Embed Size (px)
Citation preview

RARE OR OBSCURE CASES 157
The crcscentic incision on each side of thc patella, and the patella-splitting approach, werc all insuflicieiit to discover the very definite body present in this knee. It would appear impossible to make sure of exploring thc whole joint by using €ewer than three incisions : one anterior, either the usual cres- centic incision or the patella-splitting approach ; and two posterior, one for each posterior pouch. These small posterior incisions are so easily made, and do so little harm to the joint, that their more frequent use in doubtful cases seems worth recornmcnding.
The patient made a smooth and rapid rccovery.
My thanks this case.
are due to Mr. E. W. Hey Groves for permission to publish
INTESTINAL DUE TO
OBSTRUCTION IN AN INFANT 3 DAYS OLD, ABNORMAL ROTATION OF THE MID-GUT.
BY FRANK HARVEY, LONDON.
ABNOI~JIAI, rotation of the inid-gut causing intestinal obstruction in a new-born cldtl is a rare condition. It has been shown by Normaii 11. Dott, of Edin- hurgh,l that the clinical symptom caused thereby O C C U ~ most frequently within a €ew clays of birth.
Embryology.-Duritig the early weeks of cmbryonic life the liver and mirl-gut loop grow so rapidly that there is insufficient accommodation in the abdominal cavity of the embryo, and as a consequence the mid-gut loop is situated in a funnel-shaped cavity formed by an extension of thc ccrlom- the iuinhilical ccelom-within the umbilical cnd of the cord.2
The superior mcsenteric artery supplies the mid-gut loop and divides i t into an anterior and a posterior segment. From the aiitcrior or pre-arterial wgnieiit is developcd all that part of the duodenum below the bile papilla, all the jejunum, and the ileum. From the post-artcrial segment are dcveloped the czcum, appendis, ascending colon, hepatic flexure, and two-thirds of the transverse colon, thc remaining third of the transverse colon being developed from thc hind-gut.
-4t the tcnth week the mid-gut loop returns into the abdominal cavity, and, according to Frazer and Robbins,s the pre-arterial precedes the post- arterial segnieiits, as it is impossible, owing to their bulk, for both the segments to hc reduced together.
left post
As a conseqkice ol this arrangement the hind-gut gets pushed to the side of thc abdoiniiial cavity, and the sniall intestines occupy a plane
:erior to the transverse colon with the caxuin and ascending colon on the right, as these are reduced last into the eceloin.
In the casc to be described, the post-arterial segment apparently returned first iiito thc abdominal cavity, so that the small intestines occupied an anterior plane to the large.
l)r. T. D. Manning, of Sanclhurst, nerlrs, a feniale child, 3 days old. Description of Case.-On March 16, 1924, I saw. iii consultation with
The

188 THE BRITISH JOURNAL O F SURGERY
child had passed nothing per anum since birth, and was vomiting dark- green fluid. On examination, the abdomen was very distended, especially so on the right side. The anus was small, and admitted a No. 10 Hegar dilator, which was passed for 3 in., and on its withdrawal was not stained with meconium.
An anaesthetic was administered, and, on opening the abdominal cavity by a right paramedian incision with
It was decided to operate immediately.
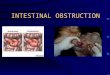
FIG. 119.-Semidiagrammatic drawing made from a sketch drawn immediately after the operation. The distended stomach with its rudimentary omenturn is shown turned up on the costal margin to enable the position of the transverse colon on the posterior abdominal wall to be demonstrated. The hepatic flexure is shown diap!sced to the right so that the con- striction of the transverse colon can be seen, where it passes through the mesentery of the small intestine. The opening in the mesentery was oval in shape and flattened in an antero- posterior direction.
its centre a t the umbilicus, gas and fluid meconium gushed out, and coils of small intestine, distended with gas, presented. The caecum was sought for and found just below the liver, not having completely descended into the right iliac fossa, and was greatly distended with gas, as was the appendix, which was blown out like the Snger of a glove.
On tracing the ascending colon it was found to dip backwards towards

RARE OR OBSCURE CASES 189
the vertebral column, and a t the hepatic flexure was a rupture of all the coats of the bowel, from which meconium and gas were escaping. On further tracing the colon, i t was seen to pass through a small opening about 5 mm. i n diameter, in the mesentery of the small intestine, below the superior mesen- teric artery. Further examination showed that the continuation of the colon, on the other side of the opening in the mesentery of the small intestine, was much reduced in size, being only about 5 or 6 mm. in diameter, as were the splenic flexure and the descending and pelvic colons.
Into the rupture of the colon was placed a drainage tube, and the opening closed around the tube by a purse-string suture of catgut, and the colon anchored to the anterior abdominal wall by a catgut suture. After sponging the abdominal cavity free from meconium, it was closed except for an opening through which the drainage tube passed.
No post-mortem was granted.
The patient survived the operation b u t a short while.
CONCLUSIONS. 1 . That adhesion and fisation of the mesentery occurs in the third month,
and is probably completed by the fourth month, as otherwise the colon would riot have been occluded in the case described above.
2 . That according to Dr. A. Low meconium reaches the rectum a t the fifth month, and that the obstruction in the case described must have occurred by the end of the fourth month.
8. That many unusual positions of the small and large bowel found during operations on adults aye due to defective or abnormal rotation of the mid-gut a-k the third or fourth month of embryonic life.
In conclusion, I wish to acknowledge my indebtedness to Dr. T. D. Manning for providing me with the case for operation ; t o Sir James Berry for helpful criticism ; t o Sir Arthur Keith for kindly advice ; to Mr. Ralph Coyte for his kindness in correcting the proofs ; and to Mr. Thornton Shiells €or his drawing of the case from a sketch madc by myself immediately after the operation (Fig . 118).
Readers of the Biu~rsrr JOURNAL OF SURGERY will yemember that the whole subject of anomalies of intestinal rotation, with a most complete biblio- graphy, bringing the subject up to date, was most admirably described and illustrated by Mr. Norman 1\1. Dott in the ,Journal for October, 1923 (vol. xi). One of the illustrations represents a condition almost identical t o that shown in the drawing of my case, which I may add was made hefore I had my atten- tion drawn to this article. I wish to record my thanks to Mr. Dott for the invaluable help I derived from his paper in forming a correct interpretation of the condition found in the case I have described.
REFERENCES. Dor'r, NORMAN W., Bril. Jour. Surg., 1923, xi, 267. KEITII, Sir ARTHUR, Ilzimati Embnjology and Morphology, 3rd. ed., 268 and 209. FRAZER, S. E., and ROBBINS, H. H., Jour. of Anat., 1915, I , 75.