Embed Size (px)
Citation preview
European Journal of Obstetrics & Gynecology and Reproductive Biology xxx (2014) xxx–xxx
G ModelEURO 8552 No. of Pages 6
Investigation of diagnostic potentials of nine different biomarkers inendometriosis
Erdem Ozhan a, Arif Kokcu a,*, Keramettin Yanik b, Murat Gunaydin b
aDepartment of Obstetrics and Gynecology, Faculty of Medicine, University of Ondokuz Mayis, Samsun, TurkeybDepartment of Medical Microbiology, Faculty of Medicine, University of Ondokuz Mayis, Samsun, Turkey
A R T I C L E I N F O
Article history:Received 7 March 2014Received in revised form 21 April 2014Accepted 22 April 2014
Keywords:EndometriosisSerum biomarkersCA125Syntaxin-5Laminin-1
A B S T R A C T
Objective: To investigate the diagnostic potentials of the serum levels of nine different biomarkers inendometriosis.Study design: In this case-controlled, prospective clinical study, 80 women underwent laparoscopy orlaparotomy with a preliminary diagnosis of chronic pelvic pain, severe secondary dysmenorrhea,infertility, pelvic endometriosis or pelvic mass. The 60 women with confirmed pelvic endometriosisconstituted the endometriosis group, and the other 20 women without endometriosis constituted thecontrol group.Preoperative blood samples were obtained for serum biomarker measurements. Serum levels of ninedifferent serum biomarkers including a-enolase, macrophage migration inhibitory factor, leptin,interleukin-8, anti-endometrial antibody, phosphoinositide dependent protein kinase 1, CA125,syntaxin-5, and laminin-1 were measured concurrently and compared between the control andendometriosis groups, and among control group and endometriosis subgroups including stage I, stage II,stage III and stage IV endometriosis.Results: The serum levels of a-enolase, macrophage migration inhibitory factor, leptin, interleukin-8 andantiendometrial antibodies showed a statistically significant difference neither between control andendometriosis groups nor among control group and endometriosis subgroups. The serum levels ofCA125, syntaxin-5 and laminin-1 showed a statistically significant difference both between the controland endometriosis groups (p < 0.01) and among control group and endometriosis subgroups (p < 0.01).Serum levels of laminin-1 in stage II and IV endometriosis; syntaxin-5 in stage I and II endometriosis; andCA125 in stage III and IV endometriosis were found to have the different levels compared to controlgroup.Conclusions: These findings show that the concurrent measurement of CA125, syntaxin-5 and laminin-1might be a useful non-invasive test in strengthening the diagnosis of endometriosis and in predicting itsseverity.
ã 2014 Elsevier Ireland Ltd. All rights reserved.
Contents lists available at ScienceDirect
European Journal of Obstetrics & Gynecology andReproductive Biology
journal homepage: www.elsevier .com/ locate /e jogrb
Introduction
Endometriosis is a common gynecological disorder affecting 7–10% women in the reproductive years. Prevalence among those withinfertility and chronic pelvic pain is reported high between 20 and90%. Endometriotic patients often have symptoms such asdysmenorrhea, coital pain and infertility. These symptoms ex-tremely disturb the quality of life of premenopausal women [1,2]. At
* Corresponding author at: Department of Obstetrics and Gynecology, School ofMedicine, University of Ondokuz Mayis, Kurupelit, 55139 Samsun, Turkey. Tel.: +900362 3121919x2452; fax: +90 362 4576029.
E-mail address: [email protected] (A. Kokcu).
http://dx.doi.org/10.1016/j.ejogrb.2014.04.0370301-2115/ã 2014 Elsevier Ireland Ltd. All rights reserved.
Please cite this article in press as: Ozhan E, et al. Investigation of diagnObstet Gynecol (2014), http://dx.doi.org/10.1016/j.ejogrb.2014.04.037
present, the definitive diagnosis of endometriosis requires surgerybecause imaging techniques, such as ultrasound and magneticresonance imaging, have not been shown to be reliable in thediagnosis or staging of the disease. Direct inspection of theabdominal cavity is recommended for the diagnosis of this disorderby means of laparoscopy or laparotomy [2,3]. The gold standard forthe diagnosis of endometriosis is diagnostic laparoscopy; however,it is an invasive procedure that requires general anesthesia andsurgical skill and is also not without hazards, which can includemajor vessel or bowel injury. Moreover, visual inspection of thepelvis has major limitations, particularly for the diagnosis ofretroperitoneal and deep infiltrating lesions [4].
Endometriosis is a pelvic inflammatory condition involving adysfunction in immune-related cells and macrophages within the
ostic potentials of nine different biomarkers in endometriosis. Eur J

2 E. Ozhan et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 2 xxx (2014) xxx–xxx
G ModelEURO 8552 No. of Pages 6
peritoneum secreting a number of products, mainly cytokines andgrowth factors [5]. An intense inflammatory reaction with elevatedpro-inflammatory cytokines and angiogenic factors, mobilizationof fibroblasts and proliferation of connective tissue characterizesendometriosis but whether these phenomena are secondary to thedisease remains elusive [6]. In an effort to find a less-invasivemethod for diagnosing endometriosis, and based on the fact thatendometriosis induces a local, and also a likely systemic,inflammatory process, numerous studies have focused on markersof inflammation in the peritoneal fluid and/or serum of womenwho have the disease. It has been shown that many inflammatoryand immunological biomarkers are provoked in patients withendometriosis [3,7].
In this case-controlled, prospective clinical study, we aimed toinvestigate the diagnostic potentials for endometriosis of ninedifferent biomarkers. We performed biomarker measurements inserum because its procurement is truly noninvasive. Most studieshave investigated these biomarkers individually; therefore, wemeasured concurrently the serum levels of the nine biomarkers inthe study groups.
Materials and methods
This study was performed in the Department of Gynecology ofUniversity of Ondokuz Mayis in Turkey, over the course of 1 year.The women recruited in this study provided informed consent for aresearch protocol approved by the Ethics Committee on humanresearch of the University. The study included the womenundergoing laparoscopy or laparotomy with a preliminarydiagnosis of chronic pelvic pain, severe secondary dysmenorrhea,infertility, pelvic endometriosis or pelvic mass. The women withlaparoscopically or laparotomically confirmed pelvic endometri-osis constituted the endometriosis group, and those withoutendometriosis constituted the control group. Endometriosis stageswere determined according to the Revised American Society forReproductive Medicine classification [8]. The subjects withautoimmune diseases, pelvic inflammatory disease, any malig-nancy, a history of delivery or abortion within the last six months,any endocrine disease, menopause, premature ovarian failure,menses, other pelvic masses out of endometrial adhesions orendometrioma, any anti-inflammatory or hormone medicationwithin the last three months before operation, were excluded fromthe study.
Blood samples were obtained 1–2 h before the operation. Thesesamples were centrifuged at 5000 rpm for 5 min to separate thecell pellet and the supernatant. The sera were then stored at �41 �Cuntil assayed. The measurements of serum biomarkers wereperformed using micro-ELISA method by the ELISA reader(awareness technology well model, USA) in the ELISA laboratory.
Table 1Characteristics of ELISA kits used for the measurements of serum biomarkers.
Serumbiomarkers
ELISA kits used for measurement
Enolase (ENO1/ENO1L1/MBPB1/MBPB1) ELISA kit, Cusabio, Belgium
MIF Human MIF ELISA kit, Cusabio, Belgium
Leptin Leptin micro ELISA kit, Diasourge, Belgium
IL-8 IL-8 micro ELISA kit, Diasourge, Belgium
AEA Human endometrium antibody (EMab) ELISA kit, Cusabio, Belgiu
PDPK1 Micro ELISA kit for phosphoinositide dependent protein kinase 1
BelgiumCA125 Human carbonhydrate antigen 125 ELISA kit, Cusabio, Belgium
STX-5 Human syntaxin-5 ELISA kit, Cusabio, Belgium
LN-1 Human laminin micro ELISA kit, USCN, Belgium
MIF: macrophage migration inhibitory factor, IL-8: interleukin-8, AEA: antiendometrial aLN-1: laminin-1.
Please cite this article in press as: Ozhan E, et al. Investigation of diagnObstet Gynecol (2014), http://dx.doi.org/10.1016/j.ejogrb.2014.04.037
Detection range, inter-assay and intra-assay coefficients ofvariation in addition to company addresses of the ELISA kits usedfor the biomarker measurements were shown in Table 1.
The serum levels of biomarkers including serum cancerantigen 125 (CA125), syntaxin5 (STX-5), laminin-1 (LN-1),a-enolase (enolase), macrophage migration inhibitory factor(MIF), leptin, interleukin-8 (IL-8), antiendometrial antibodies(AEA) and phosphoinositide dependent protein kinase 1 (PDPK1)were measured and compared both between control andendometriosis groups, and among control group and endometri-osis subgroups including stage I, stage II, stage III and stage IVendometriosis.
Statistical analysis was performed using the SPSS 15.0 software(SPSS, Inc., Chicago, IL). The comparison of the demographiccharacteristics between the groups was performed using student ttest. Kruskal–Wallis variance analysis and then a Mann–Whitney Utest were used to compare the group differences of biomarkerconcentrations. To identify the group differences, an optimal cut-off value for each biomarker using receiver operator curves (ROC)was selected. The sensitivity and specificity for each biomarkerwere determined by using ROC curves. The effects of the biomarkercombinations to distinguish between the endometriosis andcontrol groups were investigated by multivariate logistic regres-sion analysis. Nominal variables were evaluated using Pearson’sChi-square test. The levels of biomarkers were expressed asmedian and inter-quartile range (IQR), and a value of p < 0.05 wasaccepted statistically significant.
Results
The study included 60 women in the endometriosis group and20 women in the control group. The mean age was 32.33 � 7.01 inthe endometriosis group and 34.20 � 6.88 years in the controlgroup. The mean body mass index (BMI) was 23.75 � 4.39 in theendometriosis group and 24.89 � 5.10 kg/m2 in the control group.The mean age and the mean BMI between the groups were notstatistically different (p > 0.05, p > 0.05 respectively). The compari-son of age and BMI between the control group and endometriosissubgroups was shown in the Table 2.
Any statistically significant difference was not found betweenenolase, MIF, leptin, IL-8, AEA and PDPK1 median levels ofendometriosis and control groups. Also, there was not a statisti-cally significant difference in terms of the levels of these sixbiomarkers among control group and endometriosis subgroupsincluding stages I, II, III and IV endometriosis. However, CA125,STX-5 and LN-1 levels showed a statistically significant differenceboth between the control and endometriosis groups (p < 0.01) andamong control group and endometriosis subgroups (p < 0.01)(Tables 3 and 4).
Detection range Intra-assayprecision
Inter-assayprecision
1.25–80 ng/mL CV < 8% CV < 10%125–8000 pg/mL CV < 8% CV < 10%>0,04 ng/mL – –
>1,1 pg/mL – –
m Absorbance opticdensity
CV < 15% CV < 15%
(PDPK1), USCN, 0.156–10 ng/mL CV < 10% CV < 12%
15–300 U/mL CV < 15% CV < 20%23.4–1500 ng/mL CV < 8% CV < 10%78–5000 pg/mL CV < 10% CV < 12%
ntibodies, PDPK1: phosphoinositide dependent protein kinase 1, STX-5: syntaxin5,
ostic potentials of nine different biomarkers in endometriosis. Eur J
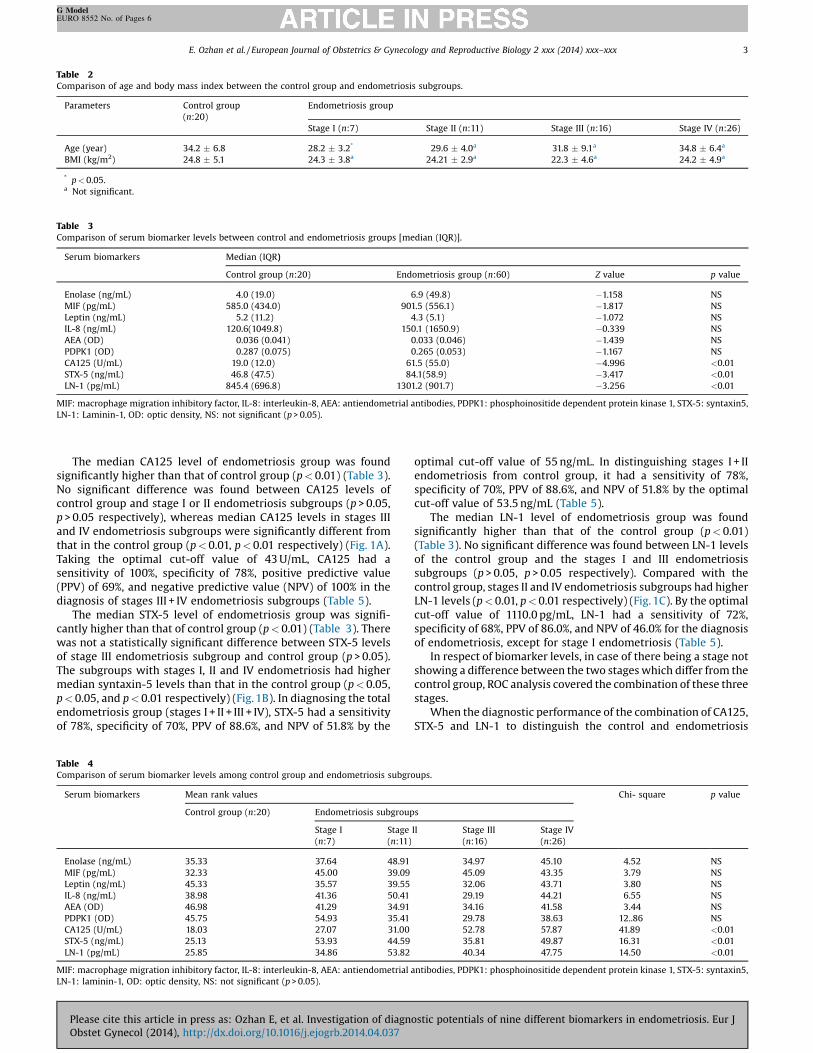
Table 2Comparison of age and body mass index between the control group and endometriosis subgroups.
Parameters Control group(n:20)
Endometriosis group
Stage I (n:7) Stage II (n:11) Stage III (n:16) Stage IV (n:26)
Age (year) 34.2 � 6.8 28.2 � 3.2* 29.6 � 4.0a 31.8 � 9.1a 34.8 � 6.4a
BMI (kg/m2) 24.8 � 5.1 24.3 � 3.8a 24.21 � 2.9a 22.3 � 4.6a 24.2 � 4.9a
* p < 0.05.a Not significant.
Table 3Comparison of serum biomarker levels between control and endometriosis groups [median (IQR)].
Serum biomarkers Median (IQR)
Control group (n:20) Endometriosis group (n:60) Z value p value
Enolase (ng/mL) 4.0 (19.0) 6.9 (49.8) �1.158 NSMIF (pg/mL) 585.0 (434.0) 901.5 (556.1) �1.817 NSLeptin (ng/mL) 5.2 (11.2) 4.3 (5.1) �1.072 NSIL-8 (ng/mL) 120.6(1049.8) 150.1 (1650.9) �0.339 NSAEA (OD) 0.036 (0.041) 0.033 (0.046) �1.439 NSPDPK1 (OD) 0.287 (0.075) 0.265 (0.053) �1.167 NSCA125 (U/mL) 19.0 (12.0) 61.5 (55.0) �4.996 <0.01STX-5 (ng/mL) 46.8 (47.5) 84.1(58.9) �3.417 <0.01LN-1 (pg/mL) 845.4 (696.8) 1301.2 (901.7) �3.256 <0.01
MIF: macrophage migration inhibitory factor, IL-8: interleukin-8, AEA: antiendometrial antibodies, PDPK1: phosphoinositide dependent protein kinase 1, STX-5: syntaxin5,LN-1: Laminin-1, OD: optic density, NS: not significant (p > 0.05).
E. Ozhan et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 2 xxx (2014) xxx–xxx 3
G ModelEURO 8552 No. of Pages 6
The median CA125 level of endometriosis group was foundsignificantly higher than that of control group (p < 0.01) (Table 3).No significant difference was found between CA125 levels ofcontrol group and stage I or II endometriosis subgroups (p > 0.05,p > 0.05 respectively), whereas median CA125 levels in stages IIIand IV endometriosis subgroups were significantly different fromthat in the control group (p < 0.01, p < 0.01 respectively) (Fig. 1A).Taking the optimal cut-off value of 43 U/mL, CA125 had asensitivity of 100%, specificity of 78%, positive predictive value(PPV) of 69%, and negative predictive value (NPV) of 100% in thediagnosis of stages III + IV endometriosis subgroups (Table 5).
The median STX-5 level of endometriosis group was signifi-cantly higher than that of control group (p < 0.01) (Table 3). Therewas not a statistically significant difference between STX-5 levelsof stage III endometriosis subgroup and control group (p > 0.05).The subgroups with stages I, II and IV endometriosis had highermedian syntaxin-5 levels than that in the control group (p < 0.05,p < 0.05, and p < 0.01 respectively) (Fig. 1B). In diagnosing the totalendometriosis group (stages I + II + III + IV), STX-5 had a sensitivityof 78%, specificity of 70%, PPV of 88.6%, and NPV of 51.8% by the
Table 4Comparison of serum biomarker levels among control group and endometriosis subgro
Serum biomarkers Mean rank values
Control group (n:20) Endometriosis subgroup
Stage I(n:7)
Stage
(n:11)
Enolase (ng/mL) 35.33 37.64 48.91
MIF (pg/mL) 32.33 45.00 39.09
Leptin (ng/mL) 45.33 35.57 39.55
IL-8 (ng/mL) 38.98 41.36 50.41
AEA (OD) 46.98 41.29 34.91
PDPK1 (OD) 45.75 54.93 35.41
CA125 (U/mL) 18.03 27.07 31.00
STX-5 (ng/mL) 25.13 53.93 44.59
LN-1 (pg/mL) 25.85 34.86 53.82
MIF: macrophage migration inhibitory factor, IL-8: interleukin-8, AEA: antiendometrial aLN-1: laminin-1, OD: optic density, NS: not significant (p > 0.05).
Please cite this article in press as: Ozhan E, et al. Investigation of diagnObstet Gynecol (2014), http://dx.doi.org/10.1016/j.ejogrb.2014.04.037
optimal cut-off value of 55 ng/mL. In distinguishing stages I + IIendometriosis from control group, it had a sensitivity of 78%,specificity of 70%, PPV of 88.6%, and NPV of 51.8% by the optimalcut-off value of 53.5 ng/mL (Table 5).
The median LN-1 level of endometriosis group was foundsignificantly higher than that of the control group (p < 0.01)(Table 3). No significant difference was found between LN-1 levelsof the control group and the stages I and III endometriosissubgroups (p > 0.05, p > 0.05 respectively). Compared with thecontrol group, stages II and IV endometriosis subgroups had higherLN-1 levels (p < 0.01, p < 0.01 respectively) (Fig. 1C). By the optimalcut-off value of 1110.0 pg/mL, LN-1 had a sensitivity of 72%,specificity of 68%, PPV of 86.0%, and NPV of 46.0% for the diagnosisof endometriosis, except for stage I endometriosis (Table 5).
In respect of biomarker levels, in case of there being a stage notshowing a difference between the two stages which differ from thecontrol group, ROC analysis covered the combination of these threestages.
When the diagnostic performance of the combination of CA125,STX-5 and LN-1 to distinguish the control and endometriosis
ups.
Chi- square p value
s
II Stage III(n:16)
Stage IV(n:26)
34.97 45.10 4.52 NS45.09 43.35 3.79 NS32.06 43.71 3.80 NS29.19 44.21 6.55 NS34.16 41.58 3.44 NS29.78 38.63 12..86 NS52.78 57.87 41.89 <0.0135.81 49.87 16.31 <0.0140.34 47.75 14.50 <0.01
ntibodies, PDPK1: phosphoinositide dependent protein kinase 1, STX-5: syntaxin5,
ostic potentials of nine different biomarkers in endometriosis. Eur J

Fig. 1A. Comparison of serum CA125 levels between control group andendometriosis subgroups (stages). NS not significant (p > 0.05), ** p < 0.01. Fig. 1B. Comparison of serum anti-syntaxin-5 autoantibodies levels between
control group and endometriosis subgroups (stages). NS not significant (p > 0.05), *p < 0.05, ** p < 0.01.
4 E. Ozhan et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 2 xxx (2014) xxx–xxx
G ModelEURO 8552 No. of Pages 6
groups was analyzed, it was found to be sensitivity of 95.0%,specificity of 70.0%, PPV of 90.5%, NPV of 82.4% and accuracy of88.7% (Table 5).
Comments
Autoantibodies against alpha-enolase, a glycolytic enzyme,have been frequently associated with autoimmune diseases;however, the genesis and function of these autoantibodies arenot known [9]. Nabeta et al. [2] reported that anti-a-enolaseautoantibody levels in endometriotic patients were significantlyelevated compared with both healthy and diseased controls. MIFlevels in the peritoneal fluid have been noted in some studies to behigher in women with endometriosis [3,10,11]. Morin et al. [10]demonstrated that MIF concentration is significantly increased inthe peripheral blood of patients suffering from endometriosis andvaried according to the severity of the disease. Some studies haveshown the presence of increased levels of leptin in the peritonealfluid of patients with endometriosis [1,12–15]. Malhotra et al. [1]reported that IL-8 level is raised in peritoneal fluid of women withendometriosis reflecting inflammation and dysregulated immu-nomodulation. In some studies, serum IL-8 has been found to behigher in women with endometriosis [16–18]. In other studies thatassessed IL-8 levels, differences could not be demonstrated[3,5,19]. Randall et al. [20] reported that there is a correlationbetween circulating AEA and surgically verified endometriosis.Fernandéz-Shaw et al. [21] showed that there were no significantdifferences in serum AEA concentrations before and aftertreatment, or between women with endometriosis and without
Table 5ROC analysis results of biomarkers to discriminate the endometriosis subgroups from
Serum biomarkers Endometriosis subgroups Cut-off value Sensitivity %
CA125 (U/mL) Stage IIII + IV(n:42)
43.0 100.0
STX-5 (ng/mL) Stage I + II + III + IV(n:60)
55.0 78.3
STX-5 (ng/mL) Stage I + II(n:18)
53.5 70.0
LN-1 (pg/mL) Stage II + III + IV(n:53)
1110.0 72.0
CA125 + STX-5 + LN-1 Stage I + II + III + IV (n:60) – 95.0
PPV: positive predictive value, NPV: negative predictive value, AUC: area under curve.
Please cite this article in press as: Ozhan E, et al. Investigation of diagnObstet Gynecol (2014), http://dx.doi.org/10.1016/j.ejogrb.2014.04.037
endometriosis. In our study, serum levels of none of anti-enolase,MIF, leptin, IL-8 and AEA showed a statistically significantdifference either between the control and endometriosis groupsor among the control group and endometriosis subgroups (Tables 3and 4).
Phosphoinositide-dependent protein kinase-1 (PDPK1) hasimportant roles in the activation and function of immune cells,different cellular functions such as glucose metabolism, cellularproliferation, cellular survival, and angiogenesis. It is essential for Bcell development and T cell activation [22–24]. Moreover, PDPK1has been reported to be involved in the genesis of non-small celllung cancer, pancreatic carcinoma, and human breast cancer[22,25,26]. Down regulation of PDPK1 levels inhibits migration andexperimental metastasis of human breast cancer cells [22].Depending on its above-mentioned characteristics, we thoughtthat PDPK1 levels might be different in women with endometriosisand compared the serum levels of PDPK1 between the groups withand without endometriosis. However, we found a statisticallysignificant difference neither between control and endometriosisgroups nor among control group and endometriosis subgroups(Tables 3 and 4).
CA125 is currently the only clinical marker for endometriosis.However, the sensitivity of CA125 in the diagnosis of this disease isnot high, especially in the early stages [7]. Elevated serum CA125levels, other than in endometriosis and ovarian cancers, can be seenin malignancies of different origin including non-ovarian gyneco-logical cancer, such as endometrial, pancreatic, lung, breast and
control group.
Specificity % PPV % NPV % Accuracy % ROC AUC Z value p value
78.0 69.0 100.0 83.0 0.949 16.6 <0.01
70.0 88.6 51.8 73.7 0.756 4.24 <0.01
83.3 82.3 71.4 92.1 0.783 3.66 <0.01
68.2 86.0 46.0 67.1 0.752 4.05 <0.01
70.0 90.5 82.4 88.7 – – <0.001
ostic potentials of nine different biomarkers in endometriosis. Eur J

Fig. 1C. Comparison of serum anti-laminin-1 autoantibodies levels betweencontrol group and endometriosis subgroups (stages). NS not significant (p > 0.05), **p < 0.01.
E. Ozhan et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 2 xxx (2014) xxx–xxx 5
G ModelEURO 8552 No. of Pages 6
colorectal cancer, and also in non-gynecological diseases such astuberculosis, liver cirrhosis and also in physiological conditions suchas pregnancy or different phases of the menstrual cycle [27]. Even inadvancedcases, its sensitivity is low (stages3 and 4 endometriosis. Ina meta-analysis, the sensitivity in patients with endometriosis hasbeen found to be between 13%and 36% [28]. In our study, the medianCA125 level of endometriosis group was significantly higher thanthatof control group(p < 0.01) (Table 3). There was not a statisticallysignificant difference between CA125 levels of control group andstages I or II endometriosis subgroups (Fig.1A). However, CA125 hada good diagnostic performance in diagnosing stages III + IVendometriosis subgroups, with a sensitivity of 100%, specificity of78% and area under curve (AUC) of 0.949 (Table 5). These findingsverified that CA125 is not a sensitive test for the diagnosis of theearly stage endometriosis (stages I and II).
The soluble N-ethylmaleimide–sensitive factor accessory pro-tein receptor (SNARE) proteins mediate the fusion events in cellmembrane. STX-5 is a member of the syntaxin-family of SNAREproteins. It is a vesicular membrane fusion protein receptor inendoplasmic reticulum membrane [7,29]. Nabeta et al. [7] reportedthat anti-STX-5 showed a high sensitivity (80%) at stage IIendometriosis. They determined that the mean levels of anti-STX-5 at stages III and IV were rather lower than that at stage II. Inthe present study, the endometriosis group had significantlyhigher STX-5 level than that in the control group (p < 0.01)(Table 3). The subgroups with stages I, II and IV endometriosis hadhigher STX-5 levels than that of the control group (p < 0.05,p < 0.05, and p < 0.01 respectively) (Fig.1B). STX-5 had a sensitivityof 78%, specificity of 70%, and AUC of 0.756 in diagnosing totalendometriosis cases (stages I + II + III + IV). In diagnosing stages I + IIendometriosis, the same values were 70.0, 83.3, and 0.783respectively (Table 5). It is seen that STX-5 measurement maybe a useful non-invasive test in diagnosing both the early-stage andthe advanced stage endometriosis.
Laminins, including LN-1, are located in the basementmembrane surrounding glandular epithelial cells and vascularendothelial cells in both endometrium and endometriotic lesions.Various components of the extracellular matrix are involved in theadhesion process of endometrial cells, and laminins also play a rolein this process [30,31]. The mRNA encoding laminin alpha1, -beta1and -gamma1 chains are found to be expressed in 90% ofendometrial lesions [6]. Inagaki et al. [30,32] and Caccavo et al.[8] showed that IgG aLN-1 autoantibodies are significantly
Please cite this article in press as: Ozhan E, et al. Investigation of diagnObstet Gynecol (2014), http://dx.doi.org/10.1016/j.ejogrb.2014.04.037
associated with endometriosis in infertile patients. In our study,the endometriosis group had a higher LN-1 level than that in thecontrol group (p < 0.01) (Table 3). LN-1 levels did not show asignificant difference in patients with stages I and III endometriosiscompared to the control group. However, its median level was seento be significantly higher in the stages II and IV endometriosissubgroups than that of the control group (p < 0.01, p < 0.01respectively) (Fig.1C). LN-1 had a sensitivity of 72%, specificity of68% and AUC of 0.752 in diagnosing endometriosis, except for stageI endometriosis (Table 5). Because stage III is an intermediategroup, its diagnostic sensitivity in endometriosis can be assumedto include more than two subgroups. However, it is difficult toexplain why stage III endometriosis had not higher STX-5 and LN1levels compared to the control group.
The combination of CA125, STX-5 and LN-1 to distinguish thecontrol and endometriosis groups had sensitivity of 95.0%,specificity of 70.0%, and accuracy of 88.7% (Table 5).
In conclusion, the concurrent measurement of the threebiomarkers including CA125, STX-5 and LN-1 might be a usefulnon-invasive test in strengthening the diagnosis of endometriosisand in predicting its severity. In the present study, because serumbiomarker measurements were performed concurrently on thesame patients and under the same conditions, we believe thatthese results are quite reliable. Of course, there is a need for moredetailed clinical studies including a larger number of women withand without endometriosis to clarify this subject.
Funding
This study was supported by the scientific research funding ofthe University of Ondokuz Mayis with the project number PYO.TIP.1904.12.038.
Acknowledgement
The authors thank Yuksel Bek, Ph.D., head of the BiostatisticsDepartment in the Faculty of Medicine at University of OndokuzMayis, for performing the statistical analyses of the study.
References
[1] Malhotra N, Karmakar D, Tripathi V, Luthra K, Kumar S. Correlation ofangiogenic cytokines-leptin and IL-8 in stage, type and presentation ofendometriosis. Gynecol. Endocrinol. 2012;28:224–7.
[2] Nabeta M, Abe Y, Kagawa L, et al. Identification of anti-a-enolase autoantibodyas a novel serum marker for endometriosis. Proteomics Clin. Appl.2009;3:1201–10.
[3] Seeber B, Sammel MD, Fan X, et al. Panel of markers can accurately predictendometriosis in a subset of patients. Fertil. Steril. 2008;89:1073–81.
[4] Othman Eel-D, Hornung D, Salem HT, Khalifa EA, El-Metwally TH, Al-Hendy A.Serum cytokines as biomarkers for nonsurgical prediction of endometriosis.Eur. J. Obstet. Gynecol. Reprod. Biol. 2008;137:240–6.
[5] Carmona F, Chapron C, Martínez-Zamora MÁ, et al. Ovarian endometrioma butnot deep infiltrating endometriosis is associated with increased serum levelsof interleukin-8 and interleukin-6. J. Reprod. Immunol. 2012;95:80–6.
[6] Carp HJ, Selmi C, Shoenfeld Y. The autoimmune bases of infertility andpregnancy loss. J. Autoimmun. 2012;38:J266–74.
[7] Nabeta M, Abe Y, Takaoka Y, Kusanagi Y, Ito M. Identification of anti-syntaxin 5autoantibody as a novel serum marker of endometriosis. J. Reprod. Immunol.2011;91:48–55.
[8] Caccavo D, Pellegrino NM, Totaro I, Vacca MP, Selvaggi L, Depalo R. Anti-laminin-1 antibodies in sera and follicular fluid of women with endometriosisundergoing in vitro fertilization. Int. J. Immunopathol. Pharmacol.2011;24:481–8.
[9] Gitlits VM, Toh BH, Sentry JW. Disease association, origin, and clinicalrelevance of autoantibodies to the glycolytic enzyme enolase. J. Investig. Med.2001;49:138–45 Review.
[10] Morin M, Bellehumeur C, Therriault MJ, Metz C, Maheux R, Akoum A. Elevatedlevels of macrophage migration inhibitory factor in the peripheral blood ofwomen with endometriosis. Fertil. Steril. 2005;83:865–72.
[11] Carli C, Leclerc P, Metz CN, Akoum A. Direct effect of macrophage migrationinhibitory factor on sperm function: possible involvement in endometriosis-associated infertility. Fertil. Steril. 2007;88:1240–7.
ostic potentials of nine different biomarkers in endometriosis. Eur J
6 E. Ozhan et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 2 xxx (2014) xxx–xxx
G ModelEURO 8552 No. of Pages 6
[12] Choi YS, Oh HK, Choi JH. Expression of adiponectin, leptin, and their receptorsin ovarian endometrioma. Fertil. Steril. 2013;100:135–41.
[13] Oh HK, Choi YS, Yang YI, Kim JH, Leung PC, Choi JH. Leptin receptor is inducedin endometriosis and leptin stimulates the growth of endometriotic epithelialcells through the JAK2/STAT3 and ERK pathways. Mol. Hum. Reprod.2013;19:160–8.
[14] Wu MH, Huang MF, Chang FM, Tsai SJ. Leptin on peritoneal macrophages ofpatients with endometriosis. Am. J. Reprod. Immunol. 2010;63:214–21.
[15] Barcz E, Milewski L, Radomski D, et al. A relationship between increasedperitoneal leptin levels and infertility in endometriosis. Gynecol. Endocrinol.2008;24:526–30.
[16] Gomez-Torres MJ, Acien P, Campos A, Velasco I. Embryotoxicity of peritonealfluid in women with endometriosis. Its relation with cytokines andlymphocyte populations. Hum. Reprod. 2002;17:777–81.
[17] Barcz E, Skopinska Rozewska E, Kaminski P, Demkow U, Bobrowska K,Marianowski L. Angiogenic activity and IL-8 concentrations in peritoneal fluidand sera in endometriosis. Int. J. Gynecol. Obstet. 2002;79:229–35.
[18] Calhaz-Jorge C, Costa AP, Santos MC, Palma-Carlos ML. Peritoneal fluidconcentrations of interleukin-8 in patients with endometriosis depend on theseverity of the disorder and are higher in the luteal phase. Hum. Reprod.2003;18:593–7.
[19] Socolov R, Butureanu S, Angioni S, et al. The value of serological markers in thediagnosis and prognosis of endometriosis: a prospective case-control study.Eur. J. Obstet. Gynecol. Reprod. Biol. 2011;154:215–7.
[20] Randall GW, Gantt PA, Poe-Zeigler RL, et al. Serum antiendometrialantibodies and diagnosis of endometriosis. Am. J. Reprod. Immunol.2007;58:374–82.
[21] Fernandéz-Shaw S, Kennedy SH, Hicks BR, Edmonds K, Starkey PM, Barlow DH.Anti-endometrial antibodies in women measured by an enzyme-linkedimmunosorbent assay. Hum. Reprod. 1996;11:1180–4.
Please cite this article in press as: Ozhan E, et al. Investigation of diagnObstet Gynecol (2014), http://dx.doi.org/10.1016/j.ejogrb.2014.04.037
[22] Fyffe C, Falasca M. 3-Phosphoinositide-dependent protein kinase-1 as anemerging target in the management of breast cancer. Cancer Manag. Res.2013;5:271–80.
[23] Kang JA, Jeong SP, Park D, Hayden MS, Ghosh S, Park SG. Transition fromheterotypic to homotypic PDK1 homodimerization is essential for TCR-mediated NF-kB activation. J. Immunol. 2013;190:4508–15.
[24] VenigallaRK, McGuireVA, Clarke R,et al. PDK1 regulates VDJ recombination, cell-cycle exit and survival during B-cell development. EMBO J. 2013;32:1008–22.
[25] Ye XW, Yu H, Jin YK, et al. miR-138 inhibits proliferation by targeting 3-phosphoinositide-dependent protein kinase-1 in non-small cell lung cancercells. Clin. Respir. J. 2014(January), doi:10.1111/crj.12100.
[26] Song SD, Zhou J, Zhou J, Zhao H, Cen JN, Li DC. MicroRNA-375 targets the 3-phosphoinositide-dependent protein kinase-1 gene in pancreatic carcinoma.Oncol. Lett. 2013;6:953–9.
[27] Anastasi E, Granato T, Falzarano R, et al. The use of HE4, CA125 and CA72-4biomarkers for differential diagnosis between ovarian endometrioma andepithelial ovarian cancer. J. Ovarian Res. 2013;6:44.
[28] Spaczynski RZ, Duleba AJ. Diagnosis of endometriosis. Semin. Reprod. Med.2003;21:193–207.
[29] Loranger SS, Linder ME. SNAP-25 traffics to the plasma membrane by asyntaxin-independent mechanism. J. Biol. Chem. 2002;277:34303–9.
[30] Inagaki J, Sugiura-Ogasawara M, Nomizu M, et al. An association of IgG anti-laminin-1 autoantibodies with endometriosis in infertile patients. Hum.Reprod. 2003;18:544–9.
[31] Inagaki J, Kondo A, Lopez LR, Shoenfeld Y, Matsuura E. Pregnancy loss andendometriosis: pathogenic role of anti-laminin-1 autoantibodies. Ann. N. Y.Acad. Sci. 2005;1051:174–84 Review.
[32] Inagaki J, Hao L, Nakatsuka M, et al. A possible mechanism of autoimmune-mediated infertility in women with endometriosis. Am. J. Reprod. Immunol.2011;66:90–9.
ostic potentials of nine different biomarkers in endometriosis. Eur J