Embed Size (px)
Citation preview

James J. Ferguson, MD
James J. Ferguson, MD
The Evolving Standard of Care for Acute Coronary
Syndromes2006

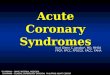
TIMI 8
BAT
GUSTO IIA
OASIS Pilot
TIMI 7
CURE
CAPRIE
CREDO
ISAR-REACT
EPICEPILOG
CAPTURE
TARGET
GUSTO IVRESTORE
IMPACT 2
ESPRIT
ACE
ISAR-SWEET
EPISTENT
PURSUIT
PRISM PRISM-PLUS
REPLACE 2
OASIS 2
GUSTO IIB
HELVETICA
FRISC
FRIC
RITA 3
A to Z
INTERACT
SYNERGY
CADILLAC
TACTICS
ESSENCE
FRAXIS
FRISC 2
FRISC 2ACUTE 2
TIMI 11B
PROTECT
How do we sort out this mess ?
The Evolving Standard of Care for Acute Coronary
Syndromes2006

Evolutionary
perspectives
Evolving physiology
Evolving data
Evolving messages
Putting it together
The Evolving Standard of Care for Acute Coronary
Syndromes2006

Evolutionary
perspectives
Evolving physiology
Evolving data
Evolving messages
Putting it together
The Evolving Standard of Care for Acute Coronary
Syndromes2006

Geological Time Scale

ACS Time Scale
Reduce demand
Treat the thrombus
Harmonize therapies
Open the vessel
Antithrombotic EpochAntithrombotic Epoch
Interventional Epoch
Interventional Epoch
Synergistic EpochSynergistic Epoch
Palliative EpochPalliative Epoch
Mechanistic Epoch
Mechanistic Epoch
Understand the biology

Evolutionary
perspectives
Evolving physiology
Evolving data
Evolving messages
Putting it together
The Evolving Standard of Care for Acute Coronary
Syndromes2006

DETERMINANTS OFRupture
ThrombosisHealing
Fibrous tissueAtheromatous material(lipid-rich)
Thrombus
Plaque hemorrhageMacrophageSmooth muscle cell
Luminal factors
Extra-luminal factors
Systemic factors
Luminal factors
Extra-luminal factors
Systemic factors
UNSTABLE PLAQUE
STABLE PLAQUE
MYOCARDIAL INFARCTION
Inflammation and repair
Core size
Capthickness
“Vulnerable” Plaque and
Acute Coronary Syndromes

Rupture
Thrombosis
Occlusion
Reduce thrombus burden
Limit thrombus progression
Promote healing / homeostasis
Open the occluded vessel
Limit the extent of the damage
Rx UA
Rx MI

ProthrombinProthrombin
Thrombin
FibrinogenFibrinogen
Fibrin Fibrin monomermonomer
Tissue FactorTissue Factor
VIIaVIIa
VIIVII
VIIa/TFVIIa/TF
IXIX IXaIXa
XX
XaXa
Fibrin Fibrin polymerpolymer
Crosslinked Fibrin
VV
VaVa
VIIIVIII
VIIIaVIIIaXIXI XIaXIa
XIIXII XIIaXIIa
PK, PK, HKHK
HKHK
XIIIXIII XIIIaXIIIa
CaCa++ ++
PLPLCaCa++ ++
PLPL
Coagulation

Question:
What do we really need to know about coagulation?
Answer:
How to treat it when it happens.
How to prevent it in the first place.
Question:
What do we really need to know about coagulation?
Answer:
How to treat it when it happens.
How to prevent it in the first place.
Coagulation

Platelet Activation
Thrombus
Injury
Platelet Aggregation
Thrombin Generation
Thrombin Activity
Coagulation

Platelet Activation
Thrombus
Injury
Platelet Aggregation
Thrombin Generation
Thrombin Activity
Aspirin
Ticlopidine
Clopidogrel
IIb/IIIa blockers
Heparin
LMW heparin
Xa inhibitors
LMW heparin
Heparin
AntithrombinsFibrinolytic Rx

Evolutionary
perspectives
Evolving physiology
Evolving data
Evolving messages
Putting it together
The Evolving Standard of Care for Acute Coronary
Syndromes2006

1990 1993 1996 1999 2002 2005
AbciximabEptifibatide
Tirofiban
P-S stent DE stent
Clopidogrel Clopidogrel ACS
Bivalirudin
DesirudinLepirudin
Argatroban
Enox ACS Dalt ACSEnoxaparin Dalteparin
UA / NSTEMI Trials
Thrombin InhibitorsThrombin Inhibitors HELVETICAHELVETICAERAERA
TIMI 8TIMI 8
BAT(original)
BAT(original)
GUSTO IIA GUSTO IIA
REPLACE 2REPLACE 2REDUCEREDUCE OASIS 2 OASIS 2
BAT(revised)
BAT(revised)
OASIS PilotOASIS Pilot
TIMI 7TIMI 7 GUSTO IIB GUSTO IIB
PROTECTPROTECT
LMW HeparinsLMW HeparinsFRICFRIC
ESSENCEESSENCE
FRISCFRISCACUTE 2 ACUTE 2
FRAXISFRAXIS
TIMI 11BTIMI 11B
INTERACT INTERACT
A to Z A to Z
RITA 3 RITA 3
FRISC 2FRISC 2SYNERGYSYNERGY
PROTECTPROTECT
ThienopyridinesThienopyridines ISARISARISAR-REACTISAR-REACT
CURECURECLASSICSCLASSICSCAPRIECAPRIE CREDOCREDO
STARSFANTASTIC
MATTIS
STARSFANTASTIC
MATTIS ISAR-SWEETISAR-SWEET
ARMYDA 2ARMYDA 2
ISAR-REACTISAR-REACTGP IIb/IIIa antagonistsGP IIb/IIIa antagonists EPICEPIC EPILOGEPILOG
EPISTENTEPISTENTCAPTURECAPTURE
TARGETTARGET CADILLACCADILLAC
GUSTO IVGUSTO IV
RESTORERESTORE
PRISMPRISMTACTICSTACTICSIMPACT 2IMPACT 2
ESPRITESPRITPURSUITPURSUIT
PRISM-PLUSPRISM-PLUS
ISAR-SWEETISAR-SWEET
ACEACE
PROTECTPROTECT
ISAR-COOLISAR-COOL
Interventional IssuesInterventional Issues
RITA 3RITA 3Wallstent restenosisWallstent restenosis
TAXUS IV TAXUS IV TACTICSTACTICS
SIRIUS SIRIUS RAVEL RAVEL FRISC 2FRISC 2STRESS
BENESTENT
STRESS
BENESTENTICTUSICTUS
ISAR-COOLISAR-COOL
ISAR-REACT 2ISAR-REACT 2
CHARISMACHARISMA
ACUITYACUITY
[ OASIS 5 ][ OASIS 5 ]

Medical Rx
No Cath
Cath PCI
Surgery
Medical Rx
Delayed surgery
Medical Rx
No disease
Delayed PCI
Time
Admission Cath PCI DischargeSurgery
UA/NSTEMI Management

Medical Rx
No Cath
Cath PCI
Surgery
Medical Rx
Delayed surgery
Medical Rx
No disease
Delayed PCI
Time
Admission Cath PCI DischargeSurgery
Patient X
UA/NSTEMI Management

Medical Rx
No Cath
Cath PCI
Surgery
Medical Rx
Delayed surgery
Medical Rx
No disease
Delayed PCI
Time
Admission Cath PCI DischargeSurgery
(82 %)
(18 %)
(52 %)
40 % < 48 hrs
12 % > 48 hrs
(12 %)
63 % < 48 hrs
19 % > 48 hrs
CRUSADERegistry
10/05-9/05n=35,897
Medical Rx
Patient X
UA/NSTEMI Management

ISAR - COOL
PROTECTCURECURE
ClopidogrelClopidogrel
Invasive StrategyInvasive Strategy LMW HeparinLMW Heparin
IIb/IIIa antagonistsIIb/IIIa antagonists
FRISC II
TACTICS / TIMI 18
RITA 3
ICTUS
FRISC II
TACTICS / TIMI 18
RITA 3
ICTUS
Important DataImportant Data UA / NSTEMI
INTERACT
A to Z
SYNERGY
INTERACT
A to Z
SYNERGY

OASIS 5
ISAR-REACT 2
ACUITY
ICTUS
OASIS 5
ISAR-REACT 2
ACUITY
ICTUS
Very Recent Data
Very Recent Data
UA / NSTEMI

OASIS 5OASIS 5 OASIS 5 InvestigatorsN Engl J Med. 2006;354: 1464-76
Patients w/ NSTE ACS
Chest pain < 24 hours2/3:
Age > 60ST-segment ∆
↑ cardiac markers
ASA, clopidogrel, IIb/IIIa, planned cath
per local practice
ExcludeAge < 21
Contraindication to enoxHemorrhagic stroke < 12
moCreat > 3 mg/dL (265
umol/L) Randomize
n = 20,000
Fondaparinux2.5 mg sc qd
Enoxaparin 1 mg/kg sc bid
PCI < 6 h: IV fondaparinux 2.5 mg w/o IIb/IIIa, 0 w/
IIb/IIIaPCI > 6h: IV fondaparinux 5 mg w/o IIb/IIIa, 2.5 mg w/
IIb/IIIa Primary Efficacy Death, MI, refractory ischemia at 9 days
Safety Major bleeding at 9 daysRisk/benefit Death, MI, refractory ischemia and major
bleeding at 9 days Secondary Above and each component separately at day 30 and 6 months Hypothesis: First test non-inferiority, then test superiority
PCI < 6 h: no UFHPCI > 6h: IV UFH
100 U/kg w/o IIb/IIIa60 U/kg w/ IIb/IIIa
Outcomes

OASIS 5OASIS 5 OASIS 5 InvestigatorsN Engl J Med. 2006;354: 1464-76
In-hospital procedures at 9 Days
Cath Lab No Cath Lab
Centers (n) 420 (73%) 156 (27%)
Patients (n) 14,028 (70%) 6050 (30%)
Angiography 73.2% 27.7%
PCI 39.6% 12.5%
CABG 6.8% 1.8%
Revascularization 46.1% 14.1%
Mean duration of therapy: Enoxaparin 5.2 + 2.3 days Fondaparinux 5.4 + 2.4 days

OASIS 5OASIS 5 OASIS 5 InvestigatorsN Engl J Med. 2006;354: 1464-76

OASIS 5OASIS 5 OASIS 5 InvestigatorsN Engl J Med. 2006;354: 1464-76

Abciximab(n=1,012)
Abciximab(n=1,012)
Placebo(n=1,010)Placebo(n=1,010)
Endpoints:Primary Endpoint: Composite of death, MI, and urgent TVR due to myocardial
ischemia within 30 daysSecondary Endpoint: In-hospital major and minor bleeding
Endpoints:Primary Endpoint: Composite of death, MI, and urgent TVR due to myocardial
ischemia within 30 daysSecondary Endpoint: In-hospital major and minor bleeding
ISAR-REACT 2: Trial Design
Clopidogrel(Pre-treatment high-dose 600 mg loading dose for at least 2 hour pre-procedure, 2 x 75
mg/d through discharge, 75 mg/d for 4 weeks)
Clopidogrel(Pre-treatment high-dose 600 mg loading dose for at least 2 hour pre-procedure, 2 x 75
mg/d through discharge, 75 mg/d for 4 weeks)
↑ troponin T or new ST ↓Transient (<20 min) ST ↑ of > 0.1 mVNew BBB
↑ troponin T or new ST ↓Transient (<20 min) ST ↑ of > 0.1 mVNew BBB
Significant lesion in native vessel or bypass graftAmenable to and requiring PCI
Significant lesion in native vessel or bypass graftAmenable to and requiring PCI
2,022 patients with ACS and new angina episode within past 48 hours
Kastrati A, et al. JAMA. 2006; 295: 1531-8

ISAR-REACT 2: Primary EndpointPrimary Endpoint
Death, MI, or urgent TVR in 30 daysPrimary EndpointBy Troponin Status
p = .02 p = .98p = .03
Kastrati A, et al. JAMA. 2006; 295: 1531-8

ISAR-REACT 2: Bleeding
•There was no difference between the abciximab and placebo groups in in-hospital major and minor bleeding (p=NS for both).
•There was one intracranial bleed in each group.
•2.5% of patients received transfusions in the abciximab group compared with 2.0% in the placebo group (RR 1.25)
In-hospital Major and Minor Bleeding (%)P=NS
Kastrati A, et al. JAMA. 2006; 295: 1531-8

Moderate-high risk
ACS
ACUITY
An
gio
gra
ph
y w
ith
in 7
2h
Moderate-high risk unstable angina or NSTEMI undergoing an invasive strategy (N=13,800)
Medicalmanagement
PCI
CABG
Endpoints: Death, MI, and unplanned revascularization for ischemia (30 days and 1 year); major bleeding (30-days); composite of the above (30-days)
Stone G. American College of Cardiology 2006 Scientific Sessions; March 12, 2006; Atlanta, GA.
ASA in allclopidogrel
dosing and timingper local practice
UFH orEnoxaparin+ GP IIb/IIIa
Bivalirudin+ GP IIb/IIIa
BivalirudinAlone
R

Moderate-high risk
ACS
ACUITY
An
gio
gra
ph
y w
ith
in 7
2h
Moderate-high risk unstable angina or NSTEMI undergoing an invasive strategy (N=13,800)
Medicalmanagement
PCI
CABG
Endpoints: Death, MI, and unplanned revascularization for ischemia (30 days and 1 year); major bleeding (30-days); composite of the above (30-days)
Stone G. American College of Cardiology 2006 Scientific Sessions; March 12, 2006; Atlanta, GA.
ASA in allclopidogrel
dosing and timingper local practice
UFH orEnoxaparin+ GP IIb/IIIa
Bivalirudin+ GP IIb/IIIa
BivalirudinAlone
R
Ischemic Composite
BleedingNet Clinical Outcome
7.3 % 5.7 % 11.7 %
7.7 % 5.3 % 11.8 %
7.8 % 3.0 % 10.1 %

Moderate-high risk
ACS(n=13,819)
ACUITY Second Randomization – GP IIb/IIIa Inhibitor Timing
Moderate-high risk unstable angina or NSTEMI undergoing an invasive strategy (N=13,819)
Aspirin in allClopidogrel
dosing and timingper local practice
BivalirudinAlone
(n=4,612)
UFH or Enoxaparin
Bivalirudin
Routine upstream GPI in all pts
GPI started in CCL for PCI only
UF
H, E
no
xa
pa
rin,
or B
ivaliru
din
Routine upstreamGPI in all pts
(4,605)
Deferred GPIfor PCI only
(n=4,602)
VS
Endpoints: Death, MI, and unplanned revascularization for ischemia (30 days and 1 year); major bleeding (30-days); composite of the above (30-days)
Routine upstream GPI in all pts
GPI started in CCL for PCI only
Stone G. American College of Cardiology 2006 Scientific Sessions; March 12, 2006; Atlanta, GA.
R
R
BivalirudinAlone
(n=4,612)

Moderate-high risk
ACS(n=13,819)
ACUITY Second Randomization – GP IIb/IIIa Inhibitor Timing
Moderate-high risk unstable angina or NSTEMI undergoing an invasive strategy (N=13,819)
Aspirin in allClopidogrel
dosing and timingper local practice
BivalirudinAlone
(n=4,612)
UFH or Enoxaparin
Bivalirudin
Routine upstream GPI in all pts
GPI started in CCL for PCI only
UF
H, E
no
xa
pa
rin,
or B
ivaliru
din
Routine upstreamGPI in all pts
(4,605)
Deferred GPIfor PCI only
(n=4,602)
VS
Endpoints: Death, MI, and unplanned revascularization for ischemia (30 days and 1 year); major bleeding (30-days); composite of the above (30-days)
Routine upstream GPI in all pts
GPI started in CCL for PCI only
Stone G. American College of Cardiology 2006 Scientific Sessions; March 12, 2006; Atlanta, GA.
R
R
Ischemic Composite
BleedingNet Clinical Outcome
7.1 % 6.1 % 11.7
7.9 % 4.9 % 11.7 %
7.8 % 3.0 % 10.1 %Bivalirudin
Alone(n=4,612)

Mehta SR, et al. JAMA. 2005;293:2908-2917.
Routine vs Selective Invasive StrategyRoutine vs Selective Invasive Strategy:Summary of Odds Ratios for All Major OutcomesSummary of Odds Ratios for All Major Outcomes
No./Total (%)
Outcome Routine Selective Odds Ratio (95% CI) P Value
Randomization to Hospital Discharge
Death 82/4608 (1.8) 51/4604 (1.1) 1.60 (1.14 – 2.25) .007
Nonfatal MI 171/4608 (3.7) 139/4604 (3.0) 1.24 (0.99 – 1.56) .07
Death or MI 238/4608 (5.2) 177/4604 (3.8) 1.36 (1.12 – 1.66) .002
After Hospital Discharge to End of Follow-up
Death 172/4526 (3.8) 223/4552 (4.9) 0.76 (0.62 – 0.94) .01
Nonfatal MI 164/4370 (3.8) 294/4430 (6.6) 0.56 (0.46 – 0.67) <.001
Death or MI 323/4370 (7.4) 486/4430 (11.0) 0.64 (0.56 – 0.75) <.001
Randomization to End of Follow-up
Death 254/4608 (5.5) 274/4604 (6.0) 0.92 (0.77 – 1.09) .33
Nonfatal MI 335/4608 (7.3) 433/4604 (9.4) 0.75 (0.65 – 0.88) <.001
Death or MI 561/4608 (12.2) 663/4604 (14.4) 0.82 (0.72 – 0.93) .001

Routine vs Selective Invasive Strategies in ACS
Adapted from Mehta S, et al. JAMA. 2005;293;2908-2917.
Composite of Death or Myocardial InfarctionNo./Total (%)
Source Routine Invasive
Selective Invasive
TIMI IIIB 86/740 (11.6) 101/733 (13.8)
VANQWISH 152/462 (32.9) 139/458 (30.3)
MATE 16/111 (14.4) 11/90 (12.2)
FRISC II 127/1222 (10.4) 174/1235 (14.1)
TACTICS 81/1114 (7.3) 105/1106 (9.5)
VINO 4/64 (6.3) 15/67 (22.4)
RITA 3 95/895 (10.6) 118/915 (12.9)
Total 561/4608 (12.2) 663/4604 (14.4)
0.1 1.0 10
Odds Ratio (95% CI)
FavorsRoutineInvasive
FavorsSelectiveInvasive
OR - 0.8295% CI, 0.72-0.93
P < 0.001

ICTUS N Engl J Med 2005; 353: 1095-1104
•1200 ACS patients•Presenting within 1 day of onset of chest pain•42 Dutch hospitals (12 were high-volume PCI centers)•↑ Troponin T (≥ 0.03 μg/L)•Either ECG evidence of ischemia or documented Hx CAD•Randomized
Early invasive (n=604) Angio within 24-48 hours PCI within 48 hours, CABG as soon as possibleSelective invasive (n=596) Angio for refractory angina, provocable
ischemia
Primary Endpoint:
Death / MI / rehospitalization at 1 year

Early Invasive
Selective Invasive
Death 2.2 % 2.0 %
MI 14.6 % 9.4 %
Rehospitalization
7.0 % 10.9 %
Total 21.7 % 20.4 %
ICTUS N Engl J Med 2005; 353: 1095-1104

22 .7 %
21.2 %
[ RR 1.07, 95 % CI 0.87 - 1.33; p=0.33 ]
ICTUS N Engl J Med 2005; 353: 1095-1104

Median time to PCI23 hours (25th to 75th percentile, 15 to 44) with early invasive Rx283 hours (25th to 75th percentile, 142 to 647) with selective invasive Rx
ICTUS N Engl J Med 2005; 353: 1095-1104

All-Cause Mortality
Bavry et al. J Am Coll Cardiol 2006; 48: 1319-25
Even after ICTUS ...Even after ICTUS ...

All-cause mortality as a function of time of angio and extent of revascularization
Bavry et al. J Am Coll Cardiol 2006; 48: 1319-25
Even after ICTUS ...Even after ICTUS ...

Optimize supply / demand Optimize supply / demand
AcuteAcute
Treat underlying atherosclerosis
Prevent recurrent events
Stabilize the plaques
Enhance endothelial function
Chronic anti-thrombotic Rx
Treat underlying atherosclerosis
Prevent recurrent events
Stabilize the plaques
Enhance endothelial function
Chronic anti-thrombotic Rx
Long - termLong - termStatins
ASA
Clopidogrel
ASA / Clopidogrel
Warfarin
Risk factor ↓
Other things not to forgetOther things not to forget
BP control
Glucose control
Smoking cessation
ACE inhibitors
And don’t
forget . . .
O2Nitrates
β-blockers

Evolutionary
perspectives
Evolving physiology
Evolving data
Evolving messages
Putting it together
The Evolving Standard of Care for Acute Coronary
Syndromes2006

Lessons LearnedLessons Learned
Invasive is better than conservative in high and medium risk patientsFRISC II
TACTICS / TIMI 18RITA 3?? ICTUS ??
UA / NSTEMIUA / NSTEMI

Lessons LearnedLessons Learned
Invasive is better than conservative in high and medium risk patientsAntiplatelet therapy is important
Clopidogrel is beneficialIIb/IIIa blockers are beneficialEarlier is better in high risk“Standard” is more than ASA
UA / NSTEMIUA / NSTEMI

Lessons LearnedLessons Learned
Invasive is better than conservative in high and medium risk patientsAntiplatelet therapy is important
Antithrombin therapy is importantEnoxaparin - SYNERGY
Bivalirudin - ACUITYFondaparinux - OASIS 5“Standard” moving beyond UFHChallenges of multiple management pathways
UA / NSTEMIUA / NSTEMI

Lessons LearnedLessons Learned
Invasive is better than conservative in high and medium risk patientsAntiplatelet therapy is important
Interaction among agentsInteraction with treatment strategies
Antithrombin therapy is importantHow you put them together is important
UA / NSTEMIUA / NSTEMI

Lessons LearnedLessons Learned
Invasive is better than conservative in high and medium risk patientsAntiplatelet therapy is important
Antithrombin therapy is importantHow you put them together is importantLong term therapy is important
Statins ACE InhibitorsAntiplatelet Rx Antithrombotic Rx
UA / NSTEMIUA / NSTEMI

Evolutionary
perspectives
Evolving physiology
Evolving data
Evolving messages
Putting it together
The Evolving Standard of Care for Acute Coronary
Syndromes2006



ASA
IIb/IIIa antagonists
1995 1998
EPISTENT
PURSUIT
2001
ESPRIT
GUSTO 4
2004
ISAR REACT
Clopidogrel CURE
2000
Anti-platelet agents
2006
1997 1999
UFH
LMWH TIMI 11B
2004
SYNERGY
Bivalirudin
2003
REPLACE 2
2001
Anti-thrombotic agents
2006
1992 1995 1998 2001 2004 2007
ISAR REACT 2
Fondaparinux
ACUITY
ACUITY
ACUITY
? ? ?OASIS 5
Our Evolving Anticoagulant Armamentarium

The predictive value of a diagnostic test
is a function not only of sensitivity and specificity,
but also the prevalence of the disease
in the population being tested.
The predictive value of a diagnostic test
is a function not only of sensitivity and specificity,
but also the prevalence of the disease
in the population being tested.
Bayes’ Theorem

Stuff you do works best
in people who really need it.
Stuff you do works best
in people who really need it.
Bubba’s Theorem

AgeAge
(+) Biomarkers(+) Biomarkers
(+) ST-segment (+) ST-segment ΔΔss
DiabetesDiabetes
Refractory symptomsRefractory symptoms
Acute Risk StratifiersAcute Risk Stratifiers
Extent of damageExtent of damageEF, CK, CKMB,
troponinEF, CK, CKMB,
troponin
Extent of homeostatic derangement
Extent of homeostatic derangement
CRP, CD40L, BNP, IL-6, Fibrinogen, P-selectin
CRP, CD40L, BNP, IL-6, Fibrinogen, P-selectin
Extent of diseaseExtent of diseaseEF, DMEF, DM

Evolutionary
perspectives
Evolving physiology
Evolving data
Evolving messages
Putting it together
The Evolving Standard of Care for Acute Coronary
Syndromes2006

Evolutionary
perspectives
Evolving physiology
Evolving data
Evolving messages
Putting it together
Therapeutic epochsBuilding on what has gone
beforeChanging itAdding to it

Evolutionary
perspectives
Evolving physiology
Evolving data
Evolving messages
Putting it together
Plaque ruptureHomeostatic forcesDynamic balance
Multiple interlocking mechanisms

Evolutionary
perspectives
Evolving physiology
Evolving data
Evolving messages
Putting it together
OASIS 5, ISAR-REACT 2, ACUITYICTUS
Stay tuned ... more to come

Evolutionary
perspectives
Evolving physiology
Evolving data
Evolving messages
Putting it together
Open vesselsKeep them open
Adjunctive therapy importantPerfusion rather than
patency

Evolutionary
perspectives
Evolving physiology
Evolving data
Evolving messages
Putting it together
Look at the big pictureEvaluate the data yourself
Risk stratification is keyDon’t just do ... think