Embed Size (px)
DESCRIPTION
Ivi strategicplan 2008
Citation preview




Contents
I. Institutional Vision and Mission
II. Executive Summary
III. Origins and Development of the IVI
IV. The Distinctive Contribution and Role of the IVI
V. The IVI’s Disease Priorities and Recent Achievements
VI. Remaining Gaps and Opportunities for Combating
Infectious Diseases Targeted by the IVI
VII. Proposed Program Development: 2008-2012
VIII. Maintaining a Strong Institution
4
5
11
13
18
22
28
46

Annexes
A. Signatories to the IVI Establishment Agreement
B. Board of Trustees of the IVI
C. The IVI’s Collaborators
D. Growth of the IVI
52
53
54
58

6
Institutional Vision and Mission | Executive Summary
I. Institutional Vision and Mission
IVI’s Mission
IVI’s Vision
The effective control of poverty-related infectious diseases in developing countries through the accelerated and sustainable introduction of new-generation vaccines
To combat infectious diseases through innovations in vaccine design, development and introduction, addressing the needs of people in developing countries

IVI Strategic Plan | 2008-2012
7
II. Executive Summary
Beginning in 1993 the United Nations Development Programme (UNDP) established the International Vaccine Institute (IVI) in the belief that there was a need for an international, public sector research organization in Asia that would address the development and utilization of new vaccines, specifically for people in developing countries. The IVI was formally established as an autonomous international organization in 1997, with the Republic of Korea as its host country. Its first Director General took up that post in 1999, and its laboratory programs started in 2003 with the opening of its headquarters building in Seoul, Republic of Korea.
The IVI focuses on vaccines against diseases that have a significant public health impact in developing countries, but whose development and/or introduction have received insufficient attention. To date, the Institute has targeted vaccines against specific diseases affecting the poorest populations, which in aggregate cause more than four million deaths annually:
• Diarrheal and enteric diseases, including cholera, typhoid and paratyphoid fevers, shigellosis, and rotavirus;
• Respiratory infections and meningitis, caused by Haemophilus influenzae type b (Hib), pneumococcal disease (Streptococcus pneumoniae), and, more recently, influenza (seasonal and pandemic) and tuberculosis;
• Vector-borne viral diseases, namely dengue fever and Japanese encephalitis (JE).
In the past several years, the IVI has conducted major programs of “translational” field research on typhoid fever, cholera and dengue, establishing multi-country networks of field sites to generate evidence to inform policy decisions regarding the introduction of new or under-utilized vaccines. It has also conducted numerous epidemiological and economic studies to inform policy decisions on the use of vaccines against Japanese encephalitis, rotavirus, shigellosis and respiratory infections. In addition, the IVI has developed innovative methods for vaccine evaluation, including improved assessment of vaccine herd protection and of vaccine safety.
In undertaking these programs, which have taken place in 28 developing countries in Asia, Africa, and Latin America, the IVI has created a new paradigm to address the vaccination needs of developing countries. The new paradigm involves identifying the specific needs of developing country policymakers in making decisions about the introduction of new vaccines and responding to those needs proactively. The IVI’s approach is to provide – for a specific disease – full packages of evidence on disease burden, vaccine demand and acceptability, and the feasibility, impact and cost-effectiveness of vaccination. This approach is novel in its breadth, in its focus on providing evidence at the country level, in its emphasis on designing research in collaboration with local-level policymakers, and in its timing, as it is often initiated

8
Executive Summary
before a vaccine is licensed in order to avoid long delays between licensure and introduction in developing countries.
Using this paradigm, the IVI has generated evidence that has led to new global recommendations for the use of typhoid vaccines in endemic countries, as well as evidence that has influenced recent national decisions about introducing new vaccines against typhoid fever, Hib, and Japanese encephalitis.
During the past three years, the Institute has built a laboratory science program designed to complement and synergize with its downstream research activities, focusing, inter alia, on molecular microbiology, molecular vaccinology, immunology and vaccine product development. Although young, the laboratory program has already made several achievements, including the identification and molecular characterization of a new, more virulent form of cholera that has emerged in Africa and Asia; discovery of an entirely new way of delivering vaccines, sublingually; and development of three new or improved vaccines against cholera and typhoid fever (a reformulated killed whole-cell based oral cholera vaccine, a high-yield typhoid Vi vaccine and a Vi-diphtheria toxoid conjugate vaccine), with transfer of these vaccines to emerging producers in developing countries.
The combination of downstream and laboratory research programs and capacities has given the IVI in-house capabilities along the entire vaccine continuum – from vaccine discovery to vaccine introduction, or from “bench to community”.
Recognizing that the gains made possible by the IVI’s research are sustainable only if the research is complemented by developing and strengthening the skills of developing country professionals, training and capacity-building have assumed great importance in all of the IVI’s programs. In addition, the IVI organizes stand-alone courses for developing country professionals, including an annual week-long advanced vaccinology course.
To make these programs and achievements possible, the IVI has grown rapidly, and now has a staff of more than 140 persons and an annual budget of $28 million.
Proposed Program Development
As a result of the accomplishments described above, the IVI is now recognized as a leading global partner in the development and deployment of vaccines against cholera, typhoid fever, and dengue fever, as well as in sublingual immunization. The Institute is also a valuable global contributor in the other areas in which it is engaged. This third Strategic Plan, for the period 2008-2012, builds upon the activities described above to achieve or further advance the introduction of needed vaccines into developing countries.
IVI Strategic Plan | 2008-2012
9
In developing the third Strategic Plan, the Board of Trustees and Director General were guided by the following principles:
• Addressing vaccines for diseases disproportionately affecting developing countries1;
• Ensuring that the IVI’s activities complement and create synergies with those of other organizations addressing new vaccines for the world’s poorest people;
• Building on the IVI’s achievements and areas of excellence as the fastest way to ensure public health impact from its efforts;
• Exploiting the Institute’s multi-faceted technical expertise to enhance laboratory-to-field linkages and to ensure cohesiveness in its activities along the vaccine ‘bench to community’ continuum;
• Expanding the IVI’s programmatic activities, particularly in the policy area;
• Extending the IVI’s activities geographically, particularly in sub-Saharan Africa, and, where appropriate, in Latin America; and
• Enhancing the sustainability of the IVI’s activities for developing countries by building training and capacity-strengthening activities for developing country vaccine professionals and institutions into all programs.
All of the IVI’s planned activities fall under the following six strategic objectives that fit into the “bench to community” continuum:
Vaccine Design:• To design new or improved vaccines and routes of delivery;
Vaccine Development:• To enhance the availability of an adequate, affordable and high-quality vaccine
supply through development of manufacturing processes and quality control procedures and assays, technology transfer and regulatory support;
• To conduct clinical assessments of vaccine candidates to establish safety, immunogenicity and efficacy, including, where necessary, the development of improved immunological and diagnostic assays for use in the clinical assessments;
Vaccine Introduction:• To generate evidence to guide rational vaccine introduction of new and under-
utilized vaccines in developing countries;
1 Recognizing that these might also have benefit for middle income and sometimes industrialized countries.

10
Executive Summary
• To accelerate vaccine introduction through data synthesis, analysis and dissemination;
Capacity-Building:• To increase the capacity of professionals in developing countries in vaccine
development, introduction and manufacturing through programs of training, technology transfer and technical assistance, and through conferences and seminars.
Disease-specific programs
The current plan envisions continuing work on vaccines for which the IVI has already launched research programs. Selected highlights for the next five years of proposed research on diseases in which IVI is a leading global partner include:
• Typhoid fever: The IVI will address remaining gaps in global capacity to successfully control typhoid and other enteric fevers by completing technology transfer and licensure of the high-yield Vi polysaccharide and Vi-diphtheria toxoid conjugate vaccines by high-quality developing country producers; developing a pan-enteric fever vaccine against typhoid and paratyphoid fevers in the IVI laboratories; conducting disease burden and other studies to generate evidence for policy in Africa and Central Asia, where such evidence is currently lacking; and conducting data synthesis and information dissemination activities, including preparation of a global investment case, to accelerate the adoption of new global recommendations for vaccination against typhoid fever in endemic countries.
• Cholera: The IVI will complete the technology transfer to qualified emerging producers and assist with clinical studies for licensure of the improved oral killed whole-cell (WC) cholera vaccine developed by the IVI, and will complete the clinical development program for the single-dose live oral Peru-15 vaccine candidate. The program will also provide additional evidence to inform policy decisions about the use of cholera vaccines to control epidemic and endemic cholera, including preparing a global investment case to support a recommendation for cholera vaccination in affected countries, and will continue upstream research into novel WC-based vaccines.
• Dengue fever: The Pediatric Dengue Vaccine Initiative (PDVI) will develop improved diagnostic and immunological assays for the clinical evaluation of dengue vaccines, working with external partners; conduct large-scale clinical studies of leading dengue vaccine candidates in field sites developed by the IVI; conduct disease burden, economic and other studies in Asia and Latin America to inform policy; and prepare a global investment case for the use of dengue vaccines in developing countries.

IVI Strategic Plan | 2008-2012
11
For other diseases for which the IVI is a global contributor (rotavirus, shigellosis, respiratory illnesses and meningitis, and Japanese encephalitis), the IVI will continue to conduct downstream research to gather epidemiological, economic and other evidence to support the introduction of vaccines against these diseases, with a focus on the Asia-Pacific region. Exploiting the opportunities created by the Biosafety Level (BSL) 3+ laboratory now being refurbished in the IVI headquarters building, the Institute will also pursue new programs addressing tuberculosis and emerging respiratory viruses, including avian influenza.
Cross-cutting programs
In addition to disease-specific activities, the IVI will continue its work on cross-cutting laboratory and downstream research activities, as follows:
• Vaccine design: The IVI will further develop the four innovative platforms that it has established: a) a genotyping platform the dedicated to genotypic analysis of pathogens isolated in the IVI’s field research programs; b) a novel genomic discovery platform, making use of the IVI’s genotyping studies as well as available genomic databases, for identifying protective antigens (e.g., common proteins) of bacterial pathogens; c) the sublingual delivery platform for immunization; and d) new enterotoxin-based adjuvants, especially for vaccines delivered via mucosal tissue.
• Clinical assessment of vaccines: The IVI will continue the development of new methods for assessing vaccine safety (using large-linked databases) and vaccine protection (including measuring herd protection), as well as improved immunoassays to evaluate immune responses to vaccines in children and to predict the duration of protection (immune memory) in developing country vaccine evaluations.
• Improved support to policy formulation for new vaccine introduction: The IVI will create a Policy Unit devoted to generating, synthesizing and disseminating better evidence to inform vaccine policy decisions in developing countries and to building capacity at the country level in the use of this evidence. This will include developing “best practices” to support policy decisions and developing model approaches for the preparation of global vaccine investment cases.
Capacity-building in vaccine sciences for developing countries
The IVI will continue to conduct courses, workshops, and hands-on training devoted to vaccine development, introduction and production in developing countries. These activities will be enhanced and expanded by the availability of the Institute’s recently refurbished BSL3+ laboratory and a new vaccine production training facility at the

12
Executive Summary | Origins and Development of the IVI
IVI headquarters. The IVI also plans to establish a post-graduate degree-conferring training program in vaccinology and to provide additional opportunities for young scientists to receive pre- and post-doctoral training in the IVI laboratories.
Maintaining a strong institution
Under this third Strategic Plan, the IVI will continue to expand as an international institution with increases in staff, facilities, and budget. This expansion will require continued management support to ensure compliance in the areas of security management, facilities maintenance, biosafety monitoring, contractual obligations, and ethical research standards. Risk assessment and management will also be expanded in these areas.
The IVI also aims to increase and diversify its funding base, for both unrestricted (core) and project-related funds, and to increase its public awareness activities both internationally and within Korea. As part of these efforts, the Institute will strive to obtain the signature of additional countries to the IVI Establishment Agreement, with a particular focus on industrialized countries, and will explore the possibility of obtaining funding commitments from signatory countries.
The headquarters of the IVI on the campus of Seoul National University in Seoul, the Republic of Korea

IVI Strategic Plan | 2008-2012
13
III. Origins and Development of the IVI
The IVI’s Constitution stipulates two main aims of the Institute:
1. To undertake and promote study, research, development and dissemination of knowledge in the vaccine-relevant sciences and directly related areas of public health, management sciences and technology to generate affordable and effective means to prevent death and disability arising from infectious diseases and, thereby, to improve the health status and general welfare of children and low income people; and
2. To provide, in collaboration with relevant national and international institutions, facilities and training programs aimed at strengthening expertise and capacity...to conduct work in the areas of the Institute’s interest and competence.
The IVI has grown steadily since 2003, when the last Strategic Plan was prepared. The IVI headquarters building, which includes 20,000 square feet of research laboratory space, opened that year, resulting in the launch of the Laboratory Sciences Division. The IVI has developed field research projects in 28 countries in Asia, the Americas and Africa. Its budget has more than doubled – from around $11 million in
The IVI’s refurbished Biosafety Level (BSL) 3+ laboratories will enable the Institute to advance its work on vaccines against tuberculosis, avian influenza and other dangerous pathogens.
Beginning in 1993 the United Nations Development Programme (UNDP) established the International Vaccine Institute (IVI), as an outgrowth of the Children’s Vaccine Initiative. The UNDP and others shared the belief that there was a need for an international, public sector research organization in Asia that would address the development and utilization of new vaccines, specifically for people in developing countries. The Republic of Korea was selected as the host for the IVI by an independent site selection committee in mid-1994. In 1995, the IVI was provided temporary facilities on the campus of Seoul National University (SNU), while its permanent headquarters was being constructed in SNU’s Research Park. The Institute became an independent, international organization established under the Vienna Convention of 1969 when its Establishment Agreement went into effect in 1997. At that time 12 countries and the World Health Organization had become signatories to the Establishment Agreement. The inaugural meeting of the Board of Trustees was held in October 1997 and the Institute’s first Director General, Dr. John Clemens, began his first term in 1999.
The Institute became
an independent
international
organization in
1997.

14
Origins and Development of the IVI | The Distinctive Contribution and Role of the IVI
2003 to more than $25 million in 2007, and its staff has grown by almost 90% between 2003 and 2007 – from 74 to over 140.
The two preceding IVI Strategic Plans, covering 1997- 2001 and 2002-2007, focused on developing the Institute by establishing and utilizing the capabilities required to address the priority diseases and vaccination needs of developing countries, as described in subsequent sections of this document. Further evolution of the IVI’s activities and use of additional capacities, such as the recently refurbished Biosafety Level (BSL) 3+ laboratories and a production training facility, which will become operational under this third Strategic Plan, will be guided by the same philosophy, namely placing emphasis on the needs of – and empowering – developing countries to better control their infectious disease threats through the appropriate deployment of new-generation vaccines.
The IVI has had programs in 28 countries (as of March 2008)
IVI Strategic Plan | 2008-2012
15
IV. The Distinctive Contribution and Role of the IVI
A. The IVI’s contribution to the U.N. Millennium Development Goals
At the United Nations Millennium Summit in September 2000, world leaders adopted eight Millennium Development Goals (MDGs), which set clear targets to significantly improve the human condition by 2015 by reducing poverty, hunger, disease, illiteracy, environmental degradation, and discrimination against women. The IVI’s work supports four of the MDGs, as follows:
Millennium Development Goal 1, “Eradicate extreme poverty and hunger”. By preventing unnecessary deaths from infectious diseases and allowing people, especially children, to lead healthier lives, the IVI contributes to alleviating poverty and strengthening economies.
Millennium Development Goal 4, “Reduce child mortality” and Millennium Development Goal 6, “Combat HIV/AIDS, malaria and other diseases”. The research programs at the IVI contribute to the target of reducing the under-five mortality rate by two-thirds between 1990 and 2015, by developing and/or accelerating the use of new and under-utilized vaccines against diarrhea and enteric infections, respiratory and central nervous system infections, and vector-borne viral diseases. Together these diseases claim the lives of over four million persons each year, most of whom are children living in impoverished conditions in developing countries.
Millennium Development Goal 8, “Develop a global partnership for development”. The mission of the IVI is to develop and accelerate the introduction of new vaccines at affordable prices into public health programs of developing countries. The IVI facilitates transfer of vaccine technologies to producers in developing countries to create cost-effective vaccines for the world’s poor. The Institute also provides training and technical assistance in the clinical evaluation of vaccines and in vaccine production and regulation to professionals in developing countries.
B. Establishment of a new paradigm to address the vaccination needs of developing countries
Beginning in 1999, the IVI has created a new paradigm to meet the needs of developing countries in making decisions about the introduction of new vaccines to control infectious diseases. Historically, new vaccines have been developed and tested primarily for industrialized country markets, and it has often taken decades for new vaccines to be introduced into developing country immunization programs.
The new paradigm, first developed by the IVI for its Diseases of the Most Impoverished (DOMI) Program, involves identifying the specific needs of developing country policymakers in making decisions about the introduction of new vaccines
The IVI’s work
supports four of
the Millennium
Development Goals.

16
The Distinctive Contribution and Role of the IVI
(through policymaker surveys) and responding to those needs proactively. The IVI’s approach is to provide – for a specific disease – full packages of evidence on disease burden, vaccine demand and acceptability, and the feasibility, impact and cost-effectiveness of vaccination (see figure below). This approach is novel in its breadth, in its focus on providing evidence at the country level, in its emphasis on designing the research in collaboration with local policymakers, and in its timing, as it is often initiated before a vaccine is licensed in order to avoid long delays between licensure and introduction in developing countries.
A new paradigm to generate evidence for policy decisions on the introduction of new and under-utilized vaccines
Rational and sustainable vaccine introduction
Reduced disease burden
Data synthesis
(cost-effectiveness
and
impact analyses),
dissemination and advocacy
Data synthesis (cost-effectiveness
andimpact analyses),
dissemination and advocacy
Rational and sustainable vaccine introduction
Rational and sustainable vaccine introduction
Cost-of-illnessstudies
Diseasesurveillance
studies
Policymaker surveys
Pre- and post-licensure
clinical trials& vaccine
demonstrations
Market demandsurveys
Socio-cultural surveys
Economicstudies
Diseasesurveillance
studies
Policymaker surveys
Pre- and post-licensure
clinical trials& vaccine
demonstrationsMarket demand
surveys
Socio-cultural surveys
The IVI’s success in establishing this new paradigm for addressing developing country needs is the result of its mandate and a special set of attributes, assets, and operating strategies.
C. The IVI’s special mandate, attributes and assets
A unique international mandate
The IVI’s legal status as an international, politically-independent organization with 40 countries and the World Health Organization as signatories to its Establishment
The IVI has created
a new paradigm
to address the
vaccination needs
of developing
countries.

IVI Strategic Plan | 2008-2012
17
Agreement provides international legitimacy to the Institute. This has allowed it to establish strong links and networks with a broad range of collaborators world-wide, including government agencies, private companies and non-profit organizations.
Among international organizations the IVI has a unique constitutional mandate to work exclusively on vaccine development and introduction, specifically for people in developing countries. This focus allows the Institute to attract and build extensive, highly motivated expertise in a broad range of vaccine-related areas.
The mandate also encourages the IVI to deal with a diverse portfolio of target diseases and vaccines. This not only facilitates operational efficiencies, cross-fertilization and synergies, but also enhances the Institute’s credibility as an impartial source of information, advice and assistance.
The IVI’s special attributes and assets • In-house capabilities and expertise that span the entire “bench to community”
continuum. Since the opening of the IVI laboratories in 2003, there now co-exists within the Institute skills and facilities in laboratory sciences, vaccine production, and field research (including epidemiology, vaccine evaluation, economic and socio-behavioral research) that cover the entire vaccine design – development – introduction continuum (see figure on p.16). The laboratories have focused on designing new and improved vaccines for poverty-related diseases; developing needle-free methods of vaccine administration to make vaccination safer, easier and less costly; and developing improved immunoassays for use in vaccine trials in developing countries. The IVI is also developing and transferring to qualified producers in developing countries production technologies for vaccines against neglected diseases predominantly affecting the poor, to ensure a reliable supply of affordable, yet high-quality vaccines. In addition, soon-to-be-completed facilities, such as the Biosafety Level 3+ laboratory and the planned vaccine production training facility, will enable the Institute to conduct unique research and training in-house that would be difficult to contract at a distance.
• Cross-fertilization and synergies created by this broad range of in-house capabilities. The IVI’s surveillance studies and vaccine clinical trials have benefited from the development in the IVI laboratories of improved diagnostics and immunoassays. Conversely, discoveries from IVI field studies, such as the demonstration of great geographic and temporal variations in the distribution of Shigella strains, have stimulated the design of vaccines using novel approaches, such as the discovery of common proteins across Shigella species and serotypes that could lead to a pan-Shigella vaccine. These synergies would be more difficult to achieve if these capabilities did not exist in-house.
• A nimble management structure that allows the Institute to rapidly initiate and efficiently conduct large, innovative programs, such as the Diseases of the Most Impoverished (DOMI) Program (vide infra).
Among international
organizations,
the IVI has a
constitutional
mandate to work
exclusively on
vaccine development
and introduction.

18
The Distinctive Contribution and Role of the IVI
RATIONAL AND SUSTAINABLE VACCINE INTRODUCTION
VACCINE DISCOVERY& DESIGN
• Genotyping of pathogens
• Novel antigens
• Novel adjuvants
• New delivery mechanisms
• New routes of administration
RESEARCH TOGENERATE EVIDENCE
FOR POLICY
• Collection of epidemio- logical, economic & socio-behavioral data
• Studies of vaccine feasibility, acceptance & field effectiveness
• Data synthesis (cost- effectiveness and impact analyses) and dissemination
VACCINEDEVELOPMENT
• Laboratory process development
• Assay development (immuno-monitoring)
• Technology transfer for large-scale production
• Clinical trials
The IVI’s in-house capabilities and activities along the “bench to community” continuum
• High-quality staff in all facets of vaccine research, development and introduction, selected for their potential to be specialists and innovators in their respective disciplines, as well as capable managers;
• Strong support, both moral and financial, from the host country government of the Republic of Korea;
• Proximity to a rapidly growing biotechnology community in Korea and to prestigious Korean academic and research institutions that facilitate and enhance the IVI’s research and training activities.
D. The IVI’s operating strategies
The IVI conducts its programs following several operating strategies:
• A coordinated, multi-country approach towards research to enable policymakers to judge whether the results are applicable to entire regions or even globally;
• A strategy of working closely with governments, particularly Ministries of Health, in developing countries, rather than solely with academic or independent research groups, to engender a sense of local ownership of the research and to enhance the likelihood of government action based on the research results;
• A focus on capacity-building in all of its activities;
The IVI has in-
house capabilities
that span the entire
‘bench to community’
continuum.

IVI Strategic Plan | 2008-2012
19
• A commitment to conduct comprehensive due diligence to select partner vaccine producers in order to ensure that the technology transfer of vaccines to developing country manufacturers leads to the sustainable production of these vaccines, including the selection of producers only in countries with national regulatory authorities accredited by WHO;
• Respect for intellectual property rights (IPR) and their proactive management to ensure access to products for poorer populations.
E. The IVI’s synergy and complementarity with other players in the global vaccine community
While the IVI has a significant set of attributes and assets that contribute to its ability to pursue its mandate effectively, it operates in concert with a wide range of other players in the global vaccine community, in order to achieve both synergy and complementarity. The IVI works closely with the World Health Organization at the global, regional and country levels. At the country level, the IVI has forged close working relationships with national and local governments, including Ministries of Health, and with both government and private research institutes.
In addition, the IVI collaborates extensively with a number of new players that have emerged at the international level in recent years. These include the GAVI Alliance, a range of accelerated vaccine introduction programs (e.g., the Rotavirus Vaccine Program, PneumoADIP), and a number of vaccine-oriented product development partnerships (PDPs).
A list of organizations with which the IVI has collab-orated is shown in Annex C. The IVI’s collaboration with emerging developing coun-try producers and regulators is noteworthy. In transferring vaccine production technolo-gies to developing countries, the IVI frequently works with members of the Developing Country Vaccine Manufac-turers Network (DCVMN), an organization of emerging producers that are committed to manufacturing high-quality vaccines for developing country populations. And in seeking to establish regulatory pathways for new or under-utilized vaccines, the IVI collaborates with the recently-created Developing Country Vaccine Regulators Network (DCVRN).
Director-General Dr. John Clemens with pre-school children in the Democratic People’s Republic of Korea, where the IVI has a program of training and research to set the stage for introducing modern vaccines against Haemophilus influenzae type b (Hib) and Japanese encephalitis (JE).
The IVI operates
in concert with a
wide range of other
players in the global
vaccine community.

20
B. Achievements during the past five years
The Second IVI Strategic Plan, for 2003-2007, outlined a broad agenda of laboratory and field research on a range of pathogens. Among recent major accomplishments arising from that agenda are the following:
Vaccine design
• Discovery of new protein anti-gens that protect across Shigella species and serotypes in the aim of developing a common protein vaccine against different strains of shigellosis (bacterial dysentery). This work was stimulated by the IVI’s disease surveillance studies in Asia that revealed complex geographic and temporal patterns of Shigella species and sero-type distributions, complicating the development of multivalent vaccines;
• Demonstration of the safety and immunogenicity of vaccine delivery via the sublingual route, which could lead to the development of safe, low-cost, effective, needle-free vaccines attractive to developing countries;
The IVI’s Disease Priorities and Recent Achievements
V. The IVI’s Disease Priorities and Recent Achievements
A. The IVI’s disease priorities
The IVI has chosen to work on vaccines against diseases that have a significant public health impact in developing countries, but whose development and/or introduction are otherwise receiving insufficient attention. To date, the Institute has targeted vaccines against several diseases: a) diarrheal and other enteric diseases, b) respiratory infections and meningitis; and c) vector-borne viral diseases.
The IVI is now recognized as a leading global partner for vaccines against typhoid fever, cholera and dengue fever, and is a significant global contributor for vaccines against rotavirus diarrhea, shigellosis, respiratory pathogens (Haemophilus influenzae type b (Hib), pneumococcal disease, influenza and tuberculosis), and Japanese encephalitis.
The IVI’s Current Disease Priorities
Diarrheal and other enteric diseases:• Cholera• Typhoid/paratyphoid fever• Shigellosis (bacterial dysentery)• Rotavirus
Respiratory infections and meningitis:• Haemophilus influenzae type b (Hib) • Pneumococcal disease• Influenza (seasonal and pandemic)• Tuberculosis
Vector-borne viral diseases: • Dengue fever• Japanese encephalitis
To date the IVI has
targeted several
diseases – diarrheal/
enteric diseases,
respiratory
infections and
meningitis, and
vector-borne viral
diseases.

IVI Strategic Plan | 2008-2012
21
The IVI is now
recognized as a
leading global
partner for vaccines
against typhoid
fever, cholera and
dengue fever.
• Identification of a newly-emergent, genetically distinct form of the El Tor biotype of cholera that expresses a classical biotype cholera toxin, causing a more clinically severe illness than the conventional El Tor biotype that preceded it, and that is now predominant in Asia and Africa;
• Discovery of a safe cholera toxin-based adjuvant that can be used to enhance the effectiveness of mucosal vaccines against a variety of pathogens.
Ms. Song Joo-Hye and Dr. Kweon Mi-Na working on the development of needle-free vaccines administered sublingually (under the tongue)
Vaccine development
• Development of three new or improved enteric vaccines: a reformulated, oral killed whole-cell cholera vaccine; a high-yield, low-cost typhoid Vi polysaccharide vaccine; and a typhoid Vi-diphtheria toxoid (DT) conjugate vaccine designed to be effective in infants – all of which are being transferred to qualified vaccine producers in developing countries;
• Design of the first animal model of Shigella colitis, which will greatly facilitate the development and testing of vaccines against shigellosis;
• Completion of clinical trials of vaccines against cholera, rotavirus, shigellosis, typhoid fever and Japanese encephalitis in developing countries of Asia and Africa;
• Development of prototype miniaturized assays (ELISPOT test) for measuring immune responses to mucosal vaccines in infants and young children, using very small quantities of blood.
22
The IVI’s Disease Priorities and Recent Achievements
Vaccine introduction
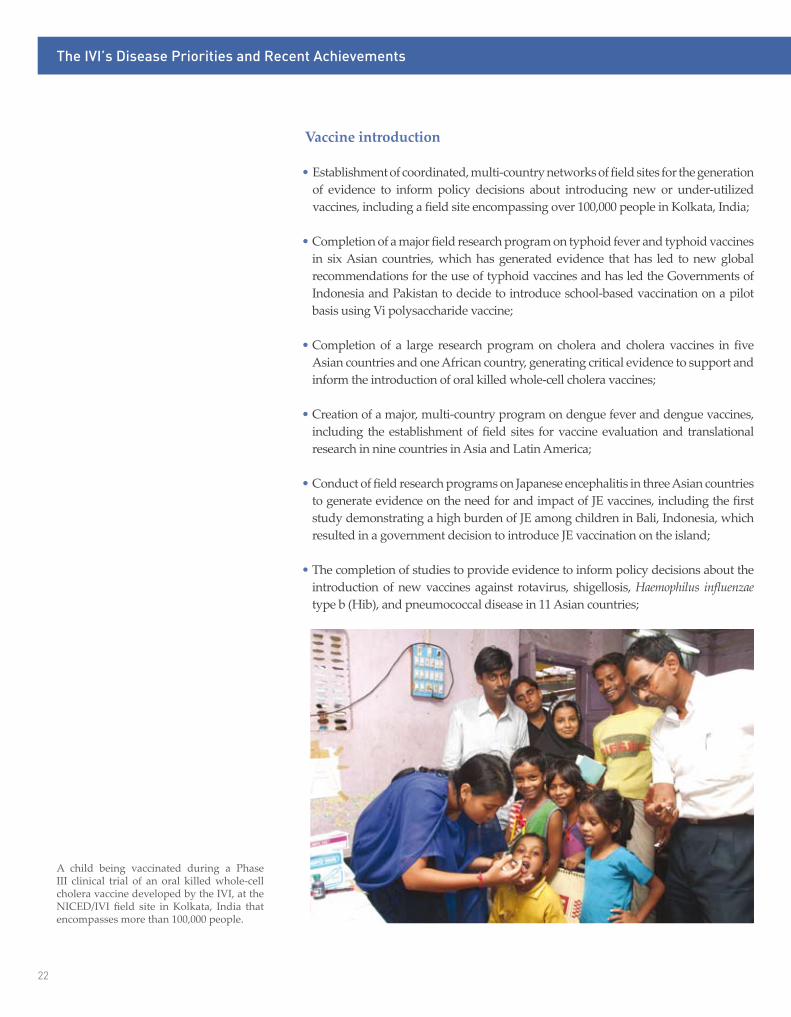
• Establishment of coordinated, multi-country networks of field sites for the generation of evidence to inform policy decisions about introducing new or under-utilized vaccines, including a field site encompassing over 100,000 people in Kolkata, India;
• Completion of a major field research program on typhoid fever and typhoid vaccines in six Asian countries, which has generated evidence that has led to new global recommendations for the use of typhoid vaccines and has led the Governments of Indonesia and Pakistan to decide to introduce school-based vaccination on a pilot basis using Vi polysaccharide vaccine;
• Completion of a large research program on cholera and cholera vaccines in five
Asian countries and one African country, generating critical evidence to support and inform the introduction of oral killed whole-cell cholera vaccines;
• Creation of a major, multi-country program on dengue fever and dengue vaccines, including the establishment of field sites for vaccine evaluation and translational research in nine countries in Asia and Latin America;
• Conduct of field research programs on Japanese encephalitis in three Asian countries to generate evidence on the need for and impact of JE vaccines, including the first study demonstrating a high burden of JE among children in Bali, Indonesia, which resulted in a government decision to introduce JE vaccination on the island;
• The completion of studies to provide evidence to inform policy decisions about the introduction of new vaccines against rotavirus, shigellosis, Haemophilus influenzae type b (Hib), and pneumococcal disease in 11 Asian countries;
A child being vaccinated during a Phase III clinical trial of an oral killed whole-cell cholera vaccine developed by the IVI, at the NICED/IVI field site in Kolkata, India that encompasses more than 100,000 people.

IVI Strategic Plan | 2008-2012
23
• Development of innovative methods for vaccine evaluation, including improved assessments of vaccine herd protection and of vaccine safety (using large-linked databases).
Capacity-building
• Establishment of the only international vaccinology course in the Asia-Pacific region given annually, through which more than 400 professionals from 30 countries have received a week-long, comprehensive overview of issues related to vaccine design, development, evaluation, production, regulation, introduction and policy;
• Training of numerous local researchers at IVI field sites in the areas of field epidemiology, Good Clinical Practice, clinical evaluation of vaccines, microbiological and immunological procedures, social science and economic research, and computerized data management;
• Training of manufacturers in India, Indonesia and Vietnam on Good Manufacturing Practice (GMP) and on production technologies for vaccines against cholera and typhoid fever.
The IVI is transferring the production technology for several enteric vaccines to high-quality producers in developing countries, including Shantha Biotechnics of Hyderabad, India. Pictured from left to right are: Dr. Aldo Tagliabue; Dr. Luis Jodar; Dr. John Clemens; Shantha President, Varaprasad Reddy; and Rodney Carbis.

24
Remaining Gaps and Opportunities for Combating Infectious Diseases Targeted by the IVI
VI. Remaining Gaps and Opportunities for Combating Infectious Diseases Targeted by the IVI
A. Diarrheal and enteric diseases
Typhoid and other enteric fevers
Typhoid fever causes an estimated 22 million cases and more than 200,000 deaths per year, almost all in developing countries, according to one recent estimate. Two safe and effective new-generation vaccines – the live oral Ty21a, which is given in three or four doses, and the single-dose injectable Vi polysaccharide (PS) vaccine –
According to UNICEF, 9.7 million children under the age of five died in 2006 worldwide, mainly from infectious diseases. Overwhelmingly these deaths occurred in developing countries, especially in the poorest populations in sub-Saharan Africa, South and Southeast Asia.
In the last few years additional attention and resources have been directed at the better known infectious diseases of developing countries, particularly HIV/AIDS, tuberculosis, and malaria. This has resulted in a range of vaccine development initiatives targeting these diseases. New resources have also emerged for other diseases strongly associated with poverty – diarrheal and enteric diseases, respiratory infections and meningitis, and vector-borne viral diseases – but generally to a lesser extent. These diseases are the focus of the IVI’s activities. The Institute’s work to date on these “neglected” diseases and current gaps and opportunities are summarized below.
Enteric infections proliferate in unsanitary living conditions commonly found in devel-oping countries.

IVI Strategic Plan | 2008-2012
25
have been licensed for approximately two decades, but their use has been limited to date in developing countries, due to the lack of accurate data on typhoid incidence to guide policymakers, and until recently, the relatively high cost of these vaccines. The IVI’s Typhoid Vaccine Program was developed to accelerate the rational introduction of modern typhoid vaccines, with a focus on Vi polysaccharide vaccine. Multi-faceted evidence through prospective disease surveillance studies, post-licensure clinical trials and demonstration projects, economic studies of cost-of-illness and vaccine demand, and socio-behavioral studies was collected in five Asian countries and used to analyze the impact and cost-effectiveness of Vi vaccination in those settings. These multi-country data led to decisions by the governments of Pakistan and Indonesia to introduce school-based Vi vaccine on a pilot basis and to the formulation of new global recommendations on typhoid vaccination by WHO.
The IVI’s efforts to ensure a cost-competitive and adequate supply of existing and newer generation vaccines include: the development in the IVI laboratories and transfer to developing country producers of a new manufacturing process for Vi that increases yields three-fold; the development, in collaboration with the US National Institutes of Health, of a Vi diphtheria toxoid (Vi-DT) conjugate vaccine that can be given to infants; the technology transfer and clinical evaluation of the Vi-conjugate vaccine; the clinical evaluation of the single-dose, live attenuated ZH09 oral typhoid vaccine candidate; and the in-house development of a Salmonella Paratyphi A (SPA) conjugate vaccine as a component of a multivalent conjugate vaccine against typhoid and paratyphoid fevers.
Gaps and Opportunities
Despite increased understanding of typhoid fever in Asia, little is still known about the magnitude of this disease in several other regions, including Central Asia and Africa. There are still operational research and policy questions that need to be addressed to ensure that currently available typhoid vaccines are affordable and are introduced at the country level. Finally, while there are newer generation typhoid vaccines under development that target infants and that potentially provide longer and greater protection than currently licensed vaccines, concerted efforts are needed to ensure that these newer vaccines are further developed and transferred to high-quality producers willing to make the vaccines available to developing countries in sufficient supply and at affordable prices. Support for clinical trials of these newer vaccines will also be needed to ensure that they are licensed in a timely fashion.
Cholera
Cholera is estimated to cause 120,000 deaths worldwide each year, and the reported incidence is increasing. At the time that the IVI’s Cholera Vaccine Program began, two new-generation oral cholera vaccines were licensed internationally: a) a killed whole-cell vaccine, marketed by SBL under the name DukoralTM, which also contains a purified recombinant B-subunit of cholera toxin (rBS-WC), is licensed for persons two years and older and requires two doses; and b) a live oral single-dose
Typhoid fever causes
an estimated 22
million cases and
more than 200,000
deaths per year.

26
Remaining Gaps and Opportunities for Combating Infectious Diseases Targeted by the IVI
vaccine, marketed under the name OrocholTM, which is licensed for travelers from industrialized countries, but was found not to be protective in a randomized trial in a cholera-endemic setting.
To provide evidence to inform policy decisions about the introduction of modern oral cholera vaccines, the IVI has conducted prospective disease surveillance studies in several Asian and African countries; completed a demonstration study of cholera vaccination in Beira, Mozambique using the DukoralTM vaccine; analyzed the herd protective effects of oral cholera vaccines; and conducted social science research to estimate the economic burden of cholera, population demand for cholera vaccines in endemic areas, and the cost-effectiveness of cholera vaccination in Asia and African settings. The IVI has also reformulated an existing oral killed whole-cell (WC) vaccine used in Vietnam, resulting in a more immunogenic vaccine that is compliant with WHO standards. Technology transfer of this vaccine to developing country producers has been initiated, and studies are underway to assess its immunogenicity after one dose for potential use during outbreaks and for administration to infants in the conventional EPI schedule. The goal is to make this low-cost vaccine available internationally and pre-qualified by WHO for use in controlling endemic and epidemic cholera. In addition, the Program has conducted Phase I and II trials of a newer generation single-dose oral live attenuated vaccine candidate (Peru-15) and is planning large-scale efficacy trials of this vaccine.
Gaps and Opportunities Much work remains to introduce safe, effective and affordable oral cholera vaccines
for the control of both epidemic and endemic cholera. This work includes completion of clinical development plans for the oral killed WC and Peru-15 vaccines to bring them to licensure; pilot-testing the introduction of cholera vaccines in high-risk countries; synthesizing evidence to inform policy decisions about the use of vaccines to control epidemic and endemic cholera; and disseminating this information to both national governments and the global health community.
The IVI is a leading global partner in combating cholera through the use of new-generation oral vaccines.
Reported incidence
of cholera is
increasing.

IVI Strategic Plan | 2008-2012
27
Shigellosis and rotavirus
Of the estimated 1.8 million deaths from diarrhea in children under five years old each year, shigellosis (bacterial dysentery) is considered responsible for 200,000 – 600,000 and rotavirus for approximately 400,000. An especially virulent form of Shigella (S. dysenteriae type 1) has also been responsible for severe epidemics with high mortality, including in refugee situations. The IVI’s Shigellosis Vaccine Program conducted prospective disease surveillance and cost-of-illness studies in six Asian countries. Prompted by findings of the great geographic and temporal diversity of Shigella species and serotypes, IVI molecular microbiologists used innovative genomic search strategies to discover a common protein that could lead to the development of a low-cost Shigella vaccine that protects across all strains of the disease.
The IVI’s Rotavirus Vaccine Program has also conducted multi-country studies of the incidence, serotype distribution and cost of rotavirus diarrhea, as well as evaluations of two newly-available oral rotavirus vaccines – GlaxoSmithKline’s RotaRix®, a two-dose monovalent human strain vaccine, and Merck’s RotaTeq®, a five-strain human-bovine reassortant vaccine administered in three doses. The IVI collaborated on a Phase II study of RotaRix® in Vietnam and is currently conducting a Phase III trial of RotaTeq® at the same study site.
Gaps and Opportunities
Since no Shigella vaccine is yet available internationally, much work is still needed to develop and test effective vaccines, including the pan-Shigella common protein vaccine under development at the IVI. And despite the recent availability of two safe and effective rotavirus vaccines, data on the efficacy and impact of these vaccines are still needed for the poorest regions of Asia and Africa before WHO can issue recommendations on their use in these regions.
B. Respiratory infections and meningitis
Certain invasive respiratory bacteria, including Streptococcus pneumoniae (pneumococcus) and Haemophilus influenzae type b (Hib), cause pneumonia, meningitis and sepsis, resulting in more than one million deaths per year in children under five years of age, as well as hospitalizations and long-term neurologic sequelae in millions more. Tuberculosis, a new area for the IVI, caused an estimated 1.6 million deaths in 2005, with the highest mortality rates in Africa (due especially to HIV/AIDS co-infection), followed by Southeast Asia. Seasonal influenza is known to be a major killer, especially among the elderly, in both industrialized and developing countries. Interest in the disease in children, especially the dynamics of transmission, is increasing. In addition, there is growing concern that a global influenza pandemic will emerge from the currently circulating avian influenza virus, H5N1, which could exert many times the toll of mortality and morbidity attributed to seasonal influenza.
Invasive respiratory
bacteria cause more
than one million
deaths per year in
children under five
years of age.

28
Remaining Gaps and Opportunities for Combating Infectious Diseases Targeted by the IVI
The IVI’s Respiratory Pathogen Vaccine Program has conducted multi disciplinary research in the Asia-Pacific Region on the magnitude, circulating phenotypes and costs of Hib, pneumococcal disease and influenza to inform policy decisions about introducing currently existing vaccines and those under development. Research is currently underway in the IVI laboratories to develop novel vaccines against seasonal and pandemic influenza and pneumococcal disease, using sublingual administration and common protein antigens, as well as novel delivery systems, such as adenoviruses to deliver influenza virus antigens. Research is also ongoing to assess a vaccination strategy against tuberculosis that involves sublingual administration of an improved BCG vaccine, followed by a booster containing purified proteins.
Gaps and Opportunities
Many countries in Asia have yet to introduce the currently available Hib and pneumococcal conjugate vaccines, because of the relatively high cost of these vaccines and the lack of information on the disease burden and epidemiology of these diseases at the country level, and on the impact and cost-effectiveness of these vaccines. It is therefore critical in the next several years to demonstrate the need for and value of these vaccines in the Asia-Pacific region. Work must also continue on the development and clinical testing of novel vaccines against pneumococcal disease, tuberculosis and seasonal and pandemic influenza – which all need to be designed to be low-cost and easy to administer and thus specifically geared for use in developing countries. Finally, there is a pressing need for more information on the incidence and mortality of seasonal influenza in developing countries in order to inform decisions about the use of routine immunization against influenza in these settings.
C. Vector-borne viral diseases
Dengue fever
The incidence, geographic spread and frequency of epidemics of dengue fever, a mosquito-borne viral disease, have all increased in recent years. Each year an estimated 36 million people have clinically-apparent dengue virus infection (dengue fever), and 2.1 million progress to severe dengue – dengue hemorrhagic fever (DHF) or dengue shock syndrome (DSS) – resulting in an estimated 20,000 deaths. Two dengue vaccine candidates will soon be ready for large-scale clinical trials and two others are well advanced. The Pediatric Dengue Vaccine Initiative (PDVI), launched in 2002 to accelerate the development, licensure and use of dengue vaccines for children in dengue-endemic developing countries, has advanced the development of improved dengue diagnostics and assays, working with external partners; and has established a consortium of 11 field sites in nine countries of Asia and the Americas, where vaccine clinical trials, disease surveillance studies and other field research can take place. The Initiative is generating evidence on dengue disease burden, as well as on potential population demand for and the impact and cost-effectiveness of dengue vaccines. It has also established regional Dengue Prevention Boards in Asia and the Americas to disseminate this evidence and to address key issues regarding dengue research and the introduction of dengue vaccines.
The incidence,
geographic spread
and frequency of
epidemics of dengue
fever…. have all
increased in recent
years.

IVI Strategic Plan | 2008-2012
29
Gaps and Opportunities
A number of activities are critical to bringing safe and effective dengue vaccines to licensure and introduction over the next several years. These activities include clinical trials of promising vaccine candidates in developing countries, facilitated by the further development and use of improved immunoassays and diagnostic tests; the generation and dissemination of evidence on the need for, market potential, potential impact and cost-effectiveness of dengue vaccines; and the coordination and promotion of plans for the production, distribution and sustainable financing of dengue vaccines. The PDVI will continue to play a key coordinating role in all of these activities.
Japanese encephalitis
Japanese encephalitis (JE), a viral infection transmitted by mosquitoes, is a neglected disease that affects many Asian countries, especially in rural areas inhabited by the poorest populations. While national surveillance systems report 25,000-50,000 JE cases annually, the true JE disease burden remains unknown in many Asian countries and is likely to be considerably higher than these figures indicate. The clinical signs and symptoms of JE are typically severe, with a 10-30% of acute cases resulting in death and around 40% of survivors suffering neurological sequelae, including paralysis and mental retardation. Children 15 years old or younger are typically at greatest risk of getting the disease.
Vaccination of children against JE, using inactivated mouse brain-derived vaccines that require two primary doses and a booster dose, has successfully controlled the disease in the Republic of Korea, Japan and Taiwan for decades. JE vaccination also takes place in China, Thailand and parts of Vietnam. However, a number of presumably JE-endemic Asian countries have yet to use JE vaccines, because of a lack of local information on the disease incidence and its consequences, and the relatively high cost of mouse-brain derived vaccines. The goal of the IVI’s JE Vaccine Program is to accelerate the use of JE vaccines in JE-endemic countries where vaccines have yet to be introduced or where vaccines are used inadequately to effectively control the disease. The Program has conducted JE surveillance in several countries, including in Bali, Indonesia, where the IVI’s finding of high JE incidence in children led to a government decision to introduce JE vaccination on the island. The program has also conducted JE vaccination demonstration projects in Vietnam and North Korea, assessed different JE vaccination strategies in Vietnam, analyzed the long-term disability arising from JE in China, and assessed the cost-effectiveness of JE vaccination in China, Thailand, and Vietnam.
Gaps and Opportunities
A single-dose live attenuated SA 14-14-2 vaccine produced in China at very low cost, which has a reported efficacy of 96-100% lasting for at least five years, has recently become available world-wide. The emergence onto the global market of this vaccine has created new opportunities to demonstrate the safety and impact of vaccination against JE in endemic areas and thus to promote and facilitate the introduction of JE vaccines into child immunization programs in the Asian region.

30
Proposed Program Development: 2008-2012
2 Recognizing that these might also have benefit for middle income and sometimes industrialized countries.
VII. Proposed Program Development: 2008-2012
A. Principles guiding the 2008-2012 strategic planning process
In developing the IVI Strategic Plan for the period 2008-2012, the Board of Trustees and Director General were guided by the following principles:
• Addressing vaccines for diseases disproportionately affecting developing countries2;
• Ensuring that the IVI’s activities complement and create synergies with those of other organizations addressing new vaccines for the world’s poorest people;
• Building on the IVI’s achievements and areas of excellence as the fastest way to ensure public health impact from its efforts;
• Exploiting the Institute’s multi-faceted technical expertise to enhance laboratory-to-field linkages and to ensure cohesiveness in its activities along the vaccine ‘bench to community’ continuum;
• Expanding the IVI’s programmatic activities, particularly in the policy area;
• Extending the IVI’s activities geographically, particularly in sub-Saharan Africa and, where appropriate, in Latin America; and
• Enhancing the sustainability of the IVI’s activities for developing countries by building training and capacity-strengthening activities for developing country vaccine professionals and institutions into all programs.
B. Overview of the IVI’s strategies for 2008-2012
The IVI’s overall strategic objectives are shown in the Box on the next page, grouped by major categories along the “bench to community” continuum. The IVI does not conduct all of these activities for each targeted disease or vaccine, but rather tailors its activities according to the stage of vaccine development and use and the particular problems encountered in advancing vaccine development and deployment.
This plan identifies where the IVI believes it can make the most valuable contribution to vaccines against diseases that the Institute has targeted. Areas of proposed activity for 2008-2012 are summarized in Table 1 by Strategic Objective and target disease.
As noted in Section V.A, the IVI has become a leading global partner for vaccines against typhoid fever, cholera and dengue fever. It is also a significant global contributor
The Third Strategic
Plan builds on the
IVI’s achievements
and areas of
excellence as the
fastest way to ensure
public health impact.

IVI Strategic Plan | 2008-2012
31
The IVI’s Overall Strategic Objectives
Vaccine design
• To design new or improved vaccine candidates and routes of delivery;
Vaccine development
• To enhance the availability of an adequate, affordable and high-quality vaccine supply through development of manufacturing processes and quality control procedures and assays, technology transfer and regulatory support;
• To conduct clinical assessments of candidate vaccines to establish safety, immunogenicity and efficacy, including, where necessary, the development of improved immunological and diagnostic assays for use in the clinical assessments;
Vaccine introduction
• To generate evidence to guide rational vaccine introduction of new and under-utilized vaccines in developing countries;
• To accelerate vaccine introduction through data synthesis, analysis and dissemination;
Capacity-building in vaccine sciences for developing countries
• To increase the capacity of professionals in developing countries in vaccine development, introduction and manufacturing through programs of training, technology transfer, and technical assistance, and through conferences and seminars.
to vaccines against shigellosis, rotavirus, Hib, pneumococcal disease, influenza, tuberculosis and Japanese encephalitis. The focus of field activities for this latter group of diseases is in the Asia-Pacific region, where the IVI has gained recognition as an important center for vaccine-related research and technical assistance.
Attainment of the milestones identified below will in some cases depend on mobilization of additional resources. In addition, the IVI may explore and develop new research activities in response to emerging needs and opportunities.

32
Proposed Program Development: 2008-2012
Table 1. Proposed IVI activities by targeted disease and strategic objective
Respiratory infections and meningitis
Vector-borneviral diseases
Typhoid Cholera Shigellosis Rotavirus Hib Pneumo-coccal
disease
Influenza TB Dengue JE
Design new or improved vaccines √ √ √ √ √ √
Enhance the availability of an adequate, affordable and high-quality vaccine supply through development of manufacturing processes and quality control procedures and assays, technology transfer and regulatory support
√ √ √
Conduct clinical assessments of candidate vaccines, including development of improved immunological and diagnostic assays for use in the clinical assessments
√ √ √ √ √ √ √ √ √
Generate evidence to guide rational vaccine introduction
√ √ √ √ √ √ √ √ √ √
Accelerate vaccine introduction through data synthesis, analysis and dissemination
√ √ √ √ √ √ √ √ √ √
Increase the capacity of professionals in developing countries in vaccine development, introduction and manufacturing
√ √ √ √ √ √ √ √ √ √
Strategic Objective Enteric diseases

IVI Strategic Plan | 2008-2012
33
C. Diseases for which the IVI is a leading global partner
Typhoid and other enteric fevers
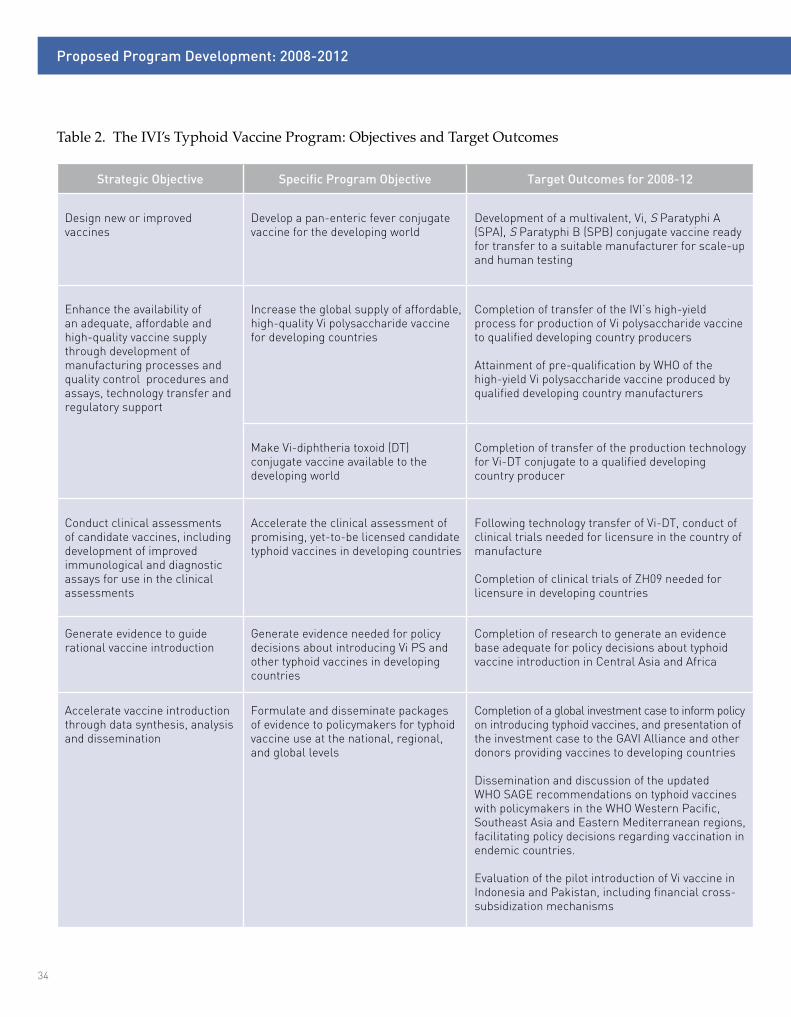
The goal of the IVI’s Typhoid Vaccine Program is to reduce morbidity and mortality due to enteric fever caused by typhoid and other invasive Salmonella pathogens. To reach this goal, the IVI will continue to work in all areas of the vaccine continuum, including designing a new typhoid Vi-paratyphoid A/B conjugate vaccine and completing the technology transfer and clinical development program of a high-yield Vi polysaccharide (PS) vaccine and a Vi-DT conjugate vaccine to qualified producers. Additionally, the IVI will pilot test Vi vaccine introduction in two countries (Pakistan and Indonesia), which will include an experimental financing strategy in which public school vaccination is subsidized by users’ fees for Vi vaccination provided to private school students. The program will also gather evidence to guide policy decisions about the use of typhoid vaccines in Central Asia and Africa, and will continue to synthesize data and communicate the results to policymakers (see Table 2).
Dr. Greg Smith working on the development of a Vi conjugate vaccine that can protect people of all ages – including infants – against typhoid fever.
The Typhoid Vaccine
Program will complete
the technology
transfer and clinical
development of Vi
and Vi conjugate
vaccines to qualified
producers.
34
Proposed Program Development: 2008-2012
Strategic Objective Specific Program Objective Target Outcomes for 2008-12
Design new or improved vaccines
Develop a pan-enteric fever conjugate vaccine for the developing world
Development of a multivalent, Vi, S Paratyphi A (SPA), S Paratyphi B (SPB) conjugate vaccine ready for transfer to a suitable manufacturer for scale-up and human testing
Enhance the availability of an adequate, affordable and high-quality vaccine supply through development of manufacturing processes and quality control procedures and assays, technology transfer and regulatory support
Increase the global supply of affordable, high-quality Vi polysaccharide vaccine for developing countries
Completion of transfer of the IVI’s high-yield process for production of Vi polysaccharide vaccine to qualified developing country producers
Attainment of pre-qualification by WHO of the high-yield Vi polysaccharide vaccine produced by qualified developing country manufacturers
Make Vi-diphtheria toxoid (DT) conjugate vaccine available to the developing world
Completion of transfer of the production technology for Vi-DT conjugate to a qualified developing country producer
Conduct clinical assessments of candidate vaccines, including development of improved immunological and diagnostic assays for use in the clinical assessments
Accelerate the clinical assessment of promising, yet-to-be licensed candidate typhoid vaccines in developing countries
Following technology transfer of Vi-DT, conduct of clinical trials needed for licensure in the country of manufacture
Completion of clinical trials of ZH09 needed for licensure in developing countries
Generate evidence to guide rational vaccine introduction
Generate evidence needed for policy decisions about introducing Vi PS and other typhoid vaccines in developing countries
Completion of research to generate an evidence base adequate for policy decisions about typhoid vaccine introduction in Central Asia and Africa
Accelerate vaccine introduction through data synthesis, analysis and dissemination
Formulate and disseminate packages of evidence to policymakers for typhoid vaccine use at the national, regional, and global levels
Completion of a global investment case to inform policy on introducing typhoid vaccines, and presentation of the investment case to the GAVI Alliance and other donors providing vaccines to developing countries
Dissemination and discussion of the updated WHO SAGE recommendations on typhoid vaccines with policymakers in the WHO Western Pacific, Southeast Asia and Eastern Mediterranean regions, facilitating policy decisions regarding vaccination in endemic countries.
Evaluation of the pilot introduction of Vi vaccine in Indonesia and Pakistan, including financial cross-subsidization mechanisms
Table 2. The IVI’s Typhoid Vaccine Program: Objectives and Target Outcomes

IVI Strategic Plan | 2008-2012
35
Cholera
The overall goal of the IVI’s Cholera Vaccine Program is to reduce the global mortality and morbidity due to cholera. To reach this goal, the program will: a) help to bring a low-cost, effective oral cholera vaccine onto the international market by supporting the completion of the clinical development plan and technology transfer of the oral killed whole-cell (WC) cholera vaccine improved and reformulated by the IVI; b) provide additional evidence to inform policy decisions about the use of oral cholera vaccines for the control of both endemic and epidemic cholera, including conducting pilot cholera vaccine introduction projects in endemic countries, assessing the feasibility of establishing a WHO stockpile using oral killed WC cholera vaccine for outbreak control, and determining how the stockpile should be used; c) synthesize and disseminate evidence addressing the use of oral cholera vaccines; d) accelerate the clinical assessment of the oral live attenuated, single-dose Peru-15 cholera vaccine candidate; and e) conduct upstream research into novel cholera vaccines, such as WC-based vaccines delivered sublingually (see Table 3).
Dengue fever
Over the next five years, the IVI’s Pediatric Dengue Vaccine Initiative(PDVI) will collaborate on clinical trials (Phase IIb/III) of existing late-stage vaccine candidates at PDVI field sites in Asia and the Americas, support research on dengue diagnostics, establish correlates of protection against dengue infection, and work with national regulatory authorities to harmonize regulatory pathways for dengue vaccines – all in the aim of having safe and effective dengue vaccines licensed and available by 2015. A series of studies and analyses will take place to inform national and international policymakers, vaccine producers and the donor community concerning the production, introduction and use of dengue vaccines. The results of these analyses will be compiled into a global investment case for dengue vaccine for developing country populations, to help ensure technical and financial support for the introduction of dengue vaccines in developing countries where the disease is endemic (see Table 4).
The inaugural meeting of PDVI’s Dengue Prevention Board for the Asia-Pacific region.
The activities of the
Pediatric Dengue
Vaccine Initiative
are aimed at having
safe and effective
dengue vaccines
licensed and
available by 2015.
The IVI’s Cholera
Vaccine Program
will help bring a
low-cost, effective
oral cholera vaccine
onto the international
market.

36
Proposed Program Development: 2008-2012
Table 3. The IVI’s Cholera Vaccine Program: Objectives and Target Outcomes
Strategic Objective Specific Program Objective Target Outcomes for 2008-12
Design new or improved vaccines
Develop a new whole-cell based cholera vaccine for sublingual vaccination
Completion of safety and immunogenicity trials in humans of a WC-based vaccine formulated for sublingual delivery
Enhance the availability of an adequate, affordable and high-quality vaccine supply through development of manufacturing processes and quality control procedures and assays, technology transfer and regulatory support
Increase the global supply of affordable, high-quality cholera vaccines for developing countries by transferring the production technology of the reformulated, oral killed WC cholera vaccine to qualified developing country manufacturers
Completion of technology transfer of the reformulated, oral killed WC vaccine to qualified developing country producers.
Conduct clinical assessments of candidate vaccines, including development of improved immunological and diagnostic assays for use in the clinical assessments
Support clinical studies of the reformulated, oral killed WC cholera vaccine for licensure in countries with WHO-approved national regulatory authorities
Completion of safety and immunogenicity trials of the reformulated, oral killed WC cholera vaccine in infants and after one dose
Completion of Phase III efficacy trials of the reformulated, oral killed WC cholera vaccine in Kolkata, India
Licensure of the reformulated, oral killed WC cholera in India
Pre-qualification by WHO of the reformulated, oral killed WC cholera vaccine for purchase by UN agencies
Validation in the field of rapid diagnostic tests for cholera (e.g. one-step immunochromatographic dipstick)
Accelerate the clinical development of the Peru-15 oral live attenuated cholera vaccine candidate
Completion of safety and immunogenicity trials of Peru-15, when co-administered with other EPI vaccines and when given to HIV+ individuals
Launch of a Phase III efficacy trial of Peru-15 in a cholera-endemic setting
Generate evidence to guide rational vaccine introduction
Provide evidence needed for policy decisions about introducing cholera vaccines into immunization programs for controlling endemic and epidemic cholera in Asia and Africa
Completion of evaluation of the scientific and programmatic feasibility of oral killed WC cholera vaccines for use in a stockpile
Development of improved tools for prediction of cholera epidemics to better target the use of cholera vaccines
Completion of pilot introduction projects using oral killed WC cholera vaccine in cholera-endemic countries
Accelerate vaccine introduction through data synthesis, analysis and dissemination
Formulate and disseminate packages of evidence to policymakers for cholera vaccine use at the national, regional, and global levels
Completion of a global investment case to inform policy on introducing cholera vaccines, and presentation of the investment case to the GAVI Alliance and other donors supporting vaccine programs in developing countries
Dissemination of updated data on cholera disease and cholera vaccination to the WHO SAGE and to WHO Regional Offices

IVI Strategic Plan | 2008-2012
37
Table 4. The IVI’s Pediatric Dengue Vaccine Initiative Program: Objectives and Target Outcomes
Strategic Objective Specific Program Objective Target Outcomes for 2008-12
Enhance the availability of an adequate, affordable and high-quality vaccine supply through development of manufacturing processes and quality control procedures and assays, technology transfer and regulatory support
Establish appropriate regulatory pathways and review processes for dengue vaccine clinical trials and vaccine registration
Harmonization of regulatory pathways in endemic countries for dengue vaccine licensure through collaboration with the Developing Countries Vaccine Regulators Network (DCVRN)
Conduct clinical assessmentsof candidate vaccines, including development of improved immunological and diagnostic assays for use in the clinical assessments
Develop improved assays to measure immune responses to dengue virus infection and to vaccination, to diagnose dengue infections, and to detect antibody-enhanced disease
Development of immunological correlates of protection and risk for antibody-enhanced disease for the evaluation of dengue vaccines
Development of high through-put diagnostic assays for clinical trials of dengue vaccines
Improve quality of rapid diagnostic tests and other diagnostic kits to detect acute dengue virus infection
Establishment of international standards for dengue assays and diagnostics
Establish Good Clinical Practice (GCP) monitoring throughout the PDVI field site consortium
Establishment of GCP in all 9 countries of the PDVI field site con-sortium
Accelerate the clinical assessment of dengue vaccine candidates in developing country populations
Completion of Phase IIb and Phase III vaccine clinical trials of promising dengue vaccine candidates in multiple countries
Licensure of at least one safe and effective dengue vaccine by 2015
Generate evidence to guide rational vaccine introduction
Generate evidence needed for policy decisions about introducing dengue vaccines in developing countries
Data on dengue disease burden available from ongoing prospective surveillance studies
Completion of cost-of-illness studies and cost-benefit/cost-effectiveness analyses of dengue vaccination
Completion of socio-behavioral studies of the potential community barriers to dengue vaccine introduction
Completion of models of disease transmission and dengue vaccine introduction to estimate the impact of dengue vaccine use on disease incidence
Assess dengue vaccine markets and marketing strategies
Completion of initial assessments of the potential market and demand for dengue vaccines
Accelerate vaccine introduction through data synthesis, analysis and dissemination
Formulate and disseminate packages of evidence to policymakers for dengue vaccine use at the national, regional, and global levels
Completion of a global investment case to inform policy on introducing dengue vaccines and presentation of the investment case to the GAVI Alliance and other donors supporting vaccine programs in developing countries
Advocacy by the regional Dengue Prevention Boards leads to policy decisions in endemic countries regarding dengue control, including vaccination

38
Proposed Program Development: 2008-2012
D. Diseases for which the IVI is a global contributor
Shigellosis and rotavirus
The overall goal of these programs is to assist in global efforts to reduce the mortality and morbidity due to enteric pathogens through the development and evaluation of new vaccines against shigellosis and the evaluation and introduction of newly-developed vaccines against rotavirus. The Shigellosis Vaccine Program will focus on gathering further data on the disease and its costs, especially in Africa, and on continued development and testing in humans of novel Shigella vaccines, including a common protein pan-Shigella vaccine. Rotavirus activities will focus on conducting vaccine evaluations and synthesizing and disseminating information to accelerate the use of rotavirus vaccines in infants in developing countries (see Table 5).
The IVI is conducting clinical trials of new rotavirus vaccines in Vietnam to determine their efficacy in Asian populations.
The IVI will continue
development and
testing of novel
Shigella vaccines,
including a common
protein pan-Shigella
vaccine.

IVI Strategic Plan | 2008-2012
39
Table 5. The IVI’s Shigellosis and Rotavirus Vaccine Programs: Objectives and Target Outcomes
Strategic Objective Specific Program Objective Target Outcomes for 2008-12
Design new or improved vaccines
Develop new vaccination approaches for shigellosis
Completion of optimized production and formulation of a subunit-based, common protein pan-Shigella vaccine
Conduct clinical assessmentsof candidate vaccines, including development of improved immunological and diagnostic assays for use in the clinical assessments
Clinically evaluate new-generation vaccines against shigellosis
Identification of correlates or surrogates of protection for Shigella Completion of safety and immunogenicity trials in humans of new candidate vaccines against shigellosis
Support clinical studies for licensure of experimental rotavirus vaccines and evaluate alternative schedules of already licensed vaccines
Conduct of trials of experimental rotavirus vaccines for licensure in developing countries
Evaluation of alternative vaccination schedules for already licensed rotavirus vaccines in clinical trials
Generate evidence to guide rational vaccine introduction
Provide evidence to inform policy decisions about the use of Shigella and rotavirus vaccines in immunization programs in developing countries
Completion of studies of Shigella disease burden, serotype distribution and cost-of-illness in African countries
Evaluation of the effectiveness (including herd protection) and feasibility of rotavirus vaccination in Asian countries using currently available vaccines
Accelerate vaccine introduction through data synthesis, analysis and dissemination
Formulate and disseminate packages of evidence regarding rotavirus to policymakers to assist vaccine introduction at the national, regional, and global levels
Preparation and dissemination of multi-disciplinary packages of evidence on rotavirus disease and vaccination for regional and country-level policymakers in the Asia-Pacific region

40
Proposed Program Development: 2008-2012
Respiratory infections and meningitis
The focus of the IVI’s activities in respiratory infections and meningitis will be on further developing and field testing novel vaccines, including sublingual vaccines, against influenza, pneumococcal disease and tuberculosis. Laboratory work on pathogens, such as H5N1 influenza and tuberculosis, will be facilitated by the recently refurbished BSL3+ laboratory at IVI headquarters. These programs will also gather and synthesize evidence on the disease burden of pneumococcal, Hib disease, influenza and tuberculosis, especially for the Asia-Pacific region, and on the impact and cost-effectiveness of vaccines against these diseases (see Table 6).
The IVI conducts surveillance for pathogens that cause respiratory illnesses and/or meningitis in Asia, including invasive pneumococcal disease, Hib and influenza, to better understand the magnitude and epidemiology of these diseases.
The IVI will develop
and conduct pre-
clinical testing of
mucosal vaccines
against influenza,
tuberculosis and
pneumococcal
disease.
Japanese encephalitis
The JE Vaccine Program will continue to focus on generating and synthesizing evidence to assist policymakers in making decisions about the introduction of JE vaccination or ways to improve and expand their existing JE vaccine programs. This will include evaluating pilot JE vaccine introduction projects in Bali, Indonesia and elsewhere (see Table 7).
E. Cross-cutting research
In addition to the disease-specific programs outlined above, the IVI will continue research that has implications across diseases (see Table 8).
Design of new or improved vaccines
The Laboratory Sciences Division has developed four types of platforms to assist in the design of new-generation vaccines. First, to facilitate the design of novel

IVI Strategic Plan | 2008-2012
41
Table 6. The IVI’s Respiratory Infections and Meningitis Vaccine Programs: Objectives and Target Outcomes
Strategic Objective Specific Program Objective Target Outcomes for 2008-12
Design new or improved vaccines
Develop new vaccination approaches for seasonal and/or pandemic influenza, tuberculosis and pneumococcal pneumonia
Development and pre-clinical testing of a candidate influenza vaccine formulated for mucosal delivery
Development and pre-clinical testing of an improved BCG vaccine followed by a mucosal booster
Development and pre-clinical testing of a common protein-based candidate pneumococcal vaccine formulated for sublingual delivery
Conduct clinical assessmentsof candidate vaccines, including development of improved immunological and diagnostic assays for use in the clinical assessments
Clinically evaluate candidate vaccines against pneumococcal disease, influenza and tuberculosis, and alternative schedules and new routes of administration for existing vaccines
Development of standardized immunoassays for measuring mucosal immune responses to influenza, pneumococcal disease and tuberculosis
Identification of mucosal correlates of protection against influenza, pneumococcal disease and tuberculosis
Completion of safety and immunogenicity trials in humans of new candidate vaccines and/or new immunization routes for vaccines against pneumococcal disease, influenza and tuberculosis
Completion of field trials of alternative vaccination schedules for already-licensed pneumococcal conjugate vaccines
Generate evidence to guide rational vaccine introduction
Provide evidence to inform policy decisions about the introduction of Hib, pneumococcal, influenza, and tuberculosis vaccines in immunization programs in Asian countries
Completion of studies and analyses of the disease burden of Hib, pneumococcal disease and influenza for different target age groups in selected Asian countries
Completion of analyses of the cost-effectiveness of pneumococcal and influenza vaccination in selected Asian countries
Establishment of field sites to gather epidemiological and economic data on tuberculosis, working with international and local partners
Measurement of the direct and indirect effects of influenza vaccination in Asian countries
Accelerate vaccine introduction through data synthesis, analysis and dissemination
Formulate and disseminate syntheses of evidence to policymakers at the national, regional, and global levels on Hib, pneumococcal, and influenza vaccines
Preparation and dissemination of multi-disciplinary packages of evidence on Hib and pneumococcal disease and influenza, and on vaccines against these diseases to regional and country-level policymakers in the Asia-Pacific region

42
Proposed Program Development: 2008-2012
Table 7. The IVI’s Japanese Encephalitis Vaccine Program: Objectives and Target Outcomes
Strategic Objective Specific Program Objective Target Outcomes for 2008-12
Generate evidence to guide rational vaccine introduction
Provide evidence on the disease and economic burden of JE and the feasibility, effectiveness and cost-effectiveness of JE vaccination in Asian countries
Completion of studies of JE disease and economic burden in JE-endemic countries in Asia
Evaluation of the feasibility and/or impact of the pilot introduction of new JE vaccines in JE-endemic countries of Asia
Completion of the analysis of the impact and acceptability of different JE immunization strategies
Accelerate vaccine introduction through data synthesis, analysis and dissemination
Develop regional, sub-regional and country-level consensus on recommendations for the use of JE vaccines in the Asia-Pacific region
Presentation of evidence to national and regional policymakers in Asia to inform policy decisions about the introduction of JE vaccination or modification or expansion of existing JE immunization programs
vaccines against targeted pathogens, the IVI’s Molecular Microbiology Program employs state-of-the-art techniques for genotyping clinical isolates detected in the Institute’s field research programs, with a particular focus on bacterial enteric agents. Second, to identify novel antigens that protect across bacterial species and serotypes, the IVI has developed an innovative reverse genomics approach for identifying common protective antigens, making use of information from the IVI’s in-house pathogen genotyping, as well as from available genotyping databases, bioinformatics, genetic engineering and pre-clinical testing. To date, the IVI has used this approach for the design of a common protein vaccine against shigellosis. Third, to overcome limitations of contemporary vaccines in eliciting broad immune responses in both the systemic and mucosal compartments of the immune system, the IVI laboratories have developed a new approach to immunization whereby the vaccine is administered under the tongue (sublingually). Fourth, to enhance immune responses to vaccines administered via mucosal tissue, IVI scientists have developed a new enterotoxin-based adjuvant capable of amplifying both mucosal and systemic immune responses. Extensive animal testing has established that this adjuvant is safe. With the development of these four powerful platforms, the IVI has laid the basis for designing new and improved vaccines against a wide range of diseases.
Improved clinical assessment of vaccines
The clinical evaluation of vaccines is hampered by a lack of well standardized assays for measuring vaccine-induced mucosal and T cell immune responses, especially in neonates and infants who constitute a major target population for immunization. The
IVI laboratories
have developed
a new approach
to immunization
whereby the vaccine
is administered
under the tongue
(sublingually).
IVI Strategic Plan | 2008-2012
43
IVI’s Clinical Immunology Program is developing miniaturized assays suitable for measuring mucosal responses in the small volumes of blood that can be obtained from pediatric subjects, as well as assays to measure immunological memory induced by vaccines. The next steps will be to test these immuno-monitoring tools in developing country populations and transfer them to laboratories in developing countries.
Another challenge is the difficulty in evaluating whether a vaccine causes rare but severe side effects. In Vietnam the IVI has pioneered the use of large-linked, dynamic, computerized population databases that link vaccination histories with severe clinical events, to provide a mechanism for quickly identifying and investigating potential side effects.
A third challenge confronting the clinical evaluation of vaccines is the need to measure vaccine “herd protection”, which can significantly enhance the protection of a vaccinated population by reducing the transmission of pathogens that are spread from person to person. IVI scientists have developed innovative methods for measuring herd protective effects of vaccines in clinical trials. Future work will focus on refining these methods and assessing their applicability to other vaccines and diseases.
Improved support to policy formulation for new vaccine introduction
Over the past years the IVI has conducted multiple programs of research to generate evidence to inform policy regarding the introduction of vaccines against diverse diseases, including cholera, typhoid fever, shigellosis, Hib, pneumococcal disease, Japanese encephalitis and dengue fever. The Institute has also synthesized this evidence into cost-effectiveness and impact analyses, including analyses of innovative vaccine financing mechanisms, for consideration by policymakers.
Several important challenges have become apparent while conducting these activities: 1) there is a paucity of evidence at the national level; 2) there are few analyses that examine both vaccine and non-vaccine interventions against specific diseases in order to inform the selection of disease control interventions; and 3) there is a dearth of analyses of innovative financing mechanisms to support the introduction of new vaccines, especially mechanisms that do not depend on the traditional model of external donor assistance.
To help address these challenges, the IVI will create a special Policy Unit. The unit’s activities will focus on generating better evidence for making rational decisions about vaccine introduction; on providing technical assistance to country policymakers on using this evidence for decision-making; and on developing innovative financing mechanisms to support vaccine introduction. Because of the Institute’s substantial experience and expertise on enteric fever, cholera, and dengue fever, the Policy Unit will initially focus on these diseases.
The IVI will create
a Policy Unit to
generate better
evidence for making
rational decisions
about vaccine
introduction.

44
Proposed Program Development: 2008-2012
Table 8. The IVI’s Cross-cutting Vaccine Research: Objectives and Target Outcomes
Strategic Objective Specific Program Objective Target Outcomes for 2008-12
Design of new or improved vaccines
Further develop new genotyping methods to characterize pathogens obtained from IVI field sites
Identification of new pathogens and antigens for new vaccine development, using IVI’s genotyping platform
Develop broadly applicable approaches for identifying conserved protective antigens in bacteria
Clinical evaluation of IVI’s new Shigella vaccine candidate, and deployment of the IVI’s reverse genomic platform for identification of attractive antigens for pneumococcal disease and Salmonella
Develop simpler, safer routes of vaccination that elicit both antibodies and cell-mediated immunity in mucosal and systemic body sites
Clinical evaluation of potential utility of sublingual vaccination for inducing broad immune responses in humans
Develop improved adjuvants to enhance protection by vaccines
Clinical evaluation of the IVI’s lead adjuvant in humans
Conduct clinical assessmentsof candidate vaccines, including development of improved immunological and diagnostic assays for use in the clinical assessments
Develop improved methods for monitoring immune responses to candidate vaccines
Evaluation in developing countries of the IVI’s new immuno-monitoring tools for measuring vaccine-induced immune responses in children and young infants and vaccine-induced immunological memory
Develop methods for large-linked databases for assessing rare but severe vaccine side effects in developing countries
Scale-up of the IVI prototype system in Vietnam
Development of systems in additional Asian and African countries
Assessment of the utility of the systems for monitoring the safety of new-generation vaccines introduced into developing countries
Develop innovative approaches for assessing vaccine protection
Refinement of the IVI’s new methods for measuring vaccine herd protection in pre-licensure efficacy trials
Exploration of how results from the IVI’s new method can be incorporated into mathematical models of disease transmission and into cost-effectiveness analyses of vaccines
Accelerate vaccine introduc-tion through data synthesis, analysis and dissemination
Develop improved and simplified methods for obtaining and synthesiz-ing evidence for vaccine policy at the national level
Creation of a Policy Unit at the IVI
Development of ‘best practices’ for addressing policy support for the rational introduction of new vaccines, based on disease-specific experiences for vaccines against cholera, typhoid fever, and dengue fever
Completion of model approach for global investment case preparation, based on disease-specific experience with cholera, typhoid fever, and dengue vaccine introduction
Develop options for innovative financing mechanisms for introducing new vac-cines into developing countries
Development of ‘best practices’ for addressing innovative financing for new vaccines, based on disease-specific experiences with vaccines against cholera, typhoid fever, and dengue fever
Provide technical assistance to country policymakers on using this evidence for decision-making
Provision of direct assistance to national policymakers in establishing special Vaccine Advisory Committees and in deliberations on the introduction of new vaccines

IVI Strategic Plan | 2008-2012
45
F. Capacity-building through courses, training, technology transfer, conferences and seminars
Since its inception the IVI has made capacity-building of health professionals and scientists in the area of vaccine science a major priority, with a predominant focus on professionals from developing countries. This emphasis reflects the recognition that training of professionals in developing countries in areas as diverse as laboratory sciences, clinical trials, social science research, and vaccine production and regulation is critical to empowering developing countries to produce and rationally introduce new vaccines in a sustainable fashion. The IVI’s in-house expertise and access to a wide range of experts from outside organizations provide a strong basis to conduct programs to strengthen scientific, vaccine regulation, and vaccine production skills.
The IVI’s capacity-building programs currently focus on the following areas:
• Formal courses in the field of vaccinology for professionals and students. Each year, the IVI offers a week-long “International Advanced Course on Vaccinology in the Asia-Pacific Region” for public health officials, scientists and policymakers from developing countries. The course – the only international course of its kind in the Asian region – provides an overview of the vaccine continuum, from vaccine development, evaluation, regulatory and ethical principles, to production, introduction, and policy issues. Additional training courses are also organized periodically for developing country professionals on the clinical evaluation of vaccines and topics of relevance to laboratory sciences.
The IVI conducts an annual Advanced Vaccinology Course for professionals in the Asia-Pacific region.

46
Proposed Program Development: 2008-2012
• Training in field research. As a key component of its field research activities, the IVI conducts on-site training, both informal and in workshops, of its local research collaborators in methods of field epidemiology, computerized data management, clinical evaluation of vaccines, Good Clinical Practice (GCP), microbiological and immunological procedures, and social science and economic research.
• Technology transfer and training in vaccine production and regulation. The IVI’s Vaccine Product Development group actively transfers to developing country producers the production technologies for several vaccines of importance to developing countries. In conjunction with technology transfer, the IVI provides hands-on and formal training to partner producers in vaccine manufacturing and quality control, including vaccine lot release and validation. Training is also provided to staff of national regulatory authorities. In addition, the IVI participates in training emerging producers and national regulatory authorities as a member of the WHO Global Training Network (GTN).
• Technology transfer of assays. The IVI is active in transferring immunological and diagnostic assays and providing training on their use for field studies and clinical trials to partner organizations in the developing world.
• Pre- and post-doctoral training and internships. Training in vaccine science has been provided to pre- and post doctoral researchers from Korea and from several developing countries. This includes placing young Korean scientists in laboratories overseas in anticipation of their employment at the IVI upon their return to Korea, as well as providing pre- and post-doctoral training for Korean and developing country scientists at IVI headquarters.
• Conferences and seminars. IVI periodically holds international conferences on topics of importance. These have included international meetings on pneumococcal and influenza vaccines, and an international symposium on vaccines for the 21st century. The IVI also actively exposes its staff, students, and interns to the world’s leading authorities in vaccinology through seminars at the IVI, including the Merck-funded “Scholars in Residence Program”, in which international experts spend a week at the IVI delivering lectures and advising IVI staff on their research.
Strategic objectives and target outcomes for 2008-12
In the next five years, the IVI will continue and expand its current capacity-building activities. Expanded activities will include:
• The establishment, in collaboration with a Korean university, of a Masters degree program in vaccinology for scientists throughout the world, with a focus on those from developing countries;

IVI Strategic Plan | 2008-2012
47
• Increased training in vaccine production and regulation for staff from vaccine producers and national regulatory authorities. This will include completion of a production training facility at the IVI to provide training in producing vaccines at scale;
• Training in Biosafety Level 3 management and practice, targeted to professionals in the Asia-Pacific region and using the IVI’s BSL3+ laboratories, which are currently being refurbished;
• Expansion of opportunities for young scientists from developing countries and Korea to receive pre- and post-doctoral training in laboratory sciences in the IVI laboratories.
IVI’s capacity-
building programs
will be enhanced
by the refurbished
BSL 3+ laboratory
and the production
training facility.
Dr. Shigeru Omi, Director of the WHO Regional Office for the Western Pacific, addresses the First Symposium on Pneumococcal Vaccination in the Asia Pacific Region, co-hosted by the IVI.

48
Maintaining a Strong Institution
VIII. Maintaining a Strong Institution
Efforts to ensure that the IVI’s operations remain efficient as the Institute grows will continue to receive close attention, since this will be essential for effective implementation of the IVI’s program.
A. Human resources
As the IVI expands its field research activities and explores new areas of research within its newly refurbished Biosafety Level 3+ facilities, it will face new challenges in the areas of compliance oversight and monitoring, safety management and program management.
To meet new challenges over the next five years, the IVI’s staff is expected to grow from 140 at present to 190 by the end of 2012.
To attract and retain a staff of highly qualified professionals, regular compensation studies will be undertaken to ensure that compensation packages are competitive. Staff development and training will also take place to enhance skills and to provide career growth opportunities within the Institute for both Korean and expatriate staff. Staff development will focus on specific skills training and participation in local, regional and international conferences and workshops. Periodic sensitivity training will also take place to inculcate staff with an understanding and appreciation of different national cultures within the IVI and in the countries in which they work.
Members of IVI’s Scientific Advisory Group and staff of the IVI.
The IVI’s staff is
expected to grow
from 140 in 2008 to
190 by the end of
2012.

IVI Strategic Plan | 2008-2012
49
B. Public awareness-raising and resource mobilization
The IVI’s programs depend on resources. The Institute’s budget is projected to grow from $28 million in 2008 to about $36 million by 2012. The personnel budget as a percentage of the total operating budget is expected to grow from 34% in 2008 to 41% by 2012. Funding is projected to be from a mix of unrestricted core funding from a larger constituent base of member states and fund-raising events and restricted project funding from foundations, local and international organizations, pharmaceutical companies, and government sources. Raising these resources from a variety of donors depends on the ability of the IVI to communicate its goals, programs, and accomplishments effectively to the correct audiences.
Public awareness-raising
In recent years the IVI has sought to raise public awareness about the Institute, both inside and outside of Korea, through a variety of methods, including communication of the Institute’s activities in the print media and television; maintenance of a website; mass mailing of the Institute’s Annual Report, Strategic Plan, Brochure, and quarterly Newsletter; sponsoring of domestic and international scientific seminars; and organizing special events, such as the annual IVI Charity Golf Tournament. Recognizing a need to better coordinate the IVI’s communications activities and to strengthen its resource mobilization efforts, the IVI Director-General formed a Communication and Development Unit in July 2007 to incorporate and expand upon these activities.
The IVI raises funds through events such as the annual IVI Charity Golf Tournament.
The Institute’s
budget is projected
to grow...to about
$36 million by 2012.

50
Maintaining a Strong Institution
The Communications and Development Unit will pursue the following objectives over the next five years:
• Expand the development of public awareness and advocacy materials, tools and strategies to raise the IVI’s visibility internationally and within Korea, including strategic use of the IVI Website and Newsletter;
• Participate in international advocacy activities for vaccines and immunization through collaboration inter alia with WHO, the GAVI Alliance, UNICEF, national governments, and vaccine product development partnerships (PDPs);
• Increase the presence and visibility of the IVI at major international public health and scientific conferences and events;
• Build networks of Korean and international media to expand coverage of the IVI’s activities;
• Develop materials identifying the significance and implications of IVI research results for dissemination to policymakers at international, regional and national levels;
• Expand public relations and media coverage for international symposia hosted by the IVI;
• Organize public relations events with collaborating governments for new field projects;
• Provide communications support for expanded resource mobilization efforts (see below), both in Korea and internationally; and
• Organize training in communications and resource development for
Communications and Development Unit and IVI staff.
Resource mobilization
During its relatively short existence, the IVI’s resources have grown rapidly to more than US $28 million in 2008, the majority of which comes from research grants and contracts. Support from the Korean Government – around $5 million in 2008 – and from the broader Korean community has been consistent and noteworthy. In less than two years, the Institute raised nearly $2 million from special fundraising events such as charity golf tournaments, corporate fundraising (including the establishment of ‘Giving Club’ donors, who each contribute at least $10,000 per year), and other efforts. Corporate support has included contributions from sources not traditionally associated with the health sector, such as LG Electronics, which has made a substantial donation for research and youth activities.

IVI Strategic Plan | 2008-2012
51
Nevertheless, the proportion of the IVI’s budget that comes from unrestricted (core) funding is only around 20%. These unrestricted funds are critical not only to support recurrent expenses such as those required to operate and maintain the IVI headquarters building, but also to provide flexibility in launching new initiatives and sustain staff professional development and growth. In addition, much of the IVI’s project support comes from a small number of donors. During the next five years the main resource mobilization goals of the IVI will therefore be to: a) increase its core funding; and b) increase the diversity of its funding sources for project-related support, including support from government donors. This will be accomplished by hiring a full-time development officer who will coordinate:
• Establishment of a Resource Mobilization Committee as an adjunct to the Board of Trustees or as a special support group to the Director General;
• Continuation and expansion of the number of Korean donors, networks and events;
• Launch of an international resource mobilization initiative to explore a comprehensive range of opportunities and sources for financial support;
• Examination of a possible role for IVI signatory countries to provide flexible and sustainable financing for the IVI;
• Solicitation of grants and contracts from a wider array of donors, including private donors and foundations.
C. The IVI’s Organizational Structure
As of early 2008, the IVI is organized into four main divisions that report to the Office of the Director General. These are: the Laboratory Sciences Division; the Translational Research Division, which conducts downstream research to inform policy decisions; the Pediatric Dengue Vaccine Initiative (PDVI); and the Administration and Finance Division (see figure on next page). The current Strategic Plan foresees no change in this organizational structure.
D. Governance and Management
As an international organization seeking to address the needs of developing countries, the IVI today has a membership of 40 countries and the WHO that are signatories to its Establishment Agreement. The Institute will continue to increase the number of signatories, especially among industrialized countries. The Institute Support Council, which consists of the IVI’s signatories and supporters, will be requested to assist in this effort.
To increase the involvement of signatory countries and stakeholders in institutional matters, the size of the IVI Board of Trustees was expanded in 2006 from seventeen
Main resource
mobilization goals
will be to increase
and diversify
unrestricted (core)
funding.

52
Maintaining a Strong Institution
Organizational Structure
Special Advisors
Scientific Advisory Group Institute Support CouncilBoard of Trustees
Director General
Policy Unit
Communications & Development Unit
Public Awareness / Advocacy
Marketing and Fund Raising
Institutional Review Board
Deputy Director General Deputy Director General Deputy Director General Deputy Director General
Strategic Partnerships
Vaccine Evaluation
Vaccine Access
Supportive Researchand Development
Department of Immunology: • Mucosal Immunology • Clinical Immunology • Neonatal Immunology
Department of Microbiology: • Molecular Vaccinology • Molecular Microbiology
Department of Vaccine Product Development andTechnology Transfer
Administration and Finance Division
LaboratorySciences Division
TranslationalResearch Division
Pediatric DengueVaccine Initiative
Division
Respiratory PathogenVaccine Program
Data Management andBiostatistics
Program Administration
Typhoid Vaccine Program
Cholera Vaccine Program
Shigellosis Vaccine Program
Rotavirus Vaccine Program
DPR Korea Program
JE Vaccine Program
Accounting and Finance
Computer Services
Library and InformationServices
Building andMaintenance
Human Resources andAdministrative Support Services

IVI Strategic Plan | 2008-2012
53
to twenty-two, including five signatory country representatives. As new countries become signatories to the IVI Establishment Agreement, the size of the Board will be reviewed periodically, since review of the IVI’s operations is ultimately the responsibility of the signatories.
To ensure that the IVI operates in an effective, transparent and accountable fashion, an internal auditing function has been established under the oversight of the Finance and Administration Committee of the Board and ultimately the full Board of Trustees. This will complement the existing external audit conducted each year by internationally-known accounting firms. The internal audits will also examine the activities of IVI collaborator institutions to ensure financial and operational compliance.
In 2008-2012 an increased emphasis will be also placed on management support to ensure compliance. In conjunction with the Internal Audit section, this will involve continued attention for both headquarters and off-site activities to the following:
• Compliance with requirements for facilities maintenance and security management (internal security and building parameters);
• Compliance with international Institutional Review Board (IRB) requirements;
• Centralized monitoring of all projects for compliance with respect to budgets, financial and technical reporting and payments, and risks exposures.
In addition, risk assessment and management will be continued in the areas of building security, biosafety monitoring and compliance, general project contractual compliance, and compliance with contractual obligations of institutional collaborators.
Members of the IVI Board of Trustees at its 2008 meeting.

54
Annex A | Annex B
Signatories to the IVI Establishment Agreement (as of March 2008)
Annex A
Bangladesh Bhutan Brazil China Ecuador Egypt India Indonesia
Israel Cote’ d Ivoire Jamaica Kazakhstan Kuwait Kyrgyzstan Lebanon Liberia
Malta Mongolia Myanmar Nepal Netherlands Oman Pakistan Panama
Peru Philippines Romania Senegal Slovakia Spain
Sri Lanka Sweden Tajikistan Thailand Turkey Uzbekistan Vietnam
World Health Organization
Papua New Guinea
Republic of Korea
United Arab Emirates

IVI Strategic Plan | 2008-2012
55
Board of Trustees of the IVI (as of March 2008)
Trustees serving in their individual capacities:
Dr. Abdul Rahman Al-AwadiExecutive SecretaryRegional Organization for Protection of Marine Environment (ROPME)Dahia Abdullah Salem, Kuwait
Prof. Barry R. Bloom (Chairman Emeritus)Dean, Harvard School of Public HealthBoston, Massachusetts, USA
Dr. John D. ClemensDirector GeneralInternational Vaccine InstituteSeoul, Republic of Korea
Prof. Gordon DouganPrincipal Research ScientistThe Wellcome Trust Sanger InstituteCambridge, UK
Dr. Roger GlassDirector, Fogarty International CenterNational Institutes of HealthBethesda, Maryland, USA
Mr. Michel GrecoIndependent Vaccine Expert Lyon, France
Prof. Nguyen Tran Hien DirectorNational Institute of Hygiene and EpidemiologyHanoi, Vietnam
Prof. Samuel Katz Professor Emeritus of PediatricsDuke University Medical CenterDurham, North Carolina, USA
Annex B
Prof. Margaret Ann Liu (Vice Chairman)Adjunct Professor Karolinska InstituteStockholm, Sweden Prof. Ragnar Norrby (Chairman)Director GeneralSwedish Institute for Infectious DiseaseControlStockholm, Sweden
Dr. Francisco SonganeDirectorPartnership for Maternal Newborn and Child Health (PMNCH) Geneva, Switzerland
Trustees serving as ex officio members or representatives of signatory coun-tries or organizations:
Dr. Margaret Chan Director GeneralWorld Health OrganizationSwitzerland
Dr. Akira HommaDirectorInstitute of Technology for Immunologicals/Bio-Manguinhos of the Oswaldo Cruz Foundation (Fiocruz)Rio de Janeiro, Brazil
Prof. Nay HtunProfessorStony Brook SouthamptonState University of New YorkSouthampton, New York, USA
Dr. I. Nyoman Kandun Director General of Disease Control and Environmental Health Ministry of HealthJakarta, Republic of Indonesia
Prof. Shin Bok KimVice President Seoul National UniversitySeoul, Republic of Korea
Dr. Shigeru OmiRegional DirectorWHO Regional Office for the Western Pacific (WPRO)Manila, Philippines
Mr. Young-Wan SongDirector General International Organizations Ministry of Foreign Affairs & Trade (MOFAT)Seoul, Republic of Korea
Prof. Ann-Mari Larsdotter SvennerholmProfessor and chairmanDepartment of Microbiology and Im-munologyUniversity of GothenburgGothenburg, Sweden
Prof. B.A.M. Van Der Zeijst DirectorNetherlands Vaccine Institute Al Bilthoven, The Netherlands
Dr. Isabel Noguer ZambranoDeputy Director of International Research Programs and Institutional RelationsInstituto de Salud Carlos III Ministry of Health and Consumption Madrid, Spain

56
Annex C
The IVI’s Collaborators
• Australia: Queensland Institute of Medical Research; Panbio• Bangladesh: ICDDR,B; Center for Health and Population Research; Dhaka Shishu
Hospital, Dhaka• Belgium: GlaxoSmithKline Biologicals• Brazil: Butantan; National Dengue Control Program Branch, Health Surveillance
Secretariat, Ministry of Health; Federal University of Goias; Institute Oswaldo Cruz• Cambodia: Communicable Disease Control, Ministry of Health; Kantha Bopha
Pediatric Hospital; National Dengue Control Program; National Center for Parasitology; Entomology and Malaria Control, Ministry of Health; National Immunization Program, Ministry of Health; National Pediatric Hospital; Epidemiology Unit, Institut Pasteur
• Canada: Ministry of Health; University of Western Ontario; National Microbiology Laboratory, Public Health Agency of Canada
• China: Anhui Provincial Anti-Epidemic Center; Beijing Friendship Hospital; Changchun Children’s Hospital; Chinese Centers for Disease Control; Dong-nan University School of Public Health; Fudan University; Guangxi Center for Disease Control and Prevention; Guangxi Maternal and Child Hosptial; Guangxi Medical University; Guangxi Centers for Disease Control and Prevention; Guangxi Provincial Hospital; Guangxi Province Anti-Epidemic Station; Hebei Provincial Anti-Epidemic Center; Jiangsu Provincial Anti-Epidemic Center; Kunming Children’s Hospital; Lanzhou Institute of Biological Products; Lulong County Health and Anti-Epidemic Center; Ma-An-Shan Hospital; Ministry of Health; Nanning Second City Hospital; National Institute of Virology; Sinovac Biotech; Suzhou Medical School; Suzhou Children’s Hospital; Wuhan Institute of Biological Products; Wuming County Hospital; Yongning County Hospital; Xiamen University; Hechi City Centers for Disease Control and Prevention; Jin Cheng Jiang Centers for Disease Control and Prevention
• Cuba: Instituto of Tropical Medicine “Pedro Kouri”• Egypt: Ministry of Health and Population; U.S. Naval Medical Research Unit 3;
Vacsera• El Salvador: Unit of Epidemiology, Ministry of Public Health and Social Assistance• Finland: National Public Health Institute• France: Centre National de la Recherche Scientifique; Epicentre; Institut National
de la Santé et de la Recherche Médicale (INSERM); Institut Pasteur; sanofi pasteur• Germany: Sartorius AG; Max Planck Institute for Infection Biology (MPIIB), Max
Planck Society for the Advancement of Science (MPG)• Guatemala: National Health Laboratory, Ministry of Public Health and Social
Assistance• India: All India Institute of Medical Sciences (AIIMS); Bharat Biotech; Biological E;
Indian Council of Medical Research; Indian Academy of Paediatrics; International Center for Genetic Engineering and Biotechnology; INCLEN India; Ministry of
Annex C

IVI Strategic Plan | 2008-2012
57
Health; MOSC Medical College Hospital; National Institute of Cholera and Enteric Diseases (NICED); National Institute of Virology; Shantha Biotechnics; Indian Immunologicals, Limited
• Indonesia: BioFarma; Centers for Disease Control and Environmental Health, Ministry of Health; Central Public Health Laboratory; Gadjah Mada University; National Institute of Health Research and Development; Udayana University; U.S. Naval Medical Research Unit 2; Sanglah Hospital, Bali; Provincial Center for Disease Control, Bali
• Japan: Life Sciences Division, Pentax; National Institute of Infectious Diseases; Research Institute for Microbial Diseases, Osaka University; Institute of Medical Science, University of Tokyo; Nagasaki University
• Laos PDR: Mahosot Hospital; National Institute of Public Health, Ministry of Health
• Malaysia: Faculty of Medicine, University of Malaya• Mongolia: National Maternal and Child Health Research Center; Sukhbaatar
District Hospital; Ministry of Health; Health Sciences University of Mongolia• Mozambique: Ministry of Health, CHAEMS• Netherlands: Crucell; Netherlands Vaccine Institute• Nicaragua: National Center for Diagnosis and Reference, Ministry of Health• Pakistan: Aga Khan University; Amson Pharmaceuticals; Ministry of Health• Panama: Instituto Conmemorativo Gorgas• Philippines: Cebu Institute of Medicine; Research Institute for Tropical Medicine• Republic of Korea: Busan National University Hospital; Catholic University
Hospitals (St. Paul Hospital, Seoul, and St. Mary’s Hospital); Changwon Fatima Hospital; Chonbuk National University; Chonbuk National University Hospital; Chonbuk Provincial Department of Health; Chonju Presbyterian Hospital; Green Cross Clinical Reference Laboratory; Hallym University Hospital; Hanyang University Hospital; Inha University Hospital; Jeju National University Hospital; Jung-Eub Hospital; Korea Centers for Disease Control; Korea Research Institute of Bioscience and Biotechnology; Korea University; Korean Food and Drug Administration; Korean Institute of Tuberculosis; Korean National Institute of Health; Kyunghee University Hospital; Kyungpook National University; LG Life Science; Nam Won Medical Center; Pohang University of Science and Technology; Postech University; Sam Kwang Clinical Laboratories; Seoul Clinical Laboratories; Seoul National University; Social Security Research Institute; Soonchunhyang University Hospital; Standard Diagnostics; Ulsan University; Yonsei University; Won Kwang University Hospital
• Singapore: K.K. Women’s and Children’s Hospital; Novartis Institute for Tropical Diseases
• Sri Lanka: Epidemiology Unit, Ministry of Health; Lady Ridgeway Hospital and Ministry of Health
• Sweden: Swedish Bacteriology Laboratories; Swedish Institute for Infectious Disease Control; University of Gothenburg
• Switzerland: Médecins sans Frontiéres
58
Annex C
• Thailand: Armed Forces Research Institute of Medical Science (AFRIMS); Center for Disease Control, Ministry of Public Health; Center for Vaccine Development (CVD), Mahidol University; Faculty of Public Health, Mahidol University; Faculty of Tropical Medicine, Mahidol University
• United Kingdom: Wellcome Trust Sanger Institute; Health Protection Agency; Imperial College of Science, Technology and Medicine; London School of Hygiene and Tropical Medicine; Emergent BioSolutions, Inc; National Institute of Biological Standards and Control; Rockhopper TV; Oxford University
• United States: Arizona State University; AVANT Immunotherapeutics; Brandeis University; California Institute of Technology; Center for Biologics Evaluation and Research, Food and Drug Administration; Centers for Disease Control and Prevention; Chiron Corp.; Colorado State University; Harvard University; Hawaii Biotech; Henry M. Jackson Foundation for the Advancement of Military Medicine; InViragen; Johns Hopkins Bloomberg School of Public Health; Johns Hopkins University; Hawaii Biotech; Merck & Co.; National Institutes of Health; Naval Medical Research Institute; Portland State University; Program for Appropriate Technology in Health (PATH); Purdue University; The Scripps Research Institute; University of Alabama; University of California at Berkeley; University of California at Los Angeles; University of Maryland; University of North Carolina at Chapel Hill; University of Pennsylvania; University of Rochester Medical Center; University of Texas Medical Branch at Galveston; Walter Reed Army Institute of Research; Washington University School of Medicine; Wayne State University; West Virginia University; Wyeth Vaccines
• Venezuela: Epidemiological Surveillance Headquarters, Ministry of Health and Social Development
• Vietnam: Bach Mai Hospital; Hanoi Health Service; Ha Tay Provincial Preventive Medicine Center; Ho Chi Minh City Pasteur Institute; Hue City Hospital; Hue Provincial Preventive Medicine Center; Institute for Vaccines and other Biological Substances (IVAC); Khan Hoa Provincial Hospital; Ministry of Health; National Institute of Hygiene and Epidemiology (NIHE); National Institute of Pediatrics; Nha Trang Pasteur Institute; Ninh Hoa District Hospital; Phu Tho Provincial Center for Preventive Medicine; Phu Tho Provincial Hospital; VaBiotech; Wellcome Tropical Diseases Research Unit
• International: World Health Organization

IVI Strategic Plan | 2008-2012
59
Collaborators at the National Institute of Cholera and Enteric Diseases (NICED) with IVI staff in Kolkata, India.

60
Annex D
Growth of the IVI
Annex D
Annual Budget from 1997 to 2007 (US$)
Staff Growth from 1997 to 2007
-
5,000,000
10,000,000
15,000,000
20,000,000
25,000,000
1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
0
20
40
60
80
100
120
140
160
1999 2000 2001 2002 2003 2004 2005 2006 2007
Tota
l No.
of S
taff
51
70
96
115 121
134
38
1829
AdministrationScientific SupportScientific & Technical
OtherUnrestricted
Restricted
-
5,000,000
10,000,000
15,000,000
20,000,000
25,000,000
1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
0
20
40
60
80
100
120
140
160
1999 2000 2001 2002 2003 2004 2005 2006 2007
Tota
l No.
of S
taff
51
70
96
115 121
134
38
1829
AdministrationScientific SupportScientific & Technical
OtherUnrestricted
Restricted

IVI Strategic Plan | 2008-2012
61
Night view of the IVI headquarters on the campus of Seoul National University in Seoul, the Republic of Korea

Further information concerning this material can be obtained from:
The International Vaccine Institute
Seoul National University Research ParkSan 4-8 Bongcheon-7 dongKwanak-gu, Seoul, Korea 151-919
Tel: +82-2-872-2801Fax: +82-2-872-2803Contact: [email protected]
www.ivi.int
This document is a publication of the International Vaccine Institute, and all rights are reserved by the IVI.However, the document may be freely reviewed, reproduced, and translated, in part or as a whole, upon receipt of permission from the Institute.
Designed by: Couchpotato DesignPrinted: September 2008



![SolarSystem p.loration Division StrategicPlan€¦ · SolarSystem p.loration Division StrategicPlan Preparing the way to the new frontzer of the 21 't century _!:iiiii_]]]]]ii]/ (NASA-TM-IO7d43)](https://img.dokumen.tips/doc/110x75/5f0b29647e708231d42f26e9/solarsystem-ploration-division-strategicplan-solarsystem-ploration-division-strategicplan.jpg)



























