Embed Size (px)
Citation preview
Pediatric Diabetes 2009: 10(Suppl. 12): 17–32doi: 10.1111/j.1399-5448.2009.00584.x © 2009 John Wiley & Sons A/SAll rights reserved
Pediatric Diabetes
ISPAD Clinical Practice Consensus Guidelines 2009 Compendium
Type 2 diabetes in children and adolescents
Rosenbloom AL, Silverstein JH, Amemiya S, ZeitlerP, Klingensmith, G Type 2 diabetes in the child andadolescent.Pediatric Diabetes 2009: 10 (Suppl. 12): 17–32.
Arlen L. Rosenblooma,Janet H. Silversteinb,Shin Amemiyac,Phil Zeitlerd andGeorgeanna J Klingensmithe
abDivision of Endocrinology, Department of Pediatrics,University of Florida College of Medicine, Gainesville, FL, USA;cDivision of Endocrinology, Department of Pediatrics, SaitamaMedical University, Saitama, Japan; dDivision of Endocrinology,Department of Pediatrics, The Children’s Hospital, University ofColorado Denver, Aurora, CO, USA; eDepartment of Pediatrics,The Children’s Hospital and Barbara Davis Center, University ofColorado Denver, Aurora, CO, USA.
Corresponding author:Professor Emeritus Arlen L RosenbloomDivision of Endocrinology Department of Pediatrics, Universityof Florida College of Medicine, 1701 SW 16th AvenueGainesville, FL 32608 USA.e-mail: [email protected]
Conflicts of interest: The authors have declared no conflicts ofinterest.
Editors of the ISPAD Clinical Practice Consensus Guide-lines 2009 Compendium: Ragnar Hanas, Kim Donaghue,Georgeanna Klingensmith and Peter Swift.
This article is a chapter in the ISPAD Clinical Practice ConsensusGuidelines 2009 Compendium. The complete set of guidelines canbe found at www.ispad.org. The evidence grading system used inthe ISPAD Guidelines is the same as that used by the AmericanDiabetes Association. See page 2 (the Introduction in PediatricDiabetes 2009; 10 (Suppl. 12): 1–2).
Introduction
Type 2 diabetes mellitus (T2DM) in children andadolescents is becoming an increasingly importantpublic health concern throughout the world (1–17).Because of the relatively recent recognition of theproblem in this age group, many children withnew onset T2DM may be misclassified as havingT1DM. Conversely, as the population becomes heavier,overweight adolescents with autoimmune diabetesmay be misdiagnosed as having T2DM. T2DM isoften associated with risk factors for cardiovasculardisease that may already be present at the time ofdiagnosis, making normalization of blood glucoselevels and diagnosis and treatment of hypertensionand dyslipidemia important (18).
Definition and classification of non-T1DM(non-immune mediated)
Type 2 diabetes (T2DM). T2DM occurs when insulinsecretion is inadequate to meet the increased demandposed by insulin resistance (19). Thus, T2DM iscommonly associated with other features of theinsulin resistance syndrome [hyperlipidemia, hyperten-sion, acanthosis nigricans, ovarian hyperandrogenism,
non-alcoholic fatty liver disease (NAFLD)] (20).Insulin secretion depends on disease status and dura-tion, and can vary from delayed but markedly elevatedin response to a glucose challenge, to absolutely dimin-ished (19). Adults with symptoms have 50% reductionat the time of diagnosis, and may become insulin depen-dent within a few years (21).
T2DM occurs:
• in youth most often during the second decade oflife, with a mean age of diagnosis of ∼13.5 years.This coincides with the peak of physiologic pubertalinsulin resistance, which may lead to onset of overtdiabetes in previously compensated adolescents.
• in all races, but at a much greater prevalence in thoseof non-white European descent, e.g. those of blackAfrican descent, native North American, Hispanic(especially Mexican)-American, Asian, South Asian(Indian Peninsula), and Native Pacific islanders. TheSEARCH for Diabetes in Youth population-basedstudy found the proportion of physician diagnosedT2DM among 10–19-year-olds to vary greatly byethnicity in the US: 6% for non-Hispanic whites, 22%for Hispanics, 33% for blacks, 40% for Asians/PacificIslanders, and 76% for Native Americans (8). InHong Kong > 90% of young onset diabetes is
Update of guidelines previously published in Pediatric Diabetes 2008; 9: 512–526. 17
Rosenbloom et al
T2DM (10), in Taiwan 50% (11) and nearly 60%in Japan (Ogawa et al. personal communication).
• in > 75% of cases in youth in the USA there is a firstor second-degree relative with T2DM.
• in youth in the USA and Europe with body massindex (BMI) above 85th percentile for age andsex. In Japan, however, ∼30% of T2DM are notobese (17), in Asian Indian urban children, half ofthose with T2DM had normal weight (< 120% idealfor height) (12), and half of Taiwanese children withT2DM were not obese (11).
• in some asymptomatic individuals in high-riskpopulations during medical, school, or sportsexaminations (22,23).
• in the presence of ketosis/ketoacidosis, one thirdor more of newly diagnosed patients (24). Thispresentation is responsible for misclassification ofT2DM patients as T1DM.
• occasionally with severe dehydration (hyperosmolarhyperglycemic coma, hypokalemia) at presentation,which can be fatal (24,25)
• with a sex ratio (male:female) that varies from 1:4–1:6 in native North Americans to 1:1 in Asiansand Libyan Arabs
• without associated HLA specificities.• without associated islet cell autoimmunity (see
autoimmunity T2DM).
Autoimmune T2DM
• The pathophysiology of autoimmune ’T2DM’ isunclear. It most likely represents autoimmune T1DMin overweight or obese individuals with underlyinginsulin resistance. It has been postulated that obesityand insulin resistance may promote an inflammatoryresponse to antigen exposure caused by apoptosis ofbeta cells (26).
• Youth and adults in US and Europe who areclinically diagnosed with T2DM are found to haveT1DM-associated auto-antibodies in 15–40% ofcases, including many who are not receiving insulinone year after diagnosis (27–30).
• Antibody positive young adult individuals withthe T2DM phenotype are significantly less over-weight and younger than antibody negativepatients (21, 27).
• Hemoglobin (HbA1c) concentrations are signifi-cantly higher in young adults with T2DM who areantibody positive compared with those who are anti-body negative (27).
• ß-cell function is significantly less in antibody posi-tive individuals, the most dramatic difference beingreported in younger adult patients (25–34 years),resulting in more rapid development of insulin depen-dence, usually by 3 years duration (27, 30).
• The presence of islet cell antibodies (ICA) and glu-tamic acid decarboxylase antibodies in adults withclinically typical T2DM has been referred to aslatent autoimmune diabetes of adults (27, 31). Nei-ther the autoimmunity nor the diabetes is latent,however (26).
Atypical diabetes mellitus or ‘‘Flatbush’’diabetes (32, 33)
• Atypical diabetes mellitus (ADM) occurs throughoutchildhood, but rarely begins past age 40. It has onlybeen described in young people of African descent.
• There is a strong family history in multiplegenerations with an autosomal dominant patternof inheritance, but an abnormal sex ratio (M : F =1 : 3).
• ADM is not associated with HLA specificities andislet autoimmunity does not occur.
• Ketosis or ketoacidosis is typical at onset.• Insulin secretion is present but diminished and with-
out long-term deterioration of function. Interest-ingly, insulin is often not required for survival aftertreatment of acute metabolic deterioration, althoughdiabetes control may be poor and ketoacidosis mayrecur without insulin, e.g. with illness or pregnancy.
• ADM is not associated with obesity beyond that inthe general population and it is not associated withinsulin resistance.
Monogenic diabetes (formerly referred to as maturityonset diabetes of the young or MODY) For more indepth information see the ISPAD Clinical ConsensusGuidelines for Monogenic Diabetes (34).
• Identified in families with multigenerational dia-betes; including asymptomatic individuals identifiedthrough testing of family members.
• Monogenic diabetes is not associated with obesitybeyond that in the general population and it is notassociated with insulin resistance
Uncertainties of Classification
Distinguishing T2DM from T1DM or monogenicdiabetes
The clinician is obliged to weigh the evidence in eachindividual patient to distinguish between T1DM andT2DM. The reasons for this conundrum are:
• with increasing obesity in childhood, as many as15–25% of newly diagnosed T1DM (or monogenicdiabetes) patients may be obese.
• the significant number of pediatric patients withT2DM demonstrating ketonuria or ketoacidosis atdiagnosis (2).
18 Pediatric Diabetes 2009: 10 (Suppl. 12): 17–32
Type 2 diabetes
• T2DM is common in the general adult population,with a random family history of ∼15% or greaterin minority populations, reducing the specificity of apositive family history.
• positive family history for T2DM is increased forpatients with T1DM as much as threefold over thenon-diabetic population and T1DM is more frequentin relatives of patients with T2DM (35, 36).
• There is considerable overlap in insulin or C-peptidemeasurements between T1DM, T2DM and MODYat onset of diabetes and over the first year orso. This overlap is due to the recovery phase ofautoimmune-mediated T1DM (the honeymoon) anddegree of glucotoxicity/lipotoxicity impairing insulinsecretion at the time of testing in both T1DM andT2DM. In addition the insulin resistance of obesityraises residual C-peptide levels in obese adolescentswith T1DM. Such measurements are thus relativelyvalueless in the acute phase.
[The role of C peptide may be more helpful inestablished diabetes as persistent elevation of C-peptideabove the level of normal would be unusual in T1DMafter 12–24 months.]
Diagnosis of type 2 diabetes
The criteria and classification of diabetes are presentedin greater detail in the ISPAD Clinical Practice Consen-sus Guidelines: Definition, Epidemiology, Diagnosisand Classification of Diabetes (37)
Diagnostic criteria for type 2 diabetes in childhood andadolescence. Diagnostic criteria for diabetes are basedon BG measurements and the presence or absence ofsymptoms (E) (38,39).
Three ways to diagnose diabetes are possible andeach, in the absence of unequivocal hyperglycemia,must be confirmed, on a subsequent day, by any one ofthe three methods given below.
• Diabetes is diagnosed when:
• A fasting plasma glucose (FPG) is ≥ 7.0 mmol/l(126 mg/dl)or
• The post challenge plasma glucose is >
11.1 mmol/l (200 mg.dl)
• performed as described by the World HealthOrganization (39), using a glucose load contain-ing the equivalent of 75 g anhydrous glucosedissolved in water.
or• Symptoms of diabetes and a casual plasma glucose
≥ 200 mg/dl (11.1 mmol/L).
• Casual is defined as any time of day without regardto time since last meal. The classic symptomsof diabetes include polyuria, polydipsia, andunexplained weight loss.
• Diabetes in children, including T2DM, usuallypresents with characteristic symptoms such aspolyuria, polydipsia, blurring of vision, and weightloss, in association with glycosuria and, in somecases, ketonuria.
• In its most severe form, ketoacidosis or hyper-glycemic hyperosmolar state may develop and leadto stupor, coma, and in absence of effective treat-ment, death.
• The diagnosis is usually confirmed quickly insymptomatic individuals by measurement of amarked elevation of the blood glucose level. In thissituation, if ketones are present in the blood or urine,treatment is urgent. Waiting another day to confirmthe hyperglycemia may be dangerous in allowingketoacidosis or hyperosmolarity to evolve.
• In the absence of symptoms or presence ofmild symptoms of diabetes, hyperglycemia detectedincidentally or under conditions of acute infective,traumatic, circulatory, or other stress may betransitory and should not in itself be regarded asdiagnostic of diabetes. The diagnosis of diabetes, inthe absence of symptoms, should not be based on asingle plasma glucose concentration. Diagnosis mayrequire continued observation with fasting and/or2-h postprandial BG levels and/or an oral glucosetolerance test (OGTT).
• An OGTT should not be performed if diabetes canbe diagnosed using fasting, random, or postprandialcriteria, as excessive hyperglycemia can result usinga fasting OGTT in these circumstances. (E).
• If doubt remains, periodic re-testing should beundertaken until the diagnosis is established orrefuted.
Diagnostic criteria for impaired glucose tolerance andimpaired fasting glycemia. There are individuals whoseglucose levels do not meet the criteria for diabetes, butare too high to be considered normal.
• Impaired glucose tolerance (IGT) and impairedfasting glycaemia (IFG) are intermediate stagesin the natural history of disordered carbohydratemetabolism between normal glucose homeostasisand diabetes (E).
• IFG and IGT are not interchangeable and representdifferent abnormalities of glucose regulation. IFG isa measure of disturbed carbohydrate metabolism inthe basal state, while IGT is a dynamic measureof carbohydrate intolerance after a standardizedglucose load.
Pediatric Diabetes 2009: 10 (Suppl. 12): 17–32 19
Rosenbloom et al
• Patients with IFG and/or IGT are now referredto as having ‘pre-diabetes’, indicating the relativelyhigh risk for development of diabetes in thesepatients (38).
• IFG and IGT may be associated with the metabolicsyndrome (MS), which includes obesity (especiallyabdominal or visceral obesity), dyslipidemia of thehigh-triglyceride and/or low-high density lipoproteintype, and hypertension.
• Individuals who meet the criteria for IGT or IFGmay be euglycemic in their daily lives as shown bynormal or near-normal glycated hemoglobin levels,and those with IGT may manifest hyperglycemiaonly when challenged with an OGTT.
Categories of fasting plasma glucose (FPG) aredefined as follows:
• FPG < 5.6 mmol/L (100 mg/dL)= normal fastingglucose.
• FPG 5.6–6.9 mmol/L (100–125 mg/dL)= IFG.
• FPG ≥ 7.0 mmol/L (126 mg/dL)= provisional diag-nosis of diabetes (the diagnosis must be confirmed, asdescribed above under ‘Diagnostic criteria for type 2diabetes’).
The corresponding categories for IGT when theOGTT is used are as follows:
• 2-h postload glucose < 7.8 mmol/l (140 mg/dl)=normal glucose tolerance.
• 2-h postload glucose 7.8–11.1 mmol/l (140–199 mg/dl)= IGT.
• 2-h postload glucose > 11.1 mmol/l (200 mg/dl)=provisional diagnosis of diabetes (the diagnosis mustbe confirmed with additional testing, as describedabove).
After the diagnosis of diabetes is established,autoantibody testing should be considered whendiagnosing and treating T2DM. Diabetes autoantibodytesting should be considered in all pediatric patientswith the clinical diagnosis of T2DM because of thehigh frequency of islet cell autoimmunity in otherwise‘‘typical’’ T2DM. Antibodies will indicate an earlierneed for insulin as well as the need to monitorfor thyroid autoimmunity and to consider otherautoimmune disorders associated with T1DM. (E)
Diabetes autoantibody testing also should be con-sidered in overweight/obese children > 13 years of agewith a clinical picture of T1DM (weight loss, keto-sis/ketoacidosis), some of whom may have T2DM (E)
T2DM and the insulin resistance syndrome
Insulin resistance is an impaired response to thephysiologic effects of insulin, including effects on
glucose, lipid, and protein metabolism, and on vascularendothelial function. Insulin resistance occurs in mosttissues including liver, muscle, and fat tissue and is influ-enced by sex, age, race/ethnicity, stage of sexual mat-uration, and total adiposity. While visceral adiposityis important in insulin resistance in adults, the specificcontribution of visceral adiposity to insulin resistancein the pediatric population remains uncertain.
Several events in development may be associatedwith increased risk for the insulin resistance syndrome.These include premature adrenarche in girls (pubichair appearing before the age of 8 years) and beingborn small for gestational age. Girls with a historyof premature adrenarche are at increased risk forovarian hyperandrogenism and PCOS and thus, insulinresistance (40). Children born small for gestational ageare at increased risk for insulin resistance related todecreased intrauterine growth (41) and also at increasedrisk for premature adrenarche.
Diabetes is only one manifestation of the insulinresistance syndrome or the MS (22, 42–50).
Other associations include:
(i) Obesity: Obesity has deleterious associations withmorbidity and cardiovascular risk independentof effects related to insulin resistance and dia-betes (51–54).
(ii) Nephropathy: Albuminuria (either micro- ormacro-) is present at the time of diagnosisin a substantial number of adolescents withT2DM and prevalence increases with durationof diabetes (24). Proteinuria and focal segmentalglomerular sclerosis have also been reported inAfrican-American adolescents with severe obe-sity, in the absence of diabetes (55).
(iii) Hypertension; Hypertension is estimated toaccount for 35–75% of diabetes complications,both microvascular and macrovascular (56). Dia-betes or impaired glucose tolerance doubles therisk of developing hypertension (57). In addi-tion, there is a possible genetic predisposition tohypertension in T2DM related to the associatedangiotensin converting enzyme genotype (58).Hypertension in T2DM is due to volume expan-sion and increased vascular resistance (59) relatedto reduced (NO)-mediated vasodilatation andincreased activity of the renin-angiotensin system.
(iv) Dyslipidemia: Hypertriglyceridemia and decrea-sed high-density lipoprotein cholesterol are thehallmarks of T2DM dyslipidemia. Additionalfindings include elevated very low-density lipopro-tein (VLDL), elevated LDL-c, elevated lipopro-tein(a), and increased small dense LDL particles.Decreased lipoprotein lipase activity, increasedlipoprotein glycation and increased lipoproteinoxidation render the lipoproteins more athero-genic. (60,61)
20 Pediatric Diabetes 2009: 10 (Suppl. 12): 17–32
Type 2 diabetes
(v) Ovarian hyperandrogenism and premature adre-narche (62): PCOS is being increasingly rec-ognized in adolescents as part of the insulinresistance syndrome. Adolescents with PCOShave ∼40% reduction in insulin-stimulated glu-cose disposal compared to body composi-tion matched non-hyperandrogenic control sub-jects (59). Decreasing insulin resistance mayimprove ovarian function and increase fertility.
(vi) NAFLD: Hepatic steatosis is present in 25–45%of adolescents with T2DM and more advancedforms of NAFLD, such as non-alcoholic steato-hepatitis, are increasingly common and associatedwith progression to cirrhosis (24, 64). NAFLDnow represents the most common cause of cirrho-sis in children and the most common reason forliver transplantation in adults in the US.
(vii) Systemic inflammation: elevated C-reactive pro-tein, inflammatory cytokines and white blood cellcounts in obese adolescents have been associatedwith increased risk for cardiovascular disease inadults (54).
Additional health problems related to obesityinclude Obstructive sleep apnea (OSA) with associatedpulmonary hypertension (65), orthopedic problemsresulting in diminishing physical activity (66,67),pancreatitis, cholecystitis and pseudotumor cerebri.
In adults, there is a strong association between levelof hyperglycemia and increased risk of macrovasculardisease. Hyperglycemia, dyslipidemia, and hyperten-sion are contributors to the acceleration of atheroscle-rosis in T2DM, along with oxidative stress, glycation ofvascular proteins, and abnormalities of platelet func-tion and coagulation. Defective endothelium depen-dent vasodilatation is an additional factor acceleratingatherosclerosis in T2DM. It is an early sign of increasedrisk for cardiovascular disease, and predictive of car-diovascular events (68) (B) and occurs in obese childrenrelative to their level of obesity and degree of insulinresistance (69) (B).
The aggregation of risk factors for cardiovasculardisease in the presence of insulin resistance anddiabetes may result in a high risk for coronaryevents and increased mortality in youngadulthood (A)
Testing for Co-morbidities and Complications. Co-morbidities characteristic of the insulin resistancesyndrome are commonly seen at diagnosis or appearearly in the course of T2DM and should be testedfor sooner than in T1DM, where these disordersare complications of the diabetes rather than co-morbid conditions (70, 71) (B). A more completediscussion of testing for complications/co-morbidities is
presented in the ISPAD Clinical Practice Guidelines formicrovascular and macrovascular complications (72).
Specific complications are more common in type 2diabetes and need special attention.
• Either micro- or macro-albuminuria, may be presentat the time of diagnosis and albuminuria should beevaluated at diagnosis and annually thereafter (55,72)(E). Likewise, hypertension may be presentat, or prior to diagnosis of diabetes and eachindividual should be evaluated at every visit forhypertension. Dyslipidemia is more common intype 2 diabetes and in family members, (60,61) andshould be screened for when metabolic stabilityis achieved. Evaluation for NAFLD should bedone at diagnosis and annually thereafter (24)(E).Inquiries about puberty, menstrual irregularities andobstructive sleep apnea should be made at diagnosisand regularly thereafter (65)(E).
Treatment of comorbidities/complications
Additional information is available in the ISPADClinical Practice Guidelines on complications. (72).
Dyslipidemia, hypertension and albuminuria aremore common in type 2 diabetes compared to type 1diabetes and may be present at diagnosis and should beassessed after blood glucose control has been optimized.
Hypertension and albuminuria.
• Confirmed hypertension (BP> 95% for age, genderand height) or albuminuria should be treated withan ACE inhibitor or, if not tolerated, an angiotensinreceptor blocker (E).
• Combination therapy may be required if hyperten-sion or albuminuria does not normalize on singleagent treatment (E).
(a) Side effects are cough, hyperkalemia, headacheand impotence (73). In addition, major con-genital malformations have been reported withfirst trimester exposure to ACE inhibitors butnot with other antihypertensive agents in non-diabetic women (74).
Dyslipidemia. Testing for dyslipidemia should beperformed soon after diagnosis when BG control hasbeen achieved and annually thereafter. (60,61) E
• Goal is LDL-C < 2.6 mmol (100 mg/dl) (68).• If LDL-C is borderline (2.6-3.4 mmol;100–129 mg/
dl), or elevated (� 3.4 mmol; 130 mg/dl), repeat lipidprofile should be performed in 6 months and dietaryintervention to decrease total and saturated fatinitiated.
Pediatric Diabetes 2009: 10 (Suppl. 12): 17–32 21
Rosenbloom et al
• If LDL-C remains elevated after 3-6 months ofattempting to optimize blood glucose control anddiet, pharmacotherapy is warranted (72).
• Statin therapy has been shown to be safe and effectivein children as in adults and should be the firstpharmacologic intervention (72) although long termsafety data are not available. Special attention shouldbe paid to symptoms associated with muscles andconnective tissues, as there is an increased risk ofrhabdomyolysis (72,75).
Treatment of T2DM
Management differences Between Type 2 and Type 1Diabetes. The emergence of T2DM in children andadolescents has required that specialists familiar withthe management of T1DM in children and adolescentsrecognize the vast differences between the treatmentchallenges of these two disorders.
• Lower socioeconomic status. Whereas T1DM isdistributed throughout the population proportionateto socioeconomic distribution, T2DM in NorthAmerica and Europe disproportionately affectsthose with fewer resources, e.g. lower income
levels, less educated parents, less well insured. Thissocioeconomic bias has not been described for AsianT2DM.
• Older age. T1DM occurs throughout childhood,when parental influence is predominant, whereasT2DM occurs typically in adolescence, when peerinfluence predominates.
• More family experience. Only ∼5% of families witha child with T1DM have family experience with thedisease, while 75% or more of families of the childwith T2DM have such experience. The failure of thesefamily members to control weight and glycemia iscommon, with resultant complications in the familymembers and a feeling of fatalism and resignation inthe child.
• Different treatment priorities. In most T1DM,lifestyle modification, beyond insulin administrationand glucose monitoring, is only needed for thoseindividuals who are overweight and inactive. Inall youth with T2DM, the emphasis is on lifestylemodification and secondarily on glucose monitoringand medication.
• Negative effects of technology. Technologicaladvancements have revolutionized the managementof T1DM (insulin purity and delivery systems, blood
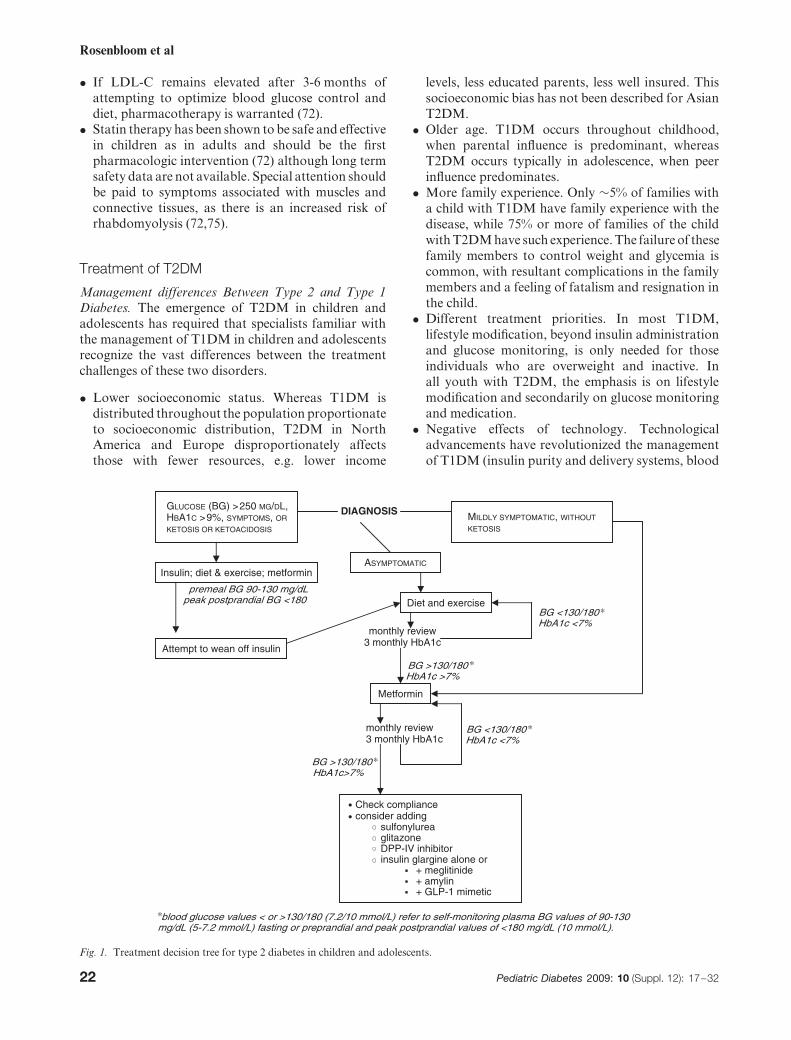
DIAGNOSIS
premeal BG 90-130 mg/dLpeak postprandial BG <180
BG <130/180HbA1c <7%
monthly review3 monthly HbA1c
BG >130/180HbA1c >7%
monthly review3 monthly HbA1c
BG <130/180HbA1c <7%
BG >130/180HbA1c>7%
MILDLY SYMPTOMATIC, WITHOUT
KETOSIS
GLUCOSE (BG) >250 MG/DL,HBA1C >9%, SYMPTOMS, OR
KETOSIS OR KETOACIDOSIS
ASYMPTOMATIC
Diet and exercise
Attempt to wean off insulin
Insulin; diet & exercise; metformin
Metformin
Check complianceconsider adding
sulfonylureaglitazoneDPP-IV inhibitorinsulin glargine alone or
+ meglitinide+ amylin+ GLP-1 mimetic
blood glucose values < or >130/180 (7.2/10 mmol/L) refer to self-monitoring plasma BG values of 90-130mg/dL (5-7.2 mmol/L) fasting or preprandial and peak postprandial values of <180 mg/dL (10 mmol/L).
Fig. 1. Treatment decision tree for type 2 diabetes in children and adolescents.
22 Pediatric Diabetes 2009: 10 (Suppl. 12): 17–32
Type 2 diabetes
glucose monitoring, insulin analogues). In contrast,technological advances in entertainment, labor sav-ing devices, transportation, together with an eco-nomic environment that makes calorically densefood increasingly available, desirable, and inexpen-sive, have led to the emergence of T2DM in childrenand complicate its therapy.
Management Goals. Overall goals
• Weight loss• Increase in exercise capacity• Normalization of glycemia• Control of comorbidities, including hypertension,
dyslipidemia, nephropathy, and hepatic steatosis,
Reduction in the rate of complications may requiremore stringent control in insulin resistant T2DMthan in T1DM, and especially diligent attention tocomorbidities, as suggested by the United KingdomProspective Diabetes Study (21).
Education. See also the ISPAD Clinical PracticeGuidelines for diabetes education (76).
Patient and family education for youth with type2 diabetes is as important as it is in type 1 diabetes.Initial and on-going education for T2DM will focuson behavioral changes (diet and activity). Education ininsulin therapy and hypoglycemia may not be requiredimmediately.
• Education in T2DM will place a greater emphasison behavioral, dietary and physical activity changesthan is generally required for T1DM.
• Education should be given by team members withspecial expertise and knowledge of the dietary,exercise, and psychological needs of youth withT2DM
• Education should be provided in a culturally sensitiveand age appropriate manner
• Because the majority of youth with T2DM areadolescents, the ISPAD Guidelines for AdolescentCare are appropriate to the education of youth andfamilies with T2DM
• The entire family will need education to understandthe principles of treatment of T2DM and tounderstand the critical importance of the lifestylechanges required to manage T2DM
• Care providers should acknowledge that the initialuncertainty in the diagnosis i.e. type 1 vs type 2, ina minority of patients can be confusing and anxietyprovoking for the youth and family. The anxietycan be minimized by emphasizing the importanceof normalizing blood glucose metabolism usingwhatever therapy is appropriate to the metaboliccircumstances of the specific individual, regardless ofthe ‘type’ of diabetes.
Behavioral Change. Lifestyle change is the corner-stoneof treatment of T2DM
• The family and child should understand the medicalimplications of obesity and T2DM.
• Clinicians must have an understanding of the healthbeliefs and behaviors of the family/community todesign an effective behavioral plan.
• Changes should be made in small achievableincrements and with the understanding that thesechanges need to be permanent.
• The patient and family should be trained to monitorthe quantity and quality of food, eating behavior,and physical activity.
• As in any behavioral change, a changing andsustainable reward system is essential for success.
• The education and treatment team for T2DM ideallyshould include a nutritionist, psychologist and/orsocial worker (77).
Dietary Management. Referral to a nutrition-ist/dietitian with knowledge and experience in nutri-tional management of children with DM is necessary.Dietary recommendations should be culturally appro-priate, sensitive to family resources, and should beprovided to all caregivers (78, 79). The family shouldbe encouraged to make dietary changes consistent withhealthy eating recommendations, including individu-alized counseling for weight reduction, reduced totaland saturated fat intake, increased fiber intake, andincreased physical activity (80). More specific dietaryrecommendations are given in the ISPAD Guidelinesfor dietary management (81).
Dietary management should include:
• Initial focus on eliminating sugar-containing softdrinks and juices in large quantities.
• Complete elimination of these drinks and substitut-ing water, diet soft drinks, and artificial sweetenersfor beverages can result in substantial weight lossand is one of the most important dietary/behavioralchanges for successful weight loss.
• Lifestyle (diet and activity) modification for the entirefamily and for the patient in an age appropriatemanner, including guidance about healthy dietaryand activity habits
• Emphasizing healthy rearing patterns related to dietand activity by teaching parental modeling of healthyhabits, avoiding overly strict dieting, and avoidingusing food for reward
• Recommending that meals should be taken onschedule, in one place, with no other activity(television, studying, reading, playing), preferablyas a family unit.
• Portion control. Food and snacks should be servedin a plate or bowl and not eaten directly from a boxor can.
Pediatric Diabetes 2009: 10 (Suppl. 12): 17–32 23
Rosenbloom et al
• Limiting availability of high-fat, high caloric densityfood and drink in the home, the reading of labels andcontrol of purchasing.
• Encouraging positive reinforcement of minorachievement (e.g. no or minimal weight gain, reduc-tion in high caloric drinks) and avoiding blame forfailure.
• Maintaining food and activity logs as beneficial forraising awareness of food and activity issues and formonitoring progress.
Exercise management. Specific, negotiated and enjoy-able exercise prescriptions should be developed for eachpatient and family that are sensitive to family resourcesand environment, and should be provided to all care-givers. A family member or friend should be identifiedwho is available to participate in physical activity withthe patient. Pedometers may be motivating to patientsand family members.
Frequent follow up to determine success with thedietary and exercise changes is important to the successof the program.
Exercise management should include:
• Developing and encouraging an achievable dailyexercise program is essential to breaking thevicious cycle of increased weight-increased torpor-decreased activity-increased weight. Approachesaimed primarily at reducing sedentary time, such asturning off the TV and decreasing the time spent incomputer related activities, may be the most effectiveinitially (82) (A).
• Physical activity needs to be promoted as a family.This should include daily efforts to be physicallymore active, such as using stairs instead of elevators,walking or bicycling to school and to shop, and doinghouse and yard work (E).
• Educate parents for healthy behavior reinforcement,teach them to encourage and praise physical activity,including increases in daily activities (E).
Glycemic Monitoring.
(i) Self monitoring of blood glucose (SMBG)should be performed regularly. Frequency ofSMBG should be individualized, and include acombination of fasting and postprandial glucosemeasurements. Once glycemic goals have beenachieved, several fasting values a week and dailypost prandial values, taken after the biggest mealare satisfactory while the values remain withinthe target range (E). If values rise into theimpaired glucose tolerance range, more frequenttesting should be recommended for adjustment oftherapy. During acute illness or when symptomsof hyper- or hypoglycemia occur, patients should
perform more frequent testing and be in contactwith their diabetes care team for advice (E).Patients on insulin or sulfonylureas need tomonitor for asymptomatic hypoglycemia (E).
(ii) HbA1c concentration should be determined atleast twice a year and quarterly if insulin is beingused or metabolic control is unsatisfactory.
Pharmacologic therapy. Lifestyle change should becontinued in addition to pharmacologic therapy(Fig. 1). The aim of pharmacologic therapy is todecrease insulin resistance, increase insulin secretion,or to slow postprandial glucose absorption. The firstmedication used should be metformin. It has theadvantage over sulfonylureas of similar reduction inHbA1c without the risk of hypoglycemia. Furthermore,weight is either decreased or remains stable, and LDL-Cand triglyceride levels decrease during treatment.
Failure of monotherapy with metformin over3 months indicates the need to add a Glitazone,sulfonylurea, or insulin alone or in combination withmeglitinide, amylin, a GLP-1 mimetic, or a DPP-IVinhibitor (Fig. 1).
• Patients at-risk for pregnancy should be counseled onthe effects of diabetes and oral agents on conceptionand fetal development. No oral agent should be usedduring pregnancy.
• Only metformin and insulin are approved for usein children/adolescents in the majority of countries.Sulfonylureas are approved for use in children insome countries; other oral agents are described belowwith the understanding that some adolescents maybenefit from their use.
• Thiazolidinediones may be used in older adolescentsbut these are not approved in those under 18 years.Combination formulations may improve compliancein these older patients.
Available hypoglycemic agents. Biguanides. Metforminacts on insulin receptors in liver, muscle, and fat tissue,with a predominant action on the liver.
• Hepatic glucose production is reduced by decreasinggluconeogenesis
• Insulin stimulated glucose uptake is increased inmuscle and fat
• An initial anorexic effect may promote weight loss• Long-term use is associated with a 1–2% reduction
in HbA1c.• Intestinal side effects (transient abdominal pain,
diarrhea, nausea) may occur. These can be eliminatedin most patients with slow dosage titration over 3–4weeks, and instructions to always take the medicationwith food. The side effects may be attenuated by theuse of extended release formulations.
24 Pediatric Diabetes 2009: 10 (Suppl. 12): 17–32
Type 2 diabetes
• The risk of lactic acidosis with metformin is extremelylow. Metformin should not be given to patientswith renal impairment, hepatic disease, cardiacor respiratory insufficiency, or who are receivingradiographic contrast materials. Metformin shouldbe temporarily discontinued during a gastrointestinalillness (A).
• Metformin may normalize ovulatory abnormalitiesin girls with PCOS and increase pregnancy risk (A).
Insulin. Despite hyperinsulinemia and insulin resis-tance, relatively small doses of supplemental insulinare often effective. If there is inadequate glycemic con-trol on oral agents, a long-acting insulin analoguewithout peak effects may provide satisfactory ther-apy without meal related therapy. Metformin shouldbe continued to improve insulin sensitivity. Thiazo-lidinediones are not recommended in combination withinsulin because of increased risk for fluid retention withthe combination.
• If post-prandial hyperglycemia occurs, pre-mealmeglitinide is a good initial choice. If post-prandialhyperglycemia persists, rapid or short acting insulincan be substituted.
• The side effects of insulin are hypoglycemia, whichhas not been common in T2DM treated with insulin,and weight gain, a substantial problem in thispopulation if dietary measures are not attended to.
• In adults with inadequately controlled T2DM frommultiple centers in Europe and Australia, a singledaily injection of insulin glargine, a long acting(24 hours) analog with little or no peak action, wasalmost as effective as three times a day rapid insulinanalog (83).
Sulfonylurea and meglitinide/repaglinide (may notbe approved for use in those < 18 years)
• Increase insulin secretion; thus most useful whenthere is residual beta cell function
• Sulfonylureas bind to receptors on the K + /ATPchannel complex causing K+ channels to close,resulting in insulin secretion
• Meglitinide and repaglinide bind to a separate siteon the K + /ATP channel complex
• Sulfonylurea sites equilibrate slowly and bindingpersists for prolonged periods; thus, traditionalsulfonylureas have prolonged effects
• Meglitinide/rapaglinide have an intermediate equili-bration and binding duration and are, thus, used forrapid enhancement of insulin secretion, e.g. beforemeals
• Major adverse effects of sulfonylureas are hypo-glycemia, which can be prolonged, and weight gain.
TZDs (only approved for use in adults). Clinical trialshave been, or are underway in children with this classof drugs.
• TZDs increase insulin sensitivity in muscle, adipose,and liver tissue, with a greater effect on muscleglucose uptake than biguanides.
• TZDs bind to nuclear proteins, activating per-oxisome proliferator activator receptors (PPARgamma), which are ubiquitous orphan steroid recep-tors particularly abundant in adipocytes. This acti-vation ultimately increases formation of proteinsinvolved in the nuclear based actions of insulin,including cell growth, adipose cell differentiation,regulation of insulin receptor activity, and glucosetransport into the cell. The binding of the thiazo-lidinediones to PPARgamma receptors is ubiqui-tous, affecting muscle cell growth and migration inresponse to growth factors, including arterial wallssmooth muscle.
• Long-term treatment in adults is associated with areduction in HbA1c of 0.5–1.3%.
• Thiazolidinediones have differing effects on lipidprofiles.
• Side effects include edema, weight gain, anemia,and possible increased risk of heart disease inadults (84,85).
• Liver enzyme elevations were found in ∼1% of thosetaking the original member of this group, troglita-zone, with fatalities resulting in its withdrawal. Thenewer thiazolidinediones (rosiglitazone and pioglita-zone) appear not to have hepatotoxicity in adults.
Glucosidase inhibitors (these drugs are onlyapproved for use in adults)
Alpha glucosidase inhibitors (acarbose, miglitol)reduce the absorption of carbohydrates in theupper small intestine by inhibiting breakdown ofoligosaccharides, thereby delaying absorption in thelower small intestine. This reduces the postprandial riseof plasma glucose.
• Long-term therapy is associated with 0.5-1%reduction in HbA1c (86).
• The frequent side effect of flatulence makes theseagents unacceptable to most adolescents.
Amylin (amylin is not approved for those under18 years, and is only approved for use in the USfor patients with T1DM and T2DM who aretaking insulin)
• Amylin is administered by subcutaneous injectionbefore meals.
Pediatric Diabetes 2009: 10 (Suppl. 12): 17–32 25
Rosenbloom et al
• Amylin peptide is co-secreted with insulin frompancreatic beta cells in response to food. Itlowers BG by decreasing glucagon release, slowinggastric emptying and decreasing food intake. Theprincipal adverse effects are hypoglycemia andnausea, prompting the manufacturer to recommenddecreasing the insulin dose by 50% when treatmentwith amylin is initiated (87).
• Treatment produces mild reductions in HbA1c.• Modest weight loss or weight stabilization is
generally seen with amylin treatment.• There is a reported study of amylin use in children
with T1DM (88)
Incretin mimetics (glucagon-like peptide-1receptor agonists) (exenatide) (89) (these drugsare only approved for use in adults)
• Incretin mimetics are given as a twice-daily subcuta-neous injection, usually with breakfast and dinner.In normal physiology, GLP-1 is rapidly secreted byL-cells in the small intestine into the circulation inresponse to food, increasing insulin secretion propor-tionate to BG concentrations, suppressing glucagon,prolonging gastric emptying, and promoting satiety.They are rapidly degraded by dipeptidyl peptidase-IV (DPP-IV); both native GLP-1 and the injectedmimetic have a half life of 2 minutes.
• Clinical trials in adults have shown reduced fastingand post-prandial BG, weight loss, and lowerHbA1c. Adverse effects include nausea, vomiting,diarrhea, with nausea occurring in up to 44% ofpatients; and infrequent dizziness, headache, anddyspepsia. The nausea decreases over time.
DPP-IV Inhibitors (89) (these drugs are onlyapproved for use in adults)
• DPP-IV inhibitors inhibit the enzyme that breaksdown GLP-1, resulting in higher concentrations ofGLP-1 producing effects similar to those of GLP-1 mimetics.
• Unlike GLP-1 mimetics, they have no effect ongastric emptying, satiety or weight loss.
• They are administered orally with metformin or athiazolidenedione once daily.
initial medical treatment:
Initial treatment modality is determined by symptoms,severity of hyperglycemia, and presence or absence ofketosis/ketoacidosis. As in T1DM, those with symptoms,particularly vomiting, can deteriorate rapidly and needurgent assessment and treatment (E)
1. If metabolically stable, metformin is the treatment ofchoice (E)
a. Begin with 250 mg daily x 3–4 days, if tolerated,increase to 250 mg BID, titrate in this manner over3–4 weeks until the maximal dose of 1000 mg BIDis reached.
2. Insulin may be required for metabolic stabilization(A)
3. Transition from insulin to metformin can usuallybe made over 2-6 weeks beginning when metabolicstability is reached, usually 1-2 weeks after diagnosis(E)
4. Transition can usually be achieved safely by titrationof the metformin as in # 1 above. Insulin may bedecreased by 10–20% each time the metformin isincreased with a goal of eliminating insulin therapy(E)
5. Blood glucose testing may be decreased to twice aday, fasting and 2-3 hours after the largest meal, wheninsulin is eliminated (E)
6. If at any time during the insulin taper, the glucosevalues rise into the impaired range, the taper shouldbe slowed until values stabilalize. If the glucosevalues are in the diabetic range, the diagnosis ofT2DM should be reconsidered and lifestyle changesreinforced (E)
GASTRIC SURGERY
• Bariatric surgery may be considered for adoles-cents with obesity-related comorbidities, includingT2DM (90).
• Gastric bypass, the traditional surgical procedurefor weight loss, can have significant complicationsincluding nutrient malabsorption and even death.Newer techniques, which appear to be safer, includegastric banding and vagal nerve stimulators. ASwedish study of over 2000 subjects undergoinga variety of bariatric surgery procedures foundpersistence of weight loss after 10 years and reducedmortality compared to conventionally treated obesepatients (91).
• A randomized controlled trial of gastric band-ing versus conventional treatment for recentonset T2D in a small population of obese indi-viduals from Australia achieved a 73% remis-sion rate which correlated with weight loss andlower baseline HbA1c, without serious complica-tions (92).
• Although the morbidity and mortality rates inadults have decreased over the last 5 years, thistreatment is still uncommon in children andshould be undertaken only in centers with anestablished program designed to collect outcomedata (E).
26 Pediatric Diabetes 2009: 10 (Suppl. 12): 17–32
Type 2 diabetes
Testing (case finding) for T2DM
Justification for case finding in a population at risk (93):
• The condition tested for is sufficiently common tojustify the investment. A large screening programidentified only < 1% of high risk children with type 2diabetes (22). (B) Whether this is sufficiently frequentin adolescents to justify testing those with high-riskethnicity or family history is still unclear (E).
• The condition tested for is serious in terms of morbid-ity and mortality. Unquestionably true of T2DM inadolescents because of the association with increasedcardiovascular risk factors and renal dysfunction.
• The condition tested for has a prolonged latency periodwithout symptoms, during which abnormality can bedetected. Impaired glucose tolerance in youth hasbeen detected in asymptomatic adolescents, but albu-minuria and dyslipidemia may already be present,indicative of a period of dysmetabolism and poten-tially a long latency period for overt type 2 diabetes,as in adults.
• A test is available that is sensitive (few false negatives)and accurate with acceptable specificity (minimalnumber of false positives). The fasting plasma glu-cose and 2-hour plasma glucose have been appliedto high risk populations and are exceptionally sen-sitive and specific. Random opportunistic glucosemeasurements may be appropriate, and are likely tobe sensitive. The cost of this if the yield is low mustbe considered in any screening program.
• An intervention is available to prevent or delay diseaseonset or to more effectively treat the condition detectedin the latency phase.
In the face of an apparent rapid increase in type2 diabetes in US youth, The American DiabetesAssociation issued a Consensus Statement in 2000,recommending screening youth for type 2 diabetesbased broadly on known risk factors (2) (E). Concernshave been raised about these recommendationsas more information has accumulated since thispublication.
Concerns about these criteria are:
• they were established without a database and,therefore, not evidence-based
• although the fasting plasma glucose was consid-ered preferable because of lower-cost and greaterconvenience, sensitivity is compromised because the2-hour plasma glucose increases earlier in the courseof development of T2DM
• while some ethnicities may be overrepresented inpopulations of affected individuals, not being amember of such a group is not protective andtherefore may be a spurious basis for selection ofindividuals to be tested
Studies in the 7 years following publication of thesecriteria, from Europe, the US, Japan, Taiwan, India,and Israel, have provided a data base for refining case-finding recommendations (11,22, 23, 43–49, 94) (C)
• These studies emphasize the limitation of fastingglucose determination for testing purposes in obeseyoungsters.
• Studies of large numbers of school children inJapan and Taiwan, using urine tests for initialscreening indicate a very low yield (∼0.02%) ofdiabetes and an unjustifiable cost-benefit ratio inmost populations (11, 93).
• Some studies demonstrate a relatively low yield ofidentifying cases even in high risk populations usingan OGTT, 0.1% were found to have a 2 hour postglucose > 200 mg/dl (11 mmol/l) in a primarily non-white, predominantly overweight US population (22)and 0.4% had diabetes in a Native Americanpopulation (23). In these studies 2–3% had impairedglucose tolerance or impaired fasting glucose.
• Several studies, including all ethnicities have alsonoted the high frequency of detection of non-glycemic features of the insulin resistance syndromein children and youth with BMI greater than 85thpercentile (95).
These new data indicate that screening to identifydiabetes in asymptomatic youth has a low yield andfurther research is required to determine the optimalstrategy for testing, including the frequency of testing.(C/E) In populations with high incidence of T2DM,if resources are available, currently some cliniciansmay favor screening while awaiting more informationon optimal screening strategies. However, in manypopulations screening outside of a research setting isnot cost effective.
Because abnormal glucose tolerance may be presentin 2–3% of high risk groups and additional findings ofinsulin resistance may be also be present prior to overtdiabetes, a high index of suspicion should be maintainedand at risk children should be advised on approaches toprevent T2DM (see subsequently). Children at risk forT2DM diabetes and metabolic syndrome include (C/E):
• Children with BMI 85–95th percentile:• if there is an immediate family history of T2DM,
early cardiovascular disease, or• if there are signs of insulin resistance (acanthosis
nigricans, dyslipidemia, hypertension, PCOS)
Asian children regardless of BMI, if history ofabnormally low or high birth weight (89), or familyhistory of diabetes (90).
Children with BMI > 95th percentile, regardless offamily history or associated features.
Pediatric Diabetes 2009: 10 (Suppl. 12): 17–32 27
Rosenbloom et al
Prevention of T2DM
• Worldwide, obesity is increasing in all segmentsof the population. The epidemic of obesity andits complications accounts for a substantial andincreasing proportion of direct and indirect healthcare costs. Prevention of T2DM requires preventionof obesity in those who are not overweight andtreatment of obesity in those who have a BMI> 85th percentile (or even less in non-Europeanpopulations) (11, 95). (A)
• Primary prevention of T2DM is directed towardthe obesity pandemic and involves reversing eatingand entertainment trends in homes, schools, andcommunities that have resulted in excess caloricintake and marked decrease in energy expenditure bychildren and adults; optimizing the fetal environmentin pregnancy; and the promotion of breast-feeding.
• Studies have shown that relatively minimal weightloss can decrease rate of diabetes in at riskpopulations (96,97) (A,C)
• Intervention in adult populations reflects difficultyin altering lifestyle and dietary habits (98).
• The challenge is huge, of countering eating andentertainment trends that provide popular socialoutlets and are highly attractive, ubiquitous, andheavily promoted (E).
• The societal changes required are of such magni-tude that enormous community and governmentalcommitment is required (E).
Recommendations:
Autoantibody testing when diagnosing and treatingT2DM:
• Diabetes autoantibody testing should be consideredin all pediatric patients with the clinical diagnosisof T2DM because of the high frequency of islet cellautoimmunity in otherwise ‘‘typical’’ T2DM:
• Antibodies will indicate an earlier need forinsulin. (E)
• Antibodies will indicate the need to check forthyroid autoimmunity and to consider otherassociated autoimmune disorders. (E)
• Diabetes autoantibody testing should be consideredin overweight/obese children > 13 years of agewith a clinical picture of T1DM (weight loss,ketosis/ketoacidosis), some of whom may haveT2DM (E)
• C–peptide measurements should be considered inoverweight/obese children > 13 years of age whohave worsening levels of control on oral agentsto confirm those requiring insulin therapy and toreconsider the diabetes classification.(E)
• Because of the multitude of cardiovascular riskfactors associated with insulin resistance, T2DMis likely to be associated with earlier severecomplications than T1DM in childhood (E).
• The insidious onset in much of T2DM, the lipiddysmetabolism, and the unknown duration of IGTpreceding diagnosis may, as in adults, be associatedwith micro- and macrovascular disease alreadypresent at diagnosis (E).
Recommendation for initial medical treatment oftype 2 diabetes* (98):
* Preadolescent children are unlikely to have T2DM,even if obese (8)
* Overweight adolescents should have both T1DMand T2 DM considered in the diagnosis (4,8)
* Antibody determination is the only way todefinitively determine the presence of autoimmunediabetes (T1DM)
Initial treatment modality is determined by symptoms,severity of hyperglycemia, and presence or absence ofketosis/ketoacidosis. As in T1DM, those with symptoms,particularly vomiting, can deteriorate rapidly and needurgent assessment and appropriate treatment. (E).
Lifestyle changes in diet and exercise are essential andshould be recommended for all individuals with T2DM
Complication testing specific to T2DM in youngpeople:
• Testing for either micro- or macro-albuminuria,should be performed at the time of diagnosis andannually thereafter (55, 72) (E).
– Elevated levels of urine albumin should beconfirmed on 2 of 3 samples
• Blood pressure should be monitored at every visitaccording to standardized techniques specific forchildren ( (72), E) On-line instructions are availableat: www.nhlbi.nih.gov/health/prof/heart/hbp/hbp_ped.pdf
– Elevated BP should be confirmed on 2 additionaldays. Hypertension is defined as an averagesystolic or diastolic BP � 95 percentile for age,sex and height percentiles, with high normal BPbeing 90 to < 95percentile .
– Normal BP levels for age, sex, and height areavailable at the above website.
• Testing for dyslipidemia should be performed soonafter diagnosis when BG control has been achievedand annually thereafter (60,61) E
• Evaluation for NAFLD should be done at diagnosisand annually thereafter (24) (E).
• Inquiries about puberty, menstrual irregularities andobstructive sleep apnea should be made at diagnosisand regularly thereafter (65) (E).
28 Pediatric Diabetes 2009: 10 (Suppl. 12): 17–32
Type 2 diabetes
• Examination for retinopathy should be performed atdiagnosis and annually thereafter (E).
Recommendations for case finding:
• Case finding for research purposes should determineabnormal glucose tolerance, IFG and IGT in astandardized manner by blood glucose level obtainedfasting before an oral glucose load of 1.75g/kg bodyweight up to 75 g, and 2 hours following ingestion ofthe glucose (E).
• For longitudinal research purposes, frequency oftesting at risk individuals may be annually (E).
• The clinical diagnosis of T2DM in an asymptomaticindividual requires at least two abnormal glucosevalues, diagnostic of diabetes, on 2 separate days (E).
Recommendation for prevention:
• The societal, family, community, and personnelresources required to prevent, or delay, the develop-ment of T2DM and the other serious manifestationsof the insulin resistance syndrome are daunting andneed to be addresses (E).
References1. ROSENBLOOM AL, JOE JR, YOUNG RS, WINTER WE.
The emerging epidemic of type 2 diabetes mellitus inyouth. Diabetes Care 1999: 22: 345–54.
2. American Diabetes Association. Type 2 diabetes inchildren and adolescents: Consensus conference report.Diabetes Care 2000: 23: 381–389.
3. DUNCAN GE. Prevalence of diabetes and impairedfasting glucose levels among US adolescents: NationalHealth and Nutrition Examination Survey, 1999–2002.Arch Pediatr Adolesc Med 2006: 160: 523–528.
4. PINHAS-HAMIEL O, ZEITLER P. The global spread oftype 2 diabetes mellitus in children and adolescents. JPediatr 2005: 146: 693–700.
5. DRAKE AJ, SMITH A, BETTS PR, CROWNE EC,SHIELD JP. Type 2 diabetes in obese white children.Arch Dis Child 2002: 86: 207–208.
6. KITAGAWA T, OWADA M, URAKAMI T, YAMAUCHI K.Increased incidence of non-insulin dependent diabetesmellitus among Japanese schoolchildren correlates withan increased intake of animal protein and fat. Clin Pediatr1998: 37: 111–115.
7. EHTISHAM S, HATTERSLEY AT, DUNGER DB, BAR-RETT TG. First UK survey of paediatric type 2 diabetesand MODY. Arch Dis Child 2004: 89: 526–529.
8. The Writing Group for the SEARCH for Diabetes inYouth Study Group. Incidence of diabetes in youth inthe United States. JAMA 2007: 297: 2716–2724.
9. KADIKI OA, REDDY MR, MARZOUK AA. Incidence ofinsulin-dependent diabetes (IDDM) and non-insulin-dependent diabetes (NLDDM) (0-34 years at onset) inBenghazi, Libya. Diabetes Res Clin Pract 1996: 32:165–173.
10. CHAN JC, CHEUNG CK, SWAMINATHAN R,NICHOLLS MG, COCKRAM CS. Obesity albumin-uria, and hypertension among Hong Kong Chinese
with non-insulin dependent diabetes mellitus (NIDDM).Postgrad Med J 1993: 69: 204–210.
11. WEI JN, SUNG FC, LI CY, CHANG CH, LIN RS,LIN CC, CHIANG CC, CHUANG LM. Low birth weightand high birth weight infants are both at an increased riskto have type 2 diabetes among schoolchildren in Taiwan.Diabetes Care 2003: 26: 343–348.
12. RAMACHANDRAN A, SNEHALATHA C, SATYAVANI K,SIVASANKARI S, VIJAY V. Type 2 diabetes in Asian-Indian urban children. Diabetes Care 2003: 26:1022–1023.
13. SAYEED MA, HUNSAIN MZ, BANU A, RURNI MAK,AZAD KHAN AK. Prevalence of diabetes in a suburbanpopulation of Bangladesh. Diabetes Res CIin Pract 1997:34: 149–155.
14. BRAUN B, ZIMMERMAN MB, KRETCHMER N,SPARGO RM, SMITH RM, GRACEY M. Risk fac-tors for diabetes and cardiovascular disease in youngAustralian aborigines: a 5-year follow-up study. DiabetesCare 1996: 19: 472–479.
15. MCGRATH NM, PARKER GN, DAWSON P. Early pre-sentation of type 2 diabetes mellitus in young NewZealand Maori. Diabetes Res Clin Pract 1999: 43:205–209.
16. EPPENS MC, CRAIG ME, JONES TW, SILINK M, ONG S,PING YJ on behalf of the International DiabetesFederation Western Pacific Region Steering Committee.Type 2 diabetes in youth from the Western Pacific region:glycemic control, diabetes care and complications. CurrMed Res Opinion 2006: 22: 1013–1020.
17. SUGIHARA S, SASAKI N, KOHNO H, AMEMIYA S,TANAKA T, MATSURA N. The Committee for MedicalTreatment of Childhood-onset Type 2 Diabetes melli-tus, The Japanese Society for Pediatric Endocrinology.Survey of current medical treatments for childhood-onset Type 2 daibetes mellitus in Japan. Clin PediatrEndocrinol 2005: 14(2): 65–75.
18. WEISS R, DUFOUR S, TAKSALI SE, TAMBORLANE WV,PETERSEN KF, BONADONNA RC, BOSELLI L, BAR-BETTA G, ALLEN K, RIFE F, SAVOYE M, DZIURA J,SHERWIN R, SHULMAN GI, CAPRIO S. Prediabetes inobese youth: a syndrome of impaired glucose tolerance,severe insulin resistance, and altered myocellular andabdominal fat partitioning. Lancet 2003: 362: 951–957.
19. DRUET C, TUBIANA-RUFI N, CHEVENNE D, RIGAL O,POLAK M, LEVY-MARCHAL C. Characterization ofinsulin secretion and resistance in type 2 diabetes ofadolescents. J. Clin Endocrinol Metab 2006: 91: 401–404.
20. MILLER J, SILVERSTEIN JH, ROSENBLOOM AL. Type 2diabetes in the child and adolescent. In: LIFSHITZ F (ed)Pediatric Endocrinology: fifth edition, volume 1. NewYork: Marcel Dekker 2007: pp 169–188.
21. UKPDS Group: Intensive blood glucose control withsulphonylureas or insulin compared with conventionaltreatment and risk of complications in patients with type2 diabetes (UKPDS 33) Lancet 1998: 352: 837–853.
22. MORALES A, ROSENBLOOM AL. Death caused by hyper-glycemic hyperosmolar state at the onset of type 2diabetes. J Pediar 2004: 144: 270–273.
23. PINHAS-HAMIEL O, ZEITLER P. Acute and chroniccomplications of type 2 diabetes mellitus in childrenand adolescents. Lancet 2007: 369: 1823–1831.
Pediatric Diabetes 2009: 10 (Suppl. 12): 17–32 29
Rosenbloom et al
24. ROSENBLOOM AL. Obesity, insulin resistance, beta cellautoimmunity, and the changing clinical epidemiology ofchildhood diabetes. Diabetes Care 2003: 26: 2954–2956.
25. TURNER R, STRATTON I, HORTON V, MANLEY S, ZIM-MET P, MACKAY IR, SHATTOCK M, BOTTAZZO GF,HOLMAN R, for the UK Prospective Diabetes Study(UKPDS) Group. UKPDS 25: Autoantibodies to isletcell cytoplasm and glutamic acid decarboxylase for pre-diction of insulin requirement in type 2 diabetes. Lancet1997: 350: 1288–93.
26. HATHOUT EH, THOMAS W, EL-SHAHAWY et al. Dia-betic autoimmune markers in children and adolescentswith type 2 diabetes. Pediatrics 2001: 107: e102 .
27. UMPAICHITRA V, BANERJI MA, CASTELLS S. Autoanti-bodies in children with type 2 diabetes mellitus. J PediatrEndocrinol Metab 2002: 15: 525–30 .
28. REINHARD T, SCHOBER E, WIEGAND S, THON A,HOLL R; on behalf of the DPV-Weiss Study Group.β-cell autoantibodies in children with type 2 diabetesmellitus: subgroup or misclassification? Arch Dis Child2006: 91: 473–4 77.
29. LANDIN-OLSSON M. Latent autoimmune diabetes inadults. Ann N Y Acad Science 2002: 958: 112–116.
30. WINTER WE, MACLAREN NK, RILEY WJ,CLARKE DW, KAPPY MS, SPILLAR RP. Maturityonset diabetes of youth in black Americans. N Engl JMed 1987: 316: 285–291.
31. BANERJI MA. Diabetes in African Americans: uniquepathophysiologic features. Curr Diab Rep 2004: 4:219–23.
32. HATTERSLEY A, BRUINING J, SHIELD J, NJOLSTAD P,DONAGHUE K. ISPAD Clinical Practice ConsensusGuidelines 2006–2007. The diagnosis and managementof monogenic diabetes in children. Pediatric Diabetes2006: 7: 352–360.
33. GOTTLIEB MS. Diabetes in offspring and siblings ofjuvenile- and maturity-onset-type diabetics. J ChronicDis 1980: 33: 331–339.
34. DAHLQUIST G, BLOM L, TUVEMO T, NYSTROM L,SANDSTROM A, WALL S. The Swedish childhood dia-betes study–results from a nine year case register anda one year case-referent study indicating that type 1(insulin-dependent) diabetes mellitus is associated withboth type 2 (non-insulin-dependent) diabetes mellitusand autoimmune disorders. Diabetologia 1989: 32: 2–6.
35. BANERJEE S, RAGHAVAN S, WASSERMAN EJ, LIN-DER BL, SAENGER P, DIMARTINO-NARDI J. Hormonalfindings in African American and Caribbean Hispanicgirls with premature adrenarche: implications for poly-cystic ovarian syndrome. Pediatrics 1998: 102: E35.
36. IBANEZ L, POTAU N, MARCOS MV, DEZEGHER
F. Exaggerated adrenarche and hyperinsulinism inadolescent girls born small for gestational age. J ClinEndocrinol Metab 1999: 84: 4739–4741.
37. PLOURDE G. Impact of obesity on glucose and lipidprofiles in adolescents at different age groups in relationto adulthood. BMC Family Practice 2002: 3: 18,[http://www.biomedcentral.com/1471-2296/3/18].
38. INVITTI C, GUZZALONI G, GILARDINI L, MORBITO F,VIBERTI G. Prevalence and concomitants of glucoseintolerance in European obese children and adolescents.Diabetes Care 2003: 26(118-1): 24.
39. TRESACO B, BUENO G, MORENO A, GARAGORRI JM,BUENO M. Insulin resistance and impaired glucose
tolerance in obese children and adolescents. J PhysiolBiochem 2003: 59: 217–224.
40. MISRA A, VIKRAM NK, ARYA S, PANDEY RM,DHINGA V, CHATTERJEE A, DWIVEDI M, SHARMA R,LUTHRA K, GULERIA R, TALWAR KK. High preva-lence of insulin resistance in postpubertal Asian Indianchildren is associated with adverse truncal body fat pat-terning, abdominal adiposity and excess body fat. Int JObesity 2004: 28: 1217–1226.
41. WABITSCH M, HAUNER H, HERTRAMPF M, MUCHE R,HAY B, MATER H, KRATZER W, DEBATIN K-M,HEINZE E. Type II diabetes mellitus and impaired glu-cose regulation in Caucasian children and adolescentswith obesity living in Germany. Int J Obesity 2004: 28:307–313.
42. WIEGAND S, MAIKOWSKI U, BLANKENSTEIN O,BIEBERMANN, TARNOW P, GR ¤UTERS A. Type 2 diabetesand impaired glucose tolerance in European childrenand adolescents with obesity-a problem that is no longerrestricted to minority groups. Eur J Endocrinol 2004:151: 199–206.
43. SHALITIN S, ABRAHAMI M, LILOS P, PHILLIP M. Insulinresistance and impaired glucose tolerance in obesechildren and adolescents referred to a tertiary care centerin Israel. Int J Obesity 2005: 29: 571–578.
44. The STOPP-T2D Prevention Study Group. Presence ofdiabetes risk factors in a large US eighth-grade cohort.Diabetes Care 2006: 29: 212–217.
45. GORAN MI, BERGMAN RN, AVILA Q, WATKINS M,BALL GDC, SHAIBI GQ, WEIGENSBERG MJ,CRUZ ML. Impaired glucose tolerance and reducedβ-cell function in overweight Latino children witha positive family history for type 2 diabetes. J ClinEndocrinol Metab 2004: 89(200): 7–212.
46. LEE S, BACHA F, GUNGOR N, ARSLANIAN SA. Waistcircumference is an independent predictor of insulinresistance in black and white youths. J Pediatr 2006:148: 188–194.
47. FREEDMAN DS, KHAN LK, DIETZ WH, SRINI-VASAN SR, BERENSON GS. Relationship of childhoodobesity to coronary heart disease risk factors in adult-hood: the Bogalusa heart study. Pediatrics 2001: 108:712–718.
48. BERENSON GS, SRNIVASAN SR. Cardiovascular riskfactors in youth with implications for aging: the BogalusaHeart Study. Neurobiol Aging 2005: 26: 303–307.
49. JUONALA M, JARVISALO MJ, MAKI-TORKKO N,KAHONEN M, VIIKARI JS, RAITAKARI OT. Risk factorsidentified in childhood and decreased carotid arteryelasticity in adulthood: the Cardiovascular Risk inYoung Finns Study. Circulation 2005: 112: 1486–1493.
50. VISSER M, BOUTER LM, MCQUILLAN GM,WENER MH, HARRIS TB. Low-grade systemicinflammation in overweight children. Pediatrics2001: 107: e13.
51. ADELMAN RD, RESTAINO IG, ALON US, BLOWEY DL.Proteinuria and focal segmental glomerulosclerosis inseverely obese adolescents. J Pediatr 2001: 138: 481–485.
52. GRESS TW, NIETO FJ, SHAHAR E, WOFFORD MR,BRANCATI FL. Hypertension and antihypertensive ther-apy as risk factors for type 2 diabetes mellitus.Atherosclerosis Risk in Community Study. N Engl JMed 2000: 342: 905–912.
30 Pediatric Diabetes 2009: 10 (Suppl. 12): 17–32
Type 2 diabetes
53. SALOMAA VV, STRANDBERG TE, VANHANEN H,NAUKKARINEN V, SARNA S, MIETTINEN TA. Glucosetolerance and blood pressure: long-term follow-up inmiddle-age men. BMJ 1991: 302: 493–496.
54. WIERZBICKI AS, NIMMO L, FEHER MD, COX A, FOX-TON J, LANT AF. Association of angiotensin-convertingenzyme DD genotype with hypertension in diabetes. JHum Hypertens 1995: 9: 671–673.
55. KIRPICHNIKOV D, SOWERS JR. Diabetes mellitus anddiabetes-associated vascular disease. Trends EndocrinolMetab 2001: 12: 225–230.
56. LAAKSO M. Lipids in type 2 diabetes. Semin Vasc Med2002: 2: 59–66.
57. GOLDBERG IJ. Diabetic dyslipidemia: causes and conse-quences. J Clin Endocrinol Metab 2001: 86: 965–971.
58. LEWY VD, DANADIAN K, WITCHEL SF, ARSLANIAN S.Early metabolic abnormalities in adolescent girls withpolycystic ovarian syndrome. J Pediatr 2001: 138: 38–44.
59. NORMAN RJ, DEWAILLY D, LEGRO RS, HICKEY TE.Polycystic ovary syndrome. Lancet 2007: 370(9588):685–697.
60. STRAUSS RS, BARLOW SE, DIETZ WH. Prevalence ofabnormal serum aminotransferase values in overweightand obese adolescents. J Pediatr 2000: 136: 727–733.
61. SMITH JC, FIELD C, BRADEN DS, GAYMES CH, KAST-NER J. Coexisting health problems in obese children andadolescents that might require special treatment consid-erations. Clin Pediatr 1999: 38: 305–307.
62. DIETZ WH, GROSS WL, KIRKPATRICK JA. Blount dis-ease (tibia vara): another skeletal disorder associatedwith childhood obesity. Pediatr 1982: 101: 735–737. .
63. LODER RT, ARONSON DD, GREENFIELD ML. The epi-demiology of bilateral slipped capital femoral epiphysis.A study of children in Michigan. J Bone Joint Surg 1993:75: 1141–1147 .
64. POREDOS P. Endothelial dysfunction and cardiovasculardisease. Pathophysiol Haemost Thromb 2002: 32: 274–7.
65. TOUNIAN P, AGGOUN Y, DUBERN B, VARILLE V, GUY-GRAND B, SIDI D, GIRARDET JP, BONNET D. Presenceof increased stiffness of the common carotid artery andendothelial dysfunction in severely obese children: aprospective study. Lancet 2001: 358: 1400–1404.
66. EPPENS MC, CRAIG ME, CUSUMANO J, HING S,CHAN AK, HOWARD NJ, SILINK M, DONAGHUE KC.Prevalence of diabetes complications in adolescents withtype 2 compared with type 1 diabetes. Diabetes Care2006: 29(6): 1300–1306.
67. KERSHNAR AK, DANIELS SR, IMPERATORE G,PALLA SL, PETITTI DB, PETTITT DJ, MARCOVINA S,DOLAN LM, HAMMAN RF, LIESE AD, PIHOKER C,RODRIGUEZ BL. Lipid abnormalities are prevalent inyouth with type 1 and type 2 diabetes: the SEARCH forDiabetes in Youth Study. J Pediatr 2006: 149: 314–319.
68. DONAGHUE KC, CHIARELLI F, TROTTA D, ALL-GROVE J, DOHL-JORGENSEN K. ISPAD Clinical PracticeConsensus Guidelines 2006–2007. Microvascular andmacrovascular complications. Pediatr Diabetes 2007: 8:163–170.
69. STRIPPOLI GF, CRAIG M, DEEKS JJ, SCHENA FP,CRAIG JC. Effects of angiotensin converting enzymeinhibitors and angiotensin II receptor antagonists onmortality and renal outcomes in diabetic nephropathy:systematic review. BMJ 2004: 329(7470): 828.
70. COOPER WO, HERNANDEZ-DIAZ S, ARBOGAST PG,DUDLEY JA, DYER S, GIDEON PS, HALL K, RAY WA.Major congenital malformations after first-trimesterexposure to ACE inhibitors. N.Engl.J.Med 2006: 354:2443–2451.
71. GRAHAM DJ, STAFFA JA, SHATIN D, ANDRADE SE,SCHECH SD, LA GRENADE L, GURWITZ JH, CHAN KA,GOODMAN MJ, PLATT R. Incidence of hospitalizedrhabdomyolysis in patients treated with lipid-loweringdrugs. JAMA 2004: 292: 2585–2590.
72. SWIFT PG. Diabetes education. ISPAD Clinical PracticeConsensus Guidelines 2006–2007. Pediatr Diabetes 2007:8: 103–109.
73. DELAMATER AM. Psychological care of children andadolescents with diabetes. ISPAD Clinical PracticeConsensus Guidelines 2006–2007. Pediatric Diabetes2007: 8: 340–348.
74. WALDRON S, HANAS R, PALMVIG B. How do we edu-cate young people to balance carbohydrate intake withadjustments of insulin? Horm Res 2002: 57(Suppl. 1:):62–65.
75. JOE JR. Perceptions of diabetes by Indian adolescents.In: JOE JR, YOUNG RS, eds. Diabetes as a Disease ofCivilization: the Impact of Culture Change on IndigenousPeoples. Mouton de Gruyter: Berlin, 1994: pp. 329–356.
76. LEVINE MD, RINGHAM RM, KALARCHIAN MA, WIS-NIEWSKI L, MARCUS MD. Is family based behavioralweight control appropriate for severe pediatric obesity?Int J Eat Disord 2001: 30: 318–328.
77. Ellen Aslander-van Vliet, Carmel Smart and SheridanWaldron. Nutritional management in childhood andadolescent diabetes. ISPAD Clinical Practice ConsensusGuidelines 2006–2007. Pediatric Diabetes 2007: 8:323–339.
78. ROBINSON TM. Reducing children’s television viewing toprevent obesity. A randomized controlled trial. JAMA1999: 82: 1561–1567.
79. BRETZEL RG, NUBER U, LANDGRAF W, OWENS DR,BRADLEY C, LINN T. Once-daily basal insulin glargineversus thrice-daily prandial insulin lispro in peoplewith type 2 diabetes on oral hypoglycaemic agents(APOLLO): an open randomised controlled trial. Lancet2008: 371: 1073–1084.
80. LINCOFF AM, WOLSKI K, NICHOLLS SJ, NISSEN SE.Pioglitazone and risk of cardiovascular events in patientswith type 2 diabetes mellitus. A meta-analysis ofrandomized trials. JAMA 2007: 298: 1180–1188.
81. SINGH S, LOKE YK, FURBERG CD. Long-term riskof cardiovascular events with rosiglitazone: A Meta-analysis. JAMA 2007: 298: 1189–1195.
82. CHIASSON J, JOSSE R, HUNT J, PALMASON C,RODGER NW, ROSS SA, RYAN EA, TAN MH,WOLEVER TM. The efficacy of acarbose in thetreatment of patients with non-insulin-dependentdiabetes mellitus. A multicenter controlled clinical trial.Ann Int Med 1994: 121: 928–935.
83. RYAN GJ, JOBE LJ, MARTIN R. Pramlintide in thetreatment of type 1 and type 2 diabetes mellitus. ClinTher 2005: 27: 1500–1512.
84. RODRIGUEZ LM, MASON KJ, HAYMOND MW, HEP-TULLA RA. The role of prandial pramlintide in thetreatment of adolescents with type 1 diabetes. PediatrRes 2007: 62: 746–749.
Pediatric Diabetes 2009: 10 (Suppl. 12): 17–32 31
Rosenbloom et al
85. RIDDLE MC, DRUCKER DJ. Emerging therapies mim-icking the effects of amylin and glucagon-like peptide 1.Diabetes Care 2006: 29: 435–449.
86. INGE TH, ZELLER M, GARCIA VF, DANIELS SR. Surgi-cal approach to adolescent obesity. Adolesc Med Clin2004: 15: 429–453.
87. SJOSTROM L, NARBRO K, SJOSTROM D et al. Effects ofbariatric surgery on mortality in Swedish obese subjects.N Engl J Med 2007: 357: 741–752.
88. DIXON JB, O’BRIEN PE, PLAYFAIR J, CHAPMAN L,SCHACHTER LM, SKINNER S, PROIETTO J, BAILEY M,ANDERSON M. Adjustable gastric banding and conven-tional therapy for type 2 diabetes. JAMA 2008: 299:316–323.
89. SACKETT DL, HOLLAND WW. Controversy in detectionof disease. Lancet 1965: ii: 357–359.
90. URAKAMI T, MORIMOTO S, NITADORI Y et al. Urineglucose screening program at schools in Japan to detectchildren with diabetes and its outcome-Incidence andclinical characteristics of childhood type 2 diabetes inJapan. Pediatr Res 2007: 61: 141–145.
91. COOK S, WEITZMAN M, AUINGER P, NGUYEN M,DIETZ WH. Prevalence of a metabolic syndromephenotype in adolescents: findings from the thirdNational Health and Nutrition Examination Survey,1988–1994. Arch Pediatr Adolesc Med 2003: 157:821–827.
92. WEI JN, SUNG FC, LI CY et al. Low birth weight andhigh birth weight infants are both at an increased risk tohave type 2 diabetes among schoolchildren in Taiwan.Diabetes Care 2003: 26: 343–348.
93. KNOWLER WC, BARRETT-CONNOR E, FOWLER SE,HAMMAN RF, LACHIN JM, WALKER EA,NATHAN DM. Diabetes Prevention Program ResearchGroup. Reduction in the incidence of type 2 diabeteswith lifestyle intervention or metformin. N Engl J Med2002: 346(6): 393–403.
94. URAKAMI T, OWADA M, KITAGAWA T. Recent trendtoward decrease in the incidence of childhood type 2diabetes in Tokyo, Diabetes Care 2006: 29: 2176–2177.
95. JEFFREY RW. Community programs for obesity preven-tion: The Minnesota Heart Health Program. Obesity Res1995: 3(Suppl. 2): 283S–288S.
96. CRAIG M, HATTERSLEY A, DONAGHUE K. Definition,epidemiology, diagnosis and classification. ISPADClinical Practice Consensus Guidelines 2006–2007.Pediatric Diabetes 2006: 7: 343–51.
97. American Diabetes Association. Diagnosis and Classi-fication of Diabetes Mellitus. Diabetes Care 2008: 31:S55–S60.
98. World Health Organization. Definition, Diagnosis andClassification of Diabetes Mellitus and its Complications.Part 1: Diagnosis and Classification of Diabetes Mellitus.1999: Geneva: WHO/NCD/NCS/99.2.
32 Pediatric Diabetes 2009: 10 (Suppl. 12): 17–32





























