Embed Size (px)
Citation preview

J6
D
p
C
t
V
t
v
D
U
e
©
0
d
Oral Maxillofac Surg4:924-930, 2006
Cherubism: A Clinical, Radiographic, andHistopathologic Comparison of
7 CasesMiguel Peñarrocha, DDS, PhD,* Jaime Bonet, DDS, PhD,†
Juan Manuel Mínguez, DDS, PhD,‡
José Vicente Bagán, DDS, PhD,§ Francisco Vera, DDS, PhD,¶
and Ignacio Mínguez, DDS, PhD�
Purpose: Cherubism is an uncommon fibro-osseous disorder of the jaws that presents with varyingdegrees of involvement and a tendency toward spontaneous remission. Lesions are characterized byreplacement of bone with fibrovascular tissue containing abundant multinucleated giant cells. Weattempted to study the relationships among the degree of cherubism, the radiographic extent of the jawlesions, the histopathologic findings, and the clinical course of 7 patients.
Patients and Methods: In 7 patients diagnosed with cherubism, we evaluated the degree of fibrosisand perivascular cuffing, the presence of focal hemosiderin deposits, and giant multinucleated celldensity (absent, few, moderate, or severe). Clinical course and progression were also assessed using a4-point scale (improvement, no changes, modest progression, and marked progression).
Results: The patients were followed up for an average of 8.5 years. Two patients exhibited clinical andradiographic improvement, while 3 showed no changes, and 2 progressed despite surgical treatment in1 of them.
Conclusion: The course of cherubism in 1 of our patients may represent evidence of an associationbetween the presence of abundant multinucleated giant cells, an increased extent of the lesions, and amore aggressive behavior of the disease.© 2006 American Association of Oral and Maxillofacial Surgeons
J Oral Maxillofac Surg 64:924-930, 2006CsstdotcbpdaBoecrdgtrH
*Associate Professor of Oral Surgery, Faculty of Medicine and
entistry, Valencia University, Valencia, Spain.
†Section Chief of Maxillofacial Surgery, “La Fe” University Hos-
ital Children’s Center, Valencia, Spain.
‡Consultant in Maxillofacial Surgery, “La Fe” University Hospital
hildren’s Center, Valencia, Spain.
§Full Professor of Oral Medicine, Faculty of Medicine and Den-
istry, Valencia University; Head of the Service of Stomatology,
alencia University General Hospital, Valencia, Spain.
¶Associate Professor of Pathology, Faculty of Medicine and Den-
istry, Valencia University; Chairman of Pathology II, “La Fe” Uni-
ersity Hospital, Valencia, Spain.
�Professor of the Master in Oral Surgery, Faculty of Medicine and
entistry, Valencia University, Valencia, Spain.
Address correspondence and reprint requests to Dr Peñarrocha:
nidad Médico-Quirúrgica, Gascó Oliag 1, 46021 Valencia, Spain;
-mail: [email protected]
2006 American Association of Oral and Maxillofacial Surgeons
278-2391/06/6406-0009$32.00/0
toi:10.1016/j.joms.2006.02.003
924
herubism is a childhood disease that exhibits an auto-omal dominant hereditary pattern with variable expres-ion. The penetrance can be up to 100% in males and upo 70% in females.1 Some sporadic cases have beenescribed with no apparent familial history.2,3 Mutationf the gene encoding for fibroblast growth factor recep-or III (FGF-RIII) has also been found in some cases ofherubism.4,5 The condition constitutes an uncommon,enign fibro-osseous lesion that results in progressive,ainless, symmetrical expansion of the jaws with a pre-ilection for the mandible, resulting in a cherubic facialppearance.6,7 Affected children appear normal at birth.ilateral swelling tends to occur between 2 and 4 yearsf age. An increase in jaw size is noted, with maximumnlargement occurring within 2 years of onset in mostases. By age 7, the lesions become static or progresselatively slowly until puberty. During the late teens, theisease may undergo spontaneous involution, with re-ression of the maxillary lesions tending to occur earlierhan those in the mandible.8 Facial appearance mayeturn to almost normal by the fourth or fifth decade.owever, some patients seek surgical recontouring of
heir residual deformity during their twenties.8,9

asatroccigago
lgsismhcelihm
aat
P
oacacybwo
pwfdicpdl
S
S
S
P
R
aotdstel4(sItc
G
I
I
F
P
PEÑARROCHA ET AL 925
Arnott8 proposed a grading system for cherubism,ccording to lesion location and the degree of expan-ion. Accordingly, grade 1 cases are limited to bothscending rami of the mandible; grade 2 cases involvehe maxillary tuberosities and mandibular ascendingami (resulting in congenital absence of the third andccasionally the second molars); and grade 3 casesorrespond to massive involvement of both jaws ex-ept the coronoid processes and condyles, resultingn considerable facial disfigurement. Ramon and En-elberg10 added grade 4 in application to cases wherell of the classical features of the disorder exceedingrade 3 are present. The grade may change dependingn findings at follow-up examination.10,11
The lesions of cherubism are not distinctive histo-ogically and are difficult to differentiate from otheriant cell-containing fibro-osseous disorders. As a re-ult, the diagnosis also depends on the clinical find-ngs. Microscopy shows a highly vascular fibroustroma with unevenly distributed osteoclastic-likeultinucleated giant cells that tend to cluster nearemorrhagic foci and deposits of hemosiderin.9 Vas-ular channels are well formed and lined by largendothelial cells.12 The presence of eosinophilic, col-agenous material around small capillaries is of valuen the diagnosis of cherubism.13 Mature lesions ex-ibit more dense fibrous tissue, while the number ofultinucleated giant cells decreases.12
We studied 7 cases of cherubism in which wettempted to relate the clinical degree of the disorder,nd the radiographic and histopathologic characteris-ics of the lesions to the course of the disease.
atients and Methods
This retrospective study involved 9 patients treatedver a 15-year period and diagnosed with cherubismt the Children’s Maxillofacial Surgery Department inonjunction with the Department of Oral Medicinend Surgery. We reviewed all patients diagnosed withherubism and presenting a minimum follow-up of 1ear. Two patients were excluded from the studyecause of a lack of sufficient follow-up. Patientsere classified according to the grading system devel-ped by Arnott.8
A quantitative assessment of the histopathologicarameters was carried out (all histologic studiesere made by F.V., based on a 4-point scale: absent,
ew, moderate, or marked): giant multinucleated cellensity, interstitial hemorrhage, inflammatory activ-
ty, and the density of fibrosis. Three subtypes wereonsidered: I, predominance of multinuclear cells; II,redominance of inflammatory activity; and III, pre-ominance of fibrosis (Table 1), characterized as fol-
ows: (
ubtype I: Great abundance of large giant cells totallyoccupying the lesion surface. High cell density: 160to 180 giant cells per �200 field, interminglingwith small areas of interstitial microhemorrhage.
ubtype II: Lesser presence of giant cells, which rep-resent only part of the lesion. Abundant activeinflammatory component, with extensive vascular-ization, associated to giant cells of variable size.Low cell density: 10 to 15 giant cells per � 200field, intermingling with inflammatory and intersti-tial microhemorrhagic areas.
ubtype III: Abundant fibrosis with a reduced pres-ence of giant cells. The inflammatory component isscarce, although there may also be interstitial mi-crohemorrhagic areas. Low cell density: 5 to 8 giantcells per �200 field, associated to an extensive andoften dense or highly cellular fibrotic component.
atient evolution was also assessed by a 4-point scale:1) improvement (lesion reduction during the pro-cess); 2) no change (no significant lesion changes);3) progression (slow and moderate lesion growth);and 4) marked progression (rapid and constantlesion growth, and/or alterations appearing inother systems).
esults
The 7 patients (4 girls, 3 boys) were between 2nd 7 years of age at the onset of clinical evidencef disease, and presented a mean age of 8.2 years athe time of the diagnosis (Table 2). Five of the casesescribed were nonfamilial, and cases 4 and 5 wereiblings; none of the remaining family members ofhese 2 patients were affected. In all cases, clinicalxamination revealed enlargement of the mandibu-ar angle. Maximum growth was recorded between
and 5 and 7 and 8 years of age. Five patientscases 2, 3, 4, 5, and 7) presented bilateral midfacialwelling caused by involvement of the upper jaw.n case 3, in which the involvement was greater,here was thickening of the maxillary alveolar pro-esses, with partial obliteration of the palatal vault
Table 1. HISTOPATHOLOGIC SUBTYPES INCHERUBISM
Subtype I Subtype II Subtype III
iantcells
��� �/�� �/��
nterstitialhemorrhage
�/�� ��/��� �/��
nflammatorycomponent
– ��� �/�
ibrosis – � ���
eñarrocha et al. Cherubism. J Oral Maxillofac Surg 2006.
Fig 1). In the permanent dentition, dental crowd-

Ftm
P
h
Peñarrocha et al. Cherubism. J Oral Maxillofac Surg 2006.
926 CHERUBISM
IGURE 1. Case 3. A, Facial appearance of the patient showing symmetrical swelling of the mandibular angles. B, Intraoral image showinghickening of the alveolar processes, with partial obliteration of the palatal vault. C, Panoramic radiograph showing bilateral, sharply defined,ultilocular maxillary and mandibular radiotransparencies.
Table 2. CASES OF CHERUBISM—STUDY OF THE CLINICOPATHOLOGIC FEATURES AND PATIENT COURSE
Case No. Age (yr)Age On.
(yr) Gender TD (yr) TCGradeArnott Subtype Surgical Treatment Patient Course
1 20 2 F 11 9 1 II No Improvement2 14 3 M 13 1 3 III No No change3 12 3 F 4 8 2 II No Improvement4* 8 4 M 5 3 2 III No Progression5* 10 7 F 7 3 2 III No No change6 12 6 M 10 2 1 III No No change7 14 4 F 4 10 4 I Curettage expanded
lesions (3 times)Marked
progression
Abbreviations: Age On., age at onset of symptoms; F, female; M, male; TD, age at diagnosis; TC, control time; FD, fibrous density; DH, focalemosiderin deposits; PC, perivascular cuffing; GC, giant cells.*Two siblings (case nos. 4 and 5).
eñarrocha et al. Cherubism. J Oral Maxillofac Surg 2006.

it
rrsamfbitxdtmpt2rd
tmmmidt
w3wtcwys
sblgeatdwtoldct
D
lbuoiTiastbAc4
npapMdpaicnlps
idetspiceiaioboemcoa
o
PEÑARROCHA ET AL 927
ng and/or malpositioning was observed in all pa-ients except 1 (case 6).
Radiographically, all patients exhibited symmet-ical multilocular transparencies in the mandibularami and angles. Two patients (cases 2 and 7) alsohowed involvement of the coronoid processes,nd case 7 moreover presented involvement of theandibular symphysis. The condyles were unaf-
ected in all cases. The upper jaw was affectedilaterally in 5 patients (cases 2, 3, 4, 5, and 7), and
n case 7 there was additional partial bilateral infil-ration of the maxillary sinuses. In all cases the-rays revealed retained permanent teeth that wereisplaced from their usual position, and absenthird molars (with occasional absence of secondolars as well). Maxillofacial computed tomogra-hy in 4 patients (cases 2, 4, 5, and 7) revealedhese bone alterations in greater detail (Fig 2). Case
showed mastoid bone involvement presumablyesulting from occupation of these structures byysplastic soft tissues.In all patients, the histopathology showed substitu-
ion of bone by proliferating fibrous tissue exhibitingature fibroblasts embedded within an intercellularatrix, with a number of unevenly distributedultinucleated giant cells. Eosinophilic vascular cuff-
ng was seen in all cases, as well as focal hemosiderineposits. Assessment of the histopathologic parame-ers is reported in Table 1 (Fig 3).
Of the 6 patients in whom surgical interventionas limited to the obtainment of a biopsy, cases 1 andwere found to improve clinically and radiologically,ith a follow-up duration of 9 and 8 years, respec-
ively. Cases 2, 5, and 6 remained practically withouthange (up to ages 14, 10, and 12 years, respectively),hile case 4 showed progression between 5 to 7
ears of age, with a clear increase in bilateral midfacialwelling.
In case 7, at the age of 6 years, there was aignificant deformity of the mandibular rami, andone remodeling was carried out. Posteriorly, the
esions suffered marked progression. This girl pro-ressively lost all of her permanent teeth, withxfoliation of the resorbed roots. Serum calciumnd phosphorous levels were normal. Starting athe age of 12, several wine-red soft tissue masseseveloped in the mandible (Fig 2G); these lesionsere ulcerated as a result of chewing trauma with
he upper jaw, and were excised on a number ofccasions to facilitate chewing. Biopsies of these
esions always showed similar features, with abun-ant multinucleated giant cells. Nonetheless, theontrol of disease progression proved elusive, and
he lesions continued to grow. oiscussion
Radiographically, cherubism is characterized by bi-ateral, multilocular, radiolucent areas within the jaw-ones. The lesions usually appear around the mandib-lar angle and spread to the ascending rami and bodyf the lower jaw. The maxillary processes may also be
nvolved, and lesions can spread to other facial bones.he extent of the lesions varies from minor to massive
nvolvement of both jaws.11 In our study, plain x-raysnd computed tomography images demonstrated le-ions confined to the jaws in 6 cases, and with addi-ional facial bone involvement in case 2 (mastoidone). According to the grading system developed byrnott,8 our cases would be classified as grade 1 (2ases), grade 2 (3 cases), grade 3 (1 case), and grade(1 case).In general, cherubism does not have a poor prog-
osis. It has been noted that the condition does notrogress beyond puberty. As the patient grows todulthood, the jawbone lesions tend to resolve, and arogressively more normal jaw configuration is noted.11
axillary lesions are the first to regress, while man-ibular lesions are often still active at age 20.3 Ouratients were followed up for an average of 8.7 yearsfter the onset of clinical manifestations. Two casesmproved spontaneously, 3 remained stable, andases 4 and 7 worsened. In case 4, worsening wasoted from 4 to 8 years (a critical age when the
esions complete their evolution), while in case 7rogression was attributed to the particularly aggres-ive nature of the disease despite surgical treatment.
Because cherubism is considered to be a self-limit-ng condition that improves over time,14 treatmentepends on the individual patient’s functional andsthetic needs. Most investigators prefer to wait untilhe end of puberty before performing surgery. Earlyurgical intervention is contraindicated because it ap-ears to predispose to recurrences.15 Surgery is only
ndicated in cases characterized by impaired speech,hewing or swallowing difficulties, or with the pres-nce of major deformities that may cause psycholog-cal problems for the patient.12 Clinical managementnd surgical treatment decisions are dependent uponndividual evaluation in accordance with the degreef disease involvement. Surgical treatment appears toe unnecessary for grade 1 and 2 cases in the absencef secondary disturbances. Excision of tissue throughnucleation or curettage appears to be necessary inore aggressive cases (grade 3), to reduce maxillofa-
ial deformity after puberty and to ensure a successfulutcome without the risk of progression requiringdditional resection.11
The course of the disease was as expected in 6 ofur 7 patients, with worsening between 4 and 7 years
f age, followed by clinical and radiographic evidence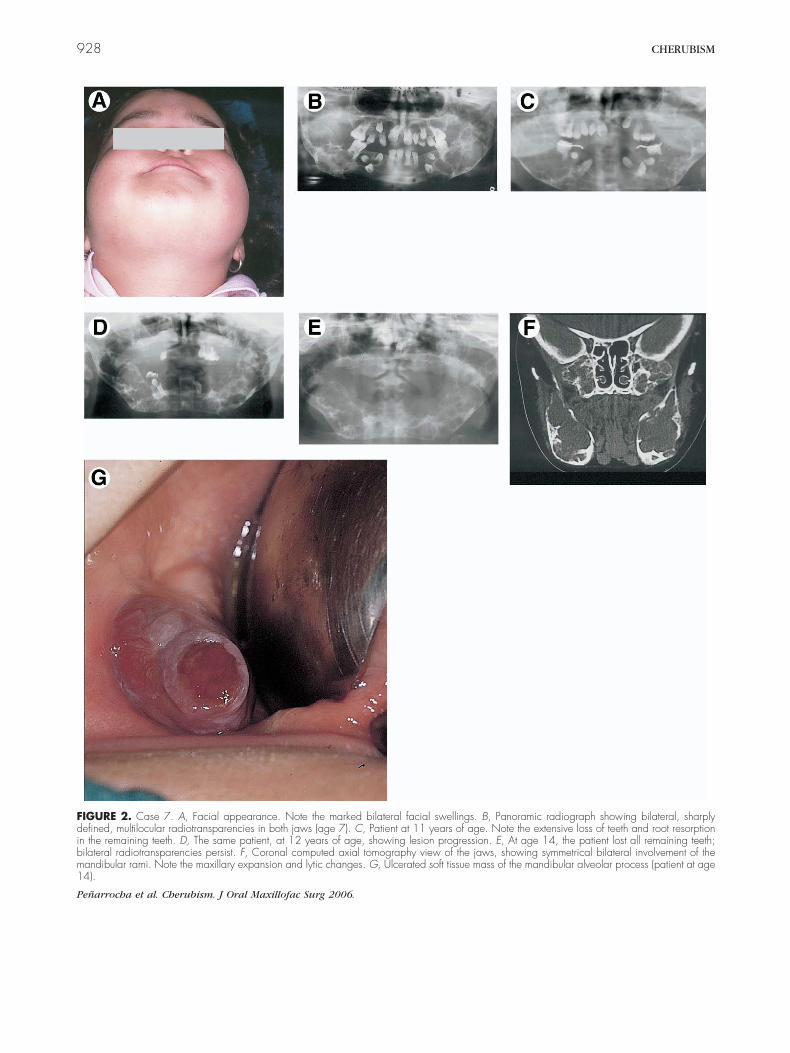
Fdibm1
P
928 CHERUBISM
IGURE 2. Case 7. A, Facial appearance. Note the marked bilateral facial swellings. B, Panoramic radiograph showing bilateral, sharplyefined, multilocular radiotransparencies in both jaws (age 7). C, Patient at 11 years of age. Note the extensive loss of teeth and root resorption
n the remaining teeth. D, The same patient, at 12 years of age, showing lesion progression. E, At age 14, the patient lost all remaining teeth;ilateral radiotransparencies persist. F, Coronal computed axial tomography view of the jaws, showing symmetrical bilateral involvement of theandibular rami. Note the maxillary expansion and lytic changes. G, Ulcerated soft tissue mass of the mandibular alveolar process (patient at age4).
eñarrocha et al. Cherubism. J Oral Maxillofac Surg 2006.

ohcrae
atAcflmpZrtswK
ctcmmidgv
agtpodatcs
Fecw
P
PEÑARROCHA ET AL 929
f improvement. The course was different in case 7,owever, with worsening from 4 years of age untilontrol was achieved at age 14. This was the only caseequiring surgical management because the patientlready had significant deformities including intraoralxophytic lesions.Long-term studies have shown the convenience
nd effectiveness of surgery in cherubism. Conserva-ive approaches to management are advisable.14
mong our patients, surgery was only performed inase 7, to correct bothersome lesions and facial de-ormity. Curettage with remodeling of the corticalayer was carried out in the same procedure because
ost investigators regard this as the best ap-roach.15,16 Following surgery in a 5-year-old boy,achariades et al12 used homogeneous bone grafts toeplace the diseased tissue to avoid pathologic frac-ure of the mandible. Since then, these authors ob-erved gradual involvement of other sites in the jaws,ith the displacement of teeth and tooth germs.
IGURE 3. Microscopy reveals the following: A, Subtype I: great abosin stain; magnification �100); 160 to 180 giant cells per �200 fiomponent (hematoxylin-eosin stain; magnification �100); 10 to 15 gith scattered multinucleated giant cells (hematoxylin-eosin stain; mag
eñarrocha et al. Cherubism. J Oral Maxillofac Surg 2006.
oury et al17 described a case in which the usual c
ourse of the lesions changed dramatically duringreatment, with unilateral growth associated with vas-ular proliferation after surgical recontouring. Theost active areas show a vascular, loose stroma andore numerous giant cells, whereas slower-progress-
ng lesions show increased collagen, fibrosis, and aecreased number of giant cells. These authors sug-ested that it is very possible that surgery caused suchascular transformation.In some cases of cherubism, giant cells may be so
bundant that the histologic image alone can poseenuine differential diagnostic difficulties versus cen-ral giant cell granuloma or brown tumor of hyper-arathyroidism. Giant cell granuloma can be excludedn clinical grounds, because it is not a bilateral con-ition, is not inherited, does not regress in adulthood,nd has a predilection for the anterior mandible. Inurn, bone changes in hyperparathyroidism rarelyause unilateral jaw lesions, but do produce abnormalerum calcium and phosphorus levels.18-20 In
e of large giant cells totally occupying the lesion surface (hematoxylin-Subtype II: lesser presence of giant cells, with abundant inflammatorylls per �200 field. C, Subtype III: abundant connective tissue stroman �100); 5 to 8 giant cells per �200 field.
undanceld. B,iant cenificatio
herubism, eosinophilic collagen cuffing can be ob-

shToi
ifudcastsmK
ammdrr
R
1
1
1
1
1
1
1
1
1
1
2
2
2
930 CHERUBISM
erved around small blood vessels. Such perivascularyalinosis is considered pathognomonic of cherubism.21
his finding was evident in the tissue samples of all ofur patients, although with varying frequency and
ntensity.The tissue alterations were characteristic and were
dentified in all cases. Multinucleated giant cellsormed small disperse agglomerations or were distrib-ted around capillaries,22 and were particularly abun-ant in case 7, which showed the worst clinicalourse. In this case there were abundant multinucle-ted giant cells noted in the first biopsy. Recontouringurgery was performed several times. It would appearhat in this case the condition was intrinsically aggres-ive, and did not correspond to aggressive transfor-ation induced by surgery, as in the case reported byoury et al.17
In one of our patients, there appeared to be anssociation between the presence of abundantultinucleated giant cells, extensive lesion size, andore aggressive disease behavior. Whether the abun-
ance and density of giant multinucleated cells iselated to increased aggressiveness of the conditionemains to be clarified by future studies.
eferences1. Peters WJ: Cherubism: A study of twenty cases from one family.
Oral Surg Oral Med Oral Pathol 47:307, 19792. Kaugars GE, Niamtu J, Svrirsky JA: Cherubism: Diagnosis, treat-
ment, and comparison with central giant cell granulomas andgiant cell tumors. Oral Surg Oral Med Oral Pathol 73:369, 1992
3. De Tomasi DC, Hann JR, Stewart HM Jr: Cherubism: Report ofa nonfamilial case. J Am Dent Assoc 111:455, 1985
4. Schultze-Mosgau S, Holbach LM, Wiltfang J: Cherubism: Clini-cal evidence and therapy. J Craniofac Surg 14:201, 2003
5. Zohar Y, Grausbord R, Shatai Y: Fibrous dysplasia andcherubism as an hereditary familial disease. Follow-up of fourgenerations. J Craniofac Surg 17:340, 1989
6. Bagán JV, Ceballos A, Bermejo A, et al: Medicina oral. Barce-lona, Spain, Masson, 1995, p 459
7. Burland JG: Cherubism: Familial bilateral osseous dysplasia ofthe jaws. Oral Surg 15:43, 1962
8. Arnott DG: Cherubism—An initial unilateral presentation. Br JOral Surg 16:38, 1978
9. Faircloth J, Edwards R, Farhood V: Cherubism involving amother and daughter: Case reports and review of the literature.J Oral Maxillofac Surg 49:535, 1991
0. Ramon Y, Engelberg IS: An unusually extensive case ofcherubism. J Oral Maxillofac Surg 44:325, 1986
1. Hitomi G, Nishide N, Mitsui K: Cherubism. Diagnostic imagingand review of the literature in Japan. Oral Surg Oral Med OralPathol 81:623, 1996
2. Zachariades N, Papanicolau S, Xypolyta A, et al: Cherubism. IntJ Oral Surg 14:138, 1985
3. Hamner JE, Ketcham AS: Cherubism: An analysis of treatment.Cancer 23:1133, 1969
4. Katz JO, Dunlap CL, Ennis RL: Cherubism: Report of a caseshowing regression without treatment. J Oral Maxillofac Surg50:301, 1992
5. Belloc JB, Divaris M, Cancemi GF, et al: Le chérubisme. Apropos d́un cas majeur. Rev Stomatol Chir Maxillofac 94:152,1993
6. Peters WJ: Cherubism. A study of twenty cases from onefamily. Oral Surg 47:307, 1979
7. Koury ME, Stella JP, Epker BN: Vascular transformation incherubism. Oral Surg Oral Med Oral Pathol 76:20, 1993
8. Weldon L, Cozzi G: Multiple giant cell lesions of the jaws. J OralMaxillofac Surg 40:520, 1982
9. Cawson RA, Eveson JW: Oral Pathology and Diagnosis. London,William Heinemann Medical Books, 1987
0. Kerley TR, Schow CE: Central giant cell granuloma orcherubism. Report of a case. Oral Surg Oral Med Oral Pathol51:128, 1981
1. Davis G, Sinn DP, Watson SW: Clinicopathologic conferencesCase 43, Part I. J Oral Maxillofac Surg 41:47, 1983
2. Penfold CN, McCullagh P, Eveson JW: Giant cell lesions com-plicating fibro-osseous conditions of the jaws. Int J Oral Max-
illofac Surg 22:158, 1993











![Investigation of the SH3BP2 Gene Mutation in Cherubism · genetic advances have been made in relation to cherubism with the identification of the gene SH3BP2 [2, 5]. SH3BP2 was initially](https://img.dokumen.tips/doc/110x75/5ed57c2b0bd3843450408d1d/investigation-of-the-sh3bp2-gene-mutation-in-genetic-advances-have-been-made-in.jpg)
















