Embed Size (px)
Citation preview

ORIGINAL PAPER
Introducing tablet computers into medical practice: designof mobile apps for consultation services
Martin Radzuweit & Ulrike Lechner
Received: 1 September 2013 /Accepted: 12 December 2013 /Published online: 27 December 2013# IUPESM and Springer-Verlag Berlin Heidelberg 2013
Abstract Regular patients consultations are important ele-ments of intervention programs that try to reduce incidenceof chronic diseases and lower related healthcare expenses.Tablet computer offer novel approaches for design and deliv-ery of services like intervention consultations. In case of theINVADE intervention program, a shared tablet computer isintroduced to promote consultations between patients andassistant nurses. Following a Design Science approach, threeiterations of building the application prototype have beencompleted and are described along with results from prototypeevaluation. The paper at hand is focused on the implementa-tion of the desired IT-artifact and we reflect on the applicationdevelopment process. We contribute to the understanding ofbuilding mobile applications for co-located service deliverythat are designed to foster interaction and supportcommunication.
Keywords Patient consultation . Co-located collaboration .
Tablet computer .Mobile app
1 Introduction
The INVADE intervention program, established in year 2001,combines about 60 general practitioners (GP) and about 4,000patients in the Bavarian district of Ebersberg, near Munich.The interventions’ goal is to lower incidence of stroke anddementia and related healthcare costs by continuously moni-toring cardiovascular disease status and treatment of risk
factors like hypertension, diabetes, lipometabolic disorder,overweight and sedentary lifestyle as well as stress, smokingand alcohol consumptions [1]. Several studies validated pos-itive effects and the intervention success [2–5].
Besides regular patient examinations, an intensive consulta-tion program was established, in which enlisted patients areregularly supervised by specially trained doctoral assistants,who are called intervention assistants. The patient consultationsfollow the principle of motivational interviewing [6], in whichintervention assistants record health conditions, educate patientsto foster health literacy and set and control health related goals aswell as try to motivate patients towards compliant behavior.
The INVADE management wants to support the interven-tion outcomes by delivering a standardized program, ensuringquality of data for analysis and fostering quality of care. Oneelement to meet the management goals is to improve thepatient consultations by introducing a shared tablet computerapplication, which offers a novel way of delivering the con-sultations. The desired application should support both thepatient and intervention assistant during consultation andshould augment the communication, the existing consultationprocess and further attract patients.
Tablet computers form a new class of computer and arecharacterized by their mobility due to size and weight, intui-tive handling through touchscreen and gesture navigation aswell as low barriers concerning operations and maintenance incontrast to personal computers [7, 8]. Besides, tablet com-puters offer an innovative concept of software delivery, asthere are generally no broad comprehensive applications formultiple uses, instead there are many small programs fordedicated use cases. These applications or so called “apps”or “mobile apps” are an important success factor for tabletcomputer in consumer sector and offer innovative ways forservice design and delivery in organizational context.
Following a Design Science approach [9], we develop andevaluate the so called INVADE consultation assistant tool
M. Radzuweit (*) :U. LechnerUniversität der Bundeswehr München, Werner-Heisenberg-Weg 39,85577 Neubiberg, Germanye-mail: [email protected]
U. Lechnere-mail: [email protected]
Health Technol. (2014) 4:31–41DOI 10.1007/s12553-013-0070-7

(ICAT), which is conceived as an app for co-located collabo-ration during patient consultations. Co-located collaborationare situations, in which individuals work together to seek acommon goal and are co-present, i.e. they are in the sameplace at the same time [10]. In general, collaboration technol-ogy are Information Systems designed to support interactionsbetween individuals by replacing or augmenting verbal com-munication and to facilitate processing of information [11].Typical co-located collaboration technologies are tabletopsystems and interactive spaces like electronic meeting rooms[12].
Models for co-located collaboration technology differ indesign of the user interfaces for input and output. Stewart et al.[13] define a general model of Single-Display-Groupware,which are shared computer systems with one public outputchannel and many private input channels. Other models com-bine multiple input and output for private work with a sharedoutput device for public work [10]. Tablet computers onlyhave a single input and output channel, so that the use of ashared tablet computer in collaborative environments is anovel approach. Nonetheless, collaboration technology usedin co-located environments like medical consultations caninhibit the interaction between individuals and lower engage-ment [14]. Thus, our research goal is to determine how todevelop and implement a shared tablet computer applicationsfor co-located service delivery like medical consultations.
We conducted three iterations of design and implementa-tion of a co-located collaborative tablet application for theINVADE intervention program. The paper at hand is an ex-tension of [15], in which we presented the first two designcycles. We demonstrate our design iterations and explain thechanging approaches and technologies. We further describeand examine results from evaluation of the prototype. Byanalyzing the results of our research approach, we contributeto the understanding of the ar t i fact design andimplementation.
The remainder of this paper is structured as follows. Sec-tion 2 describes our research design against the background ofDesign Science and strategies for mobile app development.The following three sections describe the three iterations ofprototype development and evaluation. Section 6 discussesour findings and conclusions concerning artifact design andimplementation.
2 Research design
Following a Design Science approach we develop and evalu-ate an IT-artifact that is indented to solve an organizationalproblem [9, 16]. IT-artifacts are constructs, models, methodsor instantiations [9, 17]. Instantiations like implemented sys-tems and prototypes are suitable to address a new problemarea and to deliver a sufficient problem solution [18]. March
and Smith [17] define the general design process as to buildand evaluate, in which building a prototype demonstratesfeasibility and evaluation analyzes, how well an IT-artifact issolving the organizational problem. Conducting Design Sci-ence is a search process, which is inherently iterative [9].
We conducted a cyclical process of problem formulation,suggestion, development and evaluation [19, 20]: The prob-lem formulation aims to justify a solution by showing themotivation for the research and explaining the comprehensi-bility of a problem. Objectives of the solution are developed tofurther operationalize goals from problem formulation, whichare implemented through design and development and mea-sured through demonstration and evaluation.
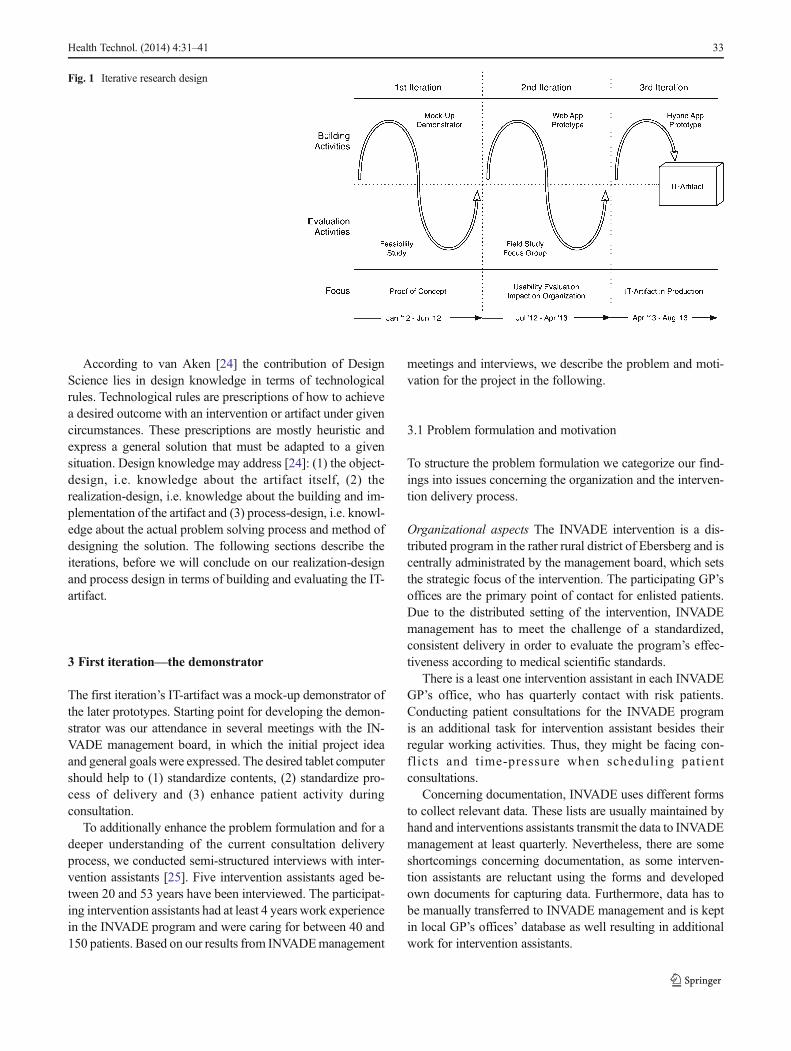
Figure 1 depicts our iterative design approach consisting ofthree cycles of building and evaluation starting from the firstiteration that was a demonstrator, a mock-up of the later ICATprototype from second and third iteration. When building theprototypes, we used two different implementation paradigmsfor tablet computer applications; Web app and hybrid app.General implementation strategies for mobile apps are de-scribed in the following.
Charland and Leroux [21] distinguish between apps basedon native andWeb code. Huy and vanThanh [22] take a closerlook on Web apps and define four application categories:native apps, mobile widgets, mobile Web apps and HTML5mobile apps, whereas Heitkötter et al. [23] differentiate be-tween native apps and cross-platform approaches and give acomprehensive comparison of development paradigms. Wewill follow the later and distinguish three development ap-proaches: (1) native, (2) Web and (3) hybrid applications.
Native apps are developed for a specific target operatingsystem (OS). As native apps are usually compiled andinstalled, they generally run faster thanWeb apps, whose codeis interpreted. Native apps have broader support for and accessto low-level libraries to use hardware features like storage,geo-location, camera and other sensors. The user interface ofnative apps offers the look-and-feel of the OS. Using nativeapps with different OS means developing the same app sepa-rately for each target device resulting in more effort [21, 23].
In contrast, Web apps are not installed; they are hosted by aWeb server and accessed via an URL. As they are opened in abrowser, they can be accessed from any OS that includes aWeb browser. They make use of common Web technologieslike HTML, CSS and JavaScript. Thus, Web apps do not haveaccess to hardware features and might not offer a native userinterface. Web apps support devices with less effort on pro-gramming and deliver adequate performance [21], which isminor in case of ICAT.
Finally, hybrid apps are bridging the gap between thebefore-mentioned approaches. Hybrid approaches can be usedfor cross-platform app development like Web apps, as theyrely on Web technology, but they also offer native-like accessto hardware features [21, 23].
32 Health Technol. (2014) 4:31–41
According to van Aken [24] the contribution of DesignScience lies in design knowledge in terms of technologicalrules. Technological rules are prescriptions of how to achievea desired outcome with an intervention or artifact under givencircumstances. These prescriptions are mostly heuristic andexpress a general solution that must be adapted to a givensituation. Design knowledge may address [24]: (1) the object-design, i.e. knowledge about the artifact itself, (2) therealization-design, i.e. knowledge about the building and im-plementation of the artifact and (3) process-design, i.e. knowl-edge about the actual problem solving process and method ofdesigning the solution. The following sections describe theiterations, before we will conclude on our realization-designand process design in terms of building and evaluating the IT-artifact.
3 First iteration—the demonstrator
The first iteration’s IT-artifact was a mock-up demonstrator ofthe later prototypes. Starting point for developing the demon-strator was our attendance in several meetings with the IN-VADE management board, in which the initial project ideaand general goals were expressed. The desired tablet computershould help to (1) standardize contents, (2) standardize pro-cess of delivery and (3) enhance patient activity duringconsultation.
To additionally enhance the problem formulation and for adeeper understanding of the current consultation deliveryprocess, we conducted semi-structured interviews with inter-vention assistants [25]. Five intervention assistants aged be-tween 20 and 53 years have been interviewed. The participat-ing intervention assistants had at least 4 years work experiencein the INVADE program and were caring for between 40 and150 patients. Based on our results from INVADEmanagement
meetings and interviews, we describe the problem and moti-vation for the project in the following.
3.1 Problem formulation and motivation
To structure the problem formulation we categorize our find-ings into issues concerning the organization and the interven-tion delivery process.
Organizational aspects The INVADE intervention is a dis-tributed program in the rather rural district of Ebersberg and iscentrally administrated by the management board, which setsthe strategic focus of the intervention. The participating GP’soffices are the primary point of contact for enlisted patients.Due to the distributed setting of the intervention, INVADEmanagement has to meet the challenge of a standardized,consistent delivery in order to evaluate the program’s effec-tiveness according to medical scientific standards.
There is a least one intervention assistant in each INVADEGP’s office, who has quarterly contact with risk patients.Conducting patient consultations for the INVADE programis an additional task for intervention assistant besides theirregular working activities. Thus, they might be facing con-flicts and time-pressure when scheduling patientconsultations.
Concerning documentation, INVADE uses different formsto collect relevant data. These lists are usually maintained byhand and interventions assistants transmit the data to INVADEmanagement at least quarterly. Nevertheless, there are someshortcomings concerning documentation, as some interven-tion assistants are reluctant using the forms and developedown documents for capturing data. Furthermore, data has tobe manually transferred to INVADE management and is keptin local GP’s offices’ database as well resulting in additionalwork for intervention assistants.
Fig. 1 Iterative research design
Health Technol. (2014) 4:31–41 33

Delivery process The intervention assistants’ tasks duringpatient consultation are to record health status, educate pa-tients foster health literacy and set and control health relatedgoals as well as motivate patients towards compliant behavior.In general, intervention assistants start consultations withmeasuring patients’ current blood pressure and build the fol-lowing conversation on the results and lead over to an educa-tional part before they discuss and set health-related goals.However, the process of delivery is not programmed and isadapted by intervention assistants depending on patients’behavior. For instance, when patients raise questions in thevery beginning, intervention assistants will relate to the ques-tions in the following, instead of proceeding and omitting thequestion.
Although, intervention assistants undergo the same train-ing, INVADE is facing differences concerning contents andprocess of patient consultations. Generally, intervention assis-tants use almost the same set of relevant topics, which are in-line with the INVADE goals, e.g. blood pressure self-measuring, physical activity, healthy food etc. Though, inter-vention assistants tend to focus on certain topics they favorand they also try to adapt themes and intensity to patients’progress and participation. Intervention assistants also takeaccount of their implicit knowledge about patients’ historyand personal circumstances like hobbies, family and partner-ship. Consequently, intervention assistants take in a dominantrole during consultations, whereas patients act primarilypassive.
At the same time, INVADE patients demand specific de-livery, as typical high-risk patients are aged between 70 and80 years, intervention assistants experienced, that patients’concentration and attention reduces considerably after10 min during consultations. Thus, they try to keep lessonsshort and make use of precise and simple language. Further-more, patients might loose interest or reject the INVADEprogram, when they are constantly reminded on the samehealth issues. Here, the intervention assistants refer to exam-ples like telling smokers about smoke cessation repeatedly ortelling overweight people to loose weight. Thus, interventionassistants try to alternate topics on the one side, but repeatinglessons is considered important to regain patients’ knowledge,on the other side.
Partly, some intervention assistants use brochures and leaf-lets from INVADE or third-party organizations for supportingthe educational lessons or as handouts for patients afterwards.Partly, some intervention assistants do without any kind ofinformation material, as they considered it as too general ortoo comprehensive for INVADE patients. Others use self-developed information material during education. Thus,supporting information material to be used in consultationsis heterogeneous, hardly formatted and scarcely medialsupported.
3.2 Objectives of the solution
Based on interview results and goal definitions made by theINVADE management, following three objectives were de-fined for the design of the IT-artifact and are discussed in thefollowing.
Firstly, standardizing contents is a primary objective ofICAT, as fostering patients’ health literacy is a major aspectof the patient consultations and crucial for the interventionsuccess. In general, health literacy increases patients’ controlover decisions and actions affecting their health [26] and isdefined as “motivation and ability of individuals to gain accessto, understand and use information in ways which promote andmaintain good health” [27]. Hence, a group of educationallessons should be developed to avoid differences in subjectsdiscussed during consultations and to provide a general set ofinformation that encompasses topics most relevant for IN-VADE patients. Unlike leaflets or brochures, educational les-sons for ICAT should not solely provide factual information,which is referred to as functional health literacy [28]. ICATlessons should also support the consultations by giving advice,so that patients act more self-confidently and independently, incombination with motivation by intervention assistants, whichis defined as interactive health literacy [28].
Secondly, the process of delivery should be standardized.Therefore, the IT-artifact should propose a guideline for thedelivery process formed by three core modules, which reflectthe workflow starting from status assessment to education andclosing with setting of health-related goals. Therefore, thereare modules for capturing patients’ health status and health-related goals besides the educational lessons. Nevertheless,intervention assistants may also change the order of modulesduring consultations to address patients individually and aspatients should not interact without interventions assistantswhen using the ICAT, the intervention assistants can stillintervene to meet patients’ needs. Additionally, the modulesfor status assessment and health-related goals should improvedocumentation of patient consultations and could replacepaper-based recording.
Finally, in order to enhance patient activity the IT-artifactshould offer additional features that deliver individual moni-toring to patients. On the one side, patients should be betterinformed, when their health status and health-related goals arecaptured. This should facilitate tracking patients’ progressover time throughout consultations. On the other side, inter-ventions assistants have better control over patients’ goals andachievements to better encourage them. Furthermore, contentsprovided during consultation should be designed in an attrac-tive, informative way and should be accomplished by interac-tive elements likes quizzes and risk calculator that attractpatients and make them think about their health status andrisk factors.
34 Health Technol. (2014) 4:31–41

3.3 Design and development
The first version demonstrator was a paper-based mock-up.It’s main part, the educational lessons, are designed as five toten pages concentrating on a specific topic, e.g. self-measuring blood pressure or the correlation of overweightand blood pressure. Already, it was very important to ensurequality criteria for health information [adapted from 29] likeevidence, completeness and readability, so that lessons werechecked by INVADE doctors and intervention assistants re-peatedly throughout the development.
Three main modules were developed that reflect themain task of intervention assistants during consultation:health status assessment, training patients with educationallessons as well as goal setting and monitoring. These threemodules are considered as guideline for consultation andshould provide a consistent process for consultation. Beforestarting with health status assessment, the intervention as-sistant needs to login and select a patient file. Beforeclosing a patient consultation, she needs to save the fileand can logout.
The demonstrator was also used to suggest on the applica-tion layout. The demonstrator layout is divided into threesections: a header section with primary navigation elementsand the current title, a footer section with additional informa-tion on the consultation sessions like patient name and date aswell as the main section as content area. Furthermore, iconsfor menus were introduced to allow an intuitive navigation.Each page has forward and backward arrows to browse thepages.
3.4 Demonstration and evaluation
The final demonstrator is a set of pages in a PDF-file,which are linked among each other, so we could alsodesign and demonstrate workflows and navigation in thisearly phase. The goal of the evaluation of the demonstratorfrom first iteration was to demonstrate general feasibilityand acceptance. Therefore, an analysis with interventionassistants from initial interviews and members of the IN-VADE management was conducted for evaluating thedemonstrator.
In order to simulate consultation sessions, participantsformed groups of two and used the demonstrator, which wasalready available on provided tablet computers. Our observa-tion was focused on handling the tablet computer and use ofmodules throughout the consultation. Results indicated gen-erally acceptance, although not all features were available atthis time. Suggestions for improvements were mainly abouteducational lessons in terms of readability, comprehensibilityand relevance of text or graphics.
4 Second iteration—the web application
As the first iteration showed promising results, the problemformulation and motivation for the ICAT project did notchange. The primary goal of the second iteration was todevelop an executable prototype building on the demonstratorfollowing the same objectives as defined in first iteration.Though, in the beginning of prototype development it wasstill unclear, which tablet computer will be provided in theINVADE GP’s offices and not all GP’s offices would mostlikely be provided with tablet computers, so that ICAT shouldalso be available on desktop computer, when needed. There-fore, the prototype had to be independent from target deviceoperating system and we decided to develop ICATasWeb appand not as native application programming.
4.1 Design and development
The Web app prototype is conceived as a three-layered Webapplication following the MVC-Pattern [30], see also [13].The object-oriented PHP framework ZEND [31] was used asbasis for the application structure and defines process andbusiness logic (Controller) as well as interactions with thedatabase (Model). The data layer is a MySQL database. Thus,no data is stored on the device. AWeb server was implement-ed to host the Web application and database. Finally, theView-Layer is extended with the JavaScript libraries jQuery[32] and jQuery Mobile [33], which offers a native look andfeel for mobile apps.
Figure 2 displays the Web app main page after an interven-tion assistant has logged in and loaded a patient record at thebeginning of a consultation session. The basic layout de-scribed in first iteration’s demonstrator can be recognized.The three modules for health status assessment (“MeineGesundheitsdaten”), educational lessons (“Schulungen”) andgoal setting (“Meine Gesundheitsziele”) form the guidelinefor interventions assistants during consultations. The otherthree elements are facilitating modules for important patientinformation (“Patientendaten”), access to archived consulta-tion sessions (“Letzte Sitzungen”) and charts for graphicallydisplaying measured and targeted health data (“Analyse”).
The facilitating modules are an add-on to the modules fromfirst iteration and accomplish patient monitoring features. Thepatient information module shows the summary of education-al lessons and offers a field to capture individual questions andremarks. The archive module offers patients and interventionassistants access to past sessions, so they can both track goalsset during last consultation and discuss the patients’ progress.The graphical analysis module visualizes the patients’ prog-ress by showing patients measured and targeted risk factorslike weight, body-mass-index and systolic blood pressure.
Health Technol. (2014) 4:31–41 35

4.2 Demonstration and evaluation
The demonstration and evaluation of the Web app prototypewas twofold: (1) a field study for usability evaluation duringpatient consultations with observation and questionnaire and(2) a focus group analysis with INVADE management boardto assess the impact on the organization.
Field study A field study was conducted with interventionassistants and patients for usability evaluation. The questionwas, how ICAT prototype supports both intervention assis-tants and patients during consultation. Thus, intervention as-sistants were asked to invite patients to routine consultationmeetings and a tablet computer with access to the Web appwas provided for each session. GP’s offices and interventionassistants that took part in interviews and evaluation fromdemonstrator development were not part of the prototypeevaluation. Two intervention assistants and eight patients werepart of the evaluation. Patients were aged between 59 and80 years; five female and three male participants. The consul-tations lasted between 15 and 22 min.
To assess usability, patients were given a questionnaireafter consultation meeting, intervention assistants were givena questionnaire after all sessions. The questionnaire was basedon constructs taken from the United Theory of Acceptanceand Use of Technology (UTAUT) [34]: performance expec-tancy, effort expectancy and facilitating conditions. Constructslike social influence were not considered, as ICAT is stillprototype and has not been introduced in INVADE GP’soffices yet.
Performance expectancy describes a person’s beliefs thatusing a system will help to improve his or her job perfor-mance. Venkatesh et al. [34] found performance expectancy as
strongest predictor of behavioral intention to use a system.Questions regarding performance expectancy contained per-ceptions about improved usefulness, efficiency and quality ofpatient consultation through ICAT usage. Effort expectancy isa person’s beliefs of ease that is associated with system usageand was assessed using questions regarding perceived ease ofuse, time and effort to learn and handle ICAT. Facilitatingconditions relates to a person’s beliefs on how organizationaland technical infrastructure supports use of a system. Consid-ering facilitating conditions, we examined ICAT’s compatibil-ity and fit to the aspects of consultations perceived by patientsand intervention assistants.
Furthermore, we wanted to examine if ICAT use is per-ceived as appealing and pleasant and consequently improvesconsultations by producing interest and fostering involve-ment. Therefore we used the construct of perceived enjoy-ment. Perceived enjoyment is defined as perceptions, thatusing a system is enjoyable ignoring any performance issues[35]. Perceived enjoyment has been found as cause and affectof perceived ease of use (effort expectancy) depending on thetype of information system under research [36]; in terms ofutilitarian information systems, that provide value to satisfyexternal objectives, e.g. improve job performance [37], per-ceived enjoyment is regarded as antecedent to perceived easeof use. In terms of hedonic information systems, that “provideself-fulfilling value to the user” [37 p.696], perceived enjoy-ment is a consequence. Furthermore the purpose of interactionwith hedonic systems lies in interaction per se and to promotecontinued usage is the main objective of hedonic systemdesign [37]. Though, ICAT is regarded as primarily utilitariansystem, information system design for lifestyle interventionsshould also consider hedonic aspects from patients for long-term usage to support long-term behavior change.
Fig. 2 Main page of Web appprototype
36 Health Technol. (2014) 4:31–41

Before attending the consultations for evaluation, we con-ducted a pre-test of the questionnaire with experts [see 38]. Thequestionnaire was presented to a group of two interventionassistants and three GPs from INVADE management board.Comprehensibility, structure and wording as well as relevancyof questions were evaluated and adapted if necessary.
To further analyze usage of ICAT, two researches partici-pated in each session to observe the process and the interactionof intervention assistants as well as patients with the ICATapplication. An observation sheet was created to record andanalyze the ICAT usage during consultation and identifyshortcomings. Besides patient gender and age, the observationsheet consisted of a timeline and a sketch area. The later wasused to layout the general positions of intervention assistants,patients and the tablet computer throughout the consultationsession. The timeline was used to record succession of ICATmodules and interactions of the intervention assistant likelogin, logoff and filling out forms as well as interactions ofpatients like navigating through educational modules. Diffi-culties in handling ICAT and patient questions were recordedas well. The timeline was used as it allows drawing conclu-sions from the sequence of actions while using the system.Additionally, noteworthy comments and remarks from bothpatients and intervention assistants were recorded on the ob-servation sheet.
All participants were asked for approval before consulta-tions. To avoid data privacy issues fictional user accounts andpatient profiles were set up and intervention assistants wereinstructed to record fictional data as well. Participating inter-vention assistants were given an introduction to ICAT similarto the presentation during focus group analysis with INVADEmanagement board. To assure comparability between familypractices, the introduction followed a written instruction guidecontaining explanations of the main menu and the consulta-tion process.
Focus group The objective of the focus group analysis withINVADE management was to assess the organizational fit ofthe prototype and tried to answer the question, how the pro-totype impacts the consultations in reference to the goals setby INVADE management.
The INVADE management was given an introduction tothe Web app prototype user interface and an overview aboutthe implementation and technical issues. The live prototypewas presented to the audience while explaining the standardworkflow. Afterwards the audience had the opportunity to tryout the prototype on their ownwith provided tablet computers.
In the following, the members of INVADE managementshould express their beliefs about the impact on the identifiedproject goals. A workshop technique was used [see 39], inwhich participants first note associations to a given topic onsticky notes. The center of a white board represents the maintopic; sections around the center denote relevant aspects of the
topic. Afterwards, sticky notes are arranged on the whiteboard; the more central a note, the more impact is associatedwith it. A group discussion moderated by two researches[following 40, 41] followed, in which participants explainedand discussed their associations and reasons for positioning.
Results from field study At one family practice, the interven-tion assistant and the patients were sitting opposite at the table.The tablet computer was laid down between them. At theother office, the intervention assistant was sitting next to thepatient on the edge of the table. The intervention assistant washolding the tablet computer during the conversation. Theanalysis of the timeline shows that in two out of eight consul-tations, the intervention assistant started consultation withgoal setting instead of health status assessment. Thepredefined guideline for consultations starting from healthstatus assessment, educational module to goal setting wasused the other times. Furthermore, observation analysis re-veals two other concerns concerning educational modules.Educational modules were partly regarded as too comprehen-sive. Some patient stated they already knew contents fromeducational modules, so that the intervention assistant skippedpages to save time. Whereas patients consider advice at theend of educational lessons as very positive and practicable tofoster healthier lifestyle and change habits.
Two patients were rather reluctant in first place and leaningbackwards in the beginning of the consultation. This changedduring consultation progress after about 14 to 16min and boththe patients leaned forward for better sight on ICAT duringpresentation of an educational module. The other patientswere rather open-minded, interested and were sitting close tothe tablet computer all the time.
Five patients actively used ICAT by operating the applica-tion, for instance to navigate through the educational lesson.These patients had no precariousness to control the applica-tion, which is remarkable regarding the rather high age ofparticipating patients. Patients navigated through the lesson ontheir own pace, so that their personal involvement and partic-ipation were increased.
The observed consultation sessions lasted rather long, asconsultations are usually between 10 and 15 min. This can berelated to the evaluation situation, in which intervention as-sistants had no experience with ICAT before except the intro-duction given by the researchers.
Out of eight questionnaires for patients, one was not com-pleted and was not considered for evaluation. From the re-maining seven patients, four rated ICAT in general high andvery high, respectively. All patients perceived usefulness andimpact of ICATon efficiency and quality of consultations highand very high except one patient, who rated performanceexpectancy very low. This patient was also very critical abouteffort expectancy. He or she was indicated to be overwhelmedand stated that ICAT was not easy to use at all, whereas all
Health Technol. (2014) 4:31–41 37

other patients valued ease of use as high, two of them evenvery high. All patients appreciated ICAT usage during con-sultation and stated, that ICAT fits the way his or her inter-vention assistant executes consultations. Concerning per-ceived enjoyment, all patients indicated ICAT usage wasneither boring nor dull and found it rather interesting andpleasant, but fun and entertainment while using ICAT wasperceived limited.
The questionnaire results from intervention assistants’show, that one intervention assistant perceived overall usabil-ity as very high; the other was generally a bit more reluctant.One rated all aspects of performance expectancy very high,whereas the other was ambiguous concerning improved effi-ciency of patient consultation through ICAT usage. ICATprototype was not perceived as hard to use or frustrating andoverwhelming, but both intervention assistants stated that theywould need somemore time to learn to handle the application.
Results from focus group Focus group analysis shows thatICAT is associated to have a high impact on contents throughthe educational lessons. The INVADE management believesthat all patients will be better educated and trained troughICAT, in general. Also, it is useful that the same informationis provided visually in forms of text and additional pictures.ICAT will give INVADE a new, modern image, according toINVADE management. The tablet computer application willraise interest of patients as well intervention assistants and willpromote patients’ attention and participation.
The impact on data quality was rated to be rather moderate,although the ICAT Web app offers features to record patients’health related goals and to track the lessons patient conducted.In fact, intentions and goals as defined by INVADE manage-ment changed afterwards, resulting in the development of thefinal hybrid app prototype, see next section.
5 Third iteration—the hybrid application
The Web app prototype was generally well accepted. Never-theless, the ICAT project was facing a turning point after thesecond evaluation. The objectives, which the INVADE man-agement was seeking in the beginning of the demonstratordevelopment, were modified due to changing priorities andconditions.
5.1 Changing objectives
The main contribution of the second iteration Web app proto-type was on guiding the consultation process through threecore modules and the support of information processingthrough data capturing modules. Furthermore, patients shouldbe activated through individualized analysis of health-relatedinformation. This resulted in a set of complex requirements in
terms of roles and access privileges for the database and theWeb app itself. In addition, ICATWeb app demands provisionof an appropriate infrastructure and a connection to the serverhosted by INVADE management.
It turned out in a survey initiated by the INVADE manage-ment that only one third of INVADE GP’s offices areequipped with Wireless LAN and mobile connection via 3Gis not available in every GP’s office of the rural district ofEbersberg. Additionally, some participating GP’s offices wererather reluctant to provide and use the needed infrastructure.Also, the costs and managerial complexity of operating anadditional server plus providing software for encrypted con-nections have been a factor. INVADE management ratedimportance of information processing capabilities rather mod-erate after second iteration evaluation and questioned theimpact on data quality. Thus INVADE management decidedto suspend the data processing features for status assessmentand goal setting and monitoring.
Furthermore, the intention behind activation of patientchanged from offering individualized monitoring features likethe graphical analysis of risk factors. The main contribution ofthe final tablet computer application concerning patient activ-ity is to foster participation during educational lessons. Thus,the desired objectives of third iteration changed: the followingICAT iteration should still offer a way of delivering standard-ized contents, on the one side, and activating patients bysupporting the interaction between intervention assistantsand patients, on the other side.
5.2 Design and development
The altering objectives resulted in fundamental change oftechnology switching from Web app to hybrid app approach.The third prototype was conceived as hybrid app that offers thedesired features and still can be run on any target OS. Themajor parts of the Web app could be transferred to the offlinepart of the hybrid app with rather minimal effort, as both relyon the same technology. Still, the hybrid app can be furtherdeveloped to offer additional functions, for example server-side access to database for more individual risk assessment andanalysis similar to the ideas from first and second iteration.
For implementing interactive elements, we relied onJavaScript technology. Primarily, sliders, forms and compara-ble elements were used to build quizzes, e.g. caloric consump-tion while doing different physical activities, calculation ofrisk factors, e.g. waist-to-hip-ratio, and estimation of nutrition,e.g. recommended alcohol consumption.
The interactive “Food Circle” exemplifies the principlebehind interactive elements created during third iteration.The “Food Circle”, which advices on healthy nutrition, isshown in Fig. 3: Patients operate sliders representing foodcategories to estimate percentage of intake for a dietary life-style. After submitting, sliders are greyed-out, but still visible,
38 Health Technol. (2014) 4:31–41

and patients and intervention assistants can compare anddiscuss results with the recommended nutrition, which isvisualized in the center as “Food Circle”.
Furthermore, tool-tip elements were used to offer on-sitehelp to explain interactive elements (see Fig. 3 “Hilfe”-But-ton). In a similar way to the Web app prototype, JavaScriptwas used to improve the layout by using appropriate structur-ing elements and provide a native look-and-feel based onJQuery Mobile libraries.
Lining up and balancing the scope of contents was veryimportant and realized through regular revision by INVADEmanagement. The additional revision of contents by interven-tion assistants was also important, as they helped improvingthe appropriate wording. The final educational lessons providegeneral, factual knowledge, especially in the beginning, alongwith interactive elements and are summarized and closed withpractical advice and hints for day-to-day decision making asdesired by patients.
Finally, INVADE management decided to increase thenumber of topics available and contributed additional educa-tional lessons and additional content. The researchers designefforts in this last round included standardization of layoutthroughout the various lessons in order to create a common,convenient layout for older patients that they are likely to read.For example, the concept of practical advice was enhanced, sothat lessons close with “INVADE empfiehlt Ihnen”, i.e. IN-VADE’s recommendations on the most relevant, practicalinstruction.
6 Summary and conclusion
In this paper we presented three iterations of a mobile appdevelopment for tablet computers, which will be used during
patient consultations to improve standardization of deliveryand foster patients’ participation and interest. We summarizeour findings from design iterations, before we conclude on therealization and process design.
Building the mock-up during first iteration was a suitableway for the ICAT development to generate fast results andshow feasibility of the project. The mock-up alreadycontained the modular structure of the final prototype withrelevant contents, primary processes and layout elementswithout regarding any implementation issues like choice oftechnology, target device and operating system. The visibledemonstration of the mock-up enhanced understanding be-tween researchers and end-users.
For second iteration, it was important to advance the dem-onstrator to a prototype, which can be brought into action. TheWeb app delivered a cross-platform prototype, which could beused within patient interaction and was evaluated in real-lifesetting during patient consultation. Results from second iter-ation evaluation show general acceptance of ICAT by patientsand intervention assistants. It is noteworthy, that patientsagreed, that applications provided on tablet computers likeICAT are suitable and fit, how intervention assistants executeconsultations. Simultaneously, patients found the ICAT appli-cation interesting and pleasant. Thus, the notion of INVADEmanagement is supported, that a tablet computer can positive-ly influence perception of the intervention program by pa-tients, which should result in a higher level of interest andparticipation.
Finally, worries concerning infrastructure and changingfocus of activation of patients from individual monitoring toactive participation changed objectives and resulted in a hy-brid app prototype. The final prototype is focused on aug-menting the communication between patients and interventionassistants, in a way that both patient and intervention assistant
Fig. 3 Interactive “Food Circle”of the nutrition lesson
Health Technol. (2014) 4:31–41 39

can navigate through lessons and handle the interactive partsof the content, whereas the second design iteration was influ-enced by ideas of integration of the prototype into the IT-landscape of the GP’s offices and of individualized capabili-ties like tracking health risks and outcomes—an idea central tothe “traditional” Web and many interactive Website designs.The third prototype is different, innovative in this respect. Theapp after the third iterations has a single purpose and isdesigned to facilitate collaboration and activation of the pa-tients during consultations.We argue that this one purpose andthis particular interactivity are two concepts that are specificfor tablet computers and service delivery through tablet com-puters in a co-located collaborative environment.
The choice of technology and implementation were majorchallenges and undergo several changes during the project.Each iteration followed different approaches for realizationand advanced the understanding of the collaborative settingand related requirements for co-located service delivery.
The implementation of a non-native application for tabletcomputers, i.e. Web app or hybrid app, was a suitable solutionfor developing fast prototypes with few distinct requirementsand cross-platform capability. In case of ICAT, the compo-nents of the IT-artifact are content-focused and should primar-ily provide information in terms of educational lessons tousers. Therefore HTML-based technology in combinationwith JavaScript frameworks is suitable to structure and layoutinformation needed. Furthermore, the layout is transferred toCSS-files and can be separately designed.
The educational lessons are a major benefit for INVADE.Standardization of contents was one primary goal of theproject. By delivering contents through ICAT, all participatingGP’s offices will work with a common set of information.Thus, the reliability of studies conducted by INVADE isimproved, as intervention assistants will educate patients ac-cording to a corporate standard. Nevertheless, INVADE isfacing the contradiction between the goal of standardizationand the needs of individual patients, as described in theproblem formulation. ICAT is conceived as augmenting com-munication and enhancing patient activity and patients willnot operate the application without guidance and in presenceof intervention assistants. Thus, intervention assistants canindividually explain and discuss health risks and behaviorand develop personalized health related goals together withpatients.
The execution of iterations of problem formulation, defin-ing objectives, development and evaluation allows construct-ing of evolving applications from primary, low-fidelity proto-types to final applications. Simultaneously, ongoing evalua-tion and close co-operation with users leads to better under-standing of their needs and adaption of requirements. Bringingprototypes into interaction and evaluation of usability is animportant part of the process, when designing mobile apps fortablet computers, as users need to touch and feel the prototype,
especially in co-located settings like medical consultation.Questionnaires were suitable for assessing usability duringthe field study and the construct of perceived enjoyment mightcontribute to design of applications for tablet computer andneeds further research. However, most important insight camefrom observations, which should include more users andconsider prolonged use. Therefore, third iteration prototypeevaluation will be focused on observing the interaction be-tween patients and intervention assistants as well as the impactof ICAT on their communication.
Conflict of interest The authors declare that they have no conflict ofinterest.
References
1. Scherpinski U, Bickel H, Gnahn H, et al. Interventionsprojekt zuzerebrovaskulären Erkrankungen und Demenz im LandkreisEbersberg (INVADE). Nervenarzt. 2002;73:1199–204.
2. Sander K. Signifikante Reduktion vaskulärer Risikofaktoren imRahmen des populationsbasierten Interventionsprojektes INVADE -Eine 2-Jahres-Verlaufsuntersuchung. DtschMedWochenschr DMW.2006;131:1853–9.
3. Sander D, Schulze-Horn C, Bickel H, et al. Combined effects ofhemoglobin A1c and C-reactive protein on the progression of sub-clinical carotid atherosclerosis: the INVADE study. Stroke. 2006;37:351–7. doi:10.1161/01.STR.0000199034.26345.bc.
4. Ulm K, Huntgeburth U, Gnahn H, et al. Effect of an intensive nurse-managed medical care programme on ambulatory blood pressure inhypertensive patients. Arch Cardiovasc Dis. 2010;103:142–9.
5. Etgen T, Sander D, Huntgeburth U, et al. Physical activity andincident cognitive impairment in elderly persons: the INVADE study.Arch Intern Med. 2010;170:186–93. doi:10.1001/archinternmed.2009.498.
6. Torsi S, Wright P, Mawson S, et al. The self-management of chronicillnesses: Theories and technologies. In: Pervasive computing tech-nologies for healthcare (PervasiveHealth), 2010 4th InternationalConference on-NO PERMISSIONS; 2010. p. 1–4.
7. Sturm S. Digitales storytelling: Eine Einführung in neue Formen desQualitätsjournalismus. 2013. doi:10.1007/978-3-658-02013-2.
8. Oelmaier F, Hörtreiter J, Seitz A. Apple’s Ipad Im Enterprise-Einsatz:Einsatzmöglichkeiten, Programmierung, Betrieb Und Sicherheit ImUnternehmen. 1–5. 2011. doi:10.1007/978-3-642-15437-9_1.
9. Hevner AR, March ST, Park J, Ram S. Design science in informationsystems research. MIS Q. 2004;28:75–105.
10. Arvola M. Interaction design patterns for computers in sociable use.IJCAT. 2006;25:128–39. doi:10.1504/ijcat.2006.009063.
11. Brown S, Dennis A, Venkatesh V. Predicting collaboration technol-ogy use: integrating technology adoption and collaboration research.J Manag Inf Syst. 2010;27:9–54. doi:10.2753/MIS0742-1222270201.
12. Scott S, Grant K, Mandryk R. System guidelines for co-located,collaborative work on a tabletop display. In: Kuutti K, Karsten E,Fitzpatrick G, et al., editors. ECSCW 2003. Netherlands: Springer;2003. p. 159–78.
13. Stewart J, Bederson BB, Druin A. Single display groupware: a modelfor co-present collaboration. In: Proceedings of the SIGCHI confer-ence on Human Factors in Computing Systems. Pittsburgh, PA:ACM; 1999. p. 286–293.
40 Health Technol. (2014) 4:31–41

14. Rodden T, Rogers Y, Halloran J, Taylor I. Designing novel interac-tional workspaces to support face to face consultations. 2003. 57–64.doi:10.1145/642611.642623.
15. Radzuweit M, Grütz S, Wenke B, Lechner U. Prototype design andevaluation of ICAT: A health application for tablet computer. 26thBled eConference eInnovations: Challenges and Impacts forIndividuals, Organizations and Society. 2013. doi:10.1145/777005.777015.
16. Baskerville R. What design science is not. Eur J Inform Syst.2008;17:441–3. doi:10.1057/ejis.2008.45.
17. March ST, Smith GF. Design and natural science research on infor-mation technology. Decis Support Syst. 1995;15:251–66.
18. March ST, Storey VC. Design science in the information systemsdiscipline: an introduction to the special issue on design scienceresearch. MIS Q. 2008;32:725–30.
19. Vaishnavi V, Kuechler W. Design research in information systems;2004.
20. Peffers K, Tuunanen T, Rothenberger M, Chatterjee S. A designscience research methodology for information systems research. JManag Inf Syst. 2007;24:45–77. doi:10.2753/MIS0742-1222240302.
21. Charland A, Leroux B. Mobile application development: web vs.native. Commun ACM. 2011;54:49–53. doi:10.1145/1941487.1941504.
22. Huy NP, Do vanThanh. Evaluation of mobile app paradigms. In:Proceedings of the 10th International Conference on Advances inMobile Computing and Multimedia (MoMM '12), Ismail Khalil,editors. New York: ACM; 2012. p. 25–30.
23. Heitkötter H, Hanschke S, Majchrzak TA. Evaluating cross-platformdevelopment approaches for mobile applications. In: Cordeiro J,Krempels K-H, editors. Lecture notes in business information pro-cessing. Berlin: Springer; 2013. p. 120–38.
24. van Aken JE. Management research based on the paradigm of thedesign sciences: the quest for field-tested and grounded technologicalrules. J Manag Stud. 2004;41:219–46.
25. Radzuweit M, Wenke B, Lechner U. Konzeption einesBeratungsassistenten für ein Interventionsprojekt. In: Goltz U,Magnor MA, Appelrath H-J, Matthies HK, Balke W-T, Wolf LC,
editors. GI-Jahrestagung (pp. 1182-1193), : GI. ISBN: 978-3-88579-602-2.
26. Nutbeam D. Evaluating health promotion—progress, problems andsolutions. Health Promot Int. 1998;13:27–44. doi:10.1093/heapro/13.1.27.
27. Nutbeam D. Health promotion glossary. Health Promot Int. 1998;13:349–64. doi:10.1093/heapro/13.4.349.
28. Nutbeam D. Health literacy as a public health goal: a challenge forcontemporary health education and communication strategies into the21st century. Health Promot Int. 2000;15:259–67. doi:10.1093/heapro/15.3.259.
29. Coulter A. Engaging patients in healthcare. Open University Press;2011.
30. Reenskaug T. The common sense of object orientated programming;2008.
31. Zend Framework. Zend Technologies Ltd; 2006.32. jQuery. The jQuery Foundation; 2013.33. jQuery Mobile. The jQuery Foundation; 2013.34. Venkatesh V, Morris MG, Davis GB, Davis FD. User acceptance of
information technology: toward a unified view. MIS Q. 2003;425–478.
35. Davis FD, Bagozzi RP, Warshaw PR. Extrinsic and intrinsic motiva-tion to use computers in the workplace. J Appl Soc Psychol. 1992;22:1111–32.
36. Sun H, Zhang P. Causal relationships between perceived enjoymentand perceived ease of use: an alternative approach. J Assoc Inf Syst.2006;7:618–45.
37. van der Heijden H. User acceptance of hedonic information systems.MIS Q. 2004;28:695–704.
38. HäderM. Empirische Sozialforschung.Wiesbaden: Eine Einführung;2006.
39. Andler N. Tools für Projektmanagement,Workshops und Consulting:Kompendium der wichtigsten Techniken und Methoden. 4th ed.Limited: John Wiley & Sons; 2011.
40. Morgan DL. Focus groups. Annu Rev Sociol.1996;129–152.41. Byers PY, Wilcox JR. Focus groups: a qualitative opportunity for
researchers. J Bus Commun. 1991;28:63–78.
Health Technol. (2014) 4:31–41 41





























