Embed Size (px)
Citation preview

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 1/186
PHYSIOTHERAPY IN THEPHYSIOTHERAPY IN THE
MANAGEMENT OFMANAGEMENT OFPARKINSONPARKINSON·S DISEASE·S DISEASE
Presented byPresented byIROGUE.EGHOSA. KENNEDY IROGUE.EGHOSA. KENNEDY
MRH/2005/024MRH/2005/024
Student PhysiotherapistStudent PhysiotherapistDepartment Of Medical RehabilitationDepartment Of Medical Rehabilitation
Faculty of Basic Medical Science,O.A.U Ile IfeFaculty of Basic Medical Science,O.A.U Ile Ife
SPECIAL TOPIC SEMINAR MRH 507SPECIAL TOPIC SEMINAR MRH 507

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 2/186
PRESENTATION OBJECTIVESPRESENTATION OBJECTIVES
To define To define key issues in the management of key issues in the management of Parkinson·sParkinson·s disease (PD) relating disease (PD) relating to physiotherapy to physiotherapy treatmenttreatment..
To To inform our knowledge of currentinform our knowledge of current evidenceevidence--
basedbased recommendations of physiotherapy inrecommendations of physiotherapy inParkinson's disease.Parkinson's disease.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 3/186
OUTLINEOUTLINE DefinitionDefinition
ClassificationClassification
Background /Background / History History
DiagnosisDiagnosis
Differential diagnosisDifferential diagnosis Pathophysiology Pathophysiology
Epidemiology Epidemiology
Clinical features /Clinical features / presentation.presentation.
Prognostic factorPrognostic factor
ManagementsManagements of of Parkinson·sParkinson·s diseasedisease
Medical therapy Medical therapy
Surgical therapy Surgical therapy
Physiotherapy Physiotherapy

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 4/186
Overview of Parkinson·s diseaseOverview of Parkinson·s disease
Also known as : Also known as :
Paralysis agitansParalysis agitans
Shaking palsy.Shaking palsy.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 5/186
Why Parkinson·s disease ? Why Parkinson·s disease ?
The The evidenceevidence availableavailable toto practitioners practitioners with with regardsregards toto appropriateappropriate
physiotherapy physiotherapy interventionintervention forfor people people with with Parkinson'sParkinson's diseasedisease upup
tilltill thethe RESCUERESCUE ProjectProject randomisedrandomised controlcontrol trialtrial hashas eithereither beenbeen
of of poor poor qualityquality oror absentabsent.. PhysiotherapyPhysiotherapy hashas thereforetherefore hadhad toto relyrely
onon unsubstantiatedunsubstantiated anecdotalanecdotal reportsreports fromfrom professionals, professionals, people people
with with Parkinson·sParkinson·s oror carerscarers regardingregarding thethe effectivenesseffectiveness of of inputinput.. An An
effectivenesseffectiveness bulletinbulletin onon neurologicalneurological conditionsconditions (Chartered(Chartered
SocietySociety of of PhysiotherapyPhysiotherapy 20012001)) concludedconcluded thatthat manymany areasareas of of
physiotherapy physiotherapy hadhad yet yet toto bebe sufficientlysufficiently evaluatedevaluated..

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 6/186
InIn neurologicalneurological problems, problems, Parkinson·sParkinson·s diseasedisease isis thethe
mostmost commoncommon disorderdisorder leadingleading toto gaitgait disturbancedisturbance andand
fallsfalls (Stolze(Stolze etet al,al, 20052005))..
DespiteDespite advancesadvances inin pharmacological pharmacological treatmentstreatments andand
surgicalsurgical techniques,techniques, gaitgait andand balancebalance deficitsdeficits stillstill
persist persist andand areare associatedassociated with with lossloss of of independence,independence,
immobilityimmobility andand highhigh costcost forfor healthcarehealthcare systemssystems..
(Grimbergen(Grimbergen etet alal..,, 20042004))..
OtherOther mobilitymobility deficits,deficits, includesincludes difficultiesdifficulties with with
transferstransfers andand posture posture..

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 7/186
This frequently leads to loss of independence, (fear of) falls, This frequently leads to loss of independence, (fear of) falls,
injuries, and inactivity, resulting in social isolation and aninjuries, and inactivity, resulting in social isolation and an
increased risk of osteoporosis or cardiovascular disease. (Bloem,increased risk of osteoporosis or cardiovascular disease. (Bloem,
et al., 2001; Garrett, et al., 2004).et al., 2001; Garrett, et al., 2004).
Consequently, costs increase (Pressley, et al., 2003) and qualityConsequently, costs increase (Pressley, et al., 2003) and quality
of life decreases (Schrag, et al., 2000).of life decreases (Schrag, et al., 2000).
These mobility deficits are difficult to treat with drugs or These mobility deficits are difficult to treat with drugs or
neurosurgery. (Schrag et al., 2002; Bloem et al., 1996)neurosurgery. (Schrag et al., 2002; Bloem et al., 1996)
Physical therapy is often prescribed next to medical treatmentPhysical therapy is often prescribed next to medical treatment
(Keus, et al., 2004). Therefore, the awareness and application of (Keus, et al., 2004). Therefore, the awareness and application of
rehabilitation approaches that work in conjunction with currentrehabilitation approaches that work in conjunction with current
treatment is important to manage thesetreatment is important to manage these problems. problems.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 8/186
However, there is presently the first evidenceHowever, there is presently the first evidence--basedbased
international guideline for physical therapy in Parkinson·s diseaseinternational guideline for physical therapy in Parkinson·s disease
developed according to international standards of guidelinedeveloped according to international standards of guideline
development with practical recommendations graded accordingdevelopment with practical recommendations graded according
to scientific evidence.to scientific evidence.
This is the KNGF guidelines for physical therapy in patients This is the KNGF guidelines for physical therapy in patients
with Parkinson·s disease. The guidelines identify six core areas of with Parkinson·s disease. The guidelines identify six core areas of
physiotherapy practice: physical capacity and prevention of physiotherapy practice: physical capacity and prevention of
inactivity; transfers; gait; posture; reaching and grasping; andinactivity; transfers; gait; posture; reaching and grasping; and
balance and falls. To this guideline we based currentbalance and falls. To this guideline we based current
physiotherapy management on Parkinson·s disease physiotherapy management on Parkinson·s disease

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 9/186
InIn Africa, Africa, NigeriaNigeria toto bebe precise precise aa recentrecent researchresearch onon thethe
clinicalclinical profile profile of of Parkinson·sParkinson·s diseasedisease patients patients showsshows thatthat itit
isis thethe samesame with with otherother population population butbut characterisedcharacterised byby
delayeddelayed presentation presentation asas hashas beenbeen reportedreported inin otherother
developingdeveloping countriescountries.. Young Young--onsetonset Parkinson·sParkinson·s diseasediseaseoccursoccurs butbut maymay bebe lessless commonlycommonly encounteredencountered andand
frequencyfrequency of of positive positive familyfamily historyhistory isis lowerlower thanthan inin
western western population population (Okubadejo(Okubadejo etet alal..,, 20102010))..physiotherapy physiotherapy
isis thereforetherefore advocatedadvocated inin combinationcombination with with optimaloptimal timingtiming
of of medications(Morrismedications(Morris etet alal..,,19981998))

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 10/186
DEFINITIONDEFINITION
MarsdenMarsden ((19941994)) defineddefined parkinson·s parkinson·s diseasedisease asas aa
clinicalclinical syndromesyndrome of of movementmovement consistingconsisting of of tremortremor atat
rest,rest, rigidity,rigidity, elementselements of of bradykinesiabradykinesia (slowness(slowness of of
movement),movement), akinesia(lossakinesia(loss of of movement)movement) andand postural postural
abnormalitiesabnormalities associatedassociated with with aa distinctivedistinctive pathology pathology
consistingconsisting of of degenerationdegeneration of of pigmented pigmented brainbrain stemstem
nuclei,nuclei, includingincluding thethe dopaminergicdopaminergic SubstantiaSubstantia NigraNigra
ParPar Compacta(SNPC)Compacta(SNPC) with with thethe presence presence of of lewylewy
bodiesbodies inin thethe remainingremaining nervenerve cellscells..

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 11/186
HISTORY/BACKGROUNDHISTORY/BACKGROUND InIn 18171817,, James James ParkinsonParkinson firstfirst describeddescribed thethe
ParkinsonParkinson diseasedisease.. HisHis descriptiondescription of of thethe diseasedisease
was was asas followsfollows..
InvoluntaryInvoluntary tremuloustremulous motion,motion, with with lessenedlessened
muscularmuscular power power inin parts parts notnot inin actionaction andand eveneven when when
supportedsupported with with aa propensity propensity toto bendbend thethe trunk trunk forwardforward andand toto pass pass fromfrom aa walking walking toto runningrunning paces paces;;
thethe sensessenses andand intellectsintellects beingbeing uninjureduninjured..

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 12/186
In 1867, Trousseau noted the muscular rigidity andIn 1867, Trousseau noted the muscular rigidity and
cog wheeling appearance.cog wheeling appearance.
In 1877, Charcot named first disease as Parkinson·sIn 1877, Charcot named first disease as Parkinson·s
disease as he noted the absence of facial expressiondisease as he noted the absence of facial expression
(masked faces) as a feature of the disorder.(masked faces) as a feature of the disorder.
In 1880, Charcot listed PD as the 5In 1880, Charcot listed PD as the 5thth most commonmost common
disease.disease.
In 1888, Gower noted that, the malady usuallyIn 1888, Gower noted that, the malady usually
commences after 40years of age.commences after 40years of age.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 13/186
InIn 18981898,, PurvesPurves Stewart,Stewart, recognizedrecognized distinctdistinct
positioning positioning of of thethe feet,feet, usuallyusually provoked provoked byby exerciseexercise
butbut occasionallyoccasionally relievedrelieved byby walking walking andand which which couldcould
bebe thethe firstfirst symptomsymptom of of thethe maladymalady..
InIn 19131913,, lewylewy firstfirst describeddescribed thethe concentricconcentric hyalinehyalinecytoplasmiccytoplasmic inclusioninclusion andand calledcalled itit asas lewylewy bodybody.. ItIt isis
observedobserved inin thethe nucleusnucleus of of substantiasubstantia innominatainnominata..
InIn 19191919,, Tretiakoff Tretiakoff was was thethe firstfirst toto observeobserve thethe
characteristiccharacteristic lesionslesions of of substantiasubstantia nigranigra ii..ee depletiondepletion
of of pigmented pigmented cellscells..

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 14/186
InIn 19371937,, HasslerHassler describeddescribed thethe anatomyanatomy of of substantiasubstantia
nigranigra andand inin 19381938,, noticednoticed pathological pathological processes processes of of PDPD
forfor thethe ventrolateral ventrolateral pars pars compactacompacta cellcell groupgroup..
InIn 19571957,, CarlsonCarlson showedshowed thatthat cerebralcerebral dopaminedopamine was was
concentratedconcentrated inin thethe striatumstriatum..
InIn 19601960,, EhingerEhinger andand HonykiewiczHonykiewicz demonstrateddemonstrated thatthat inin
PD,PD, dopaminedopamine was was markedlymarkedly reducedreduced inin thethe substantiasubstantia
NigraNigra caudatecaudate nucleusnucleus andand putamen putamen..
InIn 19671967,, CotziasCotzias showsshows thethe clinicalclinical benefitsbenefits of of highhigh dosedose
of of levolevo--dopadopa inin chronicchronic patients patients with with PDPD..

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 15/186
CLASSIFICATIONCLASSIFICATION BASED ONBASED ON
AETIOLOGY AETIOLOGY
PrimaryPrimary oror idiopathicidiopathic Parkinson·sParkinson·s diseasedisease
SecondarySecondary oror acquiredacquired oror symptomaticsymptomatic
Parkinson·sParkinson·s diseasedisease
Parkinson·sParkinson·s plus plus syndromesyndrome.. (adapted(adapted fromfromFahnFahn andand Jankovic Jankovic 19921992))

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 16/186
PRIMARY OR IDIOPATHICPRIMARY OR IDIOPATHIC
PARKINSON·S DISEASEPARKINSON·S DISEASE
ItIt is a progressive, disabling,is a progressive, disabling, primary primary
neurodegenerativeneurodegenerative disorder. There are fourdisorder. There are four signs:signs:
Rest tremorRest tremor
RigidityRigidity
BradykinesiaBradykinesia
Postural instabilityPostural instability
((The first three are together called the classical triad) The first three are together called the classical triad)

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 17/186
SECONDARY OR SYMPTOMATIC OR SECONDARY OR SYMPTOMATIC OR
ACQUIRED PARKINSONISM ACQUIRED PARKINSONISM
ItIt isis thethe collectivecollective termterm forfor aa groupgroup of of conditionsconditions thatthat
indicateindicate PDPD asas well well asas severalseveral otherother degenerativedegenerative brainbrain
disordersdisorders.. The The signssigns andand symptomssymptoms includesincludes thethe fourfour
cardinalcardinal signssigns of of PDPD.. ParkinsonParkinson resultsresults fromfrom aa variety variety
of of causescauses thatthat includeinclude infections,infections, toxins,toxins, drugs,drugs, vascular vascular lesions,lesions, tumortumor andand traumatrauma.. ((neuropepticneuropeptic
drugsdrugs areare consideredconsidered toto bebe thethe commonestcommonest causecause of of
secondarysecondary ParkinsonParkinson today)today)

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 18/186
PARKINSONPARKINSON--PLUS SYNDROME OR PLUS SYNDROME OR
PARKINSONISM SYNDROMEPARKINSONISM SYNDROME
ItIt constitutesconstitutes of of heterogeneousheterogeneous groupgroup of of
multifacetedmultifaceted disorderdisorder characterisedcharacterised byby
parkinsonia parkinsonia features,features, with with various various combinationscombinations
of of pyramidal, pyramidal, cerebella,cerebella, andand autonomicautonomic
dysfunctionsdysfunctions.. (The(The mostmost commoncommon formform of of
ParkinsonismParkinsonism seenseen byby neurologistsneurologists todaytoday isis thethe
idiopathicidiopathic variety variety of of Parkinson·sParkinson·s disease)disease)..

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 19/186
ExamplesExamples of Parkinsonof Parkinson--plus syndrome are: plus syndrome are:
1 )1 ) PROGRESSIVE SUPRANUCLEAR PALSY:PROGRESSIVE SUPRANUCLEAR PALSY:
EarlyEarly postural postural instabilityinstability andand fallsfalls Vertical gaze palsy Vertical gaze palsy
Rigidity of trunk Rigidity of trunk
Speech and swallowing problemSpeech and swallowing problem Unusual tremorUnusual tremor
Symmetrical onsetSymmetrical onset

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 20/186
Examples of ParkinsonExamples of Parkinson--plus syndrome: plus syndrome:
2 )2 ) MULTIPLE SYSTEMIC ATROPHY MULTIPLE SYSTEMIC ATROPHY
EarlyEarly autonomic features (postural BP decrease andautonomic features (postural BP decrease and
bladder dysfunctionbladder dysfunction))
Cerebella pyramidalCerebella pyramidal signsign
Rigidity>tremorsRigidity>tremors
3)3) LE W Y BODY LE W Y BODY DEMENTIA DEMENTIA
4)4) VASCULAR VASCULAR PARKINSONISMPARKINSONISM
5)5) PUGILISTIC ENCEPHALOPATHY PUGILISTIC ENCEPHALOPATHY
(TRAUMA)(TRAUMA)

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 21/186
Examples of ParkinsonExamples of Parkinson--plus syndrome: plus syndrome:
6 )6 ) POSTPOST ENCEPHALOPATHY ENCEPHALOPATHY
7) DRUG7) DRUG INDUCED E.G NEUROLEPTICS,INDUCED E.G NEUROLEPTICS,
PROCHLORPERAZINEPROCHLORPERAZINE AND ANDMETOCLOPRAMIDE.METOCLOPRAMIDE.
8) TOXIN8) TOXIN INDUCED E.G MANGANESE,INDUCED E.G MANGANESE, COPPER COPPER
(( WILSON·S DISEASE) WILSON·S DISEASE)

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 22/186
DIAGNOSISDIAGNOSIS
a)a) The diagnosis of PD is based on the clinical symptoms & The diagnosis of PD is based on the clinical symptoms &signs.signs.
b)b) Blood & CSF examination and cerebral imaging such as CTBlood & CSF examination and cerebral imaging such as CT
Scan, MRI are non contributory in making the diagnosis of Scan, MRI are non contributory in making the diagnosis of
PD.PD.
c)c) Positron Emission Tomography (PET) using fluorodopa hasPositron Emission Tomography (PET) using fluorodopa has
been useful in detecting loss of dopa uptake in the striatum . Itbeen useful in detecting loss of dopa uptake in the striatum . It
shows 60% reduction of fluorodopa uptake.shows 60% reduction of fluorodopa uptake.
d)d) Single Photon Emission Computerised TomographySingle Photon Emission Computerised Tomography
(SPECT).(SPECT).

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 23/186
DIAGNOSISDIAGNOSIS
DN A Analysis:DN A Analysis: -- mitochondrial complex 1 activity ismitochondrial complex 1 activity isreduced, alterations in DN A, Monoamine oxidasereduced, alterations in DN A, Monoamine oxidase--BB(M AO(M AO--B) activity increased.B) activity increased.
The diagnosis is usually made on the basis of history The diagnosis is usually made on the basis of history & clinical examination. Handwriting samples,& clinical examination. Handwriting samples,speech analysis, interview questions that focus onspeech analysis, interview questions that focus on
developing symptomatology & physical examinationdeveloping symptomatology & physical examination
are used in the preclinical stage to detect early are used in the preclinical stage to detect early manifestations of the disease.manifestations of the disease.
The diagnosis of PD can be made if at least two of The diagnosis of PD can be made if at least two of
the cardinal features are present.the cardinal features are present.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 24/186
DIAGNOSISDIAGNOSIS
g)g) EMG may be done to find out the level of rigidity & alsoEMG may be done to find out the level of rigidity & also
to know the increase in the reaction time & movementto know the increase in the reaction time & movement
time.time.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 25/186
A TYPICAL EMG A TYPICAL EMG

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 26/186
DIFFERENTIAL DIAGNOSISDIFFERENTIAL DIAGNOSIS

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 27/186
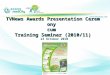
PATHOPHYSIOLOGY PATHOPHYSIOLOGY
Fig. 1: Coronal section of the brain, showing nigrostriatal pathways andlocation of selective dopaminergic degeneration in patients with
Parkinson's disease
Guttman, M. et al. CMAJ 2003;168:293-301

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 28/186
PATHOPHYSIOLOGY PATHOPHYSIOLOGY
InIn Parkinson·s disease, there is degeneration of Parkinson·s disease, there is degeneration of
dopaminergic neurondopaminergic neuron in the substantialin the substantial NigraNigra
par compacta associated with par compacta associated with lewylewy body;body;
causing decreased striatal dopamine (putamencausing decreased striatal dopamine (putamen
and caudate nucleus) level. This is thought toand caudate nucleus) level. This is thought to
be related tobe related to mitochondrialmitochondrial DNA dysfunction.DNA dysfunction.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 29/186
EPIDEMIOLOGY EPIDEMIOLOGY
PREVALENCE:PREVALENCE:
Worldwide Worldwide, based on the available prevalence, based on the available prevalence
studies, there are likely more than 6 Millionstudies, there are likely more than 6 Million
people with PD. However, due to many people people with PD. However, due to many people
with PD remaining undiagnosed, there may be with PD remaining undiagnosed, there may be
millions more. In China alone there are moremillions more. In China alone there are more
than 1.7Million people with PD.than 1.7Million people with PD.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 30/186
EPIDEMIOLOGY EPIDEMIOLOGY
DecreasingDecreasing orderorder of of prevalence prevalence ::
Amish Amish community>Brescia>Nebraska,>community>Brescia>Nebraska,> PersiaPersia
ByBy countrycountry per per 100100,,000000 of of population population
USA USA--329329--107107,, Japan Japan 193193--7676««NigeriaNigeria 6767««««KoreaKorea
1919,, EthiopiaEthiopia 77
PrevalencePrevalence of of PS/PDPS/PD isis risingrising slowlyslowly with with agingaging
population population

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 31/186
EPIDEMIOLOGY EPIDEMIOLOGY
INCIDENCEINCIDENCE RATESRATES
Sweden 22.5Sweden 22.5--7.9>7.9>faroesfaroes Island>US A 20.3Island>US A 20.3--13.013.0
«««««««.England 12««««.. Libya 45.«««««««.England 12««««.. Libya 45.
AGE AGE DISTRIBUTION:DISTRIBUTION:
InIn 1875, Henri1875, Henri HuchaudHuchaud(1844(1844--1911) detailed the first1911) detailed the first
case Juvenile Parkinson·s disease. He described a 3case Juvenile Parkinson·s disease. He described a 3
year year old who had all the clinical features of PD.old who had all the clinical features of PD.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 32/186
EPIDEMIOLOGY EPIDEMIOLOGY
The The youngest reported case of PD. The youngest reported case of PD. The
youngest reported case of PD since then is that youngest reported case of PD since then is that
of a 10 year old girl from Oklahoma whoof a 10 year old girl from Oklahoma who
showed her first symptoms of PD at only 2yearsshowed her first symptoms of PD at only 2years
old. However, it·s very uncommon for peopleold. However, it·s very uncommon for people
under the age of 30 to develop PD.under the age of 30 to develop PD.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 33/186
EPIDEMIOLOGY EPIDEMIOLOGY
PDPD usually occurs when people are significantlyusually occurs when people are significantly
older than that and becomes increasingly moreolder than that and becomes increasingly more
common withcommon with age.age.
The The average age at which symptoms usuallyaverage age at which symptoms usually
begin differs from country to country, with thebegin differs from country to country, with theoldest average onset being in Sweden 65.6 andoldest average onset being in Sweden 65.6 and
Estonia 66.9.Estonia 66.9.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 34/186
EPIDEMIOLOGY EPIDEMIOLOGY
InIn Nigeria,Nigeria, meanmean ageage of of onsetonset forfor idiopathicidiopathic
PDPD was was 5555..66 years years (Osuntokun,(Osuntokun, 19791979))
RecentlyRecently,, meanmean ageage of of onsetonset forfor PDPD inin
NigeriaNigeria was was discovereddiscovered toto bebe 6161..55 years years
(Okubadejo(Okubadejo etet alal..,, 20102010))

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 35/186
EPIDEMIOLOGY EPIDEMIOLOGY
There There isis likelihoodlikelihood of of Parkinson·sParkinson·s diseasedisease
increasingincreasing sharplysharply atat thethe ageage of of 6060,, andand peaks peaks inin
thosethose agedaged 8585--8989 years years oldold..
The The likelihoodlikelihood of of developingdeveloping PDPD startsstarts toto declinedecline
atat 9090 years years of of ageage andand reducesreduces eveneven furtherfurther afterafter
thatthat PDPD isis very very rarerare amongstamongst thethe very very oldold--thosethose
people people overover 100100 andand eveneven inin thosethose people people overover 110110
toto 119119 years years oldold..

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 36/186
EPIDEMIOLOGY EPIDEMIOLOGY
GENDER GENDER DISTRIBUTIONDISTRIBUTION
The The ratioratio of of malesmales toto femalesfemales differsdiffers aa lotlot according according toto thethe
country country.. There There isis aa stark stark contrastcontrast betweenbetween aa clearclear MaleMale dominancedominance inin
NigeriaNigeria andand Japan Japan where where Women Women dominatedominate inin PDPD..
RATIORATIO OFOF MENMEN TO TO FEMALEFEMALE::
NigeriaNigeria 33..33,, Tanzania Tanzania 22..7272,, UU..SS.. A A 11..9191--11..00 ee..tt..cc

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 37/186
EPIDEMIOLOGY EPIDEMIOLOGY
RACIALRACIAL DIFEFRENCESDIFEFRENCES::
The The risk risk of of PDPD increasesincreases according according toto HairHair
colourcolour.. PeoplePeople with with Black Black hairhair were were foundfound toto bebe
leastleast proneprone toto PDPD..
PeoplePeople with with brownbrown hairhair areare 4040%% moremore likely likely totodevelopdevelop PDPD.. And, And, thosethose with with blondeblonde hairhair 6060%% moremore
likely likely toto developdevelop PDPD..

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 38/186
EPIDEMIOLOGY EPIDEMIOLOGY
Worst Worst atat risk risk areare peoplepeople with with RedRed hairhair which which areare twicetwice atat
risk risk.. PDPD andand hairhair colourcolour shareshare somesome biochemistry biochemistry..
OCCUPATIONALOCCUPATIONAL DIFFERENCESDIFFERENCESPDPD isis farfar moremore commoncommon amongstamongst Welders Welders.. PrevalencePrevalence isis
significantly significantly higherhigher amongstamongst Physicians,Physicians, Dentist,Dentist, Teaches, Teaches,
Lawyers,Lawyers, Scientists,Scientists, andand ReligionReligion--relatedrelated jobsjobs..

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 39/186
CLINICALCLINICAL PRESENTATION OFPRESENTATION OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
N A TUR AL COURSE OF P ARKINSON·S DISE ASEN A TUR AL COURSE OF P ARKINSON·S DISE ASE
RelativelyRelatively little is known about the natural course of little is known about the natural course of
PD. Although always progressive, the natural course isPD. Although always progressive, the natural course is
very variable. (Poewe, 1998). The first symptoms are very variable. (Poewe, 1998). The first symptoms are
usually unilateral. (Olanow, et al., 2001usually unilateral. (Olanow, et al., 2001).). Around three Around three
years after the first symptoms present, it typically years after the first symptoms present, it typically
develops into a bilateral disorder, usually still withdevelops into a bilateral disorder, usually still with
intact balanceintact balance.. (Muller, et al., 2000)(Muller, et al., 2000)

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 40/186
CLINICALCLINICAL PRESENTATION OFPRESENTATION OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
ProblemsProblems with balance develop about two to three with balance develop about two to three
years later, although some patients reach this stage years later, although some patients reach this stage
only seventeen years after the start of the disease.only seventeen years after the start of the disease.
(Muller, et al., 2000) Recurrent falling starts on(Muller, et al., 2000) Recurrent falling starts on
average ten years after the first symptoms. (average ten years after the first symptoms. ( Wenning Wenning,,
et al., 1999) Eventually, nearly all patients will haveet al., 1999) Eventually, nearly all patients will have
impaired balance and will fall repeatedlyimpaired balance and will fall repeatedly..

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 41/186
CLINICALCLINICAL PRESENTATION OFPRESENTATION OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
This This formsforms aa threatthreat toto qualityquality of of lifelife.. (Schrag,(Schrag, etet alal..,,
20002000)) Initially,Initially, patients patients with with balancebalance problems problems cancan
standstand andand walk walk onon theirtheir own,own, butbut onon averageaverage afterafter
eighteight years, years, fallingfalling becomes,becomes, inin combinationcombination with with thethe
otherother symptoms,symptoms, aa moremore severesevere problem problem.. EventuallyEventually
thethe balancebalance impairmentimpairment cancan becomebecome soso severesevere thatthat thethe
patient patient isis permanently permanently confinedconfined toto aa wheelchair wheelchair oror
bed,bed, if if hehe hashas nono helphelp of of othersothers..

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 42/186
CLINICALCLINICAL PRESENTATION OFPRESENTATION OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
LessLess than five percent of patients with PD arethan five percent of patients with PD are
confined to a wheelchair or bed eventually (Globalconfined to a wheelchair or bed eventually (Global
Parkinson Disease Survey Steering Committee, 2002).Parkinson Disease Survey Steering Committee, 2002).
In later stages non motor symptoms may arise, suchIn later stages non motor symptoms may arise, such
as dementia. In geriatric patients PD is oftenas dementia. In geriatric patients PD is often
accompanied by depression.accompanied by depression.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 43/186
CLINICALCLINICAL PRESENTATION OFPRESENTATION OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
1)1) TREMORS: TREMORS:
(a)(a) It consists of regular , rhythmic , alternate contractionIt consists of regular , rhythmic , alternate contraction
antagonist & agonist muscles @ 4antagonist & agonist muscles @ 4--6 times / second.6 times / second.
(b)(b) The tremors occurs due to uninhibited activity of the basal The tremors occurs due to uninhibited activity of the basal
gangliaganglia--corticocortico--thalamus circuit as a result of degeneration of thalamus circuit as a result of degeneration of
the striatonigral pathway.the striatonigral pathway.
(c)(c) It is a rhythmic involuntary movement normally affectingIt is a rhythmic involuntary movement normally affecting
the limbs.the limbs.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 44/186
CLINICALCLINICAL PRESENTATION OFPRESENTATION OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
d)d) It is the 1It is the 1stst complain of the patient but in some patientcomplain of the patient but in some patient
Bradykinesia is usually the first recognized symptom.Bradykinesia is usually the first recognized symptom.
e)e) Resting tremor present mainly PIN / PILL rolling type as likeResting tremor present mainly PIN / PILL rolling type as like
pin / pill rolls between the thumb & index finger. pin / pill rolls between the thumb & index finger.
f)f) Frequency is 4Frequency is 4--6 times / second in early stage & 66 times / second in early stage & 6--8 times/8 times/
second in later stage.second in later stage.
g)g) Maximal at periphery & affects the arm more frequentlyMaximal at periphery & affects the arm more frequently
than the leg.than the leg.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 45/186
CLINICALCLINICAL PRESENTATION OFPRESENTATION OF
PARKINSON·S DISEASEPARKINSON·S DISEASEh)h) Tremor is increased by stress & disappeared during sleep & Tremor is increased by stress & disappeared during sleep &
goal directed movements.goal directed movements.
i)i) The hand which is most affected assumes a posture of flexion The hand which is most affected assumes a posture of flexion
of the MCP joints with extension of the more distal joints.of the MCP joints with extension of the more distal joints.
2) RIGIDITY 2) RIGIDITY
a)a) Rigidity is defined as resistance to passive motion that is notRigidity is defined as resistance to passive motion that is not
velocity dependent. velocity dependent.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 46/186
CLINICALCLINICAL PRESENTATION OFPRESENTATION OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
b)b) It is manifested as co contraction of agonist & antagonistIt is manifested as co contraction of agonist & antagonist
muscles due to an increase in the supraspinal influences onmuscles due to an increase in the supraspinal influences on
the normal spinal system causing increase tone in the agonistthe normal spinal system causing increase tone in the agonist
& the antagonist.There is an increased discharge of gamma& the antagonist.There is an increased discharge of gamma
motor neuronsmotor neurons..
c)c) The patient usually complains of rigidity as a sensation of The patient usually complains of rigidity as a sensation of
heaviness or stiffness of the limbsheaviness or stiffness of the limbs..
d)d) Present in almost all cases of PDPresent in almost all cases of PD

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 47/186
CLINICALCLINICAL PRESENTATION OFPRESENTATION OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
e)e) Cog wheel type rigidity is present. There is intermittentCog wheel type rigidity is present. There is intermittent
resistance throughout ROM.resistance throughout ROM.
Lead pipe rigidity is also seen in some cases. There isLead pipe rigidity is also seen in some cases. There is
constant resistance throughout ROM.constant resistance throughout ROM.
f)f) It affects proximal muscles first, mainly shoulders & neck andIt affects proximal muscles first, mainly shoulders & neck and
then progress to face & extremities and then the whole body.then progress to face & extremities and then the whole body.
g)g) As the disease progresses ; Rigidity becomes more severe As the disease progresses ; Rigidity becomes more severe..
h)h) Mental concentration & Emotional tension may increase theMental concentration & Emotional tension may increase the
amount of rigidity presentamount of rigidity present..

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 48/186
CLINICALCLINICAL PRESENTATION OFPRESENTATION OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
i)i) Rigidity decreases the ability of patients to move easily. ForRigidity decreases the ability of patients to move easily. For
e.g.; loss of bed mobility , loss of reciprocal arm swing duringe.g.; loss of bed mobility , loss of reciprocal arm swing during
gaitgait..
j)j) Prolonged rigidity results in decreased available ROM &Prolonged rigidity results in decreased available ROM &
serious secondary complications of contracture & posturalserious secondary complications of contracture & postural
deformity.deformity.
k)k) Rigidity also has a direct impact on increasing RestingRigidity also has a direct impact on increasing Resting
Energy Expenditure (REE) & fatigue levelsEnergy Expenditure (REE) & fatigue levels..

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 49/186
CLINICALCLINICAL PRESENTATION OFPRESENTATION OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
3) BRADYKINESIA 3) BRADYKINESIA
a)a) Bradykinesia refers to slowness & difficulty in maintainingBradykinesia refers to slowness & difficulty in maintaining
movements. It is theoretically presumed that it could bemovements. It is theoretically presumed that it could bebecause of difficulty to the basal ganglia to integrate sensorybecause of difficulty to the basal ganglia to integrate sensory
information.information.
b)b) Movements are typically reduced in speed, range & amplitudeMovements are typically reduced in speed, range & amplitude; termed hypokinesia.; termed hypokinesia.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 50/186
CLINICALCLINICAL PRESENTATION OFPRESENTATION OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
c)c) Patient with PD typically demonstrate micrographia ; anPatient with PD typically demonstrate micrographia ; an
abnormally small hand writing that is difficult to read.abnormally small hand writing that is difficult to read.
d)d) Patient feels difficulties in ADL such as bathing, dressing,Patient feels difficulties in ADL such as bathing, dressing,
rising from a chair, turning over in bed, loss of dexterity &rising from a chair, turning over in bed, loss of dexterity &
making buttoning etc.making buttoning etc.
e)e) Patient experiences difficulty in integrating two motorPatient experiences difficulty in integrating two motor
programmes at the same time.(dual tasking) programmes at the same time.(dual tasking)
f)f) Patient feels hesitation on initiation of movements & earlyPatient feels hesitation on initiation of movements & early
fatigue.fatigue.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 51/186
CLINICALCLINICAL PRESENTATION OFPRESENTATION OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
4) POSTURAL INSTABILITY 4) POSTURAL INSTABILITY
a)a) Simians posture or Stooped postureSimians posture or Stooped posture..
b)b) Head protruded forward , flexion at neck , trunk , elbow , hipHead protruded forward , flexion at neck , trunk , elbow , hip
& knee.& knee.
c)c) Tandem stance : Tandem stance :-- walking on a single line with narrow BOS. walking on a single line with narrow BOS.
d)d) Balance is poor & patient fall if encounters even minorBalance is poor & patient fall if encounters even minor
postural perturbation ( a slight push ) due to loss of postural postural perturbation ( a slight push ) due to loss of postural
reflexes.reflexes.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 52/186
CLINICALCLINICAL PRESENTATION OFPRESENTATION OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
5) GAIT5) GAIT
a)a) Parkinsonian gait / Freezing / Festinating / Shuffling / ToeParkinsonian gait / Freezing / Festinating / Shuffling / Toe
² ²heel / Hurrying gait.heel / Hurrying gait.
b)b) Patient takes small steps on walkingPatient takes small steps on walking..
c)c) Patient feels difficulty in initiating movement & to stopPatient feels difficulty in initiating movement & to stop
walking once started. walking once started.
d)d) There is loss of normal heel toe progression. The toe strikes There is loss of normal heel toe progression. The toe strikes
first.first.
e)e) Loss of arm swing & pelvic rotation.Loss of arm swing & pelvic rotation.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 53/186
CLINICALCLINICAL PRESENTATION OFPRESENTATION OF
PARKINSON·S DISEASEPARKINSON·S DISEASEf)f) The forward leaning of the trunk moves the body·s COG forward The forward leaning of the trunk moves the body·s COG forward
thus causing the patient to hasten his/her pace in order to catchthus causing the patient to hasten his/her pace in order to catch
up COG.up COG.
g)g) Stride length decreases & speed increased therefore called asStride length decreases & speed increased therefore called as
festinating gait.festinating gait.
h)h) Stance phase & double support time are lengthened while theStance phase & double support time are lengthened while the
period of single limb support is shortened. period of single limb support is shortened.
i)i) Turning or changing direction is particularly difficult. Turning or changing direction is particularly difficult.
j)j) Patient are able to stop only when they come in contact with anPatient are able to stop only when they come in contact with an
ob ect or a wall.ob ect or a wall.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 54/186
CLINICALCLINICAL PRESENTATION OFPRESENTATION OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
INDIRECT IMPAIREMENTS & COMPLICATIONSINDIRECT IMPAIREMENTS & COMPLICATIONS
1) MASKED FACE1) MASKED FACE
a)a) Lack of facial expression.Lack of facial expression.
b)b) Subsequent loss of blinkingSubsequent loss of blinking..
c)c) Smiling may be possible only on command or volitional effort.Smiling may be possible only on command or volitional effort.
d)d) This can have a significant impact on social interaction & This can have a significant impact on social interaction &
social disability.social disability.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 55/186
CLINICAL PRESENTATION OFCLINICAL PRESENTATION OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
2) POVERTY OF MOVEMENT2) POVERTY OF MOVEMENT
a)a) Rotational movement are reduced, resulting in movementsRotational movement are reduced, resulting in movements
that are basically uniplanar (in one plane of motion ) e.g.;that are basically uniplanar (in one plane of motion ) e.g.;
flexionflexion² ²extension in sagital plane.extension in sagital plane.
b)b) There is an overall decrease in total number of There is an overall decrease in total number of
movementsmovements..c)c) Movement impoverishment can lead to mental fatigue &Movement impoverishment can lead to mental fatigue &
loss of motivation.loss of motivation.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 56/186
CLINICAL PRESENTATION OFCLINICAL PRESENTATION OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
3) FATIGUE3) FATIGUE
a)a) In a patient of PD fatigue is one of the symptom.In a patient of PD fatigue is one of the symptom.
b)b) The patient has difficulty in sustaining activity & experiences The patient has difficulty in sustaining activity & experiencesincreasing weakness.increasing weakness.
c)c) Repetitive motor acts may start out strong but decrease inRepetitive motor acts may start out strong but decrease in
strength as the activity progresses.strength as the activity progresses.
d)d) The 1 The 1stst few words spoken may be loud & strong but diminishfew words spoken may be loud & strong but diminish
rapidly as speech progresses.(palilalia)rapidly as speech progresses.(palilalia)

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 57/186
CLINICAL PRESENTATION OFCLINICAL PRESENTATION OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
4) MUSCULOSKELETAL CHANGES4) MUSCULOSKELETAL CHANGES
a)a) Patient shows the effects of generalized musculoskeletalPatient shows the effects of generalized musculoskeletal
deconditioning.deconditioning.
b)b) The more chronic & generalized the disease becomes , the The more chronic & generalized the disease becomes , the
greater the level of muscle weakness & fatigue.greater the level of muscle weakness & fatigue.
c)c) Loss of flexibility.Loss of flexibility.
d)d) Lack of movement in any body segment leads to contractureLack of movement in any body segment leads to contracture
development of both contractile & nondevelopment of both contractile & non --contractile tissue.contractile tissue.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 58/186
CLINICAL PRESENTATION OFCLINICAL PRESENTATION OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
e)e) Contractures mainly develops in hip & knee flexors, hipContractures mainly develops in hip & knee flexors, hip
rotators & adductors, plantar flexors, dorsal spine & neck rotators & adductors, plantar flexors, dorsal spine & neck
flexors, shoulders adductors & internal rotators, and elbow flexors, shoulders adductors & internal rotators, and elbow
flexors.flexors.
f)f) Kyphosis is the most common postural deformity.Kyphosis is the most common postural deformity.
g)g) Some pt. may develop Scoliosis from leaning consistently toSome pt. may develop Scoliosis from leaning consistently toone side when sitting or walking.one side when sitting or walking.
h)h) Scoliosis generally results from unequal distribution of rigidityScoliosis generally results from unequal distribution of rigidity
in the trunk.in the trunk.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 59/186
CLINICAL PRESENTATION OFCLINICAL PRESENTATION OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
i)i) Older patient with reduced activity levels & poor diet are likelyOlder patient with reduced activity levels & poor diet are likely
to develop osteoporosis.to develop osteoporosis.
5) S W ALLO WING DYSFUNCTION5) S W ALLO WING DYSFUNCTIONa)a) Dysphagia ,impaired swallowing, is present in 50Dysphagia ,impaired swallowing, is present in 50--90 % of pt.90 % of pt.
b)b) Dysphagia can lead to choking or aspirationDysphagia can lead to choking or aspiration pnuemonia pnuemonia &&
impaired nutrition.impaired nutrition.
c)c) Dysphagia is the result of Dysphagia is the result of rigidity,reducedrigidity,reduced mobility& restrictedmobility& restricted
range of movement.range of movement.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 60/186
CLINICAL PRESENTATION OFCLINICAL PRESENTATION OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
d)d) Patient experiences problems in all four stages of swallowing;Patient experiences problems in all four stages of swallowing;
oral preparatory, oral, pharyngeal & esophagealoral preparatory, oral, pharyngeal & esophageal..
e)e) Patient typically experiences excessive drooling (sialorrhea) asPatient typically experiences excessive drooling (sialorrhea) as
a result of increased salivary production & decreaseda result of increased salivary production & decreased
spontaneous swallowing.spontaneous swallowing.
6) COMMUNICATION DYSFUNCTION6) COMMUNICATION DYSFUNCTION
a)a) Speech is impaired in 50Speech is impaired in 50-- 73 % of patient.73 % of patient.
b)b) Speech difficulties are also result of rigidity & bradykinesiaSpeech difficulties are also result of rigidity & bradykinesia..

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 61/186
CLINICAL PRESENTATION OFCLINICAL PRESENTATION OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
c)c) Hypokinetic Dysarthria; which is characterised by decreasedHypokinetic Dysarthria; which is characterised by decreased
volume , monotone or volume , monotone or monopitchmonopitch speech, imprecise orspeech, imprecise or
distorted disarticulation & uncontrolled speech rate.distorted disarticulation & uncontrolled speech rate.
d)d) Patients experiences reduced mobility , restricted range of Patients experiences reduced mobility , restricted range of
movement& uncontrolled rate of movement of musclesmovement& uncontrolled rate of movement of muscles
controlling respiration , phonation , resonation & articulation.controlling respiration , phonation , resonation & articulation.
7) VISUAL & SENSORIMOTOR DISTURBANCES7) VISUAL & SENSORIMOTOR DISTURBANCES
a)a) Conjugate gaze & saccadic eye movements may also beConjugate gaze & saccadic eye movements may also be
impairedimpaired..

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 62/186
CLINICAL PRESENTATION OFCLINICAL PRESENTATION OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
b)b) Visual disturbances are common in PD. These can include Visual disturbances are common in PD. These can include
blurring of vision & difficulty in reading which can not beblurring of vision & difficulty in reading which can not be
corrected by glasses.corrected by glasses.c)c) Eye movements may have a jerky & cog wheeling quality.Eye movements may have a jerky & cog wheeling quality.
d)d) Pupillary abnormalities are also possible with decreased reflexPupillary abnormalities are also possible with decreased reflex
responses to light & nociceptive stimuli.responses to light & nociceptive stimuli.
e)e) Akathisia; it is often described as painful and interferes with Akathisia; it is often described as painful and interferes with
relaxation & sleeprelaxation & sleep..

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 63/186
CLINICAL PRESENTATION OFCLINICAL PRESENTATION OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
f)f) 50% patient experiences50% patient experiences paresthesias paresthesias & pain. This can include& pain. This can include
sensations of numbness ,tingling, abnormal temperature &sensations of numbness ,tingling, abnormal temperature &
pain that is cramp pain that is cramp--like & poorly localizedlike & poorly localized..
g)g) Postural stress syndromePostural stress syndrome..
88) COGNITIVE DYSFUNCTION) COGNITIVE DYSFUNCTIONa)a) Dementia occurs in approximately 1/3Dementia occurs in approximately 1/3rdrd of the patients withof the patients with
PD.PD.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 64/186
CLINICAL PRESENTATION OFCLINICAL PRESENTATION OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
b)b) BradyphreniaBradyphrenia, a disorder of intellectual function, is common in, a disorder of intellectual function, is common in
pt. It is characterised by a slowing of thought processes with pt. It is characterised by a slowing of thought processes with
lack of concentration & attentionlack of concentration & attention..c)c) Patient May also demonstrate learning deficits.Patient May also demonstrate learning deficits.
d)d) Perceptual deficits also present.Perceptual deficits also present.
e)e) Deficits have been reported in vertical perception, topographicDeficits have been reported in vertical perception, topographic
orientation, body scheme and spatial relations.orientation, body scheme and spatial relations.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 65/186
CLINICAL PRESENTATION OFCLINICAL PRESENTATION OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
9) BEHAVIOURAL DYSFUNCTION9) BEHAVIOURAL DYSFUNCTION
a)a) Depression is the most common, occurring in25Depression is the most common, occurring in25--40% of patient.40% of patient.
b)b) Patient may demonstrate symptoms of major depressionPatient may demonstrate symptoms of major depression,including apathy, passivity, loss of ambition or enthusiasm &,including apathy, passivity, loss of ambition or enthusiasm &
changes in appetite, sleep and dependency. Suicidal thoughtschanges in appetite, sleep and dependency. Suicidal thoughts
may be presentmay be present..
c)c) Dysrhythmic disorder characterised by variability in dysphoricDysrhythmic disorder characterised by variability in dysphoric
mood, or typical depression characterised by intermittentmood, or typical depression characterised by intermittent
episodes of severe anxiety.episodes of severe anxiety.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 66/186
CLINICAL PRESENTATION OFCLINICAL PRESENTATION OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
d)d) Drug related psychoses can occur.Drug related psychoses can occur.
10) AUTONOMIC DYSFUNCTION10) AUTONOMIC DYSFUNCTION
a)a) DysautonomiaDysautonomia ; autonomic nervous system dysfunction occurs; autonomic nervous system dysfunction occursin patient.in patient.
b)b) Commons problems includes excessiveCommons problems includes excessive perspiration,greasy perspiration,greasy
skin,increasedskin,increased salivation,thermoregulatorysalivation,thermoregulatory
abnormalities(including uncomfortable sensation of heat orabnormalities(including uncomfortable sensation of heat or
cold)cold)..

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 67/186
CLINICAL PRESENTATION OFCLINICAL PRESENTATION OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
c)c) Bladder dysfunction includes urinary frequency, urgency &Bladder dysfunction includes urinary frequency, urgency &
nocturia.nocturia.
d)d) Sexual dysfunction includes impotence.Sexual dysfunction includes impotence.
e)e) Patient have low appetites & decreased motility of the GIT.Patient have low appetites & decreased motility of the GIT.
f)f) Constipation is also problem seen in patient.Constipation is also problem seen in patient.
11) CARDIOPULMONARY DYSFUNCTION11) CARDIOPULMONARY DYSFUNCTION
a)a) Pulmonary function impairment is reported in 84% of patientsPulmonary function impairment is reported in 84% of patients..
b)b) Airway obstruction leads to pulmonary failure. Airway obstruction leads to pulmonary failure.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 68/186
CLINICAL PRESENTATION OFCLINICAL PRESENTATION OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
c)c) Orthostatic hypotension & low resting blood pressure. CardiacOrthostatic hypotension & low resting blood pressure. Cardiac
arrhythmias can also occurs as a result of Larrhythmias can also occurs as a result of L--DopaDopa ..
d)d) Bradykinetic disorganization of respiratory movements.Bradykinetic disorganization of respiratory movements.
e)e) Restrictive dysfunction due to decreased chest expansion thatRestrictive dysfunction due to decreased chest expansion that
occurs as a result of rigidity of trunk muscles, loss of occurs as a result of rigidity of trunk muscles, loss of
musculoskeletal flexibility & kyphotic posture.musculoskeletal flexibility & kyphotic posture.
f)f) Decrease in FVC , FEV1 & increase in RV , RA W (airwayDecrease in FVC , FEV1 & increase in RV , RA W (airway
resistance).resistance).

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 69/186
CLINICAL PRESENTATION OFCLINICAL PRESENTATION OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
g)g) In long standing disease, the lower extremities may exhibitIn long standing disease, the lower extremities may exhibit
circulatory changes owing to venous pooling as a result of circulatory changes owing to venous pooling as a result of
decreased mobility & prolonged sitting. Thus pt. can presentdecreased mobility & prolonged sitting. Thus pt. can present
with mild to moderate edema of the feet & ankles, which with mild to moderate edema of the feet & ankles, which
usually subsides during sleep.usually subsides during sleep.
12) SKIN INFECTIONS12) SKIN INFECTIONS
a)a) Dermatitis can occur due to increased secretion by sweat &Dermatitis can occur due to increased secretion by sweat &
sebaceous glands.sebaceous glands.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 70/186
CLINICAL PRESENTATION OFCLINICAL PRESENTATION OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
13) GLABELLAR TAP SIGN13) GLABELLAR TAP SIGN
a)a) Tapping forehead causes repetitive blinking. Tapping forehead causes repetitive blinking.
14) OLFACTORY DYSFUNCTION14) OLFACTORY DYSFUNCTIONa)a) It is present in 75It is present in 75 ² ² 90 % of patient.90 % of patient.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 71/186
PROGNOSTIC FACTOR OF PARKINSON·SPROGNOSTIC FACTOR OF PARKINSON·S
DISEASEDISEASE
According to KNGF guideline development group of According to KNGF guideline development group of
Parkinson's disease 2004, physical therapy influences physicalParkinson's disease 2004, physical therapy influences physical
inability and falling as prognostic in Parkinson·s disease.inability and falling as prognostic in Parkinson·s disease.
Jankovic et al., distinguish Jankovic et al., distinguish TREMOR DOMINANT TYPE TREMOR DOMINANT TYPE of of
Parkinson's disease andParkinson's disease and AKINETIC RIGID TYPE AKINETIC RIGID TYPE
TREMOR DOMINANT TYPE AKINETIC RIGID TYPE
1 ) Tremor is the initial symptom. Rigidity and hypokinesia are the initialsymptoms.
2 ) Process often develop more slowly. More rapid course of Parkinson·s disease in
motor and cognitive areas.
3) Characterized by problems of balance gate
and freezing.
Characterize by less frequent dominant and
cognition impairment.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 72/186
PROGNOSTIC FACTOR OF PARKINSON·SPROGNOSTIC FACTOR OF PARKINSON·S
DISEASEDISEASE
In patients of young age cognition functions and posturalIn patients of young age cognition functions and postural
reflexes often remain unimpaired.reflexes often remain unimpaired.
Patients with recurrent falls and with insufficient physicalPatients with recurrent falls and with insufficient physical
activity has an unfavourable prognosisactivity has an unfavourable prognosis..
PD is a progressive disorder but its rate of progression isPD is a progressive disorder but its rate of progression is
variable.variable.
Before LBefore L--dopa therapy 28% of pt. became severely disabled ordopa therapy 28% of pt. became severely disabled or
died with in 5 yrs of diagnosis , 61% with in 10 yrs & 83%died with in 5 yrs of diagnosis , 61% with in 10 yrs & 83%
with in 15 yrswith in 15 yrs..
PROGNOSTIC FACTOR OFPROGNOSTIC FACTOR OF

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 73/186
PROGNOSTIC FACTOR OFPROGNOSTIC FACTOR OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
Following LFollowing L--dopa therapy only 9% becamedopa therapy only 9% became
disabled or had died at 5 yrs , 21% at 10 yrs &disabled or had died at 5 yrs , 21% at 10 yrs &
37.5% at 15 yrs.37.5% at 15 yrs.
Death may occur from aspiration pneumoniaDeath may occur from aspiration pneumonia
,septicemia from UTI, decubitus ulcer or from,septicemia from UTI, decubitus ulcer or from
secondary causes like vascular disease orsecondary causes like vascular disease or
neoplasia.neoplasia.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 74/186
MANAGEMENT OF PARKINSON·SMANAGEMENT OF PARKINSON·S
DISEASEDISEASE
The The managementmanagement of of PDPD followsfollows thethe multidisciplinarymultidisciplinary approachapproach..
This This involveinvolve thethe MULTIDISCIPLINARY MULTIDISCIPLINARY TEAM TEAM thatthat includesincludes::
NeurologistNeurologist
A rehabilitation Physician A rehabilitation Physician
A physical therapist A physical therapist
An occupational therapist An occupational therapist
A speech therapist A speech therapist
A neuropsychologist A neuropsychologist
A recreational activities supervisor A recreational activities supervisor
A social work A social work
A PD specialist Nurse A PD specialist Nurse
TT

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 75/186
MANAGEMENT OF PARKINSON·S DISEASEMANAGEMENT OF PARKINSON·S DISEASE
MEDICAL THERAPY MEDICAL THERAPY

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 76/186
MEDICAL THERAPY MEDICAL THERAPY

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 77/186
MEDICAL THERAPY MEDICAL THERAPY

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 78/186
MEDICAL THERAPY MEDICAL THERAPY

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 79/186
MANAGEMENT OF PARKINSON·SMANAGEMENT OF PARKINSON·S
DISEASEDISEASE
MEDICAL THERAPY MEDICAL THERAPY
Treatment algorithm for the Treatment algorithm for the
management of the earlymanagement of the earlystages of Parkinson·sstages of Parkinson·s
disease. As shown below disease. As shown below

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 80/186

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 81/186
MANAGEMENT OF PARKINSON·SMANAGEMENT OF PARKINSON·S
DISEASEDISEASE
SURGICAL THERAPY SURGICAL THERAPY
A. A. Stereotactic surgery is done on the basal ganglia by ruling outStereotactic surgery is done on the basal ganglia by ruling out
part of the region ( part of the region (--tomy) as in:tomy) as in:
Pallidotomy: clearing of destructive lesion in globus pallidusPallidotomy: clearing of destructive lesion in globus pallidus
internus, decrease dyskinesia.internus, decrease dyskinesia.
Thalamotomy: Clearing of destructive lesion in the ventral Thalamotomy: Clearing of destructive lesion in the ventralintermedius nucleus of the thalamus, decreases tremor.intermedius nucleus of the thalamus, decreases tremor.
Stereotactic surgery started in 1950 before LevoStereotactic surgery started in 1950 before Levo--dopa not in use.dopa not in use.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 82/186
SURGICAL THERAPY SURGICAL THERAPY
B.B. Deep Brains Stimulator(DBS) : started in 1997, stimulationDeep Brains Stimulator(DBS) : started in 1997, stimulation
takes place by implantation of electrode in the brain,takes place by implantation of electrode in the brain,
specifically in ventral intermedius nucleus of the thalamus to aspecifically in ventral intermedius nucleus of the thalamus to a
pacemaker. pacemaker.
Complications might occur as a consequence:Complications might occur as a consequence:
By intervention itself(by damaging the surrounding tissue)By intervention itself(by damaging the surrounding tissue)
The applied equipment( e.g. infection) The applied equipment( e.g. infection)
The lesion or stimulation (among others falling problems The lesion or stimulation (among others falling problems
paraesthesia and headache). paraesthesia and headache).

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 83/186
SURGICAL THERAPY SURGICAL THERAPY
C.C. Transplantation technique: grafting of foetal cells, auto Transplantation technique: grafting of foetal cells, auto
transplantation with patient·s own adrenal medullary cells.transplantation with patient·s own adrenal medullary cells.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 84/186
MOTOR FEATURES OF PDMOTOR FEATURES OF PD
Initiation problemsInitiation problems
movements under scaledmovements under scaled motor instabilitymotor instability
slowingslowing
deterioration with simultaneous tasksdeterioration with simultaneous tasks Tremor Tremor
NONNON MOTOR FEATURES OFMOTOR FEATURES OF

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 85/186
NONNON--MOTOR FEATURES OFMOTOR FEATURES OF
PDPD Sleep:Sleep:
BowelsBowels
BladderBladder
PainPain
Postural hypotension *Postural hypotension *
Sexual dysfunctionSexual dysfunction
Sweating Sweating
MANAGEMENT OFMANAGEMENT OF

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 86/186
MANAGEMENT OFMANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
PHYSIOTHERAPY PHYSIOTHERAPY
Physiotherapy intervention is broadly dividedPhysiotherapy intervention is broadly divided
into two processes:into two processes:
Diagnostic processDiagnostic process
Therapeutic process (KNGF, 2004) Therapeutic process (KNGF, 2004)
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 87/186
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
DIAGNOSTIC PROCESSDIAGNOSTIC PROCESS
This involves ASSESSMENTS and CLINICAL IMPRESSION. This involves ASSESSMENTS and CLINICAL IMPRESSION.
Subjective AssessmentSubjective Assessment
Objective AssessmentObjective Assessment
Analysis of finding Analysis of finding
Plan of treatmentPlan of treatment
Goals of treatmentGoals of treatment
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 88/186
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
Therapeutic process Therapeutic process
This involves: This involves:
Means of treatmentMeans of treatment
Evaluation and follow upEvaluation and follow up
ReportingReporting
The objectives or aims of physiotherapy are based on the The objectives or aims of physiotherapy are based on the
outcome from these two processes.outcome from these two processes.
For a patient with PD, the major objectives of physiotherapy are:For a patient with PD, the major objectives of physiotherapy are:
To improve the quality of life To improve the quality of life
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 89/186
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
To maintain the patient·s independence, safety, and well being. To maintain the patient·s independence, safety, and well being.
To improve functional activity. To improve functional activity.
To reduce or delay limitation in activities (disability). To reduce or delay limitation in activities (disability).
ASSESSMENT ASSESSMENT
REFERRALREFERRAL
Early referral (immediately after diagnosis) to a physicalEarly referral (immediately after diagnosis) to a physicaltherapist is recommended to prevent or decrease complicationtherapist is recommended to prevent or decrease complication
as a result of falls and inactivity. (Plant et al., 2000; Morris,as a result of falls and inactivity. (Plant et al., 2000; Morris,
2000;2000; ChessonChesson, 1998 ), 1998 )
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 90/186
PARKINSON·S DISEASEPARKINSON·S DISEASE
HenvelHenvel et al., stated the following information needed from theet al., stated the following information needed from the
referring physician:referring physician:
Name, date of birth and address of the patient.Name, date of birth and address of the patient.
Date of referralDate of referral
DiagnosisDiagnosis
Is other forms of parkinsonism excluded?Is other forms of parkinsonism excluded?
CoCo--morbiditymorbidity
Course of the health problemCourse of the health problem
Reason for referralReason for referral
Name, address and signature of the physicName, address and signature of the physic
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 91/186
PARKINSON·S DISEASEPARKINSON·S DISEASE
HISTORY TAKINGHISTORY TAKING
To get an accurate picture of the patient problem. To get an accurate picture of the patient problem.
Patient specific complaints questionnaire; for performance of Patient specific complaints questionnaire; for performance of
activities and assessment of the treatment goal .it determinesactivities and assessment of the treatment goal .it determines
the functional status of individual patient.the functional status of individual patient.
history of falling questionnairehistory of falling questionnaire
freezing of gait questionnaire (FOG): This is used for patientfreezing of gait questionnaire (FOG): This is used for patient who have recently experienced that their feet seemed glued or who have recently experienced that their feet seemed glued or
stocked to the ground.stocked to the ground.
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 92/186
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE For inventory of evaluation of falling or near fallingFor inventory of evaluation of falling or near falling
fall efficacy scalefall efficacy scale
fall diaryfall diary
LASA physical activity questionnaire; measure physicalLASA physical activity questionnaire; measure physical
activity of the elderly.activity of the elderly.
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 93/186
PARKINSON·S DISEASEPARKINSON·S DISEASE
Analysis to formulate the objective to be tested: Analysis to formulate the objective to be tested:
Based on the information obtained while taking the medicalBased on the information obtained while taking the medical
history, a number of problems is formulated, these are to behistory, a number of problems is formulated, these are to be
tested in physical examination.tested in physical examination.
Possible objective are:Possible objective are:
1.1. Physical capacityPhysical capacity
2.2. Transfer Transfer
3.3. Reaching and graspingReaching and grasping
4.4. Balance and gaitBalance and gait
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 94/186
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
Physical ExaminationPhysical ExaminationPhysical therapist should determine if the patient is in ON OR Physical therapist should determine if the patient is in ON OR
OFF period. For structured physical examination.OFF period. For structured physical examination.
¶QUICK REFERENCE CARD· CAN BE USE.¶QUICK REFERENCE CARD· CAN BE USE.
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 95/186
PARKINSON·S DISEASEPARKINSON·S DISEASE
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 96/186
PARKINSON·S DISEASEPARKINSON·S DISEASE
PHYSIOTHERAPY MANAGEMENT OF PARKINSON·SPHYSIOTHERAPY MANAGEMENT OF PARKINSON·S

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 97/186
DISEASEDISEASE
NEUROLOGICAL ASSESSMENTNEUROLOGICAL ASSESSMENT
(1)(1) COGNITION :COGNITION :-- memory function , conceptual reasoning ,memory function , conceptual reasoning ,
problem solving ability , attention and concentration are problem solving ability , attention and concentration are
reduced.reduced.
Assessment instrument Assessment instrument ² ² Mini Mental Status Exam (MMSE).Mini Mental Status Exam (MMSE).
2)2) AFFECTIVE & PSYCHOSOCIAL FUNCTIONING : AFFECTIVE & PSYCHOSOCIAL FUNCTIONING :--
stress, anxiety , sadness , apathy , passivity , insomnia ,stress, anxiety , sadness , apathy , passivity , insomnia ,
aprexiaaprexia , wt. loss , inactivity , suicidal thoughts may present., wt. loss , inactivity , suicidal thoughts may present.
Assessment instrument Assessment instrument ² ² Geriatric Depressions ScaleGeriatric Depressions Scale
Beck Depression Inventory.Beck Depression Inventory.
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 98/186
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
(3) VISUAL FUNCTION:(3) VISUAL FUNCTION:--
Visual acuity, peripheral vision, accommodation, light & dark Visual acuity, peripheral vision, accommodation, light & dark
adaptation are reduced.adaptation are reduced.
Depth perception, blurring of vision, cataract, glaucoma, mayDepth perception, blurring of vision, cataract, glaucoma, may
present. present.
Senile macular degeneration, diabetic retinopathy,Senile macular degeneration, diabetic retinopathy,
homonymoushomonymous hemianopiahemianopia may present.may present.
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 99/186
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
(4) DYSPHAGIA & SPEECH IMPAIREMENT:(4) DYSPHAGIA & SPEECH IMPAIREMENT:--
Dysphagia , sialorrhea ( drooling) present.Dysphagia , sialorrhea ( drooling) present.
Hypokinetic dysarthria .Hypokinetic dysarthria .
Mutism.Mutism.
Assessment instruments: The verbal learning test. Assessment instruments: The verbal learning test.
The verbal comprehension test. The verbal comprehension test.
(5) MUSCLE PERFORMANCE:(5) MUSCLE PERFORMANCE:--
SpasticitySpasticity
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 100/186
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
Strength reduced.Strength reduced.
Endurance decreased.Endurance decreased.
Assessment Instrument: Manual Muscle grading Assessment Instrument: Manual Muscle grading
Modified Ashworth scale.Modified Ashworth scale.
Isokinetic Dynamometers.Isokinetic Dynamometers.
Hand Held Dynamometers.Hand Held Dynamometers.
(6) RIGIDITY:(6) RIGIDITY: --
Present in trunk, neck, extremities & face.Present in trunk, neck, extremities & face.
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 101/186
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
(7) BRADYKINESIA:(7) BRADYKINESIA: --
Slowness of movement.Slowness of movement.
Increased Reaction Time (RT).Increased Reaction Time (RT).
Increased Movement Time (MT).Increased Movement Time (MT).
Assessment instrument : Timed test for Rapid Alternating Assessment instrument : Timed test for Rapid Alternating
Movement (RAM).Movement (RAM).EMG for RT & MT.EMG for RT & MT.
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 102/186
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
(8) JOINT RANGE OF MOTION:(8) JOINT RANGE OF MOTION: --
AROM & PROM both decreased. AROM & PROM both decreased.
Loss of hip & knee extension, shoulder flexion, elbow Loss of hip & knee extension, shoulder flexion, elbow
extension, dorsal spine & neck extension and axial rotation of extension, dorsal spine & neck extension and axial rotation of
spine.spine.
Assessment instrument: Assessment instrument: GoniometerGoniometer
(9) TREMORS :(9) TREMORS :--
Resting tremors.Resting tremors.
Mainly in periphery of upper limbs.Mainly in periphery of upper limbs.
PHYSIOTHERAPY MANAGEMENT OF PARKINSON·SPHYSIOTHERAPY MANAGEMENT OF PARKINSON·S

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 103/186
DISEASEDISEASE
(10) SENSORY INTEGRITY:(10) SENSORY INTEGRITY: --
Blunting of touch sensations.Blunting of touch sensations.
Loss of propioception more in lower extremities than upper,Loss of propioception more in lower extremities than upper,
distal than proximaldistal than proximal ParesthesiasParesthesias (sensation of numbness or tingling).(sensation of numbness or tingling).
(11) PAIN:(11) PAIN: --
Mild aching & cramp like.Mild aching & cramp like.
Poorly localized.Poorly localized.
Postural stress syndrome.Postural stress syndrome.
PHYSIOTHERAPY MANAGEMENT OF PARKINSON·SPHYSIOTHERAPY MANAGEMENT OF PARKINSON·S

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 104/186
DISEASEDISEASE Assessment Instruments: The Mc Gill Pain Questionnaire. Assessment Instruments: The Mc Gill Pain Questionnaire.
The Visual Analogue The Visual Analogue
(12) POSTURAL INSTABILITY:(12) POSTURAL INSTABILITY:
Disturbed balance.Disturbed balance.
Greater problem in single limb stance.Greater problem in single limb stance.
Assessment instrument : Timed up & go test. Assessment instrument : Timed up & go test.
Berg balance test.Berg balance test.
Functional reach.Functional reach.
Clinical Test for Sensory Interaction inClinical Test for Sensory Interaction in
Balance (CTSIB).Balance (CTSIB).
PHYSIOTHERAPY MANAGEMENT OF PARKINSON·SPHYSIOTHERAPY MANAGEMENT OF PARKINSON·S

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 105/186
DISEASEDISEASE
Assessment instrument : Assessment instrument : Tinetti·s Tinetti·s Performance Oriented MobilityPerformance Oriented Mobility
Assessment (POMA) Assessment (POMA)
(13) POSTURE :(13) POSTURE :--
Flexed or stooped.Flexed or stooped.
Kyphosis & cervicalKyphosis & cervical lordosislordosis..
Assessment instrument : Postural grids or Plumb lines. Assessment instrument : Postural grids or Plumb lines.
Still photography.Still photography.
Videotapes. Videotapes.
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 106/186
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE
(14) GAIT:(14) GAIT:--
Freezing episodes.Freezing episodes.
Shuffling gait pattern.Shuffling gait pattern.
Stride length, step width decreases.Stride length, step width decreases.
Cadence increased.Cadence increased.
(Gait should be examined during all movement directions;(Gait should be examined during all movement directions;forward, backward, sideward).forward, backward, sideward).
PHYSIOTHERAPY MANAGEMENT OF PARKINSON·SPHYSIOTHERAPY MANAGEMENT OF PARKINSON·S

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 107/186
DISEASEDISEASE
(15) AUTONOMIC CHANGES:(15) AUTONOMIC CHANGES: --
Excessive drooling (salivation).Excessive drooling (salivation).
Excessive sweating.Excessive sweating.
Greasy skin.Greasy skin.
PHYSIOTHERAPY MANAGEMENT OF PARKINSON·SPHYSIOTHERAPY MANAGEMENT OF PARKINSON·S

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 108/186
DISEASEDISEASE
CARDIORESPIRATORY EXAMINATIONCARDIORESPIRATORY EXAMINATION
Cardio respiratory endurance may be reduced from impaired respiratoryCardio respiratory endurance may be reduced from impaired respiratory
functions & long standing inactivity.functions & long standing inactivity.
(1)ABNORMAL BREATHING PATTERNS:(1)ABNORMAL BREATHING PATTERNS:--
Ribcage compliance & chest wall mobility decreases.Ribcage compliance & chest wall mobility decreases.
Restrictive breathing.Restrictive breathing.
Kyphosis present.Kyphosis present.
(2) ALTERED LUNG VOLUMES & CAPACITIES:(2) ALTERED LUNG VOLUMES & CAPACITIES: --
FVC, FEV, decreased.FVC, FEV, decreased.
RV, RA W increased.RV, RA W increased.
TLC, VC decreased. TLC, VC decreased.
PHYSIOTHERAPY MANAGEMENT OF PARKINSON·SPHYSIOTHERAPY MANAGEMENT OF PARKINSON·S

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 109/186
DISEASEDISEASE
(3) ALTERED VITAL SIGNS:(3) ALTERED VITAL SIGNS: --
HRmax reduced.HRmax reduced.
Respiratory rate increased.Respiratory rate increased.
PaO2 is decreased.PaO2 is decreased.
BP decreased (orthostatic hypotension).BP decreased (orthostatic hypotension).
Assessment instrument : 6 Minute walking test. Assessment instrument : 6 Minute walking test.
Exercise tolerance test.Exercise tolerance test.
Sphygmomanometer.Sphygmomanometer.
PHYSIOTHERAPY MANAGEMENT OF PARKINSON·SPHYSIOTHERAPY MANAGEMENT OF PARKINSON·S

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 110/186
DISEASEDISEASE
FUNCTIONAL STATUS:FUNCTIONAL STATUS:--
Difficulty in performing ADL.Difficulty in performing ADL.
Activities having a rotational component are reduced or absent. Activities having a rotational component are reduced or absent.
Assessment instrument : The functional independence measure Assessment instrument : The functional independence measure
Katz index of independence in activities of Katz index of independence in activities of
daily life.daily life.
PHYSIOTHERAPY MANAGEMENT OF PARKINSON·SPHYSIOTHERAPY MANAGEMENT OF PARKINSON·S
DISEASEDISEASE

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 111/186
DISEASEDISEASE
GENERAL HEALTH MEASURES:GENERAL HEALTH MEASURES:--
Decrease in physical & social function.Decrease in physical & social function.
Decrease in emotional well being.Decrease in emotional well being.
Assessment instrument: Rand 36 item health survey SF 36 Assessment instrument: Rand 36 item health survey SF 36
Sickness impact profile.Sickness impact profile.
SKIN INTEGRITY & CONDITION:SKIN INTEGRITY & CONDITION:--
Bruising & skin breakdown.Bruising & skin breakdown.
Pressure sore may be present in patient confined to bed.Pressure sore may be present in patient confined to bed.
FINGER DEXTERITY:FINGER DEXTERITY: --
Pt. May unable to button up three shirt buttons up to 3 minutes.Pt. May unable to button up three shirt buttons up to 3 minutes.
PHYSIOTHERAPY MANAGEMENT OF PARKINSON·SPHYSIOTHERAPY MANAGEMENT OF PARKINSON·S
DISEASEDISEASE

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 112/186
DISEASEDISEASE
OUTCOME MEASURESOUTCOME MEASURES
Outcome measure serves as an aid in charting and objectivelyOutcome measure serves as an aid in charting and objectively
assessing health problems, to evaluate preliminary treatmentassessing health problems, to evaluate preliminary treatment
effectiveness and make inventory of the patient problems for possibleeffectiveness and make inventory of the patient problems for possible
intervention.intervention.
The KNGF development group Guidelines 2004, recommends the The KNGF development group Guidelines 2004, recommends the
following outcome for PD measurement:following outcome for PD measurement:
The The RetropulsionRetropulsion test; For general impression of problems withtest; For general impression of problems withbalancebalance
The MODIFIED Parkinson·s Activity scale(PAS) The MODIFIED Parkinson·s Activity scale(PAS)--for quality of for quality of
movement during certainmovement during certain ADL;functional ADL;functional mobilitymobility
OUTCOME MEASURESOUTCOME MEASURES

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 113/186
Time up and go test(TUG) Time up and go test(TUG)--for functional mobility and balancefor functional mobility and balance
The six minute walk test The six minute walk test-- for physical capacity in the absencefor physical capacity in the absence
of freezing.of freezing.
The Ten The Ten--meter walk testmeter walk test-- To evaluate comfortable walking To evaluate comfortable walking
speed.speed.
GRADING OF PARKINSON·s DISEASEGRADING OF PARKINSON·s DISEASE
(1)(1) HOEHN & YAHR SCALE (1967).HOEHN & YAHR SCALE (1967).
(2)(2) HE UNIFIED PARKINSON·S DISEASE RATING SCALEHE UNIFIED PARKINSON·S DISEASE RATING SCALE ² ²
UPDRS (1987).UPDRS (1987).
(3)(3) THE PARKINSON·S DISEASE QUESTIONNAIRE (PDQ THE PARKINSON·S DISEASE QUESTIONNAIRE (PDQ--39).39).
OUTCOME MEASURESOUTCOME MEASURES

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 114/186
HOEHN AND YAHR SCALEHOEHN AND YAHR SCALE
STAGE 1STAGE 1 ² ² Disability or functional impairment is usually absent orDisability or functional impairment is usually absent or
minimal.minimal.
If present, unilateral involvement. If present, unilateral involvement.
STAGE 2STAGE 2 ² ² Bilateral or midline involvement.Bilateral or midline involvement.
-- Balance not disturbed.Balance not disturbed.
STAGE 3STAGE 3 ² ² Impaired righting reflexes.Impaired righting reflexes.
-- Functionally restricted in some activities but patient canFunctionally restricted in some activities but patient can
live.live.
-- Disability is mild to moderateDisability is mild to moderate..
OUTCOME MEASURESOUTCOME MEASURES

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 115/186
STAGE 4STAGE 4 ² ² All symptoms present & severally disabled. All symptoms present & severally disabled.
-- Standing & walking possible only with assistance.Standing & walking possible only with assistance.
STAGE 5STAGE 5 ² ² Confined to wheelchair or bed.Confined to wheelchair or bed.
MODIFIED HOEHN AND YAHR STAGINGMODIFIED HOEHN AND YAHR STAGING
STAGE 0 = No signs of disease.STAGE 0 = No signs of disease.
STAGE 1 = Unilateral disease.STAGE 1 = Unilateral disease.
STAGE 1.5 = Unilateral plus axial involvementSTAGE 1.5 = Unilateral plus axial involvement..
STAGE 2 = Bilateral disease, without impairment of balance.STAGE 2 = Bilateral disease, without impairment of balance.
STAGE 2.5 = Mild bilateral disease, with recovery on pull test.STAGE 2.5 = Mild bilateral disease, with recovery on pull test.
OUTCOME MEASURESOUTCOME MEASURES

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 116/186
MODIFIED HOEHN AND YAHR STAGINGMODIFIED HOEHN AND YAHR STAGING
STAGE 3 = Mild to moderate bilateral disease; some posturalSTAGE 3 = Mild to moderate bilateral disease; some postural
instability; physically independent.instability; physically independent.
STAGE 4 = Severe disability; still able to walk or standSTAGE 4 = Severe disability; still able to walk or stand
unassisted.unassisted.
STAGE 5 = Wheelchair bound or bedridden unless aided.STAGE 5 = Wheelchair bound or bedridden unless aided.
UNIFIED PARKINSON·S DISEASE RATING SCALEUNIFIED PARKINSON·S DISEASE RATING SCALE

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 117/186
It is a rating tool to follow the longitudinal course of PD.It is a rating tool to follow the longitudinal course of PD.
It is made up of :It is made up of :--
(a)(a) MentationMentation, Behavior & Mood., Behavior & Mood.
(b)(b) ADL. ADL.
(c)(c) Motor sections.Motor sections.
These are evaluated by interviewing the patient These are evaluated by interviewing the patient
A total of 199 points are possible. A total of 199 points are possible.
199 points represents the worst (total disability) & 0 point199 points represents the worst (total disability) & 0 point
represents no disability.represents no disability.
THE PARKINSON·S DISEASE QUESTIONNAIRE (PDQ 39) THE PARKINSON·S DISEASE QUESTIONNAIRE (PDQ 39)

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 118/186
The PDQ is a 39 items questionnaire. The PDQ is a 39 items questionnaire.
It focuses on the subjective reports of the impact of PD onIt focuses on the subjective reports of the impact of PD on
daily life.daily life.
These are interviewed with patients. These are interviewed with patients.
Scored are given & summarized as Parkinson·s diseaseScored are given & summarized as Parkinson·s disease
Summary Index (PDSI).Summary Index (PDSI).
ANALYSIS OF FINDINGS ANALYSIS OF FINDINGS

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 119/186
Is physiotherapy indicated?Is physiotherapy indicated?
Can the guidelines be applied to this individual patient?Can the guidelines be applied to this individual patient?Physiotherapy will be indicated if the patient;Physiotherapy will be indicated if the patient;
11.. Is limited in one or more activities (transfers, posture, reaching andIs limited in one or more activities (transfers, posture, reaching and
grasping, balance and gait);grasping, balance and gait);2.2. Has (or has the risk of) a decreased physical capacity caused by inactivity;Has (or has the risk of) a decreased physical capacity caused by inactivity;
3.3. has an increased risk of falling or has fear to fall;has an increased risk of falling or has fear to fall;
44. Has an increased chance of pressure sores; or. Has an increased chance of pressure sores; or
5.5. has the need for information or advice on the disorder, natural course andhas the need for information or advice on the disorder, natural course and
prognosis prognosis
PHYSIOTHERAPY MANAGEMENT OF PARKINSON·SPHYSIOTHERAPY MANAGEMENT OF PARKINSON·S
DISEASEDISEASE

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 120/186
DISEASEDISEASE
AIMS OF PHYSIOTHERAPY TREATMENT AIMS OF PHYSIOTHERAPY TREATMENT
According to Disease Progression According to Disease Progression
PHYSIOTHERAPY MANAGEMENT OF PARKINSON·SPHYSIOTHERAPY MANAGEMENT OF PARKINSON·S
DISEASEDISEASE

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 121/186
DISEASEDISEASE
PLAN OF TREATMENTPLAN OF TREATMENT
11. To increase safety and independence in the performance of . To increase safety and independence in the performance of
activities, with the emphasis on:activities, with the emphasis on:
Transfers; Transfers;
Posture;Posture;
Reaching and grasping;Reaching and grasping;
Balance;Balance; Gait;Gait;
2. To preserve or improve physical capacity;2. To preserve or improve physical capacity;
PLAN OF TREATMENTPLAN OF TREATMENT

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 122/186
3.3. To prevent falling; To prevent falling;
4. To prevent pressure sores;4. To prevent pressure sores;
5. To stimulate insight into impairments in functions and5. To stimulate insight into impairments in functions and
limitations in activities, especially in the area of posture andlimitations in activities, especially in the area of posture and
movement.movement.
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 123/186
PARKINSON·S DISEASEPARKINSON·S DISEASE
THERAPEUTIC PROCESS: THERAPEUTIC PROCESS:
GENERAL TREATMENT PRINCIPLESGENERAL TREATMENT PRINCIPLES
i.i. Location of the treatmentLocation of the treatment:: to improve functional
activity, it is recommended it preferably takes place at the
patient home. This can also improve physical capacity
ii.ii. Involvement of care giverInvolvement of care giver
iii.iii. Avoidance of dual tasking Avoidance of dual tasking
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 124/186
PARKINSON·S DISEASEPARKINSON·S DISEASE
iv.iv. Multidisciplinary agreementMultidisciplinary agreement
v. v. Frequency and duration of treatment:Frequency and duration of treatment: there are
indications that a period of AT LEAST FOUR WEEKS AT LEAST FOUR WEEKS is needed to
decrease limitations in functional activities (disability) while a
period of AT AT LEAST EIGHT WEEKS LEAST EIGHT WEEKS of aerobic exercises and other
exercises is necessary to improve physical capacity, in which period
of a low frequency of treatment is sufficient for example once a
week to adjust exercise program. (Kamsma et al., 1995; Comelle et
al,. 1994; Dam et al., 1996; Patti, 1996; Thaut et al., 1996)
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 125/186
PARKINSON·S DISEASEPARKINSON·S DISEASE
vi. vi. Time of treatment: Time of treatment:
Exercises in PD patients can be performed in the On- as
well as in the Off- period (including cognitive movement
strategies and cueing strategies)
It is advisable also to train physical capacity (including
strength) in patient with PD during the On- period,
because at this time, neurological problems have less
influence on the level of performance.
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 126/186
PARKINSON S DISEASEPARKINSON S DISEASE
vii. vii. Tempo of exercising: Tempo of exercising: in cognitive impairment and
fatigue. Tempo and schedule of treatment need to be
adjusted.
viii. viii. Recognising a response of fluctuation:Recognising a response of fluctuation: physical
therapist should draw the patient attention to response
fluctuation.
ix.ix. Contraindications:Contraindications:
Deep brain stimulation (S WD, M WD, electromagnetic pulses,Deep brain stimulation (S WD, M WD, electromagnetic pulses,
electromagnetic fields)electromagnetic fields)
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 127/186
PARKINSON S DISEASEPARKINSON S DISEASE
ix.ix.
Contraindications:Contraindications: FreezingFreezing ² hydrotherapy is contraindicated in freezing.
Mental impairmentMental impairment: Impairment in cognition (e.g.
poor memory, dementia and severe hallucinations),
personality and attention are relative contraindications for
the treatment of health problems related to PD.
PHYSIOTHERAPY MANAGEMENT OF PARKINSON·SPHYSIOTHERAPY MANAGEMENT OF PARKINSON·S
DISEASEDISEASE

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 128/186
DISEASEDISEASE
EvidenceEvidence--BasedBased Analysis Analysis of of PhysicalPhysical
Therapy Therapy inin Parkinson·sParkinson·s DiseaseDisease with with
RecommendationsRecommendations forfor PracticePractice andandResearchResearch.. ((keuskeus etet alal..,, 20062006))

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 129/186
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 130/186
TREATMENT STRATEGIES OR MEANS TREATMENT STRATEGIES OR MEANS
For PD patients with sufficient understanding, insight, and
memory
Cognitive movement strategies
Cueing strategies
Modifying coping strategies.
Are recommended treatment means based on Hoehn and Yahr
classification of PD into three phases as related to treatment
goal.
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 131/186
Cognitive movement strategieCognitive movement strategiess
Cognitive movement strategies can be applied by physical therapist
to improve TRANSFERS. (Morris, 2000; Kamsma et al., 1995;
Iansek, 1999; Nieuwboer, 2001; Muller et al., 1997)
In Cognitive movement strategies, complex (automatic) activities are
transformed to a number of separate elements which are executed in
a defined sequence and which consist of relatively simple movement
elements.
This will prevent dual tasking during complex (automatic) activities
in daily life. Performance is consciously controlled and can be
guided by using CUES in initiation.
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 132/186
PARKINSON·S DISEASEPARKINSON·S DISEASE
Cognitive movement strategiesCognitive movement strategiesExample; Rising from a chair.Example; Rising from a chair.
place your hands on the arms or the side of the seat; place your hands on the arms or the side of the seat;
move your feet towards the chair (just in front of the chair legs, twomove your feet towards the chair (just in front of the chair legs, two
fists apart);fists apart);
shift your hips to the edge of the chair;shift your hips to the edge of the chair;
bend your trunk (not too far, nose above the knees);bend your trunk (not too far, nose above the knees);
rise gently, from your legs, let your hands lean on the arms of therise gently, from your legs, let your hands lean on the arms of the
chair, the seat or your thighs, and then extend your trunk completelychair, the seat or your thighs, and then extend your trunk completely
(if necessary, make use of a visual cue). In case of starting problems(if necessary, make use of a visual cue). In case of starting problems
rock back and forth a few times and rise at the third count.rock back and forth a few times and rise at the third count.
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKI SO ·S DIS ASPARKI SO ·S DIS AS

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 133/186
PARKINSON·S DISEASEPARKINSON·S DISEASE
Cueing strategiesCues are used to complete or replace the fundamentalCues are used to complete or replace the fundamental
problems of internal control in PD patient as in performance of problems of internal control in PD patient as in performance of
automatic and repetitive movements.automatic and repetitive movements.
Cues are stimuli from the environment or stimuli generated byCues are stimuli from the environment or stimuli generated by
the patient which increase attention and facilitate (automatic)the patient which increase attention and facilitate (automatic)
movements.movements.
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 134/186
PARKINSON·S DISEASEPARKINSON·S DISEASECueing StrategiesCueing Strategies
CUESCUES
RhythmicalRhythmical
recurring cuesrecurring cues
OneOne--off cuesoff cues
Internal cueInternal cue
e.g. bow,e.g. bow,
stretch, wavestretch, wave.
ExternalExternal
CueCue
NonNon--moving stimulimoving stimuli
e.g. sound of metronome,e.g. sound of metronome,
Stripes on the floor,Stripes on the floor, A grip of a walking stick. A grip of a walking stick.
Moving stimuliMoving stimuli
e.g. light of laser pen,e.g. light of laser pen,
A moving foot, A moving foot,
A falling bunch of keys A falling bunch of keys
Example of cueing strategy to improve gaitExample of cueing strategy to improve gait
Freezing at the DoorwayFreezing at the Doorway

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 135/186
Example of cueing strategy to improve gaitExample of cueing strategy to improve gait
F i t th D ` h d li ht f tiF i t th D ` h d li ht f ti

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 136/186
Freezing at the Doorway` arrow show red light for correctionFreezing at the Doorway` arrow show red light for correction
Solution Solution ² ² a red line is added a red line is added
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 137/186
PARKINSON·S DISEASEPARKINSON·S DISEASE
RHYTHMICALRHYTHMICAL RECURRINGRECURRING CUESCUES areare givengiven asas aa
continuouscontinuous rhythmicalrhythmical stimulus,stimulus, which which cancan serveserve asas aa controlcontrol
mechanismmechanism forfor walking walking..
The The distancedistance betweenbetween (frequency(frequency of)of) rhythmicrhythmic cuescues duringduring
walking walking will will bebe basedbased onon thethe numbernumber of of stepssteps neededneeded toto
perform perform thethe Ten Ten--metermeter walk walk testtest atat comfortablecomfortable pace pace..
ONEONE- - OFF OFF CUES CUES areare usedused toto keepkeep balance,balance, forfor exampleexample
when when performing performing transfertransfer andand forfor initiatinginitiating ADL ADL oror when when
gettinggetting startedstarted againagain afterafter aa period period of of freezingfreezing..
PHYSIOTHERAPY MANAGEMENT OF PARKINSON·SPHYSIOTHERAPY MANAGEMENT OF PARKINSON·S
DISEASEDISEASE

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 138/186
DISEASEDISEASE
Rhythmic recurring cuesRhythmic recurring cues
Auditory Auditory
the patient moves on music of a walkmanthe patient moves on music of a walkman
the patient moves on rhythmical ticking of the patient moves on rhythmical ticking of
a metronomea metronome
the patient or someone else sings or counts the patient or someone else sings or counts
Visual Visual the patient follows another person the patient follows another person
the patient walks over stripes on the floor or the patient walks over stripes on the floor or
over stripes he projects to himself withover stripes he projects to himself with
a laser pena laser pen
the patient walks with an inverted walking the patient walks with an inverted walking--
stick and has to step over the gripstick and has to step over the grip
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 139/186
PARKINSON S DISEASEPARKINSON S DISEASE
Rhythmic recurring cuesRhythmic recurring cues Tactile Tactile thethe patient patient tapstaps hishis hiphip oror legleg
OneOne--off cuesoff cues
Auditory Auditory initiation of movement, for example, initiation of movement, for example,
stepping out at the third countstepping out at the third count
Visual Visual initiation of movement, for example, by initiation of movement, for example, by
stepping over some else·s foot, an object onstepping over some else·s foot, an object onthe floor or an inverted walkingthe floor or an inverted walking--stick stick
maintenance of posture, for example, by maintenance of posture, for example, by
using a mirror or by focusing on an objectusing a mirror or by focusing on an object
(clock, painting) in the environment(clock, painting) in the environment
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 140/186
PARKINSON·S DISEASEPARKINSON·S DISEASE
OneOne--off cuesoff cues
CognitiveCognitive initiation of movement (and continuation initiation of movement (and continuation
of walking), for example, by focusing onof walking), for example, by focusing onthe spot he wants to go to, and not on thethe spot he wants to go to, and not on the
doorway he has to go throughdoorway he has to go through
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 141/186
PARKINSON·S DISEASEPARKINSON·S DISEASE
RECOMMENDATIONS FROM EVIDENCE BASEDRECOMMENDATIONS FROM EVIDENCE BASEDRESEARCHRESEARCH
EARLY OR MAINTENANCE PHASEEARLY OR MAINTENANCE PHASE
Stimulate balanceStimulate balance
Goal: to optimize balance and training strength.Goal: to optimize balance and training strength.
Strategy : Exercises for balance and training strength.Strategy : Exercises for balance and training strength.
e.g.e.g. ² ² Taichi (two group sessions a week for fifteen weeks) Taichi (two group sessions a week for fifteen weeks)
-- walking outside three times a week, completed with a home walking outside three times a week, completed with a home
exercise program (30 minutes, 3 times a week).exercise program (30 minutes, 3 times a week).
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 142/186
PARKINSON·S DISEASEPARKINSON·S DISEASE
Taichi for balance training ,perception of posture and coordination of arms
and legs and backward and lateral large step.
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 143/186
PARKINSON·S DISEASEPARKINSON·S DISEASE
Walking on toes strengthening exercises to the legs Walking on toes strengthening exercises to the legs
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 144/186
PARKINSON·S DISEASEPARKINSON·S DISEASE
Stepping over an objectStepping over an object
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 145/186
PARKINSON S DISEASEPARKINSON S DISEASE
These decreases the number of falls These decreases the number of falls
(b) Exercise to increase the mobility of among others, neck, knees and(b) Exercise to increase the mobility of among others, neck, knees and
hips.hips.
-- Referral to occupational therapy to identify and alter any changesReferral to occupational therapy to identify and alter any changes
present in the home environment.present in the home environment.
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 146/186
PARKINSON S DISEASEPARKINSON S DISEASE
PREVENTION OF INACTIVITY OR MAINTENANCEPREVENTION OF INACTIVITY OR MAINTENANCEOF PHYSICAL CAPACITY.OF PHYSICAL CAPACITY.
Goal: Maintenance or improvement of physical capacity.Goal: Maintenance or improvement of physical capacity.
Strategy: providing information on the importance of Strategy: providing information on the importance of exercising or playing sports, training of aerobics capacity,exercising or playing sports, training of aerobics capacity,
muscle strength (with emphasis on the muscles of the trunk muscle strength (with emphasis on the muscles of the trunk
and legs), joint mobility (among others axial) and muscleand legs), joint mobility (among others axial) and musclelength (among others, muscles of the calf and hamstrings)length (among others, muscles of the calf and hamstrings)
A THERA CYCLE: to improve physical capacity A THERA CYCLE: to improve physical capacity

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 147/186
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 148/186
PROGRESSIVE RESISTANCEPROGRESSIVE RESISTANCE STRENGTHENING EXERCISESSTRENGTHENING EXERCISES
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 149/186
PARKINSON S DISEASEPARKINSON S DISEASE
Joint mobility training Joint mobility training
Exercise programs focused on improving joint mobility,Exercise programs focused on improving joint mobility,
combined with training of gait and balance, improve motor skills.combined with training of gait and balance, improve motor skills.
( (ComelleComelle et al., 1994; Patti et al., 1996;et al., 1994; Patti et al., 1996; PachettiPachetti et al., 2000;et al., 2000;
MarcheseMarchese et al., 2000 ).et al., 2000 ).
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 150/186
PARKINSON S DISEASEPARKINSON S DISEASE
Improves ADL (Improves ADL (ComelleComelle et al., 1994; Patti et al., 1996;et al., 1994; Patti et al., 1996;
PachettiPachetti et al., 2000;et al., 2000; FormisanoFormisano et al., 1992; Palmer et al., 1986)et al., 1992; Palmer et al., 1986)
Improves mental functioning (Improves mental functioning (ComelleComelle et al., 1994; Patti etet al., 1994; Patti et
al., 1996).al., 1996).
ShenkmanShenkman et al., 1998 shows that exercise program focusedet al., 1998 shows that exercise program focused
at improving joint mobility and coordinated movementat improving joint mobility and coordinated movement
incorporated in ADL improves functional axial rotation andincorporated in ADL improves functional axial rotation and
reach (balance).reach (balance).
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 151/186
PARKINSON S DISEASEPARKINSON S DISEASE
Training of strength Training of strengthExercise program which are among others, focused onExercise program which are among others, focused on
improving muscle strength (of the lower extremities and trunk)improving muscle strength (of the lower extremities and trunk)

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 152/186
Trunk rotation exercises
LUNGES
ANKLE JOINT MOBILITY
SQUATTING EXERCISES
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 153/186
PARKINSON S DISEASEPARKINSON S DISEASE
May also improve muscle strength in patients with PD (in earlyMay also improve muscle strength in patients with PD (in early
to middle phase). (Reuter et al., 1999; Scandalis et al., 2001).to middle phase). (Reuter et al., 1999; Scandalis et al., 2001).
Training aerobic Capacity Training aerobic Capacity
Aerobic exercise that improves aerobic capacity also improve Aerobic exercise that improves aerobic capacity also improve
motor skills of patient with PD in the early phase (Reuter et al.,motor skills of patient with PD in the early phase (Reuter et al.,
1999;1999; BaatileBaatile et al., 2000; Bergen et al., 2002).et al., 2000; Bergen et al., 2002).
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 154/186
PARKINSON S DISEASEPARKINSON S DISEASE
Training aerobic capacity Training aerobic capacity Group therapy
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 155/186
PARKINSON S DISEASEPARKINSON S DISEASE
Fall PreventionFall Prevention
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 156/186
PARKINSON S DISEASEPARKINSON S DISEASE
Mid or Complex PhaseMid or Complex PhaseCognitive movement strategies improve transfers
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 157/186
PARKINSON S DISEASEPARKINSON S DISEASE
CUEING STRATEGIES TO IMPROVE GAIT: As diseaseCUEING STRATEGIES TO IMPROVE GAIT: As disease
progresses and medication is not as effective, some people progresses and medication is not as effective, some people
present freezing of gait. One common problem is to freeze present freezing of gait. One common problem is to freeze
when trying to go through a when trying to go through a doorway. It is possible todoorway. It is possible to
overcome this problem with a simple visual cue, such as a lineovercome this problem with a simple visual cue, such as a line
on the floor. This cue attracts attention to the task, and theon the floor. This cue attracts attention to the task, and the
person can step over it. Another strategy to overcome freezing person can step over it. Another strategy to overcome freezingof gait is the use of auditory cues, such as a metronome, thatof gait is the use of auditory cues, such as a metronome, that
can be adjusted to the person·s walking rhythm.can be adjusted to the person·s walking rhythm.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 158/186

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 159/186
Solution Solution ² ² a red line is added a red line is added
Improving gait using modified footwearImproving gait using modified footwear

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 160/186
PhotoboardsPhotoboards providing insight to stance phase function. In both providing insight to stance phase function. In both photoboards photoboards, a, a
physiotherapist can be seen walking alongside the patient and a walking stick physiotherapist can be seen walking alongside the patient and a walking stick is being used. The top strip shows the unmodified footwear position and theis being used. The top strip shows the unmodified footwear position and the
bottom strip shows the modified footwear position.bottom strip shows the modified footwear position.
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 161/186
Normalizing body posture and upper limb functionNormalizing body posture and upper limb function::
Cueing and cognitive movement strategies are creatively usedCueing and cognitive movement strategies are creatively used
in physiotherapy to design exercises to improve posture, suchin physiotherapy to design exercises to improve posture, such
as straightening the back an maintaining posture by looking atas straightening the back an maintaining posture by looking at
a target at eye level, or training functional arm movements,a target at eye level, or training functional arm movements,
such as drinking from a cup by dividing the complex sequencesuch as drinking from a cup by dividing the complex sequence
into different steps and practicing each step separately.into different steps and practicing each step separately.
Balance training could include stepping on the spot whileBalance training could include stepping on the spot while
lifting the knees up high, following the sound of a metronome.lifting the knees up high, following the sound of a metronome.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 162/186
Boxing: Anticipatory postural adjustments, postural corrections, fast arm and footBoxing: Anticipatory postural adjustments, postural corrections, fast arm and foot
motions, backward walking, timing, sequencing actionsmotions, backward walking, timing, sequencing actions
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 163/186
Late (Palliative) PhaseLate (Palliative) Phase Aim Aim ² ² Prevention of ComplicationsPrevention of Complications
DYSKINESIASDYSKINESIAS: One of the complications in the late stage of
PD is severe unpredictable fluctuations and dyskinesias.Relaxation techniques, which include breathing exercises and
correct posture, are effective in some patients. They have only a
short-term effect of about five to 10 minutes, but despite this, patients should be allowed to enjoy a few minutes of rest or a
nap, which will make a difference to their overall quality of life.
PHYSIOTHERAPY MANAGEMENT OFPHYSIOTHERAPY MANAGEMENT OF
PARKINSON·S DISEASEPARKINSON·S DISEASE

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 164/186
W ALKING AIDS: W ALKING AIDS: Stimulating mobility as much as
possible is a goal in physiotherapy. Walking is encouraged,
sometimes with the help of walking aids. Not every walking aid
is appropriate and some are potentially dangerous if given to
the wrong person. Sometimes using a walking aid at certain
periods of the day under close supervision could maintain a
certain level of mobility, with all of the attendant benefits.
Walking Aids Walking Aids

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 165/186
W ALKING AID

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 166/186
W ALKING W ALKING AIDS AIDS

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 167/186
TREATMENT TECHNIQUES TREATMENT TECHNIQUES

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 168/186
Keep Moving Exercise ProgramKeep Moving Exercise Program
METERS(Movement Enablement TMETERS(Movement Enablement T hroughhrough Exercise Regimes)Exercise Regimes)(Plant et al. ,2001 )(Plant et al. ,2001 )
Task specific approach (Morris,2000 ) Task specific approach (Morris,2000 )
Systematic approach( Systematic approach(schenkmanschenkman et al.,1989 and 1996 )et al.,1989 and 1996 )
SensorimotorSensorimotor Agility Exercise Program Agility Exercise Program Tiachi Tiachi
Kayaking Kayaking
A
gility A
gility Boxing Boxing
LungesLunges
PrepilatePrepilate (king and Horak,2009)(king and Horak,2009)
TREATMENT TECHNIQUES TREATMENT TECHNIQUES
Relaxation techniquesRelaxation techniques

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 169/186
e o ec q ese o ec q es
Autogenic Autogenic Progressive muscleProgressive muscle
Visualization Visualization
Tiachi Tiachi
MusicMusic
Light stoking massageLight stoking massage
HarthaHartha yogayoga
ExerciseExercise ² ² Alexander technique(stallibrass,1997) Alexander technique(stallibrass,1997)
Deep Breathing techniqueDeep Breathing technique
Vestibular rehabilitation Therapy Vestibular rehabilitation Therapy
CONCLUSIONCONCLUSION
EVALUATIONEVALUATION

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 170/186
EVALUATIONEVALUATION
PATIENTS SPECIFIC COMPLAINTS QUESTIONNAIRE,PATIENTS SPECIFIC COMPLAINTS QUESTIONNAIRE,
MEASUREMENT OF THE ¶GLOBAL PERCEIVEDMEASUREMENT OF THE ¶GLOBAL PERCEIVED
EFFECT· SHOULD ALSO BE USEDEFFECT· SHOULD ALSO BE USED
AFTERCARE AFTERCARE Preservation of improved activities in daily livingPreservation of improved activities in daily living
Check Check--upup
Final evaluationFinal evaluation
ReportingReporting
REFERENCESREFERENCES B tilB til JJ L n b inL n b in WE W r F M l n CWE W r F M l n C J tJ t MBMB

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 171/186
..
BaatileBaatile J, J, LangbeinLangbein WE, Weaver F, Maloney C, WE, Weaver F, Maloney C, Jost Jost MB.MB.
Effect of exercise on perceived quality of life of Effect of exercise on perceived quality of life of individuals with Parkinson·s disease. Jindividuals with Parkinson·s disease. J RehabilRehabil ResResDev 2000 Sep;37(5):529Dev 2000 Sep;37(5):529--3434
Bergen JL,Bergen JL, Toole Toole T, Elliott III RG, Wallace B, Robinson T, Elliott III RG, Wallace B, Robinson
K, Maitland CG. Aerobic exercise interventionK, Maitland CG. Aerobic exercise interventionimproves aerobicimproves aerobic
BloemBloem BR, Beckley DJ, vanBR, Beckley DJ, van Dijk Dijk JG, JG, ZwindermanZwinderman AH, AH,RemlerRemler MP,MP, RoosRoos R A. Influence of R A. Influence of dopaminergicdopaminergicmedication on automatic postural responses andmedication on automatic postural responses andbalance impairment in Parkinson·s disease.balance impairment in Parkinson·s disease. Mov Mov DisordDisord 1996 Sep;11(5):5091996 Sep;11(5):509--21.21.
REFERENCEREFERENCE
BloemBloem BR, vanBR, van Vugt Vugt JP, Beckley DJ. Postural JP, Beckley DJ. Postural

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 172/186
instability and falls in Parkinson·s disease. A
dv instability and falls in Parkinson·s disease. A
dv NeurolNeurol 2001;87:209 223.2001;87:209 223.
BloemBloem BR, Beckley DJ, vanBR, Beckley DJ, van Dijk Dijk JG, JG, ZwindermanZwinderman AH, AH, RemlerRemler MP,MP, RoosRoos R A. Influence of R A. Influence of
dopaminergicdopaminergic medication on automatic posturalmedication on automatic postural
responses and balance impairment in Parkinson·sresponses and balance impairment in Parkinson·sdisease.disease. Mov Mov DisordDisord 1996 Sep;11(5):5091996 Sep;11(5):509--21.21.
BloemBloem BR,BR, GrimbergenGrimbergen Y A, Cramer M, Y A, Cramer M, Willemsen WillemsenM,ZwindermanM,Zwinderman AH. Prospective assessment of AH. Prospective assessment of falls in Parkinson·s disease. Jfalls in Parkinson·s disease. J NeurolNeurol 2001 2001
Nov;248(
11 ):95
0Nov;
248(
11 ):95
0--88
REFERENCEREFERENCE
Chartered Society of Physiotherapy ( 2001 )Chartered Society of Physiotherapy ( 2001 )

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 173/186
y y py ( )y y py ( )
¶Effectiveness bulletin: Neurology: Parkinson·s¶Effectiveness bulletin: Neurology: Parkinson·sdisease, Multiple Sclerosis and severe traumaticdisease, Multiple Sclerosis and severe traumatic
brain injury·brain injury· Effectiveness Bulletin Effectiveness Bulletin ² ² Evidence Evidence - -b ased b ased
Practice Practice Vol Vol 3, Issue 2, pp13, Issue 2, pp1 ² ²33
ChessonChesson R. Psychosocial aspects of measurement.R. Psychosocial aspects of measurement.
Physiotherapy 1998;84(9):435Physiotherapy 1998;84(9):435--8.8.
ComellaComella CL, Stebbins GT, BrownCL, Stebbins GT, Brown--Toms N, Goetz Toms N, Goetz
CG. Physical therapy and Parkinson·s disease: aCG. Physical therapy and Parkinson·s disease: a
controlled clinical trial. Neurology 1994 Mar;44(3controlled clinical trial. Neurology 1994 Mar;44(3Pt 1 ):376Pt 1 ):376--88
REFERENCEREFERENCE Dam M,Dam M, Tonin Tonin P,P, CassonCasson S,S, BraccoBracco F,F, PironPiron L,L,

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 174/186
PizzolatoPizzolato G,G, etaletal. Effects of conventional and. Effects of conventional andsensory sensory--enhancedenhanced physiotherapyonphysiotherapyon disability of disability of
Parkinson·s disease patients. Adv Parkinson·s disease patients. Adv NeurolNeurol1996;69:5511996;69:551--5.5.
FormisanoFormisano R,R, PratesiPratesi L,L, ModarelliModarelli F T,F T, BonifatiBonifati V, V,MecoMeco G.RehabilitationG.Rehabilitation andand Parkinson·sdiseaseParkinson·sdisease..
Scand JScand J RehabilRehabil Med1992 Sep;24(3):157Med1992 Sep;24(3):157--60.60.
Garrett N A,Garrett N A, BrasureBrasure M, Schmitz KH, Schultz MM,M, Schmitz KH, Schultz MM,HuberHuber MR.PhysicalMR.Physical inactivity: direct cost to ainactivity: direct cost to a
health plan. Am Jhealth plan. Am J Prev Prev Med2004;27:304Med2004;27:304 ² ²309.309.
REFERENCEREFERENCE
Global Parkinson·s Disease Survey Steering Committee.Global Parkinson·s Disease Survey Steering Committee.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 175/186
Factors impacting on quality of life in Parkinson·sFactors impacting on quality of life in Parkinson·sdisease: results from an international survey.disease: results from an international survey. Mov Mov DisordDisord 2002;17( 1 ):602002;17( 1 ):60--7.7.
GrimbergenGrimbergen Y, Y, MunnekeMunneke M,M, BloemBloem BR. Falls in Parkinson·sBR. Falls in Parkinson·s
disease. Review.disease. Review. CurrCurr OpinOpin NeurolNeurol 2004;17:4052004;17:405² ² 15.15. GuttmanGuttman M,KishM,Kish JS and Furukawa Y( 2003);Current concept JS and Furukawa Y( 2003);Current concept
in thein the diagnosis and management of diagnosis and management of parkinson·sparkinson·s diseasediseaseCM A J 2003,168:3CM A J 2003,168:3
HeuvelHeuvel CMF van den,CMF van den, Vogels Vogels EMHM,EMHM, Mellink Mellink M,M,DijkstraDijkstra ZM,PietersZM,Pieters HM.HM. Handreiking Handreiking verslaggeving verslaggeving..http://www.paramedisch.org http://www.paramedisch.org ..
REFERENCEREFERENCE Iansek Iansek R. Interdisciplinary rehabilitationR. Interdisciplinary rehabilitation inParkinson·sinParkinson·s disease.disease.

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 176/186
In: Stern GM, editor. Advances in Neurology. Parkinson·sIn: Stern GM, editor. Advances in Neurology. Parkinson·s
disease. 80 ed.disease. 80 ed. PhilidelphiaPhilidelphia:: LippincotLippincot Williams & Williams & Wilkins;1999. p. 555 Wilkins;1999. p. 555--99
Jankovic Jankovic J, McDermott M, Carter J, Gauthier S, Goetz C, J, McDermott M, Carter J, Gauthier S, Goetz C,
GolbeLGolbeL, et al. Variable expression of Parkinson·s disease:, et al. Variable expression of Parkinson·s disease:a basea base--line analysis of the D A T A TOP cohort. Theline analysis of the D A T A TOP cohort. TheParkinson Study Parkinson Study Group.Neurology Group.Neurology 1990 Oct;40( 10 ):15291990 Oct;40( 10 ):1529--34.34.
KamsmaKamsma YPT, YPT, BrouwerBrouwer WH, WH, LakkeLakke JPW F. Training of JPW F. Training of compensation strategies for impaired gross motor skills incompensation strategies for impaired gross motor skills inParkinson·s disease.Parkinson·s disease. PhysiotherPhysiother Theory Theory PractPract 1995;11:2091995;11:209--29.29.
REFERENCEREFERENCE KeusKeus SHJ,SHJ, BloemBloem BR,BR, Verbaan Verbaan D, et al. Physiotherapy inD, et al. Physiotherapy in Parkinson'sParkinson's
disease tilisation and patient satisfactiondisease tilisation and patient satisfaction JJ Ne rolNe rol

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 177/186
disease: utilisation and patient satisfaction.disease: utilisation and patient satisfaction. J J NeurolNeurol
2004;251:6802004;251:680 ² ² 687.687. King L A,King L A, Horak Horak FB. Delaying mobility disability in people withFB. Delaying mobility disability in people with
Parkinson disease using aParkinson disease using a sensorimotorsensorimotor agility exercise programagility exercise program. .
PhysTher PhysTher . 2009;89:384. 2009;89:384² ²393.393.
KNGF
Guidelines for Physical Therapy inKNGF
Guidelines for Physical Therapy in Parkinson·s disease,Parkinson·s disease,Supplement to theSupplement to the D utch Journal of Physiotherapy D utch Journal of Physiotherapy , 2004;11, 2004;11
LaarLaar Tv Tv,, Wolters Wolters ECMJ.ECMJ. CognitieveCognitieve stoornissenstoornissen enen psychosepsychose bijdebijdeziekteziekte van Parkinson. van Parkinson. DimensiesDimensies inin dementiedementie 2002;2:32002;2:3--7.7.
MathiesonMathieson I,CurranI,Curran S,HallamS,Hallam S,CorneS,Corne J: Improving gait performance J: Improving gait performancein Parkinson·sin Parkinson·s disease:adisease:a case report suggesting a role forcase report suggesting a role for
footwear modifications. physiotherapy 94( 2008)85footwear modifications. physiotherapy 94( 2008)85--8888
REFERENCEREFERENCE
MarcheseMarchese R,R, DiverioDiverio M,M, ZucchiZucchi F,F, LentinoLentino C,C,

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 178/186
A
bbruzzese A
bbruzzese G. The role of sensory cues in theG. The role of sensory cues in therehabilitation of rehabilitation of parkinsonianparkinsonian patients: apatients: a
comparison of two physical therapy protocols.comparison of two physical therapy protocols.Mov Mov DisordDisord 2000 Sep;15(5):8792000 Sep;15(5):879--83.83.
Mclnerney Mclnerney--LeoLeo AMS,Gwinn AMS,Gwinn--Hardy; and NussbaumHardy; and NussbaumB( 2004):Prevalence of B( 2004):Prevalence of parkinson·sparkinson·s Disease inDisease inpopulations of Africa Ancestry ; A Review Jpopulations of Africa Ancestry ; A Review J NatlNatl
Med Assoc 2004;96:974Med Assoc 2004;96:974--979979 Management of Parkinson·s disease: an evidenceManagement of Parkinson·s disease: an evidence--
based review .based review .Mov Mov DisordDisord 2002;17(Suppl. 4):S12002;17(Suppl. 4):S1 ² ²
S166
.4.S166
.4.
REFERENCEREFERENCE
Morris M et al ( 1998) ¶The role of the physiotherapistMorris M et al ( 1998) ¶The role of the physiotherapist

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 179/186
in quantifying movement fluctuations inin quantifying movement fluctuations inParkinson·s disease·Parkinson·s disease· Australian Physiotherapy Australian Physiotherapy 44,10544,105² ² 114114
Morris ME. Movement disorders in people withMorris ME. Movement disorders in people with
Parkinson disease: a model for physical therapy.Parkinson disease: a model for physical therapy.PhysPhys Ther Ther 2000 Jun;80( 6 ):5782000 Jun;80( 6 ):578--97.97.
Morris M,Morris M, Iansek Iansek R, Smithson F,R, Smithson F, HuxhamHuxham F. PosturalF. Postural
instability in Parkinson·s disease: a comparisoninstability in Parkinson·s disease: a comparison with and without a concurrent with and without a concurrent task. Gait Posturetask. Gait Posture2000 Dec;12(3):2052000 Dec;12(3):205--16.16.
REFERENCEREFERENCE Muller V, Mohr B, Rosin R,Muller V, Mohr B, Rosin R, PulvermullerPulvermuller F, Muller F,F, Muller F, BirbaumerNBirbaumerN..
ShortShort term effects ofterm effects of behavioralbehavioral treatment on movement initiationtreatment on movement initiation

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 180/186
ShortShort--term effects of term effects of behavioralbehavioral treatment on movement initiationtreatment on movement initiation
and postural control in Parkinson·s disease: a controlled clinicaland postural control in Parkinson·s disease: a controlled clinicalstudy.study. Mov Mov DisordDisord 1997 May;12(3):3061997 May;12(3):306--1414
Muller J,Muller J, Wenning Wenning GK,GK, Jellinger Jellinger K, McKee A,K, McKee A, PoewePoewe W, W, LitvanLitvan
Progression of Progression of HoehnHoehn andand Yahr Yahr stages instages in ParkinsoniandisordersParkinsoniandisorders: a: aclinic pathologic study. Neurology 2000 Sep 26;55( 6 ):888clinic pathologic study. Neurology 2000 Sep 26;55( 6 ):888--9191
NieuwboerNieuwboer A, de A, de Weerdt Weerdt W, Dom R, W, Dom R, Truyen Truyen M,M, Janssens Janssens L,KamsmaL,Kamsma The effect of a home physiotherapy The effect of a home physiotherapy programforprogramfor persons withpersons with
Parkinson·s disease. JParkinson·s disease. J RehabilRehabil Med 2001Nov;33( 6 ):266Med 2001Nov;33( 6 ):266--72.72.
Olanow Olanow CW, Watts RL,CW, Watts RL, KollerKoller WC. An algorithm (decision WC. An algorithm (decision treefortreefor thethe
management of Parkinson·s disease ( 2001 ):management of Parkinson·s disease ( 2001 ): treatmentguidelinestreatmentguidelines..Neurology 2001 Jun;56( 11 Neurology 2001 Jun;56( 11 SupplSuppl 5):S15):S1--S8 8S8 8
OkubadejoOkubadejo UN,OjoUN,Ojo OO,andOO,and OshinaikeOshinaike OO( 2010 ): clinical profile of OO( 2010 ): clinical profile of ParkinsonismParkinsonism andand parkinson·sparkinson·s disease indisease in lagoslagos, south western, south western
REFERENCEREFERENCE OsuntokunOsuntokun BO,BO, BademosiBademosi O:O: Parkinsonism in the NigerianParkinsonism in the Nigerian
African:aAfrican:a prospective study of 217 patientsprospective study of 217 patients EastEast AfrAfr Med JMed J 19791979

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 181/186
African:a African:a prospective study of 217 patients. prospective study of 217 patients. East East Afr Afr Med J Med J 1979,1979,
56:56:597597--607607 PacchettiPacchetti C, Mancini F,C, Mancini F, Aglieri Aglieri R,R, FundaroFundaro C,C, MartignoniMartignoni E,NappiE,Nappi G.G.
Active music therapy in Parkinson·s disease: Active music therapy in Parkinson·s disease: anintegrativeanintegrative methodmethod
for motor and emotionalfor motor and emotional rehabilitation.Psychosomrehabilitation.Psychosom MedMed2000;62(3):3862000;62(3):386--93.93.
Patti F. Effects of rehabilitation therapy onPatti F. Effects of rehabilitation therapy on ParkinsonsParkinsons· disability and· disability andfunctional independence . Jfunctional independence . J NeurolNeurol RehabilRehabil 1996;14(4):2231996;14(4):223--31.31.
Plant R, Jones D, Hutchinson A, Thomson J, AshburnPlant R, Jones D, Hutchinson A, Thomson J, Ashburn A,Loader A,Loader S, et al.S, et al.Physiotherapy in Parkinson·s diseasePhysiotherapy in Parkinson·s disease -- referral,contactreferral,contact and dischargeand discharge
patterns.patterns. MovDisordMovDisord 2000;15 (Suppl3):1712000;15 (Suppl3):171
REFERENCEREFERENCE Plant R & Jones D ( 2001 ) Guidelines for physiotherapy with Parkinson·sPlant R & Jones D ( 2001 ) Guidelines for physiotherapy with Parkinson·s
disease. London: Institute of Rehabilitation, University of Northumbriadisease. London: Institute of Rehabilitation, University of Northumbria

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 182/186
, y, y
Plant R ( 2000
) Physiotherapy for people with Parkinson·s disease: UK Plant R ( 2000
) Physiotherapy for people with Parkinson·s disease: UK best practicebest practiceshort report, Institute of short report, Institute of RehabilitiationRehabilitiation, University of Northumbria, Newcastle, University of Northumbria, Newcastleupon Tyne.upon Tyne.
Rescue ProjectRescue Project www.rescueproject.org/overview/welcome.htm www.rescueproject.org/overview/welcome.htm
PoewePoewe WH, WH, Wenning Wenning GK. The natural history of Parkinson·s disease.GK. The natural history of Parkinson·s disease. Ann Ann NeurolNeurol1998 Sep;44(31998 Sep;44(3 SupplSuppl 1 ):S11 ):S1--S9.S9.
Pressley JC, Louis ED, Tang MX, et al. The impact of Pressley JC, Louis ED, Tang MX, et al. The impact of comorbidity comorbidity diseasedisease andandinjuries on resource use and expenditures ininjuries on resource use and expenditures in parkinsonism.Neurology parkinsonism.Neurology 2003;60:872003;60:87² ²93. 9393. 93
Reuter I,Reuter I, EngelhardtEngelhardt M,M, SteckerStecker K, Baas H. Therapeutic value of exercise training inK, Baas H. Therapeutic value of exercise training in
Parkinson·s disease. MedParkinson·s disease. Med SciSci Sports Exerc1999 Nov;31:1544Sports Exerc1999 Nov;31:1544--9 patients.9 patients.NeuroRehabilitationNeuroRehabilitation 2002;17( 2 ):1612002;17( 2 ):161--8.8.
REFERENCESREFERENCES ScandalisScandalis T A, T A, Bosak Bosak A, Berliner JC, A, Berliner JC, HelmanHelman LL, WellsLL, Wells

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 183/186
,, , J ,, J , ,,
MR.ResistanceMR.Resistance training and gait function intraining and gait function inpatientspatients withParkinson·s withParkinson·s disease. Am J Phys Meddisease. Am J Phys Med
RehabilRehabil 2001 Jan;80( 1 ):382001 Jan;80( 1 ):38--43.43.
SchenkmanSchenkman M et al ( 1
989) ¶Management of individualsM et al ( 1
989) ¶Management of individuals with Parkinson·s disease: Rationale and case study· with Parkinson·s disease: Rationale and case study·
Physical Therapy 69(11),944Physical Therapy 69(11),944² ²955 955
StallibrassStallibrass C ( 1997) ¶ An evaluation of the AlexanderC ( 1997) ¶ An evaluation of the Alexander
technique for the management of disability intechnique for the management of disability inParkinson·s diseaseParkinson·s disease ² ² a preliminary a preliminary Reha b ilitation Reha b ilitation
11,8 11,8² ²12 12
REFERENCEREFERENCE SchenkmanSchenkman M,M, CutsonCutson TM, TM, KuchibhatlaKuchibhatla M, ChandlerM, Chandler
JM PiJM Pi CF R L t l E i t iCF R L t l E i t i

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 184/186
JM,Pieper JM,Pieper CF, Ray L, et al. Exercise to improveCF, Ray L, et al. Exercise to improve
spinal flexibility and function for people withspinal flexibility and function for people with Parkinson·sParkinson·sdisease: adisease: a randomized,controlledrandomized,controlled trial. J Amtrial. J Am GeriatrGeriatr SocSoc1998;46:12071998;46:1207--16.16.
Schrag Schrag A, A, Jahanshahi Jahanshahi M, Quinn N. How doesM, Quinn N. How doesParkinson·sParkinson·s diseaseaffectdiseaseaffect quality of life? A quality of life? A comparisoncomparison with quality of life in the general population. with quality of life in the general population. Mov Mov DisordDisord2000;15:11122000;15:1112 ² ² 11181118
Schrag Schrag A, A, Jahanshahi Jahanshahi M, Quinn N. What contributes tM, Quinn N. What contributes toquality oquality of life in patients with Parkinson·sof life in patients with Parkinson·s disease? Jdisease? JNeurolNeurosurg NeurolNeurosurg Psychiatry 2000;69(308):312.Psychiatry 2000;69(308):312.
REFERENCEREFERENCE Schultz JH,Schultz JH, LutheLuthe W. Autogenic therapy methods. New W. Autogenic therapy methods. New York:Gruen York:Gruen andand
Stratton. New York:Stratton. New York: GruenGruen and Stratton; 1969.and Stratton; 1969.
ll l bl b kk l l f d dl l f d d

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 185/186
StolzeStolze H,H, KlebeKlebe S,S, BaeckerBaecker C, et al. Prevalence of gait disorders inC, et al. Prevalence of gait disorders in
hospitalized neurological patients.hospitalized neurological patients. Mov Mov DisordDisord 2005;20:892005;20:89² ²94.94.
Thaut Thaut MH, McIntosh GC, Rice RR, Miller R A,MH, McIntosh GC, Rice RR, Miller R A, RathbunRathbun J,Brault J,Brault JM. JM.Rhythmic auditory stimulation in gait training Rhythmic auditory stimulation in gait training forParkinson·sforParkinson·sdisease patients.disease patients. Mov Mov DisordDisord 1996 Mar;11( 2 ):1931996 Mar;11( 2 ):193--200200
Wenning Wenning GK,GK, EbersbachEbersbach G,G, Verny Verny M,M, ChaudhuriChaudhuri KR,JellingerKR,Jellinger K,K,McKee A, et al. Progression of falls inMcKee A, et al. Progression of falls in postmortempostmortem--ConfirmedConfirmedparkinsonianparkinsonian disorders.disorders. Mov Mov DisordDisord 1999Nov;14( 6 ):9471999Nov;14( 6 ):947--50.50.
World Health Organisation ( 1980 ) The international classification of World Health Organisation ( 1980 ) The international classification of
impairments,disabilitiesimpairments,disabilities and handicapsand handicaps ² ² A
manual of A
manual of classificationclassificationrelating relating to the consequences of disease. Geneva; WHOto the consequences of disease. Geneva; WHO

8/3/2019 Irogue Seminar Presentation October 2010
http://slidepdf.com/reader/full/irogue-seminar-presentation-october-2010 186/186
THANK YOU VERY MUCH FOR YOUR ATTENTION
QUESTIONS AND COMMENTQUESTIONS AND COMMENT..