Embed Size (px)
Citation preview

ISP RCONNECTIONS U n I t I n g R e S e a R c h a n d P R a c t I c e
InteRnatIonal SocIety foR PhaRmacoeconomIcS and oUtcomeS ReSeaRch
novembeR/decembeR 2011 vol. 17, no. 6
IN THIS ISSUELETTER FROM THE EDITOR
PRESIDENT’S MESSagE
Is Too Much Transparency in Decision Making Bad for Your Health?
OUTcOMES aSSESSMENT
The Burden of caregiving: assessing the Status of current clinical Research
POLIcY aNaLYSIS
Payer Roadblocks and Risk-Sharing agreements around the World
The ISPOR Health Outcomes Metrics Special Interest group
The Spanish National Health System: Time for Restructuring
ISPOR cORNER
ISPOR 14th annual European congress – ¡Hala Madrid!
ISPOR 14th annual European congress Photo gallery
ISPOR 14th annual European congress Scientific awards Recipients
ISPOR 5th asia Pacfic conference call for abstracts
Student corner – comparative Effectiveness Research: Opportunities and challenges
Web connections
ISPOR Meeting Travel Scholarship award Reports
ISPOR 2009 International Fellowship Report: Towards Pharmacoeconomics and
Outcomes Research in Nigeria
Recently Published Works: Innovatively Using Outcomes Research by ISPOR Members
ISPOR 17th annual International Meeting call for abstracts

As 2011 comes to a close, our Society continues to grow and prosper in ways in which the global economy could only dream of. We recently convened ISPOR’s 14th Annual European Congress in Madrid and—¡hay caramba!— the attendance there eclipsed 3,200 persons, an all-time high for any ISPOR European Congress. ISPOR’s other meetings also set attendance records, with more than 2,700 attending the 16th Annual International Meeting in Baltimore and nearly 500 attending the 3rd Latin America Conference in Mexico City.
This issue of ISPOR CONNECTIONS contains a great deal of material from the Madrid meeting, including a policy article from the Program Chair, Xavier Badia, a summary of the meeting program by our Managing Editor, Stephen Priori, a photo gallery of meeting attendees, and a listing of presentation award recipients. In addition, we publish eight reports from ISPOR Travel Scholarship Award recipients, who were able to come to Madrid from various outposts in Eastern Europe, the Middle East, and Africa. The ISPOR chapters in these regions are already offering forums to exchange ideas and discuss local health policy issues. Expanding opportunities for members in these regions to attend ISPOR’s larger conferences benefits those who receive the travel awards as well as those who get a chance to meet them and hear their unique perspectives.
Also contained in this issue is an interesting article on risk-sharing agreements, in which the authors highlight the fact that a great deal of confusion exists surrounding precisely what these agreements are, all the while manufacturers aggressively pursue them with payers around the world. A broader taxonomy may one day be provided, but for now the authors point out that there are two main types of risk-sharing agreements, one focused solely on containing aggregate spending on a given treatment and the other involving a kind of ‘pay-for-performance’ approach in which reimbursement is tied to ex post—rather than ex ante—patient outcomes.
Finally, from our Student Corner comes a commentary on opportunities and challenges in comparative effectiveness research (CER). CER continues to be an intriguing concept and the CER movement seems to be following an independent track from ISPOR, despite the obvious areas of overlap between our research agendas. Perhaps the next generation of leaders in our field, coming from the student ranks, will bring things into better alignment in the future.
In the meantime, all of us at ISPOR CONNECTIONS offer you our best wishes for the holiday season and look forward to having you join us as we set new attendance records at our 2012 meetings.
See you there!
David Thompson, PhD Co-Editor-in-Chief, ISPOR CONNECTIONS
2 November/December 2011 ISPOR cONNEcTIONS
ISPOR 2011-2012 BOaRD OF DIREcTORS
President – Mark J. Sculpher, PhD, MSc, Professor, Centre for Health Economics, University of York, UK, [email protected]
President-elect – Deborah Marshall, PhD, MHSA, Associate Professor, University of Calgary & University of McMaster; Director, HTA Alberta, Bone and Joint Health Institute Canada; Research Chair Health Services & Systems; Research Center Health Research Innovation Centre, Canada, [email protected]
Past President – Scott D. Ramsey, MD, PhD, Member, Fred Hutchinson Cancer Research Center, University of Washington, USA, [email protected]
directors – Federico Augustovski, MD, MSc, PhD, Director, Health Economic Evaluation and Technology Assessment, Institute for Clinical Effectiveness and Health Policy, Professor, University of Buenos Aires, Argentina, [email protected]; Kati Copley-Merriman, MS, MBA, Vice President, Regulatory & Health Outcomes Strategy, RTI-HS, USA, [email protected]; Finn Børlum Kristensen, MD, PhD, Professor, Health Services Research & Health Technology Assessment (HTA), University of Southern Denmark, Director, EUnetHTA, National Board of Denmark, Denmark, [email protected]; Newell McElwee, PharmD, MSPH, PhD, Executive Director, Merck, USA, [email protected]; Donald L. Patrick, PhD, MSPH, Professor, Seattle Quality of Life Group/Center for Disability, Professor, University of Washington, USA, [email protected]; Johan (Hans) L. Severens, PhD, Professor of Evaluation in Health Care, Institute of Health Policy and Management, Erasmus University Rotterdam, Netherlands, [email protected]; Bong-Min Yang, PhD, Professor, Health Economics, School of Public Health, Seoul National University, South Korea, [email protected]
treasurer – Karen Rascati, RPh, PhD, Professor, University of Texas, College of Pharmacy, USA, [email protected]
Founding executive director – Marilyn Dix Smith, RPh, PhD, ISPOR, USA, [email protected]
ISPOR cONNEcTIONS EDITORS & EDITORIaL BOaRD
co-editors-in-cHieF – Thomas Mittendorf, PhD, Germany, herescon gmbh; David Thompson PhD, OPTUMInsight, USA, isporconnections@ ispor.org
editorial board – Syed Mohamed Aljunid, PhD, United Nations University-International Institute For Global Health, Malaysia; Rajesh Balkrishnan, PhD, MS, University of Michigan, USA; Amit Chhabra, MD, MPH, Pfizer inc., USA; Benjamin Craig, PhD, H. Lee Moffitt Cancer Center & Research Institute, USA; Mohammed F. Jabr, PharmD, MSc, MBA, Canadian Agency for Drugs and Technologies in Health (CADTH), Canada; Bonnie M. Korenblat Donato, PhD, Bristol Myers Squib, USA; Axel C. Mühlbacher, PhD, MBA, HS Neubrandenburg; Marc Nuijten, PhD, MD, MBA, Imta, Erasmus University, Netherlands; Gabriela Tannus, MSc, AxiaBio, Brazil; Michael Wonder, BSc, BPharm, Australia; Gergana Zlateva, PhD, Pfizer Inc., USA
ISPOR cONNEcTIONS PUBLISHINg, SUBScRIPTION, aND aDvERTISINg OFFIcE:
ISPOR CONNECTIONS (ISSN 1538-5108) (USPS 019121) is published bi-monthly by the International Society for Pharmacoeconomics and Outcomes Research, 3100 Princeton Pike, Building 3, Suite E, Lawrenceville, NJ 08648 USA. Phone: 609-219-0773 Toll Free: 1-800-992-0643 Fax: 609-219-0774 Website: www.ispor.org
Annual membership dues include $30 for regular members and $15 for student members for a 1-year subscription to ISPOR CONNECTIONS.
Periodicals Postage paid at Princeton, New Jersey 08540 and at additional mailing offices. POSTMASTER: Send address changes to ISPOR CONNECTIONS, 3100 Princeton Pike, Building 3, Suite E, Lawrenceville, NJ 08648 USA.
Managing editor: Stephen L. Priori, email: [email protected]
advertising Manager: Danielle Mroz, email: [email protected]
Direct advertising, photocopy permission, and reprint requests, to Managing Editor.
©2011 International Society for Pharmacoeconomics and Outcomes Research (ISPOR). All rights reserved under International and Pan-American copyright conventions.All members of the Board of Directors serve in their personal capacity and do not represent the views of their organization during Board activities. All members of the Board of Directors annually disclose any conflicts of interest concerning business relationships with the Society. See: http://www.ispor.org/board/index.asp.
LETTER FROM THE EDITOR
David Thompson, PhD

November/December 2011 ISPOR cONNEcTIONS 3
Is Too Much Transparency in Decision Making Bad for Your Health?Mark Sculpher, PhD, 2011-2012 ISPOR President, and Professor of Health Economics, centre of Health
Economics, University of York, Heslington, York, UK
PRESIDENT’S MESSagE
The vast majority of health care systems around the world face resource constraints. In some
systems, such as the National Health System (NHS) in the United Kingdom, this is obvious because a fixed budget constraint is effectively defined by government each year. Even in more open systems without explicit budgets, however, political and economic limits constrain increases in health care expenditure; this is particularly the case in today’s fiscally challenging times.
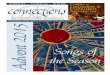
In the face of these inevitable resource challenges it follows that all systems have to give consideration to whether new medical interventions represent value for money. For example, we are often told that issues of cost are not relevant to Medicare’s coverage decisions in the United States; but recent work by Chambers et al. indicates that, even in this system, cost-effectiveness evidence is cited in national coverage determinations [1]. Therefore, it seems reasonable to conclude that value for money generally matters. What differs between jurisdictions is the degree of explicitness in defining ‘value’ and assessing this against cost. It may be helpful to characterise this phenomenon in terms of a ‘spectrum of transparency’ (see Fig. 1). Some systems are relatively explicit about their definition of value and how it is traded-off against costs. This is true of the National Institute for Health and Clinical Excellence (NICE) in England, for example, which defines a key objective in its decision making in terms of gains in population health; uses quality adjusted life-years (QALYs) as its primary measure of health; and trades health gain with costs by comparing the incremental cost-effectiveness ratio with a cost-effectiveness threshold representing the health forgone as services are displaced to fund more expensive new technologies. Despite this, NICE is clear that other considerations are brought to bear in making recommendations about new interventions (e.g. the innovative nature of technology), but how it brings in these other factors is not explicit.
Arguably, the French system of drug reimbursement is less explicit about how it defines value for money. The Amélioration du Service Médical Rendu (ASMR) score defines the relative effectiveness of a new product against existing treatments, and the more effective an intervention, the greater the scope the manufacturer has to set its own price.
It’s possible to cluster some jurisdictions around the relatively explicit cost-effectiveness approach (e.g. Canada, Sweden), with others being closer to the French approach of using clinical evidence to define an acceptable price (e.g. Germany). Medicare in the United States is an example of a system which is even less explicit about how it relates clinical efficacy with value for money.
It is interesting, however, that even systems which are relatively transparent in how they define value for money are being pressured to be more explicit about how decisions are made. This is true, for example, of NICE following the case made by manufacturers as part of the Kennedy review of how innovation should be valued [2]. As part of the current process of updating its methods guide, NICE is considering whether it should more extensively adopt multi-criteria decision analysis (MCDA) in its decision making. In principle, MCDA can be used to define all the factors NICE takes into account in decision making, to give each a weight and, through some form of aggregation, to provide a more algorithmic indication of the appropriate decision regarding a new technology. The move to value-based pricing in the UK in 2014 is likely to accentuate further the pressure for explicitness: to define the maximum price consistent with a product representing value for money in a system seeking transparency, the various attributes of value to the system, as well as the rates of exchange between them, need to be defined. Incidentally, there were several sessions at the recent ISPOR European Congress in Madrid devoted to MCDA, and there are a number of interesting methodological issues relating to these methods including what should be considered legitimate criteria and how the weights should be determined.
IN THIS ISSUE
>
LETTER FROM THE EDITOR 2
PRESIDENT’S MESSagE Is Too Much Transparency in Decision Making Bad for Your Health? 3
OUTcOMES aSSESSMENT The Burden of caregiving: assessing the Status of current clinical Research 4
POLIcY aNaLYSIS Payer Roadblocks and Risk-Sharing agreements around the World 8
The ISPOR Health Outcomes Metrics Special Interest group 10
The Spanish National Health System: Time for Restructuring 11
ISPOR cORNER ISPOR 14th annual European congress – ¡Hala Madrid! 13
ISPOR 14th annual European congress Photo gallery 14
ISPOR 14th annual European congress Scientific awards Recipients 16
ISPOR 5th asia Pacific call for abstracts
Student corner – comparative Effectiveness Research: Opportunities and challenges 18
Web connections 18
ISPOR Meeting Travel Scholarship award Reports 19
ISPOR 2009 International Fellowship Report: Towards Pharmacoeconomics and Outcomes Research in Nigeria 23
Recently Published Works: Innovatively Using Outcomes Research by ISPOR Members 24
ISPOR 17th annual International Meeting call for abstracts 27
Figure 1: the concept of a spectrum of transparency.

4 November/December 2011 ISPOR cONNEcTIONS
OUTcOMES aSSESSMENT
The Burden of caregiving: assessing the Status of current clinical ResearchNia Hamer, Ba, costello Medical consulting Ltd., cambridge, UK
Can we define the ‘correct’ location on the transparency spectrum? Inevitably, considerations about how explicit to be in defining value for money will vary between jurisdictions. In large part this is political. Although most governments are reluctant to use terms such as ‘rationing’, some are more comfortable than others in being open with the reality that not all medical interventions offer sufficient clinical benefits to justify their additional acquisition costs. Arguably, the more mature the debate in a country about how scarce collective resources are allocated, the more transparent the methods and processes used. Another political factor that may explain this variation in transparency is the role of the different professional groups in the decision-making process. If decisions are vested largely in those with a clinical background it would not be surprising for such individuals to focus on (mainly trial) evidence on clinical effectiveness, with the product’s price being modulated to help ensure value for money. Those systems which have brought in decision makers with quantitative backgrounds such as economics, mathematical modelling and biostatistics may be more likely to embrace formal analytical methods to link evidence to value for money.
How will this develop in the future? It could be argued the task of allocating finite health care resources will only grow more challenging in the face of
ageing populations, rising public expectations and continued limits on public expenditure. In circumstances where difficult and unpopular decisions are more common, health systems may be forced to be more open about how decisions are made. Indeed, increasing transparency may be seen as a way of insulating the process from political backlash: by setting up and justifying the principle of clearer criteria for reimbursement which is used consistently over time, policy makers can argue that decisions are more the realm of technical expertise than political judgements. There is likely, however, to be resistance to moving fully to the explicit end of the ‘spectrum of transparency’. Retaining some ‘wiggle room’ in decision making gives some scope to react to special circumstances whether these relate to the relevant disease, intervention or political circumstances.
References1 Chambers JD, Neumann PJ, Buxton MJ. Does Medicare have an implicit cost effectiveness threshold. Med Decision Making 2010;doi:10.1177/0272989X10371134.
2 National Institute for Health and Clinical Excellence. Kennedy Study of Valuing Innovation: Submissions. Available from: http://www.nice.org.uk/aboutnice/howwework/researchanddevelopment/KennedyStudyOfValuingInnovationSubmissions.jsp. [Accessed November 21, 2011]. London: NICE, 2009.
IC
caregiving An extremely important, but often under-recognized, group of individuals within society are those who provide informal, unpaid care on a long-term basis to a relative, friend or neighbor in need of assistance with activities of daily living.
Due to the use of different definitions of ‘informal caregiver’, estimates detailing the number of informal caregivers vary widely. For example, in the United States, it has been suggested that there are approximately 34 to 44 million adult caregivers [1,2]. By providing informal care to those in need of assistance, informal caregivers benefit society as a whole by providing an invaluable extension to formal health care systems. Although this care is unpaid, the estimated economic value of their unpaid contribution in the United States in 2007 was approximately $375 billion [1]. To put this figure in perspective, this was more than the total Medicaid spending in 2007 of $311 billion for both medical and long-term care, and approaches the total expenditures for the Medicare programme of $432 billion for the same year [1]. Furthermore, the economic value of informal care appears to be rising, reflecting the ageing population and the increase in the economic value per hour of care [1].
The Burden of caregivingAlthough informal caregivers clearly play an important and economically valuable role within society, it is widely documented that many may do so at a considerable cost to themselves [3]. First, caring for an individual over prolonged periods may be perceived as burdensome and stressful, which can impact on the mental health of the caregiver and lead to the development of illnesses such as depression and anxiety disorders [3]. These psychological burdens may be exacerbated by the negative social impacts of caregiving that arise from the changing of social roles and relationships. Furthermore, the time-consuming nature of caregiving may result in an inability to pursue personal interests and lead to social isolation.
Secondly, caregiving has been associated with an increased risk of some physical health problems, particularly in older caregivers who may be less
able to withstand the physical demands involved in the provision of care [3]. Some of the physical health risks identified in caregivers may be related to increased stress levels, such as decreased immune system functioning; however, others may reflect observations that caregivers can be less likely to engage in preventative health behaviors [3]. Finally, in addition to the health and social burdens of caregiving, the financial burden shouldered by individual caregivers can be substantial, particularly if caregivers are forced to interrupt their careers or retire early in order to meet responsibilities of informal care provision [4].
The support provided by informal caregivers is of particular importance to modern health care services, which are simultaneously facing significant budget constraints and the challenges associated with ageing populations. With these issues in mind, it is becoming increasingly important to address the multidimensional burdens associated with informal caregiving. In order to deal with the key issues facing caregivers, a better understanding of why and how caregiving is burdensome, who is most affected by caregiving, and how the negative effects of caregiving could be reduced, is required. Research into these areas is necessary from the wider societal perspective to maintain the health of caregivers and thus their ability to provide essential support to formal health care systems. The extent to which the burden of caregiving is considered in current clinical research is unclear. Therefore, we undertook a preliminary review of current clinical trials in order to evaluate the perceived importance of caregiver burden and assess the efforts being made to address the challenges faced by informal caregivers.
Evaluating the Status of caregiver Burden in current clinical ResearchA review of studies listed on ClinicalTrials.gov (a registry and results database of clinical trials) was conducted to identify current studies in which at least one aspect of caregiver burden (physical, emotional, psychological, social or financial) was measured as an outcome. One hundred and forty-three studies were identified and evaluated to detect the key aspects of the research pertaining to caregiver burden.

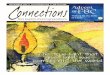
care-recipient conditionWe found that of the 143 trials that considered the burden of caregiving, the most common care-recipient conditions studied (the health conditions of those receiving the informal care) were Alzheimer’s disease and related dementias (ADRD); accounting for 41% of the studies (Fig. 1). This is relatively unsurprising due to the finding that ‘old age’ and ‘Alzheimer’s/confusion’ were identified as the two most common reasons for informal caregiving in a 2009 report of caregiving in the United States [5]; a finding that is likely to be true for many societies around the world and is likely to increase with the ageing population. The next most common care-recipient conditions identified in the review of current research were cancer (15%), and mental and behavioral disorders (11%).
caregiver burden as a Key Focus of the researchThe role of, or burden on, the informal caregiver was considered to be a key focus of the trial in just over half of the identified studies (53%). Figure 2 shows that studies involving the care of brain/spinal cord injury patients had the highest proportion of caregiver burden-focused studies (100%). This could perhaps be a reflection of the typically long-term and permanent nature of such disabilities that can often affect younger individuals and their families, compared with conditions associated with older age. As only four studies were identified for this care-recipient condition however, this finding may hold little real significance. The second highest proportion of caregiver burden-focused studies was identified as those investigating the care of cancer patients (76%). In the largest care-recipient condition category of ADRD, 53% of the studies considered the burden of caregiving as a key focus of the trial. Of the 28 ADRD studies where caregiver role was not a primary focus, 18 were trials investigating the efficacy of drug interventions in ADRD. In these studies,
< advertisement >
>
November/December 2011 ISPOR cONNEcTIONS 5
Figure 1: the care-recipient conditions.
Figure 2: caregiver burden as a key focus of identified studies.

caregiver burden was typically measured as an outcome to demonstrate the effect of the drug on improving the health and well-being of the care-recipient.
Measuring caregiver burdenA variety of instruments have been developed to quantify the burden of caregiving, including a number of questionnaires that are useful for the systematic assessment of a range of objective and subjective burdens of caregiving. Examples include the Perceived Family Burden Scale and the Zarit Caregiver Burden Scale.
In our review of current clinical research into the burden of caregiving, the specific instruments used to measure caregiver burden were explicitly stated in 47% of the ClinicalTrials.gov listings. This may be limited to some extent, however, by the quality of the study details provided in this registry. Across the studies, a range of questionnaire-based instruments were used to evaluate the physical, emotional, psychological, social and financial impacts of caregiving. The most frequently-used measure of general caregiver burden was the Zarit Burden Interview (reported in 28% of the 67 studies that stated use of specific instruments), although many other general caregiver instruments were reported.
In several studies (predominantly in the largest care-recipient condition category of ADRD), caregiver burden was measured using instruments specific to the care-recipient condition, such as the Revised Memory and Behavior Problems Checklist, a questionnaire that is completed by the caregiver and identifies the absence or presence of memory and behavioral problems in the care-recipient, along with a reaction rating of the extent to which caregivers were ‘bothered’ or ‘upset’ by each behaviour. The strength of these care-recipient condition-specific measures is that they can capture information on the specific burdensome aspects pertaining to particular care-recipient conditions; potentially providing a more accurate measure of the burden associated with the illness than a generic instrument might identify. The use of disease specific measures, however, may limit the comparison of caregiver burden experienced across different disease areas. This could have implications for public health policy and the allocation of resources for interventions to reduce caregiver burden. In such circumstances, a generic instrument may be considered more appropriate.
Intervention Type and TargetBehavioral interventions, such as advice/training on caregiving and coping techniques or cognitive therapy, were the most frequently investigated intervention types among the included studies (40%). Studies investigating drug and management strategy interventions were identified in similar numbers (22% and 23% of studies, respectively). Of note, only two of the 32 studies investigating a drug intervention measured caregiver burden as a primary focus of the trial. Instead, changes in caregiver burden were evaluated as a knock-on effect of improvements in the health of the care-recipient. In contrast, the majority (93%) of studies assessing behavioural interventions considered the role or burden of the caregiver as a key focus of the study; suggesting that behavioural interventions may be considered the most effective approach for reducing the perceived burden of caregiving and mitigating the negative health, social and financial impacts that caregiving may have.
In the trials identified by the review, the intervention under evaluation was targeted at the care-recipient in 65 studies (45%), the caregiver in 47 (33%), and both the care-recipient and caregiver in 31 (22%). Interventions targeted at the care-recipient typically intended to improve the health and well-being of the care-recipient, or to improve the provision of formal-care to the care-recipient, both of which lead to a reduction in the need for informal care and thus a reduction in caregiver burden. Interventions aimed at the caregiver were typically behavioural interventions designed to help and support the caregiver in their role, to help them cope better with the caregiving challenges that face them.
Summary and Future Directions for Research This analysis highlights how current research into caregiver burden and the efficacy of interventions for reducing caregiver burden are typically concentrated in age-related care-recipient conditions such as Alzheimer’s
disease and dementia. This is likely due to the ageing population, the prevalence of dementia in elderly patients, and the observation that caring for someone with dementia can be associated with higher levels of stress than caring for someone with functional impairment from another type of chronic disease [6]. Conclusions drawn from the body of research into caregiver burden in these specific areas, however, may not be applicable to the burden of caregiving in very different situations, such as the burden felt by parents of chronically ill children. Furthermore, even when considering caregiver burden within a single care-recipient condition, individual caregivers appear to possess unique combinations of risk factors and coping mechanisms that can determine the degree of burden they experience. It is therefore important to understand what characterizes those less able to cope and use this knowledge to assess each caregiver/care-recipient relationship in order to tailor interventions to support and help the caregiver most effectively [7].
Of the current research identified in this review of measuring the burden of caregiving, only half of the trials considered caregiver burden as a primary focus of the trial. Although changes in the burden of caregiving may be useful indicators for changes in the health and well-being of the care-recipient, the collection of this data could be valuable in a broader sense to address specific aspects of caregiver burden, such as factors that contribute to, or characterize, poorer caregiving experiences.
Measurement of the financial impact of reducing caregiver burden, and the positive impact this may have at the societal level, will be an important theme of future research in this area. Such research will be of particular interest in the allocation of limited health care resources for services and support for caregivers, the cost of which is minute in comparison to the estimated economic value of informal caregiving [1].
Assessment of caregiver burden in the clinical setting is necessary for identifying caregivers at risk for experiencing detrimental effects of caregiving on their own health and ability to care. Moreover, the assessment of caregiver burden in the experimental setting is essential for determining the effectiveness of interventions designed to alleviate the burdens of informal caregiving. Therefore, further research into this field should be encouraged and promoted in order to improve the experiences of caregivers in all aspects of their role, to ensure that the invaluable contributions to society and health care services made by caregivers are maintained and supported as the demands for informal care inevitably grow.
References1 Houser A, Gibson M. Valuing the Invaluable: The Economic Value of Family Caregiving, 2008 Update [Internet]. American Society for Retired Persons Public Policy Institute, Washington DC. November 2008. Available from: http://assets.aarp.org/rgcenter/il/i13_caregiving.pdf. [Accessed July 15, 2011]
2 The Evercare® Survey of the Economic Downturn and its impact on Family Caregiving. Evercare® by UnitedHealthcare, Minnetonka, MN; National Alliance for Caregiving, Bethesda, MD. April 28, 2009. Available from: http://www.caregiving.org/data/EVC_Caregivers_Economy_Report%20FINAL_4-28-09.pdf. [Accessed July 15, 2011].
3 Schulz R, Beach SR. Caregiving as a risk factor for mortality, the caregiver health effects study. JAMA 1999;282:2215-9.
4 Viitanen TK. The Informal and Formal Care in Europe. Discussion Paper No. 2648 [Internet]. Institute for the Study of Labour (IZA), Bonn, Germany. February 2007. Available from: http://ftp.iza.org/dp2648.pdf. [Accessed 2011 July 15, 2011].
5 Caregiving in the U.S. Executive Summary [Internet]. National Alliance for Caregiving, Bethesda, MN in collaboration with the American Association for Retired Persons, funded by MetLife Foundation. November 2009. Available from: http://www.caregiving.org/data/CaregivingUSAllAgesExecSum.pdf. [Accessed July 15, 2011].
6 Parks SM, Novielli KD. A practical guide to caring for caregivers. Am Fam Physician 2000;62:2613-22.
7 Zarit SH, Femia EE, Kim K, Whitlatch CJ. The structure of risk factors and outcomes for family caregivers: implications for assessment and treatment. Aging Ment Health 2010;14:220-31.
6 November/December 2011 ISPOR cONNEcTIONS
IC

November/December 2011 ISPOR cONNEcTIONS 7
< advertisement >

global Overview of Risk-Sharing agreementsThe increasing use of risk-sharing in reimbursement decisions across major and emerging markets necessitates that key stakeholders understand the role of this concept in shaping drug development and regulatory decision making. The goal here is very clear – to offset the risks among payers (such as insurance companies or government health care bodies) of paying high reimbursement costs for treatments where there are uncertainties over the clinical value and/or health economic value of the treatment. For pharmaceutical companies, the risk-sharing agreement can offer an important alternative to offering a discounted price, or when they are faced with an outright rejection from the reimbursement authorities.
As a concept, risk-sharing agreements mean different things in different contexts. With this in mind, two definitions have been used and are listed here for reference:
�•�IHS�Global�Insight�definition�[1]:�“an umbrella term for a host of creative pricing or costing initiatives with the goal of securing reimbursement or greater access to the drug. Agreements are put in place between manufacturer and payor to potentially spread the cost of a particular medicine, or treatment regime, by placing conditions that explicitly dictate how much the payor will spend and not spend. Risk-share conditions can significantly vary in nature depending on the drug, its mechanism of action, and the type of disease it is treating, and their implementation can often be indirect,” and
�•�University�of�Washington’s�PORPP�definition�[2]: “agreements between a payer and a pharmaceutical, device, or diagnostic manufacturer where the price level and/or nature of reimbursement is related to the actual future performance of the product in either the research or ‘real world‘ environment rather than the expected future performance.”
The taxonomy here is generally split between finance-based and outcomes-based agreements:
�•� Finance-Based:� These agreements are conditioned by a set of pre-specified budget caps, discounts or restrictions that can either be based on a particular patient or on the disease population. These can include: price-volume agreements (France), expenditure caps (Australia; United States), price cuts that are attached to forecasted spending (Japan) and conditional discounts (Italy; UK), and
•�Outcomes-Based:�These agreements are conditioned by a pre-specified endpoint or definition of response that dictate whether the payor will cover the treatment on an ex post facto basis. These can include outcomes guarantees (United Kingdom; United States) and form the traditional model of risk-sharing agreements, as payment is weighted entirely against the performance of the drug.
This is a fast-evolving concept with few best practice guidelines or standard regulations. Each country has its own approach to the issue, and each therapeutic area has different requirements and strategies with regards to the potential need for risk-sharing agreements. In some markets, and certain therapeutic areas, risk-sharing agreements are a reality to the extent that they are a near-substitute for the normal reimbursement process. These include the UK (with both NICE
and the SMC), Australia and Italy. In other markets, and other therapeutic areas, risk-sharing agreements are not seen as an efficient reimbursement tool or indeed, even feasible. These include Japan, Germany and France, although, exceptionally, risk-sharing agreements do appear in these markets as well.
This reveals an inherent paradox to the risk-sharing paradigm: the need – or demand – for risk-sharing agreements is greatest when the clinical outcomes for a treatment are uncertain, because the payer is potentially facing a high-cost product, but is not convinced by the value of the product.
It is precisely when the outcomes are uncertain, however, that risk-sharing agreements are potentially detrimental. This is because a successful risk-sharing agreement is incumbent upon a clear definition of when the treatment works, and when it does not work. If the outcomes are not clear, though, it becomes very difficult to set up clear parameters for a risk-sharing agreement and decide who pays for the treatment.
Research in this area is always limited by the often confidential nature of the agreements in question. Some agencies, however, are more transparent than others in their dealings with this subject, and there are increasing initiatives to provide more details on each agreement, particularly in the United Kingdom and Italy. . For this overview, the primary research was conducted through 50 in-depth 45-minute telephone interviews in native languages. Subjects were carefully selected and represented payers, government agencies and health technology assessment (HTA) organizations in nine markets (United Kingdom, Germany, France, Italy, Spain, Australia, New Zealand, United States and Canada) to understand their assessment of the role risk-sharing agreements have – or have not – played in their respective markets, and whether they will do so in the future. This was complemented with secondary research of reimbursement decisions around the world based on a newly created database of risk-sharing agreements (IHS Risk-Sharing Agreements Database).
In some large markets, such as the United Kingdom, Australia and Italy, for certain therapeutic areas such as oncology, these agreements are very common, but primary research indicates that this practice faces significant resistance at many layers. Many other countries are seeking to understand the potential applicability of risk-shares to their own market. Also, risk-share agreements are being examined for their potential in several other therapeutic areas. While population- and patient-level agreements remain the most popular, it is clear that health outcomes-based arrangements are significantly on the rise, with 27 having been identified through the study, the majority of which were signed since 2007. Just over half were signed for oncology therapeutics, including treatments such as bevacizumab, sunitinib and bortezomib. Outcomes-based agreements are becoming an increasingly important consideration to include in pricing models across the traditional development pathway for new molecules.
Clearly, achieving “normal” market access for a new treatment, where regulatory approval is followed immediately by drug pricing and launch, is an increasingly rare phenomenon. While health care economics is an old discipline, it is being used with increasing sophistication by reimbursement authorities. This, in turn, is requiring increasingly flexible and creative pricing arrangements. Risk-sharing is not always successful, and the vagaries of sensitivity analyses, defining clinical response and setting budget or utilisation caps, can often upset the balance of cost-effectiveness thresholds. A key
POLIcY aNaLYSIS
Payer Roadblocks and Risk-Sharing agreements around the World gustav ando, Ma, Director, Healthcare & Pharma, IHS, London, UK
8 November/December 2011 ISPOR cONNEcTIONS

problem in the rise of risk-sharing agreements is that it has not been sufficiently legislated for, nor adequately controlled or monitored. There are few guidelines on the specific criteria used to select when—and, perhaps more importantly, how—these agreements are applied. For pharmaceutical companies, risk-sharing agreements are quite clearly a last resort. By their very nature, risk-sharing agreements can call into question the validity of the clinical data supporting a drug launch. Also, agreements here can essentially transfer the entire risk onto the company, which has often spent many years, at very high cost and risk, developing the new treatment. In a world, however, where health care costs are becoming increasingly constrained both by government austerity measures, and government health care insurance expansion plans (e.g., the United States, China, and many emerging markets), the need for a strategy on risk-sharing agreements is essential, and will should be considered as part of the global launch plan for new drugs.
References1 Risk-Sharing Agreements: Creative Pricing as a Reimbursement Strategy. IHS Special Report, March 2009.
2 ISPOR Educational Symposium. “Performance-Based Risk-Sharing Arrangements: A Framework and Taxonomy. May 18, 2010.
November/December 2011 ISPOR cONNEcTIONS 9
< advertisement >
IC
The ISPOR Awards Committee is seeking nominees for:
ISPOR RESEARCH EXCELLENCE AWARDS
ISPOR Award for Excellence in Methodology in Pharmacoeconomics and Health Outcomes Research
ISPOR Award for Excellence in Application of Pharmacoeconomics and Health Outcomes Research
• • •
ISPOR BERNIE J. O’BRIEN NEW INVESTIGATOR AWARD
Recipients of these awards will be announced at the 17th Annual International Meeting,
Hilton Washington, Washington, DC, USA, June 2-6, 2012.
For awards descriptions, criteria, selection process, nature of award, and past recipients, go to:
http://www.ispor.org/awards/index.html.
Please submit nominations materials via email to [email protected].
THE DEADLINE FOR SUBMITTING NOMINATIONS IS FEBRUARY 10, 2012
ISPOR CALL FOR NOMINATIONS

10 November/December 2011 ISPOR cONNEcTIONS
The field of pharmacoeconomics and outcomes research benefits greatly from its interdisciplinary nature; we adapt and adopt methods from a variety
of disciplines including biostatistics, econometrics, psychometrics, operations research, informatics and epidemiology. Researchers in our field confront many data challenges, including missingness, non-normality, joint determination of multivariate outcomes (cost and effectiveness), clustering of observations and endogenous treatment selection. Other fields that contribute to our analytic toolset have developed approaches to deal with these issues, including: multiple imputation, generalized linear models (GLM), two-part models, structural equations, hierarchical models, propensity scores and instrumental variables, to name a few. Given that the field of pharmacoeconomics and outcomes research guides policy/decision makers, in addition to the usual concerns about internal validity and causal inference, we need to pay close attention to generalizability and quantification of uncertainty. To address these issues, we have adopted methods from the decision sciences including predictive simulation and Bayesian inference. All of these “solutions” come with their own sets of assumptions and limitations.
It’s a challenge to keep up with methodological advances in the fields in which we are trained, not to mention becoming familiar enough with the methods of other disciplines that need to be used to address different research questions in our field. The ISPOR Health Outcomes Metrics Special Interest Group (HOM) was created to “identify, highlight, and promote appropriate and novel approaches to health outcomes metrics used in pharmacoeconomics and outcomes research.” (http://www.ispor.org/sigs/HOM.asp). The HOM SIG currently has two active working groups, the Health Econometrics Working Group (HEWG) and Health Outcomes Metrics Education Working Group (HOME-WG) to help achieve its goal.
The ISPOR Health Econometrics Working Group (HEWG) was formed with the interrelated goals of promoting transparency of quantitative methods and encouraging comparative modeling (i.e., testing the sensitivity of results to modeling methods). While canned software programs are available for many of the standard econometric/statistical methods, the newer methods often lack the codes or they may be widely dispersed or the existing codes may not be user-friendly. This in turn may discourage researchers in our field who are not programming-savvy to apply those new methods in their research. Furthermore, even the canned software can be customized in variety of ways to address specific research questions, which may be inscrutable to the inexperienced user, and therefore appear daunting. The HEWG’s goal of promoting transparency in methods is meant to facilitate replication of those methods in different research contexts. Transparency of methods is mutually beneficial to both authors and consumers of research. Transparency lends credibility and allows for the rapid dissemination and adaptation (with full attribution of course!) of innovative approaches. Some journals (for example, the Journal of Applied Econometrics) have gone so far as requiring that authors deposit both the data and code necessary for the research community to replicate results (see: http://onlinelibrary.wiley.com/journal/10.1002/(ISSN)1099-1255/homepage/ForAuthors.html).
Transparency is also instrumental in achieving the second HEWG goal of promoting comparative modeling. Decision makers who rely on our research should be made aware of the sensitivity of our conclusions to the modeling
choices made. Comparative modeling is relatively simple when off-the-shelf methods are used, but when we develop “custom-made” solutions to our data challenges, the need to make code available to the research community is particularly strong.
Our main vehicle to achieve these first two goals has been the creation and maintenance of the ISPOR Health Outcomes Metrics Index of Open Source Code (http://www.ispor.org/OpenSourceIndex/Index.aspx). The HOM Index includes brief descriptions and hyperlinks to open-source code that can be downloaded for free. Currently, the HOM Index is arranged topically: treatment effects, health care costs, health care utilization, quality of life and utility, censoring and survival and “other.” We encourage ISPOR members to submit their own code or suggest links to others’ code they have found helpful in their own research by sending an email to: [email protected]. In the near future, HEWG will develop a strategy with the editorial staff of Value in Health to encourage (but not require) authors to submit open source code to the HOM Index.
The ISPOR Health Outcomes Metrics Education Working Group (HOME-WG) was created to “recognize, promote and encourage the development of outstanding online didactic material and educational resources in health outcomes metrics for use in pharmacoeconomics and outcomes research” (http://www.ispor.org/sigs/HOM_Education-Working-Group.asp). Notwithstanding the strong presence of ISPOR’s student members, it’s probably safe to say that it’s been at least a little while since the majority of us have been in graduate school. Nevertheless, in our rapidly evolving profession, each of us plays the roles of teacher and learner every day. Whether we are academics in the classroom, managers explaining results to opinion leaders, or scientists describing our methods to clients and colleagues, there is some element of didactic teaching involved in what we do on a daily basis.
Many excellent webinars, course syllabi, slide presentations, book chapters and homework exercises are widely available on the Internet – unfortunately, they are also widely dispersed. The primary aim of HOME-WG is to develop and maintain a centralized, searchable index of excellent educational materials focusing on the methods of pharmacoeconomics and outcomes research on the ISPOR website. The HOME-WG leadership group is currently developing the initial version of the index. We will then invite the ISPOR membership to contribute their own material or provide links to material they have found useful in the past. Ultimately, the HOME-WG will take steps to publicly recognize particularly excellent resources. The Health Outcomes Metrics Special Interest Group can only achieve its goals with the active support of ISPOR members. We strongly encourage you to join HEWG and/or HOME-WG (see: http://www.ispor.org/sigs/sigsindex.asp for steps on how to join) and to contribute your own code and educational materials. Please stay tuned as these exciting and useful endeavors progress. [Health Outcomes Metrics SIG Leadership Group: Anirban Basu, PhD, Bijan J. Borah, PhD, Benjamin M. Craig, PhD, Jalpa Doshi, PhD, David J. Vanness, PhD]
POLIcY aNaLYSIS
The ISPOR Health Outcomes Metrics Special Interest group David J. vanness, PhD, ISPOR Health Econometrics Working group co-chair and Health Outcomes Metrics
Education Working group co-chair, University of Wisconsin School of Medicine and Public Health, Madison WI, USa, and Bijan J. Borah,
PhD, ISPOR Health Econometrics Working group co-chair, Mayo clinic, Rochester. MN, USa
IC

November/December 2011 ISPOR cONNEcTIONS 11
The theme of the ISPOR 14th Annual European Congress was “Rational Health Care Decision
Making in Challenging Economic Time.” This article will discuss the health care reforms occurring across Europe and will cover the health care reforms recently introduced in Spain and discuss their impact. IntroductionTo provide the whole picture, we need to take into account that health care reform is a key initiative for the majority of countries around the world, including those in Europe. Although there is a mixture of funding and delivery models across the European Region, each country faces similar cost pressures in its national health program. The mounting challenges in funding these programs, combined with recent global economic conditions, have served to accelerate the pace of reform as governments try to reduce their exposure to health care funding. In many countries, this has resulted in “cost-shifting” the burden to employers and individuals.
To use Germany as an example, at the beginning of 2011, the German pharmaceutical market changed with the introduction of a new law to restructure drug market (AMNOG). Under the new law, each New Chemical Entity (NCE) must be supported by a benefit dossier defining the additional benefit of the drug in relation to the appropriate comparator.
In terms of the Congress host country, Spain, the Spanish government has been struggling to keep pharmaceutical expenditures under control in recent years due to the economic crisis. Demographic factors such as the ageing of the population, the inclusion of new services and innovative treatments, and, in general terms, greater demand for health care, put increasing pressure on public resources and on the financial sustainability of the health care system. Within this framework, a new Royal Decree (RD) has recently been approved based on cost-containment measures. Generally speaking, the primary objective of this new law focuses on prescription by active ingredient and the government expects savings of around f1500 million per year, which represents about 10% of the total pharmaceutical market.
Before going into the RD in detail, let us recall some of the basics of the Spanish health care
system and review some of the most acute problems it is facing:
DecentralizationThe Spanish health care system is one of the most decentralized health care systems in the world; health care is run independently by each of the Autonomous Regions. Spain is a large and diverse country, and there are significant variations in income levels, health care costs, and health care needs across the different autonomous communities. Health care is administered by the Autonomous Regions, but not directly financed by them. Tax revenues go to the central government, which redistributes them into the different Autonomous Regions in agreement with their needs and costs.
Private insuranceAbout 12% of the population has private health insurance. This two-tier health insurance system with a public basement and a private stage is unique in Europe. Private insurance payments account for 21% of total heath care expenditures. Further, a fair number of Spaniards pay out-of-pocket for care outside the national health system.
FundingSpain has a declining birth rate, ageing population, and an increasing life expectancy. Retirees constitute an increasingly larger proportion of public health care system users. Providing prescription medications without charge to all retired persons regardless of income level is regressive, distributing the same benefits to those with higher incomes as to those whose pensions barely cover their living expenses. In the current economic crisis, the system as a whole is unsustainable. Expert opinion favors the introduction of co-payments to reduce costs and demand for services, while public opinion resists any attempt to limit access.
Addressing regional disparities in health care and safeguarding the sustainability of public health provision has been high on the national political agenda for a long time. To cope with the sustainability of the Spanish National Healthcare System, the new RD includes a package of measures on pharmaceutical policies, a great number of which are solely for the purpose of making additional savings where public invoicing of medicines is concerned. Some of them are:
•PrescriptionbyInternationalNon-ProprietaryName (with exceptions) and the obligation to prescribe the cheapest medicine;
• Toughening up the Reference PriceSystem: the so-called “gradualness” used to progressively adapt the prices of a product to the reference price is no longer permitted, doing away with innovative Galenic protection once the first generic is on the market, etc.;
•Makingtherebatewhichisalreadyinplaceeven higher, raising it up to 15%. These rebates are applicable to medicines that don’t have a generic in Spain, that have been on the market for more than 10 years, financed by the State and that are not protected by a patent in force; and
•Establishinga systemof “selectedprices”for certain categories of medicines.
The direct consequences of these measures will be the closing down of some companies (especially the small and medium-sized ones), laying off staff, the resizing of investment in R&D, and pharmaceutical companies relocating to other countries to invest. All these aspects are very negative, not only for the pharmaceutical industry, but also for the Spanish economy as a whole. With all of the above in mind, the most serious point to make here is that these cuts do not solve the core problem of our national health care system: chronic budgetary under-financing compared to the true cost, just as it has been reported by numerous experts, and even from Regional Authorities.
Even more important than its immediate economic impact, however, is the structural change that the new RD will have on the Spanish pharmaceutical market. It will change not only the dynamics of the market, but also incentives and relations between the different agents along the medicine chain.
conclusionWith the economy at a standstill and the fact that an important sector like the pharmaceutical one is not gaining strength in gross domestic product, it is not good news for improving the Spanish economic competitiveness, nor the much needed change in the productive model boost in the medium and long term.
POLIcY aNaLYSIS
The Spanish National Health System: Time for RestructuringXavier Badia, PhD, MD, MPH, ISPOR 14th annual European congress chair and global Leader, Observational cOE
& Senior Principal, HEOR, IMS Health, Barcelona, Spain
IC

12 November/December 2011 ISPOR cONNEcTIONS
< advertisements >

November/December 2011 ISPOR cONNEcTIONS 13
The ISPOR 14th Annual European Congress was held on 5-8 November 2011 at the
Hotel Auditorium Madrid in Madrid, Spain. This was ISPOR’s first visit back to Spain since the ISPOR 6th Annual European Congress in 2003 in Barcelona. The Congress had over 3,200 attendees – a chart-topper!
As in 2003, Xavier Badia, PhD, MD, MPH, Global Leader, Observational COE & Senior Principal, HEOR, IMS Health, Barcelona, Spain served as Congress Program Chair and worked with the Program Committee to provide Congress attendees another high-level program. This year’s theme focused on rational health care decision making in challenging economic times.
Sunday 6 NovemberAfter pre-Congress Short Courses on Saturday and Sunday morning, the Congress opened with 2011-2012 ISPOR President Mark J. Sculpher, MSc, PhD, Professor of Health Economics, Centre for Health Economics, University of York, Heslington, York, UK, and Congress Program Chair Xavier Badia welcoming attendees to Madrid. Mark Sculpher also moderated the first Plenary� Session entitled “Pros and Cons of a Centralized European Pricing & Reimbursement Agency,” which explored if an agency similar in structure to the European Medicines Agency (EMA) should be established with a centralized procedure for pricing and reimbursement, as well as if this should be a decision-making agency or only undertake health technology assessment. These and other topics were discussed by speakers Hans-Georg Eichler, MD, MSc, Professor & Senior Medical Officer, European Medicines Agency and CBI Visiting Scholar, Robert E. Wilhelm Fellow, Massachusetts Institute of Technology, London, UK, and Adrian Towse, MA, MPhil, Director, Office of Health Economics, London, UK.
Issue�Panels�Session�I and Workshop�Sessions�i & ii were also held on Sunday, as well as Poster session i & exhibitors open House reception.
Monday 7 NovemberThe second�Plenary�Session,�moderated by Xavier Badia, entitled, “The Reality Of Real World Data And Its Use In Health Care Decisions In Europe,” offered attendees discussion on the issues of collecting and analyzing real-world data in Europe, such as patient-registry data, reimbursement data, prospective observational studies, or other health care practice-based information from three speakers: Leslie Levin, MD, FRCP(Lon), FRCPC, Head of the Medical Advisory Secretariat, Health Quality Ontario, Toronto, ON, Canada; Patrick
Keohane, MB, BS, MRCP(UK), Vice President, Payer Evidence, AstraZeneca, Södertälje, Sweden; and Enrique Bernal-Delgado, MD, PhD, Head, Health Services Research and Health Policy Unit (ARiHS), Health Research Institute of Aragón (IIS), Co-Chair, Atlas of Variations in Medical Practice in Spain and Scientific Coordinator, ECHO Project, Zaragoza, Spain.
Congress attendees had an opportunity to attend Poster� Session� II,� an Exhibitors’� Wine� and�Cheese� Reception, three contributed Podium Sessions,� as well as� Issue� Panels� Session� II and Workshop� Session� III.� The ISPOR Russia and Russia Far-East Regional Chapters’ forum, “The Assessment Of Medical Technologies In Russia: 15 Years Of Road Map Development,” was also held, and later in the evening, the ISPOR Social Event, “An Elegant Dinner at the Casino de Madrid,” gave attendees a chance to visit an exquisite historic private club in central Madrid.
Tuesday 8 NovemberThe third day included ISPOR�Forums,�and issue Panels�Session�III. The Third Plenary�Session titled, “Heterogeneity In The Cost-Effectiveness Of Medical Interventions: The Challenge Of Matching Patients To Appropriate Care” featured speakers Karl C. Claxton, MSc, DPhil, Professor & Senior Research Fellow, Centre for Health Economics, University of York, Heslington, York, UK; Andreas Gerber, PhD, MD, Head, Department of Health Economics, Institute of Quality and Efficiency in Health Care (IQWiG), Cologne, Germany; and Greg Rossi, PhD, Vice President, Payer Evidence, AstraZeneca, Macclesfield, Cheshire, UK. The session was moderated by Uwe Siebert, MD, MPH, MSc, ScD, Professor & Chair, Department of Public Health, Medical Decision Making and Health Technology Assessment, UMIT - University of Health Sciences, Medical Informatics and Technology and Oncotyrol Center for Personalized Cancer Medicine, Hall/Innsbruck, Austria. The session discussed issues with heterogeneity and presented perspectives of the researcher, the payer, and a manufacturer of companion diagnostic and drug combinations.
Workshop�Sessions�IV�&�V and the final viewing of exhibits and Poster session iii concluded the Congress.
ISPOR will gather again on June 2-6, 2012 in Washington, DC, USA for the ISPOR 17th Annual International Meeting. We hope to see you there and thanks for attending the ISPOR meetings this year!
ISPOR cORNER
ISPOR 14th annual European congress – !Hala Madrid! Stephen L. Priori, Director, ISPOR Publications
ISPOR President Mark Sculpher, MSc, PhD (r) presenting ISPOR 14th European Congress Program Chair Xavier Badia, PhD, MD, MPH, with a distinguished service award as Congress Program Chair.
14th annual European congress Program committee chairs Program committee chairXavier�Badia,�PhD,�MD,�MPH,�Global Leader, Observational COE & Senior Principal, HEOR, IMS Health, Barcelona, Spain
research review committee co-chairs:Jan�J.V.�Busschbach�PhD,�Interim Director, Department of Medical Psychology & Psychotherapy, Erasmus MC, Rotterdam, The Netherlands Dominik�Golicki,�MD,�PhD,�MA, Partner, HealthQuest sp z o.o., Warsaw, Poland Michael�Schlander,�PhD,�MD,�MBA,�Chairman & Scientific Director, Institute for Innovation & Valuation in Health Care (InnoVal), Wiesbaden, Germany Erkki�Soini�MSc,�RN, Chief Executive Officer, ESiOR Ltd., Kuopio, Finland
Workshop�Review�Committee�Co-Chairs:Fernando�Antoñanzas,�MA,�PhD,�Economist, Department of Economics, University of La Rioja, Logrono, SpainNancy�J.�Devlin,�PhD, Director of Research, Office of Health Economics, London, UK
decision-maker case study review committee chair: Antoni�Gilabert�Perramon,�PhD,�Managing Director of Pharmaceutical Care and Complementary Benefits, Catalan Health Service, Department of Health and Social Security, Government of Catalonia, Barcelona, Spain
Issue�Panel�Review�Committee�Co-Chairs:Peter�Hertzman,�PhD, Executive Director, HEOR, BMS Europe, Rueil Malmaison, FranceJacco�Keja,�PhD, Regional Leader, EMEA, HEOR, IMS Health, London, UK and Lecturer in Life Sciences Pricing and Management, Institute for Health Policy and Management, Erasmus University, Rotterdam, The Netherlands
IC

Developing Good Research Practices for Performance-Based Risk-Sharing Agreements Forum (l-r): Adrian Towse, MA, MPhil, J.L. (Hans) Severens PhD, Gerard de Pouvourville, PhD, and Jens Grueger, PhD.
ISPOR 14th AnnuAl
Congress Exhibitors’ Reception
Second Plenary Session speakers (l-r): Leslie Levin, MD, FRCP(Lon), FRCPC, Patrick Keohane, MB, BS, MRCP(UK), and Enrique Bernal-Delgado, MD, PhD
First Plenary Session: Pros and Cons of a Centralized European Pricing & Reimbursement Agency
Third Plenary Speaker Karl C.
Claxton, MSc, DPhil
photo
14 November/December 2011 ISPOR cONNEcTIONS

EuROPEAn COngRESS
Congress attendees during breakout in-between sessions
Third Plenary Session: Heterogeneity In The Cost-Effectiveness Of Medical Interventions: The Challenge Of Matching Patients To Appropriate Care
gallery
Madrid classical guitarists performing at Congress Social Event
Congress Poster Session
First Plenary Session Speakers Hans-Georg Eichler, MD, MSc (l) and Adrian Towse, MA, MPhil
Introduction to Modeling Short Course
November/December 2011 ISPOR cONNEcTIONS 15

16 November/December 2011 ISPOR cONNEcTIONS
14th annual European congress Research Presentation award Recipients
The ISPOR Best Research Podium and Poster Presentation Awards were established in 1998 to recognize the scientific merit of podium and poster presentations at the ISPOR Annual International Meetings, Annual European Congresses, Latin America and Asia-Pacific Conferences. At this year’s European Congress, the ISPOR Awards Committee evaluated 60 podium presentations and over 1,400 poster presentations. Evaluations of scientific merit were based upon the following criteria:
Background provides appropriate perspective/context for the subject •Objectives / research questions are clearly stated •Research design / methods / modeling is appropriate and transparent •(scores on this will determine winners in case of ties) Data sources and/or sampling procedures are clear and appropriate •Data analyses are appropriate •Research objectives are met/addressed •Implications of findings are discussed •Factual information is kept separate from interpretations or implications •Abstract is presented in an unbiased manner •Clarity of presentation •
The recipients are:
BEST PODIUM RESEaRcH PRESENTaTION aWaRDSut1: coMbining dce and tto into a single value Functionvan Hout ba1,�Oppe M2, 1University of Sheffield, Sheffield, UK, 2iMTA, Rotterdam, The Netherlands
HT4:�WHAT�DETERMINES�THE�RECOMMENDATIONS�ISSUED�BY�POLISH�HEALTH�TECHNOLOGY�AGENCY�(AHTAPOL)?�niewada M,�Polkowska MA, Jakubczyk M, Golicki D, HealthQuest, Warsaw, Poland
HT3:�UNDERSTANDING�THE�COMPLEXITY�OF�HTA�NETWORKSandreykiv M1,�Van Engen A1, Wiebinga C1, Zorzi O1, Mark R2, 1Quintiles, Hoofddorp, The Netherlands, 2Ni3 AG, Zürich, Switzerland
BEST NEW INvESTIgaTOR RESEaRcH PRESENTaTION PODIUM aWaRDS PC3:�BREAST�AND�PROSTATE�CANCER�PRODUCTIVITY�COSTS:�A�COMPARISON�oF tHe HuMan caPital aPProacH and Friction cost aPProacH Hanly�P,�Timmons A, Walsh P, Sharp L, National Cancer Registry Ireland, Cork, Ireland
HG2:�CHARACTERIZING�THE�INDIVIDUAL�COURSE�OF�HEALTH-RELATED�QUALITY�oF liFe aFter subaracHnoid HeMorrHageWinter�Y1,�Klotsche J2, Ringel F3, Spottke A4, Gharevi N4, Klockgether T4, Schramm J4, Urbach H4, Wittchen HU2, Rehm J2, Meyer B3, Dodel R1, 1Philipps-University, Marburg, Germany, 2Technical University Dresden, Dresden, Germany, 3Klinikum Rechts der Isar, Technical University, Munich, Germany, 4University of Bonn, Bonn, Germany
ad3: assessing tHe coMPliance and Persistence oF allergen IMMUNOTHERAPY�IN�ALLERGIC�RHINITIS�USING�A�RETROSPECTIVE�PHARMACY�database FroM tHe netHerlandsKiel�MA1,�Gerth van Wijk R2, Röder E2, Al MJ1, Hop WC2, Rutten-van Mölken MP1, 1Erasmus University, Rotterdam, The Netherlands, 2Erasmus Medical Center, Rotterdam, The Netherlands
ISPOR cORNER
ISPOR 14th annual European congress Scientific awards RecipientsStephen L. Priori, Director, ISPOR Publications
ISPOR award for value in Health Paper of the Year
The ISPOR Award for Value in Health Paper of the Year was established in 2011 to promote quality research, originality, and utility in health care decisions for articles published in Value in Health. The award is given to the best paper published in Value in Health (hard copy) in the previous calendar year.
The 2011 recipient of the ISPOR Award for Value in Health Paper of the Year is:
Anthony.�E.�Ades,�PhDProfessor of Public Health Science, University of Bristol, UK“Network�Meta-Analysis�with�Competing�Risk�outcomes” Value Health 2010;13:976-83.
A Special thanks to the Value in Health Editorial Board for selecting the recipient!
2011 ISPOR Research Excellence awards
The recipients of the 2011 ISPOR Research Excellence Award (one for Methodology Excellence and one for Application Excellence) are selected by the Awards Committee based upon publications that have appeared in respected peer-review journals and other communication venues (e.g., books, reports) during the preceding 12 months from January 1 of the year awarded. The award selection is based upon the publication’s clear description of methods, along with the appropriate and creative applications (or proposal thereof in conceptual methodology work) of techniques to answer important questions in the field of pharmacoeconomics and outcomes research. Such publications will be expected to have much impact on the field, due to their acceptance and application by others.
The 2011 recipient of the ISPOR Award for Excellence in Methodology in Pharmacoeconomics and Health Outcomes Research is:
Martin�Hoyle,�PhDSenior Research Fellow, Peninsula College of Medicine & Dentistry (PCMD), Universities of Exeter and Plymouth, Exeter, UK, as the senior author of the research paper:
“Whose�Costs�and�Benefits?�Why�Economic�Evaluations�Should�Simulate�Both�Prevalent�and�All�Future�Incident�Patient�cohorts” Med Decis Making 2010;30:426-37.
A Special thanks to Rajesh�Balkrishnan,�PhD,�MS, Chair, ISPOR Research Excellence Award in Methodological Excellence and the Research Excellence Award Committee for selecting the recipient!

November/December 2011 ISPOR cONNEcTIONS 17
BEST STUDENT RESEaRcH PRESENTaTION PODIUM aWaRDS RS3:�EVIDENCE,�PROCESS�OR�CONTEXT?�EXAMINING�THE�FACTORS�THAT�DRIVE�COVERAGE�DECISIONS�OF�PHARMACEUTICALS�BY�HEALTH�TECHNOLOGY�ASSESSMENT�BODIES�IN�EUROPEcerri K, Fernández JL, Knapp M, London School of Economics and Political Science, London, UK
HG4:�THE�VALUE�OF�HETEROGENEITY�FOR�COST-EFFECTIVENESS�SUBGROUP�ANALYSIS:�THEORETICAL�FRAMEWORK�AND�APPLICATION espinoza M, Manca A, Claxton K, Sculpher MJ, University of York, Heslington, York, UK
DA4:�FINDING�TREATMENT�EFFECTS�WITHIN�SUBGROUPS�WHEN�USING�THE�PROPENSITY�SCORE�TO�CONTROL�FOR�SELECTION�BIAS:�A�MONTE�CARLO�SIMULATION�STUDY�van eeren H1, Spreeuwenberg MD2, van Manen JG3, de Rooij M4, Stijnen T5, Busschbach J1, 1Erasmus University Medical Center, Rotterdam, The Netherlands, 2Maastricht University, Maastricht, The Netherlands, 3Viersprong Institute for Studies on Personality Disorders, Halsteren, The Netherlands, 4Methodology and Statistics Unit, FSW, Leiden University, Leiden, The Netherlands, 5Department of Medical Statistics & Bioinformatics, Leiden University Medical Center, Leiden, The Netherlands
BEST RESEaRcH PRESENTaTION POSTER aWaRDS PIH39:�HOW�DO�POSTMENOPAUSAL�WOMEN�DESCRIBE�BREAST�PAIN�AND�BREAKTHROUGH�BLEEDING�ASSOCIATED�WITH�HORMONAL�TREATMENTS�FOR�MENOPAUSAL�SYMPTOMS:�QUALITATIVE�INTERVIEWS�WITH�POSTMENOPAUSAL�WOMEN�IN�THE�UNITED�STATES,�CHINA,�MEXICO�AND�ITALYabraham l1, Arbuckle R2, Dennerstein L3, Humphrey L2, Maguire L2, Mirkin S4, Simon JA5, Symonds T1, Walmsley S2, 1Pfizer Ltd., Tadworth, Surrey, UK, 2Mapi Values Ltd., Bollington, Cheshire, UK, 3University of Melbourne, Melbourne, VIC, Australia, 4Pfizer Inc, Collegeville, PA, USA, 5George Washington University, Washington, DC, USA
PMs30: cost-eFFectiveness oF tociliZuMab coMPared to standard tHeraPeutic seQuences For tHe treatMent oF MODERATE/SEVERE�RHEUMATOID�ARTHRITIS�(RA)�PATIENTS�IN�Portugal Diamantopoulos�A1, Andrade S2, Bernardo A3, Branco J4, Inês L5, Pereira da Silva JA6, Santos MJ7, Monteiro I8, 1Symmetron Limited, London, UK, 2KeyPoint Group, Lisbon, Portugal, 3Hospital de São João, E.P.E, Oporto, Portugal, 4Centro Hospitalar Lisboa Ocidental – Hospital Egas Moniz, Lisbon, Portugal, 5Hospitais da Universidade de Coimbra, EPE, Coimbra, Portugal, 6Centro Hospitalar de Lisboa Norte – Hospital de Santa Maria, Lisbon, Portugal, 7Hospital Garcia de Orta, E.P.E., Almada, Portugal, 8Roche Farmacêutica Química, Lda., Amadora, Portugal
PRS4:�ECONOMIC�BURDEN�ATTRIBUTABLE�TO�OBESITY�IN�ADULT�PATIENTS�WITH�ASTHMA�IN�THE�US�Suh�DC1, La HO2, Barone J3, Chang CW3, Kim CM2, 1College of Pharmacy, Chung-Ang University, Seoul, NJ, South Korea, 2Catholic University College of Medicine, Seoul, South Korea, 3Rutgers University, Piscataway, NJ, USA
BEST NEW INvESTIgaTOR RESEaRcH PRESENTaTION POSTER aWaRDSPIN74:�A�COST-EFFECTIVENESS�ANALYSIS�OF�VACCINATING�THE�ELDERLY�WITH�23-VALENT�PNEUMOCOCCAL�POLYSACCHARIDE�VACCINE�(PPV23)�IN�GERMANY� Jiang�Y1,�Gauthier A1, Annemans L2, van der Linden M3, Nicolas-Spony L4, Bresse X4, 1Amaris Consulting UK, London, UK, 2Ghent University, Ghent, Belgium, 3National Reference Centre for Streptococci, Aachen, Germany, 4Sanofi Pasteur MSD, Lyon, France
PIN2:�SAFETY�AND�EFFICACY�OF�TENOFOVIR�AS�COMPARED�TO�OTHER�NUCLEOT(S)IDE�ANALOGUES�IN�THE�TREATMENT�OF�CHRONIC�HEPATITIS�
B�–�A�SYSTEMATIC�REVIEW�WITH�MIXED�TREATMENT�COMPARISON Wojciechowski�P1,�Stozek A1, Szmyd J1, Gwiosda B1, Mierzejewski P2, Kazmierski M2, Rys P1, Wladysiuk M1, Plisko R1, 1HTA Consulting, Krakow, Poland, 2Gilead Sciences Poland Sp. z o.o., Warszawa, Poland
Pin96: does connecting tobacco cessation intervention in TUBERCULOSIS�CARE�IMPROVE�QUALITY�OF�LIFE�OUTCOMES? awaisu a1,�Nik Mohamed MH2, Noordin NM3, Abd. Aziz N4, Syed Sulaiman SA5, Ahmad Mahayiddin A6, Muttalif AR7, 1Qatar University, Doha, Qatar, 2International Islamic University of Malaysia, Kuantan, Pahang, Malaysia, 3National Institute of Health, Kuala Lumpur, Malaysia, 4Universiti Technology Mara, Puncak Alam, Malaysia, 5University Sains Malaysia (USM), Pinang, Malaysia, 6Institut Perubatan Respiratori, Kuala Lumpur, Malaysia, 7Penang Hospital, Penang, Malaysia
BEST STUDENT RESEaRcH PRESENTaTION POSTER aWaRDSPCN168:�COST-EFFECTIVENESS�ANALYSIS�OF�DIFFERENT�CERVICAL�cancer Prevention aPProacHes in tHe united states Qiao n, noyes K,�Dolan�JG,�University of Rochester School of Medicine and Dentistry, Rochester, NY, USA
PRM57:�REVISITING�HPV�VACCINATION:�WHY�EXISTING�CEAS�UNDERESTIMATE�THE�VACCINE’S�COST-EFFECTIVENESS�AND�INCORRECTLY�ESTIMATE�ITS�THRESHOLD�PRICE�O’Mahony�J, Erasmus University Medical Center, Rotterdam, The Netherlands
PHP60:�DRUG-RELATED�MORBIDITY�–�MODELING�THE�COST-OF-ILLNESS�IN�SWEDEN�USING�PHARMACISTS’�OPINION Gyllensten�H1,�Hakkarainen KM1, Jönsson AK2, Andersson Sundell K1, Hägg S2, Rehnberg C3, Carlsten A1, 1Nordic School of Public Health, Gothenburg, Västra Götaland, Sweden, 2Linköping University and the County Council of Östergötland, Linköping, Östergötland, Sweden, 3Karolinska Institutet, Stockholm, Stockholm, Sweden
A special thanks goes to all the judges, the ISPOR Annual European Congress Research Presentation Awards Chairs as well as the ISPOR Awards Committee Chairs who volunteered their time and efforts in selecting the recipients.
isPor 14th�ANNUAL�EUROPEAN�CONGRESS�RESEARCH�AWARDS�cHairs: Podium (and filling in for Tomáš�Doležal,�MD,�PhD�as Poster chair at the Congress): Zoltan�Kalo,�PhD,�MD,�MSc, Director, Health Economics Research Unit, Eotvos Lorand University, Budapest, Hungary.
ISPOR JUDGES: Sarah Acaster, Zuleika Aponte, Rajesh Balkrishnan, Anthony Batty, Claus Becker, Mark Belger, Matthew Bending, Isabelle Borget, Bernhard Bornschein, Daniel Callejo Velasco, Sean Candrilli, Rod da Silva, Sarah Dewilde, Michelle Erdmann, Alex Exuzides, Liberty Fajutrao, Walid Fakhouri, William Gerth, Neil Hawkins, Isabel Henkel, Tove Holm-Larsen, Ian Johnson, Eva Kaltenthaler, Shital Kamble, Angela Kempel, Guvenc Kockaya, Kathrin Kreyenberg, Amit Kulkarni, Paola Lanati, Ji-Young (Lauren) Lee, Nicky Lieberman, Frank Liu, Andrew Lloyd, Jane Loftus, Peter Lynch, Marta Manso, Stephanie Manson, Aurélie Millier, Ateesha Mohamed, Jorgen Moller, Patrick Mollon, Andre Daniel Morais, Christel Naujoks, Maryam Navaie, Claudia Nicolay, Michael Ortiz, Marie-Angel Paget, Olaf Pirk, Robert Plisko, Barbara Polek, Neil Pumford, Dennis Raisch, Karen Rascati, Aran Ratcliffe, Regina Rendas-Baum, Erna Ribnicsek, Lance Richard, Diego Rosselli, Michel Rotily, Stephane Roze, Mason Russell, Evelyn Sarnes, Margarita Schultz, Karin Sennfalt, Julian Shepelev, Sonya Snedecor, Caitlyn Solem, Nyree Sweeney, Tomas Tesar, Louise Timlin, Alexander Tolkushin, Ilse Truter, Marco Turini, Nayanabhirama Udupa, Birgitta von Schéele, John Walker, Ruth Whittington, Hazel Wohlfarht, Andrew Xia, Vlad Zah, Lin Zhan, Keary Zhou IC

2-4 September 2012 Taipei, Taiwan
ISPOR 5th ASIA-PAcIfIc cOnfeRence
fOR InfORmATIOn vISIT : www.ispor.org
Evidence Requirements by Different Stakeholders for Health Care Decisions in Asia-Pacific
Conference Co-Chairs: Yen-Huei (Tony) Tarn, MS, PhD, Executive Director, Center for Pharmaceutical Care Development, Taiwan Pharmacist Association, Taipei, TaiwanChien-Jen Chen, ScD, Academician & Distinguished Re-search Fellow, Genomics Research Center, Academia Sinica and Professor, National Taiwan University, Taipei, Taiwan
Research Review Committee Co-Chairs: Ming-Chin Yang, DrPH, Associate Professor, School of Public Health, National Taiwan University, Taipei, Taiwan
Mohammad Abdollahi, PhD, PharmD, Professor, Faculty
of Pharmacy, Tehran University of Medical Science (TUMS), Tehran, Iran
Health Care Decision-Maker Case Study Review Committee Co-Chairs: Nilakantha Bhoi, PharmD, MBA, WHO Technical Consultant, and Procurement & Supply Chain Management (PSM), Ministry of Health & Family Welfare, New Delhi, IndiaJeonghoon Ahn, PhD, Senior Director, Office of Health Technology Assessment, National Evidence-Based Healthcare Collaborating Agency, Seoul, South Korea
Workshop Review Committee Co-Chairs: Wen Chen, PhD, Professor and Deputy Dean, School of Public Health, Fudan University, Shanghai, ChinaAnwarul Hassan Gilani, MSc, PhD, HEC Distinguished National Professor and Director, Medical College, Aga Khan University, Karachi, Pakistan
Issue Panel Review Committee Co-Chairs: Nathorn Chaiyakunapruk, PhD, PharmD, Associate Professor, School of Pharmacy, Naresuan University, Phit-sanulok, ThailandBruce Crawford, MPH, MA, General Manager, Asia, Mapi Values, Tokyo, Japan
CO-ORGANIZED BY• ISPOR Asia Consortium• Center for Drug Evaluation• Taiwan Society for Pharmacoeconomics
and Outcomes Research
• Bureau of National Health Insurance• Chinese Pharmaceutical Association• International Research-Based Pharmaceutical
Manufacturers Association (Taiwan-IRPMA)• National Yang-Ming University
• National Taiwan University• Pharmaceutical Society of Taiwan• Taipei Medical University• Taiwan Pharmacist Association• Taiwan Society of Health-System Pharmacists
CONFERENCE SUPPORTING INSTITUTIONS (as of November 30, 2011)
ExhIBITOver 800 attendees in 2010!Present your products and services to key outcomes researchers and health care decision-makers in pharmaceutical, medical device & diagnostics, biotechnology industries, clinical practice, government agencies, academia, and health care organizations.
Benefits to Exhibitors:• Listing & 1/4 page advertisement in the Program & Schedule
of Events• Listing & 1/4 page advertisement on the ISPOR website• Complimentary conference registration• Pre-registrant mailing labels
EvENT SUPPORTIncrease your visibility! Give your company increased prominence. For information, please email: [email protected].
Benefits to Event Supporters:• Listing & ¼ page advertisement in
the Program & Schedule of Events• Listing & ¼ page advertisement on
the ISPOR website
CORPORATE SUPPORTISPOR provides opportunities for organizations to financially support the ISPOR 5th Asia-Pacific Conference. For further information, please email: [email protected].
Benefits to All Supporters:• Recognition at the Plenary Sessions• Recognition in the Program &
Schedule of Events and ISPOR website
• Conference signage
EDUCATIONAl SYmPOSIAThese sponsored presentations are open to all delegates. The host organization chooses a subject of interest and arranges suitable speakers for the presentation. For further information, please email: [email protected].
cALL fOR ABSTRAcTS
CONFERENCE SUPPORT & PROmOTIONAl OPPORTUNITIES
ADvERTISEAdvertise in the Program & Schedule of Events!
CONFERENCE PROGRAm COmmITTEE
ABSTRAcT SuBmISSIOn DeADLIne: 22 mARch 2012 eARLY ReGISTRATIOn DeADLIne: 24 JuLY 2012

mORNING COURSES (8:00Am-12:00Pm)Introduction to PharmacoeconomicsCourse Description: This course is designed to teach clini-cians and researchers how to incorporate pharmacoeconomics into study design and data analysis. Participants will learn how to collect and calculate the costs of different health care treatments, determine the economic impact of clinical out-comes, and how to identify, track and assign costs to different types of health care resources used. The development of eco-nomic protocols and data collection sheets will be discussed. Different assessment methods including cost-effectiveness, cost-minimization, cost of illness, cost-utility and cost-benefit analysis will be introduced. The applications of pharmacoeco-nomics will be discussed and illustrated by practical examples. Level: Introductory-Intermediate. This course is designed for those with limited experience with pharmacoeconomics.
Introduction to ModelingCourse Description: This course will introduce pharmacoeco-nomic modeling techniques such as decision analytic modeling, Markov modeling, discrete event models, and other modeling techniques and their appropriate usages including a review of the ISPOR Modeling Good Research Practices. Examples will be presented using Microsoft Excel, with add on simulation soft-ware. This course will include practical steps in the selection of models and options in modeling of data inputs.Level: Introductory-Intermediate. This course is recommended as a prerequisite to the short course “Applied Modeling”.
Introduction to Retrospective Database Design and AnalysisCourse Description: Retrospective studies require strong principles of epidemiologic study design and complex analytical methods to adjust for bias and confounding. This course will provide an overview of fundamental design strategies, analytic techniques and specific best practices to improve causal inference in studies using retrospective databases. Specific topics to be covered at an introductory level include: measurement of exposure and outcome, causal graphs, new user study design, measures of comorbidity, the use of stratification analysis before multivariable modeling, multivariable regression including Cox proportional hazards survival analysis, model performance and diagnostic testing, propensity scoring, instrumental variable and structural mod-eling techniques including marginal structural models. Level: Introductory. This course is designed for those with little experience with database analysis.
New! Introduction to Health Technology AssessmentCourse Description: This course will introduce the key ele-ments, methods and terms of health technology assessment (HTA), and provide an overview of basic HTA disciplines including benefit assessment (biostatistics, clinical epidemiol-ogy, patient-relevant outcomes, risk-benefit assessment), economic evaluation (costing, cost-effectiveness analysis, pharmacoeconomic modeling, budget impact analysis, resource allocation), ethical, legal and social implications. Using real world HTA examples of drugs and devices, this course will review the practical steps involved in developing and using HTA reports in different countries and their health care systems. Group discussion will focus on the perspectives of different stakeholders and the implementation of HTA in decision-making.Level: Introductory. This course is suitable for those with little or no experience with HTA.
Introduction to Quality of Life Assessment/Patient-Reported OutcomesCourse Description: Definitions and concepts, methodolo-gies, and practical methods for measuring patient-reported
outcomes will be presented. The value of patient-reported outcomes assessment will be discussed. A strategy to aid in selecting appropriate instruments and the translation processes will be presented. Instrument development and validation will be discussed using practical examples and exercises, including “ISPOR Principles of Good Practice for the Translation and Cultural Adaptation Process for Patient-Reported Outcomes (PRO) Measures”. Level: Introductory-Intermediate. This course is designed for those with little experience with quality of life/PRO studies.
Meta-Analysis and Systematic Literature ReviewCourse Description: Meta-analysis may be defined as the statistical analysis of data from multiple studies for the pur-pose of synthesizing and summarizing results, as well as for quantitatively evaluating sources of heterogeneity and bias. A systematic literature review often includes meta-analysis and involves an explicit, detailed description of how a review was conducted. This course highlights and expounds upon four key areas: 1) impetus for meta-analysis and systematic reviews, 2) basic steps to perform a quantitative systematic review, 3) statistical methods of combining data, and 4) an introduction to methods for indirect comparisons. The material includes practical examples from the published literature relevant to pharmacoeconomic and PRO research. This course is designed for those with little experience with meta-analysis and includes interactive exercises. Level: Introductory-Intermediate. This course requires basic understanding of statistical method and is recommended as a prerequisite to the short course “Network Meta-Analysis and Indirectly Treatment Comparisons”
AFTERNOON COURSES (1:00Pm-5:00Pm)Financial Impact /Cost of IllnessCourse Description: This course will describe methods to determine the costs associated with a health condition and the budget impact of new technologies for that condition. The course will present incidence- and prevalence-based costing strategies. Treatment algorithms and event-based approaches will be demonstrated for disease-specific costs from different decision-maker perspectives. Both static and dynamic meth-ods for estimating the budget impact of adding a new drug to a health plan formulary will be presented. Issues related to imputing missing data will also be discussed. Level: Intermediate. This course is designed for those with some experience with pharmacoeconomic analysis.
New! Statistical Considerations in Clinical Trials and Economic EvaluationsCourse Description: Adoption and diffusion of new medical treatments depend increasingly on robust analysis of costs and cost-effectiveness (CEA). This course will discuss design issues for the collection of primary economic data in clinical trials as well as statistical considerations, including the effect of distributional assumptions, univariate and multivariable analyses of data, sample size and power calculations, and estimation of sampling uncertainty for cost-effectiveness analysis. Examples will be provided to illustrate concepts, as well as a discussion of the ISPOR Good Research Practices on CEA alongside Clinical Trials. Level: Introductory-Intermediate. This course is designed for those with a basic understanding of statistics.
Transferability of Cost-Effectiveness Data between CountriesCourse Description: This course will discuss factors that make economic data more difficult than clinical data to adapt from other countries and the evidence on the variability of cost-effectiveness results across countries. Potential methods to provide solutions will be reviewed and their pros and
cons will be discussed, including the ISPOR Good Research Practices for transferability of economic evaluations across jurisdictions. Finally, emerging international guidance for deal-ing with issues of transferability will be discussed. Level: Intermediate. This course is designed for those with basic understanding of economic evaluations of health care and experience in the critical assessment of cost-effectiveness studies.
Applied ModelingCourse Description: This course is a hands-on introduction to the use of software in the creation and analysis of cost-effectiveness decision models. The basic techniques for deci-sion tree modeling, simple Markov modeling and Monte Carlo simulation will be introduced. Useful techniques to manage variables and tables in the TreeAge Pro, and to develop Excel dashboard with be demonstrated. This course will also include discussions of ISPOR Modeling Good Research Practices. Level: Intermediate-Advanced. This course is suitable for those who are familiar with the various modeling methods and the short course “Introduction to Modeling” is recommended as a prerequisite for this course. All participants must bring a Windows laptop computer with a copy of TreeAge Pro Suite installed and running. You will be provided download and installation instructions when you pre-register for the course.
Pharmaceutical/Biotech Pricing & Reimburse-ment MethodologiesCourse Description: This course gives participants with a basic understanding of the key terminology and issues involved in pricing decisions and the principles of reimburse-ment methodologies. It covers the tools to document product value, the role of pharmacoeconomics and the differences in payment systems that help pricing decisions. Recent phar-maceutical spending patterns, trends and cost-containment measures will also be discussed taking account of the wider policy context. The pricing and reimbursement systems in Taiwan, South Korea, Thailand, China Mainland and other Asian countries/regions will be in-depth discussed. The case from Australia will be introduced as well.Level: Introductory-Intermediate. This introductory course is designed for those with limited experience in pharmaceutical pricing and reimbursement.
New! Network Meta-Analysis and Indirect Treatment ComparisonsCourse Description: Network meta-analysis provides an integrated and unified analysis that incorporates all direct and indirect comparative evidence about treatments, which is especially useful when there’s little or no evidence from direct comparisons. When head to head randomized controlled trials are absent, network meta-analysis offers a quantita-tive method of integrating all the data from all the available comparisons while indirect treatment comparisons can be conducted and provides useful evidence. In this course, the fundamentals and concepts of network meta-analysis will be presented. ISPOR Good Research Practices for Conducting and Interpreting Network Meta-Analysis and Indirect Treatment Comparisons will be presented. The evaluation of networks also presents special challenges and caveats, which will also be highlighted in this course. The material in this course is motivated by instructive and real examples. Case studies are implemented with the WinBUGS package. Level: Intermediate. This course is designed for those with some understanding of meta-analysis, and the short course “Meta-Analysis and Literature Review” is recommended as a prerequisite for this course.
Complete Short Course Descriptions Available at www.ispor.org
ShORT cOuRSeS Sunday, 2 September 2012
2-4 September 2012 n Taipei, Taiwan
ISPOR 5th ASIA-PAcIfIc cOnfeRence

cALL fOR ABSTRAcTSABSTRAcT SuBmISSIOn BeGInS: 23 JAnuARY 2012 / ABSTRAcT SuBmISSIOn DeADLIne: 22 mARch 2012
RESEARCh ABSTRACTS
Outcomes research on all health care interventions (including drugs, devices, behavioral modification programs, surgery, disease prevention, gene therapy, screening, diagnostic proce-dures and health education) and on all diseases or health disorders are considered. Research abstracts (except for conceptual papers) must be organized by OBJECTIVES, METHODS, RESULTS, CONCLUSIONS. All accepted research abstracts are published in Value in Health as submitted. Accepted research is presented as a 15 minute podium presentation or poster presentation (with a poster author discussion hour). Abstracts are evaluated on the quality of the study (or concept) and quality of the abstract presentation. Research topics include: Clinical Outcomes Studies, Cost Outcomes Studies, Patient-Reported Outcomes/Preference-based Studies, Health Care Use & Policy Studies, Research on Methods, Conceptual Papers. See the ISPOR website for research subtopics, diseases and health care treatments.
ISSUE PANEl PROPOSAlS
Issue panel proposals should show real debate on new or controversial issues in health economics and outcomes research or real debate on the use of outcomes research in health care decision-making. Issue panel proposals must be organized MODERATOR, PANELISTS, ISSUE, OVERVIEW. An accepted issue panel is one hour in duration with a moderator and 2-3 panel-ists representing different organizations. Panelists should present distinct views about the topic. Issue Panel topics are: Clinical Outcomes Research Issues, Economic Outcomes Research Issues, Patient-Reported Outcomes Research Issues, Health Policy Development Using Outcomes Research Issues.
WORkShOP PROPOSAlS
Workshop proposals should show novel and innovative experiences in the conduct of outcomes research (including, but not limited to, experiences with conjoint analysis, large database analysis, modeling, observational studies, record review, surveys, sensitivity analysis and patient registries) or novel and innovative experiences in the use of outcomes research (clinical, economic, or patient-reported/preference-based outcomes) in health care policy development. Workshop proposals must be organized by DISCUSSION LEADERS, PURPOSE, DESCRIPTION. Accepted workshops are one hour in duration with a minimum of 2 and maximum of 4 discussion leaders (more than one organization must be represented). An audience interactive element must be included in the proposal and during the workshop. Workshop topics include: Clinical Outcomes Research, Economic Outcomes Research, Patient-Reported Outcomes/Preference-based Research, Use of Real World Data, Health Policy Development Using Outcomes Research. See the ISPOR website for workshop subtopics.
hEAlTh CARE DECISION-mAkER CASE STUDY ABSTRACTS
Health care decision-maker case study abstracts must describe an organization’s attempt to integrate cost or outcomes research information into their health care organization’s processes and procedures. Case Study abstracts must be organized: ORGANIZATION, PROBLEM OR ISSUE ADDRESSED, GOALS, OUTCOMES RESEARCH USED IN THE DECISION, RESULTS, LESSONS LEARNED. Negative as well as positive results are encouraged. Accepted case studies are presented as a 20 minute podium presentation or poster presentation (with a poster author discussion hour). THE PRESENTER MUST BE A HEALTH CARE DECISION-MAKER.
MONDAY, 3 SEPTEMBER 8:30AM-7:00PMFirst Plenary Session: Health Technology Assessment in The Significantly evolving Health Care Systems in AsiaHealth technology assessment (HTA) is a multidisciplinary process that summarizes information about the medical, social, economic and ethical issues related to the use of a health technology in a systematic, transparent, unbiased, robust way [ref: EUnetHTA]. To ensure the HTA process is successful, a health system needs the infrastructure and human capacity, adequate data sources, PE/HTA guidelines, and an understanding of the methods used in HTA. In addition, in Asia, health systems are significantly changing and resources are severely limited. Therefore, conducting or evaluating a health technology in Asia is a real challenge. This session will discuss the key building blocks in the development of a HTA process in the Asian context and the role of HTA in improving the health care systems in Asia.
Second Plenary Session: Involving Patients & Health Care Providers in Health Care Decisions: Learning from each OtherHealth technology assessment (HTA) in Asia is a process that mainly involves specialized experts from academia, industry, and government agencies. One common observation across the region is the limited or lack of involvement by patients or health care providers in the process. If the policy of “Those conducting HTAs should actively engage all key stakeholder groups” should be established, patients and health care providers should play a significant role. In Europe, for example, the UK’s NICE Citizens’ Council provides valuable impute on contentious subjects, and European Patients’ Forum collectively lobbies for patient’s rights, including equity and access to health care technology. In this session, international experience on how views of patients and health care providers are incorporated into HTA and health care coverage decisions will be shared, and how it can be adapted in Asia will be discussed and debated.
TUESDAY, 4 SEPTEMBER 8:30AM-6:00PMThird Plenary Session: Challenges of Adopting New Innovative Technologies in Health Care Coverage Decision-Making in AsiaA constant dilemma faced by payers is limited resources they have versus the increasing demands for health technologies, whether the technology can be of high value to targeted thera-pies, therapeutic devices and diagnostic products, or surgical procedures. Novel strategies have been developed and to a lesser extent, implemented in some countries, to ease the tension caused by this dilemma. Examples include coverage with evidence development, risk sharing or performance-based agreement, and others. Speakers in this session will share the recent developments of novel strategies for adopting new technologies, pros and cons, and their potentials to be implemented in Asia.
*40 ReSeARch PODIum PReSenTATIOnS *5 ISSue PAneLS *15 WORkShOPS *300 ReSeARch POSTeR PReSenTATIOnS
SUBmISSION INSTRUCTIONSAll abstracts and proposals MUST be submitted through ISPOR’s online abstract submission system by 22 March 2012.
Abstracts accepted for other ISPOR meetings can NOT be submitted and research published or presented at other national or international meetings is discouraged.
All accepted research abstracts are published in Value in Health SUBMISSION INSTRUCTIONS, EXAMPLES & SPECIFIC EVALUATION CRITERIA AVAILABLE AT www.ispor.org
PReLImInARY PROGRAm OvER 800 ATTENDEES
IN 2010!
2-4 September 2012 n Taipei, Taiwan
ISPOR 5th ASIA-PAcIfIc cOnfeRence

PAYmenT InfORmATIOn
NAME DEGREES MEMBER ID#
POSITION ORGANIzATION
MAILING ADDRESS
CITY STATE/PROVINCE ZIP COUNTRY
TELEPHONE FAx EMAIL
ShORT cOuRSe ReGISTRATIOn: 2 September 2012
cOnfeRence ReGISTRATIOn: 3-4 September 2012
ReGISTRATIOn feeS
mail Details: If not paying by credit card online, send registration form and payment to: International Society for Pharmacoeconomics and Outcomes Research, 3100 Princeton Pike, Building 3 Suite E, Lawrenceville, New Jersey 08648, USA Tel: 1-609-219-0773 Fax: 1-609-219-0774 • E-Mail: [email protected] • Internet: www.ispor.org Payment Details: Payment may be made by check, travelers check, bank transfer (there is a USD $40 charge) or credit card. VISA, MasterCard, or American Express will be charged in US dollars. Signature, account number and expiration date must be included. Non-US checks written in US$ on banks with a US counterpart are at no charge. For Non-US checks
written in US$ on banks with NO US counterpart there is USD $25 charge. Phone charges will NOT be accepted. If payment is being made by your company, please make sure your name is indicated on the check stub or correspondence. For bank transfers, please designate the registration name and/or registration number.Cancellation Details: Cancellation fee before 24 July 2012 is US $100. No refunds given after 24 July 2012.
Please enclose a check payable in US dollars to: International Society for Pharmacoeconomics and Outcomes Research or ISPOR and send to the ISPOR address given
below or charge to: m VISA m MasterCard m American Express
Account Number: ______________________________________________________ Expiration Date: ___________
Name: ______________________________________________________________ Authorized Signature: _______________________________________________
fOR mORe InfORmATIOn: www.ispor.org
Registration Before 24 July 2012 Standard: TWD12,000 (US$418)Full-Time Government, Academia and Practitioners: General: TWD7,500 (US$262) Taiwan local: TWD3,750 (US$131)Full-Time Student: General: TWD2,500 (US$87) Taiwan local: TWD1,250 (US$44)
Registration After 24 July 2012 Standard: TWD15,000 (US$524)Full-Time Government, Academia and Practitioners: General: TWD9,000 (US$314) Taiwan local: TWD4,500 (US$157)Full-Time Student: General: TWD3,000 (US$105) Taiwan local: TWD1,500 (US$52)
Taiwan Local: Individuals residing in Taiwan.
All Courses Are Offered in English
morning Courses (8:00Am-12:00Pm)q Introduction to Pharmacoeconomicsq Introduction to Modelingq Introduction to Retrospective Database Design and Analysisq New! Introduction to Health Technology Assessmentq Introduction to Quality of Life Assessment/Patient-Reported Outcomes q Meta-Analysis and Systematic Literature Review
Afternoon Courses (1:00Pm-5:00Pm)q Financial Impact/Cost of Illnessq New! Statistical Considerations in Clinical Trials and Economic Evaluationsq Transferability of Cost-Effectiveness Data between Countriesq Applied Modelingq Pharmaceutical/Biotech Pricing & Reimbursement Methodologiesq New! Network Meta-Analysis and Indirect Treatment Comparisons
QTY FEE TOTAL Short Course Registration (2 September 2012)
Conference Registration(3-4 September 2012)
*ISPOR Membership Registration: Option 1
*ISPOR Membership Registration: Option 2
Total Registration Fee
*ISPOR Membership (optional)Member
q Option 1: US$140 (TWD4,015) per year – a 1-year online subscription to Value in Health, including access to all past issues
q Option 2: US$275 (TWD7,887) per year – a 1-year subscription to Value in Health online & hard copy, including access to all past issues
Student Member
q Option 1: US$35 (TWD1003) per year – a 1-year online subscription to Value in Health including access to all past issues
q Option 2: US$105 (TWD3,011) per year – a 1-year subscription to Value in Health online & hard copy, including access to all past issues
Full ISPOR Membership benefits available at: www.ispor.org
Exchange rate as of May 2011 (28.66TWD = 1USD). The shaded boxes should be used as a reference. All credit card payments to ISPOR are charged in US$ at the exchange rate prevailing at the time of the transition. Due to this exchange, credit card statements may vary slightly.
ShORT COURSE FEES (PER COURSE)Registration Before 24 July 2012Regular: TWD3,000 (US$105) Full-Time Student: TWD1,500 (US$52)Full-Time Student (Taiwan local): TWD750 (US$26)
Registration After 24 July 2012Regular: TWD6,000 (US$209) Full-Time Student: TWD3,000 (US$105)Full-Time Student Taiwan local: TWD1,500 (US$52)
Taiwan Local: Individuals residing in Taiwan.
2-4 September 2012 n Taipei, Taiwan
ISPOR 5th ASIA-PAcIfIc cOnfeRence

18 November/December 2011 ISPOR cONNEcTIONS
ISPOR cORNER
Student corner – comparative Effectiveness Research: Opportunities and challengesMayank ajmera, MS, Doctoral Student and Sandipan Bhattacharjee, MS, Student and Research assistant, Department of
Pharmaceutical Systems and Policy, School of Pharmacy, West virginia University, Morgantown, Wv, USa
Comparative effectiveness research (CER) as described by the Institute of Medicine (IOM) is a real world comparison of treatment options
and identifying the best treatment available. The collection and evaluation of comparative effectiveness data would help the patients, clinicians and policy makers in making informed decisions. The crucial role of CER in improving individual and population health has been recognized nationally. Considering this development, the American Recovery and Reinvestment Act (ARRA) has approved $1.1 billion in the support of CER. In order to allocate the funding, the IOM created 100 high priority research topics which were further divided into four quartiles.
The federal funding for CER has been fiercely debated due to various concerns. As with any form of research, CER is associated with several untapped opportunities and severe challenges. As mentioned in the IOM report, CER paves our way for active involvement of patients, consumers and caregivers in research. This would not only help in improving health outcomes but also lead us to long anticipated concept of individualized medicine. With that in mind we also have to address the various challenges associated with CER. The most significant concern lies in the selection of appropriate methodologies to compare treatment options. Randomized controlled trials have long been the gold standard in determining the clinical efficacy of different treatments. RCT’s, however, have not provided us with answers regarding real world effectiveness of treatment alternatives. Various methodologies have been proposed which include modification of controlled trials to pragmatic/effectiveness trials, application of observational methods to CER, etc. These methods have their own pitfalls and thus it is necessary to apply a combinatorial approach. For example the CEASAR (Comparative Effectiveness Analysis of Surgery and Radiation in localized Prostate Cancer) study has used a hybrid observational study design to control for the limitations of traditional RCT’s and observational studies. The area of applying advanced methodologies to CER poses many research questions and consequently significant potential for researchers to develop study designs which could be appropriately applied to CER.
Furthermore, a major concern with CER is related to the dissemination and translation of the information obtained. The generated evidence needs to be provided to patients and clinicians in order for them to make informed decisions. The results from the CER studies require to be systematically channeled from the research setting to the real world clinical setting. In recent times these concerns have gained significant attention by the federal government especially by the Patient Centered Outcomes Research Institute (PCORI).
Lastly, the information obtained from CER should be used for improving patient care rather than rationing it. The health care rationing due to CER has been speculated over the past few years. CER supporters argue that the comparative information obtained in real world settings can profoundly influence and guide the clinical decisions. The ALLHAT (Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial) trial is an example of comparative effectiveness trial, which provided a good insight about the fact that there is no difference in effectiveness in decreasing significant cardiovascular outcomes for patients on older and generally low-cost drugs compared to those on newer medications. The critics of CER hold the view that application of evidence from the CER studies can result in ‘rationing’ of health care. There is, however, a third group (mainly comprising of physicians and patients) with an ideology that the inclusion of reimbursement schedules, managed care, and formulary management in the health care system has already rationed the health care, and this will stay oblivious to the advent of CER.
The CER proposes to be an effective solution to the United States health care problems. Nevertheless, the aforementioned concerns have to be addressed so that we can observe improvement in patients’ health outcomes as well as reduction in economic burden on the health care system. IC
WEB cONNEcTIONS
before you begin your health care or health intervention analysis visit the centre for Review and dissemination (cRd) website: http://www.york.ac.uk/inst/crd/index.htm.
cRd is part of the national Institute for health Research (nIhR) and is a department of the University of york. visiting the cRd website one will find research-based reports regarding the effects of health and social care interventions. cRd widely distributes their research findings, which have directly impacted health care policy and practice throughout the world. there are 3 main databases from cRd: nhS economic evaluation database (eed), database of abstracts of Reviews of effects (daRe), and hta database, which are all accessible on
their website. the nhS eed contains reports regarding the economic evaluation of health care interventions. these reports are developed to provide decision makers critical information that facilitates their interpretation of increasingly complex and technical literature. daRe focuses on systematic reviews that evaluate the effects of health care interventions and the delivery and organization of health services. the hta database focuses on completed and ongoing health technology assessments from around the world.
Do you know of any websites that you would like to share with the ISPOR community? If so, contact Bonnie M. Korenblat Donato, PhD, at: [email protected].

November/December 2011 ISPOR cONNEcTIONS 19
ISPOR cORNER
ISPOR Meeting Travel Scholarship award ReportsThe ISPOR Meeting Travel Scholarship Award (formerly International Fellowship Award) was established in 2006 to support travel to ISPOR meetings or regional conferences for ISPOR members residing in economically disadvantaged countries or regions of the world and to contribute to the development of pharmacoeconomics and outcomes research or the use of outcomes research in health care decisions in these countries or regions.
After the ISPOR Meeting Travel Scholarship Award experience, recipients submit a report outlining how they contributed to the development of pharmacoeconomics and outcomes research or the use of outcomes research in health care decisions in their own country/region based on this experience. The following are the reports of the Meeting Travel Scholarship recipients from the ISPOR 14th Annual European Congress held in Madrid, Spain, from 5-8 September 2011 (subsequent reports from recipients from the Madrid Congress that did not meet this issue’s deadline will appear in future issues).
Receiving a 2011 ISPOR Meeting Travel Scholarship Award has allowed me to help contribute to the development of pharmacoeconomics by raising awareness and improving the decision-making processes to make better use of health care resources in Egypt. This award gave me the opportunity to attend the ISPOR 14th Annual European Congress in Madrid, Spain and meet many excellent ISPOR experts and learn more about performing health technology assessments (HTA) and the economic evaluations.
During the Congress, I attended three short courses; one of which was “Cost Effectiveness Analysis alongside Clinical Trials.” This course was very useful to me as I am in the process of completing my PhD program. The second course I attended was “Patient Registries.” As a coordinator of a specialized committee for pharmaceutical products through the Central Administration for Pharmaceutical Affairs (CAPA), this course assisted me with the understanding of to incorporating outcomes research into the approval process of drugs. The last course, was on “Case Studies in Pharmaceutical/Biotech Pricing,” and presented the key steps for new product pricing with a focus on the need to closely integrate
the pricing, reimbursement and pharmacoeconomic strategy for the new product with the clinical development and marketing strategies as it will be very helpful for the decision makers in government. The plenary sessions covered an array of new skills and techniques for our region such as methods to assess heterogeneity in HTA and the use of real world data in decision making.
I was very interested in all of the Congress topics. This Congress also provided a great opportunity for health care decision makers, students, and researchers to meet discuss, and learn. I would like to express my gratitude to all of the ISPOR staff, as they were very helpful. Without their great efforts and effective organization, it would not have been possible for 3000 attendees to attend the many workshops, plenary sessions, issue panels, educational symposia and ISPOR forums.
As a Secretary and Treasurer of the ISPOR Egypt Regional Chapter, I am communicating with many leading universities to actively create academic courses in various disciplines of pharmacoeconomics to hopefully be part of a dedicated academic program. I met with the ISPOR Arabic Network at the Congress
and we agreed to collaborate with each other on many activities and projects in the Middle East. I am confident that the discussions I had at the Congress will help me translate to my colleagues at CAPA ideas for better decisions and, ultimately, improved health for patients.
I plan to use the knowledge that I obtained from the ISPOR Congress along with my eight years of research experiences to form new relationships with professionals to share ideas and gain a new understanding in order to share the pharmacoeconomic methodologies and outcomes research techniques from our ISPOR Egypt Regional Chapter network to the Ministry of Health. I plan to establish a pharmacoeconomics unit at CAPA that will focus on providing updated training on pharmacoeconomics and outcomes research, targeted at both hospital pharmacists who implement this science upon selecting the pharmaceutical products of the formulary and health care decision makers at CAPA who incorporate this science into the approval process of drugs, hopefully resulting in rational health care decision making at affordable costs to all people in Egypt.
Raising awareness and Improving the Decision-Making Process in government to Make Better Use of Health care Resources gihan Hamdy Elsisi, MSc, Team Leader of Hospital Pharmacy administration, central administration for Pharmaceutical
affairs, Ministry of Health, cairo, Egypt
I had the great pleasure of attending the ISPOR 14th Annual European Congress in Madrid, Spain–my first of its kind–after seven years of research in the field. This was made possible thanks to an ISPOR Meeting Travel Scholarship Award. It was an honor to receive it as I was the only Eastern European – Slavic member to receive this award this year. It was a great pleasure to attend such a large congress dedicated to the research interests of me and my team. I used this opportunity to talk to and learn from many extraordinary, gifted and creative people, some of whom dedicate their life-time careers to
the disciplines of health economics. I acquired new cutting edge, methodological skills after attending the plenary lectures.
One of the perks of the travel award was being able to attend short courses. I chose to attend the following short courses: “Cost-Effectiveness Analysis alongside Clinical Trials”, “Advanced Retrospective Database Analysis: Econometric Methods,” and “Transferability of Cost-Effectiveness Data between Countries.” All three of these were closely related to the clinical trials and field work we conduct in Serbia.
Many of the issues discussed during these courses are applicable to our local conditions.
I also had the excellent opportunity to present a poster at the congress entitled, “Radiology Diagnostics And Interventional Radiographic Services Utilization Patterns And Economic Consequences Analysis In A Large Tertiary Care University Hospital – Three Year Trends.”
I learned a lot about the core topics of evidencing direct medical costs of care in hospital conditions,
Pharmacoeconomic assessment Based Decision Making in Delivering Health care
on the Rise among Eastern European and Balkans Policy Makers Mihajlo B. Jakovljevic, MD, PhD, assistant Professor of Pharmacology and Pharmacoeconomics, The Medical Faculty
University of Kragujevac , Leader of the Budget Financed, Research Project on Health Economics (OI 175014) approved
funding from Ministry of Education and Science of the Republic of Serbia for 2011-2014., Kragujevac, Serbia
>

20 November/December 2011 ISPOR cONNEcTIONS
drug reimbursement related policies and an overall health care funding among different national systems while attending the Congress. Comparison between markets with inherited different patterns of medical services provision and facilities network financing, is my specific focus in science. Approaches to this topic were presented at the Congress that are at the very forefront of applied contemporary econometrics. As an academic researcher, most of my time is focused on publishing and health technology assessments (HTA) at local health care markets in the region. Our long term difficulties and challenges are reflected in the necessity of heavy investment in human resources by providing advanced education and methodological insights for people involved in research. Another challenge for Eastern Europe and the Balkans in health economic evidence based decision making is its socialist heritage in health care funding and management. Official HTA agencies are still scarce and cost/effectiveness evidence is rarely
mandatory for new drug and/or medical technology approval for marketing. The region consists of a vast population of few high and many middle-to- low income economies (mostly outside EU). In a macroeconomic surrounding with scarce resources, a governmental policy-maker’s awareness of the necessity of prioritization needs to be extended. Fortunately, in recent years some room is being created to exert such influence. My research team (currently 18+ people) and I are willing to invest every effort to raise the productivity of publishing in health economics. It is essential for this local data to be widespread to core audiences. I believe we should continue to put pressure on the governmental sector, which is still in charge of most health care provisions in these countries, by delivering local evidence. In the long run, the results should be obvious in terms of achieving sustainable health care financing without the threat of causing the health budget shortages that are currently experienced in a number of countries in the region.
In conclusion, I would like to use this opportunity to once again express my gratitude to ISPOR for awarding me this grant and giving me such a wonderful experience. We all strive to allocate resources in a just manner, providing the maximal quantity and quality of evidence-based services for the society. I honestly believe that creativity and exceptional efforts could be hidden in developing nations. To that end, I strongly support further ISPOR investments in experts worldwide that reside in such areas because the potential for change and improvement is enormous. The knowledge gained by local opinion leaders can mean a lot to these communities providing bold steps forward.
AcknowledgementThe author would like to hereby express gratitude in Grant No. 175014 of the Ministry of Education and Science of The Republic of Serbia, to the aforementioned facts in this report outsourced from primary trials financed by this grant.
I am particularly grateful for the opportunity to take part in the ISPOR 14th Annual ISPOR European Congress and I sincerely thank ISPOR for the opportunity.
I must say I had been particularly worried about our inability to assess the effectiveness of our health technologies using evidence to ensure value for money in Ghana. The selection processes for our essential medicines and other pharmaceuticals requires more robust evidence with appropriate systematic reviews to support the processes as a cost containment measure.
I was amazed at the pool of evidence that was available and was virtually overwhelmed with the different papers of interest which occurred in parallel sessions, thus making it impossible for me to attend all of the sessions at the Congress. I found the
Congress Personal Scheduler useful in helping to make ‘cost effective’ choices in selecting sessions. I am looking forward to working with my colleagues to gather the necessary evidence to ensure ISPOR Ghana becomes viable to support our National Health Insurance Scheme in becoming more sustainable [1]. The externalities of the Congress are the huge networks which provided the opportunity to open important communication lines for appropriate partnerships for countries like Ghana and individuals requiring assistance in their areas of interest. I believe that these collaborations and partnerships are nurtured for ‘win – win’ situations to increase access to health in low and middle income countries with value for money collaborations to be taken forward.
The Ministry of Health in Ghana, in its medium term strategic plan for 2011-2013 [2] in the area of improving institutional care and mental health under
health objective 5, is exploring cost-effective methods of ensuring health commodity security to improve health outcomes. I look forward to supporting actions in the area of evidence based policy workings in the area of health technology assessments and also building capacities in Ghana with the appropriate skills and competences to move the health agenda forward.
I am indeed very grateful for this opportunity and I am happy I was part of the ISPOR 14th Annual European Congress and look forward to future participation in ISPOR activities.
references1 Ministry of Health Sector Review 2010: Moving from Strategies to Action.2 Ministry of Health Medium Term Strategic Plan 2011-2013.
Ensuring Evidence Based Policy Decision Making In ghana Martha gyansa-Lutterodt, Ministry of Health, accra, ghana
I feel honoured to be one of the recipients of a 2011 ISPOR Meeting Travel Scholarship Award and attending the ISPOR 14th Annual European Congress which was held on 5-8 November 2011, in the beautiful city of Madrid, Spain.
I commend this laudable initiative as it opens up new frontiers of knowledge and networking opportunities to upcoming talents and experienced professionals in the field of pharmacoeconomics and outcomes research. Additionally, it is a way of ensuring renewed interests and raising a new cadre of professionals in this subject matter.
During the Congress, I attended three short courses: Introduction to Modelling, Applications of
Pharmacoeconomics Modelling and Conjoint Analysis-Theory and Methods. From these three courses, I gained valuable knowledge that will be of immediate application and relevance to pharmacoeconomics and outcomes research in Nigeria.
In addition, I gained transferable skills and experience from the plenary sessions on the pros and cons of a centralized European pricing and reimbursement agency. This topic is of particular relevance to Nigeria as it is seeking to roll out appropriate benefit packages under its National Health Insurance Scheme.
After attending this conference, I seek to develop the capacity of Public Sector Institutions and Civil Society Organizations in the use of pharmacoeconomics and
outcomes research by decision makers and other stakeholders in health institutions in Nigeria through scheduled trainings, meetings and forums. Over time, I feel this should translate into increasing and improving the use of health resources in an equitable and cost effective manner by mainstreaming pharmacoeconomics and outcomes research principles into processes of drug selection, drug formulary management and procurement decisions, as wellas other areas. A step-down training approach through the ISPOR Nigeria chapter meetings, conferences, and updated lectures in pharmacy schools across Nigeria will also be explored.
In Nigeria, the knowledge and practice of pharmacoeconomics and outcomes research is
Bridging Knowledge and Practice gaps and Sustaining Pharmacoeconomics and Outcome Research in Nigeria Kehinde Onasanya, BPharm, MSc, Non-governmental organization Management Sciences for Health, abuja, Nigeria

November/December 2011 ISPOR cONNEcTIONS 21
in its infancy stage [1] and a wide gap often exist between knowledge and practice to deliver cost-effective and efficient healthcare to the populace. A growing interest and force, however, is gathering with the establishment of the ISPOR Nigeria Regional
Chapter in 2009. Now, a cadre of professionals has been created to sustain this initiative and promote its ideals to benefit the society at large.
reference1 Gavaza P, Rascati KL, Oladapo A, Star K. The state of health economics evaluation research in Nigeria: A systematic review. Pharmacoeconomics 2010;28: 539-53.
I truly appreciated the opportunity to participate in the ISPOR community and feel honored to have been awarded an ISPOR 2011 Meeting Travel Scholarship Award. The Congress was an opportunity for me to upgrade my knowledge in basic pharmacoeconomic methodologies and techniques in outcome research.
The ISPOR Congress was the biggest and most impressive event I have ever attended. I met interesting people and engaged in resourceful discussions. During the Congress, I attended three short courses and many other important sessions. The workshop on “Network Meta-Analysis in Relative Effectiveness Research” was especially valuable for me. I learned about indirect and mixed-treatment comparisons, about the use of different types of outcomes and other methods that should prove essential during my work. The methods discussed throughout the workshop are
very useful for countries where randomized clinical trials are not practiced. I was also interested in taking “Advanced Retrospective Database Analysis,” because a retrospective design is utilized by my studies. The opportunity to attend short courses and workshops afforded me a chance to acquire knowledge from the world’s leading experts. The Congress provided a lot of educational poster and podium presentations as well. I hope to submit one of my own studies to ISPOR in the future.
I was impressed by the intensive work of the ISPOR staff. They were quick in responding to all inquiries and questions during the organization of the Congress.
With my three years of research experience, I can state that every health care professional should know the basic principles of health economics analysis.
In Armenia, this is particularly important for the governmental decision-making process as it is mostly based on approximate estimations. The need for adaptation and development of health technology assessments is obvious, since the health care system is in the process of developing and implementing reforms to make our health services more affordable and because most of the preconditions for the establishment of the Armenian medical insurance system include rationalization and minimization of widespread inefficiencies. I hope to bring my colleagues, who are engaged in pharmacoeconomics and public health, together to create a community in Armenia which will contribute to the goals defined by ISPOR. I believe that active cooperation will benefit not only health care professionals but patients also.
Striving to Implement great Ideas for a Small country anush Perikhanyan, MS, MPH, PhD candidate at Yerevan State Medical University Department of Pharmaceutical
Management, Research Fellow at cardiology center, Yerevan, armenia
I was overwhelmed by the publication of the recipients for the ISPOR 14th Annual European Congress Travel Scholarship Award in Madrid, Spain, which included my name, because I did not expect that on my first attempt, I would receive an award.
As this was my first ISPOR congress, I wanted to maximize every opportunity at my disposal. I felt privileged to be able to attend three short courses. Two of these courses were just introduced by ISPOR, thus making me one of the pioneering students for those short courses. As a new researcher, my quest is to do quality research through good methods, and so I selected the following short courses: 1) Introduction to Retrospective Database Analysis; 2) Advanced Retrospective Database Analysis; and 3) Conjoint Analysis – Theory and Methods. These courses provided exactly what I needed and met my expectations. The faculty members not only shared their knowledge but also their experiences from the field, which was very encouraging and made the sessions very practical. Participants were given the opportunity to contribute during and after the sessions. The Plenary Sessions, Issue Panels and Workshops were all very well organized and the ISPOR staff were excellent in performing their duties. The ISPOR staff members were more than willing and readily available to provide assistance; credit to all the ISPOR staff members. The congress also gave me, for the first time, an international platform to share my findings in my poster presentation, “Cost of Diabetes management to Cocoa Clinics in Ghana.” I was also privileged to meet some key personalities of ISPOR.
Health care financing is one of six pillars of health systems. External financial assistance is often required in the average low income country to improve synergies between external and domestic funding [1,2]. The sustenance and efficient management of any health system will thus require rational health care decision making based on evidence. Health/pharmacoeconomics and outcomes research has provided evidence for economists, policy makers and health service researchers as it provides value-based pricing and estimates of the potential health care costs that can be averted to institutions and society. These have also been used in identifying the burden of disease, possible areas for future intervention, and priority settings in health care and research [3]. In Ghana–and many developing countries–health care financing has been facing many challenges. Unfortunately, there is not enough strength in health economics in Africa; many developing countries and most decision makers in this area do not have much capacity or experience in health economics and outcome research [4].
Following the sessions at the ISPOR Congress, I observed that Africa didn’t have any or much of a platform to contribute to the Congress (with the exception of the few poster presentations that were accepted). There is a clarion call for capacity building in pharmacoeconomics and outcomes research in Africa. ISPOR could greatly contribute to this through the ISPOR Distance Learning Program, as well as other training programs, tailor-made for the needs of developing countries. As a pharmacist with interest in health economics and outcomes research and a
member of ISPOR, I hope to promote the agenda of ISPOR and the development of pharmacoeconomic guidelines which we lack in Ghana.
ConclusionI am most grateful to ISPOR for supporting researchers from developing countries to learn and share experiences on such platforms. I hope the experience and knowledge I gathered will help advance the objectives of ISPOR in my region.
references1 World Health Organization (2007). Everybody’s business: strengthening health systems to improve health outcomes. WHO’s framework for action. Geneva, World Health Organization.2 World Health Organization (2008). Primary Health Care, including health system strengthening, Report by the Secretariat. Executive Board 124th Session, WHO.3 Songer TJ, Ettaro L. Studies on the Cost of Diabetes. Centers for Disease Control and Prevention, 1998.4 World Health Organization. Strengthening Health Economics Capability in Africa: Summary and Outcomes of a regional consultation of Experts and policy makers. Special Programme for Research and Training in Tropical Diseases, 2008.
Health/Pharmacoeconomics and Outcome Research: Evidence Required For Rational Health care Decision Making in Developing countries Ernest attuquaye Quaye, BPharm, MPH, Principal Pharmacist, Medical Department, ghana cocoa Board, accra, ghana

22 November/December 2011 ISPOR cONNEcTIONS
I was honored to receive a 2011 ISPOR Meeting Travel Scholarship Award, and attend the 14th Annual European Congress in Madrid, Spain. It was a great opportunity for me to get in touch with the best experts and researchers from around the world in the area of health economics and outcomes research.
The 14th Annual European Congress was my first ISPOR meeting. I got the chance to attend two short courses; the first was the Introductory to Pharmacoeconomic Evaluation course, which was a new topic for me, as it differs from my previous studies, i.e. clinical pharmacy. This course introduced me to the most important terms and the shortest and easiest methodologies for a newcomer. I also had the chance to attend the Establishing the Content Validity of Patient-Reported Outcome (PRO) Instruments short course. Even though it was an advanced course, I found it is an interesting new area, which has limited implementations in the Middle East, an area where it is much needed.
The most impressive aspect of the Congress was its organization and the dedication of the ISPOR staff and committees. Several workshops and presentations were held simultaneously with the poster sessions, exhibitions, and interactive discussions, which converted the Congress into a beehive; wherever you turned, you could hear the buzz.
As a new member of ISPOR, I was also given the opportunity to be a reviewer for the Congress workshops, which I found very exciting and proactive. In addition, I was given the chance to meet other colleagues from the area and to meet with members of the newly formed ISPOR Arabic Network. This network will help us recognize the challenges related to our area and formulate ideas to create activities for ISPOR Arabic members. Since we are aware that the idea of health economics and outcomes research is still not fully established in the Arabic area, we agreed that great challenges lie ahead, beginning with the promotion of this science to create awareness in
our region and more importantly, to increase the number of researchers in this area. The Congress gave me the chance to meet top researchers in these fields and to be exposed to different experiences and methodologies that can be used in the future to conduct research in the Arabic area.
Attending the ISPOR 14th Annual European Congress made me want to pursue further training and look for educational programs in the area of health economics. I am looking forward to networking with other ISPOR members and conducting research in Jordan. I may even take it one step further and compare the outcomes with neighboring countries. I hope within the next 5 to 10 years, the perception of health economics will change dramatically in Jordan, and be acknowledged more by decision makers. I am also looking forward to transferring some of the knowledge I obtained and teaching my students the concepts of health economics.
The Horizon of Health Economics in Jordan Sondos abdel Qader Samara, al-Isra University, amma Jordan
It was with great pleasure that I received an ISPOR 2011 Meeting Travel Scholarship Award, which made an otherwise seemingly distant ambition of attending the ISPOR 14th Annual European Congress in Madrid, Spain, possible. After an introduction to cost-effectiveness analysis by a visiting fellow at our institute, it was incumbent to present results from the analysis done with our very own data for the benefit of our country and countries in similar settings. This award made this possible.
The Congress in Madrid was my first ISPOR meeting. It was a wonderful experience! I attended three short courses in Retrospective Database Analysis and Transferability of Cost Effectiveness Data between countries. These were quite relevant given the kind of observational data that we have generated over the years at our large HIV Urban clinic and through several other studies or interventions. These data, once analyzed, can translate into important information for health-policy decision makers for the country. The course about the transferability of cost effectiveness data was also quite insightful as it will help us to properly translate lessons
from countries in similar settings to our own country without re-inventing the wheel.
During the Congress I met a number of people in different areas with similar objectives and those with a zeal to carry out more outcomes research in Africa. I also got to meet a number of professors, doctors and other professionals who were willing to give their time to help in skills and capacity building for our working group through lectures, webinars, short courses and perhaps mentorship. I hope to extend the linkages established to include more professionals in the area of outcomes research.
A note of appreciation goes to the ISPOR staff for the wonderful organization that made hosting over 3000 attendees and over 90 exhibitors seem like a simple task. Small talk with one of the exhibiting company representatives revealed how ISPOR meetings started with a handful of exhibitors and few members. He was amazed at how ISPOR has grown by leaps and bounds into a great society with a lot of influence in health care.
The Congress made me realize how outcomes research is a powerful tool for rational health care decision making in countries with resource-limited settings such as Uganda. It is my humble request that capacity building be done in this very important field in low income countries so as to ensure that we can get the best out of the scarce and limited funding for health in these settings.
With the skills and experience obtained, I now plan to energize and expand our cost-effective-analysis working group. This includes updating the group on the new methodologies learned through the conference; inviting more interested people to the group; and organizing outcomes research sessions for both researchers at the institute and students at the University. I am keen to keep in touch with the ISPOR African regional chapters through the correspondents met at the Congress and also map a way forward for an ISPOR Uganda Regional Chapter. I believe in the near future, Africa should be able to hold its inaugural ISPOR meeting.
Outcomes Research is Key in Health care Decision Making In Low Income countries Mark Ssennono, Infectious Diseases Institute, college of Health Sciences, Makerere University, Kampala, Uganda
2012-2013 BOARD OF DIRECTORS call for nominations
.............................................ISPoR is a member-driven organization. as an ISPoR member, you are encouraged to submit a nomination to
serve on the 2012-2013 ISPoR boaRd of dIRectoRS. Self-nominations are permitted.
Please email your recommendation, along with a curriculum vita, to: [email protected].
for the 2011-2012 ISPoR board of directors members (including terms of office(, see: http://www.ispor.org/board/index.asp
The deadline for submitting nominations is wednesday, January 4, 2012.
IC

November/December 2011 ISPOR cONNEcTIONS 23
IntroductionThe objectives of this report are to share my experiences as an ISPOR International Fellowship Award recipient and to highlight my contributions towards the promotion of pharmacoeconomics and outcomes research in Nigeria, West Africa. I received the 2009 ISPOR International Fellowship Award that enabled me to participate at the ISPOR International Meetings and Short Courses held in Atlanta, GA, 2010 and Baltimore, MD, 2011. My participation in the ISPOR meetings increased my interest and knowledge base and aided me in my contributions towards the promotion of Pharmacoeconomics and Outcomes Research, and the use of outcomes research in health care decisions in Nigeria.
MethodsPharmacoeconomics�Curriculum�We have introduced pharmacoeconomics as an area of specialization in the postgraduate degree program in the Department of Clinical Pharmacy and Pharmacy Practice/Management. Two candidates recently pursued the discipline of pharmacoeconomics to the PhD level. Many students in both the West African Postgraduate College of Pharmacists and Pharmacy Schools in Nigerian Universities now conduct their degree projects in the area of pharmacoeconomics and outcomes research. This trend is considered beneficial to generate evidence for the value of pharmacoeconomics and outcomes research, as well as promote the capacity of the health workforce.
ISPOR�Nigeria�Regional�ChapterThe worldwide acceptance of pharmacoeconomics and outcomes research will depend on the vibrant platform of regional chapters of ISPOR . Considering the size of the Nigerian market and its dominant role in Africa, ISPOR Nigeria will galvanize efforts toward market promotion of pharmacoeconomics and outcomes research as well as their influence on national policies.
We inaugurated the Nigerian Chapter (ISPOR Nigeria) on the October 3, 2009; foundation members came from diverse professional backgrounds including pharmacists, doctors, economists, accountants, and academicians. At that inaugural meeting, we ratified the Constitution of ISPOR–Nigeria and elected a team led by Dr. John Alfa, with Dr. Waka Udezi, (2007 ISPOR Fellowship recipient) as Secretary to pilot the affairs of the Society. At that inaugural meeting, I presented a paper on Economic Evaluation of Pharmaceuticals and also chaired the committee that produced conference communiqué which received wide publicity.
The second ISPOR Nigeria workshop was held on March 24 - 26, 2011and the third workshop “Pharmacoeconomics and Outcomes Research in Healthcare Policy Development,” was held October 5-7, 2011. At this meeting, short courses were offered in the following areas: Introduction to Pharmacoeconomics, Health Care Decision Modeling, Cost of Illness Studies, and Health Technology Assessment.
The�future�of�pharmacoeconomics�and�outcomes�research�and�utilization�in nigeriaWe are confronted with the following challenges:
•HealthpolicyformulationinNigeriahasyettohavepharmacoeconomicevidence.
•Agenerallackofawarenessoftheroleofeconomicevaluationinthe provision and utilization of health care technology, particularly pharmaceutical products, in the health care system.
•Limitedknowledgeandskillsfortheeconomicevaluationofhealthcaretechnology.
•Nopolicyontheuseofpharmacoeconomicevaluationofhealthcaretechnology in Nigeria as obtained in developed countries.
•Poordocumentationofhealthservicesandincomplete,orlack,ofmedical data in Nigeria. This is a major problem affecting research and planning for the efficiency of a health care system.
•Lackofcollaborationamonghealthworkers
•Poorqualitymedicinesincirculation.
These problems have largely contributed to the inefficiency of the Nigerian health care system.
Despite these barriers, there is a great potential for pharmacoeconomics and outcomes research and its use in Nigeria. Awareness is growing among students, researchers, and policy makers and we need to sustain the momentum through ISPOR-Nigeria. To help with this, during the ISPOR International Meeting in Baltimore, we initiated the formation of the African Consortium. Delegates from Nigeria, South Africa, and Ghana were in attendance. Establishing the African consortium will increase the impetus for pharmacoeconomics in the region that shares common socio-cultural factors that influence policy.
acknowledgementI appreciate the opportunity to be part of ISPOR. I salute the great jobs of the ISPOR team, in particular, the dedication and commitment of Stephen Priori and all the unseen hands that make ISPOR a focused international organization.
ISPOR cORNER
ISPOR 2009 International Fellowship Report: Towards Pharmacoeconomics and Outcomes Research in Nigeria azuka c. Oparah, MBa, MPH, PhD, associate Professor, Department Of clinical Pharmacy & Pharmacy Practice,
University Of Benin, Nigeria and Secretary-general, West african Postgraduate college 0f Pharmacists
IC
< advertisement >

24 November/December 2011 ISPOR cONNEcTIONS
Disease Related ResearchCardiovascular DiseaseAli AK. Pharmacovigilance analysis of adverse event reports for aliskiren hemifumarate, a first-in-class direct renin inhibitor. Ther Clin Risk Manag 2011;7:337-44.
Al-Rasadi K, Al-Zakwani I, Zubaid M, Ali A, Bahnacy Y, Sulaiman K, Al Mahmeed W, Al Suwaidi J, Mikhailidis DP. Prevalence, Predictors, and Impact of Low High-Density Lipoprotein Cholesterol on in-Hospital Outcomes Among Acute Coronary Syndrome Patients in the Middle East. Open Cardiovasc Med J 2011;5:203-9.
Chen YC, Cao WW, Cao Y, Zhang L, Chang BB, Yang WL, Liu XQ. Using neural networks to determine the contribution of danshensu to its multiple cardiovascular activities in acute myocardial infarction rats. J Ethnopharmacol 2011;138:126-34.
Grabner M, Johnson W, Abdulhalim AM, Kuznik A, Mullins CD. The value of atorvastatin over the product life cycle in the United States. Clin Ther 2011;33:1433-43.
Patients Receiving Angiotensin II Receptor Blockers in Primary Care: A Comparative Effectiveness Analysis From Electronic Medical Record Data. J Clin Hypertens (Greenwich) 2011;13:801-12.
Pink J, Lane S, Pirmohamed M, Hughes DA. Dabigatran etexilate versus warfarin in management of non-valvular atrial fibrillation in UK context: quantitative benefit-harm and economic analyses. BMJ 2011;343:d6333.
Pressler SJ, Therrien B, Riley PL, Chou CC, Ronis DL, Koelling TM, Smith DG, Sullivan BJ, Frankini AM, Giordani B. Nurse-Enhanced Memory Intervention in Heart Failure: the MEMOIR study. J Card Fail 2011;17:832-43.
Reed SD, Eapen ZJ, Schulman KA. End point selection in acute decompensated heart failure clinical trials: economic end points. Heart Fail Clin 2011;7:529-37.
Reynolds MR, Magnuson EA, Lei Y, Leon MB, Smith CR, Svensson LG, Webb JG, Babaliaros VC, Bowers BS, Fearon WF, Herrmann HC, Kapadia S, Kodali SK, Makkar RR, Pichard AD, Cohen DJ; for the Placement of Aortic Transcatheter Valves (PARTNER) Investigators. Health-Related Quality of Life After Transcatheter Aortic Valve Replacement in Inoperable Patients With Severe Aortic Stenosis. Circulation 2011;124:1964-1972.
Sheer AJ, Heckman JE, Schneider EB, Wu AW, Segal JB, Feinberg R, Lidor AO. Congestive heart failure and chronic obstructive pulmonary disease predict poor surgical outcomes in older adults undergoing elective diverticulitis surgery. Dis Colon Rectum 2011;54:1430-7.
Tsujimoto T, Kajio H, Takahashi Y, Kishimoto M, Noto H, Yamamoto-Honda R, Kamimura M, Morooka M, Kubota K, Shimbo T, Hiroe M, Noda M. Asymptomatic coronary heart disease in patients with type 2 diabetes with vascular complications: a cross-sectional study. BMJ Open
2011;1:e000139.
Xu Y, Ding X, Zou J, Liu Z, Jiang S, Xu S, Shen B, Chen Y, Shan Y, Cao X. Plasma Pentraxin 3 is Associated with Cardiovascular Disease in Hemodialysis Patients. Ren Fail 2011;33:998-1004.
DermatologyBailey EE, Marghoob AA, Orengo IF, Testa MA, White VR, Geller AC. Skin cancer knowledge, attitudes, and behaviors in the salon: a survey of working hair professionals in Houston, Texas. Arch Dermatol 2011;147:1159-65.
Endocrinology, Metabolism & DiabetesChen Y, Wang F, Long H, Chen Y, Wu Z, Ma L. GRK5 promotes F-actin bundling and targets bundles to membrane structures to control neuronal morphogenesis. J Cell Biol 2011;194:905-20.
Chiang CL, Chen SS, Lee SJ, Tsao KC, Chu PL, Wen CH, Hwang SM, Yao CL, Lee H. Lysophosphatidic Acid Induces Erythropoiesis through Activating Lysophosphatidic Acid Receptor 3. Stem Cells 2011;29:1763-73.
Gu J, Wang X, Jiang X, Chen Y, Chen L, Fang X, Sha X. Self-assembled carboxymethyl poly (l-histidine) coated poly (beta-amino ester)/DNA complexes for gene transfection. Biomaterials 2012;33:644-58.
McQueen RB, Ellis SL, Campbell JD, Nair KV, Sullivan PW. Cost-effectiveness of continuous glucose monitoring and intensive insulin therapy for type 1 diabetes. Cost Eff Resour Alloc 2011;9:13.
Quilliam BJ, Simeone JC, Ozbay AB, Kogut SJ. The incidence and costs of hypoglycemia in type 2 diabetes. Am J Manag Care 2011;17:673-80.
Roznyatovskiy VV, Lim JM, Lynch VM, Lee BS, Kim D, Sessler JL. pi-Extension in Expanded Porphyrins: Cyclo[4]naphthobipyrrole. Org Lett 2011;13:5620-3.
Tang HK, Chen KC, Liou GG, Cheng SC, Chien CH, Tang HY, Huang LH, Chang HP, Chou CY, Chen X. Role of a propeller loop in the quaternary structure and enzymatic activity of prolyl dipeptidases DPP-IV and DPP9. FEBS Lett. 2011;585:3409-14.
Yang J, Zhang F, Chen Y, Qian S, Hu P, Li W, Deng Y, Fang Y, Han L, Luqman M, Zhao D. Core-shell Ag@SiO(2)@mSiO(2) mesoporous nanocarriers for metal-enhanced fluorescence. Chem Commun (Camb). 2011;47:11618-20.
Ziegenfuss JY, Shah ND, Deming JR, Van Houten HK, Smith SA, Beebe TJ. Offering Results to Participants in a Diabetes Survey: Effects on Survey Response Rates. Patient 2011;4:241-5.
Gastro-IntestinalChaudhry S, Khan AA, Butt AK, Idrees M, Izhar M, Iqbal HA. Helicobacter pylori in Dental Plaque; Is it Related to
Brushing Frequency, Plaque Load and Oral Health Status? J Coll Physicians Surg Pak 2011;21:589-92.
Dibonaventura M, Sun SX, Bolge SC, Wagner JS, Mody R. Health-related quality of life, work productivity and health care resource use associated with constipation predominant irritable bowel syndrome. Curr Med Res Opin 2011;27:2213-22.
Kaur N, Chen CC, Luther J, Kao JY. Intestinal dysbiosis in inflammatory bowel disease. Gut Microbes 2011;2:211-6.
Yang M, Robinson AM, Pollack PF. When meta-analysis misleads. Am J Gastroenterol 2011;106:2043.
GynecologyChen CP, Su YN, Lin HH, Chern SR, Tsai FJ, Wu PC, Lee CC, Chen YT, Wang W. De novo duplication of Xq22.1-->q24 with a disruption of the NXF gene cluster in a mentally retarded woman with short stature and premature ovarian failure. Taiwan J Obstet Gynecol 2011;50:339-44.
Xu X, Macaluso M, Frost J, Anderson JE, Curtis K, Grosse SD. Characteristics of users of intrauterine devices and other reversible contraceptive methods in the United States. Fertil Steril 2011;96:1138-44.
Infectious DiseaseAljunid S, Abuduxike G, Ahmed Z, Sulong S, Nur AM, Goh A. Impact of routine PCV7 (Prevenar) vaccination of infants on the clinical and economic burden of pneumococcal disease in Malaysia. BMC Infect Dis 2011;11:248.
Brook RA, Kleinman NL, Su J, Corey-Lisle PK, Iloeje UH. MPH Absenteeism and Productivity Among Employees Being Treated for Hepatitis C. Am J Manag Care 2011;17:657-64.
Jacobs P. Are economic evaluations an important tool in vaccine policy decisions? Expert Rev Pharmacoecon Outcomes Res 2011;11:507-11.
Vieira MC, Kumar RN, Jansen JP. Comparative Effectiveness of Efavirenz, Protease Inhibitors, and Raltegravir-Based Regimens as First-Line Treatment for HIV-Infected Adults: A Mixed Treatment Comparison. HIV Clin Trials 2011;12:175-89.
Wilby K, Marra CA, da Silva JH, Grubisic M, Harvard S, Lynd LD. Randomized Controlled Trial Evaluating Pictogram Augmentation of HIV Medication Information. Ann Pharmacother 2011;45:1378-83.
Neurology & Mental HealthAngalakuditi M, Angalakuditi N. A comprehensive review of the literature on epilepsy in selected countries in emerging markets. Neuropsychiatr Dis Treat 2011;7:585-97.
Ascher-Svanum H, Zhao F, Detke HC, Nyhuis AW, Lawson AH, Stauffer VL, Montgomery W, Witte MM, McDonnell DP. Early response predicts subsequent response to olanzapine long-acting injection in a randomized, double-blind clinical
This column includes books, articles, and abstracts recently published by ISPOR members. To ensure that your published work in pharmacoeconomic or outcomes research is reported here, please keep your contact information up to date with the Society. Any questions, comments, or submissions concerning this review can be directed to Stephen Priori at: [email protected].
Recently Published Works: Innovatively Using Outcomes Research by ISPOR MembersBy Stephen Priori, Director, ISPOR Publications
ISPOR cORNER

November/December 2011 ISPOR cONNEcTIONS 25
trial of treatment for schizophrenia. BMC Psychiatry 2011;11:152.
Budd D, Burns LC, Guo Z, L’italien G, Lapuerta P. Impact of early intervention and disease modification in patients with predementia Alzheimer’s disease: a Markov model simulation. Clinicoecon Outcomes Res 2011;3:189-95.
Chang CC, Wang WF. High-dose zolpidem withdrawal seizure in a patient with spinocerebellar ataxia. Prim Care Companion CNS Disord 2011;13.
Chang TG, Lee IH, Chang CC, Yang YK, Huang SS, Chen KC, Wang CH, Chang YH. Poorer Wisconsin card-sorting test performance in healthy adults with higher positive and negative schizotypal traits. Psychiatry Clin Neurosci 2011;65:596-9.
Defrancesco M, Niederstatter H, Parson W, Oberacher H, Hinterhuber H, Canazei M, Bidner J, Deisenhammer EA, Kemmler G, Weiss EM, Marksteiner J. Influence of Serotonin Transporter Genotype and Catechol-O-Methyltransferase Val158Met Polymorphism on Recognition of Emotional Faces. J Int Neuropsychol Soc 2011;17:1014-20.
Dyrbye LN, Harper W, Durning SJ, Moutier C, Thomas MR, Massie FS Jr, Eacker A, Power DV, Szydlo DW, Sloan JA, Shanafelt TD. Patterns of distress in US medical students. Med Teach 2011;33:834-9.
Hodgkins P, Montejano L, Sasane R, Huse D. Risk of injury associated with attention-deficit/hyperactivity disorder in adults enrolled in employer-sponsored health plans: a retrospective analysis. Prim Care Companion CNS Disord 2011;13.
Hodgkins P, Montejano L, Sasane R, Huse D. Cost of illness and comorbidities in adults diagnosed with attention-deficit/hyperactivity disorder: a retrospective analysis. Prim Care Companion CNS Disord 2011;13.
Johnson S, Davis M, Kaltenboeck A, Birnbaum H, Grubb E, Tarrants M, Siderowf A. Early retirement and income loss in patients with early and advanced Parkinson’s disease. Appl Health Econ Health Policy 2011;9:367-76.
Kawashima M, Tsubota K. Effect of calorie restriction on change in lacrimal gland with age. Cornea 2011;30(Suppl. 1):S29-33.
Kong X, Chen Y, Chen X, Sun X. Influence of family history as a risk factor on primary angle closure and primary open angle glaucoma in a Chinese population. Ophthalmic Epidemiol 2011;18:226-32.
Lachaine J, Beauchemin C, Legault M, Bineau S. Economic evaluation of the impact of memantine on time to nursing home admission in the treatment of Alzheimer disease. Can J Psychiatry 2011;56:596-604.
Lin V, Golub JS, Nguyen TB, Hume CR, Oesterle EC, Stone JS. Inhibition of notch activity promotes nonmitotic regeneration of hair cells in the adult mouse utricles. J Neurosci 2011;31:15329-39.
Liu X, Chen Y, Faries DE. Adherence and persistence with branded antidepressants and generic SSRIs among managed care patients with major depressive disorder. Clinicoecon Outcomes Res 2011;3:63-72.
Lloyd A, Hodgkins P, Sasane R, Akehurst R, Sonuga-Barke EJ, Fitzgerald P, Nixon A, Erder H, Brazier J. Estimation of utilities in attention-deficit hyperactivity disorder for economic evaluations. Patient 2011;4:247-57.
Margolis JM, Fowler R, Johnson BH, Kassed CA, Kahler K. Disease-modifying drug initiation patterns in commercially insured multiple sclerosis patients: a retrospective cohort study. BMC Neurol 2011;11:122.
Montejano L, Sasane R, Hodgkins P, Russo L, Huse D. Adult ADHD: prevalence of diagnosis in a US population with employer health insurance. Curr Med Res Opin 2011;27(Suppl. 2):5-11.
Moskovitz BL, Benson CJ, Patel AA, Chow W, Mody SH, McCarberg BH, Kim MS. Analgesic treatment for moderate-to-severe acute pain in the United States: patients’ perspectives in the Physicians Partnering Against Pain (P3) survey. J Opioid Manag 2011;7:277-86.
North RB, Kumar K, Wallace MS, Henderson JM, Shipley J, Hernandez J, Mekel-Bobrov N, Jaax KN. Spinal Cord Stimulation Versus Re-operation in Patients With Failed Back Surgery Syndrome: An International Multicenter Randomized Controlled Trial (EVIDENCE Study). Neuromodulation 2011;14:330-6.
Patino GA, Brackenbury WJ, Bao Y, Lopez-Santiago LF, O’Malley HA, Chen C, Calhoun JD, Lafreniere RG, Cossette P, Rouleau GA, Isom LL. Voltage-Gated Na+ Channel {beta}1B: A Secreted Cell Adhesion Molecule Involved in Human Epilepsy. J Neurosci 2011;31:14577-91.
Peng X, Ascher-Svanum H, Faries D, Conley RR, Schuh KJ. Decline in hospitalization risk and health care cost after initiation of depot antipsychotics in the treatment of schizophrenia. Clinicoecon Outcomes Res 2011;3:9-14.
Peng X, Ascher-Svanum H, Faries DE, Stauffer VL, Kollack-Walker S, Kinon BJ, Kane JM. Cost-effectiveness of early responders versus early nonresponders to atypical antipsychotic therapy. Clinicoecon Outcomes Res 2011;3:79-87.
Reed DA, Shanafelt TD, Satele DW, Power DV, Eacker A, Harper W, Moutier C, Durning S, Massie FS Jr, Thomas MR, Sloan JA, Dyrbye LN. Relationship of Pass/Fail Grading and Curriculum Structure With Well-Being Among Preclinical Medical Students: A Multi-Institutional Study. Acad Med 2011;86:1367-73.
Schumock GT, Gibbons RD, Lee TA, Joo MJ, Valuck RJ, Stayner LT. Relationship between leukotriene-modifying agent prescriptions dispensed and rate of suicide deaths by county in the US. Drug Healthc Patient Saf 2011;3:47-52.
Shippee ND, Shah ND, Williams MD, Moriarty JP, Frye MA, Ziegenfuss JY. Differences in demographic composition and in work, social, and functional limitations among the populations with unipolar depression and bipolar disorder: results from a nationally representative sample. Health Qual Life Outcomes 2011;9:90.
Yeomans K, Payne KA, Marton JP, Merikle EP, Proskorovsky I, Zou KH, Li Q, Willke RJ. Smoking, smoking cessation and smoking relapse patterns: a web-based survey of current and former smokers in the US. Int J Clin Pract 2011;65:1043-54.
Yoon FB, Huskamp HA, Busch AB, Normand SL. Using Multiple Control Groups and Matching to Address Unobserved Biases in Comparative Effectiveness Research: An Observational Study of the Effectiveness of Mental Health Parity. Stat Biosci 2011;3:63-78.
OncologyCleeland CS, O’Mara A, Zagari M, Baas C. Integrating pain metrics into oncology clinical trials. Clin Cancer Res 2011;17:6646-50.
Chu PY, Hsu NC, Liao AT, Shih NY, Hou MF, Liu CH. Overexpression of alpha-enolase correlates with poor survival in canine mammary carcinoma. BMC Vet Res 2011;7:62.
Chu PY, Hsu NC, Liao AT, Yeh KT, Hou MF, Liu CH. Elevated Kruppel-like factor 4 transcription factor in canine mammary carcinoma. BMC Vet Res 2011;7:58.
Al-Yaarubi S, Farhan H, Al-Futaisi A, Al-Qassabi S, Al-Rasadi K, Al-Riyami S, Al-Zakwani I. Accuracy of ultrasound-guided fine-needle aspiration cytology for diagnosis of carcinoma in patients with multinodular goiter. Indian J Endocrinol Metab 2011;15(Suppl. 2):S132-5.
Holter JL, Thorp K, Smith ML, Kedzierska K, Fung KM, Chacko G, Swisher K, Epstein R, Gumerlock MK. [18F]Fluorothymidine PET imaging in the diagnosis of leptomeningeal involvement with diffuse large B-cell lymphoma. Cancer Imaging 2011;11:140-3.
Jiang X, Xin H, Sha X, Gu J, Jiang Y, Law K, Chen Y, Chen L, Wang X, Fang X. PEGylated poly(trimethylene carbonate) nanoparticles loaded with paclitaxel for the treatment of advanced glioma: In vitro and in vivo evaluation. Int J Pharm 2011;420:385-94.
Kim YH, Sung HJ, Kim S, Kim EO, Lee JW, Moon JY, Choi K, Jung JE, Lee Y, Koh SS, Rhee SG, Heo K, Kim IH. An RNA aptamer that specifically binds pancreatic adenocarcinoma up-regulated factor inhibits migration and growth of pancreatic cancer cells. Cancer Lett 2011;313:76-83.
Kim SP, Shah ND, Weight CJ, Thompson RH, Moriarty JP, Shippee ND, Costello BA, Boorjian SA, Leibovich BC. Contemporary trends in nephrectomy for renal cell carcinoma in the United States: results from a population based cohort. J Urol 2011;186:1779-85.
Mandelblatt JS, Cronin KA, Berry DA, Chang Y, de Koning HJ, Lee SJ, Plevritis SK, Schechter CB, Stout NK, van Ravesteyn NT, Zelen M, Feuer EJ. Modeling the impact of population screening on breast cancer mortality in the United States. Breast 2011;20(Suppl. 3):S75-81.
Martinelli F, Quinten C, Maringwa JT, Coens C, Vercauteren J, Cleeland CS, Flechtner H, Gotay C, Greimel E, King M, Mendoza T, Osoba D, Reeve BB, Ringash J, Koch JS, Shi Q, Taphoorn MJ, Weis J, Bottomley A; European Organisation for Research and Treatment of Cancer Clinical Groups. Examining the relationships among health-related quality-of-life indicators in cancer patients participating in clinical trials: a pooled study of baseline EORTC QLQ-C30 data. Expert Rev Pharmacoecon Outcomes Res 2011;11:587-99.
Neal JW, Gubens MA, Wakelee HA. Current management of small cell lung cancer. Clin Chest Med 2011;32:853-63.
Nuijten MJ, Aultman R, Carpeno Jde C, Vergnenegre A, Chouaid C, Walzer S, Siebert U. An indirect comparison of the efficacy of bevacizumab plus carboplatin and paclitaxel versus pemetrexed with cisplatin in patients with advanced or recurrent non-squamous adenocarcinoma non-small cell lung cancer. Curr Med Res Opin 2011;27:2193-201.
Roberts SA, Karnes EK, Allen JD, Benner JS, Sigal EV, McClellan M. Achieving the goals of effective, safe, and individualized cancer care. Clin Cancer Res 2011;17:6632-3.
Shibata T, Kokubu A, Saito S, Narisawa-Saito M, Sasaki H, Aoyagi K, Yoshimatsu Y, Tachimori Y, Kushima R, Kiyono T, Yamamoto M. NRF2 mutation confers malignant potential and resistance to chemoradiation therapy in advanced esophageal squamous cancer. Neoplasia 2011;13:864-73.
Shiroiwa T, Fukuda T, Shimozuma K. Cost-effectiveness analysis of trastuzumab to treat HER2-positive advanced gastric cancer based on the randomised ToGA trial. Br J Cancer 2011;105:1273-8.
Watanabe T, Tobinai K, Shibata T, Tsukasaki K, Morishima Y, Maseki N, Kinoshita T, Suzuki T, Yamaguchi M, Ando K, Ogura M, Taniwaki M, Uike N, Takeuchi K, Nawano S, Terauchi T, Hotta T. Phase II/III Study of R-CHOP-21 Versus R-CHOP-14 for Untreated Indolent B-Cell Non-Hodgkin’s Lymphoma: JCOG 0203 Trial. J Clin Oncol 2011;29:3990-8.
PediatricsAnderson HD. Suicide Ideation, Depressive Symptoms, and Out-of-Home Placement Among Youth in the U.S. Child Welfare System. J Clin Child Adolesc Psychol 2011;40:790-6. >

26 November/December 2011 ISPOR cONNEcTIONS
Barner JC, Khoza S, Oladapo A. ADHD medication use, adherence, persistence and cost among Texas Medicaid children. Curr Med Res Opin 2011;27(Suppl. 2):13-22.
Chen H, Chen Y, Jin X, Zhang X, Zhou J, Chen B, Pan B, Sun A, Zou Y, Ge J. A survey on blood lipid levels among newborns and healthy inhabitants in urban Shanghai (2008-2009). J Clin Lipidol 2011;5:380-6.
Sharma A, Campbell J. A sensitive period for cochlear implantation in deaf children. J Matern Fetal Neonatal Med 2011;24(Suppl. 1):151-3.
Respiratory DisordersCampbell JD, Allen-Ramey F, Sajjan SG, Maiese EM, Sullivan SD. Increasing pharmaceutical copayments: impact on asthma medication utilization and outcomes. Am J Manag Care 2011;17:703-10.
Chen J, Schooling CM, Johnston JM, Hedley AJ, McGhee SM. How does socioeconomic development affect COPD mortality? An age-period-cohort analysis from a recently transitioned population in China. PLoS One 2011;6:e24348.
Chen HY, Vanness DJ, Golestanian E. A Simplified Score for Transfer of Patients Requiring Mechanical Ventilation to a Long-Term Care Hospital. Am J Crit Care 2011;20:e122-e30.
Kesten S, Celli B, Decramer M, Liu D, Tashkin D. Adverse health consequences in COPD patients with rapid decline in FEV1 - evidence from the UPLIFT trial. Respir Res 2011;12:129.
Larenas-Linnemann DE, Pietropaolo-Cienfuegos DR, Calderon MA. Evidence of effect of subcutaneous immunotherapy in children: complete and updated review from 2006 onward. Ann Allergy Asthma Immunol 2011;107:407-16e.
Nguyen HQ, Burr RL, Gill DP, Coleman K. Validation of the StepWatch device for measurement of free-living ambulatory activity in patients with chronic obstructive pulmonary disease. J Nurs Meas 2011;19:76-90.
Oddershede L, Petersen SS, Kristensen AK, Pedersen JF, Rees SE, Ehlers L. The cost-effectiveness of venous-converted acid-base and blood gas status in pulmonary medical departments. Clinicoecon Outcomes Res 2011;3:1-7.
Skeletal/ArthritisHinchcliff M, Beaumont JL, Thavarajah K, Varga J, Chung A, Podlusky S, Carns M, Chang RW, Cella D. Validity of two new patient-reported outcome measures in systemic sclerosis: Patient-reported outcomes measurement information system 29-item health profile and functional assessment of chronic illness therapy-dyspnea short form. Arthritis Care Res (Hoboken) 2011;63:1620-8.
Hopkins RB, Goeree R, Pullenayegum E, Adachi JD, Papaioannou A, Xie F, Thabane L. The relative efficacy of nine osteoporosis medications for reducing the rate of fractures in post-menopausal women. BMC Musculoskelet Disord 2011;12:209.
Iqbal J, Pepkowitz SH, Klapper E. Platelet-rich plasma for the replenishment of bone. Curr Osteoporos Rep 2011;9:258-63.
Lin HM, Chang CT, Huang CC. Autosomal Dominant Osteopetrosis Type II. Intern Med 2011;50:2695-6.
Pinto D, Robertson MC, Hansen P, Abbott JH; on behalf of the MOA Trial Team. Economic evaluation within a factorial-design randomised controlled trial of exercise, manual therapy, or both interventions for osteoarthritis of the hip or knee: study protocol. BMJ Open 2011;1:e000136.
Ogale S, Hitraya E, Henk HJ. Patterns of biologic agent utilization among patients with rheumatoid arthritis: a
retrospective cohort study. BMC Musculoskelet Disord 2011;12:204.
Overbeek JA, Penning-van Beest FJ, Heintjes EM, Gerber RA, Cappelleri JC, Hovius SE, Herings RM. Dupuytren’s contracture: a retrospective database analysis to determine hospitalizations in the Netherlands. BMC Res Notes 2011;4:402.
Tosteson AN, Tosteson TD, Lurie JD, Abdu W, Herkowitz H, Andersson G, Albert T, Bridwell K, Zhao W, Grove MR, Weinstein MC, Weinstein JN. Comparative effectiveness evidence from the spine patient outcomes research trial: surgical versus nonoperative care for spinal stenosis, degenerative spondylolisthesis, and intervertebral disc herniation. Spine (Phila Pa 1976) 2011;36:2061-8.
general InterestHealth ServicesAbernethy AP, Currow DC. Patient self-reporting in palliative care using information technology: Yes, there is hope! Palliat Med 2011;25:673-4.
Ahmad Kiadaliri A, Najafi B, Haghparast-Bidgoli H. Geographic distribution of need and access to health care in rural population: an ecological study in Iran. Int J Equity Health 2011;10:39.
Angalakuditi M, Gomes J. Retrospective drug utilization review: impact of pharmacist interventions on physician prescribing. Clinicoecon Outcomes Res 2011;3:105-8.
Ajmera M, Wilkins TL, Sambamoorthi U. Dual Medicare and veteran health administration use and ambulatory care sensitive hospitalizations. J Gen Intern Med 2011;26(Suppl. 2):669-75.
Fischer MA, Choudhry NK, Brill G, Avorn J, Schneeweiss S, Hutchins D, Liberman JN, Brennan TA, Shrank WH. Trouble getting started: predictors of primary medication nonadherence. Am J Med 2011;124:1081.
Gilligan AM, Warholak TL, Murphy JE, Hines LE, Malone DC. Pharmacy students’ retention of knowledge of drug-drug interactions. Am J Pharm Educ 2011;75:110.
Grainger D. Can a health professional represent patient views: Industry response. Int J Technol Assess Health Care 2011;27:402.
Hasan SS, Yong CS, Babar MG, Naing CM, Hameed A, Baig MR, Iqbal SM, Kairuz T. Understanding, perceptions and self-use of complementary and alternative medicine (CAM) among Malaysian pharmacy students. BMC Complement Altern Med 2011;11:95.
Jacobs P, Dumont S, Turcotte V, Anderson D. Evaluating the economic loss of caregiving for palliative care patients. J Palliat Care 2011;27:210-5.
Kaakeh R, Sweet BV, Reilly C, Bush C, DeLoach S, Higgins B, Clark AM, Stevenson J. Impact of drug shortages on U.S. health systems. Am J Health Syst Pharm 2011;68:1811-9.
Kamal AH, Bull J, Stinson C, Blue D, Smith R, Hooper R, Kelly M, Kinsella J, Philbrick M, Gblokpor A, Wheeler JL, Downey W, Abernethy AP. Collecting data on quality is feasible in community-based palliative care. J Pain Symptom Manage 2011;42:663-7.
Kannan H, Bolge SC, Del Valle M, Alvir J, Petrie CD. The association between Alzheimer’s disease symptom severity and caregiver outcomes: a cross-sectional study. Prim Care Companion CNS Disord 2011;13.
Lau DT, Briesacher BA, Touchette DR, Stubbings J, Ng JH. Medicare Part D and quality of prescription medication use in older adults. Drugs Aging 2011;28:797-807.
Liu W, Manias E, Gerdtz M. Understanding medication safety in healthcare settings: a critical review of conceptual models. Nurs Inq 2011;18:290-302.
Maharaj S , Roopnarine K, Maharaj V, Maraj S, Sankar E, Singh M, Tayopa OG, Pandey S, Deshpande PR. Impact of chronic disease assistance program on the retail pharmacy sector: A retrospective study. J Pharmacol Pharmacother 2011;2:244-47
Mohandas A, Foley KA, Nash DB, Doria C. Role of quality improvement in prevention of inappropriate transfusions. Qual Manag Health Care 2011;20:298-310.
Morita E, Hamajima N, Hishida A, Aoyama K, Okada R, Kawai S, Tomita K, Kuriki S, Tamura T, Naito M, Kondo T, Ueyama J, Kimata A, Yamamoto K, Hori Y, Hoshinos J, Hamamotos R, Tsukamoto S, Onishi J, Hagikura S, Naito H, Hibi S, Ito Y, Wakai K. Study profile on baseline survey of Daiko Study in the Japan Multi-Institutional Collaborative Cohort Study (J-MICC Study). Nagoya J Med Sci 2011;73:187-95.
O’Reilly D, Gaebel K, Xie F, Tarride JE, Goeree R. Health economic evaluations help inform payers of the best use of scarce health care resources. Int J Circumpolar Health 2011;70:417-27.
Rushton A, Calvert M, Wright C, Freemantle N. Physiotherapy trials for the 21st century - time to raise the bar? J R Soc Med 2011;104:437-41.
Toscani M, Riedl M. Meeting the challenges and burdens associated with hereditary angioedema. Manag Care 2011;20:44-51.
Ward MA, Xu Y. Pharmacist-provided telephonic medication therapy management in an MAPD plan. Am J Manag Care 2011;17:e399-409.
Warholak TL, Holdford DA, West D, DeBake DL, Bentley JP, Malone DC, Murphy JE. Perspectives on educating pharmacy students about the science of safety. Am J Pharm Educ 2011;75:142.
Woelfel JA, Boyce E, Patel RA. Geriatric care as an introductory pharmacy practice experience. Am J Pharm Educ 2011;75:115.
Xie F, Bowen JM, Sutherland SC, Burke N, Blackhouse G, Tarride JE, O’Reilly D, Goeree R. Using health technology assessment to support evidence-based decision-making in Canada: an academic perspective. Expert Rev Pharmacoecon Outcomes Res 2011;11:513-21.
MethodologyCoons SJ, Kothari S, Monz BU, Burke LB. The Patient-Reported Outcome (PRO) Consortium: Filling Measurement Gaps for PRO End Points to Support Labeling Claims. Clin Pharmacol Ther 2011;90:743-8.
Deshpande PR, Rajan S, Sudeepthi BL, Nazir ACP. Patient-reported outcomes: A new era in clinical research. Perspect Clin Res 2011;2:137-44
Hoyle MW, Henley W. Improved curve fits to summary survival data: application to economic evaluation of health technologies. BMC Med Res Methodol 2011;11:139.
Iskedjian M, Jaszewski B, Desjardins O. Comparison of scores derived from the box score-11 scale and the pain attribute of the health utilities index-3. Patient 2011;4:259-65.
Kleijnen J, Westwood M, Whiting P. Applicability of diagnostic studies--statistics, bias and estimates of diagnostic accuracy. Z Evid Fortbild Qual Gesundhwes 2011;105:498-503.
Ram CV, Ramaswamy K, Qian C, Biskupiak J, Ryan A, Quah R, Russo PA. Blood Pressure Outcomes in Smith AB, Daly NL, Craik DJ. Cyclotides: a patent review. Expert Opin Ther Pat 2011;21:1657-72.
Zainuddin Z, Wan Daud WR, Pauline O, Shafie A. Wavelet neural networks applied to pulping of oil palm fronds. Bioresour Technol 2011;102:10978-86. IC

November/December 2011 ISPOR cONNEcTIONS 27
InteRnatIonal SocIety foR PhaRmacoeconomIcS and oUtcomeS ReSeaRch
ABSTRACT SUBmISSION DEADlINE: JANUARY 19, 2012
EARlY REGISTRATION DEADlINE: APRIl 17, 2012
Improving Health Care Efficiency
comPlete meetIng InfoRmatIon and RegIStRatIon at www.ISPoR.oRg
ExhIBIT Register now! Over 2700 attendees in 2011! Present your products and services to key outcomes researchers and health care decision-makers in pharmaceutical, medical device & diagnostics, biotechnology industries, clinical practice, government agencies, academia, and health care organizations. Benefits to Exhibitors: • Company listing & 1/4 page advertisement in the
Program & Schedule of Events • Company listing & 1/4 page advertisement on the
ISPOR website • One complimentary registration per exhibit booth • One complimentary set of pre-registrant mailing
labels per exhibitor
ADvERTISEAdvertise in the Program & Schedule of events! • Company promotion • Job opportunities • Publications • Journals - Full page, full color cover advertising available - 1/4, 1/2, and full page, one color advertising available. Prices start from $950.
SPONSOR Increase your visibility! Give your company increased prominence. Benefits to Sponsors: • Sponsorship recognition at the plenary ses-
sions • Event signage • Company listing & 1/4 page advertisement
in the Program & Schedule of Events • Company listing & logo advertisement on
the ISPOR website • One complimentary meeting registration • Preferential exhibit booth location
advertising Deadline: april 13, 2012
MEETING PROMOTIONAL OPPORTUNITIES
CALL FOR ABSTRACTSProgram Committee ChairSean Tunis, MD, MSc, Founder & Director, Center for Medical Technology Policy, Baltimore, MD, USAResearch Review Committee Co-Chairs:Howard Birnbaum, PhD, Principal, Analysis Group, Inc., Boston, MA, USA Jeff J. Guo, PhD, Professor, Division of Pharmacy Practice & Admin-istrative Sciences, University of Cincinnati Medical Center College of Pharmacy, Cincinnati, OH, USAYi Yang MD, PhD, Associate Professor of Pharmacy Administration and Research Associate Professor, Research Institute of Pharmaceuti-cal Sciences, School of Pharmacy, University of Mississippi, University, MS, USAWorkshop Review Committee Co-Chairs:William D. Marder, PhD, Senior Vice President, Thomson Reuters, Cambridge, MA, USAYa-Chen (Tina) Shih, PhD, MS, Associate Professor, University of Chicago, Section of Hospital Medicine, Chicago, IL, USAIssue Panel Review Committee Co-Chairs:Deirdre Mladsi, BA, Head, Health Economics and Market Access, RTI Health Solutions, Research Triangle Park, NC, USARichard Willke, PhD, Senior Director and Group Lead, Global Health Economics and Outcomes Research, Primary Care, Pfizer, New York, NY, USADecision-maker Case Study Review Committee Chair: TBD

28 November/December 2011 ISPOR cONNEcTIONS
SHORT COURSE PROGRAMSATURDAY, JUNE 2, 2012
(All DAY COURSES) 8:00Am-5:00Pm
Introduction to PharmacoeconomicsThis course demonstrates how to incorporate pharma-coeconomics into study design and data analysis. Participants learn to collect and calculate the costs of different alternatives, determine the economic impact of clinical outcomes, and to identify, track and assign costs to health care resources.
Bayesian Analysis – Overview and ApplicationsThis course provides an overview of the Bayesian approach and its applications to health economics and outcomes research. It covers basic elements of Bayesian statistics, contrasting briefly with classical statistics and introduces available statistical packages. Attendees then apply principles to data analysis problems using WinBUGS.
SATURDAY, JUNE 2, 2012 (mORNING COURSES) 8:00Am-12:00Pm
Introduction to Retrospective Database AnalysisThis course reviews analytic techniques and best practices to improve causal inference in studies using retrospective databases. Specific topics to be covered include: stratification analysis, multivariable regression, propensity scoring, instrumental variable and structural modeling techniques.
Introduction to ModelingThis course introduces the principles and practice of decision analysis. Participants evaluate the appropriateness of decision analysis, construct simple decision trees, understand basic mechanics of tree evaluation and sensitivity analysis, and acquire skills in the interpretation of a published decision analysis.
Cost-Effectiveness Analysis alongside Clinical TrialsThis course presents design, conduct, and reporting of cost-effectiveness analyses alongside clinical trials based in part on The ISPOR RCT-CEA Task Force Report. Analyses guided by an analysis plan and hypotheses, an incremental analysis using an intention to treat approach, characterization of uncertainty and standards for reporting results are presented.
Introduction to Patient-Reported OutcomesConceptual, methodological, and practical methods for measuring quality of life, health status and other types of health outcomes are presented. Theoretical frameworks, reliability, validity, responsiveness, methods of administration, respondent and administrative burdens, and issues of analysis and interpretation are discussed.
Elements of Pharmaceutical/Biotech Pricing I – IntroductionThis course provides a basic understanding of key terminology and issues involved in pharmaceutical pricing decisions. It covers the tools to build and document product value, the role of pharmacoeconomics and the differences in payment systems that shape pricing decisions.
SATURDAY, JUNE 2, 2012 (AFTERNOON COURSES) 1:00Pm-5:00Pm
Patient RegistriesThis course reviews patient registries and their applications in identifying “real world” clinical, safety, and patient-perspective issues. The pros and cons of registry data and how it can support health economics / outcomes research initiatives and decision making are addressed. Registry strategy, design, operations and measures of program success are discussed.
NEW! Pragmatic Trials in Comparative Effectiveness ResearchThe seminar will begin with an overview of the role of Pragmatic Clinical Trials (PCTs) in comparative effectiveness research, review a tool developed to assess the degree to which a trial is ‘pragmatic’ versus ‘explanatory’ and then delve more deeply into specific case studies conducted in the United States and the United Kingdom to highlight key considerations for designing, conducting, and analyzing data from pragmatic trials.
Meta-Analysis and Systematic Reviews in Comparative Effectiveness ResearchThis course discusses six key areas: 1) comparative effectiveness research; 2) impetus for meta-analysis and
systematic reviews; 3) basic steps to perform a quantitative systematic review; 4) statistical methods of combining data; 5) reporting of results; and 6) appraisal and use of meta-analytic reports.
Financial Impact / Cost of IllnessThis course describes methods to determine the cost-of-illness of a health condition using a “top-down” or “bottom-up” approach. Participants learn how to estimate the impact of new health care technologies on disease-specific costs from different decision-maker perspectives.
Case Studies in Pharmaceutical/Biotech Pricing II – AdvancedCase studies lead participants through key steps of new product pricing, focusing on the need to thoroughly analyze the business environment, its constraints and opportunities, and the need to integrate pricing, reimbursement and PE strategies for the new product with clinical development and marketing strategies.
Modeling: Design and Structure of a ModelThis course reviews Markov models and other techniques, referencing the ISPOR Principles of Good Practice for Decision Analytic Modeling in Health Care Evaluations. Using a series of examples, the course reviews practical steps in developing and using these models.
SUNDAY, JUNE 3, 2012 (mORNING COURSES) 8:00Am-12:00Pm
Discrete Event Simulation for Economic Analyses – ConceptsThis course provides a basic understanding of key concepts of discrete event simulation (DES). Topics to be covered are: How does it work, what are the components, where is it used, for which problems is DES well suited, what are the advantages and disadvantages of DES, PSA as a simple task.
Bayesian Analysis – AdvancedThis course focuses on the use of Markov Chain Monte Carlo methods in conducting policy-relevant outcomes research. Participants engage in hands-on exercises and address certain methodological issues, concluding with a discussion on the role of Bayesian methods in policy-making.
Applications in Using Large DatabasesThis course reviews 3 databases – GPRD (UK database), GE Centricity electronic medical record (EMR) and Medicare (USA databases). Each database is discussed in-depth including directions on accessing information and how researchers utilize this information.
Patient-Reported Outcomes – Item Response TheoryApplications of IRT have increased considerably because of its utility for instrument development and evaluation, assessment of measurement equivalence, instrument linking, and computerized adaptive testing. This short course discusses the basics of IRT models and applications to improve health outcomes measurement.
Conjoint Analysis – Theory and MethodsThis course introduces the conceptual basis for quantifying decision-maker preferences for medical interventions and the practical design and analytical issues that must be addressed to obtain valid empirical preference estimates.
Utility Measures This course explores: concepts of health-related quality of life in terms of their differences and similarities; methods used to capture utilities (standard gamble, time trade off and rating scales); and instruments to measure quality of life (EQ-5D, Health Utilities Index and SF-36).
Instrumental Variables in Addressing Selection Bias in Observational StudiesSample selection models provide a test and correction for the presence of selection bias, enabling an investigator to obtain unbiased estimates of treatment effects. This course discusses various models and their applications, in particular instrumental variables.
Statistical Considerations in Health Economic EvaluationsThis course discusses effect of distributional assumptions, analyzing univariate and multivariable analysis data, analyzing
censored data, sample size and power calculations, sampling uncertainty, point estimates for variables, net monetary benefit, and confidence intervals for cost-effectiveness ratios.
SUNDAY, JUNE 3, 2012 (AFTERNOON COURSES) 1:00Pm-5:00Pm
Applications of Statistical Considerations in Health Economic EvaluationsSpecific exercises are conducted to illustrate: effect of distributional assumptions, univariate & multivariable analysis of costs, the effect of sample size & power calculations on economic evaluations, point estimates for cost-effectiveness ratios.
Risk-Sharing/Performance-Based Arrangements for Drugs and Other Medical ProductsThere is significant and growing interest among payers and producers of medical products for arrangements that involve a “pay-for-performance” or “risk-sharing” element. Theory and practice, including incentives and barriers, of these arrangements will be analyzed along with several examples of performance-based schemes from Europe, the United States, and Australia.
Outcomes Research for Medical Devices and DiagnosticsThis course presents outcomes research practices specifically tailored for the medical device and diagnostics technology environment. Outcomes research for medical devices and diagnostics is differentiated from other health care interventions. The evidence hierarchy for medical devices and diagnostic procedures is discussed.
Network Meta-Analysis for Indirect Treatment ComparisonNetwork meta-analysis offers a quantitative method of integrating all the data from all the available comparisons. Based in part on two ISPOR Task Force Reports on Indirect Treatment Comparisons, the fundamentals and concepts of network meta-analysis are presented. The material in this course is motivated by instructive and real examples implemented with the WinBUGS package.
Propensity Scores and Observational Studies of Treatment EffectFaculty discuss how propensity scores can be used to mitigate confounding, the advantages and disadvantages of standard adjustment relative to propensity score-based methods, details of propensity score methodology and risk adjustment models that collapse predictors of outcomes and their use relative to propensity scores.
Establishing Content Validity in Clinical Outcomes Assessment (COA) for Medical Product Approval This course focuses on requirements for establishing the content validity of PRO instruments. Content covers definitions of evidence requirements, issues necessitating clarity, and logistical needs for gathering acceptable evidence. Participants will take part in practical exercises as part of the iterative process to determine and establish evidence of content validity for PRO instruments.
Discrete Event Simulation for Economic Analyses – ApplicationsThis course is structured around practical discrete event simulation exercises. Topics to be covered are: Components of a DES; How do you build a model? Modeling of processes and resource use; Modeling of variables and decisions. Simple animation will be demonstrated. Participants who wish to have hands-on experience must bring laptops.
Advanced Decision Modeling for Health Economic EvaluationsKey aspects in the development of decision modeling, how models can be made probabilistic to capture parameter uncertainty, and how to analyze and present results are discussed. How results should be interpreted and decisions should be made (including decisions with uncertainty, expected value of perfect information [EVPI], and expected value of sample information [EVSI]) are presented.
For complete short course descriptions go to www.ispor.org

November/December 2011 ISPOR cONNEcTIONS 29
CALL FOR ABSTRACTSABSTRACT SUBmISSION BEGINS: OCTOBER 19, 2011 / ABSTRACT SUBmISSION DEADlINE: JANUARY 19, 2012
SUBMISSION INSTRUCTIONSAll abstracts and proposals MUST be submitted through ISPOR’s online abstract submission system by January 19, 2012.Abstracts accepted for other ISPOR meetings can NOT be submitted and research published or presented at other national or international meetings is discouraged.SUBMISSION INSTRUCTIONS, ExAMPLES & SPECIFIC EVALUATION CRITERIA AVAILABLE AT www.ispor.org
RESEARCh ABSTRACTS Outcomes research on all health care interventions (including drugs, devices, behavioral modification programs, surgery, disease prevention, gene therapy, screening, diagnostic procedures and health education) and on all diseases or health disorders are considered. Research abstracts (except for conceptual papers) must be organized by OBJECTIVES, METHODS, RESULTS, CONCLUSIONS. All accepted research abstracts are published in Value in Health as submitted. Accepted research is presented as a 15 minute podium presenta-tion or poster presentation (with a poster author discussion hour). Abstracts are evaluated on the quality of the study (or concept) and quality of the abstract presentation. Research topics include: Clinical Outcomes Studies, Cost Outcomes Studies, Patient-Reported Outcomes & Patient Preference Studies, Health Care Use & Policy Studies, Re-search on Methods, Conceptual Papers. See the ISPOR website for research subtopics, diseases and health care treatments.
hEAlTh CARE DECISION-mAkER CASE STUDY ABSTRACTSHealth care decision-maker case study abstracts must describe an organization’s attempt to integrate cost or outcomes research information into their health care organization’s pro-cesses and procedures. Case Study abstracts must be organized: ORGANIZATION, PROBLEM OR ISSUE ADDRESSED, GOALS, OUTCOMES RESEARCH USED IN THE DECISION, RESULTS, LESSONS LEARNED. Negative as well as positive results are encouraged. Accepted case studies are presented as a 20 minute podium presentation or poster presentation (with a poster author discussion hour). THE PRESENTER MUST BE A HEALTH CARE DECISION-MAKER.
ISSUE PANEl PROPOSAlS Issue panel proposals should show real debate on new or controversial issues in health economics and outcomes research or real debate on the use of outcomes research in health care decision-making. Issue panel proposals must be organized MODERATOR, PANELISTS, ISSUE, OVERVIEW. An accepted issue panel is one hour in duration with a moderator and 2-3 panelists representing different organizations. Panelists should present distinct views about the topic. Issue Panel topics are: Clinical Outcomes Research Issues, Economic Outcomes Research Issues, Patient-Reported Outcomes & Patient Preference Issues, Health Policy Development Using Outcomes Research Issues.
WORkShOP PROPOSAlS Workshop proposals should show novel and innovative experiences in the conduct of outcomes research (including, but not limited to, experiences with conjoint analysis, large data-base analysis, modeling, observational studies, record review, surveys, sensitivity analysis and patient registries) or novel and innovative experiences in the use of outcomes research (clinical, economic, or patient-reported/preference-based outcomes) in health care policy development. Workshop proposals must be organized by DISCUSSION LEADERS, PURPOSE, DESCRIPTION. Accepted workshops are one hour in duration with a minimum of 2 and maximum of 4 discussion leaders (more than one organization must be represented). An audience interactive element must be included in the proposal and during the workshop.Workshop topics include: Clinical Outcomes Research, Economic Outcomes Research, Patient-Reported Outcomes & Patient Preference Research, Use of Real World Data, Health Policy Development Using Outcomes Research. See the ISPOR website for workshop subtopics.
PRELIMINARY PROGRAMmONDAY, JUNE 4: 8:00Am – 8:30PmFIRST PLENARY SESSION: COMPARING THE EFFECTIVENESS OF NEW DRUGS: SHOULD THE FDA / EMA BE ASKING ‘DOES IT WORK’ OR ‘DOES IT WORK BETTER’?The purpose of the FDA is to assure that drugs do more good than harm for their intended uses (i.e. does it work?). Whereas, for healthcare organizations paying for drugs, “does the new drug work better than existing treatments and is any additional cost worth incurring?” are the critical questions. Regulatory and reimbursement decisions are generally made almost simultaneously, relying on a very similar body of evidence, but by different organizations. Might it improve the efficiency with which new drugs get into the market, and overall public health, if regulatory agencies more consistently considered evidence comparing the effectiveness of new drugs to available alternatives, or should they continue their current approach? During this plenary session, the question of whether regulatory agencies should place more emphasis on evidence of comparative effectiveness will be debated.
* 20 Research Podium Presentations * 14 Workshops * 6 ISPOR Group Forums * 5 Issue Panels * Exhibits * 350 Research Poster Presentations – Session I
TUESDAY, JUNE 5: 8:00Am – 8:00PmSECOND PLENARY SESSION: HEALTH REFORM IN THE US: WILL STATE HEALTH INSURANCE EXCHANGES IMPROVE THE EFFICIENCY AND AFFORDABILITY OF HEALTH CARE IN THE US?In the US Patient Protection and Affordable Care Act (ACA) of 2010, States are required to create health insurance exchanges by 2014, with the goal of helping individuals and small businesses to become better informed and higher leverage shoppers for health insurance. Nearly 30 million US citizens are expected to gain access to health coverage through these exchanges, which are expected to reduce costs by spreading risk across a larger group of consumers, increasing price competition between plans with similar benefits, and eliminating hospital cost shifting from uninsured to insured people. During this session, quality and choice of plans, affordability of coverage, ease of enrollment, and cost-containment mechanisms for State health insurance exchanges will be discussed.
* 40 Research Podium Presentations * 14 Workshops * 5 Issue Panels * Exhibits * 350 Research Poster Presentations – Session II * Evening Social Event
WEDNESDAY, JUNE 6: 8:00Am – 4:00PmTHIRD PLENARY SESSION: PERFORMANCE-BASED RISK-SHARING ARRANGEMENTS: GOOD RESEARCH PRACTICES FOR DESIGN, IMPLEMENTATION AND EVALUATIONThere is growing interest among the payers and producers of new drugs and therapeutic devices for arrangements that involve a ‘pay-for-performance’ or ‘risk-sharing’ element. These types of arrangements can be ‘outcomes-based schemes’, ‘risk-sharing agreements’, ‘coverage with evidence development’, ‘access with evidence development’, ‘patient access schemes’, ‘conditional licensing’, and ‘managed entry schemes’. In these payment schemes, the product’s performance is tracked in a defined patient population over a specified period of time. The level of reimbursement is tied by formula to the outcomes achieved. The two critical elements of these schemes are: a) refining clinical impact and outcomes uncertainty, and b) reducing subgroup uncertainty. During this plenary session, recommendations in the Performance-Based Risk-Sharing Arrangements Good Research Practices for Design, Implementation and Evaluation: An ISPOR Task Force Report will be presented. This Report builds on the Banff Consensus Principles with respect to design, builds on the NICE Patient Access Schemes with respect to implementation, and defines good practices for assessing the overall performance of a scheme.
*10 Workshops * 5 Issue Panels * Exhibits * 350 Research Poster Presentations – Session III
Over 2700 attendees in 2011!

PAYMENT INFORMATION
NAME DEGREES
POSITION ORGANIzATION
MAILING ADDRESS
CITY STATE ZIP COUNTRY
TELEPHONE FAx EMAIL
Member ID#
HALF DAY SHORT COURSE FEES Registration Before April 17, 2012: REGULAR FEE: m US$150 / STUDENT FEE: m US$75 Registration After April 17, 2012: REGULAR FEE: m US$200 / STUDENT FEE: m US$100 ALL DAY SHORT COURSE FEESRegistration Before April 17, 2012: REGULAR FEE: m US$300 / STUDENT FEE: m US$150 Registration After April 17, 2012: REGULAR FEE: m US$400 / STUDENT FEE: m US$200
SHORT COURSES ISPOR MEETING REGISTRATION
REGISTRATION FEES QTY FEE TOTAL
Short Course All Day Registration
Short Course Half Day Registration
Meeting Registration
Continuing Education Accreditation
ISPOR Social Event
TOTAL REgISTRATION FEE:
mail Details: If not paying by credit card online, send registration form and payment to: International Society for Pharmacoeconomics and Outcomes Research, 3100 Princeton Pike, Building 3 Suite E, Lawrenceville, New Jersey 08648, USA Tel: 1-609-219-0773 Fax: 1-609-219-0774 • E-Mail: [email protected] • Internet: www.ispor.org Payment Details: Payment may be made by check, travelers check, bank transfer (there is a USD $40 charge) or credit card. VISA, MasterCard, or American Express will be charged in US dollars. Signature, account number and expiration date must be included. Non-US checks written in US$ on banks with a US counterpart are at no charge. For Non-US checks written in US$ on banks with NO US counterpart there is USD $25 charge. Phone charges will NOT be accepted. If payment is being made by your company, please make sure your name is indicated on the check stub or cor-respondence. For bank transfers, please designate the registration name and/or registration number.
* membership Details: If ISPOR cannot verify your current membership, you will be charged the non-member registration rate. When you register as a non-member, you receive an ISPOR membership which includes a one year online subscription to Value in Health - The Journal of the International Society for Pharmacoeconomics and Outcomes Research.** One Day Registration Details: One day registration does not include ISPOR membership benefits and cannot be combined.Cancellation Details: Cancellation fee before April 17, 2012 is US $100. No refunds given after April 17, 2012.
ISPOR member Non-member*
StandardRegistration Before April 17, 2012 m US$650 m US$790Registration After April 17, 2012 m US$750 m US$890
Clinical Practitioners (Clinical Practice, hospital)Registration Before April 17, 2012 m US$450 m US$590 Registration After April 17, 2012 m US$550 m US$690
Full-Time Government and AcademiaRegistration Before April 17, 2012 m US$350 m US$490Registration After April 17, 2012 m US$450 m US$590
Full-Time Students (must provide current enrollment documentation)Registration Before April 17, 2012 m US$150 m US$185Registration After April 17, 2012 m US$200 m US$235
One Day Registration (per day)** (One Day registrations cannot be combined)
__ June 4 __ June 5 __ June 6 m US$350 m US$400
Continuing Education Accreditation m US$100 m US$100
ISPOR Social Event: (Prices subject to change) Tuesday, June 5, 8:00pm-11:30pm m US$50 m US$25 student
SATURDAY, JUNE 2, 2012 All Day Courses 8:00 Am – 5:00 Pmq Introduction to Pharmacoeconomicsq Bayesian Analysis – Overview and Applicationsmorning Courses 8:00 Am – 12:00 Pm q Introduction to Retrospective Database Analysisq Introduction to Modelingq Cost-Effectiveness Analysis alongside Clinical Trialsq Introduction to Patient-Reported Outcomesq Elements of Pharmaceutical/Biotech Pricing I – IntroductionAfternoon Courses 1:00 Pm – 5:00 Pm q Patient Registriesq NEW! Pragmatic Trials in Comparative Effectiveness Research q Meta-Analysis and Systematic Reviews in Comparative Effectiveness Researchq Financial Impact / Cost of Illnessq Case Studies in Pharmaceutical/Biotech Pricing II – Advancedq Modeling: Design and Structure of a Model
SUNDAY, JUNE 3, 2012 morning Courses 8:00 Am – 12:00 Pmq Discrete Event Simulation for Economic Analyses – Concepts q Bayesian Analysis – Advancedq Applications in Using Large Databasesq Patient-Reported Outcomes – Item Response Theoryq Conjoint Analysis – Theory and Methodsq Utility Measures q Instrumental Variables in Addressing Selection Bias in Observational Studiesq Statistical Considerations in Health Economic EvaluationsAfternoon Courses 1:00 Pm – 5:00 Pmq Applications of Statistical Considerations in Health Economic Evaluationsq Risk-Sharing/Performance-Based Arrangements for Drugs and Other Medical Productsq Outcomes Research for Medical Devices and Diagnosticsq Network Meta-analysis for Indirect Treatment Comparisonq Propensity Scores and Observational Studies of Treatment Effectq Discrete Event Simulation for Economic Analyses – Applicationsq Establishing Content Validity in Clinical Outcomes Assessment (COA) for Medical Product Approval q Advanced Decision Modeling for Health Economic Evaluations
Please enclose a check payable in US dollars to: International Society for Pharmacoeconomics and Outcomes Research or ISPOR and send to the ISPOR address below.
Charge to: m VISA m MasterCard m American Express Account Number: ________________________________________________ Expiration Date: ___________
Name: _______________________________________________________________ Authorized Signature: ________________________________________________
FOR MORE INFORMATION: www.ispor.org

< advertisement >
November/December 2011 ISPOR cONNEcTIONS 31

International Society for Pharmacoeconomics and outcomes Research
3100 Princeton Pike, building 3, Suite e
lawrenceville, nJ 08648 USa