Embed Size (px)
Citation preview

Is There Space for Immunotherapy
in Non-Small Cell Lung Cancer?
Jean-Charles Soria, MD, PhD Gustave Roussy
Villejuif, France
U981

Lung Cancer: Most Common Malignancy and Leading Cause of Cancer-Related Mortality
1. Ferlay J, et al. GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11[Internet]. Lyon, France: International Agency for Research on Cancer; 2013. Available from: http://globocan.iarc.fr. Accessed September 2014; 2. Ferlay J, et al. Eur J Cancer. 2013;49(6):1374-1403.
0
500000
1000000
1500000
2000000
LungCancer
BreastCancer
ColorectalCancer
ProstateCancer
Incidence
Mortality
GLOBOCAN 2012 (worldwide, both sexes)1
1.59 million1
(1 in 5) estimated deaths worldwide
1.82 million1
estimated new cases worldwide
More people die from lung cancer than breast, colorectal and prostate
cancers combined1
Within Europe, ~1000 people die from lung cancer every day1,2

Classification Characteristics1
No
nsq
uam
ou
sc
Adenocarcinoma
(AC) 30% to 50%a
• Malignant epithelial tumors with glandular differentiation
• IASLC classification of invasive AC2:
• Lepidic, acinar, papillary, micropapillary, or solid pattern predominant
• Variants: Invasive mucinous AC, colloid, fetal, and enteric
Large cell
carcinoma 10%a
• Involves large cells (subtypes are giant cell, clear cell) with large nuclei
• No evidence of squamous or glandular differentiation
Sq
uam
ou
s
Squamous cell
carcinoma 30%b
• Involves cells of the squamous epithelium
• Two variants of clinicopathologic significance3
• Papillary variant
• Basaloid variant
Histologic Classification of NSCLC
aImage from www.surgical-pathology.com; bImage from www.lmp.ualberta.ca/resources/pathoimages/PC-S.htm; cOther less common subtypes of nonsquamous NSCLC include adenosquamous carcinoma and sarcomatoid carcinoma.3
IASCL, International Association for the Study of Lung Cancer; NSCLC, non-small cell lung cancer
1. Langer CJ, et al. J Clin Oncol. 2010;28(36):5311-5320. 2. Travis WD, et al. J Thorac Oncol 2011;4:244-285. 3. Travis WD, et al, eds. World Health Organization Classification of Tumours. Pathology and Genetics of Tumours of the Lung, Pleura, Thymus and Heart. IARC Press: Lyon; 2004.

Metastatic NSCLC Today
NSCLC
Platinum
Doublet
Cisplatin
+
Pemetrexed
Doublet
+
Bevacizumab
SQUAMOUS ADENOCARCINOMA LARGE
CELL
EGFR mutated:
Gefitinib, Erlotinib,
Afatinib
ALK
translocated:
Crizotinib
Ceridinib
80%
No Clear Driver
or Oncogenic Event
20%
NSCLC
Oncogene
Addicted
24-36
Months
12
Months
ALK, anaplastic lymphoma kinase;
EGFR, epidermal growth factor receptor

First-line combination with chemotherapy
After failure of 1 prior chemotherapy
Maintenance treatment after First-line chemotherapy
First-line or unspecified setting single agent
1970 1980 1990 2000
Erlotinib 2004
Docetaxel 1999
Gefitinibb 2003
2010
Pemetrexedc 2004
Erlotinib 2010
Pemetrexedc 2009
Crizotinibd 2011 (US)/2012 (EU)
Erlotinibe 2013 Median Overall Survival (OS), months
12+
~8-10 ~6
~2-4
24-36
Carboplatina 1989
Gemcitabine 1996
Vinorelbine 1994
Docetaxel 2002
Bevacizumabc
2006
Pemetrexedc
2008
Paclitaxel 1998
nab-Paclitaxel
2012
Cisplatina 1978
Therapeutic Overview in NSCLC
aNot approved in NSCLC, but commonly used; bRestricted to patients participating in a clinical trial or continuing to benefit from treatment already initiated; cNonsquamous NSCLC only; dALK-positive NSCLC only; eEGFR exon 19 deletions or exon 21 (L858R) substitution mutations only; fAfatinib is approved for the treatment of patients with activating EGFR mutations but only progression-free survival (PFS) data have been published (May 2014).
US Food and Drug Administration. Available at: www.fda.gov. Accessed September 1, 2014. European Medicines Agency. Available at: www.ema.europa.eu. Accessed September 1, 2014. National Comprehensive Cancer Network. NCCN Guidelines®: Non-small cell lung cancer. v6.2015. Available at: https://www.nccn.org/store/login/login.aspx?ReturnURL=http://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf. Accessed May 14, 2015.
Afatinibe,f
2013 Year

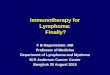
Immunotherapy Strategies for NSCLC
. mAb, monoclonal antibody; PD, programmed death; PD-L, PD-ligand
National Institutes of Health. www.clinicaltrials.gov. Accessed September 1, 2014. National Comprehensive Cancer Network. NCCN Guidelines®: Non-small cell lung cancer. v6.2015. Available at: https://www.nccn.org/store/login/login.aspx?ReturnURL=http://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf. Peters S, et al. Ann Oncol. 2012;23 Suppl 7:vii56-vii64.
Therapeutic vaccines
Enhancing immune
cell function
Adoptive Antitumor
mAbs
Bavituximab EGFR inhibition
Adoptive cell transfer
Modulate T-cell function
Cytokines
GSK1572932A TG4010
Belagenpumatucel-L Tergenpumatucel-L
Racotumomab L-BLP25 CIMAvax
Passive (adoptive) Designed to act at tumor;
immune-based mechanism
Active Designed to act on the immune system itself
Immunotherapy
Antigen dependent
Antigen independent
Immunecheckpoint
CTLA-4 inhibition PD-1 inhibition
PD-L1 inhibition

Immunotherapy Strategies for NSCLC
. mAb, monoclonal antibody; PD, programmed death; PD-L, PD-ligand
National Institutes of Health. www.clinicaltrials.gov. Accessed September 1, 2014. National Comprehensive Cancer Network. NCCN Guidelines®: Non-small cell lung cancer. v6.2015. Available at: https://www.nccn.org/store/login/login.aspx?ReturnURL=http://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf. Peters S, et al. Ann Oncol. 2012;23 Suppl 7:vii56-vii64.
Therapeutic vaccines
Enhancing immune
cell function
Adoptive Antitumor
mAbs
Bavituximab EGFR inhibition
Adoptive cell transfer
Modulate T-cell function
Cytokines
GSK1572932A TG4010
Belagenpumatucel-L Tergenpumatucel-L
Racotumomab L-BLP25 CIMAvax
Passive (adoptive) Designed to act at tumor;
immune-based mechanism
Active Designed to act on the immune system itself
Immunotherapy
Antigen dependent
Antigen independent
Immunecheckpoint
CTLA-4 inhibition PD-1 inhibition
PD-L1 inhibition


Immune Checkpoint Inhibitors

Why Is Immunotherapy Intrinsically Unique?

Paradigm Shift in Cancer Therapy
Tumor Cell
Historic Paradigm:
Targeting Tumor Cells
Lymphocyte
New Paradigm:
Targeting Immune Cells
Courtesy A Marabelle

Specificities of ICB
Potential to Improve Clinical
Outcome
Targeting the immune system, not the tumor, offers the potential for activity across multiple
tumor types
Unique MoA of I-O therapies offers the
opportunity for combination
Immune adaptability, and memory offers
the potential for long-term survival
ICB, immune checkpoint blockade; I-O, immuno-oncology; MoA, mechanism of action

Big Hope—True for Lung Cancer?

[TITLE]
Sharpe A. Presented at: 2013 American Society of Clinical Oncology Annual Meeting; May 31 - June 3, 2013: Chicago, Illinois.
What Is an Immune Checkpoint?
But the concept is not limited to T cells (NK cells, macrophages)
-

Antibody Target Company Stage in Development
Ipilimumab CTLA-4 Bristol-Myers Squibb Phase III
Tremelimumab CTLA-4 MedImmune/Astra
Zeneca Phase II
BMS-936558
Nivolumab PD-1 Bristol-Myers Squibb Phase III/Approved USA
MK-3575
pembrozilumab PD-1 Merck Phase III
MPDL-3280A
Atezolizumab PD-L1 Genentech-Roche Phase III
Medi-4736
Durvalumab PD-L1
MedImmune/Astra
Zeneca Phase III
MSB0010718C
Avelumab PD-L1 Merck/Pfizer Phase II
BMS-936559 PD-L1 Bristol-Myers Squibb Phase I
AMP-224
Fc fusion
of PD-L2 GSK Phase I
Immune Checkpoint Inhibitors in NSCLC

Neo
adjuvant
Adjuvant
Metastatic
Preventive?
Defining the Optimal Timing for Checkpoint Blockade During Disease Evolution?
Surgery
Locally
advanced

The earlier stage a drug can be used, the greater is the potential benefit
Late-stage disease
Benefit = a few months
Earlier stages of cancer
Benefit = many months
Adjuvant therapy
Benefit = months, years,
potential for cure (long-term remission)

Metastatic
Second-line and beyond
First-line monotherapy
In combination
Defining the Optimal Timing for Checkpoint Blockade During Disease Evolution?

Immune Checkpoint Blockade
TKI
Chemo
Radiation Therapy Vaccines
Other Immune
Checkpoint Blockade

Rationale for Combination Survival
! me
controls
immune/checkpoint/blockade
Survival
! me
controls
conven5onal/therapies
Survival
! me
controls
combina5ons/conven5onal/therapies/
+/immune/checkpoint/blockade
Conventional
therapies
Controls
Survival
! me
controls
immune/checkpoint/blockade
Survival
! me
controls
conven5onal/therapies
Survival
! me
controls
combina5ons/conven5onal/therapies/
+/immune/checkpoint/blockade
Immune checkpoints
blockade
Controls
Ribas A, et al. Clin Cancer Res. 2012;18(2):336-341. Champiat S, et al.J Thorac Oncol. 2014;9(2):144-153.
Time Time

Conventional
therapies
Immune checkpoints
blockade
Controls
Ribas A, et al. Clin Cancer Res. 2012;18(2):336-341. Champiat S, et al.J Thorac Oncol. 2014;9(2):144-153.

Reported Immunomodulatory Effects of Conventional Agents
Immunogenic
cell death
CT, RT
Vaccines L-BLP25, MAGE-A3, EGF,
belagenpumatucel-L
tergenpumatucel-L
TG4010
Up-regulation
of MHCI paclitaxel,
gemcitabine,
erlotinib
DC maturation paclitaxel, docetaxel,
bevacizumab
Up-regulation
of PD-L1 paclitaxel,
etoposide
T-Reg
inhibition cisplatin,
paclitaxel,
bevacizumab
Down-regulation
of PD-L1 Pi3K? MEKi?
crizotininb
Champiat S, et al.J Thorac Oncol. 2014;9(2):144-153.

20%
NSCLC
Oncogene
Addicted
NCSLC
80%
No clear driver
or oncogenic event
platinum
doublet
cisplatin +
pemetrexed
doublet +
bevacizumab
SQUAMOUS ADENOCARCINOMAS LARGE
CELL

20%
NSCLC
Oncogene
Addicted
NCSLC
80%
No clear driver
or oncogenic event
platinum
doublet
cisplatin +
pemetrexed
doublet +
bevacizumab
SQUAMOUS ADENOCARCINOMAS LARGE
CELL
EGFR mutated
gefitinib,
erlotinib
afatinib
ALK, ROS
translocated
crizotinib
IMMUNOTHERAPY ?