Embed Size (px)
Citation preview
Introduction to Geriatric Medicine
Carolyn Clevenger, DNP, GNP-BCAssistant Professor, NHW School of Nursing
VA Geriatric Research, Education, & Clinical Center
Jonathan Flacker, MD AGSFChief, Section of Geriatrics and Gerotology
Associate ProfessorEmory University School of Medicine
Industry Disclosures- CKC
I believe none of the following industry relationships are relevant to the current educational activity:
Consultancies (within last 3 years)- None Research funding- None Speakers’ bureaus, stocks, patents, family employment by
industry- None
2
Industry Disclosures- JMF
External Industry Relationships * Company Name(s) Role
Equity, stock, or options in biomedical industry companies or publishers**
JNJ Stock
Board of Directors or officer Nope
Royalties from Emory or from external entity
Nope
Industry funds to Emory for my research
Nope
Other Nope
3
Learning Objectives
Understand important demographic trends in aging Be able to explain the concept of functional status Learn a framework for understanding basic
principles affect either recovery from, or treatment during, acute illness in older patients
4
What is Geriatrics?
Geriatrics is the branch of medical science that focuses on health promotion and the treatment of disease and disability in later life.
The American Geriatrics Society5
What is a Geriatrician?
A Geriatrician is a physician who is specially trained to prevent and manage the unique and often multiple health problems of older adults.
The American Geriatrics Society 6
What is a GNP?
Gerontological Nurse Practitioners (GNPs) are advanced practice nurses with specialized education in the diagnosis, treatment and management of acute and chronic conditions often found among older adults and generally associated with aging.
Gerontological Advanced Practice Nurses Association 7
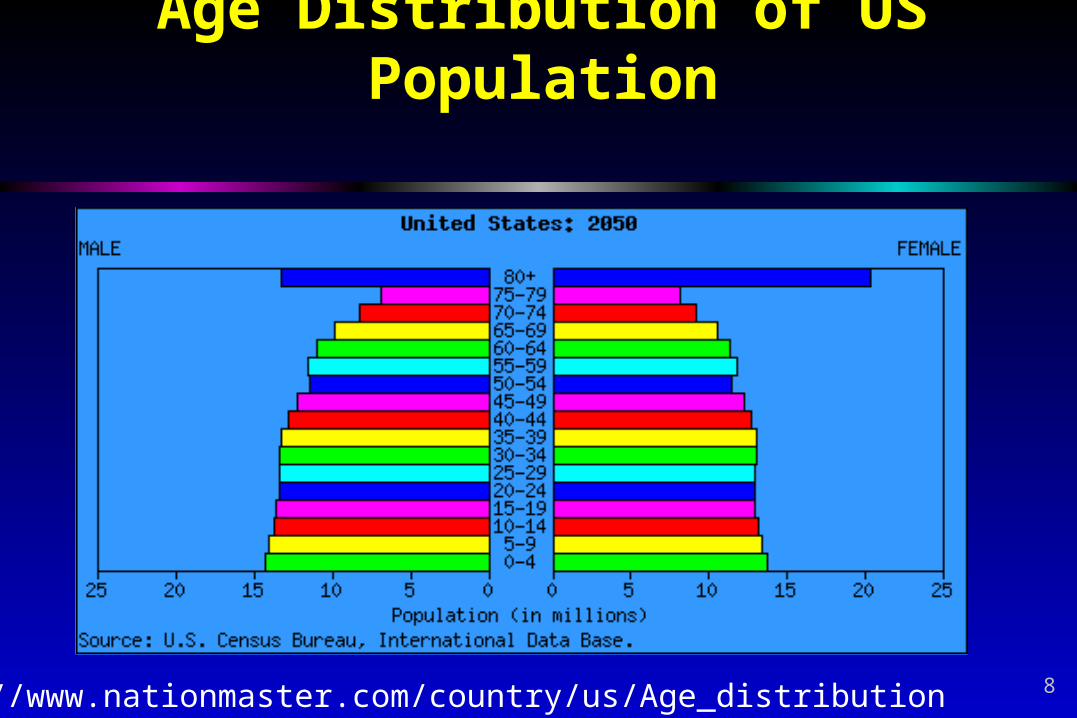
Age Distribution of US Population
http://www.nationmaster.com/country/us/Age_distribution 8

Aging in Georgia
9
The Emory University Reynolds Program
10
Basic Principles of Geriatrics
1. Aging is not a disease Disease happens to some, but aging
is not optional Aging does not generally cause
symptoms Successful aging is common
11

http://www.11alive.com/news/local/story.aspx?storyid=180571
12
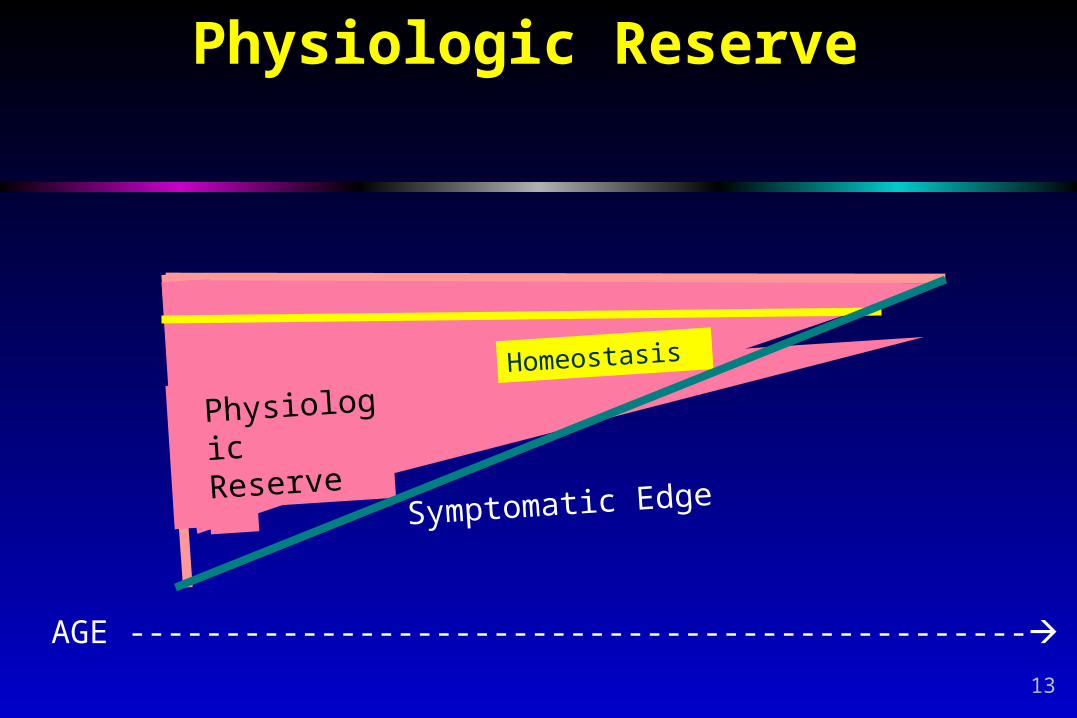
Physiologic Reserve
Physiologi
c Reserve
Homeostasis
AGE -----------------------------------------------
Symptomatic Edge
13
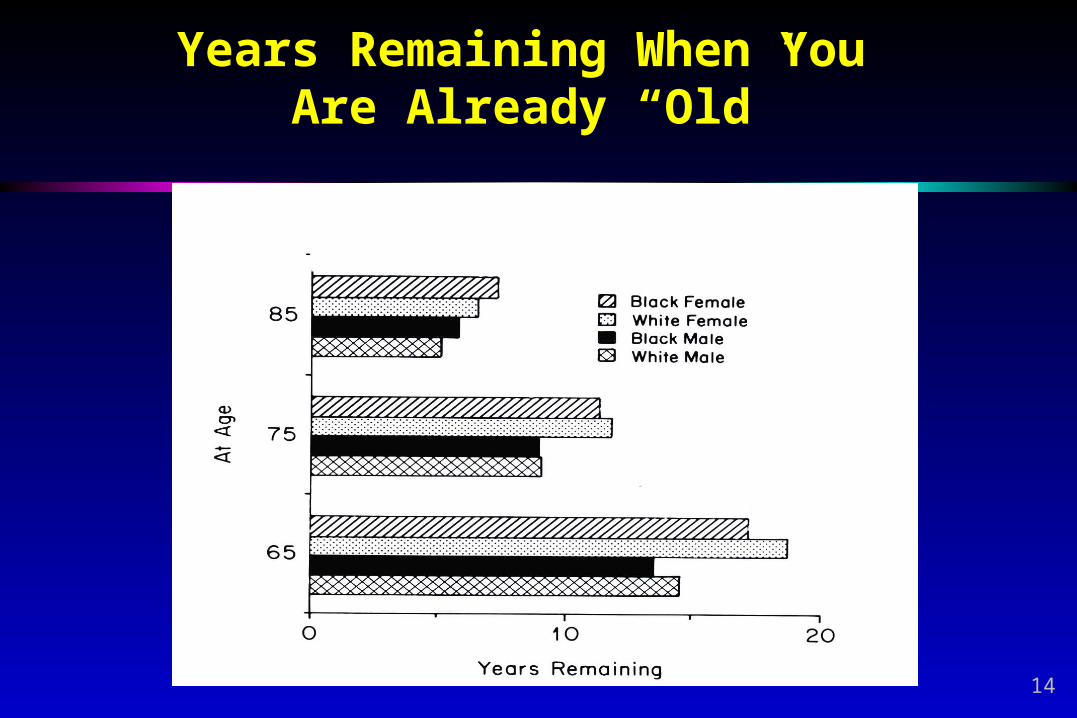
Years Remaining When You Are Already “Old”
14
Basic Principles of Geriatrics
2. Medical conditions in geriatric patients are commonly chronic and multiple, and multi-factorial in origin Acute illnesses are superimposed on
existing chronic conditions Treatment of one condition can affect
another Geriatric conditions usually have multiple
contributing factors
15
Juanita 86 year-old female comes to
the clinic for refill for thyroid med
Gait speed is slow and appears out of breath
History of: Hypothyroidism, hypertension, osteoarthritis, atrial fibrillation
Potentially new: heart failure, angina, anemia, lung disease, spinal stenosis
16
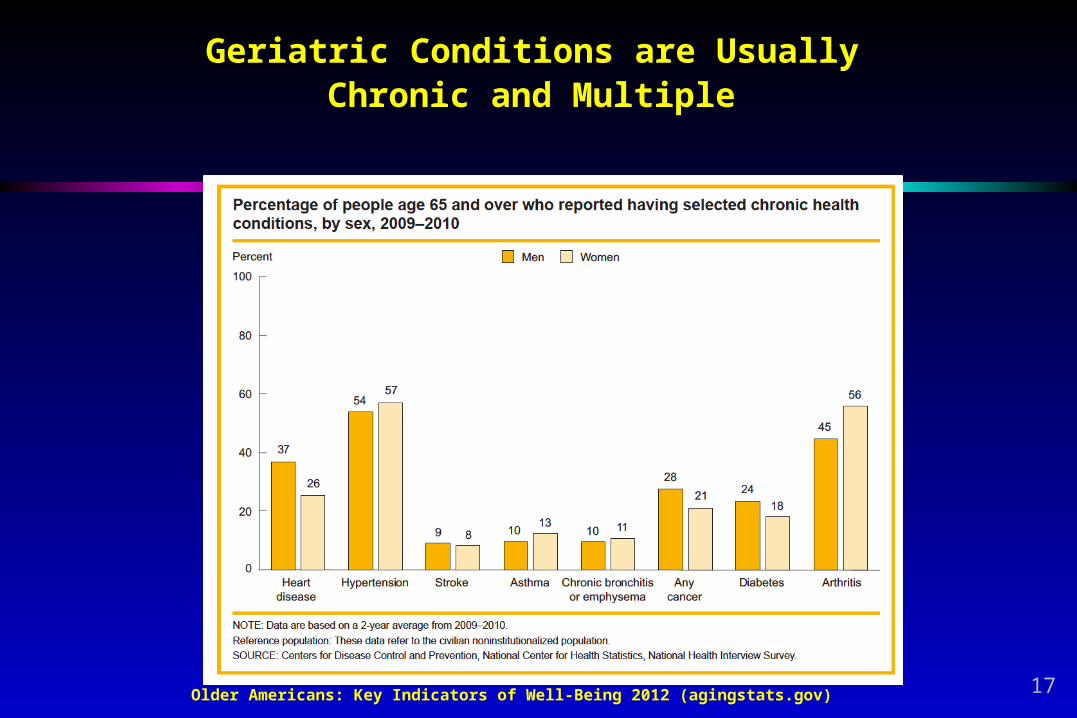
Older Americans: Key Indicators of Well-Being 2012 (agingstats.gov)
Geriatric Conditions are Usually Chronic and Multiple
17
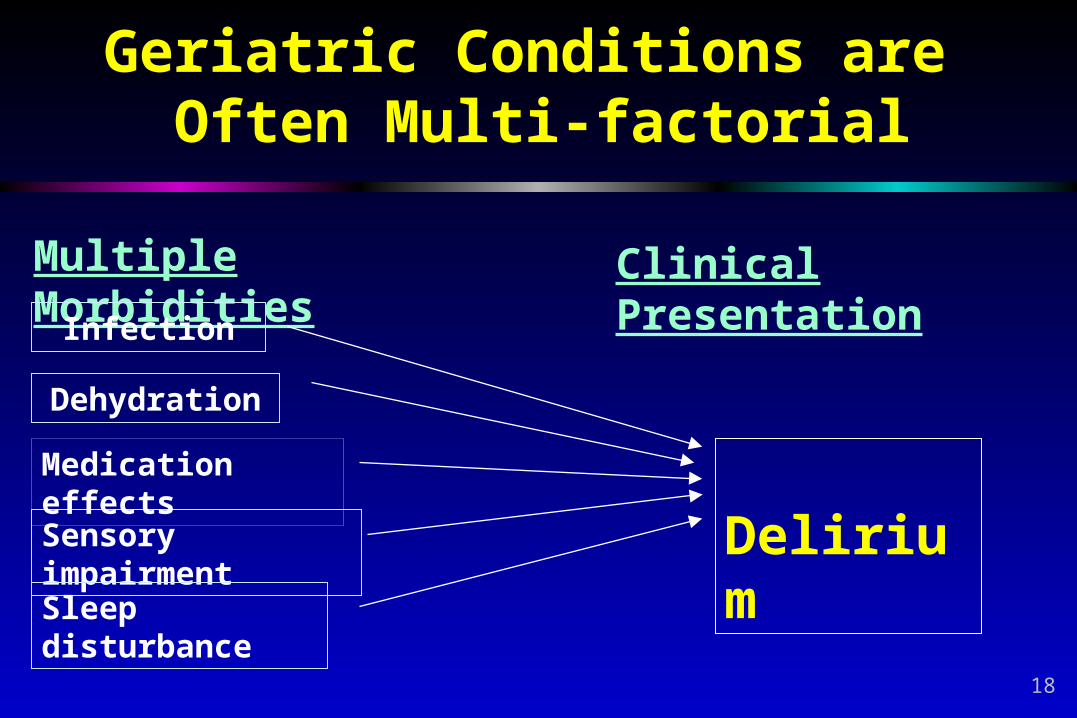
Geriatric Conditions are Often Multi-factorial
Multiple Morbidities Clinical Presentation
Delirium
Infection
Dehydration
Sensory impairment
Sleep disturbance
Medication effects
18
3. Reversible and treatable conditions are often under-diagnosed and under-treated in geriatric patients
Basic Principles of Geriatrics
19

Case
Ms J is in your clinic She is 80 years old and has hypertension and
stage II CKD You should of course ask her about?
20
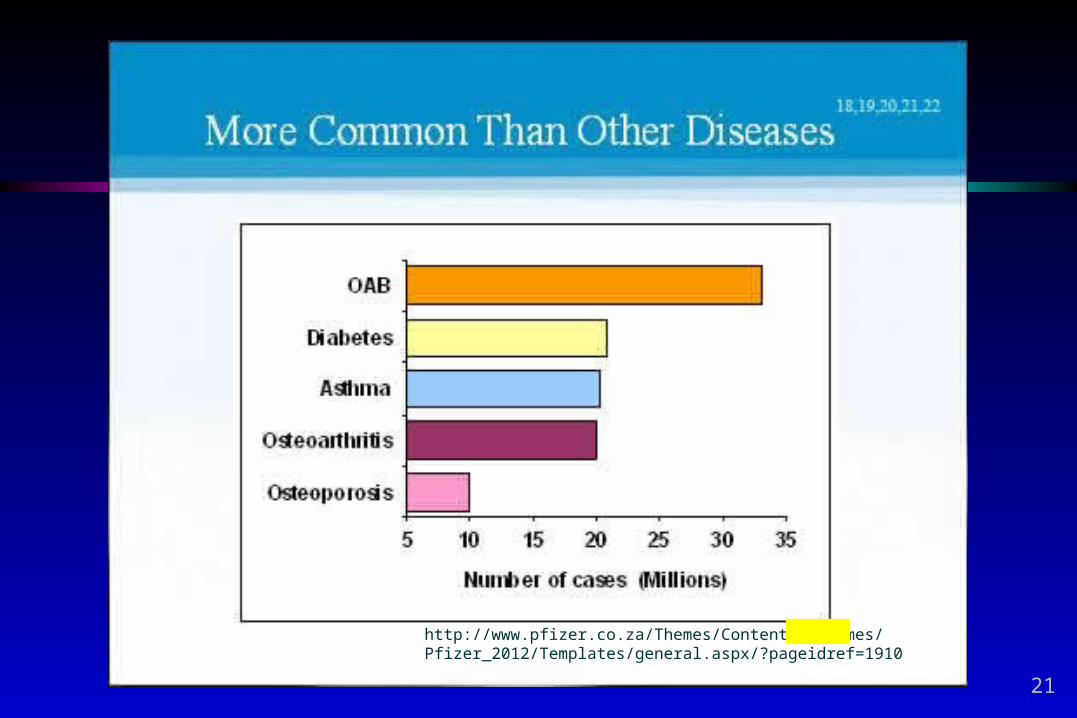
http://www.pfizer.co.za/Themes/Content%20Themes/Pfizer_2012/Templates/general.aspx/?pageidref=1910
21
Examples of Common, Treatable Geriatric Syndromes That are Often Overlooked
Constipation Incontinence Fatigue Dizziness Sleep disorders Gait instability
22
Basic Principles of Geriatrics
4. Functional ability and quality of life are critical outcomes in the geriatric population
23
John 84 year-old male with
vascular disease including dementia, diabetes, veinous insufficiency, obesity
Hospitalized for cellulitis/sepsis
Could no longer walk independently after prolonged bedrest
Moved to assisted living Profoundly depressed
24
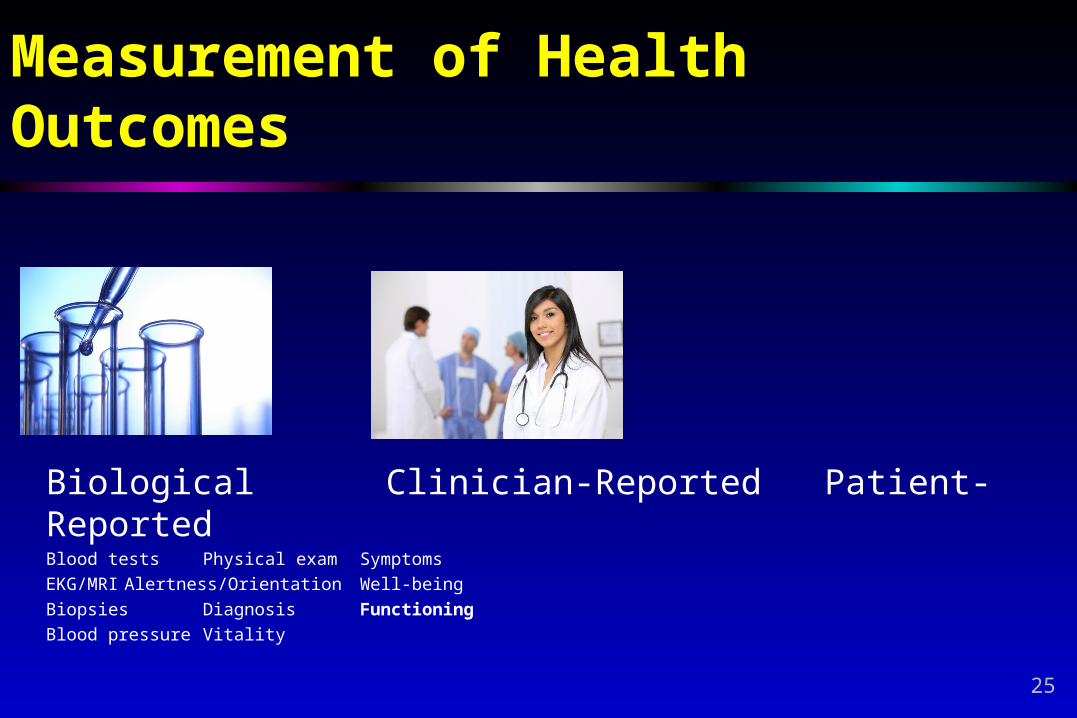
Measurement of Health Outcomes
Biological Clinician-Reported Patient-ReportedBlood tests Physical exam Symptoms
EKG/MRI Alertness/Orientation Well-being
Biopsies Diagnosis Functioning
Blood pressure Vitality
25
26
27
Basic Principles of Geriatrics
5. Social history, social circumstances, and available social support are essential aspects of managing geriatric patients
28
Case
Ms Malone is an 85 year old female admitted to the hospital from home for a pneumonia
Once he is better she should go __________
29
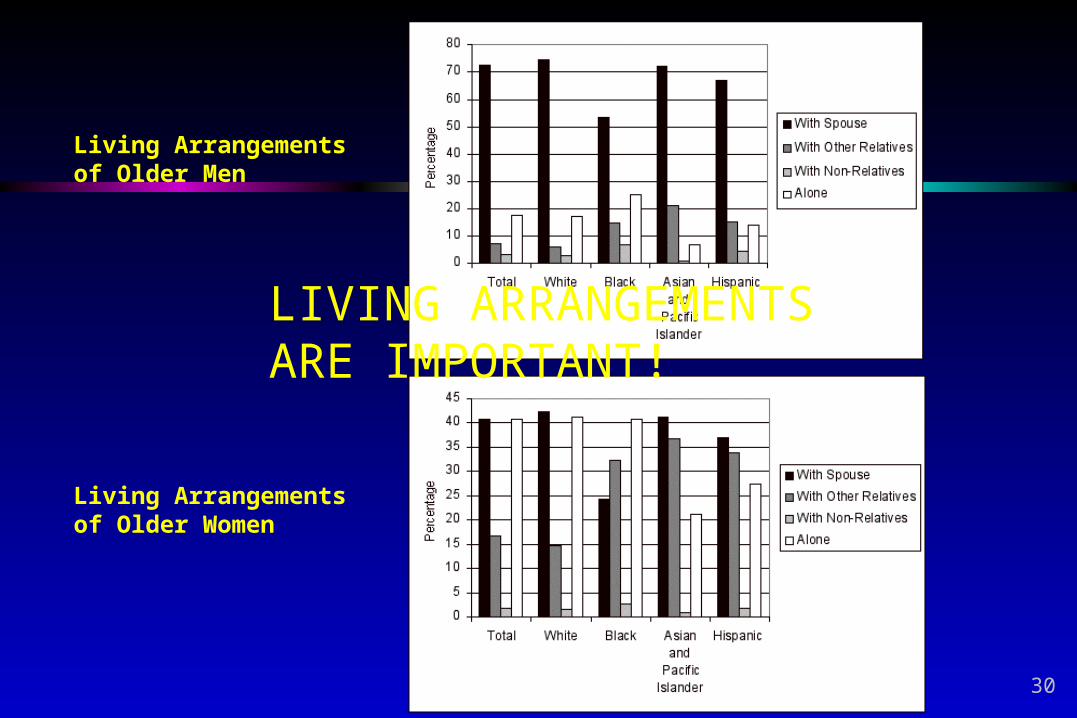
Living Arrangements of Older Men
Living Arrangements of Older Women
LIVING ARRANGEMENTS ARE IMPORTANT!
30
Hazards of Living at Home Alone
Isolation Poor nutrition Environmental hazards
and accidents Behavioral hazards
www.agingatlanta.com 404-463-3333 31

Basic Principles of Geriatrics
6. Geriatric care is commonly multidisciplinary
Multiple disciplines work together as an interprofessional team
32
MaryEllen 76-year old female with stroke;
great improvements in mobility, less so in cognition
Goals of care: to return to home to live independently
Structured family meeting on day 5 Patient and son MD and NP Physical and occupational therapy Social work and chaplain Psychologist
33
Team Members
Interdisciplinary Geriatric CareInterdisciplinary Geriatric Care
• Psychologists• Pharmacists• Housekeepers• Engineers• Pastoral care• IT support• Administration
•& Patient and Family
• Physicians• NPs, PAs• Nurses • Nurse’s Aides• Rehab therapists• Social workers• Dieticians
34
Principles of High-Functioning Teams
Clear roles and responsibilities Who does what? Who will take the lead in a given situation?
Shared mental model Same goal and general idea of how to achieve it
Mutual trust To back-up and monitor performance
Team orientation Believe that team based care is better than alone
Honest and clear communication Including negative feedback
35
Basic Principles of Geriatrics
7. Cognitive and affective disorders are highly prevalent and commonly undiagnosed at early stages
36
Case
Mr Tam is a 79 year old male brought to the clinic by his children who are concerned about weight loss
What must you consider?
37
Early cognitive impairment is commonly hidden and overlooked
Depression is commonly undiagnosed and under - treated
Behavioral symptoms such as agitation and aggression are very distressing and difficult to manage for family members
Cognitive and Affective Disorders
Cognitive and Affective Disorders
38
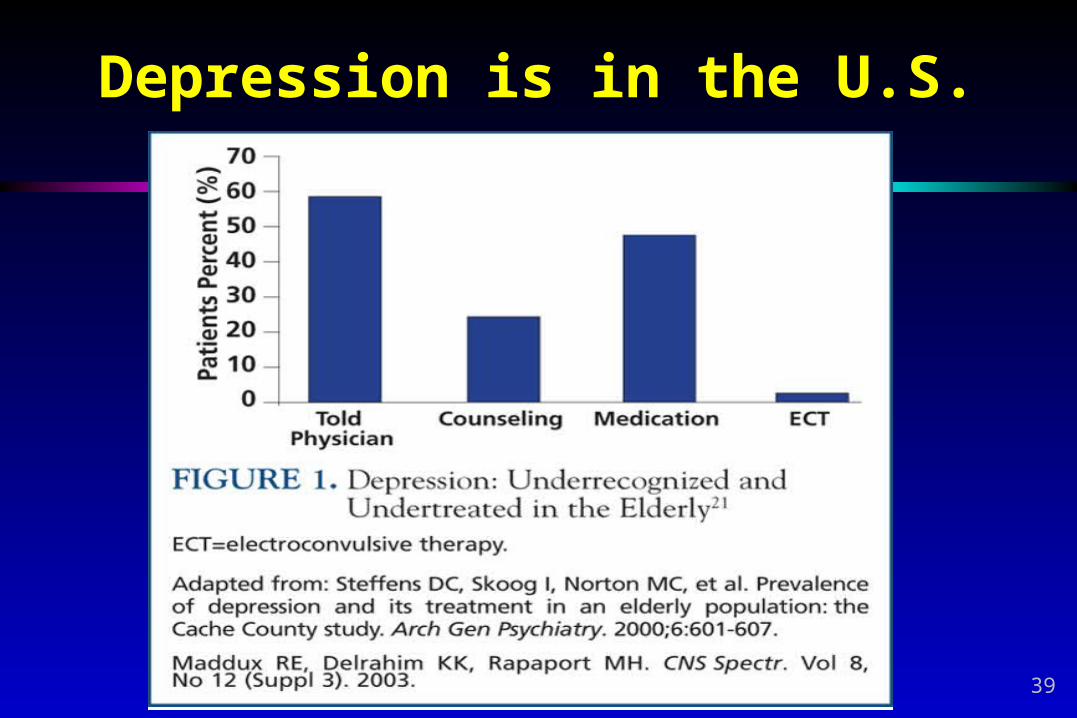
Depression is in the U.S.
39
Basic Principles of Geriatrics
8. Iatrogenic illness are common and many are preventable
Iatro = physicianGenesis = origin
Medications, diagnostic tests, and hospitalizations can be hazardous in older people
40
Betty Admitted to nursing home
from hospital following heart failure exacerbation
Unintentionally losing weight Treated with Marinol
(dronabinol) Side effect: munchies One bag of Cheetos later…
readmitted with HF exacerbation
41
Common Iatrogenic Illnesses in Geriatric Patients
Adverse drug reactions Delirium Falls and injuries Incontinence Immobility
Deconditioning Pressure ulcers Contractures
Risk Factors Normal age-related changes Atypical presentation of
disease High prevalence of chronic
disease and comorbidity Provider beliefs and attitudes Inadequate geriatric training
of healthcare providers
42
Basic Principles of Geriatrics
9. Geriatric care is provided in a variety of settings
43

Case - Sites of Geriatric CareCase - Sites of Geriatric CareCase - Sites of Geriatric CareCase - Sites of Geriatric Care
Home
Acute CareFacility
Outpatient/Facility
Long Term CareFacility
Assisted LivingFacility
Personal CareHome
Sub Acute Rehab
Home with home health
44
Basic Principles of Geriatrics
Geriatric care is provided in a variety of settings ranging from the home to long-term care institutions Criteria for levels of care Financing Care transitions and coordination
45
Sites Geriatric CareSites Geriatric Care
Acute Hospital Outpatient Clinics Nursing Home Assisted Living Facilities Home
Acute Hospital Outpatient Clinics Nursing Home Assisted Living Facilities Home
Care is not generally well coordinated
46
Basic Principles of Geriatrics
10. Ethical issues and end-of-life care are critical aspects of the practice of geriatrics
Not all people who live into extreme old age have to die in a hospital
47
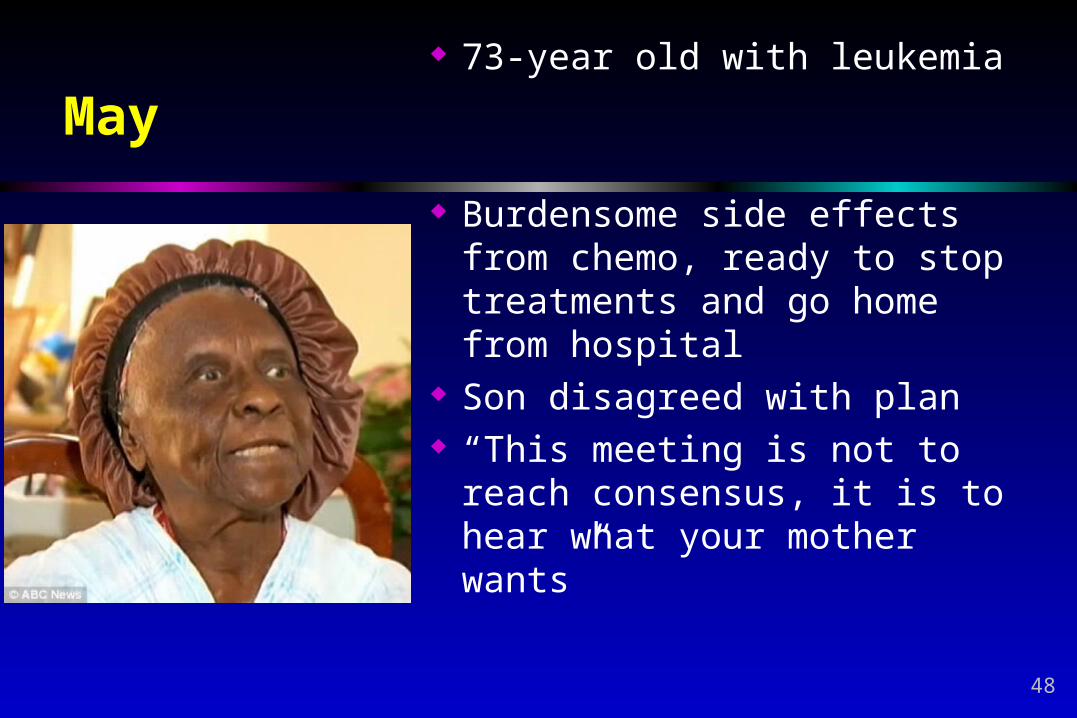
May 73-year old with leukemia
Burdensome side effects from chemo, ready to stop treatments and go home from hospital
Son disagreed with plan “This meeting is not to reach
consensus, it is to hear what your mother wants”
48
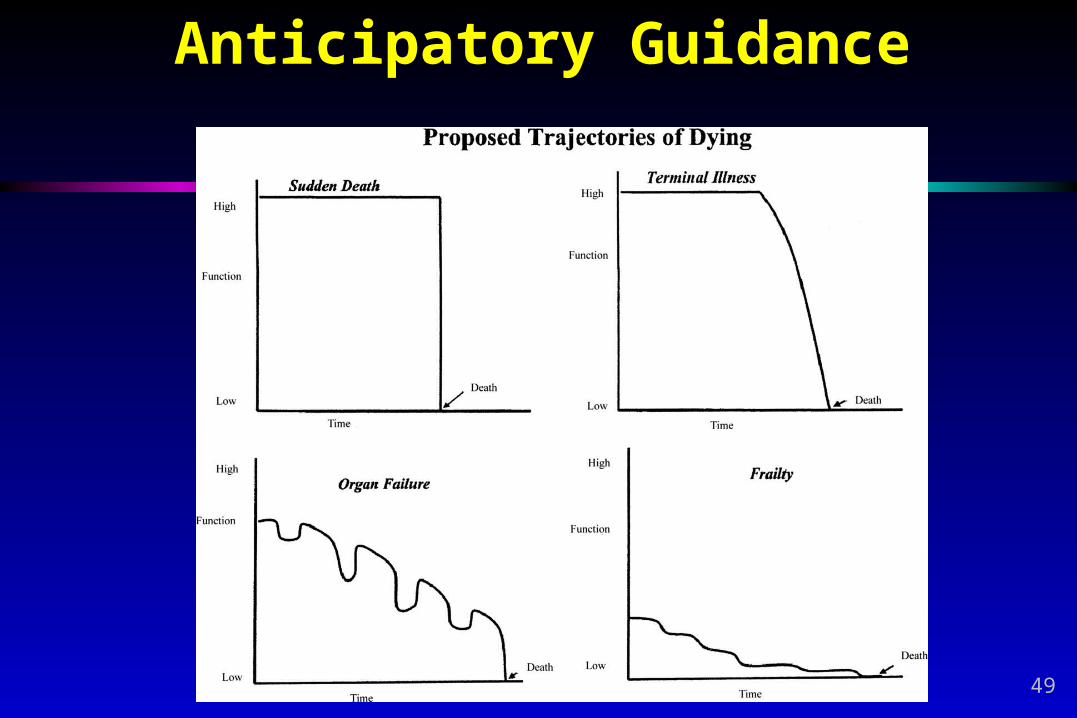
Anticipatory Guidance
49
www.chcr.brown.edu/dying/factsondying.htm
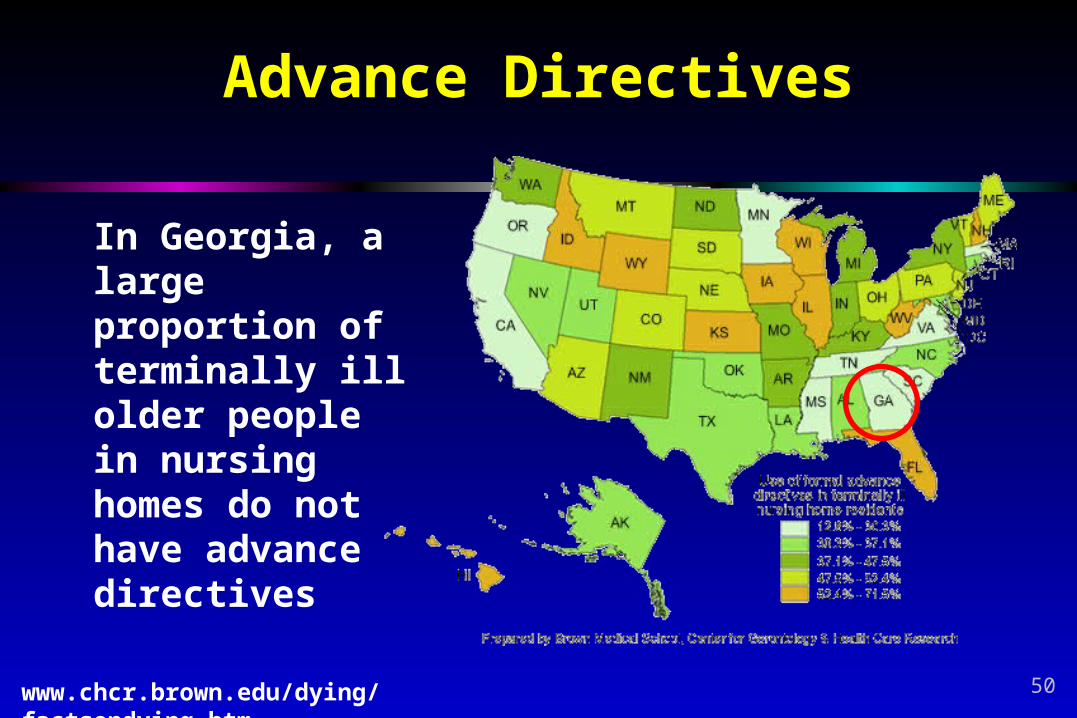
Advance Directives
In Georgia, a large proportion of terminally ill older people in nursing homes do not have advance directives
50
Learning Objectives
Understand important demographic trends in aging Be able to explain the concept of functional status Learn a framework for understanding basic
principles affect either recovery from, or treatment during, acute illness in older patients
51
WHAT GOES UP, WHAT GOES DOWN:THE PHYSIOLOGY OF AGING
Manuel A. Eskildsen, MD, MPHFinancial Relationships w Industry Disclosures
External Industry Relationships * Company Name(s) Role
Equity, stock, or options in biomedical industry companies or publishers**
None
Board of Directors or officer None
Royalties from Emory or from external entity
None
Industry funds to Emory for my research
None
Other None
53
Objectives
Understand the physiologic changes that occur with aging.
Differentiate the normal aging process from disease.
54
Outline
Discuss changes across different organ systems Body compositions Cardiac Pulmonary Gastrointestinal Renal Endocrine Reproductive Nervous System Sensory Skin
Discuss your assigned cases
55
56
Aging is not a disease
57
What is normal aging, and what is disease? Normal aging
Is an expected part of getting older
However, it may be variable
A direct consequence of the physiologic aging process
Disease Represents a
pathological change in the tissues involved
Aging may make the system vulnerable– but not a direct consequence of aging
58

Examples of cellular changes
Activation or suppression of aging genes
Telomeres Damage by free radicals
to mitochondria
59
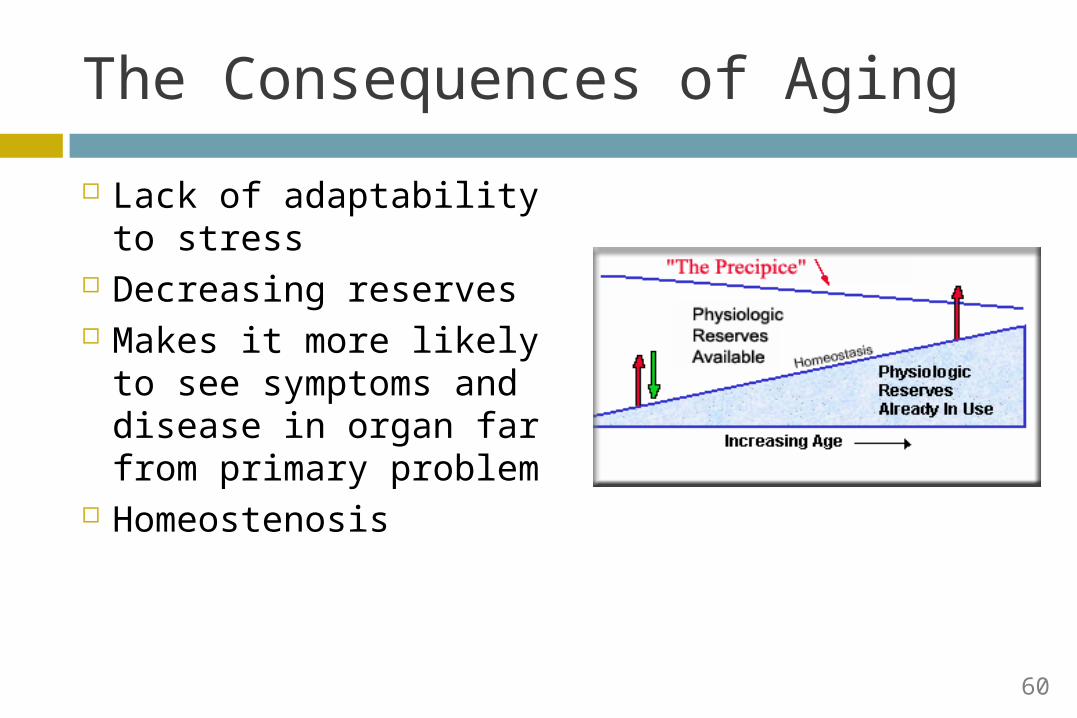
The Consequences of Aging
Lack of adaptability to stress
Decreasing reserves Makes it more likely to
see symptoms and disease in organ far from primary problem
Homeostenosis
60
Physiologic Changes
61
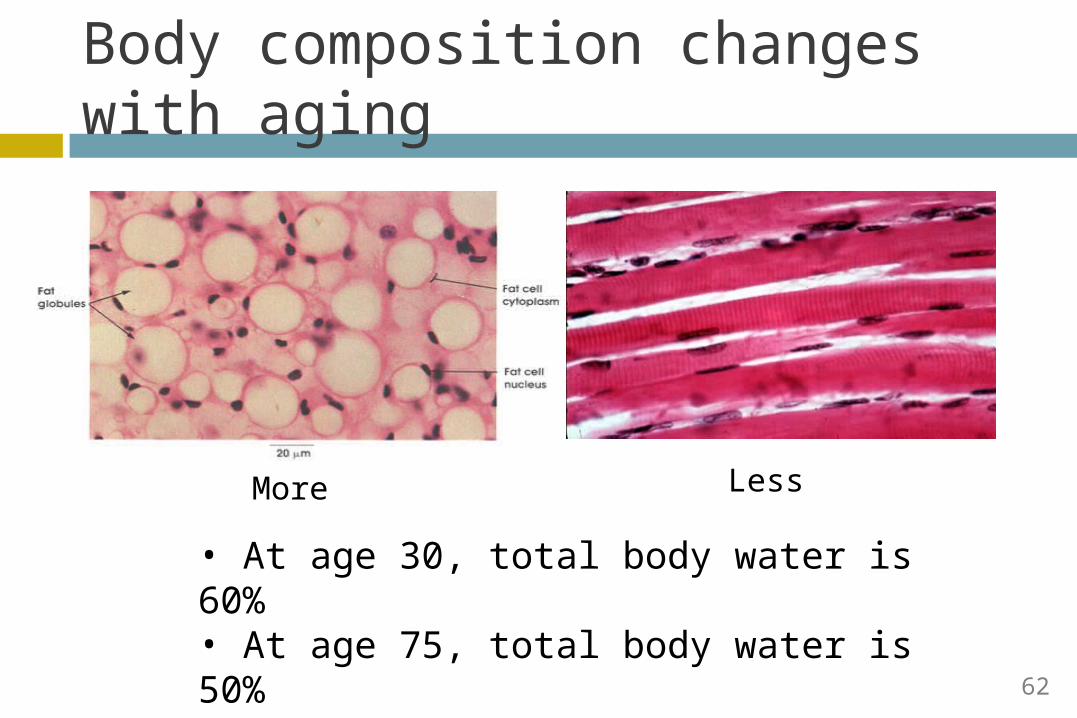
Body composition changes with aging
More Less
• At age 30, total body water is 60%• At age 75, total body water is 50%• Total body fat rises with age
62
Effects on Medications
Likely the most important to consider Lipophilic medications (e.g., diazepam)
Larger volume of distribution Stays in body longer
Hydrophilic medications (e.g., digoxin) Smaller volume of distribution Comparatively, may achieve higher plasma
concentrations
63

Cardiac Changes - Overview
Little difference at rest Structurally, muscle
thickness and heart weight increase
Functional changes: Decreased maximal heart
rate Increased dependence on
“atrial kick”
64
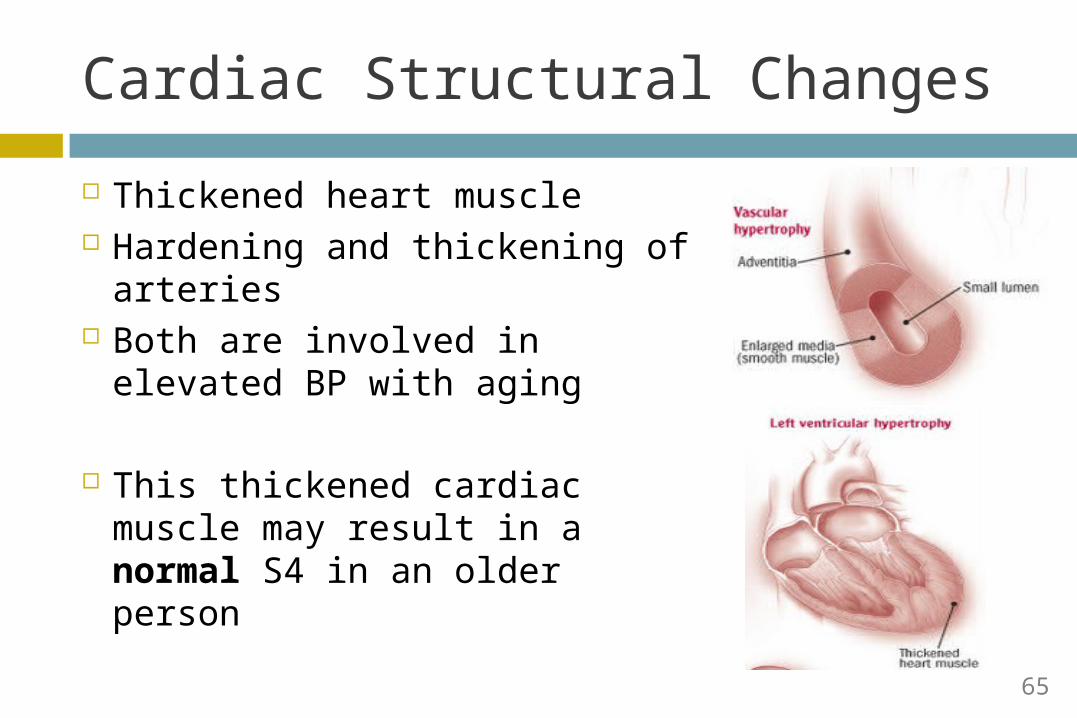
Cardiac Structural Changes
Thickened heart muscle Hardening and thickening of
arteries Both are involved in elevated
BP with aging
This thickened cardiac muscle may result in a normal S4 in an older person
65
Cardiac Functional Changes
Resting heart rate and cardiac output don’t change
However… Maximal heart rate decreases Maximal cardiac output decrease
Thickened left atrium Decreased atrial kick
More susceptible to complications like heart failure
66
Maximal heart rate
Male Maximal HR = 220 – age
Female Maximal HR = 220 – (0.6 x age)
67
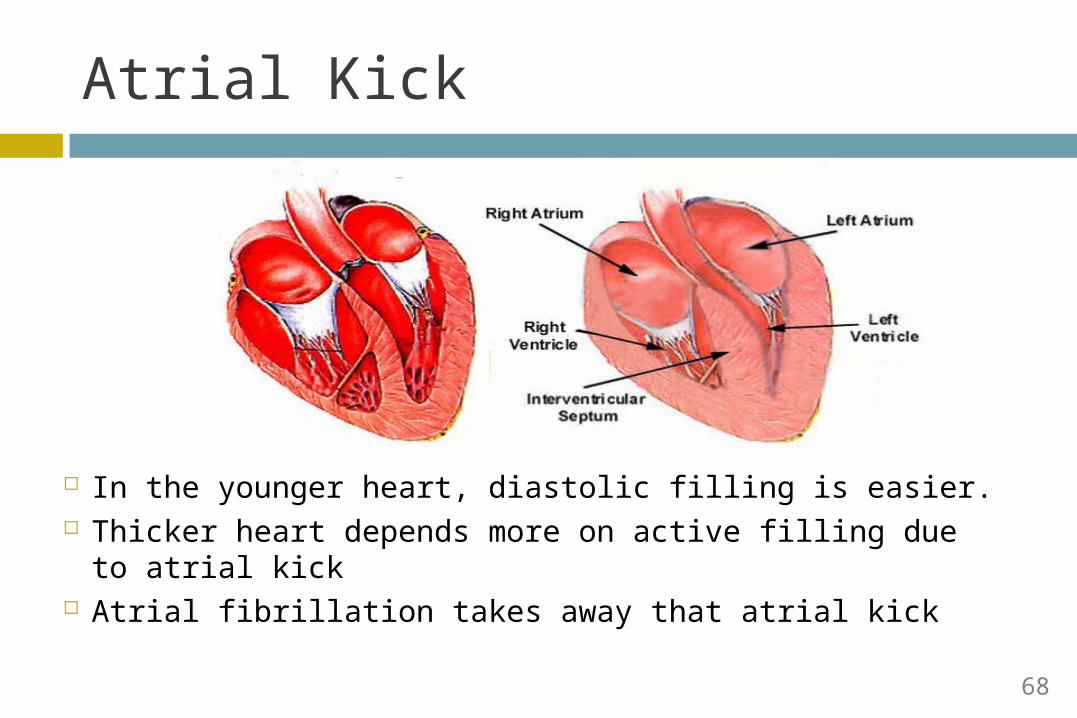
Atrial Kick
In the younger heart, diastolic filling is easier. Thicker heart depends more on active filling due to
atrial kick Atrial fibrillation takes away that atrial kick
68
Pulmonary and Lungs - Overview Also, few changes evident
at rest Structurally, generally
tissues are stiffer Maximal reserve decreases
69
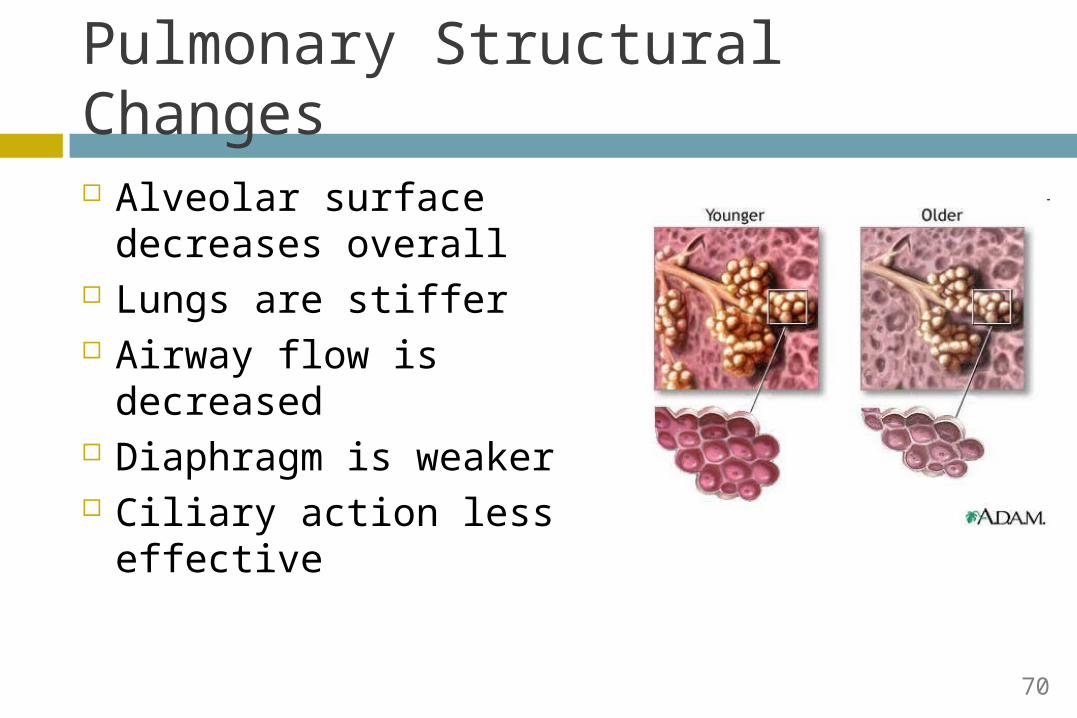
Pulmonary Structural Changes
Alveolar surface decreases overall
Lungs are stiffer Airway flow is
decreased Diaphragm is weaker Ciliary action less
effective
70
Pulmonary Function
Decreased vital capacity (amount of air that can be maximally inspired)
Increased residual volume (air trapping)
Ventilation/Perfusion (V/Q) mismatch
71
Arterial O2 changes with age
PaO2= 100 – (age/3)
Age 17 Age 87
72
PaO2= 71 mm HgPaO2= 94 mm Hg
Question An 85-year-old man has had increasingly severe shortness
of breath on exertion over the past 3 months. For the past 20 years, he has walked 30 minutes three times weekly at a fairly rapid pace without symptoms. He has no chest pain, wheezing, or cough. Blood pressure is 140/85 mm Hg. On examination, the lungs are clear and there is no evidence of wheezing. Radiographs of the chest and an electrocardiogram show normal findings. Which of the following additional findings would require further evaluation?
(A) Arterial PO2 of 80 mm Hg (B) Decreased cardiac output on ultrasonography (C) Decreased maximum heart rate on stress testing (D) Decreased vital capacity on pulmonary function testing (E) Presence of an S4 gallop

Gastrointestinal/Hepatic
74
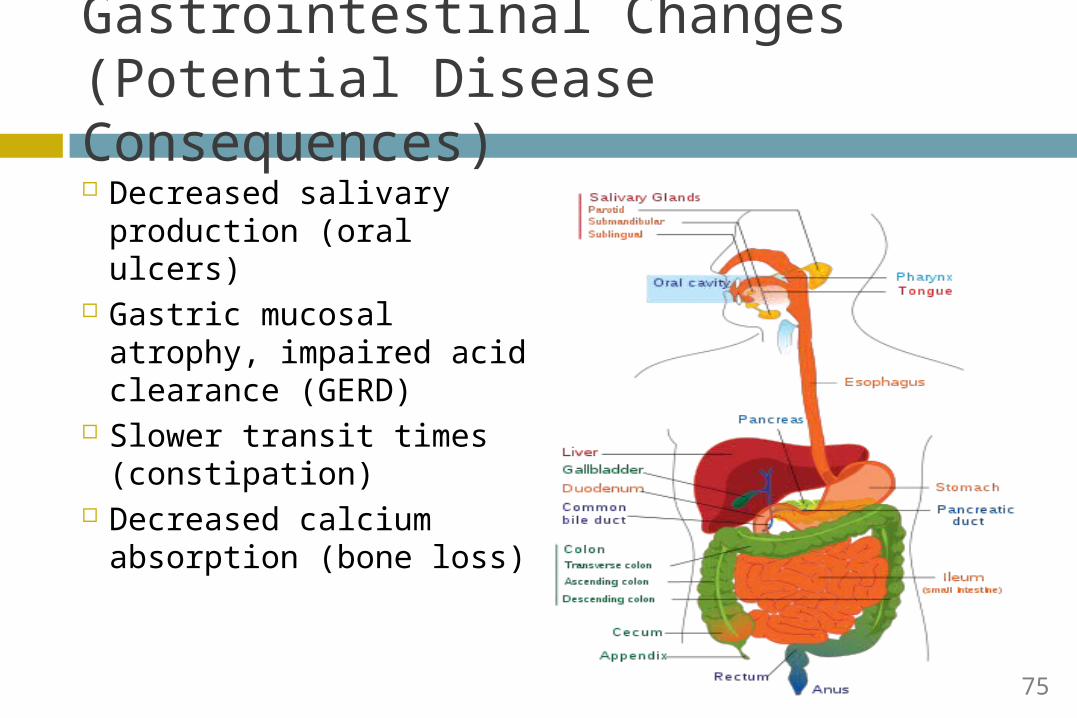
Gastrointestinal Changes (Potential Disease Consequences) Decreased salivary
production (oral ulcers)
Gastric mucosal atrophy, impaired acid clearance (GERD)
Slower transit times (constipation)
Decreased calcium absorption (bone loss)
75
Constipation
Constipation is not normal aging, but aging predisposes to it
Slower transit time plus… Low fiber Poor mobility Effects of medications (narcotics)
Equals constipation
76
Hepatic Changes
Phase I metabolism (oxidation/reduction)
Cytochrome P450 system
Significant declines with aging
Careful with diazepam (valium)
Phase II reactions (conjugation)
Like glucuronidation Facilitates renal
excretion Less affected with
aging Example:
Lorazepam (ativan)
77
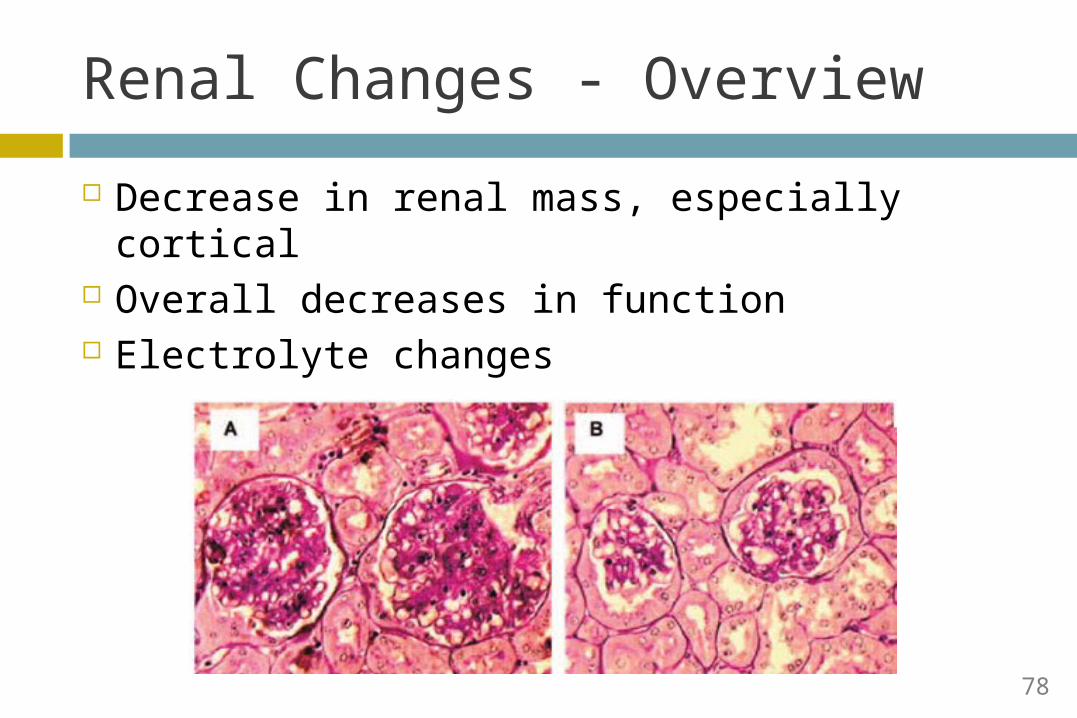
Renal Changes - Overview
Decrease in renal mass, especially cortical Overall decreases in function Electrolyte changes
78
Renal Changes
Decrease in size, especially at the expense of the cortex
Decrease in renovascular bed 30% of glomeruli lost by age 75
Decreased creatinine clearance --- serum creatinine is less of an important indicator
Decrease in concentrating capacity --- tendency toward dehydration
79
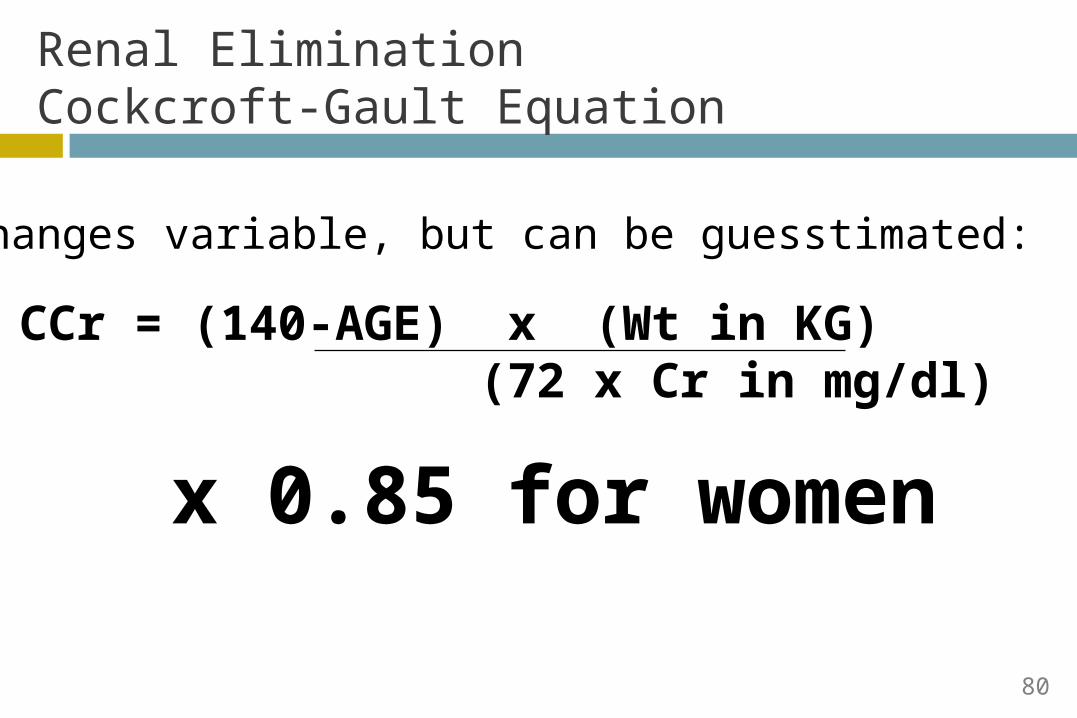
Renal Elimination Cockcroft-Gault Equation
CCr = (140-AGE) x (Wt in KG) (72 x Cr in mg/dl)
x 0.85 for women
Changes variable, but can be guesstimated:
80
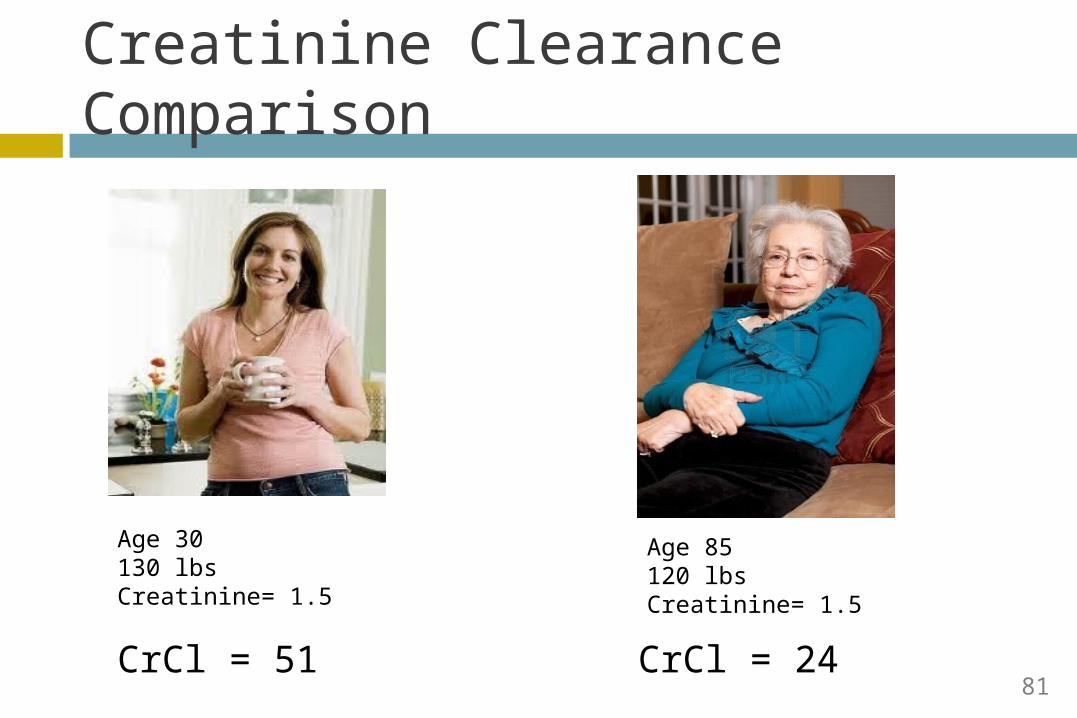
Creatinine Clearance Comparison
Age 30130 lbsCreatinine= 1.5
Age 85120 lbsCreatinine= 1.5
CrCl = 51 CrCl = 2481
Implications of Aging Changes on Kidney Need to know whether drugs are excreted
renally And whether dose needs to be adjusted Example
The 80-year old woman in the example above has CrCl of 24 ml/min
She has a DVT and her MD decides to treat with enoxaparin. Ordinary dosing is 1 mg/kg BID
For CrCl < 30, dose is 1 mg/kg Qday Dose is 55 mg Qday
82
Endocrine Changes - Overview
Changes in Glucose Tolerance Decrease in GH, Testosterone, Estrogen Ovarian failure (menopause) already happened
in 50s
83

Glucose and Insulin
Clinically insignificant increases in fasting glucose after age 20 (1% per decade)
Decreased response of peripheral tissues to insulin
SEDENTARY LIFESTYLE contributes much more to poor glucose tolerance than age
84

Reproductive/Genitourinary
85
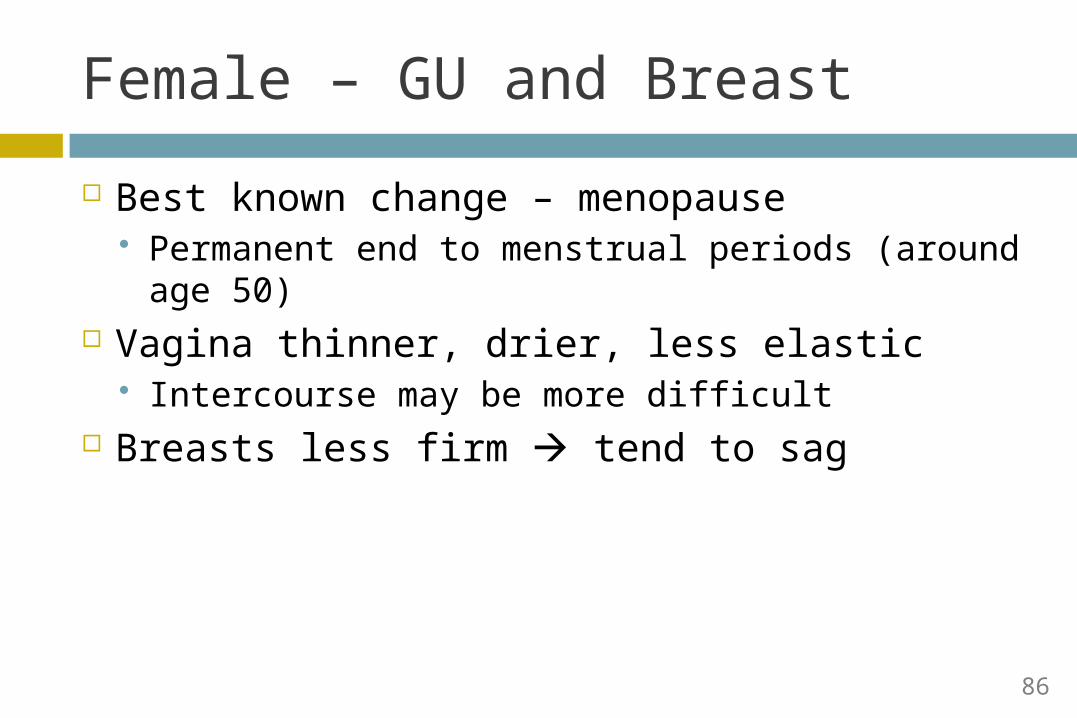
Female – GU and Breast
Best known change – menopause Permanent end to menstrual periods (around age
50) Vagina thinner, drier, less elastic
Intercourse may be more difficult Breasts less firm tend to sag
86
Male Changes
Fewer sperm and decreased sex drive over time Hormone changes are more gradual
Blood flow to penis tends to decrease Erections may not last as long; also less rigid Erectile dysfunction more common (but not part of
normal aging) Prostate enlarges
Older men may urinate with less force, take more time to initiate stream
87
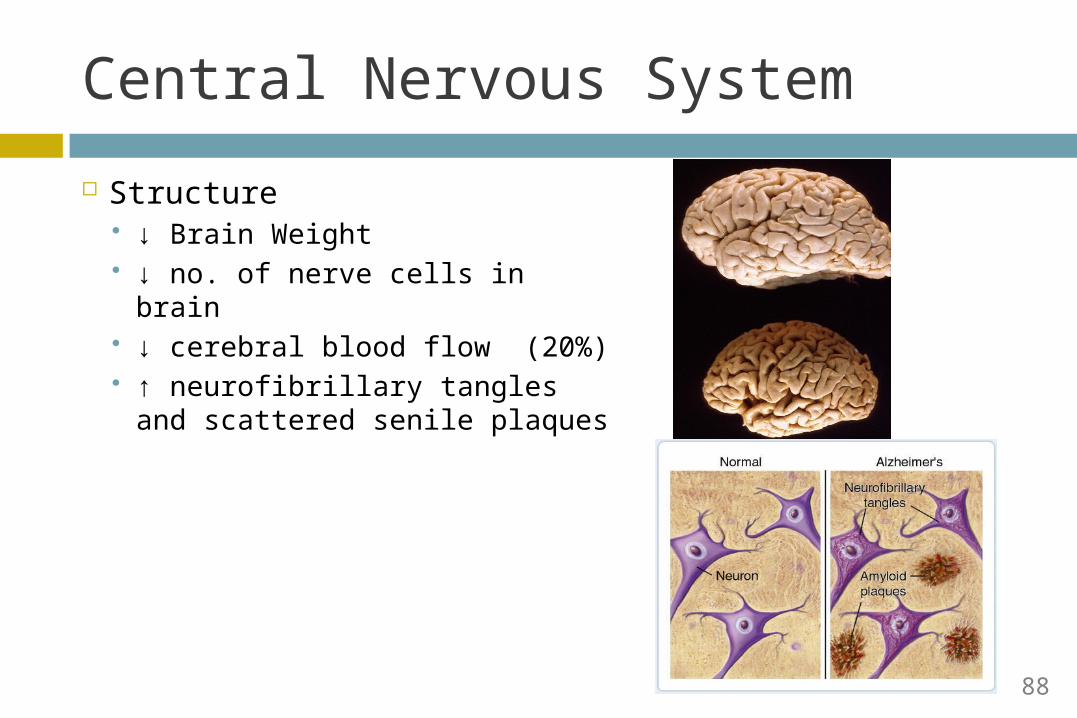
Central Nervous System
Structure ↓ Brain Weight ↓ no. of nerve cells in brain ↓ cerebral blood flow (20%) ↑ neurofibrillary tangles and
scattered senile plaques
88
Central Nervous System - Function
Intellect Maintained until at least age 80 Slowing in central processing → Tasks take longer to
perform
Verbal skills Maintained until age 70 Gradually ↓ in vocabulary, ↑ semantic errors and
abnormal prosody
Mentation Difficulty learning, especially languages and
forgetfulness in non-critical areas – doesn’t impair recall of important memories or affect function
89
Dementia vs. Normal Aging
Dementia Difficulty naming
common words Forgetting names of
known places, family members
Example: putting sweater in microwave
Normal Aging Occasional word-
finding difficulty Difficulty learning
new languages Example: Forgetting
your keys
90
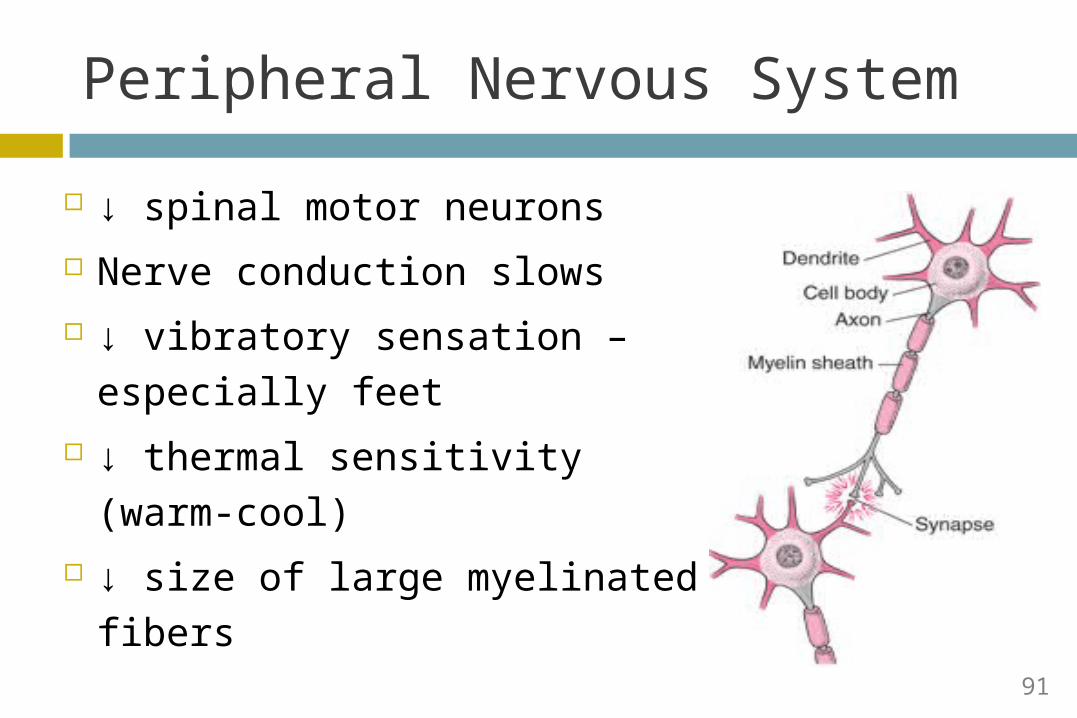
Peripheral Nervous System
↓ spinal motor neurons Nerve conduction slows ↓ vibratory sensation –
especially feet ↓ thermal sensitivity (warm-
cool) ↓ size of large myelinated
fibers91
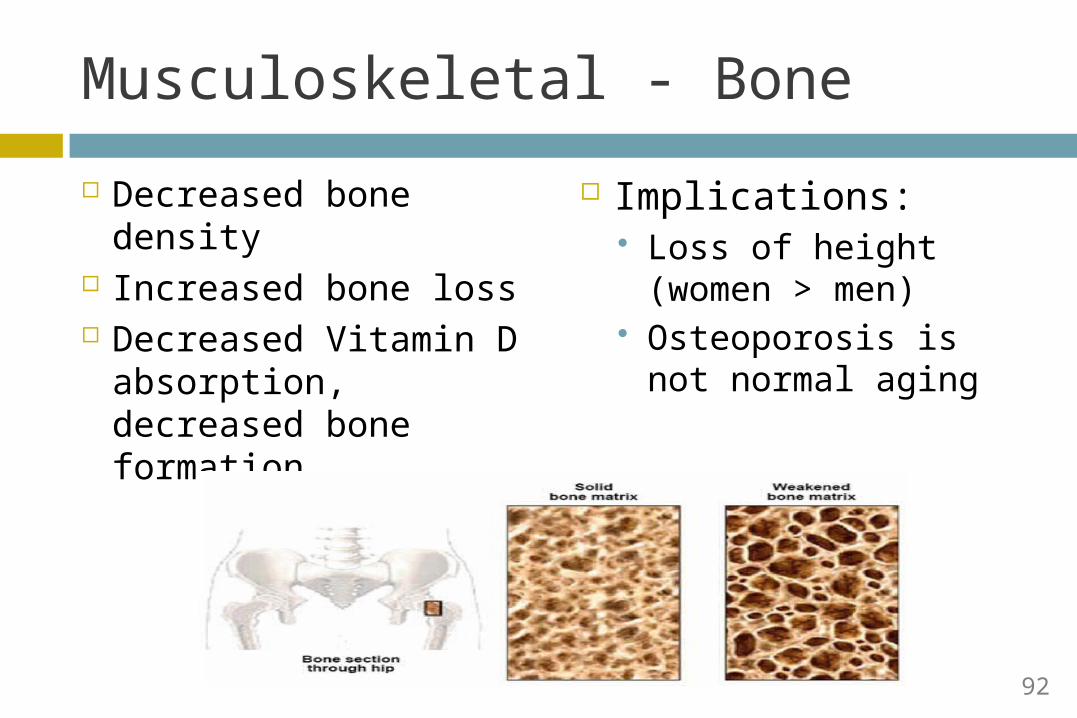
Musculoskeletal - Bone
Decreased bone density
Increased bone loss Decreased Vitamin D
absorption, decreased bone formation
Implications: Loss of height
(women > men) Osteoporosis is not
normal aging
92
Musculoskeletal - Muscle
Muscle mass decreases by 30 – 40 % linear acceleration with age Fewer motor units (so decrease power) Produce less heat per KG
Decreased transfer ability Decreased stair climbing ability Decreased gait speed Activity makes a big difference!
93
Sensory Changes
Visual Auditory Smell Taste
94
Visual Changes
Hardening of lens Difficulty with accommodation Presbyopia
After age 40; part of normal aging
Yellowing of lens Eventually can lead to cataracts (not normal aging)
Impaired dark adaptation and contrast sensitivity Implications for night driving
95
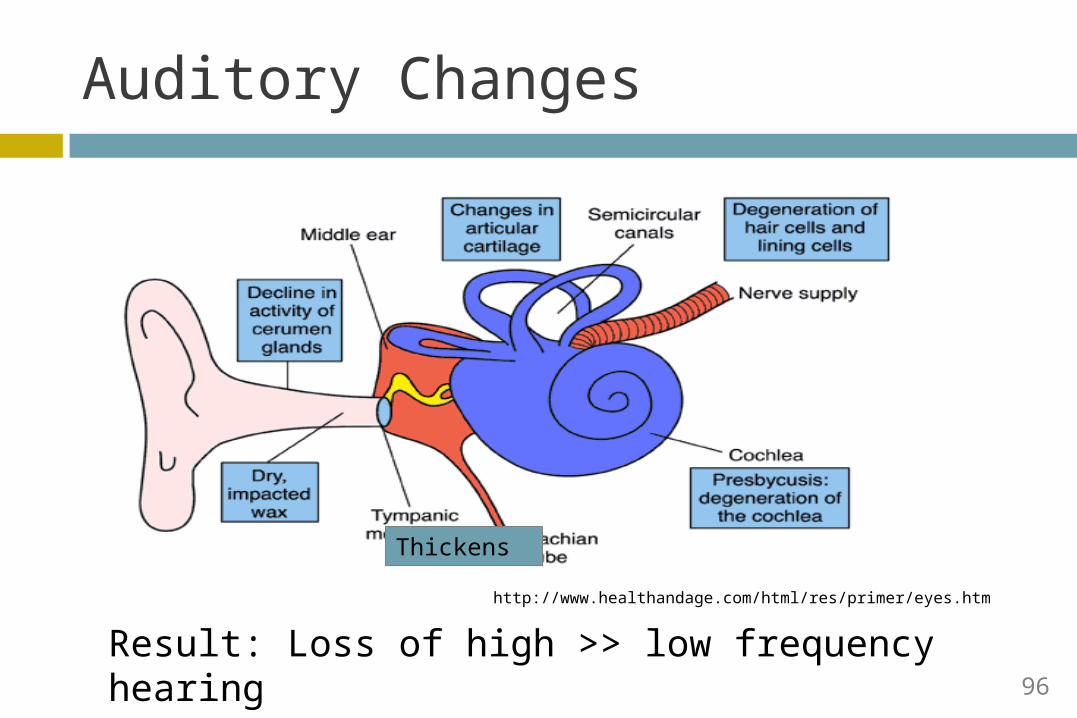
http://www.healthandage.com/html/res/primer/eyes.htm
Thickens
Result: Loss of high >> low frequency hearing
Auditory Changes
96
Hearing – Clinical Implications
Clinical Question: Describe a Strategy for Communicating With Older Patients Who Have Hearing Loss?
Clinical Question: What easy physical exam component should you carry out before referring a patient to an ENT?
97
Taste & Smell Changes
# of taste buds and responses are unchanged
Olfaction ↓↓↓ significantly Detection thresholds increase 50% by age 80
Smell recognition decreases by 15% Decreased Smell leads to Decreased
taste May predispose to malnutrition
98
Skin
99
Skin Changes
Loss of subcutaneous fat Atrophy of sweat glands Impaired vasoconstictor/vasodilator response in
skin arterioles Decreased temperature discrimination Ineffective DNA repair
100
Skin Changes-Implications
Less fat over bony prominences (pressure ulcers)
Temp discrimination impairments; Less efficient shivering; less muscle activity Hypothermia
Higher temperature for sweating, less production Hyperthermia
Ineffective DNA repair Carcinogenesis
101
Summary
Changes in multiple organ systems are a part of normal aging
They may predisposed to disease but are not in of themselves pathologic
Have clinical implications which may necessitate adjustment of treatment
102
CHRONIC DISEASE MANAGEMENT
Ugochi Ohuabunwa MDDivision of General Medicine and GeriatricsEmory University School of [email protected]
External Industry Relationships * Company Name Role
Equity, stock, or options in biomedical industry companies or publishers
None
Board of Directors or officer None
Royalties from Emory or from external entity
None
Industry funds to Emory for my research None
Other None
Ugochi Ohuabunwa, M.D.Personal/Professional Financial Relationships with Industry
104
Learning Objectives
Discuss the definition and epidemiology of chronic diseases
Describe models of care in management of chronic diseases
Compare and contrast acute and chronic disease management modalities
Discuss effective inter-professional team collaborative practice in chronic disease management
Describe the steps of management of a patient with Heart Failure using the Chronic Care Model
105
You as a patient………….
What would you consider to be excellent medical care if you had a chronic medical condition?
How best would you like your disease managed?
How do you think the medical practice where you are cared for should be best organized to provide excellent patient care?
106
You as a physician………….
What would you consider to be excellent medical care provided to your patients?
How would you like your medical practice organized to facilitate provision of excellent patient care?
What measures can your practice put in place to ensure that your patients are doing well and have good outcomes?
107
Mr. Smith – History of Present Illness
A 78-year-old man admitted to Emory University Hospital with three days of nausea and vomiting, shortness of breath, cough, and leg swelling. He had a heart attack in January 2013. Since then, he has had worsening symptoms of heart failure, necessitating five hospital admissions over the last six months
108
Past Medical History
Coronary Artery Disease with Acute Heart Attack January 2013
Congestive Heart Failure High Blood Pressure High Cholesterol Diabetes Dementia
109
Medications on Admission
Furosemide 20mg once daily Clopidogrel 75mg once daily Aspirin 325mg once daily Simvastatin 20mg at night Metoprolol 25mg twice daily Lisinopril 20mg once daily Donepezil 10mg once daily Glipizide XL 10mg once daily
110
Social History
Widowed and lives alone in an independent living senior high rise
Has 2 living children both of whom live out of state
Has a niece who checks in on him 3 times a week
Does not drink alcohol, smoke or use recreational drugs
111
Functional History
Able to complete his activities of daily living Bathing Toileting Grooming
Has had increasing difficulty in performing some instrumental activities of daily living due to his increasing shortness of breath Cooking Cleaning
112
Questions
What do you think is going on with Mr. Smith?
Why the very frequent re-hospitalizations?
As Mr. Smith’s physician, how best can you manage his acute and chronic medical problems?
113
Definition
Chronic conditions are "any conditions that require ongoing adjustments by the affected person and interactions with the health care system." (Improving chronic illness care, 2008)
Examples Asthma Diabetes Heart disease Hypertension High Cholesterol
http://www.improvingchroniccare.org
114
Epidemiology
133 million people - almost half of all Americans, live with a chronic condition
That number is projected to increase by more than one percent per year by 2030, resulting in an estimated chronically ill population of 171 million."
http://www.improvingchroniccare.org
115
Epidemiology
80% of persons over 65 have one or more chronic conditions
Chronic conditions contribute to ¾ of the healthcare budget
Need for development of innovative and impactful methods to deliver quality patient care
116
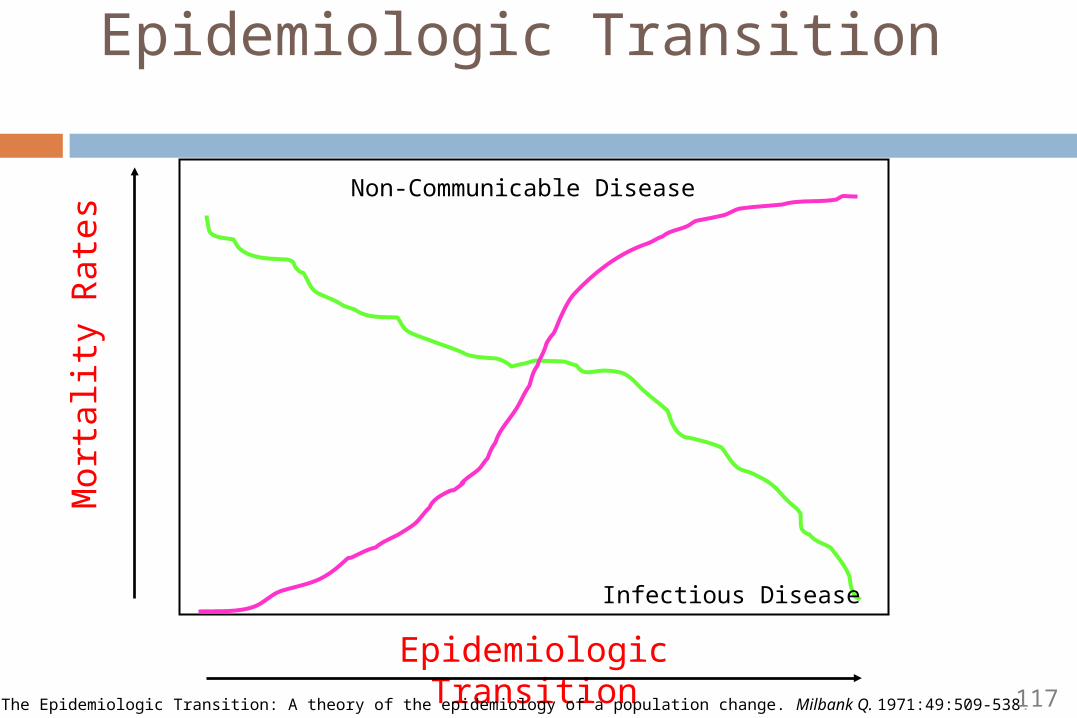
Epidemiologic Transition
Non-Communicable Disease
Infectious Disease
Epidemiologic Transition
Mo
rta
lity
Ra
tes
Omran, A. The Epidemiologic Transition: A theory of the epidemiology of a population change. Milbank Q. 1971:49:509-538. 117
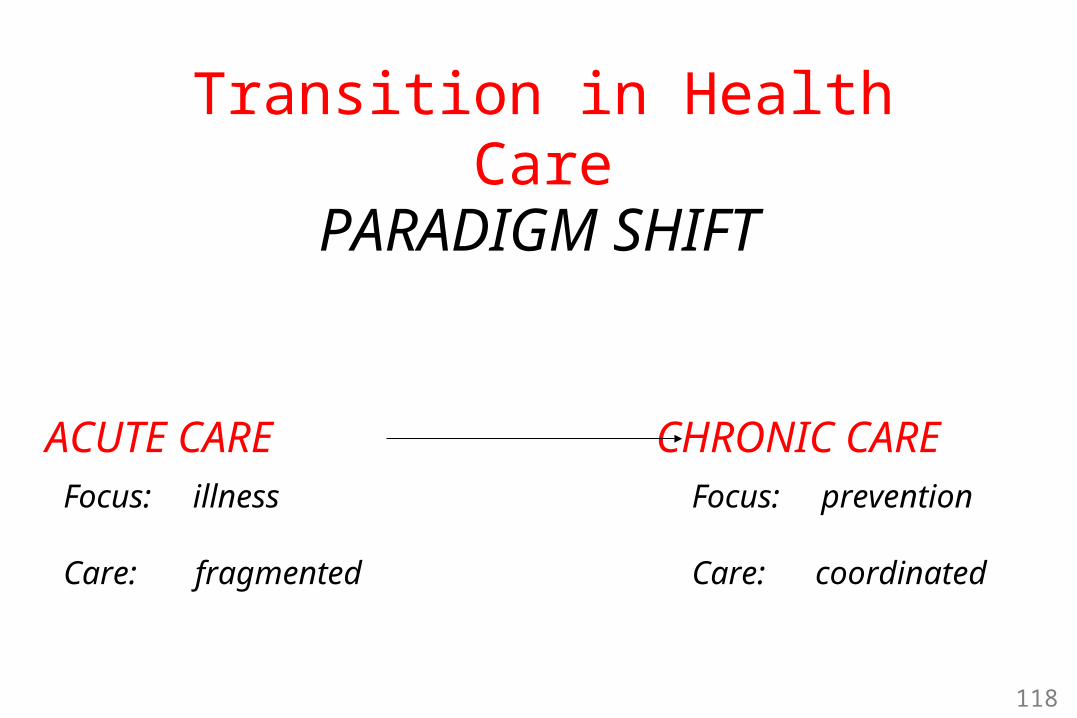
PARADIGM SHIFT
ACUTE CARE CHRONIC CAREFocus: illness
Care: fragmented
Focus: prevention
Care: coordinated
Transition in Health Care
118
Current State of Primary Care Practice
Acute Disease Management Primary care practice largely designed
To provide ready access and care to patients with acute problems
Emphasis on triage and patient flow Short appointments Diagnosis and treatment of symptoms and signs Reliance on laboratory investigations and
prescriptions Brief, didactic patient education Patient-initiated follow-up
119
Current State of Primary Care Practice
Care is not necessarily based on evidence, but experience and training
Seldom is there a team approach…care is mainly driven by the physician alone
Paternalistic and directive approach with little attention to patients’ behavioral needs
120
Current State of Primary Care Practice
Limited access Insurer limitations Reluctance of primary care referral Fragmented access
Poor information systems Poor tracking
121
Is the Current System Working?
Patients and families struggling with chronic illness have different needs
These needs are unlikely to be met by an acute care organization and culture
They require planned, regular interactions with their caregivers
Need for focus on function and prevention of exacerbations and complications
122
Ideal Healthcare System
Evidence-based, planned care Systematic assessments Attention to treatment guidelines
Reorganization of practice (team approach) Includes ancillary professionals with the patient as the
most important member
Attention to patient needs (information) Counseling, education, information feedback Behaviorally sophisticated support for the patient's
role as self-manager
123
Ideal Healthcare System
Access to clinical expertise Patient and provider education, access to
specialists
Supportive information systems Patient registries Provider feedback on preventive service
utilization
124
Models of Care in Chronic Disease Management
Chronic Care Model Guided Care Model Innovative Care for Chronic Diseases Model
(World Health Organization) Stanford Self-Management Program Fennell Four Phase Model of chronic illness
125
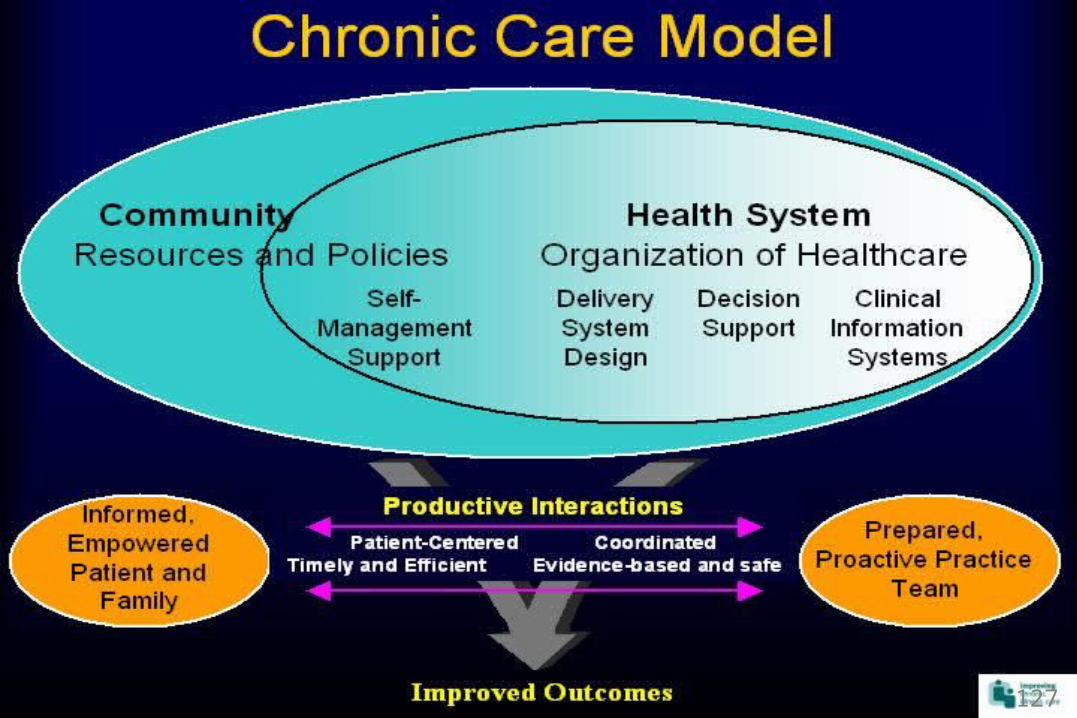
Chronic Care Model (CCM)
CCM summarizes the basic elements for improving care in health systems on different levels The community The health system Self-management support Delivery system design Decision support Clinical information systems
126
127
Guided Care Model
In Guided Care, a specially-educated registered Guided Care Nurse, based in a primary care practice, works in partnership with 2-5 primary care physicians and other members of the health care team in providing 8 processes to 50-60 chronically ill patients.
128

Guided Care Processes
Assessing the patient and primary caregiver at home
Creating an evidence-based comprehensive "Care Guide" (care plan) for providers and a patient-friendly "Action Plan" for patients and caregivers
Promoting patient self-management Monitoring patient's conditions monthly
129
Guided Care Processes
Coordinating the efforts of all health care providers, healthcare facilities, rehab facilities, home care agencies, hospice programs, and social service agencies
Smoothing transitions between sites of care, focusing more intensively on transitions into and out of hospitals
Educating and supporting family caregivers Facilitating access to community resources
130
Back to Mr. Smith
How best can we manage his illnesses?
Which model of care would be best suited for him?
How will the model work?
131
A Review of His Chronic Medical Conditions
Coronary Artery Disease with Acute Heart Attack January 2013
Congestive Heart Failure High Blood Pressure High Cholesterol Diabetes Dementia
132
His Social History
Widowed and lives alone in an independent living senior high rise
Has 2 living children both of whom live out of state
Has a niece who checks in on him 3 times a week
Does not drink alcohol, smoke or use recreational drugs
133

His Functional History
Able to complete his activities of daily living Bathing Toileting Grooming
Has had increasing difficulty in performing some instrumental activities of daily living due to his increasing shortness of breath Cooking Cleaning
134
Mr. Smith
Based on this history, can you summarize the needs of Mr. Smith?
Which of these needs would you like to address as Mr. Smith’s physician?
How best can you organize your practice and harness resources to meet these needs?
135
Needs of Mr. Smith
Medical Needs Multiple medical diseases with frequent
exacerbations Need for optimal medication management Need to ensure that these diseases are well
controlled and are at goal Need to ensure that he is well informed and
compliant
136

Needs of Mr. Smith
Social Needs Lives alone, only checked on 3ce a week by niece Has dementia and may be unable to manage his
medications May also be forgetful of dietary needs and other
self management measures Functional Needs
Increasing difficulty with completing IADLs such as cooking
May be eating the wrong things
137
Mr. Smith
Which of these needs would you like to address as Mr. Smith’s physician? Medical needs? Social needs? Functional needs
As a Clinician, which of these needs are your responsibility to meet?
How best can you organize your practice and harness resources to meet these needs?
138
Applying the Chronic Care Model to the management of his chronic medical conditions
Mr. Smith
139
Chronic Care Model Components The community The health system Self-management support Delivery system design Decision support Clinical information systems
140
1. The Community
Linkages with community- based resources Exercise programs Senior centers Self-help groups Patient education classes Home care agencies
141
1. The Community
Which community resources would Mr. Smith benefit from?
Based on his Medical History
Based on his Social History
Based on his Functional History
142
2. Self-management Support
Involves collaboratively helping patients and their families acquire skills and confidence to manage their chronic illnesses through: Education on management of illnesses including -
diet, exercise, medication use, self measurement Provision of self-management tools e.g, blood
pressure cuffs, glucometers, bathroom scales Referrals to community resources Routinely assessing problems and accomplishment
of goals
143
2. Self-management support
How can we help Mr. Smith acquire skills and confidence to manage his chronic illnesses?
What should be the content of his education?
What self-management tools can we provide Mr. Smith?
144
4. Delivery System Design
Redesign of the medical practice, creating practice teams with a clear division of labor
Non physician personnel are trained to support Patient self-management Arrange for routine periodic tasks (e.g, laboratory
tests, eye examinations, and foot examinations) Ensure appropriate follow-up
Pre - planned visits are an important feature of practice redesign
145

4. Delivery System Design
Which members of the healthcare team should be involved in the care of Mr. Smith?
Define the role of each member of the
healthcare team and what services they should provide?
146
5. Decision Support
Use of evidence-based clinical practice guidelines for optimal chronic care
Guidelines integrated into daily practice through physician reminders
Guidelines reinforced by physician “champions” leading educational sessions for practice teams
Prompt access to specialists for expert evaluation
147
5. Decision Support
You are the physician champion of the clinic
How can you ensure that members of the practice team are well equipped to provide up to date evidence based care to Mr. Smith?
What systems can you create to ensure that Mr. Smith’s physician integrates evidence based practice guidelines into his routine management ?
How can we coordinate his care to ensure ease of specialist referral?
148
6. Clinical Information Systems
Presence of computerized information system Has 3 important roles:
As reminder systems that help primary care teams comply with practice guidelines
As feedback to physicians, showing how each is performing on chronic illness measures such as HbA1c and lipid levels
As registries for planning individual patient care and conducting population-based care
149
6. Clinical Information Systems
How can we incorporate the clinical information system into the management of Mr. Smith?
Based on Mr. Smith’s medical history, what chronic illness measures would best be used for providing feedback to Mr. Smith’s doctor about his care?
How best can we plan Mr. Smith’s care prior to and during each visit based on the information received from the computerized system?
150

Mr. Smith
Summarize your goals and care plan for the management of Mr. Smith’s chronic medical illnesses
151
Conclusions
Chronic Disease Management should not be problem-based, designed to handle only acute patient problems
Should be a system that is prevention based to avoid long-term complications
Should adopt a wholesome approach, taking into account the medical, psychosocial, functional and educational needs of a patient in order to harness available resources to meet these needs
152
Conclusions
Should involve a well prepared proactive practice team with appropriately defined roles, operating with the support of clinical information systems to provide evidence based care
Should collaboratively help patients and their families acquire skills and confidence to manage their chronic illnesses
A successful chronic disease management model would
result in a more informed activated patient and a prepared proactive practice team working together in a partnership to improve functions and clinical outcomes.
153
AGING WEEK 2013CAMILLE VAUGHAN, MD, MS
ASSISTANT PROFESSORDIVISION OF GENERAL MEDICINE & GERIATRICS
TUESDAY, NOVEMBER 12TH, 2013
Appetite for Life
External Industry Relationships * Company Name(s) Role
Equity, stock, or options in biomedical industry companies or publishers**
None N/A
Board of Directors or officer None N/A
Royalties from Emory or from external entity
None N/A
Industry funds to Emory for my research
Astellas Pharma, Inc Investigator Initiated Trial
Other Kimberly-Clark, Corp. Spouse is full-time employee
*Consulting, scientific advisory board, industry-sponsored CME, expert witness for company, FDA representative for company, publishing contract, etc.**Does not include stock in publicly-traded companies in retirement funds and other pooled investment accounts managed by others.
Camille Vaughan, MD, MSPersonal/Professional Financial Relationships with Industry within the past year
155
Learning Objectives
Factors impacting the nutritional status of older adults
Physiologic changes of aging which impact nutrient requirements
Nutrients – which ones are most important?
Health benefits and risks of weight loss in overweight and obese older adults
The role of medical nutrition therapy
Programs to enhance nutrition in community dwelling older adults
156

Role of Food/Nutrition in Aging
Physiologic well-beingQuality of Life
Social Cultural Psychological
Promotes health and functionalityMedical Nutrition Therapy (MNT)
Disease management Lessen chronic disease risk Slow progression Lessen disease symptoms
Position Paper, J Acad of Nutrition & Dietetics, 2012157
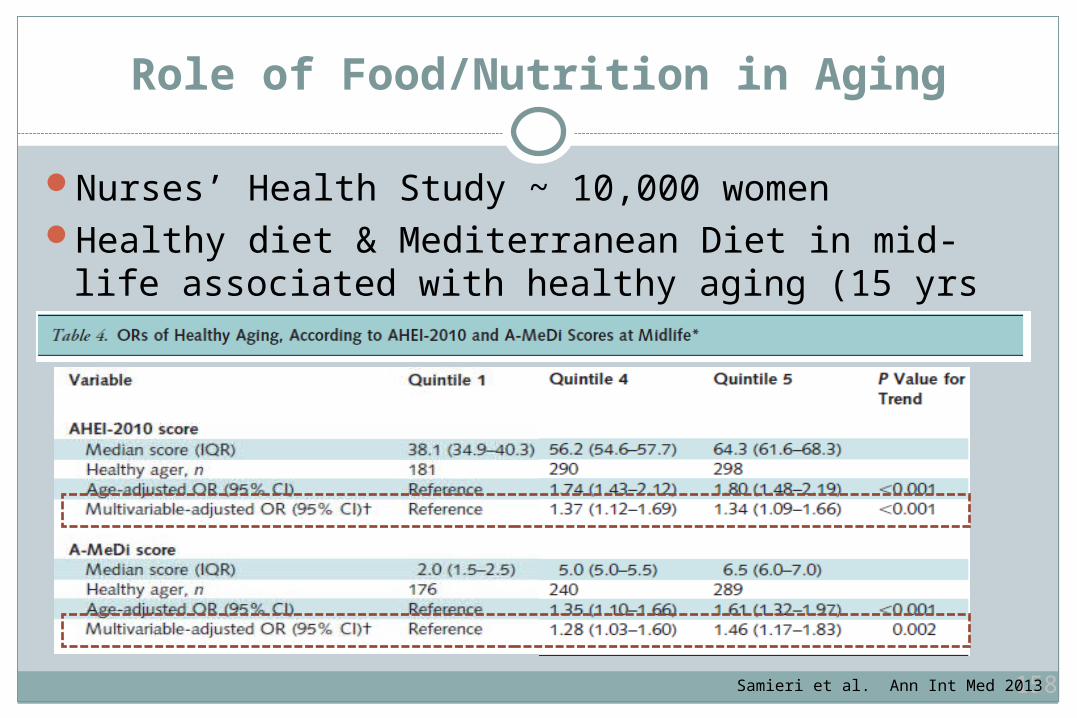
Role of Food/Nutrition in Aging
Nurses’ Health Study ~ 10,000 womenHealthy diet & Mediterranean Diet in mid-life
associated with healthy aging (15 yrs later)
158Samieri et al. Ann Int Med 2013
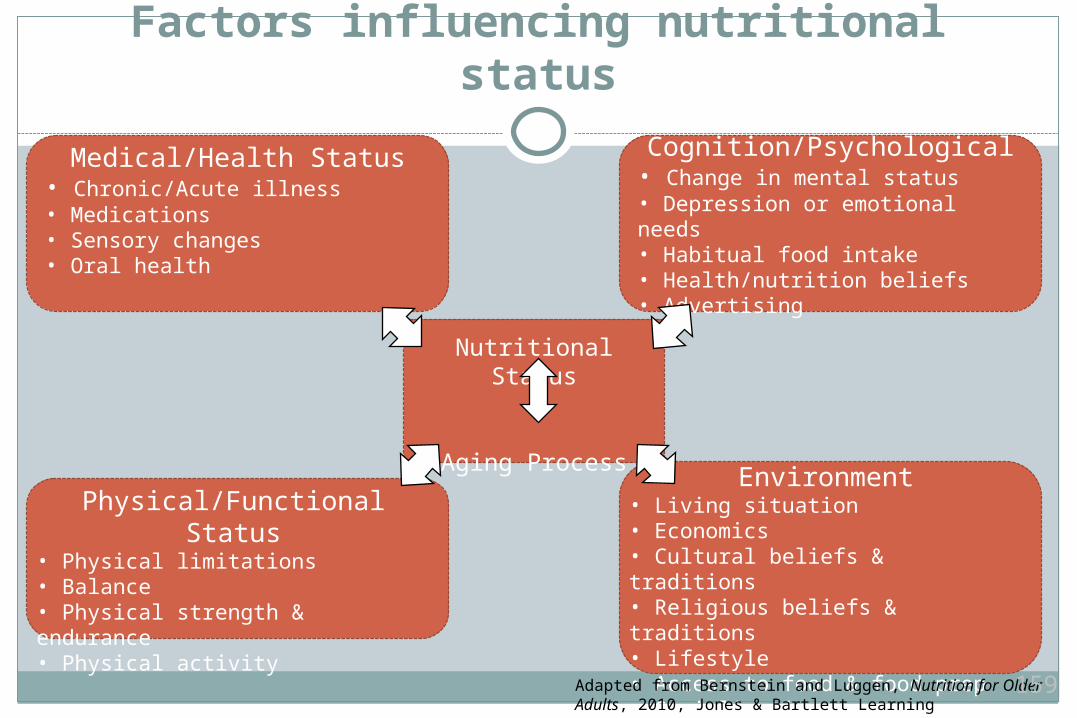
Factors influencing nutritional status
Nutritional Status
Aging Process
Physical/Functional Status• Physical limitations• Balance• Physical strength & endurance• Physical activity
Environment• Living situation• Economics• Cultural beliefs & traditions• Religious beliefs & traditions• Lifestyle• Access to food & food prep• Socialization
Medical/Health Status• Chronic/Acute illness• Medications• Sensory changes• Oral health
Cognition/Psychological• Change in mental status• Depression or emotional needs• Habitual food intake• Health/nutrition beliefs• Advertising
Adapted from Bernstein and Luggen, Nutrition for Older Adults, 2010, Jones & Bartlett Learning
159

Medical & Health Status Factors
Medical conditions – acute & chronic Diabetes, infection, head injury
Medications Common culprits
Dysgeusia: Lithium, ACE inhibitors, some antibiotics, cancer drugs, chlorhexadine mouthwash, thyroid medications, metformin
Xerostomia: Anticholinergics, diuretics Constipation: Anticholinergics, antiparkinsonian meds Altered absorption/metabolism: proton pump inhibitors, metformin
Diminished smell/taste with advancing ageOral health – less saliva
160
Physical & Functional Status
Less physical activity is commonDiminished ability to chew/swallowAbility to prepare food impacted by functional statusReduction in energy needs impacts ability to meet
nutrient requirements Eating ‘nutritionally dense’ foods even more important
161
Cognition/Psychological Impact
Impacts ability to prepare foodsFood choices may be impacted by habits (good/bad)DepressionLabeling/advertising readabilityNutrition beliefs
162
Environment
Living situation Independent Assisted living Safety
EconomicsCultural/Religious beliefs/traditionsAccess to food – food security
Availability of nutritionally adequate and safe food
Socialization
http://www.ers.usda.gov/topics/food-nutrition-assistance/food-security-in-the-us/definitions-of-food-security
163
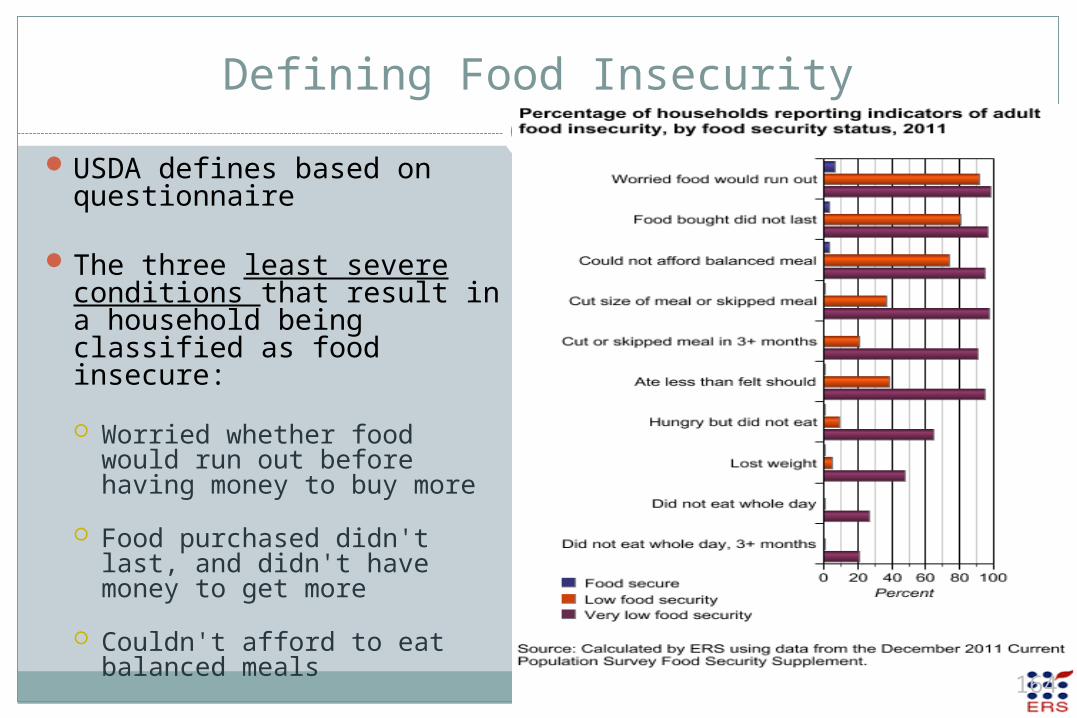
Defining Food Insecurity
USDA defines based on questionnaire
The three least severe conditions that result in a household being classified as food insecure:
Worried whether food would run out before having money to buy more
Food purchased didn't last, and didn't have money to get more
Couldn't afford to eat balanced meals
164
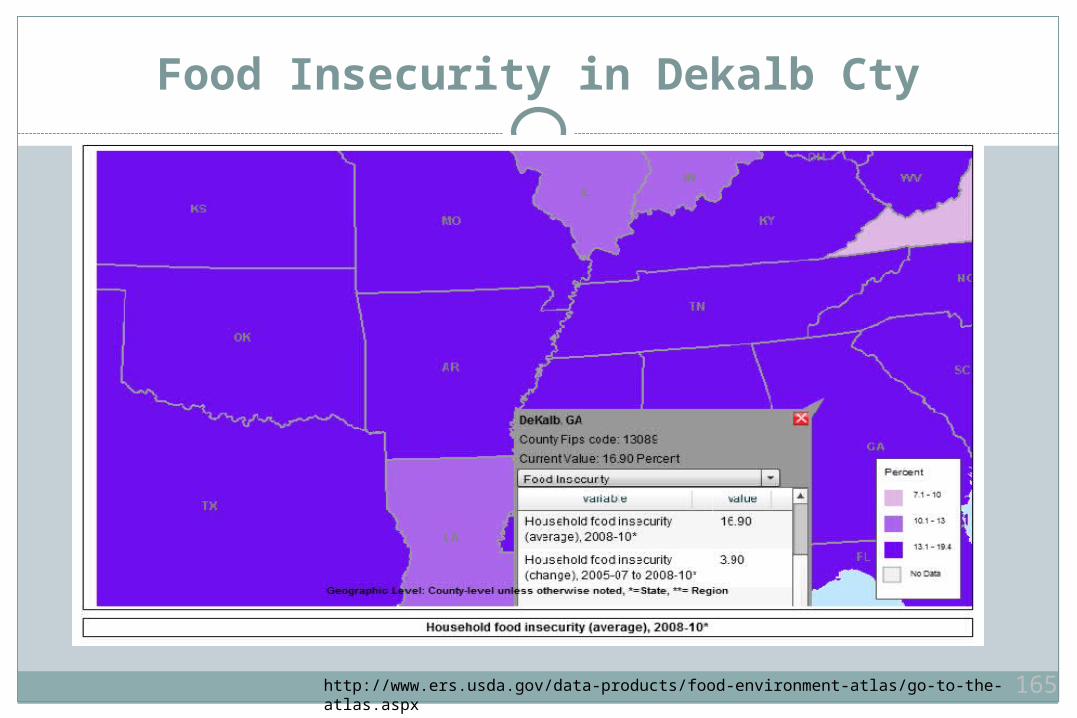
Food Insecurity in Dekalb Cty
http://www.ers.usda.gov/data-products/food-environment-atlas/go-to-the-atlas.aspx 165
Food Insecurity
Risk factors for food insecurity among older adults Income below poverty line Population subgroups – ethnic minorities/rural Lower educational level Disabled Living with a grandchild Supplemental Nutrition Assistance Program (SNAP)
166
Nutrient Requirements
Physiologic changes of aging Total energy requirements decrease with aging
Primarily due to decreased physical activity Loss of skeletal muscle mass
Loss of 15% of fat free mass between age 30 and age 80 Increase in body fat and visceral fat Renal function
Diminished ability to concentrate urine Blunted thirst sensation
Most vitamin and mineral needs remain constant or increase despite need for lower caloric intake
167
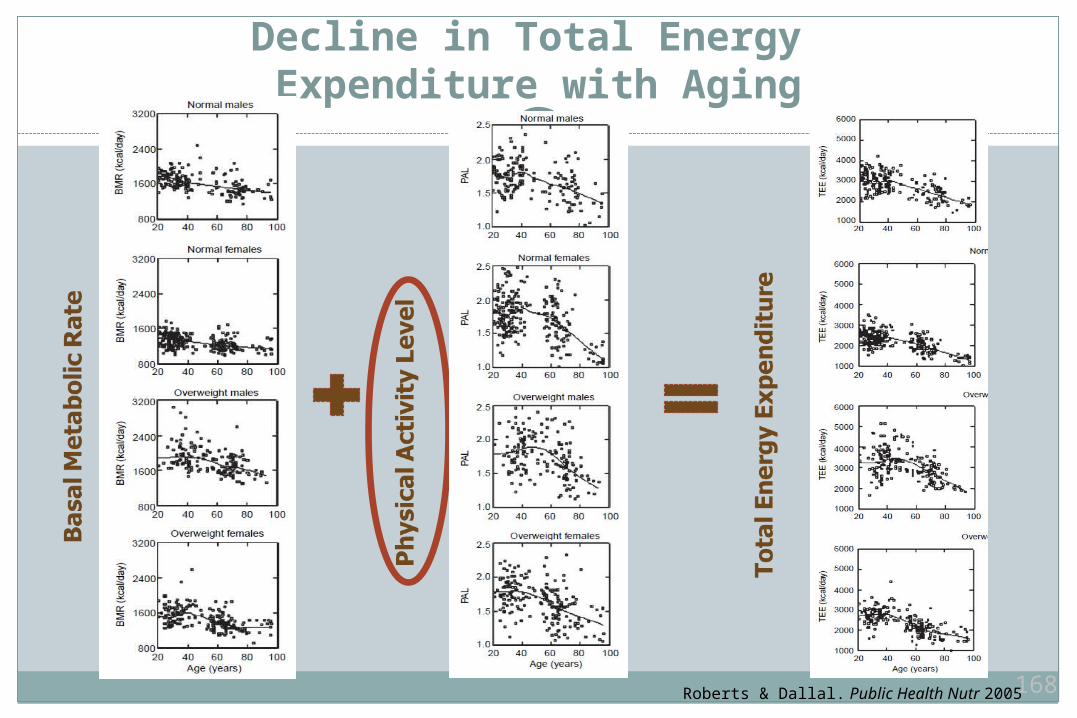
Decline in Total Energy Expenditure with Aging
Roberts & Dallal. Public Health Nutr 2005 168
Nutrients Requirements
Reference standards developed by the IOMRecommended Dietary Allowance (RDA)
Started in 1941 Intake which is adequate for about 97-98% of healthy persons
Dietary Reference Intakes (DRI) Started in early 1990’s by FDA More comprehensive – subsets for different age
groups/men/women Include RDAs as well as other measures (like Adequate Intake
[AI] when RDA is not established)
169
Nutrient Requirements
Fluid (includes high moisture foods) DRI for men ≥ 19 yrs = 3.7 L/day (no change for > 70 yrs) DRI for women ≥ 19 yrs = 2.7 L/day (no change for > 70 yrs) General recommendations in the clinic:
6-8 eight oz glasses of fluid daily
Dehydration is a major problem in older adults Increases risk of constipation, impaction Increases risk of kidney injury in the event of an acute event like infection/fall
www.iom.edu 170
Nutrient Requirements
Fiber DRI for women ≥ 50 yrs = 21 g/day DRI for men ≥ 50 yrs = 30 g/day May be difficult to meet DRI without choosing fiber-rich foods Foods low in fiber
Usually have inferior nutrient composition Contribute to discretionary energy intake (increase risk of obesity)
In patients with poor appetite – high-fiber foods may lead to early satiety
Adequate fluid intake is essential with fiber recommendations
High fiber foods: pears, bran, whole grains, prunes, walnuts
www.iom.edu 171
Nutrient Requirements
Protein RDA women & men ≥ 19 yrs = 0.8 g/kg/day
56 g/day for men, 46 g/day for women May be difficult with limited resources, reduced appetite Role of protein in the prevention of sarcopenia - unclear
www.iom.eduTroyer et al. Am J Clin Nutr 2010172
Nutrient Requirements
Sodium DRI for women & men ≥ 70 yrs = 1,200 mg/day Upper Limit = 2,300 mg/day Most Americans consume 3,000 – 4,000 mg/day Delivering meals meeting DASH guidelines can improve
adherence among older adults
High sodium foods to avoid: white breads, chips, soups, processed foods
www.iom.eduTroyer et al. Am J Clin Nutr 2010 173
Nutrient Requirements
Vitamin D Vit D RDA for men & women ≥ 70 = 800 IU/day
Classically recommended to prevent osteoporosis Vitamin D levels insufficient in most and deficient in
many older adults At least 800 IU/day associated with decreased risk of
fallingGood sources: sun exposure, salmon, fortified foods
www.iom.eduHolick et al. NEJM 2007 174
Nutrient Requirements
Calcium Calcium RDA for men & women ≥ 70 = 1200 mg/day Calcium supplements (not dietary Ca) linked to increased
risk of MI (regardless of dose)
Good sources: broccoli, low-fat yogurt/cheese/milk
www.iom.eduLi et al. Heart 2012 175
Nutrient Requirements
B12 RDA for women & men ≥ 19 = 2.4 mcg/day Estimated 6-15% of older adults are deficient Causes: pernicious anemia, atrophic gastritis, associated
with some drugs – metformin, lack of intrinsic factor No mandated fortification Complications of B12 deficiency: neurocognitive,
peripheral neuropathy, macrocytic anemia, elevated homocysteine
176
Nutrient Requirements
Folate (fortification since 1998) RDA for women & men
≥ 19 = 400 mcg/day Excessive folic acid
intake could mask B12 deficiency
177
Nutrient Requirements
Antioxidants Vitamin E, C, beta carotene, lutein, selenium, others Inconclusive research regarding antioxidant effects on vision
(macular degeneration) and cognition Recent meta-analysis: omega-3 showed modest benefit to
reduce MI risk
Vitamin K AI for women ≥ 19 yrs = 90 mcg/day AI for men ≥ 19 yrs = 120 mcg/day Important for blood clotting, bone health
www.iom.eduRizos et al. JAMA 2012 178
Overweight & Obesity in Older Adults
Weight management complicated in older adultsLoss of excess fat mass can accelerate loss of
muscle risk factor for decrease functional capacity Combining with exercise may help prevent muscle loss
Weight loss (even 5-10%) in overweight/obese older adults can result in improvements: Improved quality of Life Reduced medical complications Lower CVD/diabetes risk factors Reduced disability Less mechanical strain on joints
Frimel et al. Med Sci Sports Exercise 2008 179
Overweight & Obesity in Older Adults
Sarcopenic obesity Coexistence of age-related loss of muscle mass/function
and excess body fat Identification based on grip strength and BMI Likely potentiates effects on disability, morbidity, and
mortality Prevalence ranges from 3.0% - 12.4% depending on the
definition used
Stemholm et al. Curr Opin Clin Nutr Met Care 2008 180
Medical Nutrition Therapy
Provided by a Registered Dietician (RD) or Dietetic Technicians, registered (DTR)
Medical Nutrition Therapy can include: Nutrition assessments Individualized interventions Counseling Management of parenteral feedings End-of-life care
Covered by Medicare for diabetes and renal diseaseAlso can be bundled in some home health servicesScreening Tool: Mini-Nutritional Assessment
181
Community-based Resources
Older Americans Act Nutrition Services Title III program started in 1965 Provides congregate and home-delivered meals In 2009, 149.1 million meals were delivered to 880,135
individuals In 2008, 61% of meals delivered to homebound older adults In the Atlanta area – Senior Connections serves about 700,000
meals per year (Meals on Wheels)
Delivery of meals within DASH guidelines increases adherence to dietary recommendations for older adults with CVD
Troyer et al. Am J Clin Nutr 2010 182
Community-based Resources
USDA Food and Nutrition ProgramsSupplemental Nutrition Assistance Program (SNAP)
Coupons or electronic benefits for nutritionally adequate food Bread, fruit/vegetables, meats, fish, poultry, dairy products,
seeds, or plants that produce food US citizens and legal residents Gross income ≤130% federal poverty level
Seniors’ Farmers Market Nutrition Program Coupons/vouchers to exchange at local farmer’s markets
183
Community-based Resources
How to access or assess eligibility?Atlanta Area Agency on Aging
www.agewiseconnection.com 24-hour referral line: 404 463 3333
Senior Connections (eligibility varies by county) www.srconn.com Emory Dept of Medicine supports
184
Jonathan M. Flacker MD AGSFAssociate ProfessorDivision of General Medicine and Geriatrics(with thanks to Dr. Adam Herman)
External Industry Relationships * Company Name(s) Role
Equity, stock, or options in biomedical industry companies or publishers**
Stock (JNJ)
Board of Directors or officer No
Royalties from Emory or from external entity
Nope
Industry funds to Emory for my research
Absolutely not
Other Nah
*Consulting, scientific advisory board, industry-sponsored CME, expert witness for company, FDA representative for company, publishing contract, etc.**Does not include stock in publicly-traded companies in retirement funds and other pooled investment accounts managed by others.
Dr. Jonathan Flacker Personal/Professional Financial Relationships with Industry within the past year
187
By the end of this session the student will be able to:
Describe 3 ways to make the environment conducive to a discussion about bad news
Demonstrate how to begin a discussion of bad news
Compare and contrast effective techniques for delivering bad news with good techniques
188
An iterative processAll components revolve around
knowledge and communication Common symptoms Individual preferences Cultural beliefs and values
Recognized and communicate to patients that they are dying
189
Communication is key Ethical obligation to discuss dying with
patients
“Physicians have the DUTY to inform their patients about their illness and
patients have a RIGHT to know.“ (Nicholas Christakis MD)
Why?
190
If you are not prepared you can not plan
For a gameFor a school For a babyFor a death
Must we must tell our patients (and families?) How can they prepare otherwise?
191
So how do you broach such a sensitive topic?
You know they are dyingPatients and family often knowEvery one’s afraid to talk about it
… not discussing death and dying is the elephant in the room
192
Components:ActorsSetting/environmentCommunication (language)
193
Mrs. Benford is here today to discuss tests resultsShe knows she
Has cancer
Is weak, in pain, and has lost 20 lbs Doctor knows
Despite treatment cancer has spread
There is no curative therapies We will have ‘time-outs’ to discuss key points in discussing death and dying
194
What do you think?
195
Who should be present?
Doctor Patient Family Other
196
What is appropriate environment?Quiet
Undivided attention (no interruptions) Focus on patient and family (body
language) Limit topics Kleenex
Let’s fix what’s happened and watch some more…
197
What do you think?
198
Rule #1: Attentive Listening Listen Listen ListenCorollary : Avoid information overload
- they won’t hear it anyway
Let them tell you what they understand and what they want to know
199
The one minute managing test
200
Rule #2: Open ended questions More information in less time Allows patient and family to prioritize Listen and reflect concerns
Corollary to Rule #2: Close ended questions assumes the doctor knows the priorities of patient and family
201
Examples:
“What changes have you noticed… ?”
“What has changed for you… ? How?”
“What do you understand about your
illness(es)?
“How has it changed recently?”
202
Examples (cont):
“What do you think is happening to you”
“… Tell me more about that…”
Let’s watch some more…
203
What do you think?
What is NOT being said?
204
Rule #3: Acknowledge the elephant in the room Say the words Let it lie… Allow time for response
Corollary : Avoiding the elephant prevents you from fulfilling your duty as a physician
If accomplished, you have the ability to move forward and set priorities and goals of care 205
Rule #4: Give patient (and family) some wiggle room
Absolutes lead to polarization and
confrontation
Allows patient and family to talk
‘hypothetically’
Corollary : People put in a corner may become defensive, angry, and distrustful
206
Rule #5: Silence is your friend Let your statement and questions hang
Let your statement and questions sink in
Corollary : If there is no silence, you forgot Rule #1 and your patient can’t process
PracticeDon’t just do something…sit there…..
207
How do we acknowledge the elephant?First…
Combine direct language (“death”, “dying”)WITH…
ambiguous modifiers (“might”, “possible”) This allows ‘wiggle’ roomSecond…
Silence is your friend This allows time to consider your statement
208

Examples:“Have you ever thought that you might be
dying?”
“Have you ever thought about your own death?”
(let it hang…)
209
“No one can know for sure exactly what’s going to happen. But it’s
possible you might be dying. So, it’s important to be prepared. That way all
the bases are covered and you and your family will be ready whenever it
occurs.”
(silence…)210
“All of us need to be prepared for death so that when it happens nothing is left unsaid or undone. Whether you die today or 10 years from now, it’s
good to be prepared…”“If (hypothetically) you died today, what
would be left unsaid or undone…”(let it lie…)
211
“No matter what you choose (treatment or no treatment), your life is limited. The
task is still to get prepared for your death so you will be ready and that’s a good
thing.”
(let it hang out there…)
212
“Every day from today until the day you die is very precious. The fact that you have this __(insert condition/illness)_ means you may have even fewer days, which makes each day even
more precious… How do you want to spend that time?”
(silence…)
213
“Pretend like you knew you were going to die today. What hopes would you have?
What is your idea of a ‘peaceful’ death…”
(let it hang out there…)
214
“…I’m a bit hesitant to bring this up, yet I know it can be very important to patients in your situation to talk about. Most patients tell me they think about death as they are growing
older and getting weaker. That’s a healthy thing to do…so we can be prepared for it…”
(silence…)
215
What is the goal? …
… to acknowledge death and dying and allow patients and their families to set priorities and goals of care with this knowledge in hand.
Let’s see what happens…
216
Two major ways: The Living Will Power of Attorney for Health Care
217
Usually covers specific directives course of treatment forbidding treatment
Effective ONLY if the person can’t give informed consent
218
Appoints individual (a proxy) to direct health care decisions
Effective ONLY if the person can’t give informed consent
219
Recognizes that: Dying is a normal process of living Affirms life - neither hastens nor
postpones death Belief that through appropriate care,
individuals and their families will attain a degree of satisfaction in preparation for death
220
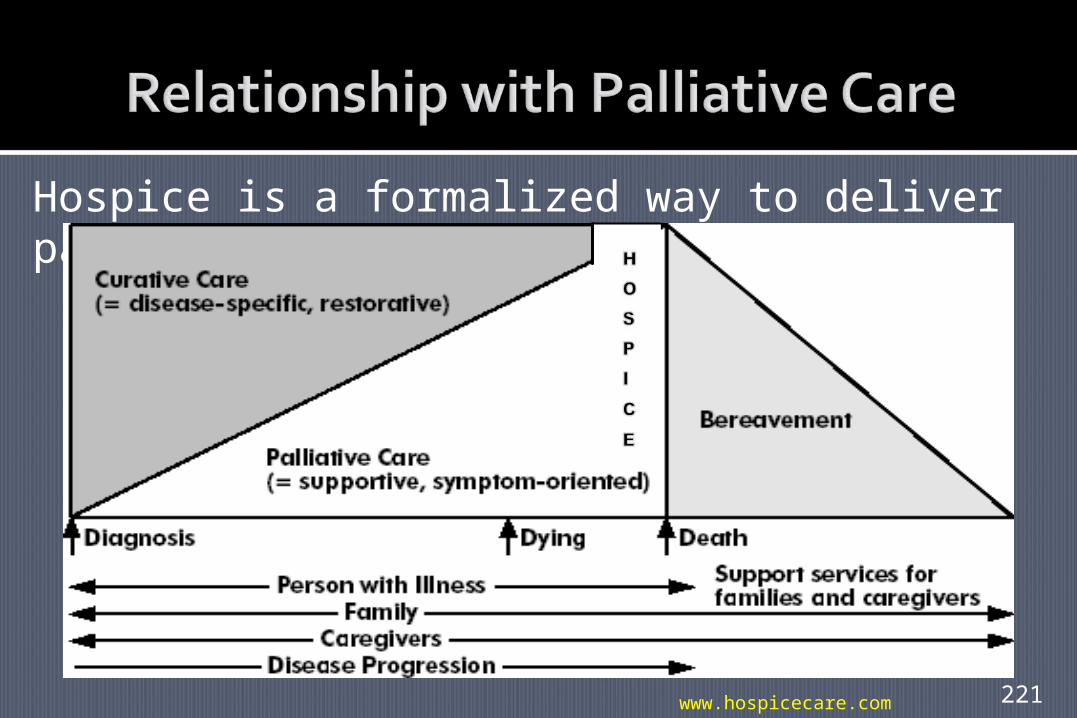
Hospice is a formalized way to deliver palliative care
www.hospicecare.com 221
Acknowledge the elephant
Tell patients what to expect
Act as a guide through the dying process
Continue to be their doctor (do not abandon)
Let’s see what happens…
222

By the end of this session the student will be able to:
Describe 3 ways to make the environment conducive to a discussion about bad news
Demonstrate how to begin a discussion of bad news
Compare and contrast effective techniques for delivering bad news with good techniques
223



























![NHW Academic Skills Level 3 TG [Shrunk]](https://img.dokumen.tips/doc/110x75/577cd8a81a28ab9e78a1ab05/nhw-academic-skills-level-3-tg-shrunk.jpg)

