Embed Size (px)
Citation preview
Is the Optic Disc Cupping or Sinking in Glaucoma?
Syed S. Hasnain M.D.

Introduction
My presentation ‘Is the Optic Disc Cupping or Sinking in Glaucoma’ is based on my personal affliction of the disease. During my residency about 40 years ago I was found to have high intraocular pressure of 30mmHg in each eye. I did not receive any treatment. My IOP is still the same, yet I see 20/20, have no field defect and have healthy discs. This was puzzling: why didn’t I develop glaucoma at 30mmHg while others at 15mmHg. To find the answer, I focused on selective destruction of arcuate fibers: How and why are they selectively destroyed in both HTG and NTG? My findings suggest that the circular border tissue may be the common site of injury in both types. On this basis I think that the optic disc may not be ‘cupping’ but instead sinking in its entirety.
What is intraocular pressure?
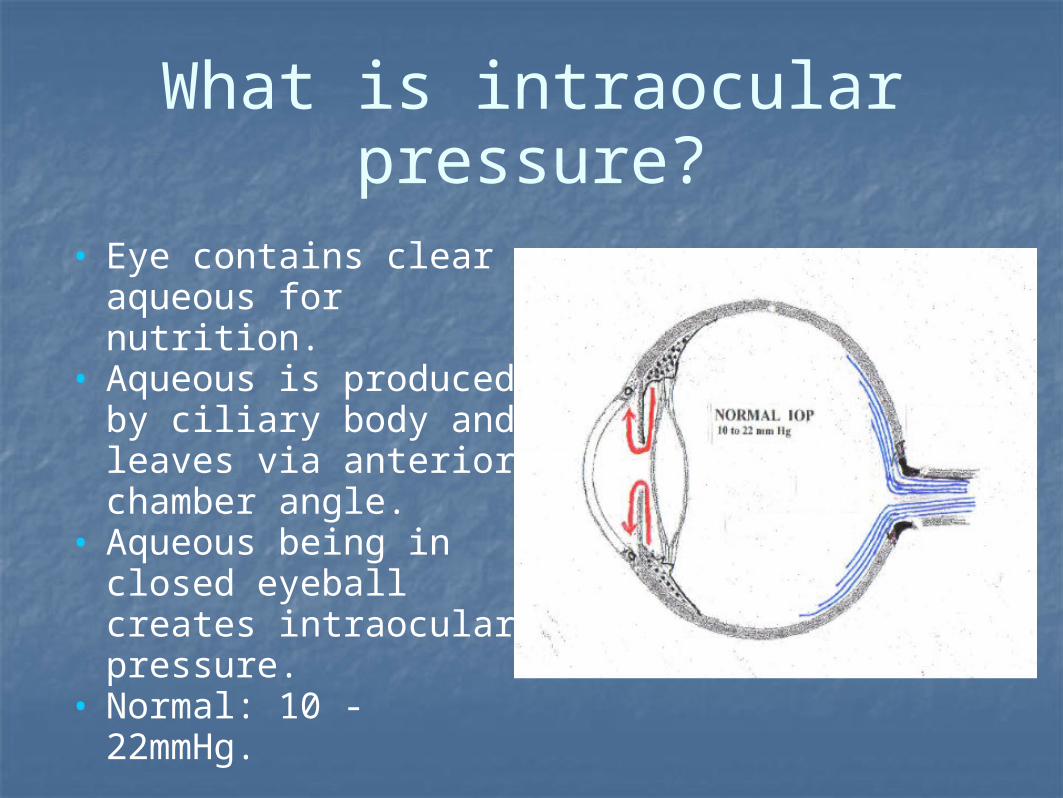
• Eye contains clear aqueous for nutrition.
• Aqueous is produced by ciliary body and leaves via anterior chamber angle.
• Aqueous being in closed eyeball creates intraocular pressure.
• Normal: 10 - 22mmHg.

Types of glaucoma
• Painful Glaucomas:• Acute onset: • uncommon variety. • Eye is painful,
congested.• Sudden rise of IOP due
to blockage at ant. chamber angle or pupillary area.
• Non-painful Glaucomas:
• Chronic: Over many years
• Common variety. • Open ant. chamber
angle.• Painless, gradual loss
of vision in a quiet eye.
• IOP may be elevated or within normal range.

Physiological optic disc cups
• Normal optic discs have central depression known as physiological cups.
• Cup is the base of the Bergmeister’s papilla left over after its atrophy in fetal life. Vary in size from 0.0 to 1.00 described as a cup/disc ratio.

What is glaucomatous cupping?
• The term glaucomatous cupping implies that the physiological cup starts enlarging in glaucoma.
• After the invention of ophthalmoscope in 1851 by Helmholtz the ophthalmologists were able to see the discs of chronic glaucoma patients.
• They described these optic discs as ‘cupped’.
• Since 150 years the term ‘cupping’ has become synonymous with glaucoma.

Simulation: Retina & disc fibers

Arcuate fibers & arcuate field defects
• In 1889 Bjerrum discovered comma shaped field defect on perimetry. Ronnie later found this comma shaped defect to be finishing as arcuate field defect.

Puzzling Question: Role of intraocular pressure in
glaucoma?• Q. Why do some develop glaucoma at
normal IOP of 15mmHg while others not at high IOP of 30mmHg?
• Medical history revealed that patients with HTG are usually in good health whereas those with NTG have cardio-pulmonary, circulatory problems and about 70% were long term smokers.
• Above findings suggest that NTG may be a systemic disease and therefore glaucoma may be a multifactorial disease.

Puzzling question: If glaucoma a multifactorial disease?
• If HTG is due to high IOP whereas NTG is due to systemic diseases, then why are there similar field defects and changes in the optic discs of these two different types of glaucoma?
• Why is it that in both HTG and NTG patients the peripheral fibers like arcuate are destroyed first whereas the central (Macular) fibers at the last?
• If HTG & NTG are different types, then there should be a common ground somewhere in the course of their pathogenesis.
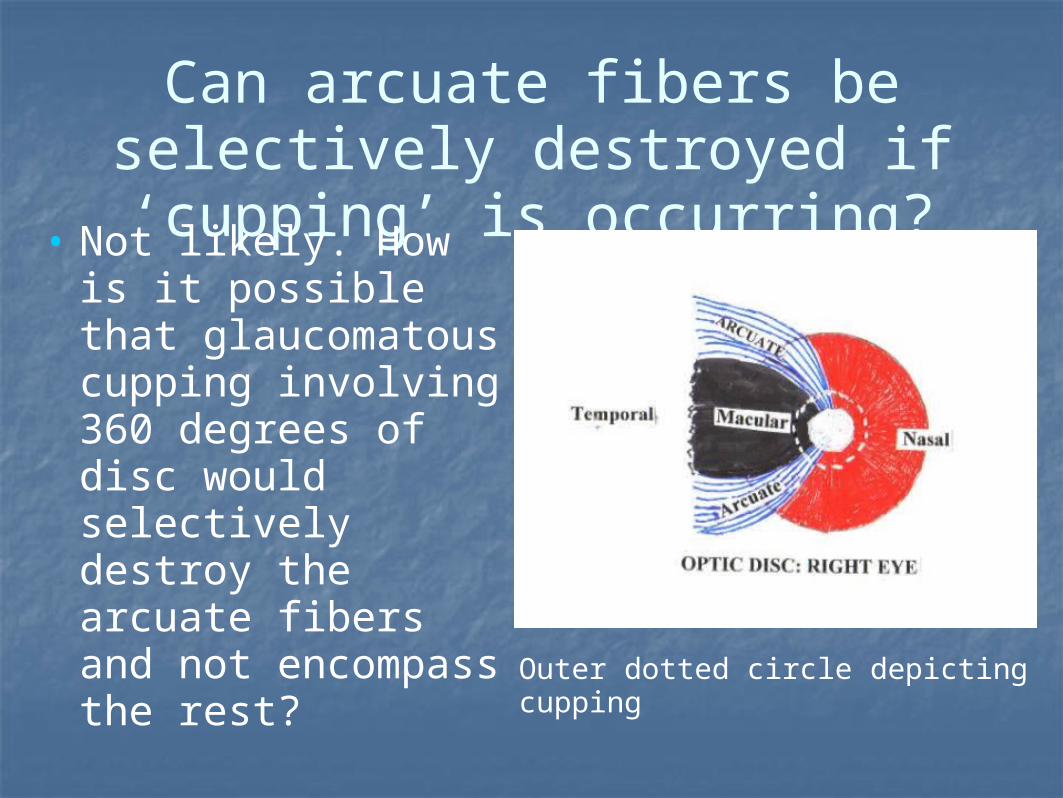
Can arcuate fibers be selectively destroyed if ‘cupping’ is occurring?• Not likely. How is it
possible that glaucomatous cupping involving 360 degrees of disc would selectively destroy the arcuate fibers and not encompass the rest?
Outer dotted circle depicting cupping

Can arcuate fibers in optic disc be selectively destroyed by any
cause?• Not likely. How is it
possible that raised IOP or any pathology could selectively destroy the arcuate fibers among the million or so densely packed fibers in the 1.5mm size disc?
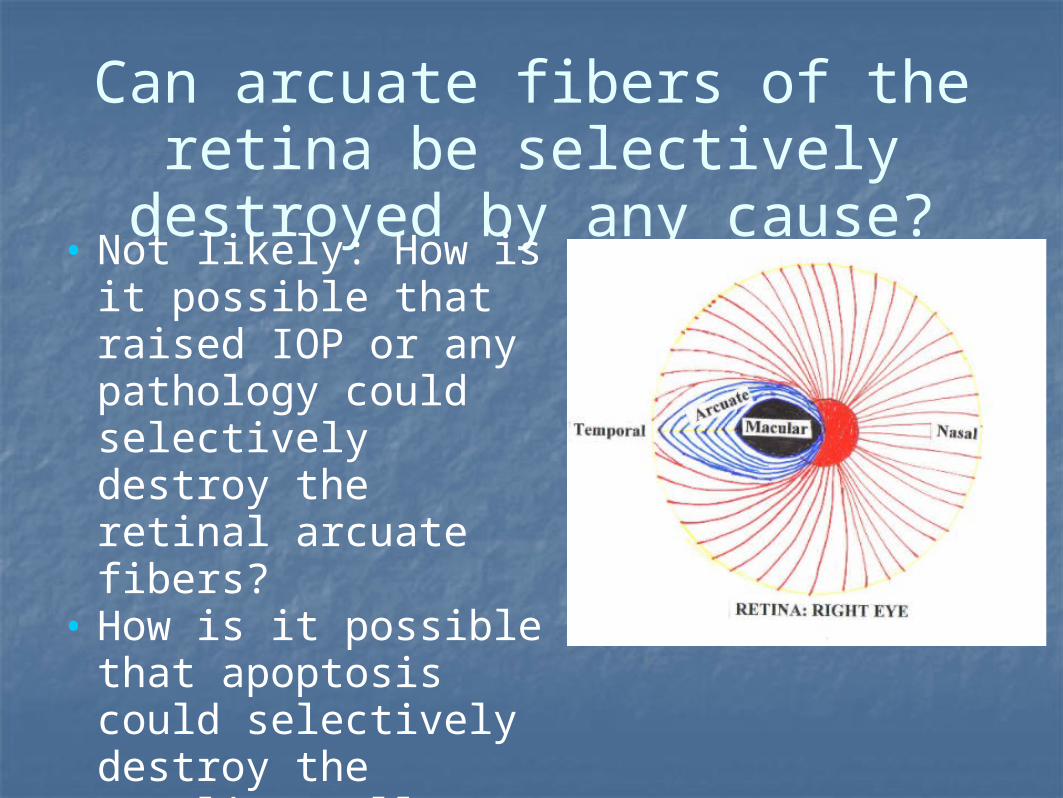
Can arcuate fibers of the retina be selectively destroyed by any
cause?• Not likely: How is it
possible that raised IOP or any pathology could selectively destroy the retinal arcuate fibers?
• How is it possible that apoptosis could selectively destroy the ganglion cells serving the arcuate fibers?

Could the border tissue be the primary site of injury?
• Likely. Circular border tissue of Elschnig lies between the scleral edge and the disc.
• Border tissue is supplied exclusively by short posterior ciliary arteries.
• Ciliary blood vessels are likely compressed by high IOP whereas ciliary circulation may be decreased systemically due to cardio-pulmonary, circulatory problems. In both instances there would be chronic ischemia of the border tissue and its atrophy. So then what happens?

Simulation: Border tissue of Elschnig
Border tissue separates the optic disc from scleral edge

What happens after the border tissue atrophies?
• Optic disc would become loose and begin to sink in the scleral foramen.
• Analogy: sinking of a manhole cover due to its poor attachments.
• If the manhole cover sinks the ‘road n. fibers’ would be stretched and severed at the edge.
• Likewise process of sinking may be occurring to the optic disc in glaucoma.

Analogy: Sinking manhole cover
Normal: Flush with road, no sinking Early Stage: Temporal sinking
Middle Stage: Loss of temporal fibers Final Stage: Total loss of optic disc
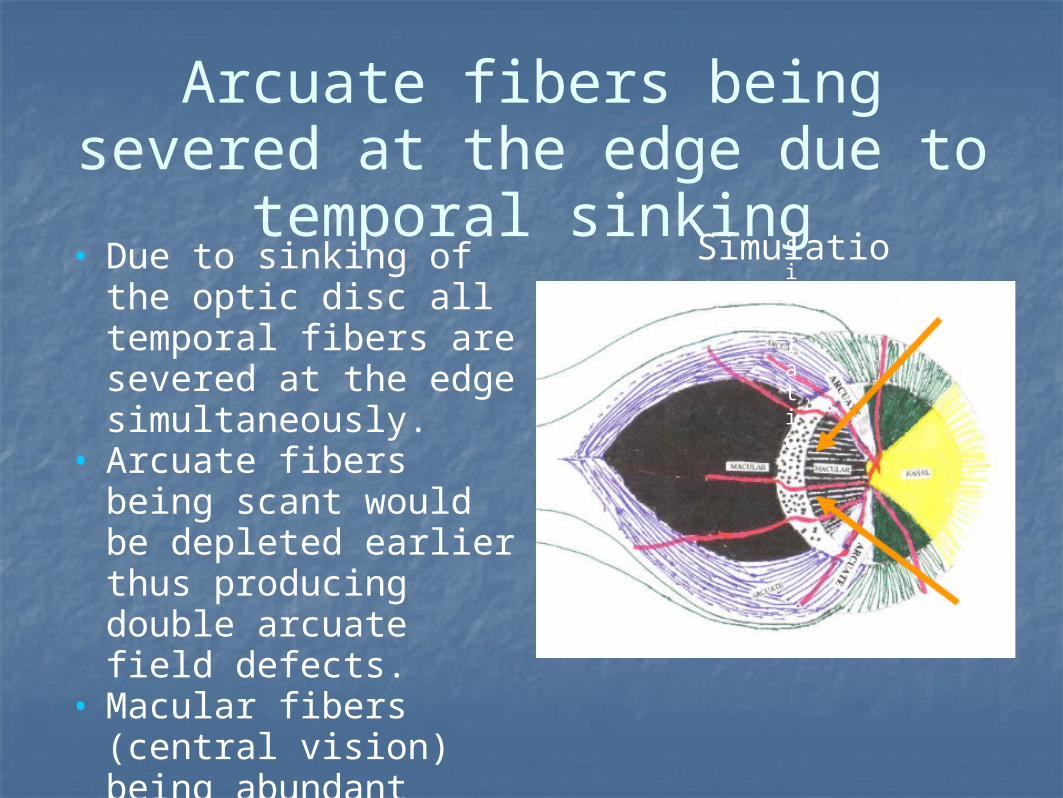
Arcuate fibers being severed at the edge due to temporal
sinking• Due to sinking of the
optic disc all temporal fibers are severed at the edge simultaneously.
• Arcuate fibers being scant would be depleted earlier thus producing double arcuate field defects.
• Macular fibers (central vision) being abundant would last till the end.
Simulation
Simulation

Destruction of arcuate fibers: Arcuate field defects
Double arcuate field defect (ring Scotoma)
Severing of the arcuate fibers at the scleral edge

What happens as the sinking of the disc progresses ?
• The retinal nerve fibers anchor the optic disc in place as roots anchor a tree.
• As the nerve fibers are being severed and depleted the optic disc becomes more loose and sinks further resulting in severing of additional fibers.
• This self-propagating cascade of loosening and sinking would continue until all the nerve fibers are cut at the edge and the disc is totally perished.
• Optic disc area is replaced with an empty crater with larger vessels hanging on the edge.

Simulation: Normal & Sinking disc
• Upper Diagram: Normal disc, arrangement of nerve fibers in the retina & optic disc
• Lower Diagram: Glaucomatous,
As the disc sinks the deeper peripheral fibers are stretched and cut at the edge whereas the central fibers move closer to the edge.
Scleral
Sclera
Border Tissue Scleral
edge
Border Tissue Scleral Edge
Arcuate
MacularArcuateArcuate
Arcuate
AArcuate Macular
MacularNasal
Nasal
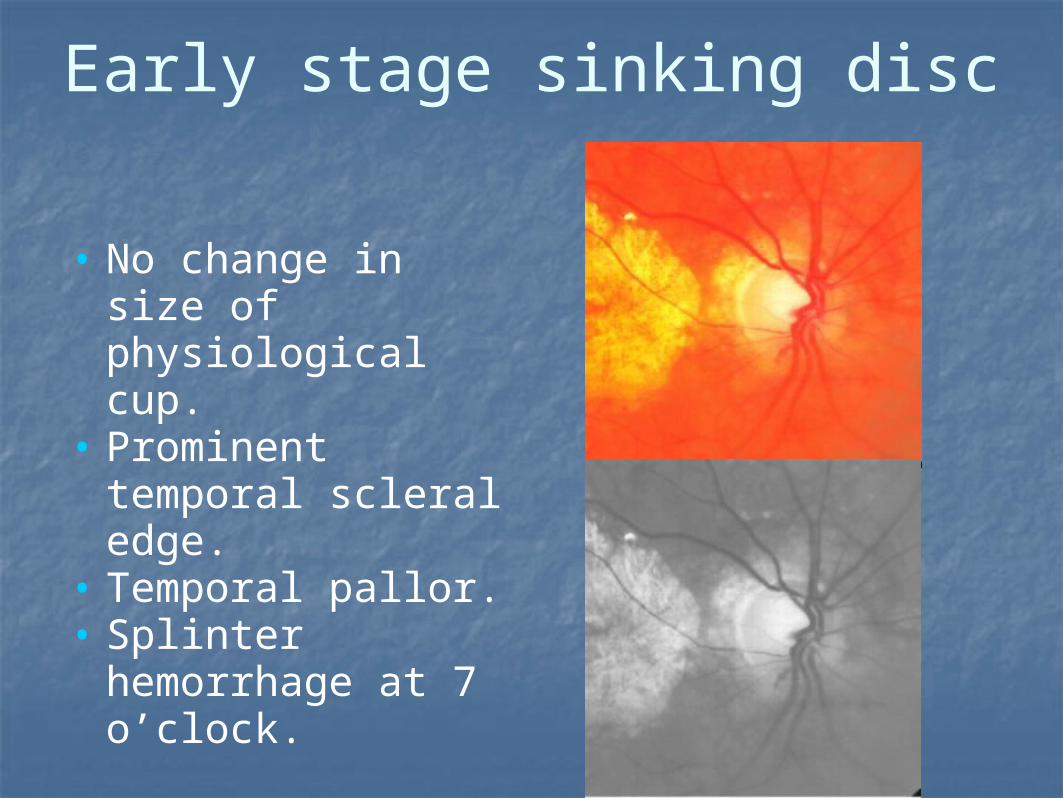
Early stage sinking disc
• No change in size of physiological cup.
• Prominent temporal scleral edge.
• Temporal pallor.• Splinter
hemorrhage at 7 o’clock.

Middle stage sinking disc
• Confluence of cup pallor with temporal pallor.
• Prominent scleral edge & baldness 7 to 9 o’clock.
• Arcuate field defect present.

Final stage sinking disc
• Optic disc area is pale due to loss of nerves and vasculature.
• Entire scleral opening is visible.
• Nasal shifting of vessels due to loss of anchorage from temporal fibers.
• Marked kinking of vessels at the edge due to absence of nerve fibers.

Conclusion based on sinking
• Optic disc may not be cupping.• Optic disc may be sinking in its entirety.• High tension glaucoma is the disease of the
eyeball itself whereas normal tension glaucoma may be a systemic disease.
• Glaucoma is a multifactorial disease. The more risk factors present, the higher likelihood and severity of development of glaucoma; akin to ischemic heart disease.
• In glaucoma the nerve fibers are being cut & depleted. At the end stage there is no disc and no nerve fibers. This is what end stage histology reveals.
NIAGARA FALLS
Just as the water flow is being cut at the edge similarly nerve fibers are being cut at scleral edge in glaucoma.





























