Embed Size (px)
Citation preview

Intravenous lidocaine infusions
Dr Ian McConachie FRCA FRCPC

Thank the organisers for inviting me.
No conflicts or disclosures
Lidocaine
• 1st amide local
anesthetic
• Synthesized in 1943
by Lofgren in
Sweden.
• 1st marketed in 1949.

2016
Epidural Lidocaine IV

IV Lidocaine infusions Timeline
1960s
• General
Analgesia
1970s
• MI
Arrythmias
1980s
• Chronic Pain
1990s
• Renewed
Interest in
Intraoperative
infusions
2000s 2010s
• Postoperative infusions

IV Lidocaine infusions Timeline
1960s
• General
Analgesia
1970s
• MI
Arrythmias
1980s
• Chronic Pain
1990s
• Renewed
Interest in
Intraoperative
infusions
2000s 2010s
• Postoperative infusions

Bartlett EE. Anesth Analg 1961 ; 40 : 296-304


IV Lidocaine infusions Timeline
1960s
• General
Analgesia
1970s
• MI
Arrythmias
1980s
• Chronic Pain
1990s
• Renewed
Interest in
Intraoperative
infusions
2000s 2010s
• Postoperative infusions

MI
• Lidocaine infusions for minimum of 24hrs
following MI were standard therapy in in
the 1970s and 1980s in an attempt to
reduce arrhythmias.
Doses of up to 4g in 1st 24hrs.
• Pharmacokinetics of IV Lidocaine were
extensively investigated.

IV Lidocaine infusions Timeline
1960s
• General
Analgesia
1970s
• MI
Arrythmias
1980s
• Chronic Pain
1990s
• Renewed
Interest in
Intraoperative
infusions
2000s 2010s
• Postoperative infusions

Lidocaine and chronic pain
Resurgence of interest in
IV Lidocaine for acute pain
came from chronic pain
studies in 80s and 90s
where brief, high dose IV
infusions ( eg 5mg/kg
over 30minutes) can result
in long term pain relief.
This role is well
established

• 3 doses 1,3 and 5mg/kg.
• 1 and 3 no better than placebo
• Implies need a minimum blood level for analgesia
A randomized, double-masked, placebo-controlled pilot
trial of extended IV lidocaine infusion for relief of ongoing
neuropathic pain. Clin J Pain. 2006 ; 22 : 266-71.

IV Lidocaine infusions Timeline
1960s
• General
Analgesia
1970s
• MI
Arrythmias
1980s
• Chronic Pain
1990s
• Renewed
Interest in
Intraoperative
infusions
2000s 2010s
• Postoperative infusions

Mechanisms of action of systemic
lidocaine
• Not likely classic local anesthetic effects
on Na channels
• Not fully understood
• Not conventional pain pathways
• systemic effect of lidocaine occurs
predominantly in damaged ( postop ) and
dysfunctional ( chronic pain ) nerves

• Peripheral nervous system
• Spinal and supraspinal mechanisms
• Suppression of both peripheral and central
hyperalgesia
• Active at Spinal NMDA receptors
• Selectively inhibit GPCRs which activate Gαq proteins.
• Anti inflammatory

Anti inflammatory actions

For the skeptics - TAH
Anesth Analg 2009 ; 109 : 1464–9
Placebo
Lidocaine

Cortisol stress repsonse - LSCS
Placebo
Lidocaine
Journal of Anesthesia 2009;23:215–21

Stress response - Abdominal
ANZ J Surg 85 (2015) 425–429
S
L

Is it safe ?

• Lidocaine is intrinsically
one of the least toxic
LA drugs
• Only lidocaine has
been considered safe
for IV use because of
its long history of
administration as an
antiarrhythmic drug.


• Plasma levels lower with infusion
• Levels often higher with other uses of Lidocaine eg BP block, epidural etc
• Safety also established in MI studies in 80s
• So….caution but not lightly dismiss potential benefits
Beneficial paradox ?
• No evidence for accumulation in healthy
individuals.
But
• The effect of intraoperative lidocaine
administration is sustained beyond its
infusion period and continues into the
post- operative period.
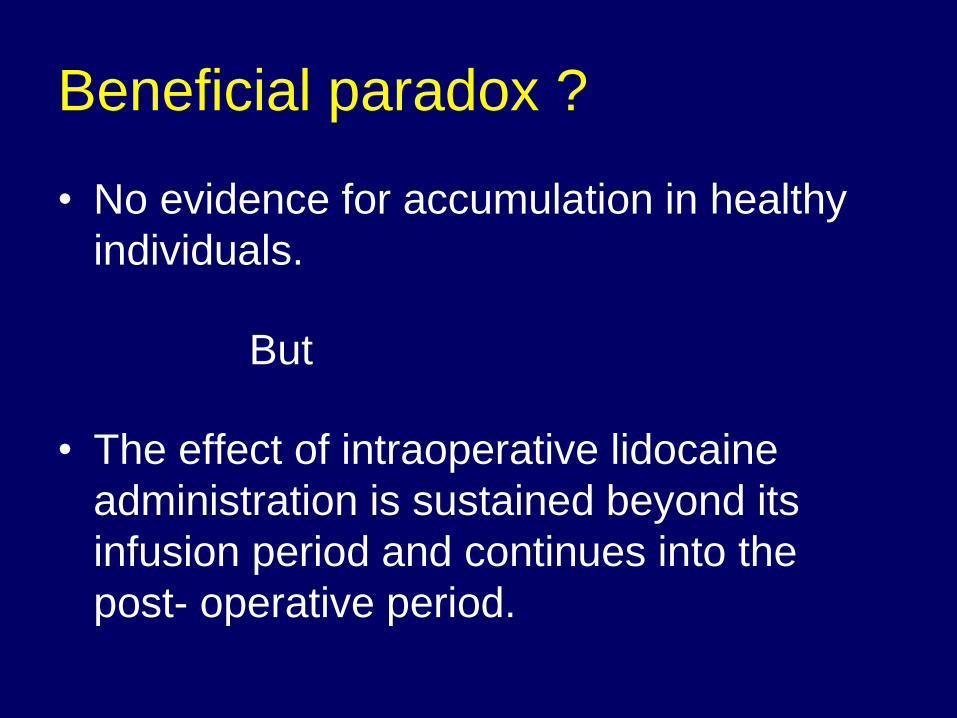
Plasma levels summary
Surgery Regime Levels μg/ml
Groudine SB
Anesth Analg 1998 ; 86
: 235-9.
Open
Prostatectomy
1.5mg/kg bolus
3mg/min
1.3-3.7
Koppert W
Anesth Analg 2004 ; 98
; 1050-5
Major Abdominal 1.5mg/kg bolus
1.5mg/kg/hr
1.9+/-0.7
Kaba A
Anesthesiology 2007 ;
106 : 11-18
Laparoscopic
colectomy
1.5mg/kg bolus
2mg/kg/hr
1.3-4.6
Herroeder S
Ann Surg 2007 ; 246 :
192-200
Colorectal surgery 1.5mg/kg bolus
2mg/min
1.1-4.2
Martin F
Anesthesiology 2008 ;
109 ; 118-123
Hip Arthroplasty 1.5mg/kg bolus
1.5mg/kg/hr
2.1+/-0.4
Bryson GL
Can J Anes 2010 ; 57 :
759-66
Total Abdominal
Hysterectomy
1.5mg/kg bolus
3mg/kg/hr
2.63 SD 0.6

Caution with comorbidities
• Caution if on drugs inhibiting Cyt P450
system eg
Ca Blockers SSRIs
Cimetidine Protease inhibitors
Ciprofloxacin Clarithromycin
Antifungals
Practical implication
Turn down the vapour !
• Bolus 1.5mg/kg
• Infusion 1.5mg/kg/hr
Time to extubation :
14.43 +/- 3.5 min
v
6.73 +/-1.76 min
Nepal Med Coll J 2010; 12 :
215-220

Different intraoperative regimens !
Bolus : Infusion rate :
100mg 2mg/min
1.5mg/kg 3mg/min
1.5mg/kg 2mg/kg/hr
1.5mg/kg 1.5mg/kg/hr
2mg/kg 3mg/kg/hr
- 3mg/kg/hr
100mg 3mg/min
2mg/kg 1.5mg/kg/hr

“The dose of i.v. lidocaine necessary for
analgesia in the peri- operative period is 1–2
mg kg−1 as an initial bolus followed by a
continuous infusion of 0.5–3 mg kg−1 h−1.
The most widely reported and clinically
effective dose range appears to be from 1 to
2 mg kg−1 h−1.”
BJA Education 2016 ; 16 (9) : 292–298

Clinical results
• Several meta analyses and systematic
reviews have been published.
• Many in Surgical journals !
• Most recent systematic review is abridged
version of 2015 Cochrane review :
Weibel S, Jokinen J, Pace NL, Schnabel A et al. Efficacy
and safety of intravenous lidocaine for postoperative
analgesia and recovery after surgery : a systematic review
with trial sequential analysis.
Br J Anaesth 2016 ; 116 : 770-83

2011 Meta Analysis
Can J Anes 2011 ; 58 : 22–37


GI recovery : time to 1st flatus

Cumulative postoperative opioid
consumption

Length of stay

Lidocaine related side effects
• Eighteen of the 21 included trials reported no significant
lidocaine-related adverse events.
• One trial reported cardiac arrhythmia with stable vital
signs in 1 patient receiving lidocaine intervention.
• One study reported mild headache in 10% of patients in
the lidocaine group.
• Another study reported that the incidence of
lightheadedness and dry mouth was significantly higher
in the lidocaine group.

Lidocaine related side effects
• Eighteen of the 21 included trials reported no significant
lidocaine-related adverse events.
• One trial reported cardiac arrhythmia with stable vital
signs in 1 patient receiving lidocaine intervention.
• One study reported mild headache in 10% of patients in
the lidocaine group.
• Another study reported that the incidence of
lightheadedness and dry mouth was significantly higher
in the lidocaine group.

IV Lidocaine infusions Timeline
1960s
• General
Analgesia
1970s
• MI
Arrythmias
1980s
• Chronic Pain
1990s
• Renewed
Interest in
Intraoperative
infusions
2000s 2010s
• Postoperative infusions

Postoperative Lidocaine
infusions • Double blind placebo
controlled RCT
• Open cholecystectomy
• 100mg bolus 30min prior to
incision then 2mg/min IVI
for 24hr versus saline.
• Levels of 1.75 +/- 0.34
μg/ml at 20hrs
• Pain scores and analgesia
requirements reduced
Anesth Analg 1985 ; 64 :971-4

No benefit added to PCA
• Double blind RCT
• Morphine 1mg/ml v
Morphine 1mg/ml +
lidocaine 10 or 20mg/ml
• No difference in pain
scores, opioid use or side
effects
• No benefit from adding
Lidocaine to Morphine
PCA
Anesth Analg 1996 ; 83 :102

APS experience
• Some receive 1-2hrs in PACU.
• Others ( especially chronic pain patients )
receive up to 3 days.
• We require ECG telemetry monitoring,
Ottawa does not.
• APS monitoring as for PCA etc.
• Education of nursing staff important.
• Intralipid on arrest cart.

• Ottawa have most experience in post
operative Lidocaine infusions – since
2009.
• Protocol and brief summary of their
experience and results have been
published.
Eipe N, Gupta S, Penning J. Intravenous lidocaine for
acute pain: an evidence-based clinical update. BJA
Education 2016 ; 16 (9) : 292–298

Comparison with Epidurals
• 1 study found epidural provided best
analgesia but IV Lidocaine better than
PCA Reg Anesth Pain Med 2011; 36 : 241-248
• 1 study found equivalent analgesia in
infusions given for up to 5 days postop. Reg Anesth Pain Med 2010 ; 35 : 370-376

IV Lidocaine for ERAS ?
• Retrospective comparison of epidural and IV
lidocaine analgesia. 108 patients each.
• Matched for age, gender and chronic opioid use.
• Lidocaine infusions intraop were 2-3mg/kg/hr,
reduced to 0.5-1mg/kg/hr postop.
• Most patients also had PCA. Multimodal
analgesia for all.
• Epidural v Lidocaine based on personal
preference.
Reg Anesth Pain Med 2016;41: 28–36

• Retrospective comparison of epidural and IV
lidocaine analgesia. 108 patients each.
• Matched for age, gender and chronic opioid use.
• Lidocaine infusions intraop were 2-3mg/kg/hr,
reduced to 0.5-1mg/kg/hr postop.
• Most patients also had PCA and multimodal
analgesia.
• Epidural v Lidocaine based on personal
preference.
Reg Anesth Pain Med 2016;41: 28–36
Noted clear increase in
Lidocaine usage during period
of study !

IV lidocaine :
• Not inferior to epidural analgesia overall with
respect to pain scores. Inferior 12-24hrs.
• Inferior to epidural analgesia with respect to
opioid consumption.
• Fewer episodes of hypotension and less
postoperative nausea and vomiting, pruritus,
and urinary retention. Earlier 1st GI function.
• Mental status similar.


• Hypotension necessitating changes in analgesic
therapy (either holding or dose adjustment)
occurred in approximately 25% of patients on
POD1 and approximately 10% of patients on
POD2 in the epidural patients.
• Pruritus (probably resulting mainly from
neuraxial opioid) also almost eliminated.
• Nausea and vomiting were reduced by 50%.
• Trend toward earlier discharge by 24hr in
Lidocaine group.

Implications for ERAS protocols
• Most protocols include epidural analgesia.
However, epidural analgesia often results
in increased IV fluids because of
hypotension and decreased mobilization.
• In addition, the rate of failure and
reductions in infusion rates because of
hypotension are problemaric.
• Using IV lidocaine may be an attractive
option.

• Their colorectal ERAS program now uses
subarachnoid morphine before surgery
and IV lidocaine thereafter.
• Results have been very positive, with a 2
day reduction in length of hospitalization
as compared with historical controls (most
of whom received epidural analgesia).

Poor man’s epidural
• Will not mimic all beneficial effects of epidural infusion of LA.
• Nevertheless, may be of benefit in patients who cannot or will not have an epidural
Medical Hypotheses 2004 ; 63 : 386–389

Preventive analgesic effect ?
• Preventive analgesia is defined as a reduction of
post operative pain for more than 5.5 half-lives
of a drug ie approximately 8hrs for lidocaine.
• 13 of 16 studies demonstrated preventive
analgesia by IV administration of lidocaine.
• “IV lidocaine administration may be a
reasonable analgesic approach when regional
techniques are contraindicated or not
performed.”
Anesth Analg 2013 ; 116 : 1141–61
•

Additional potential benefits
• Prevent development of chronic pain Clin J Pain 2012 ; 28 : 567–572
• Attenuate the “stress” response Anesth Analg 1987 ; 66 : 1008-13
• Improve quality of recovery scores Anesth Analg 2012 ; 115 : 262-7
• Improve ability to ambulate British Journal of Anaesthesia 2009 ; 103 : 213–19
• Treat postoperative paralytic ileus Anesth Analg 1990 ; 70 : 414-9.

Which Patients Could Benefit?
• Patients with pre-existing chronic pain
• Patients with pre-existing opioid use
– Chronic pain
– Drug abuse or methadone maintenance
• Patients who have contraindications to or
refuse a regional technique
• Patients in whom a laparoscopic
procedure unexpectedly converts to an
open procedure

• Suggested that extent/magnitude of
surgery determines the success or failure
of IV Lidocaine.
• Thus, Lidocaine more effective for open v
laparoscopic prostatectomy and open v
laparoscopic colectomy.
Anesth Analg 2009 ;109 :1718–9

Cochrane Review – 2 broad
conclusions
“Thus, the effects of a relatively simple
intervention such as the administration of
intravenous lidocaine should be considered
relevant and worthwhile to be discussed with
patients if the site of the surgical procedure
or the expected pain level is appropriate.”
Cochrane Database of Systematic Reviews 2015, Issue 7. Art. No.:
CD009642.DOI: 10.1002/14651858.CD009642.pub2.

“The described effects may be considered
especially relevant if conditions are
prevalent that worsen the risk-to-benefit ratio
of more invasive treatments such as
(thoracic) epidural analgesia or peripheral
regional analgesia techniques."
Cochrane Database of Systematic Reviews 2015, Issue 7. Art. No.:
CD009642.DOI: 10.1002/14651858.CD009642.pub2.

Conclusions
• Despite some concerns re quality of the
evidence, it seems that Intraoperative IV
Lidocaine provides analgesic benefit
especially in the 1st 24hrs.
• Some ( less convincing evidence ) for
other benefits such as reduced LOS.
• Postoperative infusions, on limited
evidence seem to show promising benefit
especially in selected patients.

Final thought : Systemic effects
of Blocks
British Journal of Anaesthesia 2008 ; 101 : 45–7