Embed Size (px)
Citation preview

Intraoral Esthetic Repair of Dental Restorations
R O N A L D E . G O L D S T E I N , D D S " SHANE N . W H I T E , B D F N I S C , MS, MA+
any restorations are M replaced for reasons unre- lated to recurrent disease. Repair of superficial parts of otherwise sound dental restorations is often desirable, both to correct current defects and to prevent future prob- lems. This approach conserves tooth structure, decreases patient suffering, and reduces health care costs. Long-term clinical trials of direct amalgam and composite restorations have shown that up to half of all unsatisfactory restora- tions have been replaced due to fracture, wear, unsatisfactory con- tour or anatomic form, marginal discrepancies, staining, open con- tacts, o r color mismatch.'-' Porcelain fracture and marginal discrepancies are common causes of early failure of crowns and fixed partial dentures.'-"' This article reviews current repair techniques and suggests appropriate clinical pro roco 1 s .
I S 0 I. A l ' I 0 N
Rubber dam isolation is strongly recommended, whenever possible, for adhesive procedures. Isolation can prevent salivary contamination,
allow moisture control, protect soft tissues from acids, prevent inhala- tion of airborne abrasives, and retract soft tissues. Moreover, a uniform-colored background facili- tates achieving the chosen shade.
R E I ' A I K M E T H O D S
Many intraoral methods have been used to prepare the surfaces of restorations for adhesive bonding. These methods can be divided into two groups. The first group of techniques roughens restoration surfaces to create micromechanical retention. Methods include roughening with a diamond bur, sandblasting, high-energy a brasion, etching with strong acids, and tin plating. The second group of tech- niques promotes adhesion of restorative composites to the roughened surfaces. These include silane coating and treating with multipurpose adhesives. The best results are obtained using a combi- nation of techniques. Predictable results can now be achieved in a single routine office visit.
Roughening with Diamond Burs A diamond bur can be used to roughen most restorative surfaces, but this method is not as effective as other techniques and should not be relied on."-" Burs can also be used to create macromechanical retentive undercuts, but excessive removal of tooth structure or restoration should be avoided. Surface preparation using multi- fluted carbide finishing burs or smooth finishing diamond burs should be avoided.
Sandblasting Sandblasting can improve retention to fractured porcelain, exposed cast metal, or composite sur- faces*lz,".1' Lh This not only creates micromechanical roughening, but also produces compositional changes and increases surface energy, thus increasing wetability by adhesives." Small intraoral sandblasters are now available (Micro Etcher, Danville Engineering, Danville, CA). Optimal effects are obtained using large (50 to 100 pm) alumina particles at high pressures (80 to 100 psi). The sandblaster should
,-Chicid Professor of Oral Kehahl~i tat lo~, Schooi of Dentistry, Medical Cidlege of Georgia. Adjunct Clinical Professor of I'rosthodontrcs a t Boston University, Visiting Professor of Oral and Maxillofacial Imaging and Continuing Education at t h University of Southern California School o f Dentistry, 1.0s Angeles, Californra, Adjunct Professor of Restoratnw Dentistry ut The University of Texas Health Science Center at Sun Antonio, 'Texas, and Private Practice, Atlanta, Georgiu .Assistant Professor and Director ~f Clinical Research, Department of Restorative DentistrylSiomaterials, School o f Dentistry, University of Southern Califimria, Los Angeles, California v o i 11h41- 7 . N I I Z ~ R ~ K i 219

hit raoral Esthetic Repair of Dcrital Restorations
Figure I . A scanning electron micrograph (X2000 original magnification) of a hybrid composite (Herculite XRV, Kerr) that has been treated using high-energy abrasion (KCP 2000, American Dental Technology). Exposure of individual filler particles has created an extremely retentive surface.
be attached to the main air supply line before it is down regulated to approximately 40 psi for hand- pieces. Since the patient’s eyes and airway must be protected, rubber dam isolation and protective gog- gles are recommended.
differs from conventional air abra- sion in several ways.Lx.” Higher pressures and smaller nozzles are used to increase particle velocity and energy. The equipment also has con- sidera ble reserve volume to ensure that pressure does not drop during use. For most restorative materials, that the best results are obtained by using 50 pm alumina abrasive a t the medium setting.’’ Optimal results are obtained when the tip of the nozzle is held a t an angle several millimeters back from the surface. It is recommended that both patients and clinicians wear protective eye- wear. Clinicians should wear masks and patients’ airways should be iso- lated by rubber dam.’l High-volume evacuation should be used for removal of abrasive and saliva, but the system’s own integral high-
High-Energy Air Abrasion Recently, a surface preparation method using high-energy a brasion has become available (American Dental Technology, Troy, MI, Sunrise Technologies, Freemont, CA, Kreativ Inc., Albany, OR).’* This technique enhances adhesion to a very wide variety of restorative materials (Figures 1 and 21, as well as to enamel and The high-energy air abrasion technique Figure 2. A scanning electron micrograph ( X l 000 original magnification)
of a stainless steel surface that has been treated using high-energy abrasion ( K C P 2000). Despite the soft and tough nature of stainless steel, micromechanical retention has been created.

volume evacuation system should be used primarily for dry, airborne abrasive. The abrasive need only be directed at the target area for very short periods, and a uniform change in surface texture is sufficient. Prolonged application times are unnecessary and will remove too much restorative material. This system is very quick and easy to use.
Etching Thirty-seven percent phosphoric acid is used to etch enamel adja- cent to repairs. Weaker acid solutions (e.g., 10% phosphoric acid or 2.5% nitric acid) can be used to condition adjacent dentin prior to bonding; that is, to open up tubules and remove the smear layer and other debris.
Several acids can be used to etch porcelain. They act by differentially dissolving porcelain components to create micromechanical undercuts. Hydrofluoric acid, usually used at 8% to 10% concentrations for 2 to 4 minutes, is highly effective.”-’4.”-” However, it is also extremely dangerous and must be used with careful isolation and great caution. A weaker 2.5% solution of hydro- fluoric acid, which may be less dangerous, is also effective (Porcelock, Den-Mat, Santa Maria, CA).” Acidulated phosphated fluo- ride, applied in the form of a 1.2% fluoride gel for an extended time, ha only limited ability to etch porcelain. IL,14,1 i 3 3 Phosphoric acid enamel etchant can be used to clean
.S
exposed porcelain surfaces and make them more receptive to silane. However, phosphoric acid has no etching effect on porcelain. Acid etching is the most important step in feldspathic porcelain re~air , ’~,’~.~’ but it is much less effective on stronger, highly crystalline ceramics such as In-Ceram (Vita Zahnfabrik, Bad Sackingen, Germany), Empress (Ivoclar-Vivadent, Amherst, NY) or Dicor (Dentsply York Division, York, PA).24,25 Sandblasting or high- energy abrasion is the primary method of roughening high-strength ceramic^.^^^^' It may be prudent to replace damaged high-strength all- ceramic restorations, rather than to attempt major repairs.
Sandblasting prior to etching increases surface roughness and allows the etchant to penetrate deeper into the surface defects on all porcelains and ceramic materials.”~l‘~Zh
Some acids may be used to etch the glassy filler in composites, but they may not be very effective in improving bond strength and may stain or damage some conipos- ites.lx,’y As well as attacking the filler, acids tend to damage the polymeric matrix and the interface between filler and matrix.
When several different acids are to be used to treat different adjacent materials, the strongest one should be used first (e.g., 10% hydrofluo- ric acid on porcelain), followed by
the intermediate acid (e.g., 37% phosphoric acid on enamel), and finally the weakest acid (e.g. 2.5% nitric or 10% phosphoric acid on dentin). The repair should be thor- oughly washed using airlwater spray for at least 10 seconds after each acid application.
Tin Plating Intraoral tin plating may be used to coat precious metals with a layer of sharp retentive tin oxide crystals.’L~L‘l This may be preferred to conventional sandblasting alone, which is less effective on precious metals. However, high-energy abrasion is effective on precious or homogeneous metals such as Type 111 gold and titanium.” Tin plating may stain adjacent tooth-colored materials. Sandblasting prior to tin plating is recommended. ” Several small tin platers suitable for intra- oral use are commercially available (Micro Tin, Danville Engineering; Kerr, Glendora, CA).
Silane Organosilane coupling agents have the ability to form covalent bonds with siliceous glassy composite filler and with resinous polymer^.'".^" These bonds are stable, but may be slow to form. Tests on the enhance- ment of repairs by silane coupling agents have produced conflicting and often disappointing
This may be due to the susceptibility of organosilanes to hydrolysis by moisture and to their slow reaction
results. I I . l l , lh . lY. lh .~h.?Y4 I
hit raoral Esthetic Repair of De I I t a1 Rcs t o r*ations
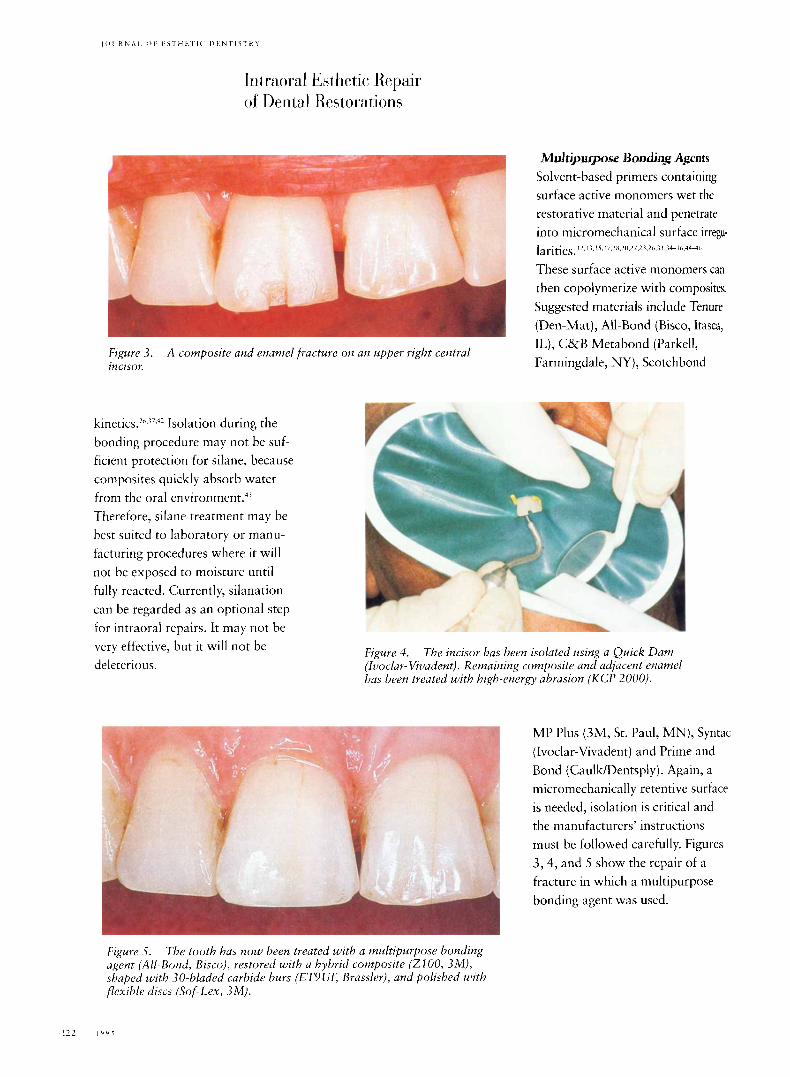
Figure 3 . incisor.
A composite and enamel fracture on an upper right central
kineticS.Lf,.17.42 Isolation during the bonding procedure may not be suf- ficient protection for silane, because composites quickly absorb water from the oral en~ironment .~ ' Therefore, silane treatment may be best suited to laboratory or manu- facturing procedures where it will not he exposed to moisture until fully reacted. Currently, silanation can be regarded as an optional step for intraoral repairs. It may not be very effective, but it will not be deleterious.
Mdu$urgo~w Boadaag Agents Solvent-based primers containing surface active monomers wet the restorative material and penetrate into micromechanical surface irregk larities. I2.i 1.1 ~.I;.IX,LII,LI.L1.L6,1I,14~;~,,444h
These surface active monomers can then copolymerize with composites. Suggested materials include Tenure (Den-Mat), All-Bond (Bisco, Itasca, IL), C&B Metabond (Parkell, Farmingdale, NY), Scotchbond
Figure 4. (Ivoclar- Vivadent). Remaining composite and adjacent enamel has been treated with high-energy abrasion (KCP 2000).
The incisor has been isolated using a Quick Dam
MP Plus (3M, St. Paul, MN), Syntac (Ivoclar-Vivadent) and Prime and Bond (Caulk/Dentsply). Again, a micromechanically retentive surface is needed, isolation is critical and the manufacturers' instructions must be followed carefully. Figures 3,4, and 5 show the repair of a fracture in which a multipurpose bonding agent was used.
Figure S. The tooth has now been treated with a multipurpose bonding agent (All-Bond, Bisco), restored with a hybrid composite (2 100, 3M), shaped with 30-hladed carbide burs (ET9UF, Brassler), and polished with flexible discs (Sof-Lex, 3M).
' 2 2 I Y Y ~

C L F A N I N G A N 1) L j E L R E A S I N G
Clean, dry surfaces are essential for adhesion. Sandblasting, high- energy abrasion and acid etching will all remove superficial debris and salivary contaminants. However, it is also essential that acid gels and abrasive particles be completely washed off conditioned surfaces. Oil from lubricated hand- pieces or compressors can be removed by carefully cleaning with acetone or a commercial degreas- inddrying agent such as Dry-Bond (Den-Mat).
Figure 6. of a porcelain laminate.
A traumatic porcelain fracture on the incisal edge
(: o M I' o s I T E P L A <: t:, M E N 'i-
Several types of composite may be used for different repairs. Hybrid composites should be used if resistance to occlusal stresses is necessary, such as for incisal angles (Figures 6, 7, and 8). Suggested hybrid materials include Herculite XRV (Kerr, Glendora, CA), Prisma TPH (Caulk/Dentsply), ZlOO (3M) and Aelitefil (Bisco). Figure 7.
high-energy abrasion for several seconds. Porcelain and adjacent enamel are treated by
Microfilled materials should be used when optimal esthetics and polishability are needed but stress resistance is less important (e.g., gingival fractures). Microfills can be used to veneer hybrids or fractured porcelain. Suggested microfills include Durafil (Heraeus Kulzer, Irvine, CA), Silux Plus (3M), Perfection (Den-Mat) or Rename1 (Cosmedent, Chicago, IL).
Figure 8. acid, and the enamel etched with 37% phosphoric acid. A multipurpose bonding agent (Tenure, Den-Mat), and a hybrid composite (Prisma TPH, CaulklDentsply) completed the repair.
The porcelain was etched with 10% hydrofluoric

l r r l moral kktlietic Repair of Derital Restorations
Fluoride-releasing materials, or resin-modified glass ionomers, can be used when the patient is at risk for caries. These materials are gen- erally weaker, less wear-resistant, less polishable, and less dimension- ally stable than conventional composites. However, they possess sustained fluoride release, accept- able esthetics, and acceptable adhesive properties. Suggested resin-modified glass ionomers include Fuji I1 LC (GC America, Chicago, IL), Vitremer (3M), Dyract (Caulk/Dentsply), Geristore (Den-Mat) and Photac-Fill (ESPE Premier, Norristown, PA).
Opaque composites may be used to hide exposed metal. Some resinous materials such as Panavia (J Morita, Tustin, CA), Geristore (Den-Mat) or Resinomer (Bisco) are adhesive on their own, but can be enhanced by a multipurpose bonding agent.” Layers of trans- lucent composite should be added and cured incrementally, allowing internal characterization and avoiding excessive polymerization shrinkage. If possible, polymeri- zation should be initiated by directing the curing light through the tooth, rather than from the external surface, thus initiating curing at the tooth/composite interface and allowing some stress relaxation during polymerization. The composite must be protected from moisture until fully cured. After complete curing, the compos- ite can be recontoured using fine diamonds or inultifluted carbide
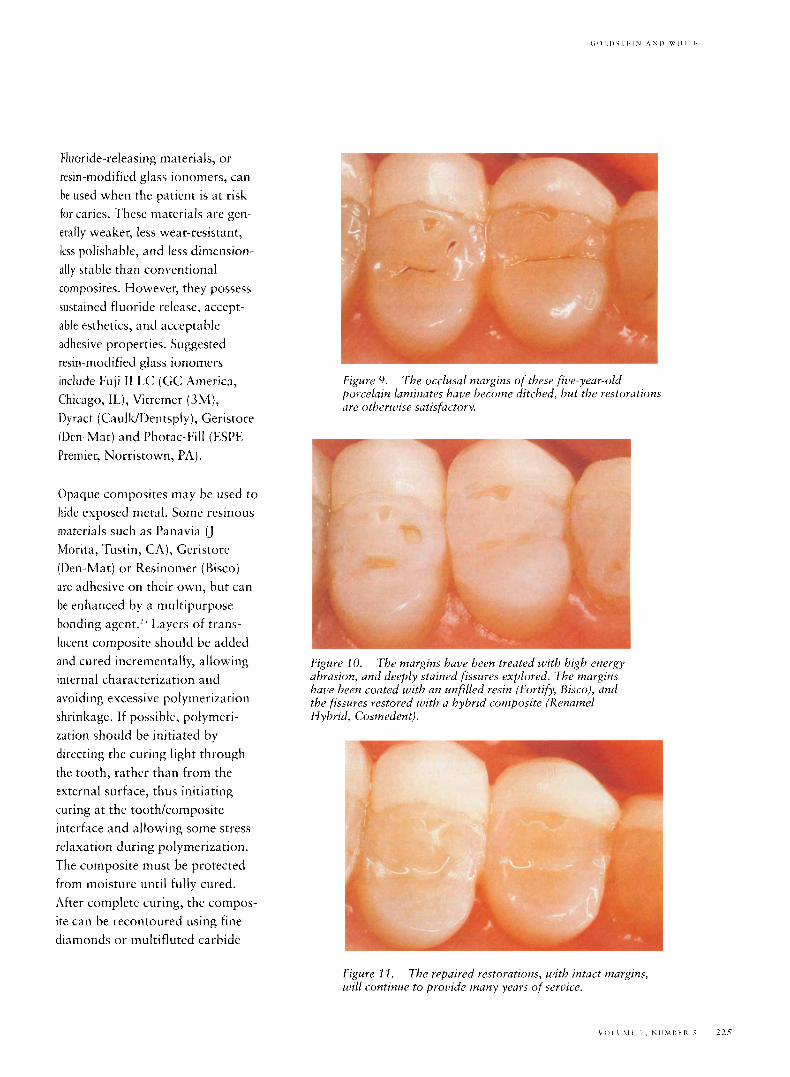
Figure 9. porcelain laminates have become ditched, hut the restorations are otherwise satisfactory.
T h e occlusal margins of these five-year-old
Figure 10. abrasion, and deeply stained fissures explored. The margins have been coated with a n unfilled resin (Fortify, Bisco), and the fissures restored with a hybrid composite (Rename1 Hybrid, Cosmedent).
T h e margins have been treated with high-energy
Figure 2 I . will continue to provide many years of serrtice.
The repaired restorations, with intact margins,

finishing burs (ET, Brassler, Savannah, GA) and polished using abrasive discs (Soflex, 3M; Flexidiscs, Cosmedent; and Super- Snap, Shofu, Menlo Park, CA) or very fine diamond polishing paste. Recuring the composite after fin- ishing may improve its physical properties.
D I $ ( U I S I O N
Table 1 gives suggested protocols for repair of various materials. These repair procedures were suggested by consideration of the scientific literature and by clinical experience. Other opinions and procedures may be valid. New information, materials, or tech- nologies may influence future protocols. In all cases, a combina- tion of techniques provides the best results. Since many adhesive tech- niques are operator-sensitive, the simplest effective protocol should be chosen.
These adhesive techniques may be applied in many imaginative ways to solve many different problems; for example, a porcelain veneer could be bonded to a bridge pontic that had lost its porcelain facing. New types of restorations will demand novel solutions to brand- new problems.
Repair techniques vary widely in their ability to produce durable bonds to different materials. For example, bond strengths to porce- lain may be so strong as to exceed their cohesive strength, but bonds
to repaired amalgam are usually weak. Therefore, if possible, con- ventional retention and resistance form should be used to augment the adhesive repair. Each clinical repair should be evaluated sepa- rately. Figures 9, 10, and l l show a combination approach taken to porcelain laminates with ditched margins.
Little long-term clinical data exists on the performance of repaired restorations. We should advise our patients with caution, because many lab studies have shown that bond strength decreases after stor- age, artificial aging, or fatig~e.'",'~." (However, one clinical study of repaired amalgams has achieved a loo%, 1-year success rate.46) Our patients must be fully informed as to the risks of failure. We cannot yet give our patients any estimates of repair longevity. We must also stress the importance of continued follow-up and maintenance therapy. This will allow early diagnosis of problems and may lead to less invasive interceptive treatments.
When making treatment decisions, we must evaluate the consequences of possible future failure of the repair. These may often be less seri- ous than the potential consequences of failure of a com- pletely new replacement restoration. However, we must be careful to fully diagnose any restoration-related disease, such as deep caries or periodontal disease, before opting for repair instead of replacement.
If a damaged restoration can be removed from the mouth, many more adhesive repair techniques are possible. Such restorations could be cleaned using ultrasonic or steam cleaning. Additional tech- niques include silane coating, silica coating (Silicoater, Hereaus Kulzer and Rocatec, ESPE Premier), oxidization, electrolytic etching, and plasma spraying. Composite repairs could be post-cured using heat, pressure, and more intense light sources.
C: 0 N C 1. U S I 0 N S
Preventive repair of existing restorations has the potential to conserve tooth structure, reduce patient suffering, and decrease treatment costs. Many new tech- niques for intraoral repairs are now available. Lack of clinical data limits our ability to predict the long-term performance of repairs.
R F F E R E N <: E S Moffa J P . Comparative pcrformunce of amalgam and composite resin restorrrtions und criteria f o r their use. In: A I ~ L I S ~ U I C ~ KJ, ed. Quality evaluation of drntal restoratto~is. Criteria ~ I ) Y
placemc~iit arid replacement. !'roc-uetiings o f the Internafiowal Sympr,sit4m ou Criteria for I'lirceme~it atid Replaremertt of Dental Restorations. Chic-i7go: Quintessence. 1989.
I.einfeldcr Kb. Criteria for c-linic-ul evaluation of composite resin restorations. In: Anusavice K ) , en. Quality evaluation of dentnl restorutioizs. (:riteria for placement and repliicrment. 1'roreediizgs of the liiterriatioitul Symposium on Criteria for Pl~cement and Replacement of !>ento/ Restorations. Chicago: Quintessence, 1989.
Qvist 1( Qvist J, M j o r IA. I'luceriierrt unil longevity of tooth-colored restordtions t i1
Iletinznrk. Acta Odontol Scaiid 1990:48:.10.7-3 1 I .
2 2 6 I Y Y ~

4. York AK, Arthur JS. Reasons for plurenient and replacement of derital restorations i i i the United Stutes Navy Ilentul ( ;orps . Oper /)elit 1993;18:201-208.
Smules RJ, Wchster L)A. Restoration deteriorutiiiii related t o later failure. Oper /lent l99.3:IS:l 10-1.37.
Sclituartz NK, Whitset l.D, Berry TC;, Stewart 11,. Unseruiceahle crowns and /?xed partial dentures: lifespan iirid CUUSM for l oss ofserviceubility. J A m Dent
!.
6.
ASSCIC 1 Y84;81: 1 19.Y- 1401.
7. (~‘lrntz Pj Ryge G, Jeiidrescn MD, Niliier K . Quality o f extensive fixed prostheses after fiue yeurs. J Prosthet Dent 1984; 12:475-479.
8. Marynink G A , Kaplan S W. Longevity of restomtiom: Siiruey results of dentists’ estimates and attitudes. J A m Dent Assoc 19X6:I 12:39-4.5.
9. Walton ,IN, C‘ardiier FM, Agar lR . A survey of crown und fixed partial denture fizilures: length of seruil-e and reasons for replucement. .I Prostbet Dent 19X6:.16:4 16-42 1 .
10. Morris HF. C:/inical performance of metal ceramic restorations: A i-yrur progress report. In: Annsauice KJ, ed. Quality evalnatiow o f dental restoratims. Criteria fiir plu~-cnieirt mzd repl~cenzeirt. Proreedings o f the liitrrriutionnl Synrposrum o t i Criteria for Placement and Replacement of /)entul Kestorutions. Chicugo:C_)tcintessence, 1 989.
1 1 . I.acy AM, l .al .uzJ, Watanahe 1.G. Dellinges M . Effect of porcelain surface treritnteiit 0 1 1 the h i i d to ciiniposite. Prostbet Dent 19XX;hO:ZXX-Z9I.
f2 . Ilertolotti I</ . , f.acy AM, Wiztand~e 1.G. Arihesiiv inoriomers f o r porce1ain repair. lnt J Prosthodoizt 1989:2:48 3-JS9.
1 3. Wolf DM, I’owers J M , O’Keefe Kl.. Bond strength of composite t o porcelain tseuted with new porcelaiii sepuis agents. Dent Muter 1992;8:1 58-161.
14. knn 1’1.. Americuii Drntul Assoriution Council on l h i t a l Materials. Porcelain repair materials. J Am Dent ASSOL. I 99 I : 122: 124-1.30.
1 $. ,Suliniati A A , Swift EJ, Perdigo 1. Effects of surface treatment and hondirig agents on howd strength of composite resin to porcelain. / I’rosthet Ilerit 199 3:70:178-/20.
16. Wood I l P , Jordan RE, Way DC;, Galil KA. Monding to porcehin and gold. A m / Orthod 1986;89:1 94-20.5.
17. Teiipma \.T, Nicholls / I , Toiunsend/T, Hurper R]. Chemical retention o f composite resin to metal. lilt I’rosthodont 1 990;.1:78-88.
I S . Swift EJ, LeValley BI) , Boyer DB. Evahatrnn of new methods for composite repazr. Dent Mater 1992;8:362-36.~.
19. Stokes A N , Tay W M , I’ereira KP. Shear bond of resin cement t o post-cured hybrid composites. Deizt Mater I 9 9.3;9:3 70-3 74.
plutiiig-surface treatmeitts to improue bonding with resin cements. Dent Update
20. McCaughy AD. Sandhlastrizg and tin
1 9V?;2O:153-1.$7.
21. Ewner CM! Meiers JC. Repair ofan aged, contaminated indirect composite resin with a direct, visible-light-cured composite resin. Oper Dent 1 993;I 8:187-194.
22. Chang /C, Powers J M , Hart D. Bond strength of composite to alloy treated with bonding systems. J Prosthodoizt 1993;2:110-114.
23. Berry EA, Powers , [M. Bond strength of adhesrue composites to dental substrates. J Prosthodont 1994;.3:126-129.
24. Russell DA, Meiers JC. Shear bond strength of resin composite to Ilicor treated with 4-META. Int J Prosthodont 1994;7:7-12.
25. Kern M , Thompson VI? Sandhlasting and silica coating of a glass-infiltrated alumina ceramic: volume loss. morphology, and changes in the surface composition. J Prosthet Dent 1994;71:4.53-461.
26. Murchack 13, Yn Z, Zhao X Y , Whrte SN. Adhesion o f denture base resin to denture tooth porcelain. J Prosthet Dent 1995; 74:242-249.
27. Tiller I I-J, ( ; o h e l K , Miipirus I $ + ( 7 1 01. I > v r sandstrahlprozcss nnd seine cinwirkung auf den oherflachenmstand yon
28. Goldstein R E , Parkins F M . Air-abrasive technology: its new role in restorative dentistry. J A m Dent Assoc I W4;12 5:; j1-.557.
29. Laurel1 K, Lord W, Beck M . Kineti<. cavity preparation effects on bonding to enamel and dentin. J Dent Kes f 993:72:27I (Abstr 1437).
30, Keen DS, uon Fraunhofer / A , Parkiris F M . Air-abrasive “etching”: composite bond strengths. ,I Dent Res 1994;7?:1 I1 (A hstr 2.3 8).
32. White SN, Yu Z , Zhao X Y . High-energy abrasion: a n innovative esthetic modality to enhance adhesion. / Esthet Dent I 9 94; 6:2 6 7-2 7 3 .
32. Kerr D A , Ramfiord S, Ramfiord GM. Effect o f inhalation of airbrasive powder. ,I Dent Res 1954;3.3:666 (Ahstr .SS).
3 I. A1 Edris A , Aljribr A , C~oiilcy R I,. Karghi N . S E M cunluutioii of rtc-13 patterns by three etchants on three porrcluins. J I’rosthet Dciit I990;64:7 14-73‘).
34. Llobel A, Nichols//, Kois .I<:. 1)izly ( ; H . Fatigue life of porcelaiu repair systems. f n t J Prosthodont 1992; S:ZO.C-2 1.3.
3.Y. Williamson KT, Mitchell RJ, Breeding I.C. The effect of fiitigne oii thP shear bond strength of resin bonded to porcelain. J I’rostbod 199.3;2:1 1 ( - 1 19.
36. Stangd I , Nuthanson I ) , Hsu strength of the conzposite bi)nd to etched porcelahi. J Dent Res 19S7;66:1460-146.5.
.37. Sorenscx /A, Knglemun M/, Torres T / . Auera SI? Sheur bond strength o/ composite resin to porceluni. Irit J I’rosthodont 1991;4:17-2 3 .
3 8 . Aihers H E Metul-resin hoiidirzg. Adept Report I99 1 :2:2 7-40.
39 . Wowen RL. I h i t u l filliiig niuteriul comprising uinyl-silarie-treated fused silica and a hiitiler consistiiig of the
glycidyl acrylatc. U S I’utent 3,066, I 12, November 27, 1962.
reL7cti(Jll prOlflict Of / J l S - f ) h E l l O ~ ‘71ld
40. llailey JH. Por~-elriiiz-to-coniposite bond strengths using four organosilaiie materials. J Prosthet Dent 1989;61:174-177.
41. Eanzes WB, Rogers LK, Feller PK, Price WR. Bonding agents for repairiiig porcelain and gold: Air eualuatioii. Oper Dent 1977;2:1 IS-124.
42. Steus A , Picard 11, Ogoli i ik R. Adhesioii of artificial teeth to ~ii~lymethncryliitp riwns. I<r ,v ) ~ i o i i t ( ~ ~ 1 ( ~ ~ 1 7 ~ 1 1 ~ ~ / I’arrs.
I w o : I u:(? 1417.
4 3 . Hunsen E K . Asniussen b:. Conipiiratiue study of dentiii udhcsives. Scrznd / Dent Res 1 98S;V.1:280-287.
44. Styner D , Scherer W, Iml’resti /, Penngondu B . Bonding c-omposite to giuss iononicr with adhesive rcsin cements. / Esthet Dent 1992:4:1 3-1 .5 .
4.:. Hasegawa T Retief I ~ H . Russel CM, Denys FR. A luboriztory stl4dy of thr umalgam-bond udhesiiie systeni. Am / L)c/it 1992:.F:161-186.
46. Ualanku M . Bonded silucr amu/gani restorations. / Esthet Deut 1992;4:.14-.57.
Reprint requests: Shone N. White, RlliwtSc, MS, MA, Pincus Biomatrriuls Research I.ub, University of Suutherri Culifortiiii School of Dentistry # 41 12, 1,os Angeles, CA 90089-0641 0 199.5 Derker Periodicals





























