Embed Size (px)
Citation preview

Jacki S. Witt, JD, MSN, WHNP-BCUniversity of Missouri – Kansas City
Project Director, Title X Clinical Training Center for Family Planning

What is RLP?
Why should we integrate RLP into clinical practice?
How can we make RLP meaningful to individuals and the community?
What barriers do the men & women in our clinic/community face when making RLPs?

Planning for pregnancy – or not
Access to health care services for prevention/health promotion, preconception planning & contraception
Case finding of women with previous adverse pregnancy outcomes to reduce risk for future adverse outcomes
Dialogue between health care staff & women/couples

A set of interventions that aim to identify & modify biomedical, behavioral, & social risks to a woman's health or pregnancy outcome through prevention & management
It is more than a single visit & less than complete well-woman care
It includes care before a first pregnancy or between pregnancies (interconception care)
4

Early Prenatal Care is Not
Enough
Why RLP?

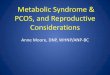
Critical Periods of DevelopmentCritical Periods of Development
4 5 6 7 8 9 10 11 12Weeks gestation from LMP
Central Nervous SystemCentral Nervous System
HeartHeart
ArmsArms
EyesEyes
LegsLegs
TeethTeeth
PalatePalate
External genitaliaExternal genitalia
EarEar
Missed Period Mean Entry into Prenatal Care
Most susceptible time for major malformation

The heart begins to beat at 22 days after conception
The neural tube closes by 28 days after conception
The palate fuses at 56 days after conception Critical period of teratogenesis – Day 17 to
Day 56
7

I don’t believe indoing anythingto stop fromhaving children
It wasn’t my fertile time
My d
octo
r said
I cou
ldn
’t get p
reg
nan
t
We
had
use
d
con
do
ms
exce
pt
on
e ti
me!
I was using birth control pills !
My b
oyfrien
d
do
esn’t
like usin
g
con
do
ms
I thought if it’s God’s will, I would get pregnant

Unintended: occur earlier than desired,
29%
Intended, 51%
Unintended: occur after
women have reached their desired family
size,20%
Approximately 6.4 million pregnancies per year

Improve the health of each woman prior to conception by identifying risk factors
Provide education Stabilize medical condition(s) to optimize maternal
and fetal outcomes
The process should be ongoing
“Every woman – every time”
Finer,2006

Improving Preconception Health & Pregnancy Outcomes
All women & men of childbearing age
have high reproductive awareness (i.e., understand risk & protective factors related to childbearing).
All women have a reproductive life plan
(e.g., whether or when they wish to have children, & how they will maintain their reproductive health).

All pregnancies are intended & planned.
All women & men of childbearing
age have health coverage. All women of childbearing age are
screened before pregnancy for risks related to the outcomes of pregnancy.

Four Goals:1. Improve the knowledge, attitudes,
& behaviors of men & women related to preconception health
2. Assure that all women of child-bearing age in the U. S. receive preconception care services

Four Goals (continued):3. Reduce risks indicated by a previous
adverse pregnancy outcome through interventions during the interconception period, which can prevent or minimize health problems for a mother or her future children
4. Reduce the disparities in adverse pregnancy outcomes

Action StepsResearch – Surveillance – Clinical
interventionsFinancing – Marketing – Education and
training
RecommendationsIndividual Responsibility - Service Provision
Access – Quality – Information – Quality Assurance
GoalsCoverage – Risk Reduction
Empowerment – Disparity Reduction
Vision Improve health and pregnancy
outcomes

U.S. maternal & infant mortality is higher than in many countries
Despite more women receiving early prenatal care rates of preterm birth & low birth weight are increasing in U.S.

United States, Table 1: Health 2008
7.26.9
6.46.3
6.2
5.45.2
5.155
4.94.7
4.64.4
4.24.2
4.14
3.93.8
3.73.6
3.53.4
3.13
2.82.42.4
2.1
6.2
0 1 2 3 4 5 6 7 8
SlovakiaUnited States
PolandN. Ireland
CubaHungaryCanada
ScotlandNew Zealand
AustraliaEngland
NetherlandsItaly
IsraelDenmark
AustriaSwitzerland
SpainIreland
GermanyGreece
BelgiumFrance
PortugalCzech Republic
NorwayFinland
JapanHong Kong
SwedenSingapore IMR: Deaths per 1,000 live
births

2 National Center for Health Statistics, 2010
All Races………………………………….…….White ..……………………………………..…..Black …………………………………………….Native American ……………………………Asian …………………………………………….Hispanic ………………………………………… Mexican …..………………………………… Puerto Rican …………………………….… Cuban ……………………………………….. Central and South American ………….
1995
7.66.3
14.69.05.36.36.08.95.35.5
2005
6.95.713.6
8.14.95.65.58.34.44.7

Delays in initiating prenatal care
Reduced likelihood of breastfeeding
Poor maternal mental health
Lower mother-child relationship quality
Increased risk of physical violence during pregnancy

Pieces of the puzzle: Education Health Vocation/career Relationships/family Reproductive life plans
Set against backdrop of culture, society, religion,
economic status

Encourage young people to develop a “RLP” by asking themselves questions:
Do I want children and if so, how many and when?
How will I feel if I cannot have children?

How will I feel if I have an unwanted pregnancy?
How do I feel about abortion?
What do I most want to accomplish in life?
How much education do I want?
How compatible are my reproductive plans with my religious and moral beliefs?
Hatcher, 1980

Is there scientific data to
support it?

Rubella vaccination HIV/AIDS screening Management and
control of: Diabetes Hypothyroidism PKU Obesity
Folic Acid supplements
Avoiding teratogens: Smoking Alcohol Oral anticoagulants Isotretinoin




Priority # 4: “Emphasizing the importance of
counseling family planning clients on
establishing a reproductive life plan, and
providing preconception counselingas a
part of family planning services, as appropriate”

Guidelines
Best Practice = Reproductive Life Plan for Everyone

▪ Most clinicians don’t provide it
▪ Most insurers don’t pay for it
▪ Most consumers don’t ask for it
Preconception care is not being consistently delivered today

Funding Staff buy in Patient buy in Time Competing priorities Need to know best strategies for your
population

Consider your population/community
Statistics: unplanned pregnancy rates, infant & maternal morbidity & mortality
Cultural preferences related to health care, pregnancy, social challenges
Health care access

Consider your setting’s characteristics
Who counsels women?
Your best educational methods?
Social and mental health services?
Coverage for contraceptives?

RLP is patient-centered
Makes no assumptions (not all want to contracept)
Dynamic: plans & goals can & do change, sometimes from visit to visit

Plans about having children are simple for no one, ambivalence is common
RLPs are NEVER right or wrong*
Reproductive life planning should be offered to everyone, irrespective of assumptions about an individual’s circumstances*

Can increase perceived control of [reproductive] future
Reframes conception Chance Choice
Challenges us to make the FP interaction [more?] patient-centered
Encourages use of behavioral change model for counseling
Could decrease unintended pregnancies, short interconceptional periods & poor pregnancy outcomes
Could increase women’s wellness in reproductive years & beyond

Social marketing & health promotion for consumers [state and national]
Clinical practice [individuals and couples]
Public health and community [collaborations]
Public policy and finance [state by state]
Data and research [all levels]


Current RLP services in your setting?
RLP tools you need?
Most effective ways to train staff?
Strategies to maximize implementation

Collaboration is essential to provide a comprehensive approach. Examples of organizations:
Other Clinics & Doctor's Offices Faith Based Organizations Community Based Organizations WIC and social services sites Hospital Based Organizations Businesses (nail salons, hair salons, others)

Do you hope to have any (or any more) children?
If no, how will you prevent having more pregnancies?
If yes, how many more children do you want, how would you like to space them, how do you plan to keep from getting pregnant until you are ready for the next child?
How can I help you achieve your plan?

Patient-centered Empowering Invites goal setting and action steps Tested with target population Short Culturally-sensitive, respectful tone If self-administered then appropriate for
health and general literacy Makes no assumptions

Folic Acid Supplements: Reduce the occurrence of neural tube defects by two thirds
Rubella testing &/or immunization: Rubella immunization provides protective sero-positivity & prevents the occurrence of congenital rubella syndrome
HIV/AIDS: timely antiretroviral treatment can be administered, pregnancies can be better planned
Hepatitis B: Vaccination is recommended for men & women who are at risk for acquiring hepatitis B virus (HBV) infection.

Pertussis: very contagious & can cause serious illness―especially in newborns. Teen & adult vaccination is important, especially for families with (or planning) newborns.
Diabetes: 3-fold increase in birth defects among infants of women with type 1 & type 2 diabetes, without management
Hypothyroidism: Dosage of levothyroxine should be adjusted in early pregnancy to maintain levels needed for fetal neurological development

Maternal PKU: Low phenylalanine diet before conception & throughout pregnancy may prevent mental retardation in infants born to mothers with PKU
Obesity: Associated adverse outcomes include neural tube defects, preterm birth, c-section, hypertensive & thromboembolic disease
STDs: have been strongly associated with ectopic pregnancy, infertility, & chronic pelvic pain

Alcohol: Fetal alcohol syndrome (FAS) and other alcohol-related birth defects can be prevented.
Anti-seizure drugs: Some anti-seizure drugs are known teratogens
Isotretinoin : Use of isotretinoin in pregnancy results in miscarriage & birth defects
Oral anticoagulants: Warfarin is a teratogen; medications can be switched before the onset of pregnancy
Smoking: Associated adverse outcomes include preterm birth, low birth weight.

Exercise: 30 minutes Vitamin: 400 mcg folic
acid Educate yourself:
medicines/toxins that can cause birth defects
RLP Yearly Dr’s visits:
discuss physical & mental wellness
Diet: vegetables, fruits, & whole grains
Avoid tobacco, drugs, & alcohol
Your partner, friends, & family as sources of support
Everywomancalifornia.org

Pregnancy Test Results
STD Test Results
Other?

Could be presented in a way that offends women (or men)
Care offered may not be consistent with plan (provider bias)
Could be interpreted as suggesting who should or should not have children
Can be treated by providers as static (“but last time you said you did not want kids”)
Could be seen as ‘blaming’ a woman or man when their RLP is not carried out as planned

Case Study #1 - Sonya is a 32 year old G6 P0330. Her LNMP was 5 weeks ago. She is at the health care center for a pregnancy test.
What do you want to know about Sonya?

Sonya’s prior pregnancies included: two miscarriages at 19 weeks, one preterm delivery at 26 weeks and one at 24 weeks, both resulting in early
neonatal deaths She had one pregnancy termination at 9
weeks gestation Gynecologic history is significant for
painful mensesFamily history is significant for adult onset
diabetes (F) and hypertension (F & M)Does not use illicit drugs or drink alcoholHas a supportive 30 year old male partner
who is HIV positive and doing very well

What other questions do you have for Sonya ?

Pregnancy intention• Contraception• Age• Health status
▪ Maternal outcome▪ Fetal/newborn outcome
Sonya and partner’s knowledge of her Sonya and partner’s knowledge of her HIV statusHIV status
Safe conceptionSafe conception Medications Use of tobacco?

What can you do for her?

Pregnancy prevention
Pregnancy planning
HIV transmission prevention Health
maintenance/ support
Referrals
Screening
Substance use
Family history (including
genetic)
Pregnancy history
Folic acid

Case Study #2 – Annie is a 20-year old who presents for emergency contraception after ‘the condom broke’ two days ago.
What do you want to know about Annie?

Never been pregnant Never used prescription birth control
method Sexually active X 3 years New boyfriend X 2 months (3rd partner
in lifetime) BP: 130/88 P: 80 BMI: 35 Significant Family History: Father died
age 48 – complications of diabetes

What other questions do you have for Annie ?

Pregnancy intention• Contraception
Medications? Use of tobacco? Illicit drug use?

What can you do for her?

Pregnancy prevention options
Pregnancy planning
Screening for diabetes
Screening for STDs
Weight loss message
Folic acid

Ad Hoc Committee of PCCHC Select Panel on Reproductive Life Planning, Washington, DC, Nov 23, 2009.
Canady, R.B., Tiedje, L.B. & Lauber, C. (2008). Preconception care and pregnancy planning. American Maternal Child Nursing Journal, 13 (2), 90-97.
CDC Vaccine Information Statement (VIS) (Interim) MMR Vaccine (3/13/08)
CDC Vaccine Information Statement (VIS) (Interim) d & Tdap Vaccines (11/18/08)
Centers for Disease Control and Prevention. Recommendations to improve preconception health and health care - United States: a report of the CDC/ATSDR Preconception Care Work Group and the Select Panel on Preconception Care. Morbidity & Mortality Weekly Report. 2006;55:1-23. Retrieved March 4, 2011 from http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5506a1.htm
Cheng D, Schwarz E, Douglas E, et al. Unintended pregnancy and associated maternal preconception, prenatal and postpartum behaviors. Contraception. 2009 Mar;79(3):194-8.
D’Angelo, D, Colley Gilbert B, Rochat R, et al. Differences between mistimed and unwanted pregnancies among women who have live births. Perspect Sex Reprod Health. 2004 Sep–Oct;36(5):192-7.
Ecologic Model of Health. (Adapted from Healthy People 2020).
Hatcher, R. (1980). Contraceptive Technology Update. 1(9): 131-132.

Hernández Jennings, M. Preconception Health Care: Integrating Reproductive Life Plans into Title X Settings, Colorado Family Planning Initiative Conference, October 23, 2009
Hovell MF, Wahlgren DR, Adams MA. The Logical and Empirical Basis for the Behavioral Ecological Model. In RJ DiClemente, R Crosby, M Kegler, (eds.). Emerging Theories and Models in Health Promotion Practice and Research (2nd edition). San Francisco: Jossey-Bass Publishers; 2009. p. 415-49.
Kendall, C. Afable-Munsuz, A. Speizer, I., Avery, A., Schmidt, N., & Santelli, J. (2005). Understanding pregnancy in a population if inner city women in New Orleans-Results of qualitative research. Social Science and Medicine. 60, 297-311.
Kost K, Landry D, Darroch J. Predicting maternal behaviors during pregnancy: Does intention status matter? Fam Plann Perspect. 1998 Mar–Apr;30(2):79-88.
Logan C, Holcombe E, Manlove J, et al. The consequences of unintended childbearing: A white paper [Internet]. Washington: Child Trends, Inc.; 2007 May [cited 2009 Mar 3]. Available from: http://www.childtrends.org/Files/Child_Trends-2007_05_01_FR_Consequences.pdf

Moos, M-K. Establishing Some Foundations for the RLP Discussion. Presentation at the Office of Population Affair’s Expert Work Group Meeting Implementing Reproductive Life Planning Counseling in Family Planning Clinics. Sep 22-23, 2010.
Moos, MK. (2003). Unintended pregnancies: a call for nursing action. Maternal Child Nursing. 28: 25-31.
National Campaign to Prevent Teen and Unplanned Pregnancy. Unplanned Pregnancy Rate in the U.S. Retrieved March 31, 2011 from http://www.thenationalcampaign.org/national-data/unplanned-pregnancy-birth-rates.aspx