Embed Size (px)
Citation preview

IVUS Observations in IVUS Observations in Acute (vs Chronic) Acute (vs Chronic) Coronary Artery Coronary Artery
Disease: Disease: Structure vs Structure vs FunctionFunction
Gary S. Gary S. MintzMintz, MD, MD

Important IVUS Observations: Remodeling
Important IVUS Observations: Remodeling
••Originally used (first by Originally used (first by GlagovGlagov) to explain ) to explain atherosclerosis in the absence of lumen atherosclerosis in the absence of lumen compromise compromise -- mostly in reference segmentsmostly in reference segments••Regardless of the definition, assessing lesion Regardless of the definition, assessing lesion remodeling requires a comparison to the remodeling requires a comparison to the reference segmentreference segment
••Positive (outward) remodeling in ACSPositive (outward) remodeling in ACS
••Negative (constrictive or inward) remodeling in Negative (constrictive or inward) remodeling in stenosis stenosis formation in chronic stable anginaformation in chronic stable angina

Reference SegmentsReference Segments
Mintz Mintz et al, J Am et al, J Am Coll Cardiol Coll Cardiol 1995;25:14791995;25:1479--8585
Positive Positive remodelingremodeling
Intermediate Intermediate remodelingremodeling
Negative Negative remodelingremodeling
Nishioka Nishioka et al. J Am et al. J Am Coll Cardiol Coll Cardiol 1996; 27:15711996; 27:1571--7676
LesionsLesions

--RemRemIntermediateIntermediate++RemRem
Transplant Transplant atherosclerosis (4,21,22)atherosclerosis (4,21,22)
Vasospastic Vasospastic anginaangina(15)(15)
Advanced Advanced fibrocalcific fibrocalcific disease (2,5,9)disease (2,5,9)
Advanced age (26)Advanced age (26)Smoking (5,14)Smoking (5,14)
InsulinInsulin--treated DM (6)treated DM (6)
Reference segment disease (12)Reference segment disease (12)Early atherosclerosis (1)Early atherosclerosis (1)
Soft plaques (9)Soft plaques (9)Chronic stable angina or Chronic stable angina or
old MI (2,3,5,14,17,20)old MI (2,3,5,14,17,20)
Increased Increased restenosis restenosis and and CKCK--MB postMB post--PCI PCI
(13,17,18,23,24)(13,17,18,23,24)
1) 1) GlagovGlagov. N . N Engl Engl J Med 1987;316:1371J Med 1987;316:1371--552) 2) MintzMintz. Circulation 1997;95:1791. Circulation 1997;95:1791--883) 3) NishiokaNishioka. JACC 1996;27:1571. JACC 1996;27:1571--664) Lim. Circulation. 1997;95:8554) Lim. Circulation. 1997;95:855--995) 5) TauthTauth. AJC 1997;80:1352. AJC 1997;80:1352--556) 6) KornowskiKornowski. AJC 1998; 81:1298. AJC 1998; 81:1298--130413047) 7) SchwarzacherSchwarzacher. Circulation 1998;98:I. Circulation 1998;98:I--1451458) 8) SchoenhagenSchoenhagen. Circulation 2000;101:598. Circulation 2000;101:598--6036039) 9) SabateSabate. AJC 1999;84:135. AJC 1999;84:135--40.40.10) von 10) von BirgelenBirgelen. JACC 2001;37:1864. JACC 2001;37:1864--707011) 11) KawagoeKawagoe. Circulation 1998;98:I. Circulation 1998;98:I--36836812) 12) MintzMintz. JACC 1995;25:1479. JACC 1995;25:1479--858513) 13) DangasDangas. Circulation1999;99:3149. Circulation1999;99:3149--545414) 14) WeissmanWeissman. AJC 1999;84:37. AJC 1999;84:37--404015) Hong. Am Heart J 2000;140:39515) Hong. Am Heart J 2000;140:395--40140116) 16) AbizaidAbizaid. JACC 1999;33:53A. JACC 1999;33:53A17) 17) WexbergWexberg. JACC 2000;36:1860. JACC 2000;36:1860--9918) 18) MehranMehran. Circulation 2000;101:604. Circulation 2000;101:604--101019) Taylor. JACC 1999;34:76019) Taylor. JACC 1999;34:760--7720) Nakamura. JACC 2001;37:6320) Nakamura. JACC 2001;37:63--9921) 21) PethigPethig. Am Heart J 1998;135:628. Am Heart J 1998;135:628--333322) 22) KobashigawaKobashigawa. J Heart Lung Transplant . J Heart Lung Transplant
2000;19:5462000;19:546--505023) Endo. JACC 2001;37:7023) Endo. JACC 2001;37:70--5524) Okura. JACC 2001 (in press)24) Okura. JACC 2001 (in press)25) 25) NishiokaNishioka. AJC 2001;87:387. AJC 2001;87:387--919126) 26) GyongyosiGyongyosi. . Coron Coron Artery Artery Dis Dis 1999;10:2111999;10:211--9927) Ward. Atherosclerosis 2001;154:17927) Ward. Atherosclerosis 2001;154:179--8383
Hypercholesterolemia (5)Hypercholesterolemia (5)High HDLHigh HDL--cholesterol (19)cholesterol (19)
New New stenosis stenosis in another location in another location (17)(17)
Acute coronary syndromes Acute coronary syndromes (7,8,10,11,16,20)(7,8,10,11,16,20)
Proximal disease, eccentric Proximal disease, eccentric lesions surrounded by lesions surrounded by
pericardium (9,25)pericardium (9,25)
OstialOstial, distal disease, , distal disease, eccentric lesions surrounded eccentric lesions surrounded
by myocardium (9,25,27)by myocardium (9,25,27)
↓↓ Plaque burdenPlaque burden↑↑ Plaque burdenPlaque burden

Remodeling in Acute Coronary SyndromesRemodeling in Acute Coronary Syndromes
pStableACS
0.0080.0080.940.94±±±±±±±±0.20.21.061.06±±±±±±±±0.0.22
Remodeling IndexRemodeling Index
0.0050.00511.111.1±±±±±±±±4.84.813.913.9±±±±±±±±5.5.55
P&M CSA (mmP&M CSA (mm22))
0.30.31.91.9±±±±±±±±0.40.42.32.3±±±±±±±±1.11.1Lumen CSA (mmLumen CSA (mm22))
0.0040.00413.013.0±±±±±±±±4.84.816.116.1±±±±±±±±6.6.22
EEM CSA (mmEEM CSA (mm22))
LesionLesion
0.90.96.26.2±±±±±±±±3.53.56.16.1±±±±±±±±2.62.6P&M CSA (mmP&M CSA (mm22))
0.060.067.97.9±±±±±±±±2.82.89.19.1±±±±±±±±3.63.6Lumen CSA (mmLumen CSA (mm22))
0.20.214.214.2±±±±±±±±5.25.215.215.2±±±±±±±±5,5,22
EEM CSA (mmEEM CSA (mm22))
Proximal referenceProximal reference
Schoenhagen Schoenhagen et al. Circulation 2000;101:598et al. Circulation 2000;101:598--603603
RemodelingRemodeling
0
10
20
30
40
50
60
Positive No Negative
ACSStable
P=0.001P=0.001

Diabetes Modulates Remodeling in ACS and Stable Angina (n=927)
Diabetes Modulates Remodeling in ACS and Stable Angina (n=927)
42/187 42/187 (22.3%)(22.3%)
17/88 17/88 (19.6%)(19.6%)Stable AnginaStable Angina
225/469225/469(48.0%)(48.0%)
59/183 59/183 (32.0%)(32.0%)
Acute Acute Coronary Coronary SyndromeSyndrome
No DMDM
AbizaidAbizaid, unpublished observations, unpublished observations
Frequency of Positive RemodelingFrequency of Positive Remodeling

In Some Patients with Chronic Stable Angina Negative Remodeling Appears to Occur Early During Stenosis
Formation
In Some Patients with Chronic Stable Angina Negative Remodeling Appears to Occur Early During Stenosis
Formation
0
10
20
30
40
50
60
NegativeRemodeling
IntermediateRemodeling
PositiveRemodeling
104 intermediate stenoses (QCA DS<60%)
104 intermediate stenoses (QCA DS<60%)
Hirose M, AJC in pressHirose M, AJC in press
274 RCA stenoses, stratified according to reference disease274 RCA stenoses, stratified
according to reference disease
0
5
10
15
20
25
30
35
40
45
50
<20% (n=91) 20-40% (n=91) 40-60% (n=92)
Negative remodeling
Intermediate remodeling
Positive remodeling
Hong MHong M--K, JACC in pressK, JACC in press
Reference plaque burden

0
10
20
30
40
50
MACE (%) Target LesionRestenosis (%)
New StenosisFormation (%)
Positive Pre-PCI Remodeling (n=70)Intermediate Pre-PCI Remodeling (n=110)
Negative Pre-PCI Remodeling (n=64)
244 Patients with Stable Angina and Single Vessel Intervention
244 Patients with Stable Angina and Single Vessel Intervention
Wexberg Wexberg et al. J Amet al. J Am Coll Cardiol Coll Cardiol 2000;36:18602000;36:1860--99
p=0.007p=0.007
p=0.036p=0.036p=0.024p=0.024

Important IVUS Observations: Lesion Morphology
Important IVUS Observations: Lesion Morphology
••Acute coronary syndromesAcute coronary syndromes••Hypoechoic Hypoechoic plaqueplaque
••Eccentric lesionsEccentric lesions
••Ruptured plaquesRuptured plaques
••ThrombusThrombus--containing plaques in ACScontaining plaques in ACS
••Fibrocalcific Fibrocalcific plaque in chronic stable angina in plaque in chronic stable angina in association with negative remodelingassociation with negative remodeling••Positive remodeling and unstable lesion morphologies Positive remodeling and unstable lesion morphologies --i.e., ruptured and thrombusi.e., ruptured and thrombus--containing plaques containing plaques -- tend to tend to occur together in ACSoccur together in ACS

Plaque Composition in Acute Coronary Syndromes
Plaque Composition in Acute Plaque Composition in Acute Coronary SyndromesCoronary Syndromes
05
1015202530354045
Echolucent Echodense Mixed Calcific
ACSStable
Schoenhagen Schoenhagen et al. Circulation 2000;101:598et al. Circulation 2000;101:598--603603
p=0.02p=0.02
p=NSp=NS
p=NSp=NS p=NSp=NS

Comparison of Patients with ACS, no MI within 3 weeks, Single de novo Culprit Lesion
Troponin (+) vs Troponin (-)
Comparison of Patients with ACS, no MI Comparison of Patients with ACS, no MI within 3 weeks, Singlewithin 3 weeks, Single de novo de novo Culprit LesionCulprit Lesion
Troponin Troponin (+) vs(+) vs Troponin Troponin ((--))
05
1015202530354045
Plaque rupture(%)
Dissection (%) Thrombus (%) Any unstablemorphology
(%)
Troponin + (n=40)Troponin - (n=45)
Fuchs et al. Am JFuchs et al. Am J Cardiol Cardiol 2002;89:11112002;89:1111--33
p=0.4p=0.4p=0.3p=0.3
p=0.048p=0.048
p=0.17p=0.17

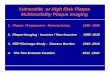
Three Vessel IVUS Imaging in 24 Pts with ACS and Positive Tn
Three Vessel IVUS Imaging in 24 Pts with ACS and Positive Tn
• 50 ruptured plaques• 9 culprit lesion• 41 nonculprit lesion
• 19 pts had at least 1 nonculprit plaque rupture
• 17 pts had 1 plaque rupture in a second artery
• 3 pts had plaque ruptures in all 3 arteries
• 50 ruptured plaques• 9 culprit lesion• 41 nonculprit lesion
• 19 pts had at least 1 nonculprit plaque rupture
• 17 pts had 1 plaque rupture in a second artery
• 3 pts had plaque ruptures in all 3 arteries 0
5
10
15
20
25
30
35
0 1 2 3 4 5
Rioufol Rioufol et al Circulation 2002;106:804et al Circulation 2002;106:804--808808
%
# of Ruptured Plaques

300 plaque ruptures in 257 arteries of 254 pts300 300 plaque ruptures in 257 arteries of 254 ptsplaque ruptures in 257 arteries of 254 pts
• Thrombus in 46%• more frequent in pts with
USA or peri-MI, p=0.02• more frequent in arteries with
multiple rupture sites, p=0.04• Ca++ in 55%,
• arc=36±±±±47°°°°• located at the base of the
rupture in 86%• Tear in fibrous cap identified
in 59%,• at shoulder of plaque in 68%
in center of plaque in 32%• Multiple rupture sites in 14%
of ACS patients
•• Thrombus in 46%Thrombus in 46%•• more frequent in pts with more frequent in pts with
USA orUSA or periperi--MI, p=0.02MI, p=0.02•• more frequent in arteries with more frequent in arteries with
multiple rupture sites, p=0.04multiple rupture sites, p=0.04•• CaCa++++ in 55%, in 55%,
•• arc=36arc=36±±±±±±±±4747°°°°°°°°•• located at the base of the located at the base of the
rupture in 86%rupture in 86%•• Tear in fibrous cap identified Tear in fibrous cap identified
in 59%,in 59%,•• at shoulder of plaque in 68% at shoulder of plaque in 68%
in center of plaque in 32%in center of plaque in 32%•• Multiple rupture sites in 14% Multiple rupture sites in 14%
of ACS patientsof ACS patients
Asymptomatic
Stable anginaPeri MI
USA 11%11%11%11%
32%32%
46%46%
The frequency of stable angina or The frequency of stable angina or no symptoms in patients with no symptoms in patients with plaque rupture suggests that plaque rupture suggests that asymptomatic rupture and healing asymptomatic rupture and healing are common and may be one of the are common and may be one of the mechanisms of progression of CADmechanisms of progression of CAD
Maehara Maehara et al J Am et al J Am Coll Cardiol Coll Cardiol 2002;40:9042002;40:904--1010

5511Simple lesions Simple lesions (smooth surface (smooth surface w/o thrombus)w/o thrombus)
2288Complex lesions Complex lesions (irregular surface (irregular surface ±±±±±±±±thrombus)thrombus)
Negative Remodeling
(Lesion EEM<0.95 Reference)
Positive Remodeling
(Lesion EEM>1.05 Reference)
Smits Smits et al.et al. Cardiovasc Res Cardiovasc Res 1999;41:4581999;41:458--464464p=0.035p=0.035
22 patients with single de novo lesions studied using angioscopy and IVUS showed a
relationship between thrombus and remodeling
22 patients with single de novo lesions studied using angioscopy and IVUS showed a
relationship between thrombus and remodeling

0102030405060708090
100
Positive Negative
Frequency of Plaque RuptureFrequency of Plaque Rupture Frequency of ThrombusFrequency of Thrombus
Gyongyosi Gyongyosi et al. Heart 1999;82:68et al. Heart 1999;82:68--7474
Remodeling Remodeling
Culprit Lesion Morphology vs Remodeling in 60 Patients with Unstable Angina
Culprit Lesion Morphology vs Remodeling in 60 Patients with Unstable Angina
Intermediate Intermediate0
102030405060708090
100
Positive Negative

Remodeling vs plaque compositionRemodeling vs plaque composition
0
0.2
0.4
0.6
0.8
1
1.2Remodeling indexRemodeling index
00 11 22 00 11 22
IVUS & histology in 29 patients IVUS & histology in 29 patients (17 stable angina, 12 ACS) (17 stable angina, 12 ACS)
treated with DCAtreated with DCA
Inflammatory Inflammatory cellscells
Lipid scoreLipid score
Uemura Uemura et al. ACC 2003et al. ACC 2003
Remodeling indexRemodeling index
IVUS & OCT in 82 lesions in 50 IVUS & OCT in 82 lesions in 50 patientspatients
Mac Neill et al. ACC 2003Mac Neill et al. ACC 2003
**Remodeling also correlated with Remodeling also correlated with quadrants of lipid (p=0.001)quadrants of lipid (p=0.001)
0
0.2
0.4
0.6
0.8
1
1.2
Lipidrich*
Mixed Fibrous

CaCa++ ++ CSA (%)CSA (%)
Lipid CSA (%)Lipid CSA (%)
Maximal stress (Maximal stress (kPakPa))
Stable(n=10)
Ruptured(n=10)
p
4.14.1
14.114.1
286286
5.45.4
2.82.8
458458
0.40.4
0.30.3
0.0380.038
Calcium Lipid
When fibrous plaque was When fibrous plaque was replaced with calcium, stress replaced with calcium, stress changed insignificantly changed insignificantly (p=0.85). In contrast, stress (p=0.85). In contrast, stress decreased by 26% (p=0.02) decreased by 26% (p=0.02) when lipid was replaced with when lipid was replaced with fibrous plaque. fibrous plaque.
x=stablex=stablex=rupturedx=ruptured
x
xxx
xxxxx
x
xxxx
x xxxx
00
16001600
00 3030
x
xx
xx
xxx
x x
x
xxxxx
xxxx
6060
16001600
0000
kPakPa kPakPa
% % area of calciumarea of calcium % % area of lipidarea of lipid
p=NSp=NS p=0.024p=0.024
Calcium Does Not Increase the Biomechanical Calcium Does Not Increase the Biomechanical Instability of Atherosclerotic Plaques!Instability of Atherosclerotic Plaques!
Huang. Circulation 2001;103:1051Huang. Circulation 2001;103:1051--66

0 600
1.0
Square Root of Calcium Score
Specificity
Sensitivity
0 600
1.0
Square Root of Calcium Score
Specificty
Sensitivity
Specificity
Sensitivity
MACE (n=1172)MACE (n=1172)
Death/MI (n=1172)Death/MI (n=1172)
Arad Arad et al. J Am et al. J Am Coll Cardiol Coll Cardiol 2000;36:12532000;36:1253--6060
0
100
200
300
400
500
600
700
0 10 20 30 40 50 60
# with no events(n=1155)
# with events(n=18)
Arad Arad et al. Circulation 1996;93:1951et al. Circulation 1996;93:1951--33
Square Root of Calcium Score
0
1
2
3
4
6
7
5
0
100
200
300
400
500
600
700
Multiple studies have shown that EBCT calcium score predicts acute coronary events at 1 year follow-up
Multiple studies have shown that EBCT calcium score predicts acute coronary events at 1 year follow-up

Important IVUS Observations: Calcium
Important IVUS Observations: Calcium
••If calcium is uncommon in ACS lesions and If calcium is uncommon in ACS lesions and if calcium does not affect plaque vulnerability if calcium does not affect plaque vulnerability and instability, why does the EBCT calcium and instability, why does the EBCT calcium score predict acute events?score predict acute events?

Volumetric IVUS analysis of 19 RCA's with 1 or 2 focal de novo stenoses
Volumetric IVUS analysis of 19 RCA's with Volumetric IVUS analysis of 19 RCA's with 1 or 2 focal de novo1 or 2 focal de novo stenosesstenoses
020
4060
80100
120140
160180
0 250 500 750 1000<0.0001<0.000133.4 33.4
±±±±±±±±13.513.59.4 9.4 ±±±±±±±±7.67.6Length (mm)Length (mm)
<0.0001<0.0001231 231 ±±±±±±±±14014090 90 ±±±±±±±±8686P&MP&M vol vol (mm(mm33))
<0.0001<0.0001228 228 ±±±±±±±±15615629 29 ±±±±±±±±3030LumenLumen vol vol (mm(mm33))
<0.0001<0.0001459 459 ±±±±±±±±283283119 119 ±±±±±±±±111111EEMEEM vol vol (mm(mm33))
pNon-
Stenotic Segment
Lesion r=0.57, p=0.011r=0.57, p=0.011
Volumetric index of total calcium
Total plaque volume (mm3)7272±±±±±±±±12% 12% of the plaque volume (range 46of the plaque volume (range 46--86%) 86%) is in is in nonstenotic nonstenotic segments. Plaque volume segments. Plaque volume
l t ith l il t ith l iTinana Tinana et al. Am J et al. Am J Cardiol Cardiol 2002;89:7572002;89:757--6060

ProximalProximal 33mmmm00 1212mmmm
EEM CSA = 21.0mmEEM CSA = 21.0mm22
Lumen CSA = 9.5mmLumen CSA = 9.5mm22
P+M CSA = 11.5mmP+M CSA = 11.5mm22
EEM CSA = 23.5mmEEM CSA = 23.5mm22
Lumen CSA = 5.5mmLumen CSA = 5.5mm22
P+M CSA = 18.0mmP+M CSA = 18.0mm22
EEM CSA = 13.7mmEEM CSA = 13.7mm22
Lumen CSA = 9.3mmLumen CSA = 9.3mm22
P+M CSA = 4.4mmP+M CSA = 4.4mm22

11mmmm 44mmmm00

22mmmm 66mmmm00

Important IVUS Observations: Lumen Compromise
Important IVUS Observations: Lumen Compromise
••What separates lesions with What separates lesions with asymptomatic plaque rupture from asymptomatic plaque rupture from plaque ruptures that cause acute plaque ruptures that cause acute symptoms?symptoms?

Clinical Follow up in 357 intermediate lesions in 300 pts deferred intervention after IVUS imaging
Clinical Follow up in 357 intermediate lesions in 300 pts deferred intervention after IVUS imaging
•• Independent predictors of death/MI/TLR was IVUS MLA (p=0.0041)Independent predictors of death/MI/TLR was IVUS MLA (p=0.0041)•• Independent predictors of TLR were DM (p=0.0493) and IVUS MLA (pIndependent predictors of TLR were DM (p=0.0493) and IVUS MLA (p=0.0042)=0.0042)•• Although the number of patients with death and MI was small (n=6Although the number of patients with death and MI was small (n=6), the only ), the only
independent predictor was IVUS MLD (p=0.0498).independent predictor was IVUS MLD (p=0.0498).
IVUS MLD (mm)IVUS MLD (mm)
QCA MLD (mm)QCA MLD (mm)
00
11
22
33
44
00 11 22 33 44
r=0.339r=0.339
IVUS MLA (mm2)IVUS MLA (mm2)
Death/MI/TLRDeath/MI/TLR
22--33 33--44 44--55 ≥≥≥≥≥≥≥≥550
5
10
15
20
25
30
35
0
5
10
15
20
25
30
35
IVUS MLA (mm2)IVUS MLA (mm2)
TLRTLRDMDMno-DMno-DM

Risk of MIRisk of MI
• 29 patients had a newly occluded artery• In 19 pts, the artery
previously had a <50% DS• In only 10 pts the
occlusion was at the site of the most severestenosis
•• 29 29 patients had a newly patients had a newly occluded arteryoccluded artery•• In 19 pts, the artery In 19 pts, the artery
previously had a <50% DSpreviously had a <50% DS•• In only 10 pts the In only 10 pts the
occlusion was at the occlusion was at the site of the most severesite of the most severestenosisstenosis 0
24
68
1012
141618
0-49 50-69 70-89 90-98
42 42 Consecutive Pts with Consecutive Pts with Angiography Both Angiography Both
Before and After MIBefore and After MI
Little et al. Circulation 1988;78:1157Little et al. Circulation 1988;78:1157--6666
""Because the aggregate risk of rupture associated with many nonBecause the aggregate risk of rupture associated with many non--significant lesions significant lesions (each with an(each with an admitedly admitedly lower individual risk potential) exceeds that of the fewer lower individual risk potential) exceeds that of the fewer significant lesions, an MI will more likely originate from asignificant lesions, an MI will more likely originate from a nonsignificant nonsignificant lesion."lesion."
Kern and Meier. Circulation 2001;103:3142Kern and Meier. Circulation 2001;103:3142--99
118 118 Pts in CASS after Pts in CASS after Baseline AngiographyBaseline AngiographyRisk of Anterior MI within 3 years (%)Risk of Anterior MI within 3 years (%)
Baseline QCA DS (%)Baseline QCA DS (%)Ellis et al. J AmEllis et al. J Am Coll Cardiol Coll Cardiol 1988;11:9081988;11:908--1616

Comparison of Culprit and Non-Culprit Rupture Sites in ACS Patients with Rupture Sites in Non-ACS Patients
Comparison of Culprit and Non-Culprit Rupture Sites in ACS Patients with Rupture Sites in Non-ACS Patients
0.5
0.6
0.7
0.8
0.9
1
1.1
1.2
1.3
Rupture SiteRemodeling Index
0
10
20
30
40
50
60
70
Thrombus (%)0
1
2
3
4
5
6
7
Minimum LumenArea
p=0.001p=0.001 p=0.001p=0.001 p=0.001p=0.001
ACS Culprit Plaque ACS Culprit Plaque Ruptures (N=35)Ruptures (N=35)
ACS NonACS Non--Culprit Plaque Culprit Plaque Ruptures (N=20)Ruptures (N=20)
NonNon--ACS Plaque ACS Plaque Ruptures (N=27)Ruptures (N=27)
(mm2)
Independent predictors of ACS were MLA and thrombus (both p=0.01Independent predictors of ACS were MLA and thrombus (both p=0.01))
Fuji et al. Unpublished ObservationsFuji et al. Unpublished Observations

Limitations of IVUSLimitations of IVUS••Measurement of fibrous capMeasurement of fibrous cap
HistologicHistologic studies suggest that studies suggest that the fibrous cap in vulnerable the fibrous cap in vulnerable plaques measures <65 micronsplaques measures <65 micronsIVUS resolution is >100 micronsIVUS resolution is >100 microns
••Assessment of plaque compositionAssessment of plaque composition

IVUS Can Measure Fibrous Cap IVUS Can Measure Fibrous Cap Thickness In Vitro, but NOT Thickness In Vitro, but NOT In VivoIn Vivo
Hiro Hiro et al. Circulation 2001;103:1206et al. Circulation 2001;103:1206--1111

Virtual Histology™Virtual Histology™
MHz
dB
Fibrous, Fibrofatty, Lipidic-necrotic, Calcium

Predictive Accuracies of Training and Test Datasets
Predictive Accuracies of Training and Test Datasets
TestTrainingTestTrainingTestTrainingTestTraining
Lipidic-Necrotic(n=70)
Calcified(n=50)
Fibro-Lipidic(n=56)
Fibrous(n=101)
85.585.592.892.889.589.590.990.981.281.292.892.879.779.790.490.4ARAR
72.582.686.591.876.892.366.788.9Welch
71.090.982.692.881.292.369.690.4FFT^2

Ex-Vivo Validation Virtual Histology™
Ex-Vivo Validation Virtual Histology™
Fibrous, Fibro-lipidic, Lipidic-necrotic, Calcium

Ex-Vivo Validation Virtual Histology™
Ex-Vivo Validation Virtual Histology™
Fibrous, Fibro-lipidic, Lipidic-necrotic, Calcium

What about IVUS compared with other invasive diagnostic modalities?
What about IVUS compared with other invasive diagnostic modalities?
++++PalpographyPalpography
++ThermographyThermography
++++++++OCTOCT
++++IVUS+Virtual IVUS+Virtual HistologyHistology
++++IVUSIVUS
•Safe•Validated
in vivo•Practical•Available
FunctionFibrous Cap
Plaque Composition
Structure

ConclusionsConclusions••Almost everything that we know about IVUS and vulnerable plaque Almost everything that we know about IVUS and vulnerable plaque has come from extrapolating studies of IVUS in ACS has come from extrapolating studies of IVUS in ACS -- NOT from NOT from prospective correlative studiesprospective correlative studies••Culprit lesions in ACS are, Culprit lesions in ACS are, in general,in general, characterized bycharacterized by
••Positive remodelingPositive remodeling••HypoechoicHypoechoic, eccentric, ruptured plaques with evidence of thrombus, eccentric, ruptured plaques with evidence of thrombus••With a complex interaction between remodeling and plaque composiWith a complex interaction between remodeling and plaque composition tion and instability in ACS.and instability in ACS.
••Positive remodelingPositive remodeling••Prevents lumen compromisePrevents lumen compromise••"Paradoxically" may contribute to ACS and to MACE after PCI"Paradoxically" may contribute to ACS and to MACE after PCI••May be less common in diabetics with ACSMay be less common in diabetics with ACS
••Negative remodelingNegative remodeling••Contributes to lumen compromise Contributes to lumen compromise ••Probably can occur both early and lateProbably can occur both early and late
••Calcium is a marker of plaque mass, not a determinant of instabiCalcium is a marker of plaque mass, not a determinant of instabilitylity

But. . . But. . . ••The relationship between ACS/MI, positive remodeling, "vulnerabThe relationship between ACS/MI, positive remodeling, "vulnerable" le" plaques, and ruptured plaques may not be so simple.plaques, and ruptured plaques may not be so simple.
••Frequency of an MI is related to the severity of the underlyingFrequency of an MI is related to the severity of the underlying stenosisstenosis
••Not all pts with ACS/MI have positive remodelingNot all pts with ACS/MI have positive remodeling
••Not all pts with ACS/MI have plaque ruptureNot all pts with ACS/MI have plaque rupture
••Not all ruptured plaques cause ACS/MI. In some pts plaque ruptuNot all ruptured plaques cause ACS/MI. In some pts plaque rupture is re is asymptomatic and may be followed by healing, negative remodelingasymptomatic and may be followed by healing, negative remodeling, , calcification, and disease progression. In other patients the decalcification, and disease progression. In other patients the development velopment of a thrombus (superimposed on plaque rupture) decreased lumen of a thrombus (superimposed on plaque rupture) decreased lumen dimensions and results in ACS/MIdimensions and results in ACS/MI
••While the concept of using multiple complementary imaging While the concept of using multiple complementary imaging techniques may seem attractive, any clinical approach must be techniques may seem attractive, any clinical approach must be practical and safe.practical and safe.