may also elect to receive payment via direct deposit. You have a 2 ½ month grace
period (employer permitting) to incur claims with an additional 2 weeks to file claims.
Online Service to View Account Information, visit www.ffga.com
Claims Information
14

FFA Benefits Flex CardMedical reimbursement accounts only
BENEFITS FLEX CARDThe First Financial Administrators, Inc. Benefits Flex Card is avail-able for Medical Reimbursement Flexible Spending Accounts. Cards can be issued to spouses and dependent children (ages 18 to 26) for no additional fee. The initial cards are free, but if a re-placement card is issued, the cost is $10.00 per card and will be de-ducted from your account balance. Cards are good for three years from the issue date as long as you participate each consecutive plan year. Claims can also be submitted directly for reimbursement. If funds remain in your account after the end of the plan year, you may use the debit card during the 2½ month grace period (if your employer has elected to participate in the grace period option). The system will deduct all remaining funds from your old plan year and then deduct any balance from the new plan year, if you con-tinue to participate. New cards (not replacement cards) are only activated with the upcoming plan year -- they are not activated to use money from the prior plan year.
The IRS requires validation of most transactions – you must sub-mit receipts for verification of expenses when requested. If you fail to substantiate by providing a receipt to us within 60 days of purchase, your card will be suspended until the necessary receipt or explanation of benefits from your insurance provider is received. Claim forms can be found on our website, www.ffga.com.
Copies can either be mailed to: First Financial Administrators, Inc. P.O. Box 670329 Houston, TX 77267-0329
First Financial Administrators, Inc. can provide you with a list of eligible expenses associated with your Medical Reimbursement Flexible Spending Account. This card is a signature debit card and does not require a PIN for use. Transactions must always be submitted as “credit.” Participants may review Flexible Spending Account balances online at www.ffga.com.
CALL (866) 853-FLEX FOR MORE INFORMATION.
(Your FFA Benefits Flex Card cannot be used past your termination date. If you have available funds in your account, a manual claim will be required.)
» Pharmacies – always use your debit card at the pharmacy
counter only.
» In-Store Pharmacies – If “merchant code” is programmed
“pharmacy,” the expense will be authorized. However, if
the MasterCard transaction code is programmed “grocery/retail,”
the transaction may be denied. The debit card may
not work, and the expense may be declined in some
grocery/discount stores.
» Physician Offices
» Specialist Physician Offices
» Dental Offices
» Over-the-counter drugs (must be accompanied by a Physician’s Rx)
» Vision Care Providers
» Medical Facilities
» Medical Clinics
» Hospitals, including Emergency Rooms
WHERE TO USE YOUR DEBIT CARD FOR ELIGIBLE UNREIMBURSED MEDICAL EXPENSES:
or faxed to: (800) 298-7785
15

ADDRESS CHANGE? ❏ Yes ❏ No
NAME ______________________________________________________
MAILING ADDRESS __________________________________________
______________________________________________________________
CITY ____________________________ STATE _____ ZIP______________
EMPLOYER _________________________________________________
SOCIAL SECURITY # _________________________________________
E-MAIL ADDRESS ____________________________________________
TELEPHONE ( ______ ) ________________________________________
PARTICIPANT INFORMATION
BENEFIT TYPE (please check as appropriate)
NAME ______________________________________________________
ADDRESS ____________________________________________________
CITY ____________________________ STATE _____ ZIP______________
SS # ________________________________________________________
TAX ID # _____________________________________________________
_______________________________________________________________SIGNATURE OF PROVIDER
COMPLETE ONLY FOR DEPENDENT CARE PROVIDER
NAME ______________________________________________________
AMOUNT DUE $____________________ DATE _____________________
SERVICE PERFORMED ________________________________________ _
I certify that the dental procedure for the above patient
❏ HAS BEEN COMPLETED ❏ IS IN PROGRESS
_______________________________________________________________SIGNATURE OF DENTIST / ORTHODONTIST
COMPLETE ONLY FOR ORTHODONTIA REIMBURSEMENT
Flexible Benefits Reimbursement VoucherPO Box 670329, Houston, TX 77267-0326 • Telephone: (866) 853-3539 • Fax: (800) 298-7785
ADDITIONAL FORMS AVAILABLE AT: www.ffga.com and click on Participant Forms
I hereby affirm that, to the best of my knowledge, all expenses listed above are eligible for reimbursement under Section 105(h) or 129 of the IRS Code and in accordance with my contract with
First Financial Administrators, Inc. I further certify that these expenses have not been, nor will not be, reimbursed under any other health plan coverage. If you need verification of the eligibility of
an expense, please contact First Financial Administrators, Inc. at 1-866-853-3539.
SIGNATURE _________________________________________________
DATE _________________________________________________________
❏ Please send me additional envelopes (additional voucher given with every reimbursement)
NOTE: If you have direct deposit, First Financial Administrators, Inc. will not pay bank
charges for Insufficient funds. Please call your financial Institution to verify deposit
before writing any checks on the amount
Mail or Fax Completed Form To: First Financial Administrators, Inc. • P.O. Box 670329, Houston, TX 77267-0329 • Fax Number: 1-800-298-7785
DATE OF SERVICE FAMILY MEMBER DESCRIPTION OF EXPENSE AMOUNT
GRAND TOTAL ALL PAGES
❏ MEDICAL REIMBURSEMENT ❏ DEPENDENT CARE REIMBURSEMENT ❏ PREMIUM REIMBURSEMENT
IMPORTANT NOTICE Effective January 1, 2011, all over-the-counter drugs eligible for reimbursement must be accompanied by a doctor’s prescription and a reimbursement voucher.
$0.00
16

DATE OF SERVICE FAMILY MEMBER DESCRIPTION OF EXPENSE AMOUNT
SUB-TOTAL THIS PAGE
MEDICAL REIMBURSEMENT SUBMISSION GUIDELINES:ACCEPTABLE DOCUMENTATION to accompany the reimbursement voucher:
1. Professional bill or receipt that includes:» Provider of service» Type of service rendered» Original date of service» Charges for the service
2. Insurance company Explanation of Benefits
3. Pharmacy statement that includes Rx number and name of the prescription
DAYCARE SUBMISSION GUIDELINES:ACCEPTABLE DOCUMENTATION to accompany the reimbursement voucher:
1. Vouchers for Dependent Care signed by the Provider. Voucher must also be completed with the Provider’s tax identification number or Social Security number and dates of service, Or...
2. Voucher with receipt from Provider, including Provider name, Provider signature, dates of service, amount for service, and tax identification/social security number.
I.R.S Regulations prevent us from reimbursing dependent care yearly contracts. Monthly submissions are required.
UNACCEPTABLE DOCUMENTATION
1. Cancelled checks / Credit card receipts
2. Bill or receipt that only shows a balance forward or previous balance
3. Cash register receipt
Note: It is important to note that the date of service, not the date of payment, must fall within the dates of the plan year for which you are enrolled.
Reimbursement ItemizationContinued
$0.00
17

ADDITIONAL CARDSDEPENDENT CARDS – ISSUED TO SPOUSES AND/OR DEPENDENT CHILDREN (AGES 18-26)
NAME RELATIONSHIP DATE
I ACCEPT RESPONSIBILITY FOR THE FOLLOWING:
• All card transactions will be solely for qualified expenditures incurred (not billed or paid) during the plan year;
• To the extent that if I misrepresent any card transaction as a qualified expenditure when it is a non-qualified expenditure, I hold you harmless for whatever penalties and consequences that may occur as a result of my actions;
• If I misrepresent any card transaction on a non-qualified expenditure, I must immediately repay all expenses to the account upon notification; if not repaid, I understand the amount will be considered taxable income.
• I agree to submit expense receipts to the third party administrator for all purchases when requested; If failure to substantiate, card will be suspended.
• Each time I present the card for payment, I will sign a receipt evidencing that the expense has been incurred and reaffirming my representation that it is a qualified expenditure that has not been and will not be reimbursed from any other source.
PLEASE MAIL COMPLETED FORM TO: FIRST FINANCIAL ADMINISTRATORS, INC. • PO BOX 670329, HOUSTON TX 77267-0329
PHONE: 1-800-523-8422 OR 281-847-8422 FAX: 1-800-298-7785
Debit Card AgreementMedical reimbursement accounts only
PLEASE PRINT
SCHOOL DISTRICT ________________________________________ ________________________________________
NAME __________________________________________________________________________________________
SOCIAL SECURITY NUMBER ________________________________________ _______________________________
MAILING ADDRESS ________________________________________ ________________________________________
CITY / STATE / ZIP ________________________________________ _________________________________________
DAYTIME TELEPHONE NUMBER ________________________________________ ___________________________
E-MAIL ADDRESS ________________________________________ __________________________________________
SIGNATURE ________________________________________ ____________________ DATE _____________________
DEBIT CARD VALID FOR 3 YEARS OF CONTINUAL PARTICIPATION
18

1-800-327-9728 • HumanaVoluntaryBenefits.com
This is not a complete disclosure of plan qualifications and limitations. Your broker will provide you with specific limitations and exclusions as contained in the Regulatory and Technical Information Guide. Please review this information before applying for coverage. The amount of benefits provided depends on the plan selected. Premiums will vary according to the selection made.
Insured by Kanawha Insurance Company, a Humana company.
Virgina
Policy: 8000Underwritten by Kanawha Insurance Company
Disability Income Plus
Disability Income Plus provides a monthly disability income benefit as a result of a non-occupational “off-the-job” accident or sickness. If you’re totally disabled by an accident or illness, Disability Income Plus can be there to help, helping pay the bills that won’t go away just because you can’t work: housing costs, food, car payments, and additional medical costs. You can focus on a full recovery and successful return to the workplace.
Coverage type Disability Income Plus is a group disability income insurance policy that provides a monthly disability income benefit due to a non-occupational “off-the-job” accident or injury.
Benefit amount Minimum benefit of $100 and maximum benefit of $5,000 per month, not to exceed 65% of base monthly income.
Plan design Accident & Sickness: Provides coverage for disabilities caused by either an accidental injury or sickness. Pregnancy is covered the same as any other illness.
Benefit period Twelve months
Elimination period Provides non-occupational coverage for injuries after 0, 7, 14 or 30 days and off-the job sicknesses after 7, 14 or 30 days of total disability (depending on your selection).
Definition of disability Total disability: the complete inability to perform the material and substantial duties of the employee’s regular occupation as certified by the employee’s attending physician. Regular occupation is that which the employee was performing immediately before total disability began. The total disability must be the result of and accident, if accident only coverage is shown in the policy specification, or accident or sickness, if accident and sickness coverage is shown in the policy specifications. The employee must be under the regular care of a physician and not, in fact, engaged in any employment or occupation for wages or profit.
Recurrent disability: total disability that is due to the same or related causes as a prior period of disability, follows a prior period for which a monthly benefit was paid, and occurs within 180 days after the end of a prior period for which a monthly benefit was paid.
Presented by Benefit amount selected
Premium amount per paycheck
19

1-800-327-9728 • HumanaVoluntaryBenefits.comPolicy: 8000Underwritten by Kanawha Insurance Company
Disability Income Plus rates
Disability Income Plus ratesTenthly deductions, elimination period: 0/7
Age Benefit amount
$100 $200 $300 $400 $500 $600 $700 $800 $900 $1,000
18-50 $4.63 $9.26 $13.89 $18.52 $23.15 $27.78 $32.41 $37.04 $41.67 $46.30
51-64 $6.74 $13.48 $20.22 $26.96 $33.70 $40.44 $47.18 $53.92 $60.66 $67.40
65+ $10.44 $20.88 $31.32 $41.76 $52.20 $62.64 $73.08 $83.52 $93.96 $104.40
$1,100 $1,200 $1,300 $1,400 $1,500 $1,600 $1,700 $1,800 $1,900 $2,000
18-50 $50.93 $55.56 $60.19 $64.82 $69.45 $74.08 $78.71 $83.34 $87.97 $92.60
51-64 $74.14 $80.88 $87.62 $94.36 $101.10 $107.84 $114.58 $121.32 $128.06 $134.80
65+ $114.84 $125.28 $135.72 $146.16 $156.60 $167.04 $177.48 $187.92 $198.36 $208.80
$2,100 $2,200 $2,300 $2,400 $2,500 $2,600 $2,700 $2,800 $2,900 $3,000
18-50 $97.23 $101.86 $106.49 $111.12 $115.75 $120.38 $125.01 $129.64 $134.27 $138.90
51-64 $141.54 $148.28 $155.02 $161.76 $168.50 $175.24 $181.98 $188.72 $195.46 $202.20
65+ $219.24 $229.68 $240.12 $250.56 $261.00 $271.44 $281.88 $292.32 $302.76 $313.20
$3,100 $3,200 $3,300 $3,400 $3,500 $3,600 $3,700 $3,800 $3,900 $4,000
18-50 $143.53 $148.16 $152.79 $157.42 $162.05 $166.68 $171.31 $175.94 $180.57 $185.20
51-64 $208.94 $215.68 $222.42 $229.16 $235.90 $242.64 $249.38 $256.12 $262.86 $269.60
65+ $323.64 $334.08 $344.52 $354.96 $365.40 $375.84 $386.28 $396.72 $407.16 $417.60
$4,100 $4,200 $4,300 $4,400 $4,500 $4,600 $4,700 $4,800 $4,900 $5,000
18-50 $189.83 $194.46 $199.09 $203.72 $208.35 $212.98 $217.61 $222.24 $226.87 $231.50
51-64 $276.34 $283.08 $289.82 $296.56 $303.30 $310.04 $316.78 $323.52 $330.26 $337.00
65+ $428.04 $438.48 $448.92 $459.36 $469.80 $480.24 $490.68 $501.12 $511.56 $522.00
Tenthly deductions, elimination period: 7/7
Age Benefit amount
$100 $200 $300 $400 $500 $600 $700 $800 $900 $1,000
18-50 $4.57 $9.14 $13.71 $18.28 $22.85 $27.42 $31.99 $36.56 $41.13 $45.70
51-64 $6.72 $13.44 $20.16 $26.88 $33.60 $40.32 $47.04 $53.76 $60.48 $67.20
65+ $10.26 $20.52 $30.78 $41.04 $51.30 $61.56 $71.82 $82.08 $92.34 $102.60
$1,100 $1,200 $1,300 $1,400 $1,500 $1,600 $1,700 $1,800 $1,900 $2,000
18-50 $50.27 $54.84 $59.41 $63.98 $68.55 $73.12 $77.69 $82.26 $86.83 $91.40
51-64 $73.92 $80.64 $87.36 $94.08 $100.80 $107.52 $114.24 $120.96 $127.68 $134.40
65+ $112.86 $123.12 $133.38 $143.64 $153.90 $164.16 $174.42 $184.68 $194.94 $205.20
$2,100 $2,200 $2,300 $2,400 $2,500 $2,600 $2,700 $2,800 $2,900 $3,000
18-50 $95.97 $100.54 $105.11 $109.68 $114.25 $118.82 $123.39 $127.96 $132.53 $137.10
51-64 $141.12 $147.84 $154.56 $161.28 $168.00 $174.72 $181.44 $188.16 $194.88 $201.60
65+ $215.46 $225.72 $235.98 $246.24 $256.50 $266.76 $277.02 $287.28 $297.54 $307.80
$3,100 $3,200 $3,300 $3,400 $3,500 $3,600 $3,700 $3,800 $3,900 $4,000
18-50 $141.67 $146.24 $150.81 $155.38 $159.95 $164.52 $169.09 $173.66 $178.23 $182.80
51-64 $208.32 $215.04 $221.76 $228.48 $235.20 $241.92 $248.64 $255.36 $262.08 $268.80
65+ $318.06 $328.32 $338.58 $348.84 $359.10 $369.36 $379.62 $389.88 $400.14 $410.40
$4,100 $4,200 $4,300 $4,400 $4,500 $4,600 $4,700 $4,800 $4,900 $5,000
18-50 $187.37 $191.94 $196.51 $201.08 $205.65 $210.22 $214.79 $219.36 $223.93 $228.50
51-64 $275.52 $282.24 $288.96 $295.68 $302.40 $309.12 $315.84 $322.56 $329.28 $336.00
65+ $420.66 $430.92 $441.18 $451.44 $461.70 $471.96 $482.22 $492.48 $502.74 $513.00
20

1-800-327-9728 • HumanaVoluntaryBenefits.comPolicy: 8000Underwritten by Kanawha Insurance Company
Disability Income Plus rates
Disability Income Plus ratesTenthly deductions, elimination period: 14/14
Age Benefit amount
$100 $200 $300 $400 $500 $600 $700 $800 $900 $1,000
18-50 $3.62 $7.24 $10.86 $14.48 $18.10 $21.72 $25.34 $28.96 $32.58 $36.20
51-64 $5.66 $11.32 $16.98 $22.64 $28.30 $33.96 $39.62 $45.28 $50.94 $56.60
65+ $9.43 $18.86 $28.29 $37.72 $47.15 $56.58 $66.01 $75.44 $84.87 $94.30
$1,100 $1,200 $1,300 $1,400 $1,500 $1,600 $1,700 $1,800 $1,900 $2,000
18-50 $39.82 $43.44 $47.06 $50.68 $54.30 $57.92 $61.54 $65.16 $68.78 $72.40
51-64 $62.26 $67.92 $73.58 $79.24 $84.90 $90.56 $96.22 $101.88 $107.54 $113.20
65+ $103.73 $113.16 $122.59 $132.02 $141.45 $150.88 $160.31 $169.74 $179.17 $188.60
$2,100 $2,200 $2,300 $2,400 $2,500 $2,600 $2,700 $2,800 $2,900 $3,000
18-50 $76.02 $79.64 $83.26 $86.88 $90.50 $94.12 $97.74 $101.36 $104.98 $108.60
51-64 $118.86 $124.52 $130.18 $135.84 $141.50 $147.16 $152.82 $158.48 $164.14 $169.80
65+ $198.03 $207.46 $216.89 $226.32 $235.75 $245.18 $254.61 $264.04 $273.47 $282.90
$3,100 $3,200 $3,300 $3,400 $3,500 $3,600 $3,700 $3,800 $3,900 $4,000
18-50 $112.22 $115.84 $119.46 $123.08 $126.70 $130.32 $133.94 $137.56 $141.18 $144.80
51-64 $175.46 $181.12 $186.78 $192.44 $198.10 $203.76 $209.42 $215.08 $220.74 $226.40
65+ $292.33 $301.76 $311.19 $320.62 $330.05 $339.48 $348.91 $358.34 $367.77 $377.20
$4,100 $4,200 $4,300 $4,400 $4,500 $4,600 $4,700 $4,800 $4,900 $5,000
18-50 $148.42 $152.04 $155.66 $159.28 $162.90 $166.52 $170.14 $173.76 $177.38 $181.00
51-64 $232.06 $237.72 $243.38 $249.04 $254.70 $260.36 $266.02 $271.68 $277.34 $283.00
65+ $386.63 $396.06 $405.49 $414.92 $424.35 $433.78 $443.21 $452.64 $462.07 $471.50
Tenthly deductions, elimination period: 30/30
Age Benefit amount
$100 $200 $300 $400 $500 $600 $700 $800 $900 $1,000
18-50 $2.29 $4.58 $6.87 $9.16 $11.45 $13.74 $16.03 $18.32 $20.61 $22.90
51-64 $3.88 $7.76 $11.64 $15.52 $19.40 $23.28 $27.16 $31.04 $34.92 $38.80
65+ $6.97 $13.94 $20.91 $27.88 $34.85 $41.82 $48.79 $55.76 $62.73 $69.70
$1,100 $1,200 $1,300 $1,400 $1,500 $1,600 $1,700 $1,800 $1,900 $2,000
18-50 $25.19 $27.48 $29.77 $32.06 $34.35 $36.64 $38.93 $41.22 $43.51 $45.80
51-64 $42.68 $46.56 $50.44 $54.32 $58.20 $62.08 $65.96 $69.84 $73.72 $77.60
65+ $76.67 $83.64 $90.61 $97.58 $104.55 $111.52 $118.49 $125.46 $132.43 $139.40
$2,100 $2,200 $2,300 $2,400 $2,500 $2,600 $2,700 $2,800 $2,900 $3,000
18-50 $48.09 $50.38 $52.67 $54.96 $57.25 $59.54 $61.83 $64.12 $66.41 $68.70
51-64 $81.48 $85.36 $89.24 $93.12 $97.00 $100.88 $104.76 $108.64 $112.52 $116.40
65+ $146.37 $153.34 $160.31 $167.28 $174.25 $181.22 $188.19 $195.16 $202.13 $209.10
$3,100 $3,200 $3,300 $3,400 $3,500 $3,600 $3,700 $3,800 $3,900 $4,000
18-50 $70.99 $73.28 $75.57 $77.86 $80.15 $82.44 $84.73 $87.02 $89.31 $91.60
51-64 $120.28 $124.16 $128.04 $131.92 $135.80 $139.68 $143.56 $147.44 $151.32 $155.20
65+ $216.07 $223.04 $230.01 $236.98 $243.95 $250.92 $257.89 $264.86 $271.83 $278.80
$4,100 $4,200 $4,300 $4,400 $4,500 $4,600 $4,700 $4,800 $4,900 $5,000
18-50 $93.89 $96.18 $98.47 $100.76 $103.05 $105.34 $107.63 $109.92 $112.21 $114.50
51-64 $159.08 $162.96 $166.84 $170.72 $174.60 $178.48 $182.36 $186.24 $190.12 $194.00
65+ $285.77 $292.74 $299.71 $306.68 $313.65 $320.62 $327.59 $334.56 $341.53 $348.50
21

1-800-327-9728 • HumanaVoluntaryBenefits.comPolicy: 8000Underwritten by Kanawha Insurance Company
Disability Income Plus rates
Disability Income Plus ratesMonthly deductions, elimination period: 0/7
Age Benefit amount
$100 $200 $300 $400 $500 $600 $700 $800 $900 $1,000
18-50 $3.86 $7.72 $11.58 $15.44 $19.30 $23.16 $27.02 $30.88 $34.74 $38.60
51-64 $5.62 $11.24 $16.86 $22.48 $28.10 $33.72 $39.34 $44.96 $50.58 $56.20
65+ $8.70 $17.40 $26.10 $34.80 $43.50 $52.20 $60.90 $69.60 $78.30 $87.00
$1,100 $1,200 $1,300 $1,400 $1,500 $1,600 $1,700 $1,800 $1,900 $2,000
18-50 $42.46 $46.32 $50.18 $54.04 $57.90 $61.76 $65.62 $69.48 $73.34 $77.20
51-64 $61.82 $67.44 $73.06 $78.68 $84.30 $89.92 $95.54 $101.16 $106.78 $112.40
65+ $95.70 $104.40 $113.10 $121.80 $130.50 $139.20 $147.90 $156.60 $165.30 $174.00
$2,100 $2,200 $2,300 $2,400 $2,500 $2,600 $2,700 $2,800 $2,900 $3,000
18-50 $81.06 $84.92 $88.78 $92.64 $96.50 $100.36 $104.22 $108.08 $111.94 $115.80
51-64 $118.02 $123.64 $129.26 $134.88 $140.50 $146.12 $151.74 $157.36 $162.98 $168.60
65+ $182.70 $191.40 $200.10 $208.80 $217.50 $226.20 $234.90 $243.60 $252.30 $261.00
$3,100 $3,200 $3,300 $3,400 $3,500 $3,600 $3,700 $3,800 $3,900 $4,000
18-50 $119.66 $123.52 $127.38 $131.24 $135.10 $138.96 $142.82 $146.68 $150.54 $154.40
51-64 $174.22 $179.84 $185.46 $191.08 $196.70 $202.32 $207.94 $213.56 $219.18 $224.80
65+ $269.70 $278.40 $287.10 $295.80 $304.50 $313.20 $321.90 $330.60 $339.30 $348.00
$4,100 $4,200 $4,300 $4,400 $4,500 $4,600 $4,700 $4,800 $4,900 $5,000
18-50 $158.26 $162.12 $165.98 $169.84 $173.70 $177.56 $181.42 $185.28 $189.14 $193.00
51-64 $230.42 $236.04 $241.66 $247.28 $252.90 $258.52 $264.14 $269.76 $275.38 $281.00
65+ $356.70 $365.40 $374.10 $382.80 $391.50 $400.20 $408.90 $417.60 $426.30 $435.00
Monthly deductions, elimination period: 7/7
Age Benefit amount
$100 $200 $300 $400 $500 $600 $700 $800 $900 $1,000
18-50 $3.81 $7.62 $11.43 $15.24 $19.05 $22.86 $26.67 $30.48 $34.29 $38.10
51-64 $5.60 $11.20 $16.80 $22.40 $28.00 $33.60 $39.20 $44.80 $50.40 $56.00
65+ $8.55 $17.10 $25.65 $34.20 $42.75 $51.30 $59.85 $68.40 $76.95 $85.50
$1,100 $1,200 $1,300 $1,400 $1,500 $1,600 $1,700 $1,800 $1,900 $2,000
18-50 $41.91 $45.72 $49.53 $53.34 $57.15 $60.96 $64.77 $68.58 $72.39 $76.20
51-64 $61.60 $67.20 $72.80 $78.40 $84.00 $89.60 $95.20 $100.80 $106.40 $112.00
65+ $94.05 $102.60 $111.15 $119.70 $128.25 $136.80 $145.35 $153.90 $162.45 $171.00
$2,100 $2,200 $2,300 $2,400 $2,500 $2,600 $2,700 $2,800 $2,900 $3,000
18-50 $80.01 $83.82 $87.63 $91.44 $95.25 $99.06 $102.87 $106.68 $110.49 $114.30
51-64 $117.60 $123.20 $128.80 $134.40 $140.00 $145.60 $151.20 $156.80 $162.40 $168.00
65+ $179.55 $188.10 $196.65 $205.20 $213.75 $222.30 $230.85 $239.40 $247.95 $256.50
$3,100 $3,200 $3,300 $3,400 $3,500 $3,600 $3,700 $3,800 $3,900 $4,000
18-50 $118.11 $121.92 $125.73 $129.54 $133.35 $137.16 $140.97 $144.78 $148.59 $152.40
51-64 $173.60 $179.20 $184.80 $190.40 $196.00 $201.60 $207.20 $212.80 $218.40 $224.00
65+ $265.05 $273.60 $282.15 $290.70 $299.25 $307.80 $316.35 $324.90 $333.45 $342.00
$4,100 $4,200 $4,300 $4,400 $4,500 $4,600 $4,700 $4,800 $4,900 $5,000
18-50 $156.21 $160.02 $163.83 $167.64 $171.45 $175.26 $179.07 $182.88 $186.69 $190.50
51-64 $229.60 $235.20 $240.80 $246.40 $252.00 $257.60 $263.20 $268.80 $274.40 $280.00
65+ $350.55 $359.10 $367.65 $376.20 $384.75 $393.30 $401.85 $410.40 $418.95 $427.50
22

1-800-327-9728 • HumanaVoluntaryBenefits.comPolicy: 8000Underwritten by Kanawha Insurance Company
Disability Income Plus rates
Disability Income Plus ratesMonthly deductions, elimination period: 14/14
Age Benefit amount
$100 $200 $300 $400 $500 $600 $700 $800 $900 $1,000
18-50 $3.02 $6.04 $9.06 $12.08 $15.10 $18.12 $21.14 $24.16 $27.18 $30.20
51-64 $4.72 $9.44 $14.16 $18.88 $23.60 $28.32 $33.04 $37.76 $42.48 $47.20
65+ $7.86 $15.72 $23.58 $31.44 $39.30 $47.16 $55.02 $62.88 $70.74 $78.60
$1,100 $1,200 $1,300 $1,400 $1,500 $1,600 $1,700 $1,800 $1,900 $2,000
18-50 $33.22 $36.24 $39.26 $42.28 $45.30 $48.32 $51.34 $54.36 $57.38 $60.40
51-64 $51.92 $56.64 $61.36 $66.08 $70.80 $75.52 $80.24 $84.96 $89.68 $94.40
65+ $86.46 $94.32 $102.18 $110.04 $117.90 $125.76 $133.62 $141.48 $149.34 $157.20
$2,100 $2,200 $2,300 $2,400 $2,500 $2,600 $2,700 $2,800 $2,900 $3,000
18-50 $63.42 $66.44 $69.46 $72.48 $75.50 $78.52 $81.54 $84.56 $87.58 $90.60
51-64 $99.12 $103.84 $108.56 $113.28 $118.00 $122.72 $127.44 $132.16 $136.88 $141.60
65+ $165.06 $172.92 $180.78 $188.64 $196.50 $204.36 $212.22 $220.08 $227.94 $235.80
$3,100 $3,200 $3,300 $3,400 $3,500 $3,600 $3,700 $3,800 $3,900 $4,000
18-50 $93.62 $96.64 $99.66 $102.68 $105.70 $108.72 $111.74 $114.76 $117.78 $120.80
51-64 $146.32 $151.04 $155.76 $160.48 $165.20 $169.92 $174.64 $179.36 $184.08 $188.80
65+ $243.66 $251.52 $259.38 $267.24 $275.10 $282.96 $290.82 $298.68 $306.54 $314.40
$4,100 $4,200 $4,300 $4,400 $4,500 $4,600 $4,700 $4,800 $4,900 $5,000
18-50 $123.82 $126.84 $129.86 $132.88 $135.90 $138.92 $141.94 $144.96 $147.98 $151.00
51-64 $193.52 $198.24 $202.96 $207.68 $212.40 $217.12 $221.84 $226.56 $231.28 $236.00
65+ $322.26 $330.12 $337.98 $345.84 $353.70 $361.56 $369.42 $377.28 $385.14 $393.00
Monthly deductions, elimination period: 30/30
Age Benefit amount
$100 $200 $300 $400 $500 $600 $700 $800 $900 $1,000
18-50 $1.91 $3.82 $5.73 $7.64 $9.55 $11.46 $13.37 $15.28 $17.19 $19.10
51-64 $3.23 $6.46 $9.69 $12.92 $16.15 $19.38 $22.61 $25.84 $29.07 $32.30
65+ $5.81 $11.62 $17.43 $23.24 $29.05 $34.86 $40.67 $46.48 $52.29 $58.10
$1,100 $1,200 $1,300 $1,400 $1,500 $1,600 $1,700 $1,800 $1,900 $2,000
18-50 $21.01 $22.92 $24.83 $26.74 $28.65 $30.56 $32.47 $34.38 $36.29 $38.20
51-64 $35.53 $38.76 $41.99 $45.22 $48.45 $51.68 $54.91 $58.14 $61.37 $64.60
65+ $63.91 $69.72 $75.53 $81.34 $87.15 $92.96 $98.77 $104.58 $110.39 $116.20
$2,100 $2,200 $2,300 $2,400 $2,500 $2,600 $2,700 $2,800 $2,900 $3,000
18-50 $40.11 $42.02 $43.93 $45.84 $47.75 $49.66 $51.57 $53.48 $55.39 $57.30
51-64 $67.83 $71.06 $74.29 $77.52 $80.75 $83.98 $87.21 $90.44 $93.67 $96.90
65+ $122.01 $127.82 $133.63 $139.44 $145.25 $151.06 $156.87 $162.68 $168.49 $174.30
$3,100 $3,200 $3,300 $3,400 $3,500 $3,600 $3,700 $3,800 $3,900 $4,000
18-50 $59.21 $61.12 $63.03 $64.94 $66.85 $68.76 $70.67 $72.58 $74.49 $76.40
51-64 $100.13 $103.36 $106.59 $109.82 $113.05 $116.28 $119.51 $122.74 $125.97 $129.20
65+ $180.11 $185.92 $191.73 $197.54 $203.35 $209.16 $214.97 $220.78 $226.59 $232.40
$4,100 $4,200 $4,300 $4,400 $4,500 $4,600 $4,700 $4,800 $4,900 $5,000
18-50 $78.31 $80.22 $82.13 $84.04 $85.95 $87.86 $89.77 $91.68 $93.59 $95.50
51-64 $132.43 $135.66 $138.89 $142.12 $145.35 $148.58 $151.81 $155.04 $158.27 $161.50
65+ $238.21 $244.02 $249.83 $255.64 $261.45 $267.26 $273.07 $278.88 $284.69 $290.50
23

1-800-327-9728 • HumanaVoluntaryBenefits.comPolicy: 8000Underwritten by Kanawha Insurance Company
Disability Income Plus rates
Disability Income Plus ratesSemi-monthly deductions (24 pay periods), elimination period: 0/7
Age Benefit amount
$100 $200 $300 $400 $500 $600 $700 $800 $900 $1,000
18-50 $1.93 $3.86 $5.79 $7.72 $9.65 $11.58 $13.51 $15.44 $17.37 $19.30
51-64 $2.81 $5.62 $8.43 $11.24 $14.05 $16.86 $19.67 $22.48 $25.29 $28.10
65+ $4.35 $8.70 $13.05 $17.40 $21.75 $26.10 $30.45 $34.80 $39.15 $43.50
$1,100 $1,200 $1,300 $1,400 $1,500 $1,600 $1,700 $1,800 $1,900 $2,000
18-50 $21.23 $23.16 $25.09 $27.02 $28.95 $30.88 $32.81 $34.74 $36.67 $38.60
51-64 $30.91 $33.72 $36.53 $39.34 $42.15 $44.96 $47.77 $50.58 $53.39 $56.20
65+ $47.85 $52.20 $56.55 $60.90 $65.25 $69.60 $73.95 $78.30 $82.65 $87.00
$2,100 $2,200 $2,300 $2,400 $2,500 $2,600 $2,700 $2,800 $2,900 $3,000
18-50 $40.53 $42.46 $44.39 $46.32 $48.25 $50.18 $52.11 $54.04 $55.97 $57.90
51-64 $59.01 $61.82 $64.63 $67.44 $70.25 $73.06 $75.87 $78.68 $81.49 $84.30
65+ $91.35 $95.70 $100.05 $104.40 $108.75 $113.10 $117.45 $121.80 $126.15 $130.50
$3,100 $3,200 $3,300 $3,400 $3,500 $3,600 $3,700 $3,800 $3,900 $4,000
18-50 $59.83 $61.76 $63.69 $65.62 $67.55 $69.48 $71.41 $73.34 $75.27 $77.20
51-64 $87.11 $89.92 $92.73 $95.54 $98.35 $101.16 $103.97 $106.78 $109.59 $112.40
65+ $134.85 $139.20 $143.55 $147.90 $152.25 $156.60 $160.95 $165.30 $169.65 $174.00
$4,100 $4,200 $4,300 $4,400 $4,500 $4,600 $4,700 $4,800 $4,900 $5,000
18-50 $79.13 $81.06 $82.99 $84.92 $86.85 $88.78 $90.71 $92.64 $94.57 $96.50
51-64 $115.21 $118.02 $120.83 $123.64 $126.45 $129.26 $132.07 $134.88 $137.69 $140.50
65+ $178.35 $182.70 $187.05 $191.40 $195.75 $200.10 $204.45 $208.80 $213.15 $217.50
Semi-monthly deductions (24 pay periods), elimination period: 7/7
Age Benefit amount
$100 $200 $300 $400 $500 $600 $700 $800 $900 $1,000
18-50 $1.91 $3.82 $5.73 $7.64 $9.55 $11.46 $13.37 $15.28 $17.19 $19.10
51-64 $2.80 $5.60 $8.40 $11.20 $14.00 $16.80 $19.60 $22.40 $25.20 $28.00
65+ $4.28 $8.56 $12.84 $17.12 $21.40 $25.68 $29.96 $34.24 $38.52 $42.80
$1,100 $1,200 $1,300 $1,400 $1,500 $1,600 $1,700 $1,800 $1,900 $2,000
18-50 $21.01 $22.92 $24.83 $26.74 $28.65 $30.56 $32.47 $34.38 $36.29 $38.20
51-64 $30.80 $33.60 $36.40 $39.20 $42.00 $44.80 $47.60 $50.40 $53.20 $56.00
65+ $47.08 $51.36 $55.64 $59.92 $64.20 $68.48 $72.76 $77.04 $81.32 $85.60
$2,100 $2,200 $2,300 $2,400 $2,500 $2,600 $2,700 $2,800 $2,900 $3,000
18-50 $40.11 $42.02 $43.93 $45.84 $47.75 $49.66 $51.57 $53.48 $55.39 $57.30
51-64 $58.80 $61.60 $64.40 $67.20 $70.00 $72.80 $75.60 $78.40 $81.20 $84.00
65+ $89.88 $94.16 $98.44 $102.72 $107.00 $111.28 $115.56 $119.84 $124.12 $128.40
$3,100 $3,200 $3,300 $3,400 $3,500 $3,600 $3,700 $3,800 $3,900 $4,000
18-50 $59.21 $61.12 $63.03 $64.94 $66.85 $68.76 $70.67 $72.58 $74.49 $76.40
51-64 $86.80 $89.60 $92.40 $95.20 $98.00 $100.80 $103.60 $106.40 $109.20 $112.00
65+ $132.68 $136.96 $141.24 $145.52 $149.80 $154.08 $158.36 $162.64 $166.92 $171.20
$4,100 $4,200 $4,300 $4,400 $4,500 $4,600 $4,700 $4,800 $4,900 $5,000
18-50 $78.31 $80.22 $82.13 $84.04 $85.95 $87.86 $89.77 $91.68 $93.59 $95.50
51-64 $114.80 $117.60 $120.40 $123.20 $126.00 $128.80 $131.60 $134.40 $137.20 $140.00
65+ $175.48 $179.76 $184.04 $188.32 $192.60 $196.88 $201.16 $205.44 $209.72 $214.00
24

1-800-327-9728 • HumanaVoluntaryBenefits.comPolicy: 8000Underwritten by Kanawha Insurance Company
Disability Income Plus rates
Disability Income Plus ratesSemi-monthly deductions (24 pay periods), elimination period: 14/14
Age Benefit amount
$100 $200 $300 $400 $500 $600 $700 $800 $900 $1,000
18-50 $1.51 $3.02 $4.53 $6.04 $7.55 $9.06 $10.57 $12.08 $13.59 $15.10
51-64 $2.36 $4.72 $7.08 $9.44 $11.80 $14.16 $16.52 $18.88 $21.24 $23.60
65+ $3.93 $7.86 $11.79 $15.72 $19.65 $23.58 $27.51 $31.44 $35.37 $39.30
$1,100 $1,200 $1,300 $1,400 $1,500 $1,600 $1,700 $1,800 $1,900 $2,000
18-50 $16.61 $18.12 $19.63 $21.14 $22.65 $24.16 $25.67 $27.18 $28.69 $30.20
51-64 $25.96 $28.32 $30.68 $33.04 $35.40 $37.76 $40.12 $42.48 $44.84 $47.20
65+ $43.23 $47.16 $51.09 $55.02 $58.95 $62.88 $66.81 $70.74 $74.67 $78.60
$2,100 $2,200 $2,300 $2,400 $2,500 $2,600 $2,700 $2,800 $2,900 $3,000
18-50 $31.71 $33.22 $34.73 $36.24 $37.75 $39.26 $40.77 $42.28 $43.79 $45.30
51-64 $49.56 $51.92 $54.28 $56.64 $59.00 $61.36 $63.72 $66.08 $68.44 $70.80
65+ $82.53 $86.46 $90.39 $94.32 $98.25 $102.18 $106.11 $110.04 $113.97 $117.90
$3,100 $3,200 $3,300 $3,400 $3,500 $3,600 $3,700 $3,800 $3,900 $4,000
18-50 $46.81 $48.32 $49.83 $51.34 $52.85 $54.36 $55.87 $57.38 $58.89 $60.40
51-64 $73.16 $75.52 $77.88 $80.24 $82.60 $84.96 $87.32 $89.68 $92.04 $94.40
65+ $121.83 $125.76 $129.69 $133.62 $137.55 $141.48 $145.41 $149.34 $153.27 $157.20
$4,100 $4,200 $4,300 $4,400 $4,500 $4,600 $4,700 $4,800 $4,900 $5,000
18-50 $61.91 $63.42 $64.93 $66.44 $67.95 $69.46 $70.97 $72.48 $73.99 $75.50
51-64 $96.76 $99.12 $101.48 $103.84 $106.20 $108.56 $110.92 $113.28 $115.64 $118.00
65+ $161.13 $165.06 $168.99 $172.92 $176.85 $180.78 $184.71 $188.64 $192.57 $196.50
Semi-monthly deductions (24 pay periods), elimination period: 30/30
Age Benefit amount
$100 $200 $300 $400 $500 $600 $700 $800 $900 $1,000
18-50 $0.96 $1.92 $2.88 $3.84 $4.80 $5.76 $6.72 $7.68 $8.64 $9.60
51-64 $1.62 $3.24 $4.86 $6.48 $8.10 $9.72 $11.34 $12.96 $14.58 $16.20
65+ $2.91 $5.82 $8.73 $11.64 $14.55 $17.46 $20.37 $23.28 $26.19 $29.10
$1,100 $1,200 $1,300 $1,400 $1,500 $1,600 $1,700 $1,800 $1,900 $2,000
18-50 $10.56 $11.52 $12.48 $13.44 $14.40 $15.36 $16.32 $17.28 $18.24 $19.20
51-64 $17.82 $19.44 $21.06 $22.68 $24.30 $25.92 $27.54 $29.16 $30.78 $32.40
65+ $32.01 $34.92 $37.83 $40.74 $43.65 $46.56 $49.47 $52.38 $55.29 $58.20
$2,100 $2,200 $2,300 $2,400 $2,500 $2,600 $2,700 $2,800 $2,900 $3,000
18-50 $20.16 $21.12 $22.08 $23.04 $24.00 $24.96 $25.92 $26.88 $27.84 $28.80
51-64 $34.02 $35.64 $37.26 $38.88 $40.50 $42.12 $43.74 $45.36 $46.98 $48.60
65+ $61.11 $64.02 $66.93 $69.84 $72.75 $75.66 $78.57 $81.48 $84.39 $87.30
$3,100 $3,200 $3,300 $3,400 $3,500 $3,600 $3,700 $3,800 $3,900 $4,000
18-50 $29.76 $30.72 $31.68 $32.64 $33.60 $34.56 $35.52 $36.48 $37.44 $38.40
51-64 $50.22 $51.84 $53.46 $55.08 $56.70 $58.32 $59.94 $61.56 $63.18 $64.80
65+ $90.21 $93.12 $96.03 $98.94 $101.85 $104.76 $107.67 $110.58 $113.49 $116.40
$4,100 $4,200 $4,300 $4,400 $4,500 $4,600 $4,700 $4,800 $4,900 $5,000
18-50 $39.36 $40.32 $41.28 $42.24 $43.20 $44.16 $45.12 $46.08 $47.04 $48.00
51-64 $66.42 $68.04 $69.66 $71.28 $72.90 $74.52 $76.14 $77.76 $79.38 $81.00
65+ $119.31 $122.22 $125.13 $128.04 $130.95 $133.86 $136.77 $139.68 $142.59 $145.50
25

1-800-327-9728 • HumanaVoluntaryBenefits.comPolicy: 8000Underwritten by Kanawha Insurance Company
Disability Income Plus rates
Disability Income Plus rates20 pay period deductions, elimination period: 0/7
Age Benefit amount
$100 $200 $300 $400 $500 $600 $700 $800 $900 $1,000
18-50 $2.32 $4.64 $6.96 $9.28 $11.60 $13.92 $16.24 $18.56 $20.88 $23.20
51-64 $3.37 $6.74 $10.11 $13.48 $16.85 $20.22 $23.59 $26.96 $30.33 $33.70
65+ $5.22 $10.44 $15.66 $20.88 $26.10 $31.32 $36.54 $41.76 $46.98 $52.20
$1,100 $1,200 $1,300 $1,400 $1,500 $1,600 $1,700 $1,800 $1,900 $2,000
18-50 $25.52 $27.84 $30.16 $32.48 $34.80 $37.12 $39.44 $41.76 $44.08 $46.40
51-64 $37.07 $40.44 $43.81 $47.18 $50.55 $53.92 $57.29 $60.66 $64.03 $67.40
65+ $57.42 $62.64 $67.86 $73.08 $78.30 $83.52 $88.74 $93.96 $99.18 $104.40
$2,100 $2,200 $2,300 $2,400 $2,500 $2,600 $2,700 $2,800 $2,900 $3,000
18-50 $48.72 $51.04 $53.36 $55.68 $58.00 $60.32 $62.64 $64.96 $67.28 $69.60
51-64 $70.77 $74.14 $77.51 $80.88 $84.25 $87.62 $90.99 $94.36 $97.73 $101.10
65+ $109.62 $114.84 $120.06 $125.28 $130.50 $135.72 $140.94 $146.16 $151.38 $156.60
$3,100 $3,200 $3,300 $3,400 $3,500 $3,600 $3,700 $3,800 $3,900 $4,000
18-50 $71.92 $74.24 $76.56 $78.88 $81.20 $83.52 $85.84 $88.16 $90.48 $92.80
51-64 $104.47 $107.84 $111.21 $114.58 $117.95 $121.32 $124.69 $128.06 $131.43 $134.80
65+ $161.82 $167.04 $172.26 $177.48 $182.70 $187.92 $193.14 $198.36 $203.58 $208.80
$4,100 $4,200 $4,300 $4,400 $4,500 $4,600 $4,700 $4,800 $4,900 $5,000
18-50 $95.12 $97.44 $99.76 $102.08 $104.40 $106.72 $109.04 $111.36 $113.68 $116.00
51-64 $138.17 $141.54 $144.91 $148.28 $151.65 $155.02 $158.39 $161.76 $165.13 $168.50
65+ $214.02 $219.24 $224.46 $229.68 $234.90 $240.12 $245.34 $250.56 $255.78 $261.00
20 pay period deductions, elimination period: 7/7
Age Benefit amount
$100 $200 $300 $400 $500 $600 $700 $800 $900 $1,000
18-50 $2.29 $4.58 $6.87 $9.16 $11.45 $13.74 $16.03 $18.32 $20.61 $22.90
51-64 $3.36 $6.72 $10.08 $13.44 $16.80 $20.16 $23.52 $26.88 $30.24 $33.60
65+ $5.13 $10.26 $15.39 $20.52 $25.65 $30.78 $35.91 $41.04 $46.17 $51.30
$1,100 $1,200 $1,300 $1,400 $1,500 $1,600 $1,700 $1,800 $1,900 $2,000
18-50 $25.19 $27.48 $29.77 $32.06 $34.35 $36.64 $38.93 $41.22 $43.51 $45.80
51-64 $36.96 $40.32 $43.68 $47.04 $50.40 $53.76 $57.12 $60.48 $63.84 $67.20
65+ $56.43 $61.56 $66.69 $71.82 $76.95 $82.08 $87.21 $92.34 $97.47 $102.60
$2,100 $2,200 $2,300 $2,400 $2,500 $2,600 $2,700 $2,800 $2,900 $3,000
18-50 $48.09 $50.38 $52.67 $54.96 $57.25 $59.54 $61.83 $64.12 $66.41 $68.70
51-64 $70.56 $73.92 $77.28 $80.64 $84.00 $87.36 $90.72 $94.08 $97.44 $100.80
65+ $107.73 $112.86 $117.99 $123.12 $128.25 $133.38 $138.51 $143.64 $148.77 $153.90
$3,100 $3,200 $3,300 $3,400 $3,500 $3,600 $3,700 $3,800 $3,900 $4,000
18-50 $70.99 $73.28 $75.57 $77.86 $80.15 $82.44 $84.73 $87.02 $89.31 $91.60
51-64 $104.16 $107.52 $110.88 $114.24 $117.60 $120.96 $124.32 $127.68 $131.04 $134.40
65+ $159.03 $164.16 $169.29 $174.42 $179.55 $184.68 $189.81 $194.94 $200.07 $205.20
$4,100 $4,200 $4,300 $4,400 $4,500 $4,600 $4,700 $4,800 $4,900 $5,000
18-50 $93.89 $96.18 $98.47 $100.76 $103.05 $105.34 $107.63 $109.92 $112.21 $114.50
51-64 $137.76 $141.12 $144.48 $147.84 $151.20 $154.56 $157.92 $161.28 $164.64 $168.00
65+ $210.33 $215.46 $220.59 $225.72 $230.85 $235.98 $241.11 $246.24 $251.37 $256.50
26

1-800-327-9728 • HumanaVoluntaryBenefits.comPolicy: 8000Underwritten by Kanawha Insurance Company
Disability Income Plus rates
Disability Income Plus rates20 pay period deductions, elimination period: 14/14
Age Benefit amount
$100 $200 $300 $400 $500 $600 $700 $800 $900 $1,000
18-50 $1.81 $3.62 $5.43 $7.24 $9.05 $10.86 $12.67 $14.48 $16.29 $18.10
51-64 $2.83 $5.66 $8.49 $11.32 $14.15 $16.98 $19.81 $22.64 $25.47 $28.30
65+ $4.72 $9.44 $14.16 $18.88 $23.60 $28.32 $33.04 $37.76 $42.48 $47.20
$1,100 $1,200 $1,300 $1,400 $1,500 $1,600 $1,700 $1,800 $1,900 $2,000
18-50 $19.91 $21.72 $23.53 $25.34 $27.15 $28.96 $30.77 $32.58 $34.39 $36.20
51-64 $31.13 $33.96 $36.79 $39.62 $42.45 $45.28 $48.11 $50.94 $53.77 $56.60
65+ $51.92 $56.64 $61.36 $66.08 $70.80 $75.52 $80.24 $84.96 $89.68 $94.40
$2,100 $2,200 $2,300 $2,400 $2,500 $2,600 $2,700 $2,800 $2,900 $3,000
18-50 $38.01 $39.82 $41.63 $43.44 $45.25 $47.06 $48.87 $50.68 $52.49 $54.30
51-64 $59.43 $62.26 $65.09 $67.92 $70.75 $73.58 $76.41 $79.24 $82.07 $84.90
65+ $99.12 $103.84 $108.56 $113.28 $118.00 $122.72 $127.44 $132.16 $136.88 $141.60
$3,100 $3,200 $3,300 $3,400 $3,500 $3,600 $3,700 $3,800 $3,900 $4,000
18-50 $56.11 $57.92 $59.73 $61.54 $63.35 $65.16 $66.97 $68.78 $70.59 $72.40
51-64 $87.73 $90.56 $93.39 $96.22 $99.05 $101.88 $104.71 $107.54 $110.37 $113.20
65+ $146.32 $151.04 $155.76 $160.48 $165.20 $169.92 $174.64 $179.36 $184.08 $188.80
$4,100 $4,200 $4,300 $4,400 $4,500 $4,600 $4,700 $4,800 $4,900 $5,000
18-50 $74.21 $76.02 $77.83 $79.64 $81.45 $83.26 $85.07 $86.88 $88.69 $90.50
51-64 $116.03 $118.86 $121.69 $124.52 $127.35 $130.18 $133.01 $135.84 $138.67 $141.50
65+ $193.52 $198.24 $202.96 $207.68 $212.40 $217.12 $221.84 $226.56 $231.28 $236.00
20 pay period deductions, elimination period: 30/30
Age Benefit amount
$100 $200 $300 $400 $500 $600 $700 $800 $900 $1,000
18-50 $1.15 $2.30 $3.45 $4.60 $5.75 $6.90 $8.05 $9.20 $10.35 $11.50
51-64 $1.94 $3.88 $5.82 $7.76 $9.70 $11.64 $13.58 $15.52 $17.46 $19.40
65+ $3.49 $6.98 $10.47 $13.96 $17.45 $20.94 $24.43 $27.92 $31.41 $34.90
$1,100 $1,200 $1,300 $1,400 $1,500 $1,600 $1,700 $1,800 $1,900 $2,000
18-50 $12.65 $13.80 $14.95 $16.10 $17.25 $18.40 $19.55 $20.70 $21.85 $23.00
51-64 $21.34 $23.28 $25.22 $27.16 $29.10 $31.04 $32.98 $34.92 $36.86 $38.80
65+ $38.39 $41.88 $45.37 $48.86 $52.35 $55.84 $59.33 $62.82 $66.31 $69.80
$2,100 $2,200 $2,300 $2,400 $2,500 $2,600 $2,700 $2,800 $2,900 $3,000
18-50 $24.15 $25.30 $26.45 $27.60 $28.75 $29.90 $31.05 $32.20 $33.35 $34.50
51-64 $40.74 $42.68 $44.62 $46.56 $48.50 $50.44 $52.38 $54.32 $56.26 $58.20
65+ $73.29 $76.78 $80.27 $83.76 $87.25 $90.74 $94.23 $97.72 $101.21 $104.70
$3,100 $3,200 $3,300 $3,400 $3,500 $3,600 $3,700 $3,800 $3,900 $4,000
18-50 $35.65 $36.80 $37.95 $39.10 $40.25 $41.40 $42.55 $43.70 $44.85 $46.00
51-64 $60.14 $62.08 $64.02 $65.96 $67.90 $69.84 $71.78 $73.72 $75.66 $77.60
65+ $108.19 $111.68 $115.17 $118.66 $122.15 $125.64 $129.13 $132.62 $136.11 $139.60
$4,100 $4,200 $4,300 $4,400 $4,500 $4,600 $4,700 $4,800 $4,900 $5,000
18-50 $47.15 $48.30 $49.45 $50.60 $51.75 $52.90 $54.05 $55.20 $56.35 $57.50
51-64 $79.54 $81.48 $83.42 $85.36 $87.30 $89.24 $91.18 $93.12 $95.06 $97.00
65+ $143.09 $146.58 $150.07 $153.56 $157.05 $160.54 $164.03 $167.52 $171.01 $174.50
27

Voluntary permanent life insurance can be an ideal complement to the group term and optional term your employer might provide. Designed to be in force when you die, this voluntary universal life product is yours to keep, even when you change jobs or retire, as long as you pay the necessary premium. Group and voluntary term, on the other hand, typically are not portable if you change jobs and, even if you can keep them after you retire, usually costs more and declines in death benefit.
The policy, purelife-plus, is underwritten by Texas Life Insurance Company, and it has these outstanding features:
High Death Benefit.• With one of the highest death benefits available at the worksite,1 purelife-plus gives your loved ones peace of mind, knowing there will be significant life insurance in force should you die prematurely.
Minimal Cash Value.• Designed to provide high death benefit, purelife-plus does not compete with the cash accumulation in your employer-sponsored retirement plans.
Long Guarantees.• Enjoy the assurance of a policy that has a guaranteed death benefit to age 121 and level premium that guarantees coverage for a significant period of time (after the guaranteed period, premiums may go down, stay the same, or go up).
Refund of Premium.• Unique in the marketplace, purelife-plus offers you a refund of 10 years’ premium, should you surrender the policy if the premium you pay when you buy the policy ever increases. (Conditions apply.)
Accelerated Death Benefit Rider. • Should you be diagnosed as terminally ill with the expectation of death within 12 months (24 months in Illinois), you will have the option to receive 92% (84% in Illinois) of the death benefit, minus a $150 ($100 in Florida) administrative fee. This valuable living benefit gives you peace of mind knowing that, should you need it, you can take the large majority of your death benefit while still alive. (Conditions apply.)
You may apply for this permanent, portable coverage, not only for yourself, but also for your spouse, minor children and grandchildren by answering just 3 questions:
During the last six months, has the proposed insured:Been actively at work on a full time basis, performing usual duties?a. Been absent from work due to illness or medical treatment for a period of b. more than five consecutive working days?Been disabled or received tests, treatment or care of any kind in a hospital c. or nursing home or received chemotherapy, hormonal therapy for cancer, ra-diation therapy, dialysis treatment, or treatment for alcohol or drug abuse?
Flexible Premium Life Insurance to Age 121Policy Form PRFNG-NI-10
See the purelife-plus brochure for details.
1 Voluntary and Universal Whole Life Products, Eastbridge Consulting Group, October 2008
Life Insurance HighlightsFor the employee
purelife-plus
Like most life insurance policies, Texas Life policies contain certain exclusions, limitations, exceptions, reductions of benefits, waiting periods and terms for keeping them in force. Please contact a Texas Life representative for costs and complete details.
10M055-C 1040 (exp0612) Not for use in WA.28

20 per year p r em i um s
PureLife Standard Risk Table Premiums — Express & Simplified IssueGUARANTEED
20 per year Premiums for Life Insurance Face Amounts Shown PERIOD
Includes Added Cost for Age to Which
Issue Accidental Death Benefit (Ages 17-59) Coverage is
Age Employee Group Size 50-499 Guaranteed at
(ALB) $10,000 $15,000 $20,000 $25,000 $50,000 $100,000 $150,000 $200,000 $250,000 Table Premium
15D-10 3.90 63
11-15 4.20 61
16 4.65 64
17-20 5.90 10.90 20.90 30.90 40.90 50.90 60
21 6.20 11.50 22.10 32.70 43.30 53.90 62
22 6.20 11.50 22.10 32.70 43.30 53.90 61
23-25 6.35 11.80 22.70 33.60 44.50 55.40 59
26 6.50 12.10 23.30 34.50 45.70 56.90 59
27-28 6.65 12.40 23.90 35.40 46.90 58.40 58
29 6.80 12.70 24.50 36.30 48.10 59.90 58
30-31 6.95 13.00 25.10 37.20 49.30 61.40 56
32 7.25 13.60 26.30 39.00 51.70 64.40 57
33 7.55 14.20 27.50 40.80 54.10 67.40 58
34 7.85 14.80 28.70 42.60 56.50 70.40 58
35 8.30 15.70 30.50 45.30 60.10 74.90 60
36 8.60 16.30 31.70 47.10 62.50 77.90 60
37 8.90 16.90 32.90 48.90 64.90 80.90 60
38 9.35 17.80 34.70 51.60 68.50 85.40 61
39 9.95 19.00 37.10 55.20 73.30 91.40 63
40 10.55 20.20 39.50 58.80 78.10 97.40 64
41 11.30 21.70 42.50 63.30 84.10 104.90 65
42 12.35 23.80 46.70 69.60 92.50 115.40 67
43 13.40 25.90 50.90 75.90 100.90 125.90 69
44 14.45 28.00 55.10 82.20 109.30 136.40 71
45 15.65 30.40 59.90 89.40 118.90 148.40 72
46 16.85 32.80 64.70 96.60 128.50 160.40 73
47 17.90 34.90 68.90 102.90 136.90 170.90 74
48 19.10 37.30 73.70 110.10 146.50 182.90 75
49 20.45 40.00 79.10 118.20 157.30 196.40 76
50 9.38 13.62 17.86 22.10 43.30 85.70 128.10 170.50 212.90 77
51 10.16 14.79 19.42 24.05 47.20 93.50 139.80 186.10 232.40 78
52 11.12 16.23 21.34 26.45 52.00 103.10 154.20 205.30 256.40 80
53 12.08 17.67 23.26 28.85 56.80 112.70 168.60 224.50 280.40 82
54 13.04 19.11 25.18 31.25 61.60 122.30 183.00 243.70 304.40 83
55 13.88 20.37 26.86 33.35 65.80 130.70 195.60 260.50 325.40 84
56 14.48 21.27 28.06 34.85 68.80 136.70 204.60 272.50 340.40 84
57 14.90 21.90 28.90 35.90 70.90 140.90 210.90 280.90 350.90 83
58 15.38 22.62 29.86 37.10 73.30 145.70 218.10 290.50 362.90 83
59 15.98 23.52 31.06 38.60 76.30 151.70 227.10 302.50 377.90 83
60 16.38 24.12 31.86 39.60 78.30 155.70 233.10 310.50 387.90 83
61 17.76 26.19 34.62 43.05 85.20 169.50 253.80 338.10 422.40 84
62 19.44 28.71 37.98 47.25 93.60 186.30 279.00 371.70 464.40 86
63 21.30 31.50 41.70 51.90 102.90 204.90 306.90 408.90 510.90 88
64 23.16 34.29 45.42 56.55 112.20 223.50 334.80 446.10 557.40 90
65 24.90 36.90 48.90 60.90 120.90 240.90 360.90 480.90 600.90 91
66 26.94 39.96 52.98 66.00 131.10 261.30 391.50 521.70 651.90 94
67 28.50 42.30 56.10 69.90 138.90 276.90 414.90 552.90 690.90 95
68 30.12 44.73 59.34 73.95 147.00 293.10 439.20 585.30 731.40 95
69 31.50 46.80 62.10 77.40 153.90 306.90 459.90 612.90 765.90 95
70 32.70 48.60 64.50 80.40 159.90 318.90 477.90 636.90 795.90 93
PureLife is permanent life insurance to Attained Age 121 that can never be cancelled as long as you pay the necessary premiums. After the
Guaranteed Period, the premiums can be lower, the same, or higher than the Table Premium. See the brochure under ”Permanent Coverage”.
PL-B4AHB5ABD9CH
29

20 per year p r em i um s
PureLife Standard Risk Table Premiums — Express & Simplified IssueGUARANTEED
Life Insurance Face Amounts for 20 per year Premiums Shown PERIOD
Prem Includes Added Cost for Age to Which
Issue For Accidental Death Benefit (Ages 17-59) Coverage is
Age $10,000 Employee Group Size 50-499 Guaranteed at
(ALB) Face $7.00 $8.00 $10.00 $12.00 $14.00 $16.00 $18.00 $20.00 Table Premium
17-20 30,470 35,470 45,470 55,470 65,470 75,470 85,470 95,470 60
21 28,745 33,462 42,896 52,330 61,764 71,198 80,632 90,066 62
22 28,745 33,462 42,896 52,330 61,764 71,198 80,632 90,066 61
23-25 27,954 32,541 41,716 50,890 60,064 69,239 78,413 87,587 59
26 27,205 31,670 40,598 49,527 58,455 67,384 76,312 85,241 59
27-28 26,496 30,843 39,539 48,235 56,930 65,626 74,322 83,017 58
29 25,822 30,059 38,534 47,008 55,483 63,958 72,432 80,907 58
30-31 25,182 29,314 37,579 45,843 54,107 62,372 70,636 78,901 56
32 27,929 35,803 43,677 51,551 59,425 67,299 75,173 57
33 26,669 34,188 41,707 49,226 56,744 64,263 71,782 58
34 25,518 32,712 39,906 47,101 54,295 61,489 68,683 58
35 30,723 37,480 44,236 50,993 57,750 64,507 60
36 29,526 36,019 42,513 49,006 55,500 61,994 60
37 28,419 34,669 40,919 47,169 53,419 59,669 60
38 26,905 32,822 38,740 44,657 50,574 56,491 61
39 25,122 30,646 36,171 41,696 47,221 52,746 63
40 28,741 33,922 39,104 44,285 49,466 64
41 26,668 31,476 36,284 41,091 45,899 65
42 28,590 32,956 37,323 41,690 67
43 26,188 30,188 34,188 38,188 69
44 27,849 31,539 35,229 71
45 25,583 28,973 32,363 72
46 26,793 29,928 73
47 25,138 28,079 74
48 26,228 75
49 76
50 9.38 10,724 13,083 15,441 17,800 20,158 22,517 77
51 10.16 11,981 14,140 16,300 18,460 20,620 78
52 11.12 10,855 12,812 14,769 16,726 18,683 80
53 12.08 11,712 13,501 15,290 17,079 82
54 13.04 10,786 12,433 14,081 15,728 83
55 13.88 10,088 11,629 13,169 14,710 84
56 14.48 11,115 12,588 14,060 84
57 14.90 10,781 12,210 13,639 83
58 15.38 10,424 11,805 13,186 83
59 15.98 10,009 11,336 12,662 83
60 16.38 11,043 12,335 83
61 17.76 10,139 11,325 84
62 19.44 10,299 86
63 21.30 88
64 23.16 90
65 24.90 91
66 26.94 94
67 28.50 95
68 30.12 95
69 31.50 95
70 32.70 93
PureLife is permanent life insurance to Attained Age 121 that can never be cancelled as long as you pay the necessary premiums. After the
Guaranteed Period, the premiums can be lower, the same, or higher than the Table Premium. See the brochure under ”Permanent Coverage”.
PL-B4AHB5ABD9CH 30

1-800-327-9728 | HumanaVoluntaryBenefits.com
Virginia Child(ren) Summary - Portsmouth Public Schools
This is not a complete disclosure of plan qualifications and limitations. Please access our website to obtain a completed
list for the Workplace Voluntary Benefit products at Disclosure.Humana.com. Please review this information before
applying for coverage. The amount of benefits provided depends on the plan selected. Premiums will vary according to
the selection made.
Policy: 00455
Underwritten by Kanawha Insurance Company, a Humana company.
VOL8073
Humana Whole Life 65
If people depend financially on you, you need life insurance, no matter what your age or marital status. With life
insurance, you can help spare your grieving loved ones the additional stress of economic difficulties and preserve
their quality of life. Premiums for this whole life product are payable to age 65. The policy providers guaranteed
coverage and cash values stay with the policy for its lifetime – you can take funds as loans or use to buy paid-up
coverage.
Coverage type Humana Whole Life 65 is an individual whole life insurance
product with premiums payable to age 65.
Benefit typeDefined benefit
Policyholder Child
Benefit amount Benefit amounts are available at various levels. You can choose:
• Child(ren): $2,500 to $25,000 for each eligible child
Issue ages Child(ren) stand-alone coverage: 14 days - 24 years
Additional included benefits Terminal illness acceleration benefit: For the primary insured
provides an acceleration of up to 50 percent of the original
death benefit, base and term rider, amount including any ABI
amounts, upon diagnosis of a terminal illness. 12-month
waiting period.
Stand-alone Child(ren) Coverage Simplified Issue - Up to $25,000
For child stand-alone coverage Humana Whole Life to age 65 is only plan available.
31

1-800-327-9728 | HumanaVoluntaryBenefits.com
Virginia Child(ren) Summary - Portsmouth Public Schools
This is not a complete disclosure of plan qualifications and limitations. Please access our website to obtain a completed
list for the Workplace Voluntary Benefit products at Disclosure.Humana.com. Please review this information before
applying for coverage. The amount of benefits provided depends on the plan selected. Premiums will vary according to
the selection made.
Policy: 00455
Underwritten by Kanawha Insurance Company, a Humana company.
VOL8073
Humana Whole Life 65
Additional included benefits Facility Care Acceleration Benefit: provides an acceleration of
one percent of the face amount, up to $2,000/month up to a
maximum of 36 months for Licensed Adult Day Care and/or up
to two percent of the face amount, up to $4,000/month up to a
maximum of 18 months for inpatient resident care. Benefits
cannot exceed the lesser of 36 percent of the face amount,
$72,000, or the face amount of the policy less the cash value.
Product restrictions • Total amount of permanent life insurance coverage and term
life insurance coverage with Kanawha Insurance Company
not to exceed $300,000.
• If both parents are eligible employees, their eligible children
may be insured by either spouse but not both.
• Purchasing option, whether money purchase or flat face
amount, will be determined by the employer.
• When optional riders are selected, the weekly money
purchase premium will be calculated to include the base
benefit and any rider(s) (per applicant).
• If an employee's base policy, rider(s), and any additional
Kanawha Insurance Company life insurance products exceed
our company maximum of $300,000, we will first reduce the
applicant's rider(s) on this coverage. If additional reductions
are necessary, we will reduce the face amount of the
base policy.
Age calculation Age at effective date of policy
Portability Yes
Guarantee renewable Yes
Cash value Whole Life 65 is a whole life policy with guaranteed values, not
an interest sensitive policy. As such, there is not an interest rate
associated with the cash value of the policy; the cash values are
all guaranteed in the table of cash values inside each and every
Whole Life policy.
32

Humana Whole Life 65 rates
1-800-327-9728 | HumanaVoluntaryBenefits.com
Policy: 00455 Underwritten by Kanawha Insurance Company, a Humana company.
Child(ren) Summary - Portsmouth Public Schools Virginia
Humana Whole Life 65 rates Child, Non-tobacco coverage, Defined Benefit amounts displaying monthly payroll deductions based on monthly premium calculation.
Age Benefit Amount
BENEFIT: $5,000 CASH VALUE* $10,000 CASH VALUE* $15,000 CASH VALUE*
0 $3.42 $2,405 $4.76 $4,811 $6.11 $7,216
1 $3.42 $2,405 $4.76 $4,811 $6.11 $7,216
2 $3.42 $2,405 $4.76 $4,811 $6.11 $7,216
3 $3.42 $2,405 $4.76 $4,811 $6.11 $7,216
4 $3.42 $2,405 $4.76 $4,811 $6.11 $7,216
5 $3.42 $2,405 $4.76 $4,811 $6.11 $7,216
6 $3.50 $2,405 $4.91 $4,811 $6.33 $7,216
7 $3.57 $2,405 $5.06 $4,811 $6.55 $7,216
8 $3.65 $2,405 $5.21 $4,811 $6.78 $7,216
9 $3.72 $2,405 $5.35 $4,811 $6.99 $7,216
10 $3.79 $2,405 $5.51 $4,811 $7.22 $7,216
11 $3.88 $2,405 $5.69 $4,811 $7.49 $7,216
12 $3.97 $2,405 $5.86 $4,811 $7.75 $7,216
13 $4.06 $2,405 $6.05 $4,811 $8.03 $7,216
14 $4.15 $2,405 $6.23 $4,811 $8.30 $7,216
15 $4.24 $2,405 $6.41 $4,811 $8.57 $7,216
16 $4.40 $2,405 $6.73 $4,811 $9.05 $7,216
17 $4.57 $2,405 $7.05 $4,811 $9.54 $7,216
18 $4.73 $2,405 $7.38 $4,811 $10.03 $7,216
19 $4.89 $2,405 $7.70 $4,811 $10.50 $7,216
20 $5.05 $2,405 $8.02 $4,811 $10.99 $7,216
21 $5.21 $2,405 $8.35 $4,811 $11.48 $7,216
22 $5.37 $2,405 $8.66 $4,811 $11.95 $7,216
23 $5.53 $2,405 $8.99 $4,811 $12.44 $7,216
24 $5.70 $2,405 $9.31 $4,811 $12.93 $7,216
25 $5.85 $2,405 $9.63 $4,811 $13.40 $7,216
26 $6.08 $2,405 $10.09 $4,811 $14.09 $7,216
*Cash values are calculated as of age 65.
The proposed rates are for an effective date no later than January 1, 2014.
33

Humana Whole Life 65 rates
1-800-327-9728 | HumanaVoluntaryBenefits.com
Policy: 00455 Underwritten by Kanawha Insurance Company, a Humana company.
Child(ren) Summary - Portsmouth Public Schools Virginia
Humana Whole Life 65 rates Child, Non-tobacco coverage, Defined Benefit amounts displaying monthly payroll deductions based on monthly premium calculation.
Age Benefit Amount
BENEFIT: $20,000 CASH VALUE* $25,000 CASH VALUE*
0 $7.45 $9,622 $8.79 $12,027
1 $7.45 $9,622 $8.79 $12,027
2 $7.45 $9,622 $8.79 $12,027
3 $7.45 $9,622 $8.79 $12,027
4 $7.45 $9,622 $8.79 $12,027
5 $7.45 $9,622 $8.79 $12,027
6 $7.75 $9,622 $9.16 $12,027
7 $8.05 $9,622 $9.54 $12,027
8 $8.35 $9,622 $9.91 $12,027
9 $8.63 $9,622 $10.27 $12,027
10 $8.93 $9,622 $10.64 $12,027
11 $9.30 $9,622 $11.10 $12,027
12 $9.65 $9,622 $11.54 $12,027
13 $10.01 $9,622 $12.00 $12,027
14 $10.38 $9,622 $12.45 $12,027
15 $10.74 $9,622 $12.90 $12,027
16 $11.38 $9,622 $13.70 $12,027
17 $12.03 $9,622 $14.52 $12,027
18 $12.68 $9,622 $15.33 $12,027
19 $13.31 $9,622 $16.12 $12,027
20 $13.96 $9,622 $16.93 $12,027
21 $14.61 $9,622 $17.75 $12,027
22 $15.25 $9,622 $18.54 $12,027
23 $15.90 $9,622 $19.35 $12,027
24 $16.55 $9,622 $20.16 $12,027
25 $17.18 $9,622 $20.95 $12,027
26 $18.10 $9,622 $22.10 $12,027
*Cash values are calculated as of age 65.
The proposed rates are for an effective date no later than January 1, 2014.
34

1-800-327-9728 | HumanaVoluntaryBenefits.com
Virginia Employee Summary - Portsmouth Public Schools
This is not a complete disclosure of plan qualifications and limitations. Please access our website to obtain a completed
list for the Workplace Voluntary Benefit products at Disclosure.Humana.com. Please review this information before
applying for coverage. The amount of benefits provided depends on the plan selected. Premiums will vary according to
the selection made.
Policy: 00455
Underwritten by Kanawha Insurance Company, a Humana company.
VOL8073
Humana Whole Life 99
Here's a simple, voluntary whole life policy you can get at a reasonable cost during your working years, when you
and your families need coverage the most. It's also a benefit that'll stay in place when retirement rolls around, too.
You buy a policy with guaranteed coverage and actual cash value. Coverage stays level and cash values stay with the
policy for as long as you have it, enabling you to take out funds as loans or buy paid-up coverage.
Coverage type Humana Whole Life 99 is an individual whole life insurance
product with premiums payable to age 99.
Benefit typeDefined benefit
Policyholder Employee
Benefit amount Benefit amounts are available at various levels. You can choose:
• $2,500 to $300,000 for employees
Issue ages Employee base coverage: 18 - 70
Additional included benefits Terminal illness acceleration benefit: For the primary insured
provides an acceleration of up to 50 percent of the original
death benefit, base and term rider, amount including any ABI
amounts, upon diagnosis of a terminal illness. 12-month
waiting period.
Facility Care Acceleration Benefit: provides an acceleration of
one percent of the face amount, up to $2,000/month up to a
maximum of 36 months for Licensed Adult Day Care and/or up
to two percent of the face amount, up to $4,000/month up to a
maximum of 18 months for inpatient resident care. Benefits
cannot exceed the lesser of 36 percent of the face amount,
$72,000, or the face amount of the policy less the cash value.
Employee Simplified Issue Amount up to $300,000 all ages
35

1-800-327-9728 | HumanaVoluntaryBenefits.com
Virginia Employee Summary - Portsmouth Public Schools
This is not a complete disclosure of plan qualifications and limitations. Please access our website to obtain a completed
list for the Workplace Voluntary Benefit products at Disclosure.Humana.com. Please review this information before
applying for coverage. The amount of benefits provided depends on the plan selected. Premiums will vary according to
the selection made.
Policy: 00455
Underwritten by Kanawha Insurance Company, a Humana company.
VOL8073
Humana Whole Life 99
Product restrictions • Total amount of permanent life insurance coverage and term
life insurance coverage with Kanawha Insurance Company
not to exceed $300,000.
• If both parents are eligible employees, their eligible children
may be insured by either spouse but not both.
• Purchasing option, whether money purchase or flat face
amount, will be determined by the employer.
• When optional riders are selected, the weekly money
purchase premium will be calculated to include the base
benefit and any rider(s) (per applicant).
• If an employee's base policy, rider(s), and any additional
Kanawha Insurance Company life insurance products exceed
our company maximum of $300,000, we will first reduce the
applicant's rider(s) on this coverage. If additional reductions
are necessary, we will reduce the face amount of the
base policy.
Age calculation Age at effective date of policy
Portability Yes
Guarantee renewable Yes
Cash value Whole Life 99 is a whole life policy with guaranteed values, not
an interest sensitive policy. As such, there is not an interest rate
associated with the cash value of the policy; the cash values are
all guaranteed in the table of cash values inside each and every
Whole Life policy.
36

Humana Whole Life 99 rates
1-800-327-9728 | HumanaVoluntaryBenefits.com
Policy: 00455 Underwritten by Kanawha Insurance Company, a Humana company.
Employee Summary - Portsmouth Public Schools Virginia
Humana Whole Life 99 rates Employee, Non-tobacco coverage, Defined Benefit amounts displaying monthly payroll deductions based on monthly premium calculation.
Age Benefit Amount
BENEFIT: $10,000 CASH VALUE* $20,000 CASH VALUE* $30,000 CASH VALUE*
18 $6.72 $4,628 $11.36 $9,256 $16.00 $13,884
19 $6.96 $4,628 $11.85 $9,256 $16.73 $13,884
20 $7.08 $4,628 $12.08 $9,256 $17.08 $13,884
21 $7.28 $4,628 $12.48 $9,256 $17.68 $13,884
22 $7.49 $4,628 $12.90 $9,256 $18.30 $13,884
23 $7.69 $4,628 $13.30 $9,256 $18.90 $13,884
24 $7.90 $4,628 $13.71 $9,256 $19.53 $13,884
25 $8.10 $4,628 $14.11 $9,256 $20.13 $13,884
26 $8.35 $4,628 $14.61 $9,256 $20.88 $13,884
27 $8.59 $4,628 $15.10 $9,256 $21.60 $13,884
28 $8.84 $4,620 $15.60 $9,239 $22.35 $13,859
29 $9.08 $4,572 $16.08 $9,144 $23.08 $13,716
30 $9.33 $4,527 $16.58 $9,054 $23.83 $13,581
31 $9.71 $4,475 $17.35 $8,950 $24.98 $13,425
32 $10.10 $4,422 $18.11 $8,845 $26.13 $13,267
33 $10.48 $4,367 $18.88 $8,733 $27.28 $13,100
34 $10.86 $4,308 $19.65 $8,616 $28.43 $12,924
35 $11.25 $4,246 $20.41 $8,493 $29.58 $12,739
36 $11.73 $4,181 $21.38 $8,363 $31.03 $12,544
37 $12.21 $4,113 $22.35 $8,225 $32.48 $12,338
38 $12.70 $4,041 $23.31 $8,081 $33.93 $12,122
39 $13.18 $3,964 $24.28 $7,929 $35.38 $11,893
40 $13.66 $3,884 $25.25 $7,768 $36.83 $11,652
41 $14.35 $3,799 $26.61 $7,598 $38.88 $11,397
42 $15.04 $3,709 $28.00 $7,418 $40.95 $11,128
43 $15.72 $3,614 $29.36 $7,229 $43.00 $10,843
44 $16.41 $3,515 $30.75 $7,029 $45.08 $10,544
45 $17.10 $3,409 $32.11 $6,818 $47.13 $10,227
46 $18.11 $3,471 $34.15 $6,942 $50.18 $10,412
47 $19.12 $3,535 $36.16 $7,069 $53.20 $10,604
48 $20.14 $3,601 $38.20 $7,202 $56.25 $10,803
49 $21.15 $3,670 $40.23 $7,340 $59.30 $11,010
*Cash values are for age 65 through age 45 and for 20 years for ages over 45.The proposed rates are for an effective date no later than January 1, 2014.
37

Humana Whole Life 99 rates
1-800-327-9728 | HumanaVoluntaryBenefits.com
Policy: 00455 Underwritten by Kanawha Insurance Company, a Humana company.
Employee Summary - Portsmouth Public Schools Virginia
Humana Whole Life 99 rates Employee, Non-tobacco coverage, Defined Benefit amounts displaying monthly payroll deductions based on monthly premium calculation.
Age Benefit Amount
BENEFIT: $10,000 CASH VALUE* $20,000 CASH VALUE* $30,000 CASH VALUE*
50 $22.16 $3,742 $42.25 $7,483 $62.33 $11,225
51 $23.50 $3,816 $44.93 $7,631 $66.35 $11,447
52 $24.85 $3,892 $47.61 $7,783 $70.38 $11,675
53 $26.19 $3,970 $50.29 $7,939 $74.40 $11,909
54 $27.53 $4,050 $52.98 $8,099 $78.43 $12,149
55 $28.86 $4,132 $55.64 $8,265 $82.43 $12,397
56 $31.14 $4,218 $60.19 $8,436 $89.25 $12,654
57 $33.40 $4,306 $64.73 $8,613 $96.05 $12,919
58 $35.67 $4,397 $69.26 $8,794 $102.85 $13,190
59 $37.94 $4,488 $73.79 $8,977 $109.65 $13,465
60 $40.20 $4,496 $78.33 $8,993 $116.45 $13,489
61 $43.27 $4,618 $84.46 $9,237 $125.65 $13,855
62 $46.34 $4,737 $90.60 $9,474 $134.85 $14,212
63 $49.41 $4,854 $96.73 $9,707 $144.05 $14,561
64 $52.48 $4,968 $102.88 $9,936 $153.28 $14,904
65 $55.55 $5,080 $109.01 $10,159 $162.48 $15,239
66 $58.57 $5,190 $115.06 $10,380 $171.55 $15,571
67 $61.81 $5,306 $121.53 $10,612 $181.25 $15,918
68 $65.26 $5,419 $128.44 $10,838 $191.63 $16,256
69 $69.05 $5,525 $136.01 $11,051 $202.98 $16,576
70 $73.15 $5,630 $144.21 $11,260 $215.27 $16,889
*Cash values are for age 65 through age 45 and for 20 years for ages over 45.The proposed rates are for an effective date no later than January 1, 2014.
Humana Whole Life 99 rates Employee, Tobacco coverage, Defined Benefit amounts displaying monthly payroll deductions based on monthly premium calculation.
Age Benefit Amount
BENEFIT: $10,000 CASH VALUE* $20,000 CASH VALUE* $30,000 CASH VALUE*
18 $8.74 $5,293 $15.40 $10,587 $22.05 $15,880
19 $9.07 $5,293 $16.06 $10,587 $23.05 $15,880
20 $9.29 $5,293 $16.50 $10,587 $23.70 $15,880
21 $9.62 $5,293 $17.16 $10,587 $24.70 $15,880
*Cash values are for age 65 through age 45 and for 20 years for ages over 45.The proposed rates are for an effective date no later than January 1, 2014.
38

Humana Whole Life 99 rates
1-800-327-9728 | HumanaVoluntaryBenefits.com
Policy: 00455 Underwritten by Kanawha Insurance Company, a Humana company.
Employee Summary - Portsmouth Public Schools Virginia
Humana Whole Life 99 rates Employee, Tobacco coverage, Defined Benefit amounts displaying monthly payroll deductions based on monthly premium calculation.
Age Benefit Amount
BENEFIT: $10,000 CASH VALUE* $20,000 CASH VALUE* $30,000 CASH VALUE*
22 $9.95 $5,293 $17.81 $10,587 $25.68 $15,880
23 $10.28 $5,293 $18.48 $10,587 $26.68 $15,880
24 $10.61 $5,293 $19.15 $10,587 $27.68 $15,880
25 $10.94 $5,293 $19.80 $10,587 $28.65 $15,880
26 $11.38 $5,293 $20.68 $10,587 $29.98 $15,880
27 $11.82 $5,293 $21.56 $10,587 $31.30 $15,880
28 $12.26 $5,259 $22.45 $10,517 $32.63 $15,776
29 $12.70 $5,206 $23.33 $10,412 $33.95 $15,619
30 $13.14 $5,151 $24.20 $10,302 $35.25 $15,452
31 $13.70 $5,092 $25.31 $10,184 $36.93 $15,277
32 $14.25 $5,030 $26.41 $10,060 $38.58 $15,091
33 $14.80 $4,965 $27.53 $9,929 $40.25 $14,894
34 $15.35 $4,896 $28.63 $9,791 $41.90 $14,687
35 $15.90 $4,823 $29.73 $9,646 $43.55 $14,469
36 $16.65 $4,746 $31.23 $9,492 $45.80 $14,238
37 $17.40 $4,665 $32.73 $9,330 $48.05 $13,995
38 $18.15 $4,580 $34.23 $9,159 $50.30 $13,739
39 $18.90 $4,489 $35.73 $8,978 $52.55 $13,468
40 $19.65 $4,394 $37.23 $8,788 $54.80 $13,181
41 $20.60 $4,293 $39.13 $8,586 $57.65 $12,878
42 $21.55 $4,186 $41.01 $8,372 $60.48 $12,558
43 $22.50 $4,074 $42.91 $8,147 $63.33 $12,221
44 $23.44 $3,955 $44.79 $7,910 $66.15 $11,865
45 $24.39 $3,830 $46.69 $7,660 $69.00 $11,490
46 $25.86 $3,872 $49.64 $7,744 $73.43 $11,617
47 $27.35 $3,916 $52.61 $7,832 $77.88 $11,748
48 $28.82 $3,962 $55.56 $7,923 $82.30 $11,885
49 $30.30 $4,009 $58.53 $8,018 $86.75 $12,027
50 $31.78 $4,059 $61.48 $8,118 $91.18 $12,177
51 $33.72 $4,110 $65.36 $8,221 $97.00 $12,331
52 $35.66 $4,163 $69.24 $8,327 $102.83 $12,490
53 $37.60 $4,217 $73.13 $8,434 $108.65 $12,651
54 $39.54 $4,272 $76.99 $8,545 $114.45 $12,817
*Cash values are for age 65 through age 45 and for 20 years for ages over 45.The proposed rates are for an effective date no later than January 1, 2014.
39

Humana Whole Life 99 rates
1-800-327-9728 | HumanaVoluntaryBenefits.com
Policy: 00455 Underwritten by Kanawha Insurance Company, a Humana company.
Employee Summary - Portsmouth Public Schools Virginia
Humana Whole Life 99 rates Employee, Tobacco coverage, Defined Benefit amounts displaying monthly payroll deductions based on monthly premium calculation.
Age Benefit Amount
BENEFIT: $10,000 CASH VALUE* $20,000 CASH VALUE* $30,000 CASH VALUE*
55 $41.48 $4,330 $80.88 $8,661 $120.28 $12,991
56 $44.28 $4,391 $86.48 $8,782 $128.67 $13,173
57 $47.08 $4,454 $92.08 $8,909 $137.07 $13,363
58 $49.88 $4,519 $97.68 $9,037 $145.47 $13,556
59 $52.68 $4,584 $103.28 $9,167 $153.87 $13,751
60 $55.48 $4,565 $108.88 $9,130 $162.27 $13,696
61 $59.16 $4,661 $116.25 $9,322 $173.33 $13,982
62 $62.85 $4,759 $123.61 $9,519 $184.38 $14,278
63 $66.53 $4,857 $130.98 $9,714 $195.43 $14,571
64 $70.21 $4,951 $138.34 $9,902 $206.48 $14,852
65 $73.90 $5,040 $145.71 $10,079 $217.52 $15,119
66 $77.76 $5,126 $153.43 $10,251 $229.10 $15,377
67 $81.84 $5,207 $161.59 $10,413 $241.35 $15,620
68 $86.25 $5,276 $170.43 $10,553 $254.60 $15,829
69 $90.89 $5,336 $179.69 $10,673 $268.50 $16,009
70 $95.96 $5,392 $189.84 $10,784 $283.72 $16,177
*Cash values are for age 65 through age 45 and for 20 years for ages over 45.The proposed rates are for an effective date no later than January 1, 2014.
40

Humana Whole Life 99 rates
1-800-327-9728 | HumanaVoluntaryBenefits.com
Policy: 00455 Underwritten by Kanawha Insurance Company, a Humana company.
Employee Summary - Portsmouth Public Schools Virginia
Humana Whole Life 99 rates Employee, Non-tobacco coverage, Defined Benefit amounts displaying monthly payroll deductions based on monthly premium calculation.
Age Benefit Amount
BENEFIT: $40,000 CASH VALUE* $50,000 CASH VALUE* $75,000 CASH VALUE*
18 $20.65 $18,512 $25.29 $23,140 $36.89 $34,710
19 $21.61 $18,512 $26.50 $23,140 $38.70 $34,710
20 $22.08 $18,512 $27.08 $23,140 $39.58 $34,710
21 $22.88 $18,512 $28.08 $23,140 $41.08 $34,710
22 $23.71 $18,512 $29.12 $23,140 $42.64 $34,710
23 $24.51 $18,512 $30.12 $23,140 $44.14 $34,710
24 $25.35 $18,512 $31.16 $23,140 $45.70 $34,710
25 $26.15 $18,512 $32.16 $23,140 $47.20 $34,710
26 $27.15 $18,512 $33.41 $23,140 $49.08 $34,710
27 $28.11 $18,512 $34.62 $23,140 $50.89 $34,710
28 $29.11 $18,478 $35.87 $23,098 $52.77 $34,647
29 $30.08 $18,288 $37.08 $22,860 $54.58 $34,291
30 $31.08 $18,109 $38.33 $22,636 $56.45 $33,954
31 $32.61 $17,900 $40.25 $22,374 $59.33 $33,562
32 $34.15 $17,689 $42.16 $22,111 $62.20 $33,167
33 $35.68 $17,467 $44.08 $21,833 $65.08 $32,750
34 $37.21 $17,232 $45.99 $21,540 $67.95 $32,310
35 $38.75 $16,985 $47.91 $21,231 $70.83 $31,847
36 $40.68 $16,725 $50.33 $20,907 $74.45 $31,360
37 $42.61 $16,451 $52.74 $20,564 $78.08 $30,846
38 $44.54 $16,163 $55.16 $20,203 $81.70 $30,305
39 $46.48 $15,857 $57.58 $19,822 $85.33 $29,732
40 $48.41 $15,536 $59.99 $19,419 $88.95 $29,129
41 $51.14 $15,195 $63.41 $18,994 $94.08 $28,491
42 $53.91 $14,837 $66.87 $18,546 $99.26 $27,819
43 $56.64 $14,458 $70.29 $18,072 $104.39 $27,108
44 $59.41 $14,058 $73.74 $17,573 $109.58 $26,359
45 $62.14 $13,637 $77.16 $17,046 $114.70 $25,568
46 $66.21 $13,883 $82.24 $17,354 $122.33 $26,031
47 $70.24 $14,139 $87.28 $17,673 $129.89 $26,510
48 $74.31 $14,404 $92.37 $18,005 $137.51 $27,007
49 $78.38 $14,680 $97.45 $18,350 $145.14 $27,525
*Cash values are for age 65 through age 45 and for 20 years for ages over 45.The proposed rates are for an effective date no later than January 1, 2014.
41

Humana Whole Life 99 rates
1-800-327-9728 | HumanaVoluntaryBenefits.com
Policy: 00455 Underwritten by Kanawha Insurance Company, a Humana company.
Employee Summary - Portsmouth Public Schools Virginia
Humana Whole Life 99 rates Employee, Non-tobacco coverage, Defined Benefit amounts displaying monthly payroll deductions based on monthly premium calculation.
Age Benefit Amount
BENEFIT: $40,000 CASH VALUE* $50,000 CASH VALUE* $75,000 CASH VALUE*
50 $82.41 $14,966 $102.49 $18,708 $152.70 $28,061
51 $87.78 $15,263 $109.20 $19,078 $162.76 $28,617
52 $93.14 $15,567 $115.91 $19,458 $172.82 $29,188
53 $98.51 $15,878 $122.62 $19,848 $182.89 $29,772
54 $103.88 $16,198 $129.32 $20,248 $192.95 $30,372
55 $109.21 $16,530 $135.99 $20,662 $202.95 $30,993
56 $118.31 $16,872 $147.37 $21,090 $220.01 $31,635
57 $127.37 $17,225 $158.70 $21,532 $237.01 $32,298
58 $136.44 $17,587 $170.03 $21,984 $254.01 $32,976
59 $145.51 $17,954 $181.36 $22,442 $271.01 $33,663
60 $154.57 $17,986 $192.70 $22,482 $288.01 $33,723
61 $166.84 $18,474 $208.03 $23,092 $311.01 $34,639
62 $179.11 $18,949 $223.37 $23,686 $334.01 $35,529
63 $191.38 $19,414 $238.70 $24,268 $357.01 $36,401
64 $203.68 $19,872 $254.07 $24,840 $380.07 $37,260
65 $215.94 $20,319 $269.41 $25,399 $403.07 $38,098
66 $228.04 $20,761 $284.53 $25,951 $425.75 $38,926
67 $240.97 $21,224 $300.70 $26,530 $450.00 $39,796
68 $254.81 $21,675 $317.99 $27,094 $475.94 $40,641
69 $269.94 $22,102 $336.90 $27,627 $504.31 $41,440
70 $286.34 $22,519 $357.40 $28,149 $535.06 $42,224
*Cash values are for age 65 through age 45 and for 20 years for ages over 45.The proposed rates are for an effective date no later than January 1, 2014.
Humana Whole Life 99 rates Employee, Tobacco coverage, Defined Benefit amounts displaying monthly payroll deductions based on monthly premium calculation.
Age Benefit Amount
BENEFIT: $40,000 CASH VALUE* $50,000 CASH VALUE* $75,000 CASH VALUE*
18 $28.71 $21,174 $35.37 $26,467 $52.02 $39,701
19 $30.05 $21,174 $37.04 $26,467 $54.52 $39,701
20 $30.91 $21,174 $38.12 $26,467 $56.14 $39,701
21 $32.25 $21,174 $39.79 $26,467 $58.64 $39,701
*Cash values are for age 65 through age 45 and for 20 years for ages over 45.The proposed rates are for an effective date no later than January 1, 2014.
42
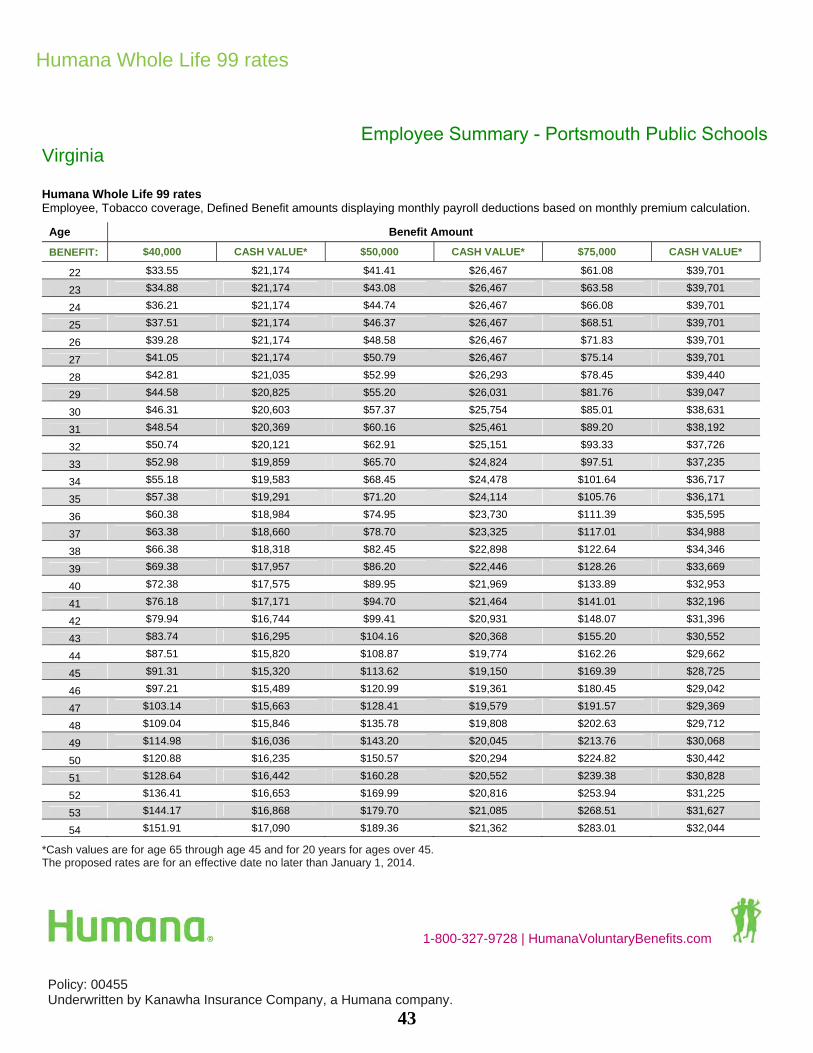
Humana Whole Life 99 rates
1-800-327-9728 | HumanaVoluntaryBenefits.com
Policy: 00455 Underwritten by Kanawha Insurance Company, a Humana company.
Employee Summary - Portsmouth Public Schools Virginia
Humana Whole Life 99 rates Employee, Tobacco coverage, Defined Benefit amounts displaying monthly payroll deductions based on monthly premium calculation.
Age Benefit Amount
BENEFIT: $40,000 CASH VALUE* $50,000 CASH VALUE* $75,000 CASH VALUE*
22 $33.55 $21,174 $41.41 $26,467 $61.08 $39,701
23 $34.88 $21,174 $43.08 $26,467 $63.58 $39,701
24 $36.21 $21,174 $44.74 $26,467 $66.08 $39,701
25 $37.51 $21,174 $46.37 $26,467 $68.51 $39,701
26 $39.28 $21,174 $48.58 $26,467 $71.83 $39,701
27 $41.05 $21,174 $50.79 $26,467 $75.14 $39,701
28 $42.81 $21,035 $52.99 $26,293 $78.45 $39,440
29 $44.58 $20,825 $55.20 $26,031 $81.76 $39,047
30 $46.31 $20,603 $57.37 $25,754 $85.01 $38,631
31 $48.54 $20,369 $60.16 $25,461 $89.20 $38,192
32 $50.74 $20,121 $62.91 $25,151 $93.33 $37,726
33 $52.98 $19,859 $65.70 $24,824 $97.51 $37,235
34 $55.18 $19,583 $68.45 $24,478 $101.64 $36,717
35 $57.38 $19,291 $71.20 $24,114 $105.76 $36,171
36 $60.38 $18,984 $74.95 $23,730 $111.39 $35,595
37 $63.38 $18,660 $78.70 $23,325 $117.01 $34,988
38 $66.38 $18,318 $82.45 $22,898 $122.64 $34,346
39 $69.38 $17,957 $86.20 $22,446 $128.26 $33,669
40 $72.38 $17,575 $89.95 $21,969 $133.89 $32,953
41 $76.18 $17,171 $94.70 $21,464 $141.01 $32,196
42 $79.94 $16,744 $99.41 $20,931 $148.07 $31,396
43 $83.74 $16,295 $104.16 $20,368 $155.20 $30,552
44 $87.51 $15,820 $108.87 $19,774 $162.26 $29,662
45 $91.31 $15,320 $113.62 $19,150 $169.39 $28,725
46 $97.21 $15,489 $120.99 $19,361 $180.45 $29,042
47 $103.14 $15,663 $128.41 $19,579 $191.57 $29,369
48 $109.04 $15,846 $135.78 $19,808 $202.63 $29,712
49 $114.98 $16,036 $143.20 $20,045 $213.76 $30,068
50 $120.88 $16,235 $150.57 $20,294 $224.82 $30,442
51 $128.64 $16,442 $160.28 $20,552 $239.38 $30,828
52 $136.41 $16,653 $169.99 $20,816 $253.94 $31,225
53 $144.17 $16,868 $179.70 $21,085 $268.51 $31,627
54 $151.91 $17,090 $189.36 $21,362 $283.01 $32,044
*Cash values are for age 65 through age 45 and for 20 years for ages over 45.The proposed rates are for an effective date no later than January 1, 2014.
43
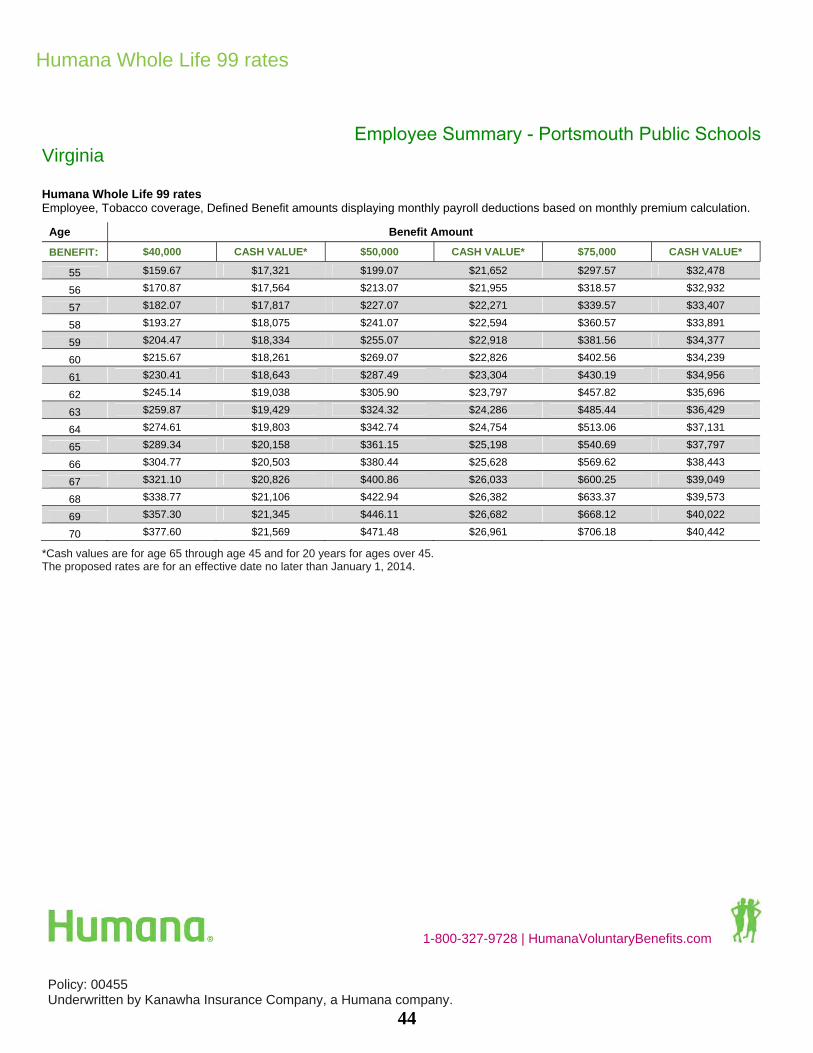
Humana Whole Life 99 rates
1-800-327-9728 | HumanaVoluntaryBenefits.com
Policy: 00455 Underwritten by Kanawha Insurance Company, a Humana company.
Employee Summary - Portsmouth Public Schools Virginia
Humana Whole Life 99 rates Employee, Tobacco coverage, Defined Benefit amounts displaying monthly payroll deductions based on monthly premium calculation.
Age Benefit Amount
BENEFIT: $40,000 CASH VALUE* $50,000 CASH VALUE* $75,000 CASH VALUE*
55 $159.67 $17,321 $199.07 $21,652 $297.57 $32,478
56 $170.87 $17,564 $213.07 $21,955 $318.57 $32,932
57 $182.07 $17,817 $227.07 $22,271 $339.57 $33,407
58 $193.27 $18,075 $241.07 $22,594 $360.57 $33,891
59 $204.47 $18,334 $255.07 $22,918 $381.56 $34,377
60 $215.67 $18,261 $269.07 $22,826 $402.56 $34,239
61 $230.41 $18,643 $287.49 $23,304 $430.19 $34,956
62 $245.14 $19,038 $305.90 $23,797 $457.82 $35,696
63 $259.87 $19,429 $324.32 $24,286 $485.44 $36,429
64 $274.61 $19,803 $342.74 $24,754 $513.06 $37,131
65 $289.34 $20,158 $361.15 $25,198 $540.69 $37,797
66 $304.77 $20,503 $380.44 $25,628 $569.62 $38,443
67 $321.10 $20,826 $400.86 $26,033 $600.25 $39,049
68 $338.77 $21,106 $422.94 $26,382 $633.37 $39,573
69 $357.30 $21,345 $446.11 $26,682 $668.12 $40,022
70 $377.60 $21,569 $471.48 $26,961 $706.18 $40,442
*Cash values are for age 65 through age 45 and for 20 years for ages over 45.The proposed rates are for an effective date no later than January 1, 2014.
44
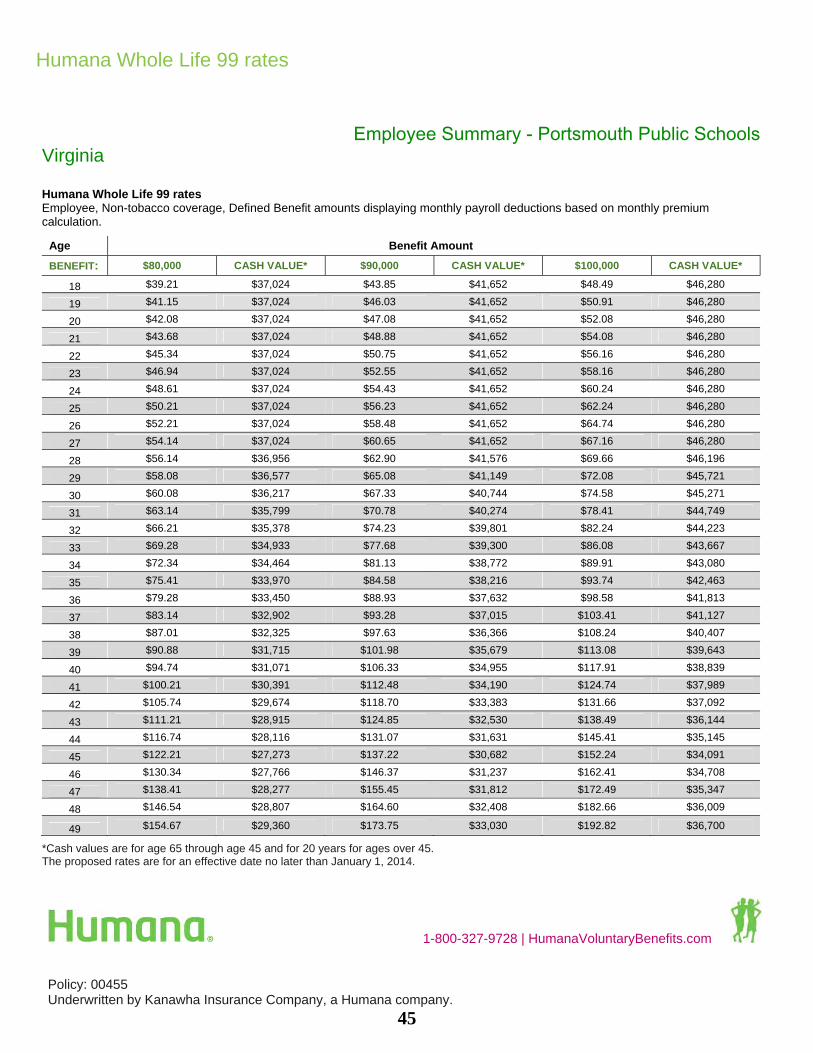
Humana Whole Life 99 rates
1-800-327-9728 | HumanaVoluntaryBenefits.com
Policy: 00455 Underwritten by Kanawha Insurance Company, a Humana company.
Employee Summary - Portsmouth Public Schools Virginia
Humana Whole Life 99 rates Employee, Non-tobacco coverage, Defined Benefit amounts displaying monthly payroll deductions based on monthly premium calculation.
Age Benefit Amount
BENEFIT: $80,000 CASH VALUE* $90,000 CASH VALUE* $100,000 CASH VALUE*
18 $39.21 $37,024 $43.85 $41,652 $48.49 $46,280
19 $41.15 $37,024 $46.03 $41,652 $50.91 $46,280
20 $42.08 $37,024 $47.08 $41,652 $52.08 $46,280
21 $43.68 $37,024 $48.88 $41,652 $54.08 $46,280
22 $45.34 $37,024 $50.75 $41,652 $56.16 $46,280
23 $46.94 $37,024 $52.55 $41,652 $58.16 $46,280
24 $48.61 $37,024 $54.43 $41,652 $60.24 $46,280
25 $50.21 $37,024 $56.23 $41,652 $62.24 $46,280
26 $52.21 $37,024 $58.48 $41,652 $64.74 $46,280
27 $54.14 $37,024 $60.65 $41,652 $67.16 $46,280
28 $56.14 $36,956 $62.90 $41,576 $69.66 $46,196
29 $58.08 $36,577 $65.08 $41,149 $72.08 $45,721
30 $60.08 $36,217 $67.33 $40,744 $74.58 $45,271
31 $63.14 $35,799 $70.78 $40,274 $78.41 $44,749
32 $66.21 $35,378 $74.23 $39,801 $82.24 $44,223
33 $69.28 $34,933 $77.68 $39,300 $86.08 $43,667
34 $72.34 $34,464 $81.13 $38,772 $89.91 $43,080
35 $75.41 $33,970 $84.58 $38,216 $93.74 $42,463
36 $79.28 $33,450 $88.93 $37,632 $98.58 $41,813
37 $83.14 $32,902 $93.28 $37,015 $103.41 $41,127
38 $87.01 $32,325 $97.63 $36,366 $108.24 $40,407
39 $90.88 $31,715 $101.98 $35,679 $113.08 $39,643
40 $94.74 $31,071 $106.33 $34,955 $117.91 $38,839
41 $100.21 $30,391 $112.48 $34,190 $124.74 $37,989
42 $105.74 $29,674 $118.70 $33,383 $131.66 $37,092
43 $111.21 $28,915 $124.85 $32,530 $138.49 $36,144
44 $116.74 $28,116 $131.07 $31,631 $145.41 $35,145
45 $122.21 $27,273 $137.22 $30,682 $152.24 $34,091
46 $130.34 $27,766 $146.37 $31,237 $162.41 $34,708
47 $138.41 $28,277 $155.45 $31,812 $172.49 $35,347
48 $146.54 $28,807 $164.60 $32,408 $182.66 $36,009
49 $154.67 $29,360 $173.75 $33,030 $192.82 $36,700
*Cash values are for age 65 through age 45 and for 20 years for ages over 45.The proposed rates are for an effective date no later than January 1, 2014.
45
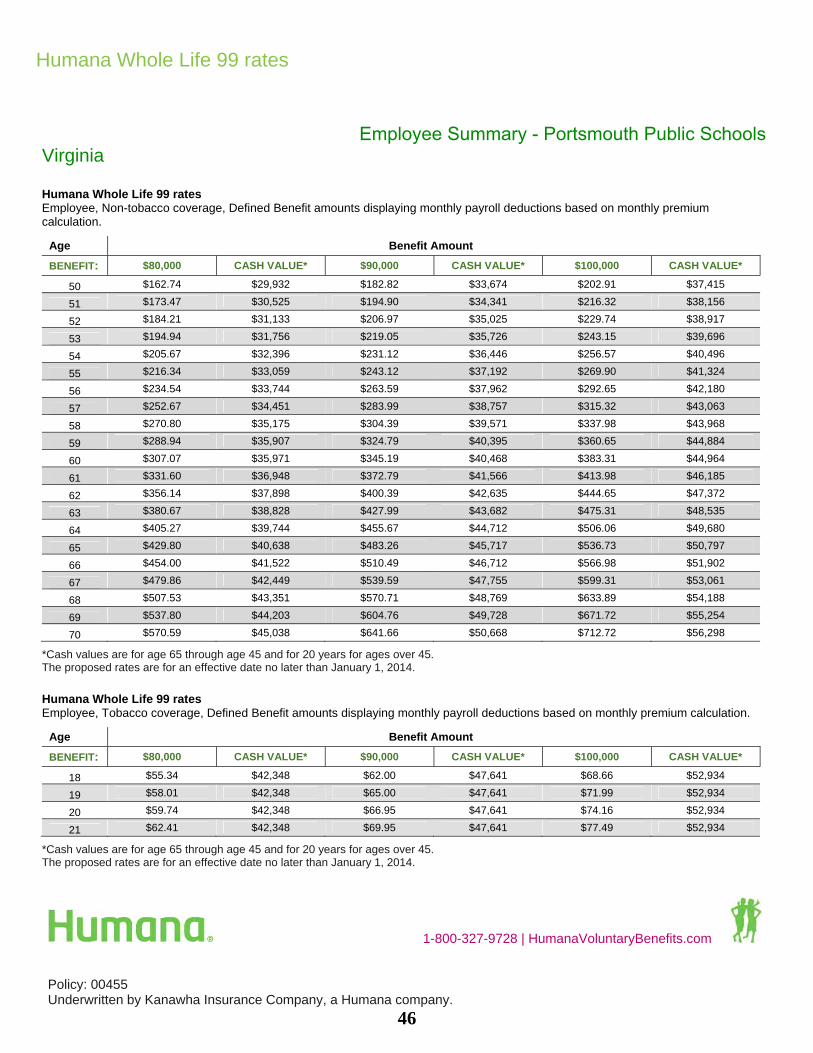
Humana Whole Life 99 rates
1-800-327-9728 | HumanaVoluntaryBenefits.com
Policy: 00455 Underwritten by Kanawha Insurance Company, a Humana company.
Employee Summary - Portsmouth Public Schools Virginia
Humana Whole Life 99 rates Employee, Non-tobacco coverage, Defined Benefit amounts displaying monthly payroll deductions based on monthly premium calculation.
Age Benefit Amount
BENEFIT: $80,000 CASH VALUE* $90,000 CASH VALUE* $100,000 CASH VALUE*
50 $162.74 $29,932 $182.82 $33,674 $202.91 $37,415
51 $173.47 $30,525 $194.90 $34,341 $216.32 $38,156
52 $184.21 $31,133 $206.97 $35,025 $229.74 $38,917
53 $194.94 $31,756 $219.05 $35,726 $243.15 $39,696
54 $205.67 $32,396 $231.12 $36,446 $256.57 $40,496
55 $216.34 $33,059 $243.12 $37,192 $269.90 $41,324
56 $234.54 $33,744 $263.59 $37,962 $292.65 $42,180
57 $252.67 $34,451 $283.99 $38,757 $315.32 $43,063
58 $270.80 $35,175 $304.39 $39,571 $337.98 $43,968
59 $288.94 $35,907 $324.79 $40,395 $360.65 $44,884
60 $307.07 $35,971 $345.19 $40,468 $383.31 $44,964
61 $331.60 $36,948 $372.79 $41,566 $413.98 $46,185
62 $356.14 $37,898 $400.39 $42,635 $444.65 $47,372
63 $380.67 $38,828 $427.99 $43,682 $475.31 $48,535
64 $405.27 $39,744 $455.67 $44,712 $506.06 $49,680
65 $429.80 $40,638 $483.26 $45,717 $536.73 $50,797
66 $454.00 $41,522 $510.49 $46,712 $566.98 $51,902
67 $479.86 $42,449 $539.59 $47,755 $599.31 $53,061
68 $507.53 $43,351 $570.71 $48,769 $633.89 $54,188
69 $537.80 $44,203 $604.76 $49,728 $671.72 $55,254
70 $570.59 $45,038 $641.66 $50,668 $712.72 $56,298
*Cash values are for age 65 through age 45 and for 20 years for ages over 45.The proposed rates are for an effective date no later than January 1, 2014.
Humana Whole Life 99 rates Employee, Tobacco coverage, Defined Benefit amounts displaying monthly payroll deductions based on monthly premium calculation.
Age Benefit Amount
BENEFIT: $80,000 CASH VALUE* $90,000 CASH VALUE* $100,000 CASH VALUE*
18 $55.34 $42,348 $62.00 $47,641 $68.66 $52,934
19 $58.01 $42,348 $65.00 $47,641 $71.99 $52,934
20 $59.74 $42,348 $66.95 $47,641 $74.16 $52,934
21 $62.41 $42,348 $69.95 $47,641 $77.49 $52,934
*Cash values are for age 65 through age 45 and for 20 years for ages over 45.The proposed rates are for an effective date no later than January 1, 2014.
46

Humana Whole Life 99 rates
1-800-327-9728 | HumanaVoluntaryBenefits.com
Policy: 00455 Underwritten by Kanawha Insurance Company, a Humana company.
Employee Summary - Portsmouth Public Schools Virginia
Humana Whole Life 99 rates Employee, Tobacco coverage, Defined Benefit amounts displaying monthly payroll deductions based on monthly premium calculation.
Age Benefit Amount
BENEFIT: $80,000 CASH VALUE* $90,000 CASH VALUE* $100,000 CASH VALUE*
22 $65.01 $42,348 $72.88 $47,641 $80.74 $52,934
23 $67.68 $42,348 $75.88 $47,641 $84.08 $52,934
24 $70.34 $42,348 $78.88 $47,641 $87.41 $52,934
25 $72.94 $42,348 $81.80 $47,641 $90.66 $52,934
26 $76.48 $42,348 $85.78 $47,641 $95.08 $52,934
27 $80.01 $42,348 $89.75 $47,641 $99.49 $52,934
28 $83.54 $42,069 $93.73 $47,328 $103.91 $52,586
29 $87.08 $41,650 $97.70 $46,856 $108.33 $52,062
30 $90.54 $41,206 $101.60 $46,357 $112.66 $51,508
31 $95.01 $40,738 $106.63 $45,830 $118.24 $50,922
32 $99.41 $40,241 $111.58 $45,272 $123.74 $50,302
33 $103.88 $39,718 $116.60 $44,682 $129.32 $49,647
34 $108.28 $39,165 $121.55 $44,061 $134.82 $48,957
35 $112.68 $38,583 $126.50 $43,406 $140.32 $48,229
36 $118.68 $37,968 $133.25 $42,714 $147.82 $47,460
37 $124.68 $37,321 $140.00 $41,986 $155.32 $46,651
38 $130.67 $36,636 $146.75 $41,216 $162.82 $45,795
39 $136.67 $35,914 $153.50 $40,403 $170.32 $44,892
40 $142.67 $35,150 $160.25 $39,544 $177.82 $43,938
41 $150.27 $34,342 $168.80 $38,635 $187.32 $42,928
42 $157.81 $33,489 $177.27 $37,675 $196.74 $41,861
43 $165.41 $32,589 $185.82 $36,663 $206.24 $40,736
44 $172.94 $31,639 $194.30 $35,594 $215.65 $39,549
45 $180.54 $30,640 $202.85 $34,470 $225.15 $38,300
46 $192.34 $30,978 $216.12 $34,850 $239.90 $38,722
47 $204.21 $31,327 $229.47 $35,243 $254.74 $39,159
48 $216.00 $31,693 $242.75 $35,654 $269.49 $39,616
49 $227.87 $32,072 $256.09 $36,081 $284.32 $40,090
50 $239.67 $32,471 $269.37 $36,530 $299.07 $40,589
51 $255.20 $32,884 $286.84 $36,994 $318.48 $41,105
52 $270.74 $33,306 $304.32 $37,470 $337.90 $41,633
53 $286.27 $33,736 $321.79 $37,953 $357.32 $42,170
54 $301.73 $34,180 $339.19 $38,452 $376.65 $42,725
*Cash values are for age 65 through age 45 and for 20 years for ages over 45.The proposed rates are for an effective date no later than January 1, 2014.
47

Humana Whole Life 99 rates
1-800-327-9728 | HumanaVoluntaryBenefits.com
Policy: 00455 Underwritten by Kanawha Insurance Company, a Humana company.
Employee Summary - Portsmouth Public Schools Virginia
Humana Whole Life 99 rates Employee, Tobacco coverage, Defined Benefit amounts displaying monthly payroll deductions based on monthly premium calculation.
Age Benefit Amount
BENEFIT: $80,000 CASH VALUE* $90,000 CASH VALUE* $100,000 CASH VALUE*
55 $317.27 $34,643 $356.67 $38,973 $396.06 $43,303
56 $339.67 $35,127 $381.86 $39,518 $424.06 $43,909
57 $362.07 $35,634 $407.06 $40,089 $452.06 $44,543
58 $384.46 $36,150 $432.26 $40,669 $480.06 $45,187
59 $406.86 $36,668 $457.46 $41,252 $508.06 $45,836
60 $429.26 $36,522 $482.66 $41,087 $536.06 $45,652
61 $458.73 $37,286 $515.81 $41,947 $572.89 $46,608
62 $488.20 $38,076 $548.96 $42,835 $609.73 $47,595
63 $517.66 $38,857 $582.11 $43,714 $646.56 $48,571
64 $547.13 $39,606 $615.26 $44,557 $683.39 $49,508
65 $576.59 $40,317 $648.41 $45,356 $720.22 $50,396
66 $607.46 $41,005 $683.13 $46,131 $758.80 $51,257
67 $640.12 $41,652 $719.88 $46,859 $799.63 $52,065
68 $675.46 $42,211 $759.63 $47,488 $843.80 $52,764
69 $712.52 $42,690 $801.33 $48,027 $890.13 $53,363
70 $753.12 $43,138 $847.00 $48,530 $940.88 $53,922
*Cash values are for age 65 through age 45 and for 20 years for ages over 45.The proposed rates are for an effective date no later than January 1, 2014.
48

1-800-327-9728 | HumanaVoluntaryBenefits.com
Virginia Spouse Summary - Portsmouth Public Schools
This is not a complete disclosure of plan qualifications and limitations. Please access our website to obtain a completed
list for the Workplace Voluntary Benefit products at Disclosure.Humana.com. Please review this information before
applying for coverage. The amount of benefits provided depends on the plan selected. Premiums will vary according to
the selection made.
Policy: 00455
Underwritten by Kanawha Insurance Company, a Humana company.
VOL8073
Humana Whole Life 99
Here's a simple, voluntary whole life policy you can get at a reasonable cost during your working years, when you
and your families need coverage the most. It's also a benefit that'll stay in place when retirement rolls around, too.
You buy a policy with guaranteed coverage and actual cash value. Coverage stays level and cash values stay with the
policy for as long as you have it, enabling you to take out funds as loans or buy paid-up coverage.
Coverage type Humana Whole Life 99 is an individual whole life insurance
product with premiums payable to age 99.
Benefit typeDefined benefit
Policyholder Spouse
Benefit amount Benefit amounts are available at various levels. You can choose:
• Spouse: $2,500 to $50,000
Issue ages Spouse stand-alone coverage: 18 - 70
Additional included benefits Terminal illness acceleration benefit: For the primary insured
provides an acceleration of up to 50 percent of the original
death benefit, base and term rider, amount including any ABI
amounts, upon diagnosis of a terminal illness. 12-month
waiting period.
Facility Care Acceleration Benefit: provides an acceleration of
one percent of the face amount, up to $2,000/month up to a
maximum of 36 months for Licensed Adult Day Care and/or up
to two percent of the face amount, up to $4,000/month up to a
maximum of 18 months for inpatient resident care. Benefits
cannot exceed the lesser of 36 percent of the face amount,
$72,000, or the face amount of the policy less the cash value.
Stand-alone Spouse Coverage Simplified Issue - Up to $50,000
49

1-800-327-9728 | HumanaVoluntaryBenefits.com
Virginia Spouse Summary - Portsmouth Public Schools
This is not a complete disclosure of plan qualifications and limitations. Please access our website to obtain a completed
list for the Workplace Voluntary Benefit products at Disclosure.Humana.com. Please review this information before
applying for coverage. The amount of benefits provided depends on the plan selected. Premiums will vary according to
the selection made.
Policy: 00455
Underwritten by Kanawha Insurance Company, a Humana company.
VOL8073
Humana Whole Life 99
Product restrictions • Total amount of permanent life insurance coverage and term
life insurance coverage with Kanawha Insurance Company
not to exceed $300,000.
• If both parents are eligible employees, their eligible children
may be insured by either spouse but not both.
• Purchasing option, whether money purchase or flat face
amount, will be determined by the employer.
• When optional riders are selected, the weekly money
purchase premium will be calculated to include the base
benefit and any rider(s) (per applicant).
• If an employee's base policy, rider(s), and any additional
Kanawha Insurance Company life insurance products exceed
our company maximum of $300,000, we will first reduce the
applicant's rider(s) on this coverage. If additional reductions
are necessary, we will reduce the face amount of the
base policy.
Age calculation Age at effective date of policy
Portability Yes
Guarantee renewable Yes
Cash value Whole Life 99 is a whole life policy with guaranteed values, not
an interest sensitive policy. As such, there is not an interest rate
associated with the cash value of the policy; the cash values are
all guaranteed in the table of cash values inside each and every
Whole Life policy.
50

Humana Whole Life 99 rates
1-800-327-9728 | HumanaVoluntaryBenefits.com
Policy: 00455 Underwritten by Kanawha Insurance Company, a Humana company.
Spouse Summary - Portsmouth Public Schools Virginia
Humana Whole Life 99 rates Spouse, Non-tobacco coverage, Defined Benefit amounts displaying monthly payroll deductions based on monthly premium calculation.
Age Benefit Amount
BENEFIT: $5,000 CASH VALUE* $10,000 CASH VALUE* $15,000 CASH VALUE*
18 $4.53 $2,405 $6.98 $4,811 $9.43 $7,216
19 $4.66 $2,405 $7.25 $4,811 $9.83 $7,216
20 $4.80 $2,405 $7.51 $4,811 $10.23 $7,216
21 $4.93 $2,405 $7.78 $4,811 $10.63 $7,216
22 $5.06 $2,405 $8.05 $4,811 $11.03 $7,216
23 $5.20 $2,405 $8.31 $4,811 $11.43 $7,216
24 $5.33 $2,405 $8.58 $4,811 $11.83 $7,216
25 $5.46 $2,405 $8.85 $4,811 $12.23 $7,216
26 $5.64 $2,405 $9.20 $4,811 $12.77 $7,216
27 $5.82 $2,405 $9.55 $4,811 $13.29 $7,216
28 $6.00 $2,394 $9.91 $4,787 $13.83 $7,181
29 $6.18 $2,371 $10.27 $4,741 $14.37 $7,112
30 $6.35 $2,346 $10.63 $4,692 $14.90 $7,039
31 $6.59 $2,320 $11.10 $4,641 $15.60 $6,961
32 $6.82 $2,293 $11.56 $4,586 $16.30 $6,880
33 $7.05 $2,265 $12.02 $4,529 $16.99 $6,794
34 $7.28 $2,234 $12.49 $4,469 $17.69 $6,703
35 $7.52 $2,202 $12.95 $4,405 $18.39 $6,607
36 $7.84 $2,169 $13.60 $4,338 $19.37 $6,506
37 $8.16 $2,133 $14.25 $4,267 $20.33 $6,400
38 $8.48 $2,096 $14.89 $4,192 $21.29 $6,288
39 $8.80 $2,057 $15.53 $4,113 $22.25 $6,170
40 $9.13 $2,015 $16.17 $4,030 $23.22 $6,045
41 $9.56 $1,971 $17.04 $3,942 $24.52 $5,913
42 $9.99 $1,924 $17.90 $3,849 $25.82 $5,773
43 $10.43 $1,875 $18.77 $3,751 $27.12 $5,626
44 $10.86 $1,824 $19.64 $3,647 $28.42 $5,471
45 $11.29 $1,769 $20.50 $3,539 $29.72 $5,308
46 $11.91 $1,800 $21.75 $3,599 $31.58 $5,399
47 $12.53 $1,831 $22.99 $3,662 $33.44 $5,493
48 $13.16 $1,864 $24.24 $3,727 $35.32 $5,591
49 $13.78 $1,897 $25.48 $3,795 $37.18 $5,692
50 $14.40 $1,932 $26.72 $3,865 $39.04 $5,797
*Cash values are for age 65 through age 45 and for 20 years for ages over 45.The proposed rates are for an effective date no later than January 1, 2014.
51

Humana Whole Life 99 rates
1-800-327-9728 | HumanaVoluntaryBenefits.com
Policy: 00455 Underwritten by Kanawha Insurance Company, a Humana company.
Spouse Summary - Portsmouth Public SchoolsVirginia
Humana Whole Life 99 rates Spouse, Non-tobacco coverage, Defined Benefit amounts displaying monthly payroll deductions based on monthly premium calculation.
Age Benefit Amount
BENEFIT: $5,000 CASH VALUE* $10,000 CASH VALUE* $15,000 CASH VALUE*
51 $15.20 $1,969 $28.33 $3,938 $41.45 $5,907
52 $16.01 $2,006 $29.94 $4,012 $43.87 $6,018
53 $16.82 $2,044 $31.55 $4,088 $46.29 $6,132
54 $17.62 $2,083 $33.16 $4,166 $48.70 $6,250
55 $18.43 $2,123 $34.77 $4,247 $51.12 $6,370
56 $19.78 $2,165 $37.48 $4,330 $55.18 $6,495
57 $21.13 $2,208 $40.19 $4,416 $59.24 $6,624
58 $22.49 $2,252 $42.90 $4,503 $63.30 $6,755
59 $23.84 $2,295 $45.60 $4,591 $67.36 $6,886
60 $25.20 $2,297 $48.31 $4,594 $71.43 $6,891
61 $27.83 $2,355 $53.58 $4,709 $79.33 $7,064
62 $30.47 $2,411 $58.85 $4,821 $87.23 $7,232
63 $33.10 $2,465 $64.12 $4,931 $95.14 $7,396
64 $35.74 $2,519 $69.39 $5,038 $103.04 $7,557
65 $38.37 $2,571 $74.66 $5,142 $110.94 $7,713
66 $40.37 $2,628 $78.66 $5,256 $116.94 $7,884
67 $42.56 $2,682 $83.04 $5,365 $123.52 $8,047
68 $44.88 $2,733 $87.67 $5,466 $130.47 $8,199
69 $47.44 $2,780 $92.80 $5,560 $138.15 $8,340
70 $50.13 $2,825 $98.18 $5,650 $146.23 $8,476
*Cash values are for age 65 through age 45 and for 20 years for ages over 45.The proposed rates are for an effective date no later than January 1, 2014.
52

Humana Whole Life 99 rates
1-800-327-9728 | HumanaVoluntaryBenefits.com
Policy: 00455 Underwritten by Kanawha Insurance Company, a Humana company.
Spouse Summary - Portsmouth Public SchoolsVirginia
Humana Whole Life 99 rates Spouse, Non-tobacco coverage, Defined Benefit amounts displaying monthly payroll deductions based on monthly premium calculation.
Age Benefit Amount
BENEFIT: $20,000 CASH VALUE* $25,000 CASH VALUE*
18 $11.88 $9,622 $14.33 $12,027
19 $12.41 $9,622 $15.00 $12,027
20 $12.95 $9,622 $15.66 $12,027
21 $13.48 $9,622 $16.33 $12,027
22 $14.01 $9,622 $17.00 $12,027
23 $14.55 $9,622 $17.66 $12,027
24 $15.08 $9,622 $18.33 $12,027
25 $15.61 $9,622 $19.00 $12,027
26 $16.33 $9,622 $19.89 $12,027
27 $17.03 $9,622 $20.77 $12,027
28 $17.75 $9,574 $21.66 $11,968
29 $18.46 $9,482 $22.56 $11,853
30 $19.18 $9,385 $23.45 $11,731
31 $20.11 $9,282 $24.62 $11,602
32 $21.05 $9,173 $25.79 $11,466
33 $21.96 $9,058 $26.93 $11,323
34 $22.90 $8,937 $28.10 $11,172
35 $23.83 $8,810 $29.27 $11,012
36 $25.13 $8,675 $30.89 $10,844
37 $26.41 $8,533 $32.50 $10,667
38 $27.70 $8,384 $34.10 $10,480
39 $28.98 $8,226 $35.70 $10,283
40 $30.26 $8,060 $37.31 $10,074
41 $32.00 $7,883 $39.47 $9,854
42 $33.73 $7,698 $41.64 $9,622
43 $35.46 $7,502 $43.81 $9,377
44 $37.20 $7,295 $45.97 $9,119
45 $38.93 $7,077 $48.14 $8,846
46 $41.41 $7,198 $51.24 $8,998
47 $43.89 $7,324 $54.35 $9,155
48 $46.39 $7,454 $57.47 $9,318
49 $48.88 $7,590 $60.58 $9,487
50 $51.36 $7,730 $63.68 $9,662
*Cash values are for age 65 through age 45 and for 20 years for ages over 45.The proposed rates are for an effective date no later than January 1, 2014.
53

Humana Whole Life 99 rates
1-800-327-9728 | HumanaVoluntaryBenefits.com
Policy: 00455 Underwritten by Kanawha Insurance Company, a Humana company.
Spouse Summary - Portsmouth Public SchoolsVirginia
Humana Whole Life 99 rates Spouse, Non-tobacco coverage, Defined Benefit amounts displaying monthly payroll deductions based on monthly premium calculation.
Age Benefit Amount
BENEFIT: $20,000 CASH VALUE* $25,000 CASH VALUE*
51 $54.58 $7,876 $67.70 $9,845
52 $57.79 $8,025 $71.72 $10,031
53 $61.03 $8,176 $75.76 $10,221
54 $64.24 $8,333 $79.79 $10,416
55 $67.46 $8,494 $83.81 $10,617
56 $72.88 $8,660 $90.58 $10,825
57 $78.29 $8,832 $97.35 $11,040
58 $83.71 $9,007 $104.12 $11,259
59 $89.13 $9,182 $110.89 $11,477
60 $94.54 $9,187 $117.66 $11,484
61 $105.08 $9,419 $130.83 $11,773
62 $115.61 $9,643 $143.99 $12,053
63 $126.16 $9,862 $157.18 $12,327
64 $136.69 $10,076 $170.35 $12,595
65 $147.23 $10,284 $183.51 $12,855
66 $155.23 $10,511 $193.51 $13,139
67 $163.99 $10,730 $204.47 $13,412
68 $173.26 $10,933 $216.05 $13,666
69 $183.51 $11,120 $228.87 $13,901
70 $194.28 $11,301 $242.32 $14,126
*Cash values are for age 65 through age 45 and for 20 years for ages over 45.The proposed rates are for an effective date no later than January 1, 2014.
54

55

56

57

58

59

60

61

62

63
64

B E W E L L . B E S M A RT. B E P R O T E C T E D .
Allstate at Work®
heart/strokeinsuranceHeartCare Plus
No one likes to think about getting heart disease or having a stroke. This year anestimated 785,000 Americans will have a new coronary attack and about 470,000will have a recurrent attack. Coronary Heart Disease is the largest killer ofAmerican males and females, but on average, someone in the U.S. has a strokeevery 40 seconds. About 795,000 people experience a new or recurrent stroke eachyear.1 While you may not be able to prevent the disease, you can help protect your-self from its costs. The American Heart Association estimates the total direct and indirect costs ofCardiovascular Diseases and stroke in 2009 is $238.8 billion; CVD costing about$165.4 billion and stroke costing about $73.4 billion.1 You can help protect your-self and your family from these costs. HeartCare Plus insurance provides benefitsthat can help with the indirect costs.
HeartCare Plus insurance helps you:
� Manage the high expenses of treatment� Preserve your savings� Protect your family from financial hardship� Concentrate on getting well
Would your finances survive a heart attack or stroke?
AWD7718-2 Page 1 of 4
1. Heart Disease and Stroke Statistics, American Heart Association, 2009 Update.
65

Hospitalization and Related Benefits
Allstate Workplace Division’s (AWD) Heart/Stroke Plus (HSP2 Policy)
Hospital Confinement – Amount shown per day for each day a covered person is admitted and confinedas an inpatient in a hospital due to a Heart Attack, Heart Disease or Stroke.
Physician’s Attendance – Amount shown per day for the services of a physician during a coveredhospital confinement. Payable only for the number of days the hospital confinement benefit is payable.
Inpatient Drugs and Medicine – Amount shown per day for drugs or medicine required during acovered hospital confinement. Payable only for the number of days the hospital confinement benefit is payable.
Private Duty Nursing – Amount shown per day for private nursing care and attendance by a nurseduring a covered hospital confinement, subject to a maximum of 60 days per continuous hospitalconfinement. Must be required and authorized by attending physician.
Physiotherapy – Amount shown per day for physiotherapy performed by a licensed physicaltherapist during a covered hospital confinement, subject to a maximum of 60 days per continuoushospital confinement.
Oxygen – Amount shown for the use of oxygen equipment during a covered hospital confinement,subject to a maximum of 1 payment per continuous hospital confinement.
Cardiograms – Amount shown for an electrocardiogram, echocardiogram, phonocardiogram or vector-cardiogram required during a covered hospital confinement, subject to a maximum of 1 payment percontinuous hospital confinement.
Cerebral or Carotid Angiogram – Amount shown for a cerebral or carotid angiogram requiredduring a covered hospital confinement, subject to a maximum of 1 payment per continuous hospitalconfinement.
Coronary Angioplasty – Amount shown for a coronary angioplasty procedure, regardless of the numberof blood vessels repaired during the procedure.
Pacemaker Insertion – Amount shown for the initial insertion of a permanent pacemaker.
Thromboendarterectomy – Amount shown for a thromboendarterectomy operation.
Coronary Artery Bypass Graft Operation – Amount shown for a coronary artery bypass graftoperation, regardless of the number of grafts performed during the operation.
Heart Transplant – Amount shown for the implantation of a natural human heart. This benefit is onlypayable once per covered person.
Cardiac Catheterization – Amount shown for a cardiac catheterization procedure.
Surgery and Anesthesia – 1. Surgery. Amount shown in the surgical schedule for a surgery performedin a hospital or ambulatory surgical center. For a surgical procedure not listed in the surgical schedule,we pay $17 per unit of coverage ($8.50 per half unit) multiplied by the 1964 California Relative ValueSchedule (C.R.V.S.) unit value for the procedure, subject to maximum of amount shown. If no 1964C.R.V.S. unit value exists for the procedure, then the payment amount will be based upon relativedifficulty and payment amounts for other procedures, up to maximum amount shown. Two or moresurgical or invasive procedures done at the same time and through a common incision or entry point areconsidered one operation and benefit is paid for the one with the largest total benefit. 2. Anesthesia.Additional percentage shown of the amount paid for surgery benefit described in “1” above foranesthesia received during the surgery. 3. Ambulatory Surgical Center. Amount shown when surgerybenefit described in “1” above is paid for a surgery performed at an ambulatory surgical center. Thesebenefits do not pay for surgeries covered by other benefits in the policy.
Surgery and Related Benefits
ENHANCEDBASIC PREMIER
* Benefit amounts in blue are the same for Basic, Enhanced, and Premier packages.
$200/day
$25/day
$25/day
$100/day
$50/day
$200
$100
$150
$750
$1,000
$2,500
$2,500
$100,000
$500
1. $5,000 maximum
2. 25%
3. $250
Page 2 of 4 AWD7718-2 66

PREMIER
Blood, Plasma and Platelets – Amount shown for the administration of blood, plasma or plateletsduring a covered hospital confinement, subject to a maximum of 1 payment per continuous hospitalconfinement.
Second Surgical Opinion – Amount shown for a second opinion obtained after a positive diagnosis thatresults in the physician recommending surgery for a covered illness. Payable only once per covered person.
Ambulance – Amount shown for transfer by ground ambulance or ambulance to a hospital oremergency room for the treatment of a covered condition.
Non-Local Transportation – Amount shown for a covered hospital confinement which is obtained morethan 100 miles from the covered person’s home because the prescribed treatment cannot be obtainedlocally. This is subject to a maximum of 1 payment per continuous hospital confinement.
Family Member Lodging and Transportation – 1. Lodging. Amount shown per day when the Non-Local Transportation benefit is paid and a family member stays in a motel, hotel, or any otheraccommodation acceptable to us, in order to be near the covered person, subject to a maximum of 60days per continuous hospital confinement. 2. Transportation. Amount shown when the Non-LocalTransportation benefit is paid and a family member travels more than 100 miles from their home to benear the covered person for a portion of their continuous hospital confinement. This is subject to amaximum of 1 payment per continuous hospital confinement.
Cancer Initial Diagnosis Rider (CIDR1) – Pays a one-time benefit ($10,000 for one unit of coverage)when a covered person is positively diagnosed for the first time ever as having cancer (other than skincancer) as defined in the rider. The first diagnosis must occur after the rider date and while the rider isin force on such covered person. This benefit is payable only once for each covered person.
Hospital Intensive Care Rider (ICR90) – The optional hospital intensive care rider is not diseasespecific and pays a benefit for a covered confinement in a hospital intensive care unit for any coveredillness or accident from the very first day of confinement.
Hospital Intensive Care Confinement Benefit - $100 each day for each unit of coverage (or $50 each dayfor each unit at age 70 and older) for intensive care unit confinement for any covered illness or accident,subject to a maximum of 45 days for each continuous hospital intensive care unit confinement.
Ambulance Benefit - Actual charges for transportation by a licensed ambulance service to the hospitalfor admission to an intensive care unit. This benefit is not paid if an ambulance benefit is paid underthe policy.
Surgery and Related Benefits - cont
Optional Rider Benefits
Issue Ages 18-64.
BASIC ENHANCED
* Benefit amounts in blue are the same for Basic, Enhanced, and Premier packages.
$200 ground$400 air
$200
1. $50/day2. $200
n/a $10,000 one $10,000 one time benefit time benefit
n/a n/a $200/day
n/a n/a Actual Charges
Basic Package Premiums - 1 unitHeartCare Plus (HSP2)
Weekly Weekly
$4.15 $8.00
Monthly Monthly
$17.96 $34.64
Enhanced Package Premiums - 1 unitHeartCare Plus (HSP2) adding 1 unit ofCancer Initial Diagnosis Rider (CIDR1)
Premier Package Premiums - 1 unitHeartCare Plus (HSP2) adding 1 unit of CancerInitial Diagnosis Rider (CIDR1) and 2 units ofHospital Intensive Care Rider (ICR90)
INDIVIDUAL FAMILY (if covered)
Weekly Weekly
$7.29 $14.27
Monthly Monthly
$31.56 $61.84
INDIVIDUAL FAMILY (if covered)
Weekly Weekly
$7.79 $15.29
Monthly Monthly
$33.76 $66.24
INDIVIDUAL FAMILY (if covered)
Transportation and Lodging Benefits Optional Rider Benefits
$100
$200
Rates and benefits shown are for states listed on the back of the brochure. For states not listed, variations to benefits, premiums,exclusions and limitations may apply. The policy and riders may not be available in all states. Ask your agent for details.
AWD7718-2 Page 3 of 467

Rev. 5/09. This material is valid as long as information remains current, but in no event later than May 1, 2012. Benefits provided by policyform HSP2, or state variations thereof. Intensive Care Rider provided by rider ICR90, or state variations thereof. Cancer Initial Diagnosis Riderprovided by rider CIDR1, or state variations thereof. Underwritten by American Heritage Life Insurance Company. This brochure highlightssome features of the policy and riders but is not the insurance contract. Only the actual policy and rider provisions control. The policy and ridersset forth, in detail, the rights and obligations of both the insured and the insurance company. The policy and optional riders are not a MedicareSupplement Policy. If eligible for Medicare, review Medicare Supplement Buyer’s Guide available from Allstate Workplace Division.
Allstate Workplace Division is the marketing name used by American Heritage Life Insurance Company (Home Office, Jacksonville, FL), awholly-owned subsidiary of The Allstate Corporation. ©2009 Allstate Insurance Company. The Workplace Marketer® www.allstate.com orallstateatwork.com
Renewability - The policy is guaranteed renewable for life, subject to change in premiums by class. A notice will be mailed in advance of anychange.
Eligibility/Termination - Family coverage may include you, your spouse and dependent children as defined in the policy. If the insured’s spouseis a covered person, the spouse’s coverage ends upon valid decree of divorce. If your child is a covered person, the child’s coverage ends on thepolicy anniversary next following the date the child is no longer eligible, which is either when the child marries or reaches age 21 (25 if a fulltime student at an educational institution of higher learning beyond high school). Coverage does not terminate on an unmarried child who: 1. is incapable of self-sustaining employment by reason of mental retardation or physical handicap; 2. became so incapacitated prior to theattainment of the limiting age for eligibility under the policy; and 3. is chiefly dependent upon you for support and maintenance. Dependentcoverage continues as long as the policy remains in force and the dependent child remains in such condition.
Policy Exclusions and Limitations - The policy provides benefits only for Heart Attack, Heart Disease or Stroke. The policy does not coverany other disease or sickness or incapacity other than Heart Attack, Heart Disease or Stroke even though such disease, sickness or incapacitymay be caused, complicated or otherwise affected by Heart Attack, Heart Disease or Stroke. If a covered confinement is due to more than onecovered condition, benefits will be payable as though the confinement were due to one condition. If a confinement due to a covered disease isalso due to a condition that is not covered, benefits will be payable only for the part of the confinement attributable to the covered condition.Exclusions and limitations to the policy also apply to the riders.
Pre-Existing Condition Limitation for Policy and Riders - A pre-existing condition is a condition not revealed in the application for which:symptoms existed within a 1 year period before the effective date of coverage; or medical advice or treatment was recommended by or receivedfrom a physician within the 1 year period before the effective date of coverage. � If a covered person has a pre-existing condition as defined,we do not pay benefits for such conditions under the policy or any riders attached to the policy during the 12 month period beginning on thedate that person became a covered person. If the loss is not due to a pre-existing condition, then the pre-existing condition limitation does notapply. All losses are subject to the Incontestability provision.
Cancer Initial Diagnosis Rider (CIDR1) and Intensive Care Rider (ICR90) Exclusions and Limitations - Hospital Intensive Care Rider(ICR90) We do not pay for intensive care confinement if you are admitted because of: a pre-existing condition as defined in the policy; or anattempted suicide or intentional self-inflicted injury (CO, MO - while sane); or intoxication or being under the influence of drugs not prescribedor recommended by a physician(n/a - DC) (OK - any loss sustained or contracted in consequence of the insured’s being under the influence ofany narcotic unless administered on the advice of a physician); or alcoholism or drug addiction (n/a - DC). We do not pay for confinements inany care unit that does not qualify as a hospital intensive care unit. The following do not qualify as “Hospital Intensive Care Units”: progres-sive care units; or sub-acute intensive care units; or intermediate care units; or private room with monitoring; or step-down units; or any otherlesser care treatment units.
Cancer Initial Diagnosis Rider (CIDR1) We do not pay a benefit under the rider for any disease other than cancer as defined in the rider.
Rates and benefits shown are for states listed on the back of the brochure. For states not listed, variations to benefits, premiums, exclu-sions and limitations may apply. The policy and riders may not be available in all states. Ask your agent for details.
The policy is a Limited Benefit Policy with Riders.
This brochure is for use in AL, AK, CO, DC, HI, IA, KS, KY, MO, NV, OH,OK, PR, AND VI.
For states not listed, this brochure is incomplete without state-specific rate and rider inserts.
Page 4 of 4 AWD7718-2 68

This brochure is a brief description of coverage and is not a contract. Read your certificate carefully for exact terms and conditions. Definitions, waiting period, pre-existing condition limitation, limitations and exclusions, benefits, termination, portability, etc., may vary based on your employer's home office. Please see your agent for the plan details specific to your employer.
groUP CritiCaL iLLness CiG
Peace of mind andreal Cash Benefits
CAI2875 IC(3/10)
Includes Cancer and Wellness
69

CiGgroUP CritiCaL iLLnessPolicy Series CAI2800 This brochure is a brief description of coverage and is not a contract. Read your certificate carefully for exact terms and conditions.
You can win the battle against a critical illness, but can you handle the added costs?a group cr i t ica l i l lness p lan he lps prepare you for the added costs of bat t l ing a spec i f ic cr i t ica l i l lness .The good news is that many people with a critical illness survive these life-threatening battles. Unfortunately, as the recovery process begins, people become aware of the medical bills that have piled up.
Your recovery doesn’ t have to be spoi led by medica l b i l ls .With this plan, our goal is to help you and your family cope with and recover from the financial stress of surviving a critical illness.
C O V E R A G E W O R K S H E E T
Employee Benefit: $ ___________________
Spouse Benefit: $ ___________________
Child Benefit: $ ___________________(25 percent of the primary insured amount)
Total Weekly Deduction: $ ___________________
This work sheet is for illustration purposes only. It does not imply coverage.70

over
1.4 Fa C t
miLLionThe number of new cancer cases that were
expected to be diagnosed in 2009.3
3Cancer Facts & Figures 2009, American Cancer Society.
CiG
$50 HeaLtH sCreening BeneFit (employee and spouse only)After the waiting period, an insured may receive a maximum of $50 for any one covered health screening test per calendar year. We will pay this benefit regardless of the results of the test. Payment of this benefit will not reduce the critical illness benefit payable under your certificate. There is no limit to the number of years the insured can receive the health screening benefit; it will be paid as long as the certificate remains in force. This benefit is payable for the covered Employee and Spouse. This benefit is not paid for Dependent Children.
C ov ered He a Lt H sCreen ing t es t s inC LUde:• Mammography • Colonoscopy • Pap smear • Breast ultrasound • Chest X-ray • PSA (blood test for prostate cancer) • Stress test on a bicycle or treadmill • Bone marrow testing • CA 15-3 (blood test for breast cancer)
• CA 125 (blood test for ovarian cancer) • CEA (blood test for colon cancer) • Flexible sigmoidoscopy • Hemocult stool analysis • Serum protein electrophoresis (blood test for myeloma) • Thermography • Fasting blood glucose test • Serum cholesterol test to determine level of HDL and LDL
B e N e F i t s This brochure is a brief description of coverage and is not a contract. Read your certificate carefully for exact terms and conditions.
First-oCCUrrenCe BeneFit After the waiting period, a lump sum benefit is payable upon initial diagnosis of a covered critical illness. Employee benefit amounts available from $5,000 to $50,000. Spouse coverage is also available in benefit amounts up to $25,000. If you are deemed ineligible due to a previous medical condition, you still retain the ability to purchase Spouse coverage.
addit ionaL oCCUrrenCe BeneFit If an insured collects full benefits for a critical illness under the plan and later has one of the remaining covered critical illnesses, then we will pay the full benefit amount for each additional illness. Occurrences must be separated by at least six months.
re-oCCUrrenCe BeneFit If an insured collects full benefits for a covered condition and is later diagnosed with the same condition, we will pay the full benefit again. The two dates of diagnosis must be separated by at least 12 months, or for cancer, 12 months treatment free. Cancer that has spread (metastasized) even though there is a new tumor, will not be considered an additional occurrence unless the Insured has gone treatment free for 12 months.
CHiLd Coverage at no addit ionaL Cost Each Dependent Child is covered at 25 percent of the primary insured amount at no additional charge.
Covered Crit iCaL iLLnesses: 1
CANCER (Internal or Invasive) 100%HEART ATTACK (Myocardial Infarction) 100%STROKE (Apoplexy or Cerebral Vascular Accident) 100%MAJOR ORGAN TRANSPLANT 100%
RENAL FAILURE (End-Stage) 100%CARCINOMA IN SITU2 25% CORONARY ARTERY BYPASS SURGERY2 25%
1All covered conditions are subject to the definitions found in your certificate.2If a benefit is paid for Carcinoma in Situ, the Internal Cancer benefit will be reduced by 25 percent. If a benefit is paid for Coronary Artery Bypass Surgery, the Heart Attack benefit will be reduced by 25 percent.
What is Not Covered, LimitatioNs aNd eXCLUsioNs, aNd terms YoU Need to KNoW
iF d iagnosis oCCUrs aFter tHe age oF 70, HaLF oF tHe BeneFit is PaYaBLe. The plan contains a 30-day waiting period. This means that no benefits are payable for any insured who has been diagnosed before your coverage has been in force 30 days from the effective date. If an insured is first diagnosed during the waiting period, benefits for treatment of that critical illness will apply only to loss starting after 12 months from the Effective Date or the Employee can elect to void the coverage and receive a full refund of premium.
The applicable benefit amount will be paid if: the date of diagnosis is after the waiting period; the date of diagnosis occurs while the certificate is in force; and the cause of the illness is not excluded by name or specific description.
exCLUsionsBenefits will not be paid for loss due to:• Intentionally self-inflicted injury or action;• Suicide or attempted suicide while sane or insane;• Illegal activities or participation in an illegal occupation;
71

• War, whether declared or undeclared or military conflicts, participation in an insurrection or riot, civil commotion or state of belligerence;
• Substance abuse; or• Pre-Existing Conditions (except as stated below).
No benefits will be paid for loss which occurred prior to the Effective Date.
No benefits will be paid for diagnosis made or treatment received outside of the United States.
Pre-existing Condit ion L imitationPre-existing Condition means a sickness or physical condition which, within the 12-month period prior to the Effective Date, resulted in the insured receiving medical advice or treatment.
We will not pay benefits for any critical illness starting within 12 months of the Effective Date which is caused by, contributed to, or resulting from a Pre-Existing Condition. A claim for benefits for loss starting after 12 months from the Effective Date will not be reduced or denied on the grounds that it is caused by a Pre-Existing Condition. A critical illness will no longer be considered pre-existing at the end of 12 consecutive months starting and ending after the Effective Date.
terms YoU need to KnoWThe effective date of your insurance will be the date shown in your Certificate Schedule.
employee means the insured as shown in the Certificate Schedule.
spouse means an Employee's legal wife or husband.
dependent Children means your natural children, stepchildren, legally adopted children, or children placed for adoption, who are unmarried, chiefly dependent on you or your Spouse for support, and younger than age 25.
However, if any child is incapable of self-sustaining employment due to mental retardation or physical handicap and is dependent on a parent(s) for support, the above age of 25 limitation shall not apply. Proof of such incapacity and dependency must be furnished to the company within 31 days following such child‘s 25th birthday.
treatment means consultation, care, or services provided by a physician, including diagnostic measures and taking prescribed drugs and medicines.
major organ transplant means undergoing surgery as a recipient of a transplant of a human heart, lung, liver, kidney, or pancreas.
myocardial infarction (Heart attack) means the death of a portion of the heart muscle (myocardium) resulting from a blockage of one or more coronary arteries. Heart Attack does not include any other disease or injury involving the cardiovascular system. Cardiac arrest not caused by a Myocardial Infarction is not a Heart Attack. The diagnosis must include all of the following criteria: 1. New and serial eletrocardiographic (EKG) findings consistent with Myocardial Infarction; 2. Elevation of cardiac enzymes above generally accepted laboratory levels of normal [in case of creatine phosphokinase (CPK), a CPK-MB measurement must be used]; and 3. Confirmatory imaging studies such as thallium scans, MUGA scans, or stress echocardiograms.
stroke means apoplexy (due to rupture or acute occlusion of a cerebral artery), or a cerebral vascular accident or incident which is first manifested on or after your Effective Date. Stroke does not include transient ischemic attacks and attacks of vertebrobasilar ischemia. We will pay a benefit for Stroke that produces permanent clinical neurological sequela following an initial diagnosis
made after any applicable Waiting Period. We must receive evidence of the permanent neurological damage provided from computed axial tomography (CAT scan) or magnetic resonance imaging (MRI). Stroke does not mean head injury, transient ischemic attack, or chronic cerebrovascular insufficiency.
Cancer (Internal or Invasive) means a malignant tumor characterized by the uncontrolled growth and spread of malignant cells and the invasion of distant tissue. Cancer includes leukemia. Excluded are Cancers that are noninvasive, such as (1) Premalignant tumors or polyps; (2) Carcinoma in Situ; (3) Any skin cancers except melanomas; (4) Basal cell carcinoma and squamous cell carcinoma of the skin; and (5) Melanoma that is diagnosed as Clark’s Level I or II or Breslow thickness less than .77 mm.
Cancer is also defined as a disease which meets the diagnosis criteria of malignancy established by The American Board of Pathology after a study of the histocytologic architecture or pattern of the suspect tumor, tissue, or specimen.
Carcinoma in situ means Cancer that is in the natural or normal place, confined to the site of origin without having invaded neighboring tissue.
renal Failure (Kidney Failure) means the end-stage renal failure presenting as chronic, irreversible failure of both of your kidneys to function. The Kidney Failure must necessitate regular renal dialysis, hemodialysis or peritoneal dialysis (at least weekly); or which results in kidney transplantation. Renal failure is covered, provided it is not caused by a traumatic event, including surgical traumas.
Coronary artery Bypass surgery means undergoing open heart surgery to correct narrowing or blockage of one or more coronary arteries with bypass grafts, but excluding procedures such as but not limited to balloon angioplasty, laser relief, stents or other nonsurgical procedures.
A doctor, physician, or pathologist does not include an insured or a family member.
P or ta B L e C ov er ageWhen coverage would otherwise terminate because the Employee ends employment with the employer, coverage may be continued. The Employee will continue the coverage that is in force on the date employment ends, including dependent coverage then in effect.
The Employee will be allowed to continue the coverage until the earlier of the date the Employee fails to pay the required premium or the date the group master policy is terminated. Coverage may not be continued if the Employee fails to pay any required premium or the group master policy terminates.
terminationCoverage will terminate on the earliest of: (1) The date the master policy is terminated; (2) The 31st day after the premium due date if the required premium has not been paid; (3) The date the insured ceases to meet the definition of an Employee as defined in the master policy; or (4) The date the Employee is no longer a member of the class eligible.
Coverage for an insured Spouse or Dependent Child will terminate on the earliest of: (1) The date the master policy is terminated; (2) The 31st day after the premium due date if the required premium has not been paid; (3) The premium due date following the date the Spouse or Dependent Child ceases to be a dependent; or (4) The premium due date following the date we receive a written request to terminate coverage for a Spouse and/or Dependent Children.
We’ve got you under our wing.®aflacgroupinsurance.com 1.800.433.3036
What is Not Covered, LimitatioNs aNd eXCLUsioNs, aNd terms YoU Need to KNoW
the certificate to which this sales material pertains is written only in english; the certificate prevails if interpretation of this material varies.
this brochure is a brief description of coverage and is not a contract. read your certificate carefully for exact terms and conditions. this brochure is subject to the terms, conditions, and limitations of Policy Form series Cai2800.
Underwritten by: Continental American Insurance Company2801 Devine Street | Columbia, South Carolina 29205
72

Age $5,000 $10,000 $15,000 $20,000 $25,000 $30,000 $35,000 $40,000 $45,000
18-29 $1.11 $2.22 $3.33 $4.44 $5.55 $6.66 $7.77 $8.88 $9.99
30-39 $2.04 $4.08 $6.12 $8.16 $10.20 $12.24 $14.28 $16.32 $18.36
40-49 $4.14 $8.28 $12.42 $16.56 $20.70 $24.84 $28.98 $33.12 $37.26
50-59 $7.48 $14.96 $22.44 $29.92 $37.40 $44.88 $52.36 $59.84 $67.32
60-69 $12.00 $24.00 $36.00 $48.00 $60.00 $72.00 $84.00 $96.00 $108.00
CAIC GROUP CRITICAL ILLNESS Series 2800 - NON- TOBACCO for Employee Buy Up Rates
Age $5,000 $10,000 $15,000 $20,000 $25,000 $30,000 $35,000 $40,000 $45,000
18-29 $1.86 $3.72 $5.58 $7.44 $9.30 $11.16 $13.02 $14.88 $16.74
30-39 $3.51 $7.02 $10.53 $14.04 $17.55 $21.06 $24.57 $28.08 $31.59
40-49 $8.70 $17.40 $26.10 $34.80 $43.50 $52.20 $60.90 $69.60 $78.30
50-59 $15.00 $30.00 $45.00 $60.00 $75.00 $90.00 $105.00 $120.00 $135.00
60-69 $24.00 $48.00 $72.00 $96.00 $120.00 $144.00 $168.00 $192.00 $216.00
Age $5,000 $7,500 $10,000 $12,500 $15,000 $17,500 $20,000
18-29 $1.11 $1.67 $2.22 $2.78 $3.33 $3.89 $4.44
30-39 $2.04 $3.06 $4.08 $5.10 $6.12 $7.14 $8.16
40-49 $4.14 $6.21 $8.28 $10.35 $12.42 $14.49 $16.56
50-59 $7.48 $11.22 $14.96 $18.70 $22.44 $26.18 $29.92
60-69 $12.00 $18.00 $24.00 $30.00 $36.00 $42.00 $48.00
Age $5,000 $7,500 $10,000 $12,500 $15,000 $17,500 $20,000
18-29 $1.86 $2.79 $3.72 $4.65 $5.58 $6.51 $7.44
30-39 $3.51 $5.27 $7.02 $8.78 $10.53 $12.29 $14.04
40-49 $8.70 $13.05 $17.40 $21.75 $26.10 $30.45 $34.80
50-59 $15.00 $22.50 $30.00 $37.50 $45.00 $52.50 $60.00
60-69 $24.00 $36.00 $48.00 $60.00 $72.00 $84.00 $96.00
CAIC GROUP CRITICAL ILLNESS Series 2800 - TOBACCO for Spouse Buy Up Rates
CAIC GROUP CRITICAL ILLNESS Series 2800 - TOBACCO for Employee Buy Up Rates
CAIC GROUP CRITICAL ILLNESS Series 2800 - NON-TOBACCO for Spouse Buy Up Rates
Rates include cancer benefit.
Maximum total benefit for Employees is $50,000 and for Spouses is $25,000.
Virginia CI Buy up Rates 20 pay Rate sheet prepared by Web User on 8/9/2013 9:08:09 AM.
Virginia Payroll Premium rates are 20pp/yr. Aflac Group coverage is underwritten by Continental American Insurance Company (CAIC). 1-800-433-3036
The rates shown on this insert page are for illustration purposes only; they do not imply coverage. For more information about policy/plan benefits and limitations, please refer to the accompanying
product brochure for each insurance policy/plan listed below.
73

LIMITED BENEFIT ACCIDENT ONLY Insurance Plan
Underwritten by American Fidelity Assurance Company
First Financial Administrators, Inc.P.O. Box 670329 • Houston, TX 77267-0329
Local (281) 847-8422 | Toll Free (800) 523-8422 | Fax (866) 265-4594www.ffga.com
Wellness Benefit · Benefits Paid Directly to You · Excellent Customer Service · Learn More » »
Marketed by:
74

Whether you’re a weekend warrior with an active lifestyle or just a busy family, accidents can happen to you anytime, anywhere without warning. First Financial is pleased to offer American Fidelity Assurance Company’s (AFA) Limited Benefit Accident Only Insurance. Accident Only Insurance can offer a solution to help you and your family prepare for those rising medical costs if you have to receive medical treatment for an Accidental injury.
Think It Couldn’t Happen to You? Consider this...
How Would You Cover Your Out-of-Pocket Costs?Just going for a walk around the block or heading to your driveway could lead to a twisted knee and torn meniscus, one of the more common claims submitted under this plan.
Know The Facts:
EMERGENCY ACCIDENT - Hypothetical Example1
Twisted knee in the parking lot resulting in a torn meniscus and treatment is received within 72 hours.
ENHANCED PLAN BENEFITSAccident Emergency Treatment $200Accident Follow-Up Treatment (4 visits) $200Physical Therapy (8 treatments) $200Medical Imaging $200X-Ray $100Appliances $100Surgical Facility $250Torn Knee Cartilage Repair $500Anesthesia $200
Total $1,950
Paid DirectlyTo You!
Accident Only Insurance
Life Provides the Accidents,First Financial Offers a Solution!
1Hypothetical example of a covered accident based on policy AO-03 and rider AMDI-258.
$19,216Total costs of accidental injuries averaged $19,216 per injury in 2010.National Safety Council, Injury Facts, 2012 Edition, p. 2-4.
75

Ready To Learn More?Contact your First Financial Account Representative for more details or to schedule an one-on-one appointment.
Marketed by: First Financial Group of America
Solutions For Life’s Accidents...
Accident Only Insurance Features:
The Accident Only Plan is the insurance policy that provides payments direct to you protecting you and your family from some of the expenses brought about by injuries suffered in an Accident, regardless of any additional coverage you may have. It’s guaranteed renewable for as long as you pay your premiums.
» No medical questions. » Benefits paid directly to you, to be
used however you see fit. » Benefits regardless of other coverage. » Coverage for you and each covered
family member 24 hours a day, 7 days a week.
» Available conveniently through your employer with payroll deduction.
» Policy is guaranteed renewable at the option of the primary insured for life as long as premiums are paid as required. Any additional insureds must meet eligibility as outlined in the policy. The company has the right to change premium rates by class.
[Account Rep Name HereFirst Financial Group of America11811 N. Freeway, Suite 900 Houston, TX 77060Local: (281) 847-8422 / Toll Free: (800)523-8422]www.ffga.com
The Choice is Yours:Be prepared with either of American Fidelity’s two plan options (Basic and Enhanced) that provide the benefit amounts you require. Plus, American Fidelity supplies the coverage you need with four choices of coverage including individual, individual and spouse, individual and child(ren), and family.
Currently participating in, or possibly moving to a High Deductible Health Plan? Health Savings Account (HSA) and qualified High Deductible Health Plan enrollments have quadrupled in the past six years and are on the rise2.
2AHIP: January 2012 Census Shows 13.5 Million People covered by HSA/High-Deductible Health Plans, May 2012, p.3.
76

Emergency Accident Benefits Basic Enhanced
Emergency Accident TreatmentEmergency Accident Treatment $150 $200
Emergency Accident Follow-up Treatment(up to four visits)
$50 $50
Accident Injury BenefitsBenefit amounts for the following Benefits are the same for Basic and Enhanced Plans for all Persons: Primary, Spouse, and Child(ren).
Basic / Enhanced
Injury TreatmentFractures Benefit (Depending on open or closed reduction, bone involved, or chip fracture). $25 to $3,000
Lacerations Benefit Not requiring sutures Sutured lacerations up to two inches Sutured lacerations totaling two to six inches Sutured lacerations totaling over six inches
$25$100$200$400
Appliances Benefit (crutches, leg braces, etc.) $100
Torn Knee Cartilage or Ruptured Disc Benefit $500
Eye Injury Benefit Injury with surgical repair, for one or both eyes. Removal of foreign body by a Physician, for one or both eyes.
$250$50
Dislocations BenefitDepending on open or closed reduction, with or without anesthesia and joint involved. No other amount will be paid under this benefit.
$25 to $3,000
Concussion Benefit $200
2nd & 3rd Degree Burns(Skin gra�s are 25% of benefit) $100 to $10,000
Internal Injuries BenefitResulting in open abdominal or thoracic surgery $1,000
Paralysis Benefit: Paraplegia / Quadriplegia $5,000 / $10,000
Tendons, Ligaments and Rotator Cuff Benefit One Tendon, Ligament or Rotator Cuff More than One Tendon, Ligament or Rotator Cuff
$500$750
Blood, Plasma and Platelets $250
Exploratory Surgery without Surgical Repair $250
Physical Therapy (per treatment up to eight treatments) $25
Prosthesis $500
Emergency Dental Work Broken teeth repaired with crown Extraction of broken teeth (regardless of number)
$150$50
Refer to Plan Benefit Highlights for complete Benefit Descriptions and limits on the Accident Only Insurance Plan.
Schedule of Benefits3
77

Wellness Benefit Basic Enhanced
WellnessAnnual Routine Physical Exam (Requires a 12-month waiting period before use and one exam per policy per calendar year.)
$50 $75
Refer to Plan Benefit Highlights for complete Benefit Descriptions and limits on the Accident Only Insurance Plan.
A Highlight of Benefits Available Under The Plan
Basic Enhanced
Non-Emergency Accident TreatmentNon-Emergency Accident Treatment $75 $100
Non-Emergency Follow-up Treatment (up to two visits) $50 $50
Hospital ConfinementHospital Admission $500 $1,000
Intensive Care Unit (up to 15 days) $300 $600
Hospital Confinement (up to 365 days) $100 $200
Medical ImagingMRI, CT, CAT, PET, US $200 $200
X-Rays $50 $100
AmbulanceGround $300 $300
Air $1,500 $1,500
TreatmentOutpatient Hospital or Ambulatory Surgical Center $150 $250
Anesthesia $150 $200
Transportation BenefitsTransportation (Patient Only)(per round trip for up to three round trips per calendar year)
$300 $300
Family Member Lodging and Meals(per day per Accident; up to 30 days per confinement)
$100 $100
Additional Accident Benefits
Accidental Death & Dismemberment BenefitAccidental Death & DismembermentBasic Primary Spouse ChildCommon Carrier $50,000 $50,000 $25,000Other Accident $15,000 $15,000 $7,500Dismemberment $1,000 to $15,000 $1,000 to $15,000 $500 to $7,500Enhanced Primary Spouse ChildCommon Carrier $100,000 $100,000 $50,000Other Accident $30,000 $30,000 $15,000Dismemberment $1,500 to $30,000 $1,500 to $30,000 $750 to $15,000
78

Plan Benefit HighlightsA Covered Person (therea¤er referred to as “Person”) under American Fidelity’s Limited Benefit Accident Only Policy can expect the following benefits when a Covered Accident (therea¤er referred to as “Accident”) happens. All benefits are paid once per Person per Accident unless otherwise specified. All benefits are only paid as a result of Injuries received in an Accident that occurs while coverage is in force. Benefits are not be paid for loss from sickness. All treatment, procedures, and medical equipment must be diagnosed, recommended and treated by a Physician. These references are not intended to change or modify any definitions in the AO-03 policy series.
Accident Emergency Treatment BenefitPayable for receiving emergency treatment in a Physician’s office or emergency room within 72 hours, including physician fees and emergency services.
Accident Follow-up Treatment BenefitPayable for necessary follow-up treatment of Injuries in addition to the emergency treatment administered within 72 hours for up to four treatments. Not payable for a visit in which a Physical Therapy Benefit or Non-Emergency Follow-Up Benefit is paid.
Accidental Death and Dismemberment BenefitThe applicable benefits apply when a Accidental Death or Dismemberment occurs within 90 days of an Accident. Or, if Accidental Death or Dismemberment occurs within one year from the date of the Covered Person’s accident and during a period of continuous total disability resulting from the Accident and commencing within 30 days of the date of the Accident, we will pay the applicable benefit. “Total Disability” as used in this benefit means that the Person is: unable to work at any job for which (s)he is qualified by education, training or experience; and not working at any job for pay or benefits; and under the care of a Physician.
Ambulance BenefitIf air and ground transportation is required for the same Accident, only the highest benefit will be paid.
Anesthesia BenefitPays the amount shown in the Schedule of Benefits for the services of an anesthesiologist for a surgery performed due to an Accident. Hospital Confinement is not required to receive this benefit. We will only pay one Anesthesia Benefit per Person in a 24-hour period even if more than one surgical procedure is performed. This benefit is not payable for local anesthesia.
Appliances BenefitPayable for one of the following: crutches, leg braces, back braces, walkers, or wheel chairs. Not payable for Prosthetic Devices.
Blood, Plasma and Platelets BenefitPayable for blood, plasma and platelets. This benefit does not provide benefits for immunoglobulins.
Burns BenefitPayable for burns when treated by a Physician within 72 hours.
Concussion BenefitPayable for a Person who sustains a concussion and is diagnosed by a Physician within 72 hours using any type of medical imaging.
Dislocations BenefitAmount payable varies by the joint involved, type of treatment, and type of anesthesia. If a Person receives more than one Dislocation in an Accident, we will pay for all Dislocations up to two times the amount shown in the Schedule of Benefits for the Dislocation involved that has the highest benefit amount. No other amount will be paid under this benefit. Benefits are payable only for the first dislocation of a joint which occurs while this policy is in force.
Emergency Dental Work BenefitPayable for repair to natural teeth when treated by a Physician or dentist. Initial dental treatment must be received within 72 hours.
Exploratory Surgery BenefitPayable when an exploratory surgical operation without surgical repair is performed.
Eye Injury BenefitPayable for one or both eyes requiring treatment.
Family Member Lodging and Meals Benefit Payable for lodging and meals for a family member to be near a Person who is Confined in a non-local Hospital. The Hospital must be at least 50 miles one way from the Person’s residence or site of the Accident.
Fractures BenefitVaries based on the bone involved, type of fracture and type of treatment. If the Person fractures more than one bone, payment is made for all fractures up to two times the amount for the bone involved that has the highest benefit amount.
Hospital Admission Benefit Pays per admission for confinement to a Hospital. This benefit does not pay for outpatient treatment, emergency room treatment, or a stay of less than 18 hours in an observation unit.
Hospital Confinement Benefit Payable for a one-time Hospital Admission Benefit due to accidental Injuries (does not include emergency room and outpatient treatment). You will also receive a daily benefit for a Hospital Confinement that is longer than 18 hours for up to 365 days and an additional daily benefit for Confinement in an Intensive Care Unit up to 15 days.
Intensive Care Unit BenefitPayable for each day of confinement in an Intensive Care Unit, as defined in the policy, up to 15 days. This benefit is paid in addition to the Hospital Confinement Benefit amount.
Internal Injuries Benefit Payable for an open abdominal or thoracic surgery performed within 72 hours.
Lacerations BenefitThis benefit varies based on the severity of the laceration.
Medical Imaging Benefit Payable for a Magnetic Resonance Imaging (MRI), a Computed Tomography (CT) scan, a Computed Axial Tomography (CAT) scan, a Positron Emission Tomography (PET) scan or an ultrasound.
79

Non-Emergency Accident Initial Treatment Benefit Payable for initial medical treatment when treatment is received more than 72 hours after the Accident. Initial medical treatment must: (1) be received in a Physician’s office or emergency room; and (2) be the first treatment; and (3) occur within 30 days.
Non-Emergency Accident Follow-up Treatment Benefit Payable only if the Non-Emergency Accident Initial Treatment Benefit is payable and later requires additional treatment: we will pay over and above the initial medical treatment administered. We will pay for up to two treatments. Not payable for the same visit that the Physical Therapy Benefit or the Accident Follow-Up Benefit is paid.
Outpatient Hospital or Ambulatory Surgical Center BenefitWhen a surgical procedure is performed on an outpatient basis in a Hospital or at an Ambulatory Surgical Center, we will pay the indemnity amount shown in the Schedule of Benefits for the facility fee charged by such Hospital or Ambulatory Surgical Center. We will only pay one Outpatient Hospital or Ambulatory Surgical Center Benefit in a 24-hour period even if more than one surgical procedure is performed. This benefit will not be paid for surgery performed in a Hospital emergency room or in a Physician’s office.
Paralysis BenefitThe duration of the Paralysis must be a minimum of 3 consecutive months. Paid once per lifetime per Person.
Physical Therapy BenefitPayable for one treatment per day for up to eight treatments by a caregiver licensed in physical therapy. This benefit is not payable for the same visit that the Accident Follow-up Treatment Benefit or Non-Emergency Follow-Up Benefit.
Prosthesis BenefitPayable for the use of a Prosthesis. This benefit is not payable for hearing aids; dental aids; eyeglasses; false teeth; or for cosmetic aids such as wigs.
Tendons, Ligaments and Rotator Cuff BenefitPayable for the repair of one or more tendons, ligaments, or rotator cuffs. The tendons, ligaments, or rotator cuff must be repaired through surgery.
Torn Knee Cartilage or Ruptured Disc BenefitPayable for surgical repair.
Transportation Benefit Payable for the transportation when specialized treatment and Hospital Confinement in a non-local Hospital is required. A non-local Hospital must be at least 50 miles away, one way, using the most direct route, from the closer of the Person’s residence or site of the Accident. Travel must be by scheduled bus, plane, train, or by car. Ambulance service does not qualify for this benefit. The treatment must be prescribed by a Physician and not be available locally.
Wellness BenefitAfter coverage is in force for the waiting period shown, you can receive a benefit for an annual routine physical exam, including immunizations and preventive testing. Services must be supervised by a Physician and a charge must be incurred for the service. The benefit does not apply to dental or eye exams and is payable once per policy per calendar year.
Limitations and ExclusionsBase PolicyNo benefits will be provided for an Accident that is caused by or occurs as a result of:
(1) intentionally self-inflicted bodily injury, suicide or attempted suicide, whether sane or insane;
(2) participation in any form of flight aviation other than as a fare-paying passenger in a fully licensed/passenger-carrying aircraft;
(3) any act that was caused by war, declared or undeclared, or service in any of the armed forces;
(4) participation in any activity or event while under the influence of any narcotic unless administered by a Physician or taken according to the Physician’s instructions;
(5) participation in, or attempting to participate in, a felony, riot or insurrection. (A felony is as defined by the law of the jurisdiction in which the activity takes place.).
Benefits will not be provided for medical treatment for an Accident received outside the United States or its territories. Benefits will not be paid for services rendered by a member of the immediate family of a Person.
An Accident is defined as a sudden, unexpected and unintended event, which results in bodily injury, which is independent of disease or bodily infirmity or any other cause. The policy will not pay benefits for injuries received prior to the Effective Date of coverage that are aggravated or re-injured by any event that occurs after the Effective Date.
A hospital is not an institution, or part thereof, used as: a hospice unit, including any bed designated as a hospice or a swing bed; a convalescent home; a rest or nursing facility; a rehabilitative facility; an extended-care facility; a skilled nursing facility; or a facility primarily affording custodial, educational care, or care or treatment for persons suffering from mental diseases or disorders, or care for the aged, or drug or alcohol addiction.
You cannot be singled out for a rate increase for any reason. The Insurer has the right to increase premium rates only if rates for all policies in this class change.
This is a brief description of the coverage. For actual benefits, limitations, exclusions and other provisions, please refer to the policy, AO-03, and Accident Only Benefit Enhancement Rider, AMDI-258 Series. This coverage does NOT replace Workers’ Compensation Insurance. This product is inappropriate for people who are eligible for Medicaid coverage.
80

Accident Only Insurance PremiumsMonthly Premiums
Basic EnhancedIndividual $19.90 $26.10
Individual & Spouse $28.30 $34.90
Individual & Child(ren) $31.50 $41.00
Family $39.90 $49.803The premium and amount of benefits provided vary based upon the plan selected.
SB-25787(VA)-0113 AO-03 Series and AMDI-258 Series
2000 N. Classen Boulevard • Oklahoma City, Oklahoma 73106 • 800-654-8489 • www.americanfidelity.com
Underwritten and administered by:
Plan Options » Individual Plan
The Insured, age 18 through 64, at the date of policy issue, is the only Person.
» Individual and Lawful Spouse Plan Covers you and your Lawful Spouse (ages 18 to 64 at Policy Issue).
» Individual and Child(ren) Plan Covers you (ages 18 to 64 at Policy Issue) and each Eligible Child, as defined in the policy, under the age of 21 or 25 if
attending school full-time.
» Family Plan Covers you, your Lawful Spouse (ages 18 to 64 at Policy Issue) and each Eligible Child, as defined in the policy, under
the age of 21 or 25 if attending school full-time.
81

Portsmouth Public Schools Focus Eye Care Highlight Sheet
Focus® Plan Summary – Comprehensive Plan VSP Network Out of Network
Deductibles Exam $15 $15 Eye Glass Lenses See materials See materials Materials $15 $15
Annual Eye Exam Covered in full Up to $45 Lenses (per pair)
Single Vision Covered in full Up to $35 Bifocal Covered in full Up to $50 Trifocal Covered in full Up to $70 Lenticular Covered in full Up to $90
Contacts Fit & Follow Up Exams 15% discount No benefit See Additional Focus Features. Elective Up to $105 Up to $105 Medically Necessary Covered in full Up to $210
Frames $120 Up to $50 Frequencies (months)
Exam/Lens/Frame 12/12/24 12/12/24 Based on date of service Based on date of service
Rates – 20 Pay Employee Only (EE) $5.82 Family $14.26 Additional Focus® Features Contact Lenses Elective Cost of the fitting and evaluation is deducted from the allowance and any amount left is deducted
from the material allowance. Allowance can be applied to disposables, but the dollar amount must be used all at once (provider will order 3 or 6 month supply). Applies when contacts chosen in lieu of glasses.
Additional Glasses 20% discount off the retail price on additional pairs of prescription glasses (complete pair). Laser VisionCare VSP offers an average discount of 15% on LASIK and PRK. The maximum out-of-pocket per eye
for members is $1,800 for LASIK and $2,300 for custom LASIK using Wavefront technology, and $1,500 for PRK. In order to receive the benefit, a VSP provider must coordinate the procedure.
Low Vision With prior authorization, 75% of approved amount (up to $1,000 is covered every two years). Eye Care Plan Member Service Focus eye care from Ameritas Group features the money-saving eye care network of VSP. Customer service is available to plan members through VSP's well-trained and helpful service representatives. Call or go online to locate the nearest VSP network provider, view plan benefit information and more. VSP Call Center: 1-800-877-7195 Service representative hours: 9 a.m. to 10 p.m. EST Monday through Friday Interactive Voice Response available 24/7 Locate a VSP provider at: ameritasgroup.com/provider View plan benefit information at: vsp.com If you would like a complete copy of your vision insurance certificate, please visit our website at www.ameritasgroup.com. This document is a highlight of plan benefits provided by Ameritas Life Insurance Corp. as selected by your employer. It is not a certificate of insurance and does not include exclusions and limitations. For exclusions and limitations, or a complete list of covered procedures, contact your benefits administrator.
82

RETIREMENT
101
1 of 2PRODUCTS AND FINANCIAL SERVICES PROVIDED BY AMERICAN UNITED LIFE INSURANCE COMPANY®, A ONEAMERICA® COMPANY
© 2013 OneAmerica Financial Partners, Inc. All rights reserved.
LEARN MORE ABOUT YOUR 403(b) PLAN
R-20447 12/24/13
Q: What is a 403(b) plan?A: A section 403(b) plan is a deferred compensation program that is available to employees of a tax exempt organization under IRC §501(c)(3), and employees of certain educational organizations, such as K-12 public schools, community colleges and state-funded colleges and universities.
Q: What advantages are there to participating in a 403(b) plan?A: Participating in a 403(b) plan is a good way to invest money for retirement. You can reduce your current income taxes and set aside money for your retirement at the same time. Most people pay taxes on their income first and use what is left over to put money into preparing for retirement. Since federal income taxes are calculated on your income after your retirement plan contribution has been deducted, you may pay less in federal income taxes. Thus, you may actually have more spendable income than you would if you were contributing a comparable amount to a savings account where contributions and earnings are subject to current income taxation.
Q: How does a 403(b) plan work?A: You decide how much of your salary you want your employer to contribute to your account within the limits established by the federal government. You then complete a salary reduction agreement with your employer.
Q: How much of my compensation can I contribute to a 403(b) plan?A: For the 2014 calendar year, you may contribute $17,500. This amount will be adjusted for inflation as needed in future years. Additional deferral amounts for participants 50 years and older and, in general, for participants who complete 15 years of service with a qualified organization are available through “catch-up” contributions. Check with your retirement plan representative to see if your plan allows “catch-up” contributions.
Q: How can I change the amount that is contributed to my 403(b) account?A: Notify your employer that you would like to change your salary deferral amount. You may increase or decrease your contributions periodically according to your employer’s plan. In some cases, changes may be done online at www.oneamerica.com.
Q: When can I withdraw my 403(b) contributions?A: Like other retirement plans, a 403(b) plan is intended to be a long-term retirement investment vehicle. As permitted by your plan, withdrawals may be allowed when you reach age 59½, terminate employment, retire, die, become disabled or experience a financial hardship. Withdrawals, both contributions and earnings, will be subject to ordinary income taxes in the year in which you receive the money. Withdrawals prior to age 59½ may also be subject to a 10 percent IRS tax penalty.
Questions and answersabout 403(b) plans
83

2 of 2PRODUCTS AND FINANCIAL SERVICES PROVIDED BY AMERICAN UNITED LIFE INSURANCE COMPANY®, A ONEAMERICA® COMPANY
© 2013 OneAmerica Financial Partners, Inc. All rights reserved.
R-20447 12/24/13
Q: What options are available when I terminate employment or retire?A: When you terminate employment or retire, depending on your account balance, you may keep your money in the plan, transfer or roll it over to another eligible retirement plan or Individual Retirement Account (IRA), receive the money in a lump sum or select annuity payments (if allowed by your plan).
Q: Can I roll over money from an existing IRA or retirement account into my 403(b) account?A: Regulations regarding rollovers may limit the ability to roll assets from one plan to another. However, tax law changes have made consolidating retirement assets easier than ever. Please check with your employer or call 1-800-249-6269 for more information.
Q: How do I obtain information about my account?A: You will receive a personalized account statement each quarter. Additionally, you can check your account online at www.oneamerica.com or by calling 1-800-249-6269. These services provide up-to-date information about your account balance, contributions, investment performance and other account data.
One day you will have a better understanding of your 403(b) plan. One Day is Today!® For more information on 403(b) plans, visit www.oneamerica.com/toolbox.
Note: Registered group variable annuity contracts, issued by AUL are distributed by OneAmerica Securities, Inc., Member FINRA, SIPC, a Registered Investment Advisor, 433 N. Capitol Ave., Indianapolis, IN 46204, 1-877-285-3863, which is a wholly owned subsidiary of American United Life Insurance Company®.
Neither AUL, OneAmerica Securities, Inc. nor their representatives provide tax or legal advice. For answers to your specific questions please consult a qualified attorney or tax advisor.
84

RETIREMENT
101
1 of 2PRODUCTS AND FINANCIAL SERVICES PROVIDED BY AMERICAN UNITED LIFE INSURANCE COMPANY®, A ONEAMERICA® COMPANY
© 2013 OneAmerica Financial Partners, Inc. All rights reserved.
LEARN MORE ABOUT YOUR 457(b) PLAN
R-23701 12/24/13
Q: What is a 457(b) Deferred Compensation Plan (DCP)?A: A 457(b) plan is a retirement plan maintained by a governmental agency or certain non-governmental, tax exempt employers. Contributions are made on a pre-tax basis and accumulate tax-deferred until withdrawn. Upon distribution, withdrawal of both contributions and earnings will be subject to ordinary income tax.
Q: How does a 457(b) DCP work?A: You decide how much of your salary you want to defer and complete a Deferred Compensation Agreement for your employer.
Q: What advantages are there to participating in a 457(b) plan?A: When participating in a 457(b) plan, you can reduce your current income taxes and set aside money for your retirement at the same time. Some people pay taxes on their income first and use what is left over to put money into preparing for retirement. Since federal income taxes are calculated on your income after your retirement plan contribution has been deducted, you may pay less in current federal income taxes. Thus, you may actually have more spendable income than you would if you were contributing a comparable amount to an account where contributions and earnings are subject to current income tax rules.
Q: How much can be contributed to a 457(b) plan?A: For the 2014 calendar year, the regular contribution limit (your contributions plus employer contributions) is $17,500. This amount will be subject to cost of living adjustments (COLAs) in future years. Deferrals to a 457(b) plan are not offset by employee elective deferrals to other retirement plans. Additionally, governmental 457(b) plans may provide for age 50 catch-up contributions and/or special 457(b) catch-up contributions.
Q: What are age 50 catch-up contributions?A: Age 50 catch-up contributions are deferrals over the regular contribution limit that governmental 457(b) plans may allow participants age 50 years and older to make. For 2014, the age 50 catch-up contribution amount is $5,500. Like the regular 457(b) contribution limit, this amount is subject to future cost of living adjustments (COLAs). Check with your plan administrator to see if your plan allows age 50 catch-up contributions.
Questions and answersabout 457(b) plans for governmental organizations
85

2 of 2PRODUCTS AND FINANCIAL SERVICES PROVIDED BY AMERICAN UNITED LIFE INSURANCE COMPANY®, A ONEAMERICA® COMPANY
© 2013 OneAmerica Financial Partners, Inc. All rights reserved.
R-23701 12/24/13
Q: What are special 457(b) catch-up contributions?A: Special 457(b) catch-up contributions are deferrals over the regular contribution limit that 457(b) plan participants may make if they are within three taxable years ending before their normal retirement age (as defined in the plan). Unlike age 50 catch-up contributions, which may be offered only by governmental 457(b) plans, any 457(b) plan may provide for this special catch-up contribution. If the plan allows special 457(b) catch-up contribution, the deferral amount is increased to the lesser of:• Twice the dollar limit or• Sum of current year limit plus unused
portion of prior year limits
The unused limit for a year is the difference between the regular contribution limit in effect for that year and the amount contributed for that year.
Important: If a governmental 457(b) plan allows both special 457(b) catch-up contributions and age 50 catch-up contributions, a participant wishing to make catch-up contributions must make the greater of the two.
Q: Can I roll over my account when I terminate my employment?A: You may roll over your account balance to another eligible retirement plan (for example, an Individual Retirement Account (IRA) or a profit-sharing, 401(k), 403(b), or governmental 457(b) plan).
Q: When can I withdraw my 457(b) deferrals?A: Like other retirement plans, a 457(b) plan is intended to be a long-term investment for your retirement. As a result, a 457(b) plan can permit distributions only in the event of death, severance from employment (termination of employment or retirement at any age), an unforeseeable emergency or attainment of age 70½. Additionally, the plan may allow a one-time withdrawal if your account value is $5,000 or less, there have been no contributions to your account for the two-year period ending on the date of the distribution and no prior withdrawals of this type have been made. Check with your plan administrator for the plan’s distribution rules.Q: How can I change the amount of my deferral?A: You can increase or decrease the amount of compensation you defer according to your employer’s plan specifics. Generally, changes are allowed at least once a year.
Q: Will I pay taxes when I withdraw my 457(b) account?A: All distributions paid to you will be subject to ordinary income tax in the taxable year the distribution is paid from the plan.
Q: Can I roll over money from an existing IRA or my account in another retirement plan into my 457(b) account?A: A 457(b) plan sponsored by a governmental employer may accept rollovers in from an IRA (except Roth IRAs, other after-tax and Coverdale Education Savings Accounts) or another retirement plan. Check with your employer or call 1-800-249-6269 for more information.
Q: How are my 457(b) deferrals invested?A: You may choose from a variety of investment options in the AUL Group Annuity contract.
One day you will have a better understanding of your 457(b) plan. One Day is Today!® For more information on 457(b) plans, visit www.oneamerica.com/toolbox.
Note: Registered group variable annuity contracts, issued by AUL are distributed by OneAmerica Securities, Inc., Member FINRA, SIPC, a Registered Investment Advisor, 433 N. Capitol Ave., Indianapolis, IN 46204, 1-877-285-3863, which is a wholly owned subsidiary of American United Life Insurance Company®.
Neither AUL, OneAmerica Securities, Inc. nor their representatives provide tax or legal advice. For answers to your specific questions please consult a qualified attorney or tax advisor.
86

Department of Finance PO Box 998
Portsmouth, Virginia 23705-0998
Carrier Agents Business Address Phone NumberAmerican Funds Jacques Cureton, PhD, MBA Capital Concepts, LLC 757-456-5344
Managing Director 5741 Cleveland St, Suite 140 fax 757-962-7054Va Beach VA 23462 www.Capital-Concepts.net
American Funds W. Xavier Randall Investors Security 757-499-3959
Financial Advisor 291 Independence Blvd, Pembroke 4 fax 757-493-3599
Suite 420 mobile 757-636-7731
Virginia Beach VA 23462 [email protected]
AXA Equitable Lori Preston - [email protected] 757-461-2210
Leonard Mochi - [email protected] 757-461-2210
Mark Johnson - [email protected] 757-673-5630
First Investors Corporation Katherine Taylor First Investors Corporation 804-346-4670, Ext 315140 East Shore Dr, Ste 105 (800) 486-4670, Ext 315Glen Allen VA 23059 Fax 804-270-2549
www.firstinvestors.com
First Investors Corporation Corey Creech First Investors Corporation 804-346-4670, Ext 308140 East Shore Dr, Ste 105 (800) 486-4670, Ext 308Glen Allen VA 23059 Fax (804) 270-2549
Great American Financial Resources Leon Fitzgerald The Insurance Network 757-486-1061
Regional Marketing Director 905 Larkhaven Lane cell 757-735-7731Virginia Beach VA 23452
Lincoln Financial Group William F. Sherrill Lincoln Financial Advisors Corp. 757-673-2963Registered Representative PO Box 3228 cell 757-647-5500
Portsmouth VA 23701 fax [email protected]
Lincoln Financial Group Wardell M. Nottingham, LUTCF Lincoln Financial Advisors Corp. 757-461-7455Investment Advisor Representative 400 North Center Drive, Suite 205 fax 757-461-7454
Norfolk VA 23502 [email protected]
MetLife Resources Vickie Pulley, CLTC Metlife Resources Direct 757-619-5819Financial Services Representative 283 Constituion Dr., Ste. 525 Office 757-687-1325
Virginia Beach, VA 23462 Fax: [email protected]
MetLife Resources Andre Dawkins Metlife Resources 800-560-5001Financial Services Representative
MetLife Resources Kyle R. Arcand MetLife 757-382-4100 ext 4129Financial Services Representative 505 Independence Pkwy, Suite 101 Fax 757-312-8986
Chesapeake, VA 23320 [email protected]
Security Benefit Ed Fissinger Securites America 757-486-4567Financial Advisor Fissinger Investment Services 757-216-3886
412 Becton Place fax 757-216-3887Va Beach VA 23452 [email protected]
Security Benefit Jason Dodzik Security Benefit 757-399-7499355 Crawford Street Suite 802 [email protected], VA 23704
Security Benefit Rich Thiesfeld Brecek & Young Advisors, Inc. 757-430-0249Financial Advisor 412 Becton Place fax 757-216-3887
Va Beach VA 23452
As of August 1, 2014
Tax Sheltered Annuity CompaniesEligible to solicit new enrollments from Portsmouth Public Schools Employees
87

Department of Finance PO Box 998
Portsmouth, Virginia 23705-0998
Carrier Agents Business Address Phone Number
As of August 1, 2014
Tax Sheltered Annuity CompaniesEligible to solicit new enrollments from Portsmouth Public Schools Employees
VALIC A. Dean Anninos, LUTCF VALIC Financial Advisors, Inc. 800-892-5558 ext 88459Investment Advisor Rep 10800 Midlothian Turnpike, Suite 200 cell 757-759-7795
Richmond VA 23235 fax 804-897-5512 [email protected]
VALIC.com
VALIC Raleigh Martin VALIC Financial Advisors, Inc. 757-398-4690Financial Advisor 3636 High Street 800-892-5558 ext 88926
Portsmouth VA 23707 cell [email protected]
VALIC.com
88

Portsmouth Public Schools January 1 2015 thru December 31, 2015
RATES
After Tax SHORT TERM DISABILITY INSURANCE Underwritten by…Humana Insurance Company
See account manager for 20 pay rates, rates are also in booklet with brochure. This product offers enhanced disability benefits unlike most short term disability
products!
After Tax LIFE INSURANCE (PURELIFE)
Underwritten By...Texas Life Insurance Company With Accidental Death Benefit
Age 35 Age 45 Age 55
Insurance Monthly Insurance Monthly Insurance Monthly Coverage Premium Coverage Premium Coverage Premium
$25,000 $13.75 $25,000 $26.00 $15,000 $33.90 $50,000 $26.00 $50,000 $50.50 $25,000 $55.50 $100,000 $50.50 $100,000 $99.50 $50,000 $109.50
Examples above based on 12 deductions. *See Account Manager for other ages and 20 pay premiums.
89

Pre-Tax CANCER PLAN
Underwritten by...American Heritage Life Insurance Co. CP10B - 300 20 Deductions W/ Int Care Rider
BASIC Individual 11.38 14.97 Family 19.58 26.77
ENHANCED Individual 15.88 19.48 Family 28.22 35.41
PREMIER Individual 19.41 23.00 Family 35.18 42.38
Pre-Tax HEART & STROKE PLAN
Underwritten By...American Heritage Life Insurance Company 20 Deductions Basic Individual 10.78 Family 20.79 Enhanced Individual 18.94 Family 37.11 Premier Individual 20.26 Family 39.75
Pre-Tax ACCIDENT PLAN Underwritten By...American Fidelity Assurance Company
Basic Plan Enhanced Plan 20 Deductions 20 Deductions Individual 11.94 15.66 Individual & Spouse 16.98 20.94 Single Parent Family 18.90 24.60 Family Plan 23.94 29.88
90

Critical Illness by Aflac
Please see rates with brochure in book. Pre Tax
Vision Insurance Underwritten by Ameritas/VSP
20 pay premiums Individual $5.82 Family $14.26
Life Insurance Underwritten by Texas Life
See brochure in booklet for age and rates
Whole Life with Facilities Benefit
Underwritten by Humana
Please see rates in booklet and discuss with account manager for 20 pay rates.
Retirement Options by AUL…American United Life
403(b) and 457 Deferred Compensation Plans available
Please discuss with Account Managers 91

PRODUCT REFERENCE MATERIAL Plan Year: January 1, 2015 thru December 31, 2015
For claim forms and information:
Flex Accounts
Claim Numbers: 75058
First Financial Administrators, Inc. 800.523.8422
www.ffga.com
Humana Short Term Disability 877-378-1505
www.humana.com
Permanent Life Insurance Texas Life Insurance Co.
800.283.9233 www.texaslife.com
Cancer Insurance
Allstate Workforce Division 800.521.3535
https://www.ahlcorp.com/ClaimForms.aspx
Heart/Stroke Insurance Allstate Workforce Division
800.521.3535 https://www.ahlcorp.com/ClaimForms.aspx
Accident Only Insurance Plan American Fidelity Assurance Co
800.323.3748 http://www.afadvantage.com/customerservice-forms.asp#claim
92

AFLAC Critical Illness
Hospital Indemnity 800.433.3036
http://www.aflacgroupinsurance.com
First Financial Group of America Retirement Services Department: 800.523.8422 Retirement Services Fax number: 281.847.8427
First Financial Group of America Customer Service Representative:
Yvette Ulisnik 800.924.3539
FOR CUSTOMER SERVICE PLEASE CALL:
First Financial Group of America 3904 Oleander Drive, Suite 200
Wilmington NC 28403 800.924.3539
www.ffga.com
93




Section 125 Services Provided By:
First Financial Group of America
5Post Office Box 670329
Houston, Texas 77267-0329
800-523-8422
Section 125 Third Party Administrator:
First Financial Administrators, Inc.
3904 Oleander Dr., Suite 200
Wilmington NC, 28403
(800) 924-3539
www.ffga.com
Account Manager EScotti Sammons