Embed Size (px)
Citation preview

PRENATAL DIAGNOSISPrenat Diagn 2008; 28: 999–1003.Published online 16 October 2008 in Wiley InterScience(www.interscience.wiley.com) DOI: 10.1002/pd.2092
Intra- and interobserver reliability of umbilical vein bloodflow
Susana Fernandez*, Francesc Figueras, Olga Gomez, Josep Maria Martinez, Elisenda Eixarch,Montserrat Comas, Bienvenido Puerto and Eduard GratacosFetal Medicine Department, Hospital Clinic, Universitat de Barcelona, IDIBAPS, Barcelona, Spain
Objectives To assess the intra- and interobserver reliability of the umbilical vein (UV) diameter, time-averaged maximum velocity (TAMX) and umbilical vein blood flow (BF).
Methods Sixty-three consecutive singleton pregnancies between 24 and 42 weeks were evaluated by twoindependent operators. UV diameter and TAMX were measured. UV flow was calculated as UV area × 60× TAMX × 0.5. Reliability analyses were performed by means of the intraclass correlation coefficient (ICC)for agreement. Differences between and within observers were explored and agreement limits calculated bymeans of the Bland–Altman test.
Results Satisfactory Doppler parameters were successfully obtained from all fetuses. The intraobserver ICCsfor UV diameter, TAMX, and BF were 0.7, 0.59, and 0.55, respectively, whereas the interobserver ICCs were0.65, 0.46, and 0.60, respectively. The 95% confidence intervals of the intraobserver differences were (+0.15,−0.14), (+8.0, −7.9), and (+150, −138.7), respectively. The 95% confidence intervals of the interobserverdifferences were (+0.16, −0.16), (+8.5, −8.2), and (+138.8, −141.9), respectively.
Conclusions Noninvasive Doppler calculation of umbilical vein blood flow and its components are reliableenough for clinical use. Copyright 2008 John Wiley & Sons, Ltd.
KEY WORDS: umbilical vein flow; reliability; Doppler; placental insufficiency; IUGR detection; fetal and placentalpathology
INTRODUCTION
Preliminary studies (Greenfield et al., 1951; Stemberaet al., 1964; Novy and Metcalfe, 1970; Berman et al.,1975) reporting measurement of umbilical vein (UV)blood flow (BF) were performed on animal models withinvasive techniques providing the experimental basis forearly studies on humans (Sauders et al., 1980; Gill et al.,1981; Eik-Nes et al., 1982). Later, noninvasive Dopplerumbilical vein blood flow (UVBF) assessment was con-sidered unreliable and inaccurate (Erskine and Ritchie,1985; Giles et al., 1986) and the spotlight turned towardthe umbilical artery which has, since then, become thebenchmark of prenatal care of high-risk pregnancies.The advent of high-technological ultrasound and pulsedDoppler has replaced the UV in the research agendaof many groups, and extensive research has been pub-lished (van Splunder et al., 1994; Barbera et al., 1999;Di Naro et al., 2001; Boito et al., 2002, 2004; Pennatiet al., 2004) since then. Pioneer studies based on animalmodels, using diffusion techniques versus Doppler mea-surements of UVBF on the same animal, found a cor-relation between placental mass and the UVBF (Galanet al., 1999). Hence, it has been suggested that UVBF isa more direct and physiological measurement of vascularplacental function than umbilical artery Doppler indicesand is also considered a better parameter of the quantity
*Correspondence to: Susana Fernandez, Fetal Medicine Depart-ment, Hospital Clinic, Sabino de Arana, 1 08034 Barcelona, Spain.E-mail: [email protected]
of oxygen and nutrients reaching the fetus. Despite theseencouraging results, UVBF has not caught on in clinicalpractice mainly due to concerns regarding its reliability.
Repeatability is the ability to reproduce the samemeasurements under identical conditions. Even thoughreliability should have been required before addressingvalidity issues, few studies have tackled this aspect. Insome studies primarily aimed at establishing normal-ity ranges of the UV parameters or evaluating clinicalvalue in growth restriction, reliability issues have beenconsidered, yielding contradictory results (van Splun-der et al., 1994; Barbera et al., 1999; Lees et al., 1999;Boito et al., 2002). In addition, the number of patientsincluded in these subanalyses was limited and the statis-tical procedures did not fulfill the current methodologicalrecommendations.
The aim of our study was to determine the intra-and interobserver reliability of ultrasound measure-ment of UV diameter, time-averaged maximum velocity(TAMX) and BF.
METHODS
Patients
Our study population comprised 63 consecutive womenwith singleton pregnancies. Inclusion criteria were:(1) confirmed gestational age by ultrasound before15 weeks; (2) absence of structural malformation orchromosomal abnormality; (3) fetal growth between the
Copyright 2008 John Wiley & Sons, Ltd. Received: 20 July 2007Revised: 23 July 2008
Accepted: 23 July 2008Published online: 16 October 2008

1000 S. FERNANDEZ ET AL.
10th and 90th percentile; and (4) umbilical artery pul-satility index (PI) within normal ranges for gestationalage. Informed consent was obtained from all patients.Our study was approved by the local Ethics Committee.
Doppler recordings
Image-directed pulsed and color Doppler equipment(Voluson 730 Pro, GE Medical Systems, Milwaukee, WI,USA) with a multifrequency sector array transabdominaltransducer was used. The UV was sampled at a free-floating loop in a longitudinal plane as parallel to thetransducer as possible and zoomed to occupy morethan 30% of the image. The internal diameter wasmeasured inner-to-inner at three different sites and themean value of the three measurements was calculated.The TAMX was measured in the same free-floatingloop portion adjusting the scanning insonation angle asclose to 0◦ as possible and always below 30◦; anglecorrection was performed when 0◦ insonation anglewas not possible. Sample volume was set to insonatethe entire diameter of the vessel. Measurements wereperformed during fetal quiescence from a 10-s steady-state velocity profile. UVBF (mL/min) was calculatedas reported elsewhere (Barbera et al., 1999): UV area(cm2) × 60 × TAMX (cm/s) × 0.5. The high pass filterwas set at 50 Hz and energy output levels were lowerthan 50 mW/cm2.
In order to assess the intraobserver reliability, oneobserver blindly obtained both the diameter and TAMXtwice, whereas to assess the interobserver reliability asecond independent observer measured the UV diameterand TAMX once.
Statistical analysis
A sample size estimation for reliability was calculated(Walter et al., 1998) using an interclass correlationcoefficient (ICC) with α = 0.05 and β = 0.2. We aimedfor an optimum reliability of at least 0.7 and accepted areliability of 0.4 as a criterion for moderate agreement.We defined H0: ρ = 0.7 and H1: ρ = 0.4, and weobtained a sample size requirement of 63 cases.
To assess interobserver reliability, a two-way randommodel (women and observers conceived as random sam-ples) single-measure ICC for absolute agreement wascalculated. To assess intraobserver reliability, a two-waymixed model (women conceived as random samples)single-measurement ICC for absolute agreement wascalculated. The ICC is a measure of concordance forcontinuous variables, correcting the correlation for sys-tematic bias and measuring the extent to which thosevariables will yield the same score when assessed in dif-ferent conditions, namely, between and within observers.The following benchmarks were used for ICC charac-terization (Fleiss, 1981): slight reliability (0–0.2), fairreliability (0.21–0.4), moderate reliability (0.41–0.6),substantial reliability (0.61–0.8), and almost perfect reli-ability (0.81–1.0).
The degree of agreement was also examined usingthe limits of agreement method or the Bland–Altman
test (Bland and Altman, 2003) which allows calculationof the range in which 95% of the disagreement betweenobservations is likely to occur and is defined as the meandifference ±1.96 standard deviation (SD).
Statistical analysis was performed using the StatisticalPackage for the Social Sciences (SPSS 10.1, SPSS Inc.,Chicago, IL, USA) and the Med Calc 8.0 (Broekstraat,Belgium) statistical software.
RESULTS
UV diameter and TAMX were successfully obtainedby both observers in all cases. The mean elapsed timebetween the first measurement of the first examiner andthe last measurement of the second examiner was 3.2(SD 1.3) min. The mean insonation angle was 15◦ (SD4.2). The mean maternal age in the study group was29.6 (SD 4.6) years and the median gestational age was33 weeks (range: 24–42; interquartile range: 28–34) atthe time of the scan.
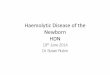
Table 1 summarizes the ICC values and their 95%confidence interval (CI) for each parameter studied. UVdiameter, TAMX, and BF showed values within therange considered moderate or substantial agreement.
Figures 1 to 3 show the Bland–Altman plots of thedifference versus the mean of paired measurementswithin observers. Figures 4 to 6 show the Bland–Altmanplots of the difference versus the mean of pairedmeasurements between observers.
DISCUSSION
Early studies (Erskine and Ritchie, 1985; Giles et al.,1986; van Splunder et al., 1994) emphasized thatalthough it was feasible, UVBF had little clinicalpotential because of measurement inaccuracies. Morerecently, by means of modern ultrasound technology,Barbera et al. (1999) reported intra- and interobservercoefficients of variation for the UV diameter, meanvelocity, and BF that varied from 2.9 to 12.7%, whichcorrespond to moderate variability. It is of note that thelowest variability was observed in the diameter calcula-tion whereas the highest was for BF. However, the coef-ficient of variation is a measure of the degree of spreadin data around the mean and is not considered a stan-dard parameter for reliability (Allison, 1993). Lees et al.(1999) reported good interobserver agreement for bothmean velocity and vein area in a subsample of sevenfetuses. Nevertheless, owing to the small sample size, noappropriate conclusions could be drawn from their data.To our knowledge, no further studies have addressedreliability, and clinical research in this field has takenthese results for granted. We have observed that bothintra- and interobserver reliability for UVBF calcula-tion are moderate, similar to reliability values reportedfor umbilical artery indices of resistance (Nakai et al.,2002) and pulsatility (Scherjon et al., 1993), which havebecome the benchmark in high-risk pregnancy care. Ourresults therefore support the clinical use UVBF.
Copyright 2008 John Wiley & Sons, Ltd. Prenat Diagn 2008; 28: 999–1003.DOI: 10.1002/pd

INTRA- AND INTEROBSERVER RELIABILITY OF UVBF 1001
Table 1—Interobserver and intraobserver intraclass correlation coefficient of umbilical vein (UV) diameter, time-averagedmaximum velocity (TAMX), and blood flow
Intraobserver ICC(95% CI)
Interobserver ICC(95% CI)
UV diameter 0.7 (0.55–0.81) 0.65 (0.48–0.78)UV TAMX 0.59 (0.4–0.74) 0.46 (0.23–0.64)UV blood flow 0.55 (0.35–0.7) 0.6 (0.4–0.74)
Slight Reliability
Fair Reliability
Moderate Reliability
Substantial Reliability
Almost perfectReliability
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
UV Diam
eter
UV TM
AX
UV Bloo
d Flow
Intraobserver ICC Interobserver ICC
ICC, intraclass correlation coefficient; CI, confidence interval.
4
UV
Dia
met
er11
- U
V D
iam
eter
12
3.5 4.5 5.5 6.5 7.5 8.5 9.5 10.5
AVERAGE of UV Diameter11 and UV Diameter12
3
2
1
0
-1
-2
Mean0,1
-1.96 SD-1,4
+1.96 SD1,5
Figure 1—Bland–Altman plot of the difference versus the mean ofpaired measurements of the umbilical vein (UV) diameter (mm) ofthe two measurements of the first observer
Small errors in the volume flow components resultin larger errors in the volume flow calculation (Eik-Nes et al., 1982). Thus, technique standardization isof paramount importance when measuring vein flow.The umbilical cord is the longest vessel in the humanfetus and it has been demonstrated that UV diameterprogressively decreases from the fetus to the placenta byalmost 1 mm (Li et al., 2005). This finding is importantbecause in the calculation of the flow the diameter issquared, so the difference between the different portionsof the cord would take a greater difference in the flow.
10 15 20 25 30
AVERAGE of TAMX11 and TAMX12 (cm/s)
15
10
5
0
-5
-10
-15
TA
MX
11 -
TA
MX
12 (
cm/s
)
Mean0,1
-1.96 SD-7,9
+1.96 SD8,0
Figure 2—Bland–Altman plot of the difference versus the meanof paired measurements of the umbilical vein TAMX of the twomeasurements of the first observer (cm/s)
Therefore, since serial samplings at a free-floating loopof the umbilical cord are likely to be obtained fromdifferent portions, this could be a source of unreliability.One could speculate that sampling the fetal (Kay et al.,1989) or placental end (Abramowicz et al., 1989) ofthe UV, where there are specific landmarks, is likelyto improve reliability. The umbilical cord placental endis not easily identifiable in many cases, especially in thethird trimester (Pretorius et al., 1996), which could limitits clinical use. Finally, other sources of unreliabilitycould specifically be relevant at the fetal end, such as
Copyright 2008 John Wiley & Sons, Ltd. Prenat Diagn 2008; 28: 999–1003.DOI: 10.1002/pd

1002 S. FERNANDEZ ET AL.
0 100 200 300 400 500
AVERAGE of UVBF11 and UVBF12
250
200
150
100
50
0
-50
-100
-150
-200
UV
BF1
1 -
UV
BF1
2
Mean6,1
-1.96 SD-138,7
+1.96 SD150,9
Figure 3—Bland–Altman plot of the difference versus the mean ofpaired measurements of the umbilical vein blood flow of the twomeasurements of the first observer (mL/min)
UV
Dia
met
er1M
- U
V D
iam
eter
2
4.0 5.0 6.0 7.0 8.0 9.0 10.0
AVERAGE of UV Diameter1M and UV Diameter2
2.5
2.0
1.5
1.0
0.5
0.00
-0.5
-1.0
-1.5
-2.0
Mean-0,01
-1.96 SD-1,68
+1.96 SD1,47
Figure 4—Bland–Altman plot of the difference versus the mean of thepaired measurements between observers of the umbilical vein diameter(mm)
10 15 20 25 30
AVERAGE of TAMX1M and TAMX2 (cm/s)
15
10
5
0
-5
-10
-15
TA
MX
1M -
TA
MX
2 (c
m/s
)
Mean0,2
-1.96 SD-8,2
+1.96 SD8,5
Figure 5—Bland–Altman plot of the difference versus the mean of thepaired measurements between observers of the umbilical vein TAMX
the effect of the umbilical ring (Skulstad et al., 2004)and the fetal breathing movements.
0 100 200 300 400 500
AVERAGE of UVBF1M and UVBF2
200
150
100
50
0
-50
-100
-150
-200
UV
BF1
M -
UV
BF2
Mean-1,6
-1.96 SD-141,9
+1.96 SD138,8
Figure 6—Bland–Altman plot of the difference versus the mean of thepaired measurements between observers of the umbilical vein bloodflow (mL/min)
Changes in the UV velocity rather than in itsdiameter are the major contributors to the reduced UVBFobserved in growth-restricted fetuses (Ferrazzi et al.,2000). Hence, technical aspects regarding this parametercould have a great impact on reliability. Some studies(Gill et al., 1981; Laurin et al., 1987; Tchirikov et al.,1998) have calculated the mean velocity by means ofDoppler shift spectral analysis which is performed afterfiltering the low-velocity component of the flow. Remov-ing this low-velocity component might result in an over-estimation of the true mean velocity when blood veloci-ties are in the range of the umbilical venous flow (Evanset al., 1989). We have estimated the mean velocity ashalf the TAMX, assuming a parabolic flow through thecord. Nevertheless, since the UV is modeled as a heli-coidal tube, a slight departure from a perfect parabolicflow could be expected. Pennati et al. (2004) used 2Dvelocity profile obtained at a cross section of the UV indifferent portions of the cord, in order to evaluate thecoefficient of variation of the velocity. They found thatthe coefficient was significantly higher in the placentalinsertion than in the free loop. So, they confirmed thatvelocity profiles vary along the cord and that a perfectparabolic flow cannot be expected. We have used the 0.5coefficient to calculate the mean velocity, and althoughthe value of the flow is not the aim of our study wemay be underestimating the flow. Consensus regardingwhether the 0.5 coefficient variation is appropriate tocalculate the flow is needed.
UVBF has been observed to closely correlate with themass of cotyledons (Galan et al., 1999) and it has beenclaimed (Ferrazzi, 2001) that this noninvasive parameterprovides the greatest information regarding the quantityof oxygen and nutrients reaching the fetus. A decreasein this contribution might cause first a decline in thegrowth rate, and later an entire cascade of hemodynamicchanges. Rigano et al. (2001) found that the UVBFdecreases weeks before the reduction in fetal growthoccurs. Identification of this early stage could lead toan effective identification of a fetus at high risk ofdeveloping growth restriction. On the other hand, whenmonitoring growth-restricted fetuses, timing of delivery
Copyright 2008 John Wiley & Sons, Ltd. Prenat Diagn 2008; 28: 999–1003.DOI: 10.1002/pd

INTRA- AND INTEROBSERVER RELIABILITY OF UVBF 1003
is still a critical issue. In the Doppler diagnostic arsenal,the integration of UVBF could provide a more compre-hensive management. Nonetheless, further investigationis required to assess the usefulness of these strategies.
In conclusion, UV flow and its components arereliable enough for clinical use, but a consensus in whichportion of the umbilical vein is optimal and how tocalculate the mean velocity is required in order to reduceits inaccuracy. The clinical use of UV flow needs furtherinvestigation in order to evaluate its possible applicationin early diagnosis, monitoring, and timing of the deliveryof growth-restricted fetuses.
REFERENCES
Abramowicz JS, Warsof SL, Arrington J, Levy DL. 1989. Doppleranalysis of the umbilical artery. The importance of choosing theplacental end of the cord. J Ultrasound Med 8(4): 219–221.
Allison DB. 1993. Limitations of coefficient of variation as index ofmeasurement reliability. Nutrition 9(6): 559–561.
Barbera A, et al. 1999. Relationship of umbilical vein blood flow togrowth parameters in the human fetus. Am J Obstet Gynecol 181(1):174–179.
Berman W Jr, et al. 1975. Measurement of umbilical blood flow infetal lambs in utero. J Appl Physiol 39(6): 1056–1059.
Bland JM, Altman DG. 2003. Applying the right statistics: analysesof measurement studies. Ultrasound Obstet Gynecol 22(1): 85–93.
Boito S, et al. 2002. Umbilical venous volume flow in the normallydeveloping and growth-restricted human fetus. Ultrasound ObstetGynecol 19(4): 344–349.
Boito SM, et al. 2004. Umbilical venous volume flow and fetalbehavioral states in the normally developing fetus. UltrasoundObstet Gynecol 23(2): 138–142.
Di Naro E, et al. 2001. Umbilical vein blood flow in fetuses withnormal and lean umbilical cord. Ultrasound Obstet Gynecol 17(3):224–228.
Eik-Nes SH, et al. 1982. Ultrasonic measurement of human fetalblood flow. J Biomed Eng 4(1): 28–36.
Erskine RL, Ritchie JW. 1985. Quantitative measurement of fetalblood flow using Doppler ultrasound. Br J Obstet Gynaecol 92(6):600–604.
Evans DH, Schlindwein FS, Levene MI. 1989. The relationshipbetween time averaged intensity weighted mean velocity, andtime averaged maximum velocity in neonatal cerebral arteries.Ultrasound Med Biol 15(5): 429–435.
Ferrazzi E. 2001. Measurement of venous blood flow in the humanfetus: a dream comes true, but now for some standardization.Ultrasound Obstet Gynecol 18(1): 1–4.
Ferrazzi E, et al. 2000. Umbilical vein blood flow in growth-restrictedfetuses. Ultrasound Obstet Gynecol 16(5): 432–438.
Fleiss J. 1981. Statistical Methods for Rates and Proportions (2ndedn). John Wiley and Sons: New York.
Galan HL, et al. 1999. Umbilical vein blood flow determination in theovine fetus: comparison of Doppler ultrasonographic and steady-state diffusion techniques. Am J Obstet Gynecol 181(5 Pt 1):1149–1153.
Giles WB, et al. 1986. Fetal volume blood flow and umbilicalartery flow velocity waveform analysis: a comparison. Br J ObstetGynaecol 93(5): 461–465.
Gill RW, et al. 1981. Fetal umbilical venous flow measured in uteroby pulsed Doppler and B-mode ultrasound. I. Normal pregnancies.Am J Obstet Gynecol 139(6): 720–725.
Greenfield AD, Shepherd JT, Whelan RF. 1951. The rate of blood-flow in the umbilical cord. Lancet 2(10): 422–424.
Kay HH, et al. 1989. Nonuniformity of fetal umbilical sys-tolic/diastolic ratios as determined with duplex Doppler sonography.J Ultrasound Med 8(8): 417–420.
Laurin J, et al. 1987. Fetal blood flow in pregnancies complicated byintrauterine growth retardation. Obstet Gynecol 69(6): 895–902.
Lees C, et al. 1999. Assessment of umbilical arterial and venous flowusing color Doppler. Ultrasound Obstet Gynecol 14(4): 250–255.
Li WC, Ruan XZ, et al. 2006. Biomechanical properties of differentsegments of human umbilical cord vein and its value for clinicalapplication. J Biomed Mater Res B Appl Biomater 76(1): 93–97.
Nakai A, et al. 2002. Reproducibility of pulsed Doppler measurementsof the maternal renal circulation in normal pregnancies and thosewith pregnancy-induced hypertension. Ultrasound Obstet Gynecol19(6): 598–604.
Novy MJ, Metcalfe J. 1970. Measurements of umbilical blood flowand vascular volume by dye dilution. Am J Obstet Gynecol 106(6):899–906.
Pennati G, et al. 2004. Spatial velocity profile changes along the cordin normal human fetuses: can these affect Doppler measurementsof venous umbilical blood flow? Ultrasound Obstet Gynecol 23(2):131–137.
Pretorius DH, et al. 1996. Placental cord insertion visualization withprenatal ultrasonography. J Ultrasound Med 15(8): 585–593.
Rigano S, et al. 2001. Early and persistent reduction in umbilical veinblood flow in the growth-restricted fetus: a longitudinal study. AmJ Obstet Gynecol 185(4): 834–838.
Sauders JB, Wright N, Lewis KO. 1980. Measurement of human fetalblood flow. Br Med J 280(6210): 283–284.
Scherjon SA, et al. 1993. Intra-observer and inter-observer reliabilityof the pulsatility index calculated from pulsed Doppler flow velocitywaveforms in three fetal vessels. Br J Obstet Gynaecol 100(2):134–138.
Skulstad SM, Kiserud T, Rasmussen S. 2004. The effect of vascularconstriction on umbilical venous pulsation. Ultrasound ObstetGynecol 23(2): 126–130.
Stembera ZK, et al. 1964. Measurement of umbilical cord blood flowby local thermodilution. Am J Obstet Gynecol 90: 531–536.
Tchirikov M, et al. 1998. Blood flow through the ductus venosus insingleton and multifetal pregnancies and in fetuses with intrauterinegrowth retardation. Am J Obstet Gynecol 178(5): 943–949.
van Splunder IP, et al. 1994. Presence of pulsations and reproducibil-ity of waveform recording in the umbilical and left portal vein innormal pregnancies. Ultrasound Obstet Gynecol 4(1): 49–53.
Walter SD, Eliasziw M, Donner A. 1998. Sample size and optimaldesigns for reliability studies. Stat Med 17(1): 101–110.
Copyright 2008 John Wiley & Sons, Ltd. Prenat Diagn 2008; 28: 999–1003.DOI: 10.1002/pd