-
8/2/2019 J Fazakas Bleeding Management in Organ
Transplantation
1/30
Bleeding management in organBleeding management in organ
transplantation and intensive caretransplantation and intensive
care
Bleeding Management Course - from theory to clinical
practice
Jnos Fazakas MD, PhD
-
8/2/2019 J Fazakas Bleeding Management in Organ
Transplantation
2/30
THE COMPLEXITY OF PERIOPERATIVECOAGULATION DISORDERS
loss
dilution
hyperfibrinolysis
consumption
supply
endogen
heparinoids
one organ failure multiorgan dysfunction
-
8/2/2019 J Fazakas Bleeding Management in Organ
Transplantation
3/30
Kidney transplantation: hemodialysis + anticoagulation
venous and arterial reperfusion: coagulation disorder
-
8/2/2019 J Fazakas Bleeding Management in Organ
Transplantation
4/30
Pancreas and kidney transplantation: hemodialysis +
anticoagulation , DM + IHD
2 grafts 2 x venous + arterial reperfusions:
coagulation disorder, fibrinolysis
-
8/2/2019 J Fazakas Bleeding Management in Organ
Transplantation
5/30
Kidney recipients: catheter associated thrombosis and stenosis,
atrial fibrillation,
coronary stents, congenital coagulation disorders
treatment with vitamin K antagonist INR 2.5-5.5
TACO
TRALI ?
CIT + 2-4 hours HDF
PCC
Clinical Practice Guidelines and Clinical Practice
Recommendations, 2006 Updates
-
8/2/2019 J Fazakas Bleeding Management in Organ
Transplantation
6/30
In patients who are receiving VKAs and require reversal of
the
anticoagulant effect for an urgent surgical or other invasive
procedure, the
guideline developers recommend treatment with low-dose (2.5 to
5.0
mg) IV or oral vitamin K (Grade 1C).
For more immediate reversal of the anticoagulant effect,
the guideline developers suggest treatment with fresh-frozen
plasma or anotherprothrombin concentrate in addition to
low-dose IV or oral vitamin K (Grade 2C).
The perioperative management ofantithrombotic therapy
American College of Chest Physicians, evidence-based clinical
practice guideline
(8th edition)
Chest, 2008 Jun; 133 (6 Suppl) : 299S-339S
-
8/2/2019 J Fazakas Bleeding Management in Organ
Transplantation
7/30
patients No RBC RBC FFP PLTCoagulation
monitoring
Dalmau et al. 2001 122 34 % 2.9 (0-6) 1.6 (0-4) 7.9 (0-15) BT,
TEG
Dalmau et al. 2004 127 38 % 2.3 (0-5) 1.25 (0-3) 5 (0-11) BT
Massicote et al. 2005 206 32 % 2.8 (0-7) 4.1 (0-8) 0.4 (0-3)
?
Frasco et al. 2005 69 ? 2.9 (0-6) 2.5 (0-5) 1.2 (0-2) ?
Mangus et al. 2007 526 17.5 % 3 7 6 ?
Boer et al. 2008 236 26 % 2.2 (0-6) 2 (0-7) 0 (0-1) BT, TEG
Massicote et al. 2008 200 81.5 % 0.3 0.8 0 0 ?
Overview of blood product transfusion
during liver transplantation
Curr Opin Organ Transplant 14 (2009) 286-290
Clear reduction of blood products requirements
Blood tests (BT) usefulness in bleeding prediction
20% no bleeding, 20% still serious bleeding
Clear reduction of blood products requirements
Blood tests (BT) usefulness in bleeding prediction
20% no bleeding, 20% still serious bleeding
-
8/2/2019 J Fazakas Bleeding Management in Organ
Transplantation
8/30
Hepatectomy: preop. coagulation profile coagulation factors :
dilution + consumption
blood loss correlate with the degree of surgical difficulty
adhesion dissection and transection of portocaval shunts
-
8/2/2019 J Fazakas Bleeding Management in Organ
Transplantation
9/30
Hepatectomy: preop. coagulation profile coagulation factors :
dilution + consumption
blood loss correlate with the degree of surgical difficulty
adhesion dissection and transection of portocaval shunts
-
8/2/2019 J Fazakas Bleeding Management in Organ
Transplantation
10/30
Anhepatic phase : no clearance of activated coagulation factors
and tPA
no supply by synthesis activity but a continuous consumption
failure of homeostasis: pH , Se Ca+ , TC
volume overload in the splanchnic area
-
8/2/2019 J Fazakas Bleeding Management in Organ
Transplantation
11/30
Venous and arterial reperfusion: coagulopathy and microvascular
diffuse bleeding (30-90 min)
endogen heparinoids ; fibrinolitic substances
the degree and duration is variable with donor graft quality
-
8/2/2019 J Fazakas Bleeding Management in Organ
Transplantation
12/30
core
skin
relative normovolemiaincreased CVP
Limbs: venous blood shiftin the abdominal and thoracic vein
Intraoperative hypothermia
Warming
-
8/2/2019 J Fazakas Bleeding Management in Organ
Transplantation
13/30
Coagulation
Hypothermia
fibrinogen
prothrombin complex
thrombocyte
Normothermia
FFP (factor VIII !!!!)
Fibrinolysis
EAC, tranexamic acid
New possibility:
rFVIIa, XIIIa
-
8/2/2019 J Fazakas Bleeding Management in Organ
Transplantation
14/30
amplification
TF VIIa
XaIIa
PLT
Ia
VIIIa
Va
IXa
XIIIa
20 x
5% 95%
Coagulation tests
Y shape modell - 1960 cell based modell - 1980
standard
testsTEG
Thrombin production
initiation propagation
-
8/2/2019 J Fazakas Bleeding Management in Organ
Transplantation
15/30
INR kva WHO etalon KVA: K vitamin antagonist blood
(PT test / PT normal)ISI
kva
Tripodi et al. Hepatology, 2007, 46: 520-27; Bellest et al.
Hepatology, 2007, 46:528-34
INRkva
A-B=0.3
C=0.5
healthy test
-
8/2/2019 J Fazakas Bleeding Management in Organ
Transplantation
16/30
INR liver etalon blood of cirrhotic patient
(PT test / PT normal)ISI
liver
Tripodi et al. Hepatology, 2007, 46: 520-27; Bellest et al.
Hepatology, 2007, 46:528-34
INRliver
A-B=0.01
C=0.02
-
8/2/2019 J Fazakas Bleeding Management in Organ
Transplantation
17/30
platelets provided phospholipid surface to complement normal
thrombin generation
Tripodi et al. Hepatology, 2007, 46: 727-733
Evidence of normal thrombin generation in cirrhosisdespite
abnormal conventional coagulation tests
-
8/2/2019 J Fazakas Bleeding Management in Organ
Transplantation
18/30
Balance of potential risks and benefits ofplatelets in liver
transplantation
Platelets in liver transplantation: Friend or foe?
BenefitsBenefits RiskRisk
Component of primary hemostasisContribution to ischemia
reperfusion
injury
Involvement in tissue repair Involvement in postoperative
thrombosis
Involvement in liver generationAssociation with adverse outcome
of
transplantation
Liver Transpl, 2008, 14: 923-931
Chest, 2008 Jun; 133 (6 Suppl) : 299S-339S
For patients receiving aspirin, clopidogrel, or both, are
undergoing surgeryand have excessive or life-threatening
perioperative bleeding, the guideline
developers suggest transfusion of platelets or administration of
otherprohemostatic agents (Grade 2C).
The perioperative management of antithrombotic therapy. American
College of ChestPhysicians evidence-based clinical practice
guidelines (8th edition).
-
8/2/2019 J Fazakas Bleeding Management in Organ
Transplantation
19/30
surgical hemostasis
pH>7,2 SeCa> 1 HGB>100g/l T> 35TEG, fibrinolysis,
aprotinin ?
fibrinogen
PCC , FFP
PLT
VII a
1) factor dilution
2) VIII , vonW syndr.
3) G 2a/3b receptor number
4) fibrin polymerization
trouble
Female, HLA DR
TRALI / TACO
FFP
Fibrinogen < 1g/l V < 20% VII < 20% PLT < 50.000
initiation amplification - propagation
normothermia ?hypothermia ?
XIIIa
-
8/2/2019 J Fazakas Bleeding Management in Organ
Transplantation
20/30
Antibody against fathers leukocyte HLA
75% of female blood donors were pregnant
Appearance of HLA antibody :
in all female donors: 15 %
in never pregnant donors: 1.6 %
after 1 pregnancy: 10.5 %
after 2 pregnancies: 15.8 %
after 3 pregnancies: 25 %
after 4 pregnancies: 36 %
Odds ratio of TRALI
all plasma 3.4 (1.2-10.2)
male plasma 2.7 (0.7-10.1) female plasma 25.6 (1.3- 49.9)
Massicote et al: Transplantation 2008 Apr 15;85(7):956-962 Rana
et al. Transfusion 2006; 46:1478-83
Massicote, 2008: The avoidance of plasma transfusion was
associatedwith a decrease in RBC transfusions during liver
transplantation.
-
8/2/2019 J Fazakas Bleeding Management in Organ
Transplantation
21/30
12 - 18 hours
4 - 6 hours
> 24 hours
healthy
Nature Medicine 2007,13: 463 469
-
8/2/2019 J Fazakas Bleeding Management in Organ
Transplantation
22/30
-
8/2/2019 J Fazakas Bleeding Management in Organ
Transplantation
23/30
O2 supply
CPAP mask
SPIROMETRY TESTING AFTER LTX
MINOR TRALI
-
8/2/2019 J Fazakas Bleeding Management in Organ
Transplantation
24/30
Components (n)Class I
n (%)
Class II
n (%)
Class I & II
n (%)
Total
n (%)
RBCs (106) 7 (6.6%) 8 (7.5%) 3 (2.8%) 18 (16.9%)
Cryo (66) 3 (4.5%) 3 (4.5%) 10 (15.1%) 16 (24.2%)
FFP (77)9
(11.6%)4 (5.2%) 9 (11.6%) 22 (28.5%)
Platelets (59) 7 (12%) 5 (9%) 1 (2%) 13 (22%)
HLA antibodies in blood componentsUnappreciated risk factors for
transplant patients
Human Immunology 65 (2004) 240-244
no published data: HLA antibodies promote allograft dysfunction
?!?
transfusion mediated rejection: HLA-Ag graft + antibodies
HLA-Ab
-
8/2/2019 J Fazakas Bleeding Management in Organ
Transplantation
25/30
0
2
4
6
Anesthe
sia
hepa
tectom
y
hepa
tectom
y
anhepa
tic
PVreperfusi
on
Artreperfusi
on
Endof
surgery
POP1ho
ur
0
10
Prepare for anhepatic phase Optimize all function
Responsiveness !
AT III
fibrinolysis Endogeneousheparinoids
-
8/2/2019 J Fazakas Bleeding Management in Organ
Transplantation
26/30
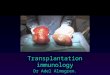
The two tales of coagulation in transplantation:the rebalancing
story
Normal patient Patient with liver disease
thrombocytopenia + function defects
enhanced NO + PGI2 production
Primary hemostasis
Delicate rebalancePromoting bleeding Promoting thrombosis
elevated levels of VWF
decreased levels of ADAMTS
(VWF protease)
Secondary hemostasis low level of II, V, VII, IX, X, XI
factors
dysfibrinogenemia
elevated levels of VIII factor
decreased levels of prot C, prot S, AT III
decreased levels of heparin cofactors
Fibrinolysis low levels of 2antiplasmin,XIII factor
elevated tPA levels
low levels of plasminogen
Current Opinion in Organ Transplantation 2008, 13: 298-303
-
8/2/2019 J Fazakas Bleeding Management in Organ
Transplantation
27/30
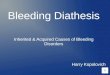
Hypercoagulability based on TEG
short R time < 4 min, increased angle (> 75), increased MA
> 75 mm
Hypercoagulable Normal
-
8/2/2019 J Fazakas Bleeding Management in Organ
Transplantation
28/30
ESDL etiology and coagulation profilePLT, INR, APTI, coagulation
factors ATIII, protein S, protein C
Plasminogen, t PA, PAI 1, PAI 2 2-antiplasmin, 2
-macroglobulin
Risk of thrombosis
Budd Chiari syndr., POPH,glycogen storage disease,
AIH, PSC, PBC
More AT III (Na Heparin) thanfibrinogen, PCC, platelets, FFP
Normothermia
YesYes GRAFT quality
Risk of bleeding
Wilsons d., HCV, HBV,ALD, hemochromatosis
NASH
Hypothermia
volume restriction
fibrinogen, PCC,
platelets, FFP fibrinogen, PCC,
platelets, FFP
TEGTEGTEGTEG
Poor quality graft
TEGTEGGood quality graft
Fibrinolysis
Heparin like effect
Diffuse bleeding
Reperfusion
Fibrinolysis
Heparin like effect
15-30 min
R, K time MA / MCF
-
8/2/2019 J Fazakas Bleeding Management in Organ
Transplantation
29/30
Anticoagulationgylcocalyx the endothelial gatekeeper
Physiologic factors: protein C, protein S, AT III
Level must be measured and corrected
Graft glycocalyx is burned out after reperfusion
AT III, Na Heparin, LMWH, platelet inhibitors /adv. vs
disadv./
According to vascular anastomosis
According to surgical field (wet or dry) According to patient
comorbidities
According to coagulation parameters measured
National and local protocols
pediatric pts. more vulnerable
Patient tailoredcoagulation profile
AT III
-
8/2/2019 J Fazakas Bleeding Management in Organ
Transplantation
30/30