Embed Size (px)
Citation preview
400
DiscussionIn our series of nephrotic patients followed up for
six years the complications due to atheroma are veryfrequent-coronary atheroma with resultant angina ofeffort and myocardial infarction, intermittent claudi-cation, and abdominal angina. Unfortunately this hasnot been mentioned as a complication of N.s. in any ofthe standard textbooks on renal disease, except onewritten by one of us.1 This is possibly due to theattribution of the atheromatous changes to hyper-tension, which is common in N.s. In our series,however, hypertension was absent in 3 of the 4 patientswho later developed myocardial infarction, so it can beconfidently excluded as a major factor. The serum-cholesterol is often raised in N.s., and this elevation is
accompanied by high levels of plasma-lipids.5 Disordersof lipid metabolism similar to, but not identical with,this are also found in diseases long associated with anincreased risk of the development of atheroma, suchas diabetes mellitus, 6 familial hyperlipaemia, and
myxœdema.’ N.S. with high levels of plasma-lipidscauses similar atheroma if it persists long enough. Themean duration of observed nephrotic syndrome in ourseries was 3-5 years, in which there was prolongedhyperlipxmia
In the treatment of N.s. a major aim should be torestore the plasma-lipid pattern to normal beforeatheroma has developed. In the present series the
coronary arteries were affected by atheroma withresultant myocardial infarction in 4 and angina of effortin 1. In 2 further patients, not included in this report,severe intermittent claudication occurred, indicatingatheromatous involvement of the limb arteries. Plasma-
lipid abnormalities are best controlled by completeremission of N.s., but this is frequently difficult orimpossible to achieve on steroid therapy alone inmembranous glomerulonephritis and proliferativeglomerulonephritis. We believe that, because of thedangers of hyperlipxmia, it is essential to use not
only steroids but also immunosuppressive agents suchas cyclophosphamide and azathioprine which, despitetheir side-effects, are considerably less dangerous thanpermitting hyperlipæmia to persist. Unfortunatelymany patients have disease which resists all presentforms of treatment; in these patients clofibrate hasbeen used to lower serum-lipid levels.8 8
In our series ischasmic heart-disease has been thesecond most common cause of death in N.S., thecommonest being ursemia. The frequency of myo-cardial infarction in N.S. should be borne in mind in thedifferential diagnosis of obscure chest pain in youngnephrotic patients.We are indebted to Prof. D. A. K. Black for advice and for
allowing us to study his patients.Requests for reprints should be addressed to G. M. B.,
Department of Nephrology, Central Negev Hospital, Beer Sheva,Israel.
REFERENCES1. Berlyne, G. M. A Course in Renal Disease. Oxford, 1966.2. Varley, H. S. Practical Clinical Biochemistry; p.232. London, 1964.3. Registrar General’s Annual Statistical Review of England and Wales.
H.M. Stationery Office, 1966.4. Jolliffe, N., Rinzler, S. H., Archer, M. Archs intern. Med. 1962,
109, 566.5. Baxter, J. H. ibid. p. 742.6. Stearns, S., Schlesinger, M. J., Rudy, A. ibid. 1947, 80, 463.7. Friedberg, C. K. Diseases of Heart; p. 425. London, 1956.8. Mallick, N. P., Berlyne, G. M. Int. Congr. Nephrol., Stockholm,
1969.
INTRALUMINAL BILE-SALT DEFICIENCY
IN THE PATHOGENESIS OF
STEATORRHŒA
B. W. D. BADLEY* G. M. MURPHY
I. A. D. BOUCHIERMedical Unit, Royal Free Hospital, London W.C.1
*Present address: Faculty of Medicine, Dalhousie University,Halifax, N.S., Canada.
Summary The lipid-solvent properties of intes-tinal contents with normal and sub-
normal bile-salt concentrations were investigated. Ateach of the bile-salt concentrations studied (3.5, 5.5,and 11.5 mmoles per litre) micellar solutions were
formed; but at 3.5 mmoles per litre (subnormalconcentration) only a small amount of lipid was
incorporated into the micellar phase. It is suggestedthat the formation of a micellar lipid solution alone isinsufficient to ensure normal fat absorption. Theconcentration of conjugated bile-salts must exceed4 mmoles per litre in order to provide the number ofmicelles necessary to dissolve the hydrolytic products ofa normal dietary lipid load. Failure to achieve this" critical physiological concentration" of bile-saltswill, despite achievement of the critical micellarconcentration (C.M.C.), result in steatorrhœa.
Introduction
DURING normal fat-absorption the products of
dietary-triglyceride hydrolysis are incorporated into amicellar solution.1 This process depends on thepresence of conjugated bile-salts within the intestinallumen in a concentration above a critical level-thecritical micellar concentration (C.M.C.).2 The c.M.c. ofany given bile-salt is variable: it depends on factorssuch as temperature, pH of the medium, and thepresence of other ions and polar lipids in solution.The c.M.c. of a physiological mixture of bile-salts,under conditions closely simulating those in theintestinal lumen, is 1-2 mmoles per litre. 3 Thusformation of a micellar solution requires an intra-luminal bile-salt concentration of at least this level.
Normally this requirement is easily met: the mean bile-salt concentration in the small-bowel lumen during thedigestion and absorption of a fat-containing meal is
approximately 10 mmoles per litre, with a lower limitof 4-5 mmoles per litre.4
5
In several- different clinical states, including the
syndrome of extensive ileal disease or resection,6-9 thestagnant-loop syndrome,10-12 the Zollinger Ellison
syndrome,13 and chronic liver disease,14 15 subnormalconcentrations of intraluminal conjugated bile-salts arefound in association with steatorrhoea. In this studywe attempted to explain why some of these patientshave steatorrhoea even though their intraluminal bile-salt levels exceed the c.M.c.
Methods
A fat-free formula meal, consisting of 50 g. glucose, 25 g.milk-protein powder, and 300 g. water, was given to anormal volunteer and to a patient with active chronic
hepatitis who excreted 15-20 g. of fat in 24 hours and wasknown to have subnormal intraluminal bile-salt concentra-tions. Samples of proximal-jejunal contents were obtainedfrom both.

401
The lipase in the aspirate was inactivated by heat. Eachpooled collection was well mixed and divided into severalaliquots of equal volume. Increasing amounts of a lipidmixture were added to each series of aliquots, to producetotal-lipid concentrations ranging from normal to well abovethose usually found after a standard fat-containing meal.The lipid mixture-corn oil 20%, mono-olein 25%, oleicacid 55%-contained both polar and nonpolar lipids inproportions similar to those found in the lumen of the smallintestine after a fat-containing meal. Normal values for
total-lipid concentrations had been established previously byanalysis of 61 jejunal aspirates obtained after ingestion of astandard formula meal containing 30 g. corn oil. Thenormal range, taken as 1 standard deviation (s.D.) above andbelow the mean total-lipid content of the samples, was6-46±6-14 mg. per ml. of intestinal contents.15 Afteraddition of the lipid mixture, each aliquot was agitated in awater bath at 37°C for 1 hour. Samples of " total phase "were obtained immediately after mixing on a ’Vortex’
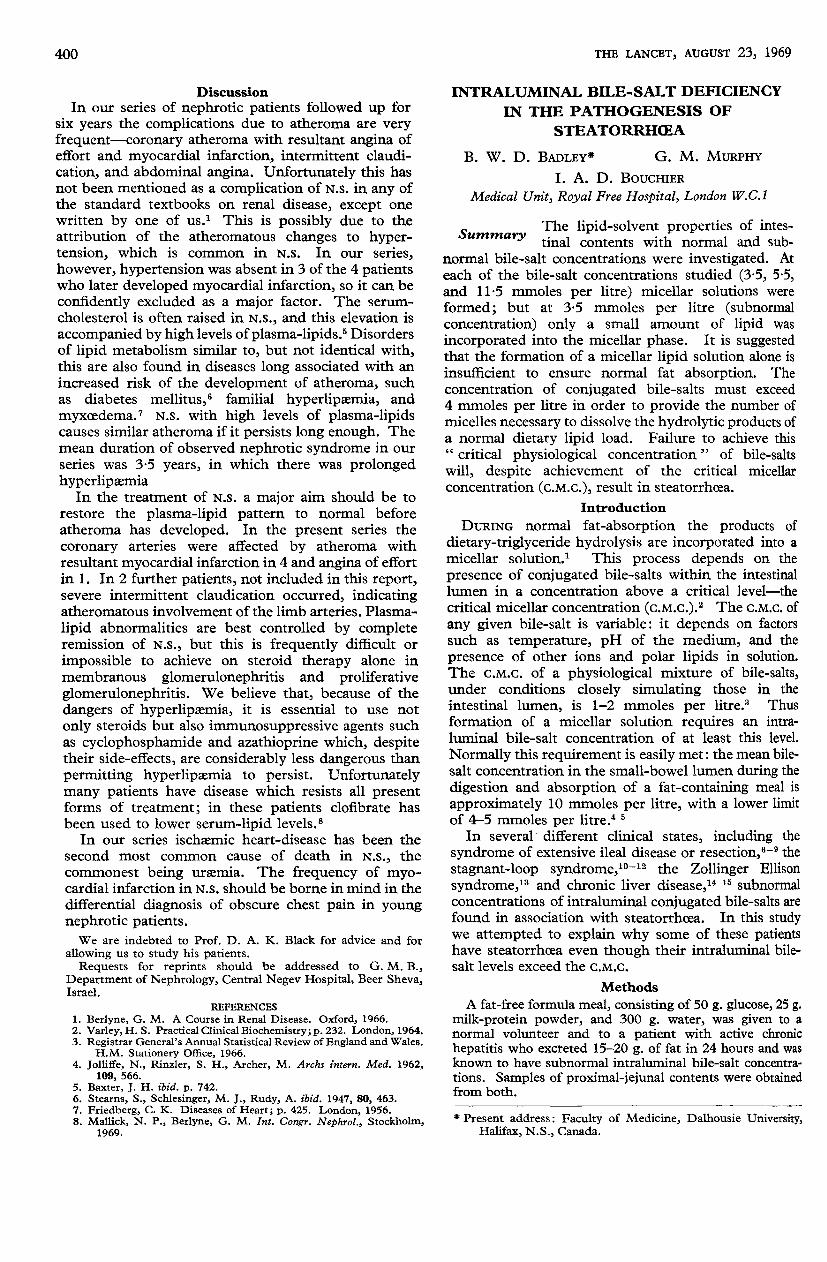
Fig. 1-Lipid-solvent properties of intestinal contents with fixedtotal bile-salt concentration.
Figures on the curves represent the total bile-salt concentrationof each series of aliquots. The shaded area denotes the mean± 1 S.D. of the level of total lipid in 61 jejunal aspirates obtainedafter a standard meal containing 30 g. fat.115
mixer. " Micellar phase " was separated by centrifugationat 100,000 g for 3 hours at a temperature of 35-40°C. Thelipid content in both phases of each sample was determinedgravimetrically,9 and the total bile-salt concentration wasmeasured by a modification of the hydroxy-steroid-dehydrogenase method of Iwata and Yamasaki.16
Results
The total bile-salt concentrations of two pooledcollections from the normal subject (11.5 and 5-5mmoles per litre) were within the normal range. Thespecimen from the patient with steatorrhoea had a bile-salt content of 3-5 mmoles per litre. This was belowthe normal range but above the c.M.c. of a mixture ofconjugated bile salts. In samples with both normal andsubnormal bile-salt concentrations there was a water-clear micellar phase in each aliquot after ultra-centrifugation. The relationship between total andmicellar lipid content at three constant concentrationsof total bile-salts is shown in fig. 1. In each caseaddition of the lipid mixture caused an initial increaseand a subsequent decrease in the amount of lipidincorporated into the micellar phase. In the twosamples with normal bile-salt concentration the point
Fig. 2-Effects of increasing lipid content on micellar bile-saltconcentration at constant total bile-salt concentration.
of saturation occurred at a total-lipid level above thatnormally found after the ingestion of a standard mealcontaining 30 g. fat. Therefore throughout thenormal total-lipid range, increase in total-lipid con-tent was matched by a proportionate increase inmicellar assimilation. By contrast, in the sample withsubnormal bile-salt concentration, micellar-lipid incor-poration was maximal around the mid-point of thenormal total-lipid range and then decreased. Thus, itwas only within a narrow range of total-lipid contentthat there was an appreciable amount of micellar lipid(fig. 1).
Although the total bile-salt concentration was
fixed by the conditions of the experiment, in thetwo samples in which it was measured the micellarbile-salt concentration decreased as lipids were added(fig. 2).
Discussion
The findings of this study are in keeping with thewell-established observation that the solvent capacityof any system containing a fixed number of detergentmolecules can be overcome by an excess of solute. It isclear also that intestinal contents with subnormal bile-salt concentrations cannot dissolve the normal pro-portion of a standard lipid load, despite the achievementof a micellar phase.
In a study of normal subjects and patients who hadundergone ileectomy, Van Deest et al. found that inmost samples with a bile-salt concentration below4 mmoles per litre, there was less than 0.8 mg. ofmicellar-phase lipid per ml. of intestinal contents,whereas when bile-salt concentrations exceeded thislevel the amount of fat in the micellar phase roseprogressively. Similarly, Badley, Murphy, Bouchier,and Sherlock 15 found that in patients with chronicliver disease who had steatorrhoea the mean intra-luminal bile-salt concentration was 4 mmoles per litreor less; such patients incorporated significantly lesslipid into the micellar phase than did normal subjects orpatients with chronic liver disease without steatorrhoea,whose mean bile-salt concentrations exceeded 6 mmoles
per litre. Thus, after ileectomy and in chronic liverdisease, steatorrhoea occurs when intraluminal bile-salt concentrations exceed the c.M.c. but are belownormal. This suggests that two conditions are required
402
for normal fat absorption: (1) that the products oftriglyceride hydrolysis must be incorporated into amicellar solution-which necessitates a bile-salt con-centration in excess of the critical micellar concentra-tion (1-2 mmoles per litre); and (2) that there must bea sufficient number of micelles in the solution todissolve the lipid load-and this requires a bile-saltconcentration in excess of 4 mmoles per litre, the" critical physiological concentration " of bile-salts.Failure to achieve such a concentration results insteatorrhoea.The decrease in micellar bile-salt content in the
samples with high lipid levels is analogous to the findingsof Barton and Glover 17 and of Hofmann.18 Althoughpolar lipid such as monoglyceride can expand a bile-saltmicelle and thereby enable it to dissolve more non-polar lipid such as cholesterol, the addition of polarlipid cannot continue indefinitely, since greaterconcentrations eventually disrupt the micellar aggre-gation. The fate of bile-salt molecules releasedfrom the micellar phase at high lipid levels wasnot determined; probably they are adsorbed on tothe insoluble fraction of intestinal contents, and arethus removed from the aqueous phase by centri-fugation.19When the bile-salt concentration is normal, micellar
disruption occurs at levels of total lipid which areseldom encountered in the intestinal lumen duringdigestion of a meal; so the resultant decrease in thesolvent capacity of intestinal contents is of minor
importance. However, at subnormal bile-salt con-centrations, disruption occurs at normal postprandiallipid levels, the solvent capacity is further diminished,and steatorrhoea results.
B. W. D. B. was a Samuel R. McLaughlin travelling fel-low. G. M. M. was supported by the Medical ResearchCouncil.
Requests for reprints should be addressed to B. W. D. B.Gastroenterology Laboratory, Victoria General Hospital, Halifax,N.S., Canada.
REFERENCES
1. Hofmann, A. F., Borgström, B. J. clin. Invest. 1964, 43, 247.2. Hofmann, A. F., Small, D. M. Ann. Rev. Med. 1967, 18, 333.3. Hofmann, A. F. Biochem. J. 1963, 89, 57.4. Sjövall, J. Acta physiol. scand. 1959, 46, 339.5. Fordtran, J. S., Locklear, T. W. Am.J. dig. Dis. 1966, 11, 503.6. Austad, W. T., Lack, L., Tyor, M. P. Gastroenterology, 1967,
52, 638.7. Hardison, W. G. M., Rosenberg, I. M. New Engl. J. Med. 1967,
277, 337.8. McLeod, G. M., Wiggins, H. S. Lancet, 1968, i, 873.9. Van Deest, B. W., Fordtran, J. S., Morawski, S. G., Wilson, J. D.
J. clin. Invest. 1968, 47, 1314.10. Kim, Y. S., Spritz, N., Blum, M., Terz, J., Sherlock, P. ibid. 1966,
45, 956.11. Rosenberg I. M., Hardison, W. G., Bull, D. M. New Engl. J. Med.
1967, 276, 1391.12. Tabaqchali, S., Hatzioannou, J., Booth, C. C. Lancet, 1968, ii,
12.
13. Go, V. L. W., Poley, J. R., Hofmann, A. F., Summerskill, W. H. J.Gastroenterology, 1968, 54, 1239. (abstr.)
14. Miettinen, T. A., Siurala, M. Scand. J. clin. Lab. Invest. 1967, 19,suppl. 95, p. 69 (abstr.).
15. Badley, B. W. D., Murphy, G. M., Bouchier, I. A. D., Sherlock, S.Programme of the 70th annual meeting of the American Gastro-enterological Association; Washington, D.C., p. A4 (abstr.)1969.
16. Iwata, T., Yamasaki, K. J. Biochem. 1964, 56, 424.17. Barton, P. G., Glover, J. in The Biliary System (edited by W.
Taylor); p. 189. Oxford, 1965.18. Hofmann, A. F. Gastroenterology, 1965, 48, 484.19. Eastwood, M. A., Boyd, G. S. Biochim. Biophys. Acta, 1967, 137,
393.
THE DIFFERENTIAL FERRIOXAMINE TESTIN THE MANAGEMENT OF
IDIOPATHIC HÆMOCHROMATOSIS
P. M. SMITH
JOANNA P. G. MILLERC. S. PITCHER
A. N. LESTAS
I. W. DYMOCK
ROGER WILLIAMS
Medical Research Council Group on Metabolism and Hœmo-dynamics of Liver Disease, Department of Medicine, andDepartment of Hœmatology, King’s College Hospital, LondonS.E.5; and Department of Hœmatology, Stoke Mandeville
Hospital, Aylesbury, Buckinghamshire
Summary The differential ferrioxamine test hasbeen used in the management of 53
cases of idiopathic hœmochromatosis. Iron stores (Fv)ranged from 877 to 2234 µg. per kg. in untreated malepatients, and did not correlate with the clinicalmanifestations. Serial readings during venesectiontherapy showed a progressive decrease with a highlysignificant correlation with the quantity of ironremoved, thus confirming the value of the test as
a measure of total body-iron stores. In 18 patientsfollowed after the completion of venesection therapythere was a rapid reaccumulation of iron in associationwith a high iron absorption of 31-95%. The rate ofreaccumulation diminished as the stores increased,although there was no decline in iron absorption,suggesting a compensatory rise in iron excretion.
Introduction
WHEN desferrioxamine is given by parenteral injec-tion it chelates with iron in the body stores to formferrioxamine, which is excreted in the urine. The
greater the iron stores the more ferrioxamine is formed,but still only a fraction is excreted. Fielding I intro-duced the differential test, in which a marker dose of69Fe-Iabelled ferrioxamine is given simultaneously withthe injection of desferrioxamine. Using this test, thetotal amount of ferrioxamine formed in vivo, the Fvvalue, can be calculated. We have shown that thedifferential ferrioxamine test can distinguish idiopathichxmochromatosis from cirrhosis with a secondarysiderosis, and the results were a more reliable index of
TABLE I-FV VALUES IN 19 UNTREATED CASES OF IDIOPATHIC
HAMOCHROMATOSIS







![Bacterial pathogenesis as an imperfect symbiosis · PDF fileSalmonella enterica. serovar Typhi, ... or activating bile defense responses [10,19]. Biofilm forma - tion not only contributes](https://img.dokumen.tips/doc/110x75/5a77ec657f8b9a4b538e574f/bacterial-pathogenesis-as-an-imperfect-symbiosis-a-salmonella-enterica-serovar.jpg)





















