Embed Size (px)
Citation preview

Is FGFR an Effective Target in Cholangiocarcinoma?
Lipika Goyal, MD, MPhil Massachusetts General Hospital Cancer Center Instructor, Harvard Medical School
Chabner Symposium October 30, 2017

Disclosures
• Consultant – DebioPharm • Consultant – Ribon Therapeutics

Cholangiocarcinoma (Bile Duct Cancer)
Intrahepatic Cholangiocarcinoma
Extrahepatic Cholangiocarcinoma

Valle, J, et al. NEJM 2010

Frequent Targetable Mutations in ICC
Riener, et al. Genes Chromosomes Cancer 2008 Desphande, et al. BMC Cancer, 2011
Borger, et al. The Oncologist, 2012 Wang, et al. Oncogene 2012
Voss, et al. Human Pathology, 2013 Sia, et al. Gastroenterology, 2013 Jiao, et al. Nature Genetics, 2013
Chan-on, et al. Nature Genetics, 2013 Wu, et al. Cancer Discovery, 2013
Ross,et al. The Oncologist, 2014 Graham, et al. Human Pathology 2014
Arai, et al. Hepatology 2014 Sia, et al. Nature Communications, 2015
Slide courtesy Shoop Saha

FGFR2 fusions in cancer
Yi-Mi Wu, et al. Cancer Discovery, 2013

FGFR Pathway
Adapted from Turner & Grose, Nature Reviews Cancer 2010
Ligand Trap FGFR FGFR
Anti-FGFR Monoclonal
Antibody
Small Molecule
TKI

FGFR Signaling in Cancer
Babina & Turner, Nature Reviews 2017
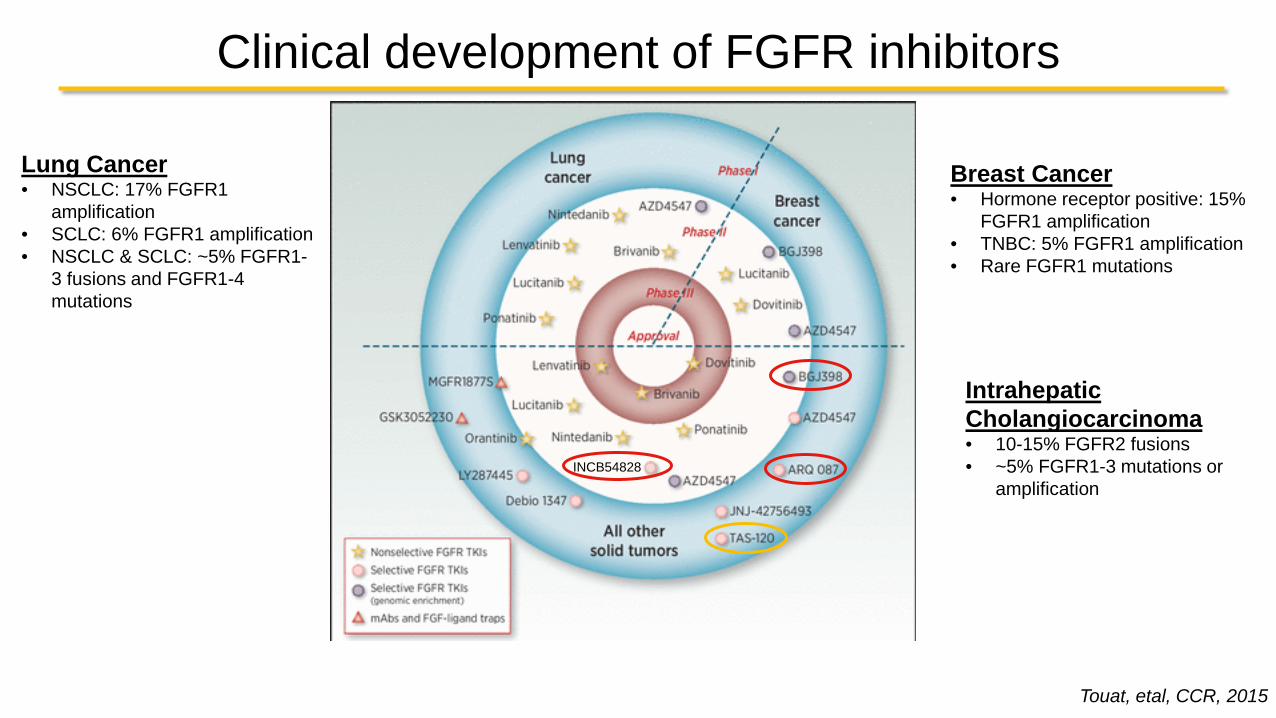
Clinical development of FGFR inhibitors
Touat, etal, CCR, 2015
INCB54828
Lung Cancer • NSCLC: 17% FGFR1
amplification • SCLC: 6% FGFR1 amplification • NSCLC & SCLC: ~5% FGFR1-
3 fusions and FGFR1-4 mutations
Breast Cancer • Hormone receptor positive: 15%
FGFR1 amplification • TNBC: 5% FGFR1 amplification • Rare FGFR1 mutations
Intrahepatic Cholangiocarcinoma • 10-15% FGFR2 fusions • ~5% FGFR1-3 mutations or
amplification

Evidence of Oncogene Addiction to FGFR2 fusions in ICC
BGJ398 FGFR2 IC50 = 1.4nM
ARQ087 FGFR2 IC50 = 1.8nM
INCB54828 FGFR2 IC50 = 3-50nM

- 1 0 0 - 1 0 0
- 8 0 - 6 0 - 4 0
- 2 0 0
2 0 4 0
6 0 8 0
1 0 0 n/N = 58/61 (95.1%)*
Bes
t Cha
nge
From
Bas
elin
e (%
)
Patients
FGFR status
FGFR2 mutation + fusion
FGFR2 amplification
FGFR2 amplification + mutation
FGFR2 mutation
FGFR2 fusion
FGFR3 amplification
Phase 2 Study of BGJ-398 in refractory FGFR-altered cholangiocarcinoma (n=61)
ORR = 14.8% (18.8% FGFR2 fusions only) DCR = 75.4% (83.3% FGFR2 fusions only)
Javle, etal, JCO, 2017, in press

Median PFS was 5.8 months (95% CI, 4.3‒7.6 months)
Phase 2 Study of BGJ-398 in refractory FGFR-altered cholangiocarcinoma (n=61)
Javle, etal, JCO, 2017, in press

Phase I/II Trial of ARQ-087: Best % Change from Baseline in Target Lesions (n=35)
Mazzaferro, etal, ASCO 2017
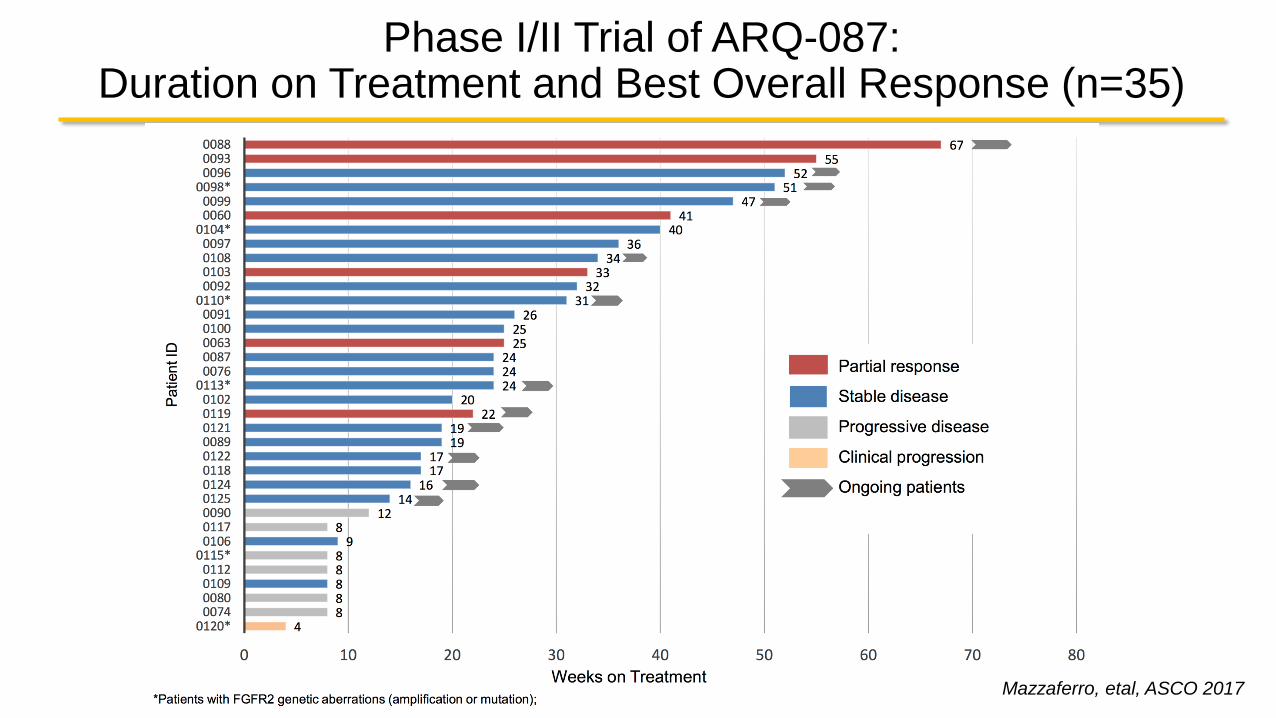
Phase I/II Trial of ARQ-087: Duration on Treatment and Best Overall Response (n=35)
Mazzaferro, etal, ASCO 2017

Phase I/II Trial of INCB54828: Best % Change from Baseline in Target Lesions
Saleh, etal, AACR 2017

Phase I/II Trial of INCB54828: Duration on Treatment and Best Overall Response
Saleh, etal, AACR 2017

Unpacking Trial Results from FGFR inhibitors in Intrahepatic Cholangiocarcinoma
1. Why is the ORR only 15-20%?
2. Why is the PFS<6 months?
3. What drug combinations might deepen and prolong responses?
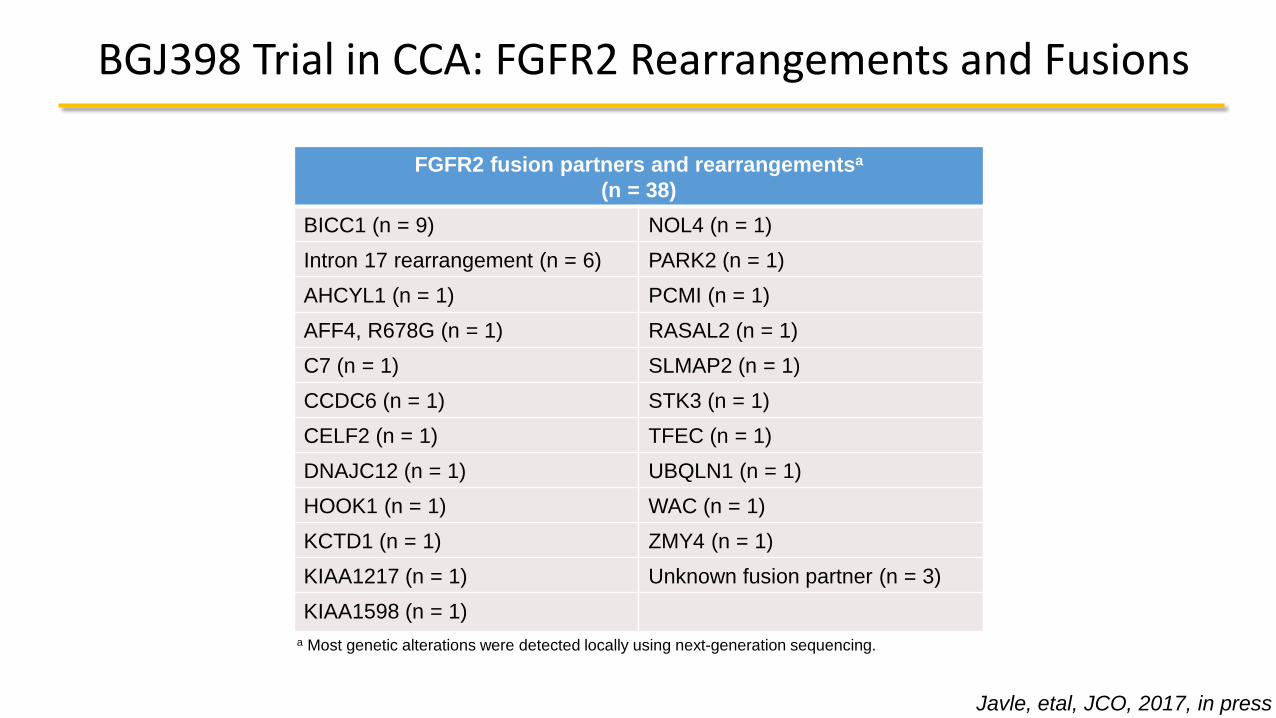
BGJ398 Trial in CCA: FGFR2 Rearrangements and Fusions
FGFR2 fusion partners and rearrangementsa
(n = 38) BICC1 (n = 9) NOL4 (n = 1) Intron 17 rearrangement (n = 6) PARK2 (n = 1) AHCYL1 (n = 1) PCMI (n = 1) AFF4, R678G (n = 1) RASAL2 (n = 1) C7 (n = 1) SLMAP2 (n = 1) CCDC6 (n = 1) STK3 (n = 1) CELF2 (n = 1) TFEC (n = 1) DNAJC12 (n = 1) UBQLN1 (n = 1) HOOK1 (n = 1) WAC (n = 1) KCTD1 (n = 1) ZMY4 (n = 1) KIAA1217 (n = 1) Unknown fusion partner (n = 3) KIAA1598 (n = 1)
a Most genetic alterations were detected locally using next-generation sequencing.
Javle, etal, JCO, 2017, in press

FGFR2 BAP1 TP53 CDKN2 A PIK3C A CDKN2B PBRM1 FGFR3 ARID1 A ARID2 A TM CDK6 FRS2 KMT2D MDM2 MET MYC TE R T TSC1 FGFR1
FGFR2 BAP1 TP53 CDKN2 A PIK3C A CDKN2B PBRM1 FGFR3 ARID1 A ARID2 A TM CDK6 FRS2 KMT2D MDM2 MET MYC TE R T TSC1 FGFR1
81% 34% 22% 16% 16%
9% 9% 9% 6% 6% 6% 6% 6% 6% 6% 6% 6% 6% 6% 3%
Likely structural variant
Known rearrangement
Known structural variant
Known amplification Known detection
BGJ398 Trial in CCA: Concurrent Genetic Alteration
Javle, etal, JCO, 2017, in press

Adverse Events associated with FGFR inhibition
Touat, etal, CCR, 2015

Acquired resistance to
BGJ398
Acquired Resistance to FGFR inhibition in ICC
Acquired resistance to
BGJ398
Published Unpublished
Overcoming BGJ398
resistance with TAS120
Acquired resistance to
TAS120

MGH Team:FGFR Resistance in Cholangiocarcinoma
Ryan B. Corcoran, MD, PhD Andrew X. Zhu, MD, PhD Dejan Juric, MD Nabeel M. Bardeesy, PhD
Leah Y. Liu, PhD Cyril Benes, PhD Shoop Saha, MD, PhD David Ting, MD, PhD


Radiological Outcomes on BGJ-398 Pre-treatment Nadir Progression
Patient #1 FGFR2-ZMYM4
Patient #2 FGFR2-OPTN
Patient #3 FGFR-BICC1
Goyal, Saha, etal, Cancer Discov, 2016
-49.9%
-28.0%
-36.9%
6 months
4 months
8 months

Biopsy: Whole Exome Seq
RNA-Seq Targeted Sequencing
Clinical Sample Acquisition Protocol
On Treatment Autopsy
Biopsy: Whole Exome Seq
RNA-Seq Targeted Sequencing
Targeted sequencing of
multiple metastases
Pre-treatment Post- Progression
ctDNA analysis: Targeted Sequencing
& Corcoran Lab
Ryan Corcoran, Nabeel Bardeesy, Leah Liu, David Ting, Dejan Juric, Andrew Zhu, Lipika Goyal
Tissue to Bardeesy Lab for PDX Generation
Tissue to Bardeesy Lab for PDX Generation
Tissue to Bardeesy Lab for PDX Generation
ctDNA analysis: Targeted Sequencing
& Corcoran Lab
ctDNA analysis: Targeted Sequencing
& Corcoran Lab
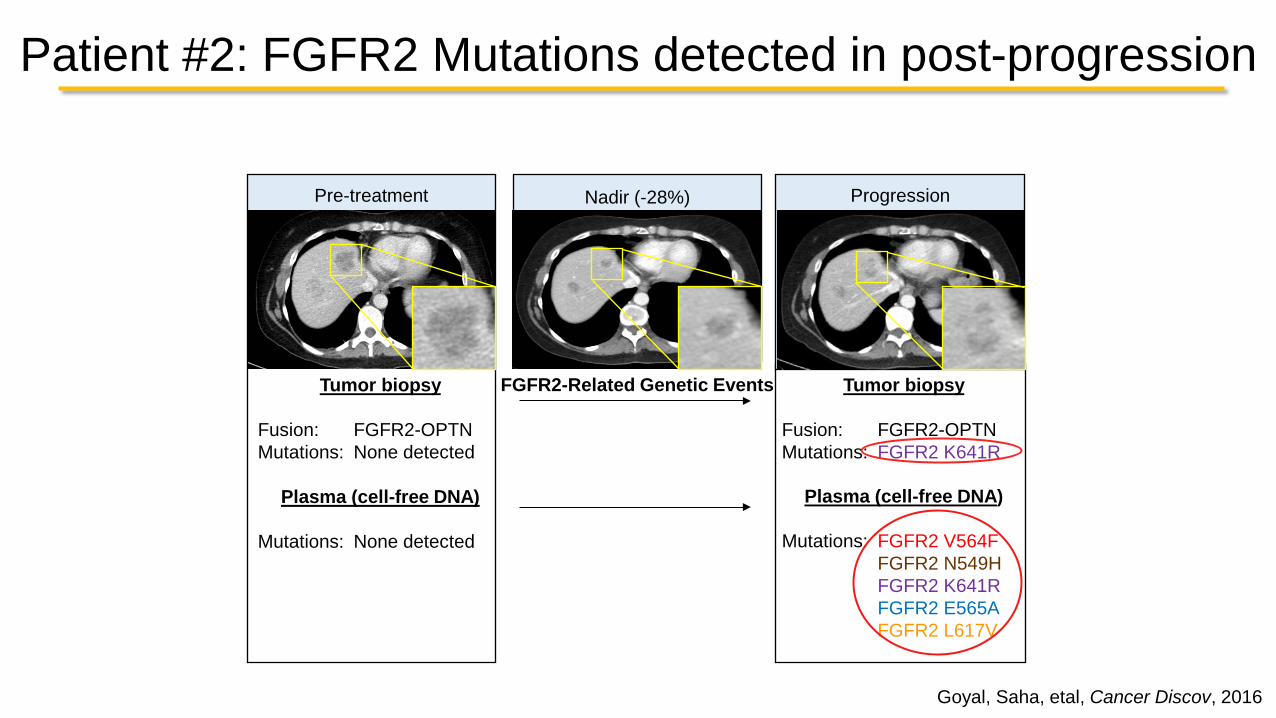
Patient #2: FGFR2 Mutations detected in post-progression
Tumor biopsy
Fusion: FGFR2-OPTN Mutations: None detected
Plasma (cell-free DNA)
Mutations: None detected
Tumor biopsy
Fusion: FGFR2-OPTN Mutations: FGFR2 K641R
Plasma (cell-free DNA)
Mutations: FGFR2 V564F FGFR2 N549H FGFR2 K641R FGFR2 E565A FGFR2 L617V
Pre-treatment Progression Nadir (-28%)
FGFR2-Related Genetic Events
Goyal, Saha, etal, Cancer Discov, 2016

Rapid autopsy Program: Dissecting Tumoral heterogeneity of resistance
1
3 4
5
1
3 4
5
CT scan
Rapid autopsy
A
Goyal, Saha, etal, Cancer Discov, 2016

Intratumoral heterogeneity of resistance
1
3 4
5 1
3
4
5

Mechanisms of FGFR Resistance
V564F N549H/K E565A V564F N549H E565A K641R
Gate Keeper Mutation
Disengagement of the molecular brake
Strengthening of the hydrophobic
spine of the kinase
Patient 1
Patient 2 L617V
K659M
Stabilization of the active conformatio
n of the FGFR2
activation loop
Byron, et al., Neoplasia 2013
Patient 3 V564F

Effect of resistance mutations on sensitivity to FGFR inhibitors
BGJ398 Ponatinib Dovitinib AZD-4547 Debio-1347 FIIN-2 LY2874455 IC50 (nM)
foldΔ IC50 (nM)
foldΔ IC50 (nM)
foldΔ IC50 (nM)
foldΔ IC50 (nM)
foldΔ IC50 (nM)
foldΔ IC50 (nM)
foldΔ SD (n) SD (n) SD (n) SD (n) SD (n) SD (n) SD (n)
BaF3 3960
1427 1478
13 1474
21 7854
683 8355
113 5865
12304 71
533 2421 (3) 446 (4) 515 (3) 2526 (3) 2850 (3) 4139 (3) 11 (3)
TEL-FGFR3 2.8
1 45
1 69
1 12
1 74
1 0.48
1 0.13
1 1.34 (4) 4 (4) 35 (4) 3.5 (4) 39 (4) 0.3 (3) 0.04 (5)
TEL-FGFR3 (L608V) 167
60 444
10 915
13 485
42 3236
44 6.7
14 0.72
5 33 (4) 29 (4) 266 (4) 98 (4) 921 (4) 2.5 (4) 0.2 (4)
TEL-FGFR3 (V555M) 1540
555 637
13 164
2 1891
164 8236
111 90
189 0.32
2 606 (4) 123 (4) 65 (4) 404 (4) 2305 (4) 31 (4) 0.01 (4)
TEL-FGFR3 (N540K) 600
216 81
2 1315
19 3454
300 6179
83 83
174 5.1
39 141 (4) 12 (4) 351 (4) 317 (4) 2037 (4) 49 (4) 1.7 (6)
TEL-FGFR3 (K650E) 41
15 309
7 991
14 230
20 1489
20 5.9
12 0.90
7 10 (4) 59 (4) 156 (4) 37 (4) 377 (4) 1.3 (4) 0.13 (4)
Goyal, Saha, etal, Cancer Discov, 2016

Acquired Resistance to FGFR inhibition in ICC
Acquired resistance to
FGFR inhibitors
Overcoming BGJ398
resistance with TAS120
Acquired resistance to
TAS120
Published Unpublished

Tan, et al., PNAS 2014
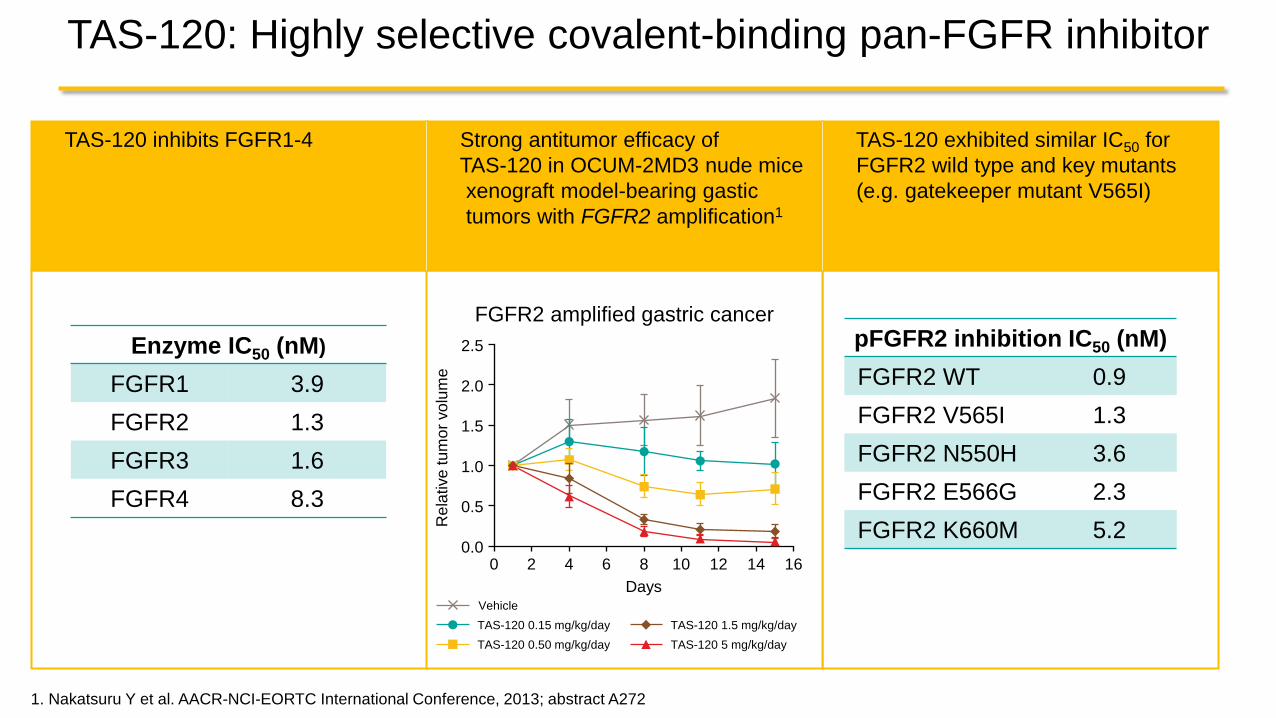
TAS-120 inhibits FGFR1-4 TAS-120 exhibited similar IC50 for FGFR2 wild type and key mutants (e.g. gatekeeper mutant V565I)
TAS-120: Highly selective covalent-binding pan-FGFR inhibitor
1. Nakatsuru Y et al. AACR-NCI-EORTC International Conference, 2013; abstract A272
pFGFR2 inhibition IC50 (nM)
FGFR2 WT 0.9 FGFR2 V565I 1.3 FGFR2 N550H 3.6 FGFR2 E566G 2.3 FGFR2 K660M 5.2
Enzyme IC50 (nM)
FGFR1 3.9 FGFR2 1.3 FGFR3 1.6 FGFR4 8.3
FGFR2 amplified gastric cancer
Strong antitumor efficacy of TAS-120 in OCUM-2MD3 nude mice xenograft model-bearing gastic tumors with FGFR2 amplification1
TAS-120 0.15 mg/kg/day TAS-120 5 mg/kg/day TAS-120 0.50 mg/kg/day TAS-120 1.5 mg/kg/day
Vehicle
2.5
2.0
1.5
1.0
0.5
0.0 0 2 4 6 8
Days
Rel
ativ
e tu
mor
vol
ume
10 12 14 16

TAS-120: Waterfall plot in FGF/FGFR aberrant CCA
-100
-50
0
50
100
*
*
Cha
nge
from
bas
elin
e in
long
est d
iam
eter
(%)
FGFR2 fusion Other FGF/FGFR alteration
uPR = unconfirmed PR, cPR = confirmed PR 4 of the 23 patients are not included as they have no scans available yet; of these, 3 had prior FGFRi; Cut-off date: May 12, 2017
uPR cPR uPR cPR
*Prior treatment with FGFR inhibitor
Goyal, etal, GI ESMO, 2017

TAS-120: Efficacy after prior FGFR inhibitor 73yo F with FGFR2-SORBS1 fusion+ ICC who progressed on Gemcitabine/Cisplatin and FOLFOX
Goyal, etal, AACR-NCI-EORTC Conference 2017

Acquired Resistance to FGFR inhibition in ICC
Acquired resistance to
FGFR inhibitors
Overcoming BGJ398
resistance with TAS120
Acquired resistance to
TAS120
Published Unpublished

Acquired resistance to TAS120 • 56yoF w/ FGFR2-BICC1 fusion+ ICC • Treated with Gem/CisFOLFOXTAS120 • Concurrent mutations in Tissue:
•Baseline : FGFR2-BICC1 fusion (SFA)
Post TAS-120 PFS 7.2 months
Pre TAS-120 Nadir -46.4% Bone Lesion Progression in Spine
Post-progression: FGFR2-BICC1 fusion, and PIK3C2B Amplification among others *FGFR2 and RAS mutations were not found

Acquired Resistance to TAS120
• Why were no FGFR2 or RAS mutations found on biopsy? • Is FGFR2 C491F the primary driver of acquired resistance? • Why did the gatekeeper mutation arise? • What is the relevance of the KRAS and NRAS mutations? • Why did she progress in her bones?
Post-TAS 120 Biopsy FGFR2-BICC1 fusion MDM4 amplification BAP1 A606fs*11 PIK3C2B amplification *CDKN2B p. D86N *IGF1R p. N135Y *KDM5A p. Q1197P *LRP1B p. N2336H *MAGI2 p. A899T *NF1 p. L2439V *NTRK1 p. G18E *PIK3C2B p. V213G *PLCG2 p. L209R ZNF703 p. H402_D403>PTHLGGSSCSTCSAHD

4. TAS120 Resistance may develop via mutation of the P-Loop cysteine and/or upregulation by bypass tracks.
• Same questions as #2 • Do tumors need a double hit to become resistant?
FGFRi in ICC: Conclusions and Future Directions
1. FGFR alterations are present in 15-20% of ICCs and in multiple tumor types. • Why is there primary resistance in many patients with FGFR2 fusions? • Which FGFR mutations and amplifications are druggable?
2. Acquired BGJ398 resistance can occur through FGFR2 kinase mutations. • Which ones emerge first and are clinically relevant? • What FGFR-independent mechanisms of resistance exist? • What non-genomic mechanisms of resistance exist? • What drugs and drug combinations can delay or overcome resistance? • Will more specific and more potent FGFR2 inhibitors lead to higher ORR&PFS?
3. BGJ398 resistance can be overcome, in some cases, by TAS120. • Which other drugs and drug combinations can delay or overcome resistance? • What is the drug development strategy for Taiho and PrincipioBio?

Acknowledgements
Clinical team: Andrew X. Zhu David P. Ryan Avinash Kambadakone Vikram Deshpande Rapid Autopsy Program Dejan Juric James R. Stone Translational Research Laboratory (TRL): A. John Iafrate Jochen Lennerz Darrell Borger Ting Laboratory: David Ting
Bardeesy Lab: Nabeel Bardeesy Leah Y. Liu Phuong Vu Supriya K. Saha Corcoran Lab: Ryan B. Corcoran Leanne G. Ahronian Bardelli Lab: Alberto Bardelli Giulia Siravegna Benedetta Mussolin Broad Institute: Ignaty Leshchiner Gad Getz
Benes Lab: Cyril Benes Novartis: Diana Graus Porta Ralph Tiedt Sabrina Baltschukat Barbara Schacher-Engstler Louise Barys Christelle Stamm Pascal Furet Research Assistants: Jordan Maurer Chandler Shapiro Stephanie Reyes Emily E. Van Seventer
Patients and their families who generously participated in research
Funding support for this project: NIH GI SPORE, ECOR Fund for Medical Discovery, Jonathan Kraft Translational Research Award, MGH American Cancer Society Grant, Cholangiocarcinoma Foundation

Patie
nts
0 16 32 48 64 80 96 112 128 144 160 176 192 208 224 240 256 272 288 304 320 336 352 368 384 400 416
Treatment Duration (days)
Investigator-Assessed Response Partial response Stable disease Progressive disease
BGJ398 dose (mg) 125 mg 100 mg 75 mg 50 mg 25 mg
BGJX2204 Trial: Time to Response

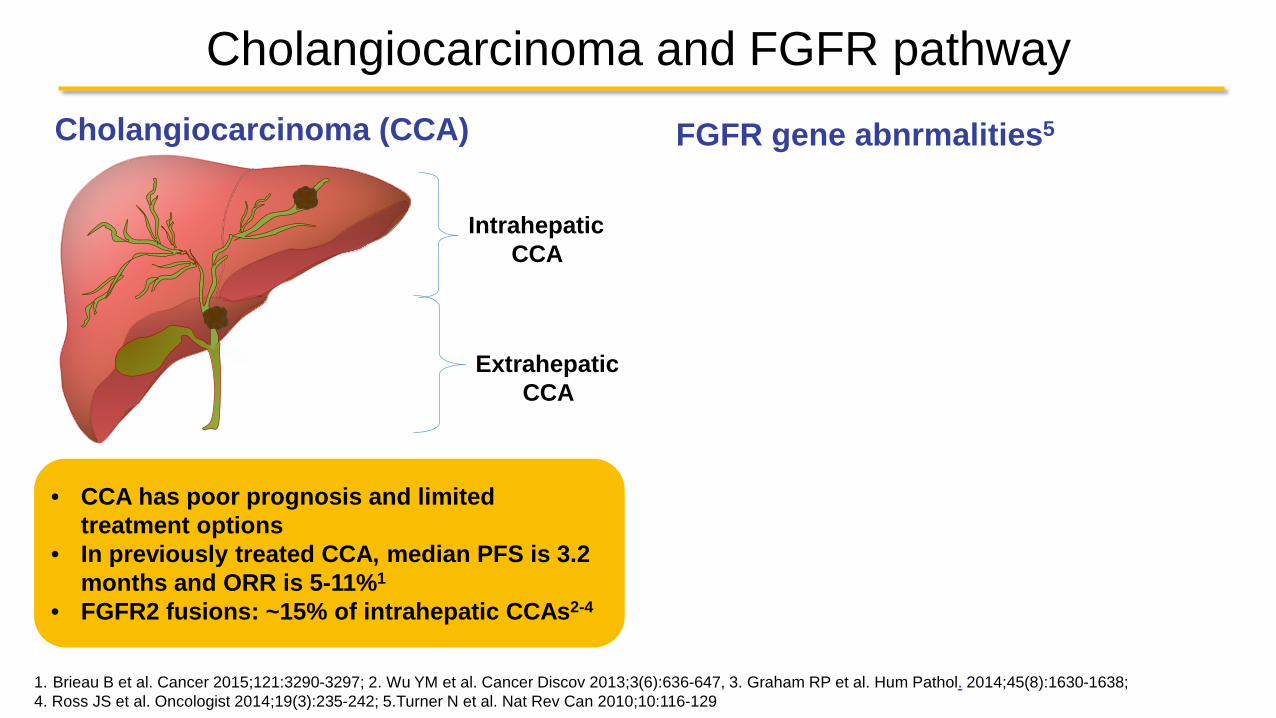
Cholangiocarcinoma and FGFR pathway FGFR gene abnrmalities5
1. Brieau B et al. Cancer 2015;121:3290-3297; 2. Wu YM et al. Cancer Discov 2013;3(6):636-647, 3. Graham RP et al. Hum Pathol. 2014;45(8):1630-1638; 4. Ross JS et al. Oncologist 2014;19(3):235-242; 5.Turner N et al. Nat Rev Can 2010;10:116-129
• CCA has poor prognosis and limited treatment options
• In previously treated CCA, median PFS is 3.2 months and ORR is 5-11%1
• FGFR2 fusions: ~15% of intrahepatic CCAs2-4
Intrahepatic CCA
Extrahepatic CCA
Cholangiocarcinoma (CCA)

Cholangiocarcinoma Mutational Spectrum (TCGA)

Phase 2 Study of BGJ-398 in refractory FGFR-altered cholangiocarcinoma
Javle, et al. GI ASCO 2015
-50% -28%
-37%

Mutation in P-loop Cysteine Confers Resistance
• FIIN-2 and TAS120 covalently bind to Cysteine residues in the kinase domain receptor of FGFR
• Mutation of FGFR kinase domain cysteine residue (C491F) in cholangiocarcinoma is associated with disease progression

MGH Efforts to study FGFR inhibition and resistance Clinical Efforts: Andrew Zhu, Lipika Goyal
Laboratory Efforts: Corcoran, Bardeesy, Benes, and Ting Labs
Patient-derived Xenograft (PDX)
Digest &
Culture
ICC Cell Lines
Genetically-Engineered Mouse Models (GEMMs)
ICC Organoid
ctDNA ddPCR 2 FGFR Altered
ICC Lines
15 FGFR WT ICC Lines
Corcoran Lab
Bardeesy Lab Benes Lab Ting Lab
CTC analysis RNA Seq
Rapid Autopsy: Dejan Juric
Breast: 18
Pancreatic: 2
Colorectal: 3
Melanoma: 2
Cholangio: 6
Lung: 13 Epithelial: 2

Phase 2 Study of BGJ-398 in refractory FGFR-altered
cholangiocarcinoma
3.6 months
5.6 months
7.4 months
Javle, et al. GI ASCO 2015
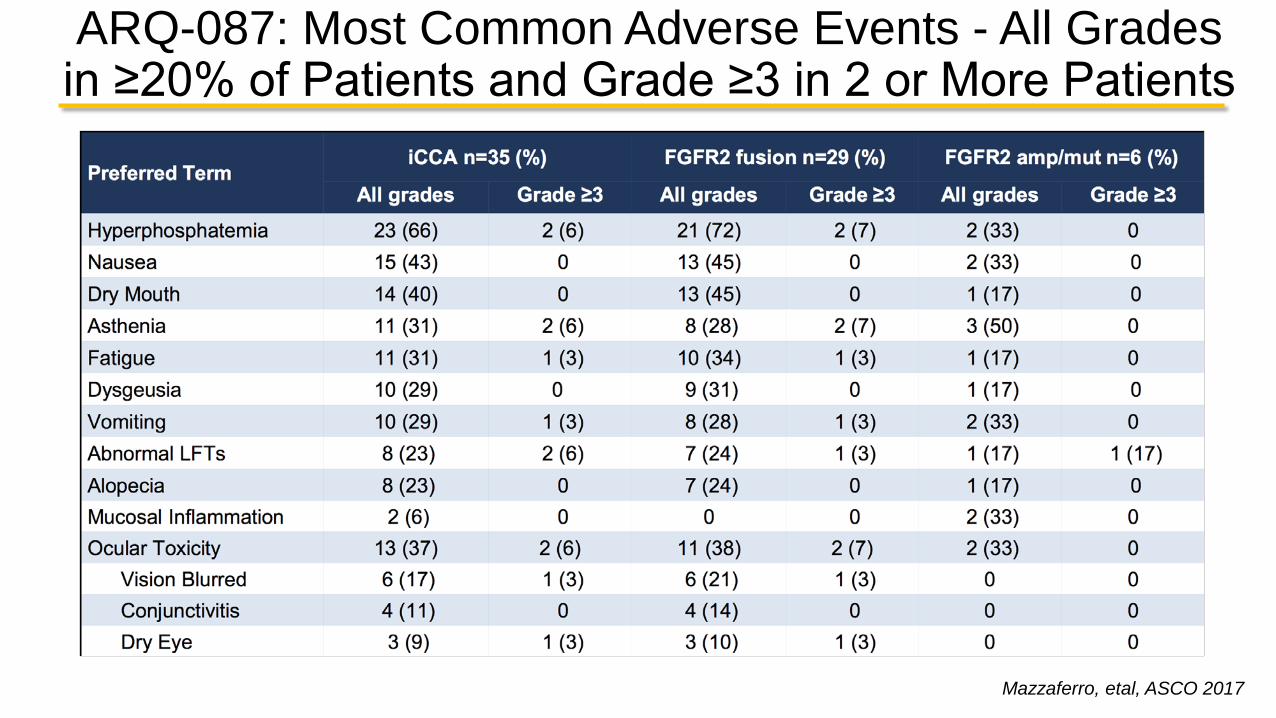
ARQ-087: Most Common Adverse Events - All Grades in ≥20% of Patients and Grade ≥3 in 2 or More Patients
Mazzaferro, etal, ASCO 2017





























