Embed Size (px)
Citation preview

Interventions to Reduce Inflammation
and Immune Activationin Treated HIV Infection
Peter W. Hunt, MD
Assistant Professor of Medicine
UCSF HIV/AIDS Division

Treating Immune Activation in HIV• What have we learned from recent
unsuccessful attempts?
• Mechanistic pathways of HIV pathogenesis inform therapeutic interventions.
• Highlight ongoing and recently reported studies of novel interventions.
– Importance of studying ART-suppressed patients
• A way forward

What have we learned from recent unsuccessful attempts to decrease immune activation?

IL-2 Increases CD4 Counts in Treated Patients
Abrams et al, NEJM, 2009
IL-2 also decreases HLA-DR and CD38 expression(Kovacs, NEJM, 1995)

However, IL-2 Had No Effect on AIDS/Death
Abrams et al, NEJM, 2009
P=0.47
P=0.55

Why Didn’t IL-2 Work?
IL-2
Preferential Expansion
of Tregs
Suppression of Healthy T Cell
Responses
Increased CD4 Count Good for
Health
Bad for Health

Maraviroc Intensification Increases CD8 Activation Compared to Placebo
Hunt, CROI, 2011, Abstract 153LB

>2-fold Increase in Plasma CCR5 Ligand Levels During Maraviroc Intensification
• Due to prevention of ligand-receptor complex internalization by CCR5+ cells (Lin/Corbeau, AIDS, 2007; Nakata, Antiviral Threrapy, 2010)
• RANTES/MIP-1a may activate monocytes/macrophages and neutrophils via CCR1

What Have We Learned?
• Immune system is complicated!
– Multiple parallel and competing pathways, feedback loops
• Primary effects assessed in vitro may fail to capture important competing secondary effects in vivo
• Need for carefully designed placebo-controlled trials, follow up studies to elucidate these mechanisms
• May need to improve more than surrogate inflammatory markers to advance to clinical endpoint trials (i.e., FMD, BMD, etc).

What specific mechanisms should we intervene upon?

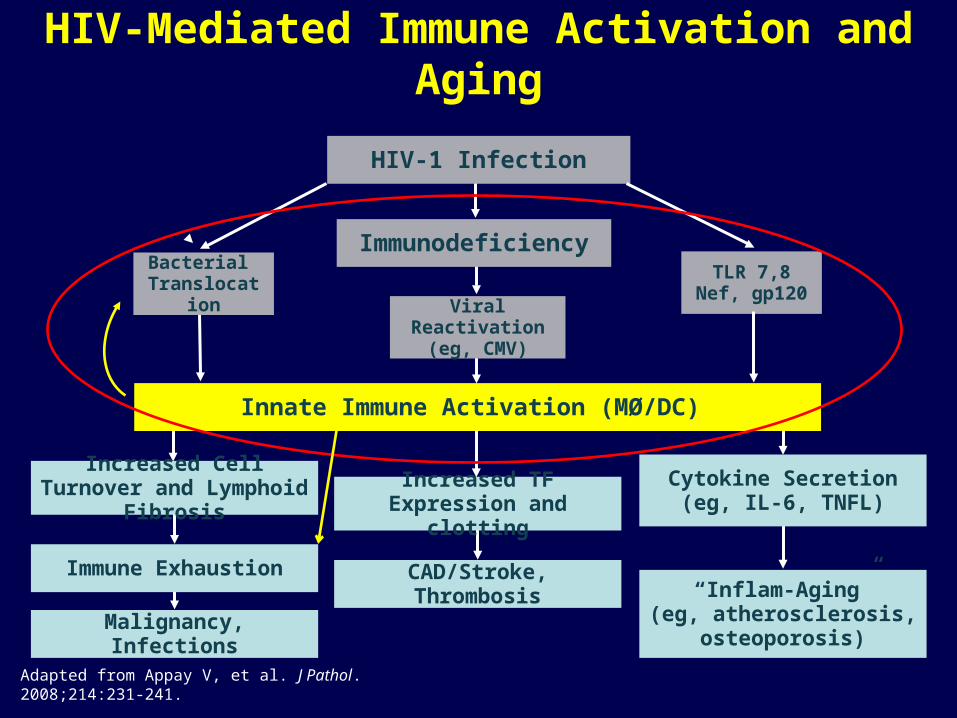
Adapted from Appay V, et al. J Pathol. 2008;214:231-241.
HIV-1 Infection
ImmunodeficiencyBacterial
TranslocationViral Reactivation
(eg, CMV)
Innate Immune Activation (MØ/DC)
Increased Cell Turnover and Lymphoid Fibrosis
Immune Exhaustion
Malignancy, Infections
Cytokine Secretion(eg, IL-6, TNFL)
“Inflam-Aging”(eg, atherosclerosis,
osteoporosis)
HIV-Mediated Immune Activation and Aging
TLR 7,8Nef, gp120
Increased TF Expression and clotting
CAD/Stroke, Thrombosis
Adapted from Appay V, et al. J Pathol. 2008;214:231-241.
HIV-1 Infection
ImmunodeficiencyBacterial
TranslocationViral Reactivation
(eg, CMV)
Innate Immune Activation (MØ/DC)
Increased Cell Turnover and Lymphoid Fibrosis
Immune Exhaustion
Malignancy, Infections
Cytokine Secretion(eg, IL-6, TNFL)
“Inflam-Aging”(eg, atherosclerosis,
osteoporosis)
HIV-Mediated Immune Activation and Aging
TLR 7,8Nef, gp120
Increased TF Expression and clotting
CAD/Stroke, Thrombosis

Adapted from Appay V, et al. J Pathol. 2008;214:231-241.
HIV-1 Infection
ImmunodeficiencyBacterial
TranslocationViral Reactivation
(eg, CMV)
Innate Immune Activation (MØ/DC)
Increased Cell Turnover and Lymphoid Fibrosis
Immune Exhaustion
Malignancy, Infections
Cytokine Secretion(eg, IL-6, TNFL)
“Inflam-Aging”(eg, atherosclerosis,
osteoporosis)
HIV-Mediated Immune Activation and Aging
TLR 7,8Nef, gp120
Increased TF Expression and clotting
CAD/Stroke, Thrombosis

Anti-LPS antibodies have no effect on CD4 recovery: CORAL
HIV+On cART
CD4<350 cells/ul∆CD4<50 past 12 months
Raltegravir HIBC+
placebo HIBC+
Raltegravir placebo+
placebo placebo+
HIBC= hyperimmune bovine colostrumEnriched in anti-LPS antibodies
n=18
n=18
n=18
n=18RESULTSNo effect on CD4 recoveryNo effect on LPS, sCD14, T cell activation
Bykawaga et al, J Infect Dis 2011 (in press) Slide courtesy of Sharon Lewin

Microbial Translocation:Cause or Consequence of Immune Activation
in Treated HIV Infection?
• Observational studies linking MT to immune activation cannot prove causality– Causality can only be formally addressed in clinical trials
• DC/Macrophage activation can cause IDO induction, ↓Th17, and microbial translocation
• Ongoing/Planned studies assessing blocking microbial translocation directly– Rifaximin (ACTG)
– Sevalamer (ACTG)

Adapted from Appay V, et al. J Pathol. 2008;214:231-241.
HIV-1 Infection
ImmunodeficiencyBacterial
TranslocationViral Reactivation
(eg, CMV)
Innate Immune Activation (MØ/DC)
Increased Cell Turnover and Lymphoid Fibrosis
Immune Exhaustion
Malignancy, Infections
Cytokine Secretion(eg, IL-6, TNFL)
“Inflam-Aging”(eg, atherosclerosis,
osteoporosis)
HIV-Mediated Immune Activation and Aging
TLR 7,8Nef, gp120
Increased TF Expression and clotting
CAD/Stroke, Thrombosis

Chloroquine Might Reduce CD8 Activationin Untreated HIV+ Patients
Chloroquine Placebo
Murray, JV, 2010
• No apparent effect on plasma HIV RNA Levels (though some missing data)• Possible early decrease in plasma LPS• Probable mechanism: TLR inhibition (3,4,7,8,9)

Hydroxychloroquine Did Not Reduce CD8 Activation in Untreated HIV+ Patients
%CD38+HLA-DR+ CD8s
Paton, IAS 2011, MOPE269
Why did viral load increase with HCQ?
And why didn’t CD8 activation increase with the increase in VL?
Viral Load
-.1
0
.1
.2
.3
.4
Me
an
(p
oin
twis
e 9
5%
CI)
0 12 24 36 48Weeks from randomisation
HCQ Placebo
Change in lrna from randomisation: by Arm
Pla
sma
HIV
RN
A L
evel
(lo
g10
co
pie
s/m
l)
-10
-5
0
5
Me
an (
poi
ntw
ise
95%
CI)
0 12 24 36 48Weeks from randomisation
HCQ Placebo
Change in cd8cd38DR_p from randomisation: by Arm

Impact of Innate Immune ResponseUntreated HIV Disease
The Bad:
Immune Activation ↑
The Good:
HIV replication ↓
Direct Antiviral Effects
Adjuvant to HIV-specific T cells
IL-6, TNFα↑
TF expression, D-dimer ↑
T cell turnover/exhaustion ↑
LN fibrosis ↑
Immune Activation ↓

Impact of Innate Immune ResponseDuring ART-mediated VL Suppression
The Good: None
VL already suppressed by
drugs
Antiviral Effects Irrelevant
The Bad
Immune Activation ↑
IL-6, TNFα↑
TF expression, D-dimer ↑
T cell turnover/exhaustion
LN fibrosis
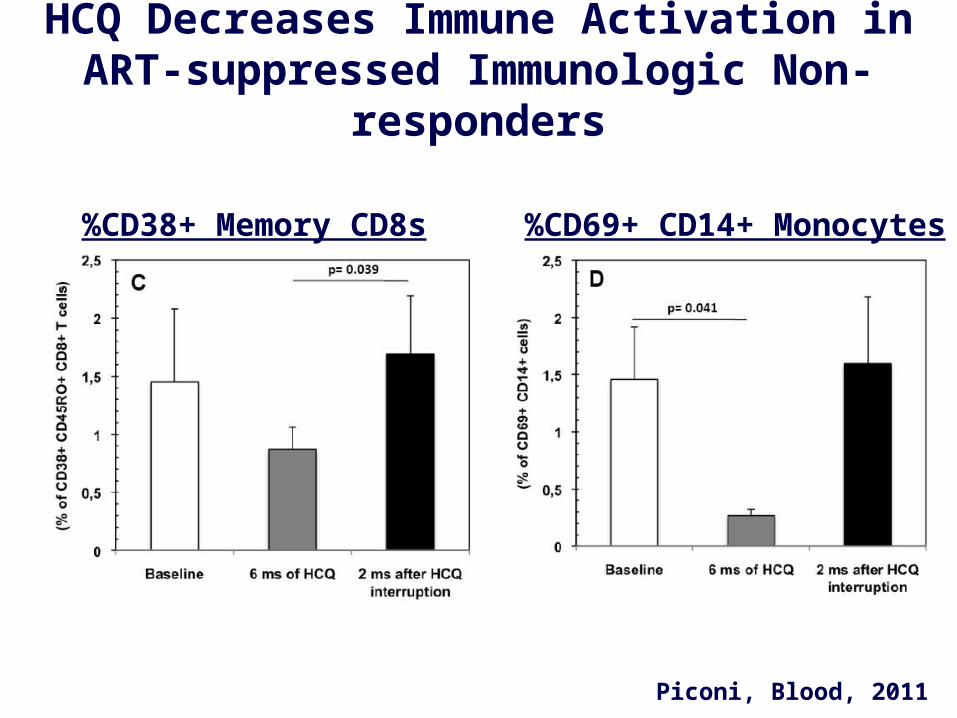
HCQ Decreases Immune Activation in ART-suppressed Immunologic Non-responders
%CD38+ Memory CD8s
Piconi, Blood, 2011
%CD69+ CD14+ Monocytes

Adapted from Appay V, et al. J Pathol. 2008;214:231-241.
HIV-1 Infection
ImmunodeficiencyBacterial
TranslocationViral Reactivation
(eg, CMV)
Innate Immune Activation (MØ/DC)
Increased Cell Turnover and Lymphoid Fibrosis
Immune Exhaustion
Malignancy, Infections
Cytokine Secretion(eg, IL-6, TNFL)
“Inflam-Aging”(eg, atherosclerosis,
osteoporosis)
HIV-Mediated Immune Activation and Aging
TLR 7,8Nef, gp120
Increased TF Expression and clotting
CAD/Stroke, Thrombosis

Decreasing Asymptomatic CMV Replication with Valganciclovir Decreases Immune Activation
in HIV+ Patients with CD4<350 despite ART
-4.4%
HIV-Median
Hunt et al, JID, 2011
• Cytopenias may limit long-term usefulness.
• Need new, safer CMV agents!

Adapted from Appay V, et al. J Pathol. 2008;214:231-241.
HIV-1 Infection
ImmunodeficiencyBacterial
TranslocationViral Reactivation
(eg, CMV)
Innate Immune Activation (MØ/DC)
Increased Cell Turnover and Lymphoid Fibrosis
Immune Exhaustion
Malignancy, Infections
Cytokine Secretion(eg, IL-6, TNFL)
“Inflam-Aging”(eg, atherosclerosis,
osteoporosis)
HIV-Mediated Immune Activation and Aging
TLR 7,8Nef, gp120
Increased TF Expression and clotting
CAD/Stroke, Thrombosis

Atorvostatin Decreases T Cell Activation in Untreated HIV Infection
Atorvostatin 80mg
Placebo
Ganesan, J Infect Dis, 2011
• 24 untreated patients, X-over design
• Significant reduction in HLA-DR on CD8s during atorvostatin Tx
• No effect on plasma HIV RNA levels
• Studies ongoing in ART-suppressed patients
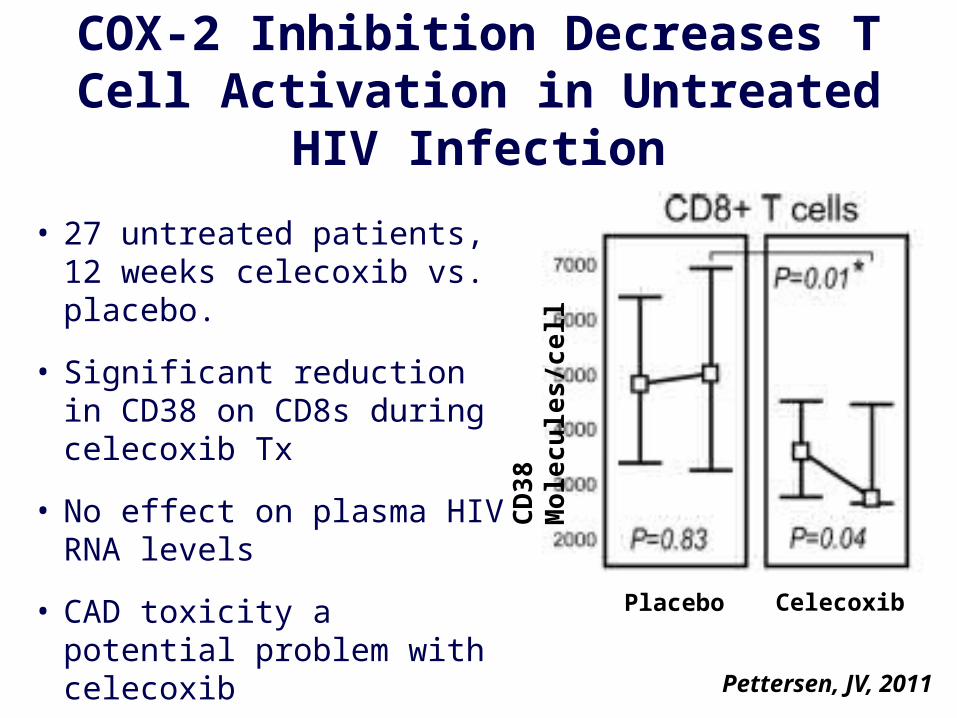
COX-2 Inhibition Decreases T Cell Activation in Untreated HIV Infection
• 27 untreated patients, 12 weeks celecoxib vs. placebo.
• Significant reduction in CD38 on CD8s during celecoxib Tx
• No effect on plasma HIV RNA levels
• CAD toxicity a potential problem with celecoxib
• ASA? Mesalamine?
CD
38
Mo
lec
ule
s/c
ell
Pettersen, JV, 2011
CelecoxibPlacebo

Other Strategies to block Monocyte/Macrophage Activation?
• Combined CCR5/CCR2 blockade?– CCR5 inhibition increased immune activation, likely
indirectly through MØ activation
– CCR2 (MCP-1 receptor) blockade might overcome this effect?
• IDO inhibitors?– Prevent proliferative defects and allow for restoration
of Th17 cells
– Might interrupt vicious circle of microbial translocation and innate immune activation

Immunosuppressive Therapies
Suppression of Healthy Immune Reponses
DecreasedImmune Activation
The Good The Bad
TNFα inhibitors IL-6 inhibitors
CTLA-4 analogs IL-23/IL-12 inhibitors
Steroids Cyclosporine
Methotrexate

A Way Forward…• Target proximal causes of monocyte activation
• Small pilot trials to establish proof of principal– “Immunologic Non-Responders” have higher immune
activation and are at highest risk for disease
– Studying treated patients allows cleaner biologic inferences
– Need to thoroughly evaluate mechanistic pathways in vivo
• Advance promising agents to mid-range trials with surrogate markers of end-organ disease– Liver, renal, bone (BMD), cardiovascular (FMD)
• Advance promising/safe/scalable interventions to clinical endpoint trials





























