-
Original Article: Clinical Investigationiju_2791 570..575
Mercaptoacetyltriglycine-3 renogram is not superior toestimated
glomerular ltration rate measurement for theprediction of long-term
renal function after nephrectomyHiroshi Kanamaru, Masakazu
Yamamoto, Kanji Nagahama, Yusuke Yagihashi, Keiji Kato,Tomoyuki
Oida, Toru Kannno, Noriyasu Takao, Yusuke Shimizu and Yasumasa
ShichiriDepartment of Urology, Kitano Hospital, Tazuke Kofukai
Medical Research Institute, Osaka, Japan
Objective: To evaluate the clinical usefulness of effective
renal plasma ow (ERPF) measured using
preoperativemercaptoacetyltriglycine-3 (MAG3) renogram for the
prediction of chronic renal insufciency after nephrectomy.Methods:
A total of 47 patients underwent preoperative MAG3 renal
scintigraphy and subsequent unilateral nephrec-tomy. Correlations
between the 5-year postoperative estimated glomerular ltration rate
(eGFR) and the preoperative ERPFof the contralateral kidney
(cERPF), ERPF of the diseased kidney (dERPF), total ERPF (tERPF),
cERPF to dERPF ratio, serumcreatinine (sCr) level, eGFR, as well as
the inuence of preoperative comorbidities (diabetes, hypertension)
on the post-operative eGFR, were evaluated with both univariate and
multivariate analyses.Results: Multiple linear regression analysis
showed that preoperative cERPF signicantly correlated with
postoperativeeGFR. However, a much stronger correlation was
observed between the preoperative and postoperative eGFR.
Multiplelogistic regression analysis showed that only preoperative
eGFR was a signicant predicator of the development ofadvanced-stage
chronic kidney disease (CKD).Conclusions: PreoperativeMAG3 renogram
is not superior to eGFRmeasurement as a prognostic indicator of
long-termrenal function after unilateral nephrectomy.
Key words: chronic kidney disease, mercaptoacetyltriglycine-3
renogram, nephrectomy.
Introduction
Surgical treatments for kidney disease are associated withthe
risk of postoperative chronic kidney disease (CKD).Among renal
surgeries, nephrectomy has the greatest riskfor CKD, because one of
the two renal units is permanentlyremoved.16 Therefore, it is
important to accurately predictlong-term postoperative renal
function before nephrectomy.It is possible to preoperatively assess
differential renalfunction using renal scintigraphy and other
modalities(computed tomography, magnetic resonance imaging).7,8
However, the predictability of such modalities for CKD aftera
long observation period has not been reported. The presentstudy was
carried out to evaluate the clinical usefulness ofeffective renal
plasma flow (ERPF) measured usingmercaptoacetyltriglycine-3 (MAG3)
renogram for the pre-diction of renal function 5 years after
nephrectomy, as com-pared with other clinical parameters.
Methods
Patients
Between 2002 and 2005, 88 patients underwent
unilateralnephrectomy in Kitano Hospital, Osaka, Japan. MAG3
renalscintigraphy was carried out in 74 of the 88 patients
beforesurgery. The present study included 47 out of the 74
patientswho were followed for more than 5 years. The reason
forsurgery was as follows: 25 cases of renal cell carcinoma,
16cases of urothelial cancer, two cases of pyonephrosis, twocases
of angiomyolipoma, one case of urolithiasis and onecase of
oncocytoma. Out of the 37 male and 10 femalepatients, the mean age
was 65 years, with a range of 3882.A preoperative medical history
of diabetes mellitus andhypertension were noted in eight and 20
patients, respec-tively. The present study was approved by the
institutionalethics committee.
MAG3 renogram
After an intravenous injection of 333 MBq of
technetium-99m-mercaptoacetyltriglycine (99mTc-MAG3), a renal
scanwas carried out using a gamma-camera (Forte; ADAC, Mil-pitas,
CA, USA). The MAG3 plasma clearance was calcu-lated based on the
renal uptake of 99m-Tc-MAG3 from 1 to
Correspondence: Hiroshi Kanamaru M.D., Ph.D., Department
ofUrology, Kitano Hospital, Tazuke Kofukai Medical
ResearchInstitute, 2-4-20, Ohgimachi, Kita-ku, Osaka 530-8480,
Japan.Email: [email protected]
Received 15 November 2010; accepted 14 May 2011.Online
publication 12 June 2011
International Journal of Urology (2011) 18, 570574 doi:
10.1111/j.1442-2042.2011.02791.x
570 2011 The Japanese Urological Association
-
2 min postinjection, according to the method described
byOriuchi,9 and effective renal plasma flow (ERPF), whichwas
normalized to a body surface area of 1.73 m2, wasdetermined. The
ERPF from the kidney that would remainafter nephrectomy was
designated the contralateral ERPF(cERPF). The ERPF from the kidney
that would be removedon operation was designated the diseased ERPF
(dERPF).The sum of ERPF from bilateral kidneys was designatedtotal
ERPF (tERPF).
eGFR
Serum creatinine (sCr) was measured before the surgery and5
years later. The eGFR levels were calculated using thefollowing
formula, which was developed by the JapaneseSociety of
Nephrology:10 eGFR = 194 sCr-1.094 age-0.287
(0.739 if female).
Statistics
We used the paired t-test to compare the differences
betweenpreoperative and postoperative renal parameters (sCr
andeGFR). Students t-test was used to compare postoperativeeGFR
between patients with and without preoperativecomorbidities. The
correlations between preoperative renalparameters and postoperative
eGFR were analyzed usingPearsons correlation test. Multiple linear
regression analy-sis was carried out to evaluate the contribution
of preopera-tive renal parameters to predicting postoperative
eGFR.Logistic regression analysis was carried out to evaluate
thepreoperative parameters used to predict advanced-stageCKD
(eGFR
-
Postop eGFR (mL/min/1.73m2)
(a)
Preop cERPF (mL/min/1.73m2)
80
60
40
20
0100 200 300
r = 0.421P = 0.003
400
Postop eGFR (mL/min/1.73m2)
(b)
Preop dERPF (mL/min/1.73m2)
80
60
40
20
01000 200 300
r = 0.515P = 0.0001
400
Postop eGFR (mL/min/1.73m2)
(c)
Preop tERPF (mL/min/1.73m2)
80
60
40
20
0100 200 300
r = 0.566P = 0.0001
600500 800400 700
Postop eGFR (mL/min/1.73m2)
(d)
Preop cERPF to dERPF ratio
80
60
40
20
020 4 6
r = 0.260P = 0.077
8
Postop eGFR (mL/min/1.73m2)
(e)
Preop sCr (mg/dL)
80
60
40
20
00 1
r = 0.672P = 0.0001
2 3
Postop eGFR (mL/min/1.73m2)
(f)
Preop eGFR (mL/min/1.73m2)
80
60
40
20
0200 40 60 80 100
r = 0.798P = 0.0001
120
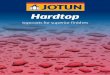
Fig. 1 (a) Correlation between preoperative effective renal
plasma ow (ERPF) of the contralateral kidney (cERPF) and
5-yearpostoperative estimated glomerular ltration rate (eGFR). (b)
Correlation between preoperative ERPF of the diseased kidney
(dERPF)and 5-year postoperative eGFR. (c) Correlation between
preoperative total ERPF (tERPF) and 5-year postoperative eGFR. (d)
Corre-lation between preoperative cERPF to dERPF ratio and 5-year
postoperative eGFR. (e) Correlation between preoperative
serumcreatinine (sCr) and 5-year postoperative eGFR. (f)
Correlation between preoperative eGFR and 5-year postoperative
eGFR.
H KANAMARU ET AL.
572 2011 The Japanese Urological Association
-
There were six patients who developed advanced-stageCKD (eGFR
less than 30 mL/min/1.73 m2) 5 years after theoperation. A multiple
logistic regression analysis includingpreoperative eGFR, cERPF and
hypertension showed thatonly preoperative eGFR was a significant
predictor foradvanced-stage CKD (Table 3).
We divided the patients into two subgroups according tothe
preoperative eGFR using the cut-off value of 60 mL/min/1.73 m2. The
5-year postoperative eGFR remained>30 mL/min/1.73 m2 in all the
patients whose preoperativeeGFR were >60 mL/min/1.73 m2. By
contrast, 5-year post-operative eGFR were less than 30 mL/min/1.73
m2 in 27%(6/22) of the patients whose preoperative eGFR were
-
preoperative function of the resected (diseased) kidney onthe
postoperative compensatory response of the contralat-eral kidney.
Funahashi18 studied the change in renal paren-chymal volume (RPV)
after unilateral nephrectomy andreported that the increase in RPV
of the contralateral kidneywas positively associated with
preoperative DMSA uptakeof the diseased kidney. We therefore
analyzed the impact oftwo diseased kidney-related parameters (cERPF
to dERPFratio and dERPF) on postoperative eGFR. However, cERPFto
dERPF ratio did not show a significant correlation
withpostoperative eGFR. Although dERPF was significantly
cor-related with postoperative eGFR on univariate analysis,
itfailed to be an independent predictor of postoperative eGFRon
multivariate analysis.
The other possible explanation is that RPF is closelyrelated,
but physiologically not equivalent, to GFR. Thelimitations of the
present study are the relatively smallsample size and the fact that
we did not assess postoperativeERPF. If we could include both eGFR
and ERPF as postop-erative renal parameters, a more detailed
analysis would bepossible.
In conclusion, the present study showed that a preopera-tive
MAG3 renogram is not superior to simple and inexpen-sive eGFR
measurements as a prognostic indicator of futurerenal function
after unilateral nephrectomy.
References
1 McKiernan J, Simmons R, Katz J, Russo P. Natural historyof
chronic renal insufficiency after partial and radicalnephrectomy.
Urology 2002; 59: 81620.
2 Najarian JS, McHugh LE, Matas AJ, Chavers BM. 20 yearsor more
of follow-up of living kidney donors. Lancet 1992;340: 80710.
3 Malcolm JB, Bagrodia A, Derweesh IH et al. Comparisonof rates
and risk factors for developing chronic renalinsufficiency,
proteinuria and metabolic acidosis afterradical or partial
nephrectomy. BJU Int. 2009; 104:47681.
4 Lucas SM, Stern JM, Adibi M, Zeltser IS, Cadeddu JA, RajGV.
Renal function outcomes in patients treated for renalmasses smaller
than 4 cm by ablative and extirpativetechniques. J. Urol. 2008;
179: 7580.
5 Weight CJ, Larson BT, Fergany AF et al. Nephrectomyinduced
chronic renal insufficiency is associated withincreased risk of
cardiovascular death and death from anycause in patients with
localized cT1b renal masses. J. Urol.2010; 183: 131723.
6 Huang WC, Levey AS, Serio AM et al. Chronic kidneydisease
after nephrectomy in patients with renal corticaltumours: a
retrospective cohort study. Lancet Oncol. 2006;7: 73540.
7 Funahashi Y, Hattori R, Yamamoto T, Kamihira O, SassaN, Gotoh
M. Relationship between renal parenchymalvolume and single kidney
glomerular filtration rate beforeand after unilateral nephrectomy.
Urology 2011; 77:14048.
8 Artunc F, Yildiz S, Rossi C et al. Simultaneous evaluationof
renal morphology and function in live kidney donorsusing dynamic
magnetic resonance imaging. Nephrol. Dial.Transplant. 2010; 25:
198691.
9 Oriuchi N, Onishi Y, Kitamura H et al. Noninvasivemeasurement
of renal function with 99mTc-MAG3gamma-camera renography based on
the one-compartmentmodel. Clin. Nephrol. 1998; 50: 28994.
10 Matsuo S, Imai E, Horio M et al. Revised equations
forestimated GFR from serum creatinine in Japan. Am. J.Kidney Dis.
2009; 53: 98292.
11 Campbell ST, Novick AC, Belldegrun A et al. Guidelinefor
management of the clinical T1 renal mass. J. Urol.2009; 182:
12719.
12 Breau RH, Crispen PL, Jenkins SM, Blute ML, LeibovichBC.
Treatment of patients with small renal masses: asurvey of the
American Urological Association. J. Urol.2011; 185: 40714.
13 Mullerad M, Kastin A, Isaq E, Moskovitz B, Groshar D,Nativ O.
The value of quantitative 99mtechnetiumdimercapto-succinic acid
renal scintigraphy for predictingpostoperative renal insufficiency
in patients undergoingnephrectomy. J. Urol. 2003; 169: 247.
14 Shirasaki Y, Tsushima T, Saika T, Nasu Y, Kumon H.Kidney
function after nephrectomy for renal cellcarcinoma. Urology 2004;
64: 438.
15 Shirasaki Y, Saika T, Tsushima T, Nasu Y, Arata R,Kumon H.
Predicting postoperative renal insufficiency inpatients undergoing
nephrectomy for renal malignancy:assessment by renal scintigraphy
using 99mtechnetiummercaptoacetyltriglycine. J. Urol. 2005; 173:
38890.
16 Levey A, Bosch J, Lewis J, Greene T, Rogers N, Roth D. Amore
accurate method to estimate glomerular filtration ratefrom serum
creatinine: a new prediction equation. Ann.Intern. Med. 1999; 130:
46170.
17 Cockcroft DW, Gault MH. Prediction of creatinineclearance
from serum creatinine. Nephron 1976; 16: 3141.
18 Funahashi Y, Hattori R, Yamamoto T, Kamihira O, MoriyaY,
Gotoh M. Change in contralateral renal parenchymalvolume 1 week
after unilateral nephrectomy. Urology 2009;74: 70812.
H KANAMARU ET AL.
574 2011 The Japanese Urological Association











![« Y NՐ JՑ T» JՎ J L MՊՐ aՑ T X J a J X JՐ L1 NՐ NՎ J _ T ] V T R JՐ Y NՐ JՑ aՒ J _Վ J _ Պ NՏ J X J _ K S ` X J X J _ Y J ] J UՍ JՐ J _ « Y NՐ JՑ T» JՎ J L](https://img.dokumen.tips/doc/110x75/5e4f0d37f807db45c21a5e63/-y-n-j-t-j-j-l-m-a-t-x-j-a-j-x-j-l-1-n-n-j-t-v-t-r-j.jpg)








![X]^’( · j–– ° ‚ 。 † 。 。](https://img.dokumen.tips/doc/110x75/5e69871d602bdb15a8288f3d/xa-jaa-a-a-.jpg)







![x x z - YPC · 2019. 7. 12. · í _ x x z Y J ^ J f h J _ T Y J _ i J c N h a k R ^ J _ n i N _ m Q Y N e a k f h J h N f a k R ^ J _ N g e J M T a ^ T ] J f T _ î y x { x x x }](https://img.dokumen.tips/doc/110x75/6030680a7c67874c120c5ff2/x-x-z-ypc-2019-7-12-x-x-z-y-j-j-f-h-j-t-y-j-i-j-c-n-h-a-k-r-.jpg)