Embed Size (px)
Citation preview

Original Studies
Interventional Cardiology and Intracoronary Stents—AChanging Practice: Approved vs. Nonapproved Indications
David R. Holmes, Jr., 1* MD, Malcolm R. Bell, 1 MD, David R. Holmes 3 III, Peter B. Berger, 1 MD,John F. Bresnahan, 1 MD, LaVon N. Hammes, 1 Diane E. Grill, 2 MS, and Kirk N. Garratt, 1 MD
Our objective was to document change in stent usage in a single practice over time and tostudy ‘‘off-label’’ compared to Food and Drug Administration (FDA)-approved indications.Although only two intracoronary stents have been approved by the FDA, the relativelylimited approved indications do not account for the dramatic increase in stent implanta-tion. This increase has important implications for patient health care delivery. This studyof stent usage in a single center over a 36-mo period included all patients treated withcoronary stents at the Mayo Clinic from January 1993–December 1995, and evaluated therelative difference in frequency between ‘‘off-label’’ and FDA-approved indications forimplantation. During the 36-mo period of study, 3,614 interventional procedures weredone and one or more stents were placed in 25.4% of patients. The proportion of patientsreceiving stents increased throughout this time: during the first 6-mo period, stents wereplaced in 6.2% of procedures; during the last 6-mo period, stents were placed in 46.3% ofprocedures, an eightfold increase. During the final 6 mo, an unapproved device or anunapproved indication for an approved device constituted 59.4% of all stent procedures.In addition, use of the non-FDA-approved adjunctive treatment regimen without warfarinincreased from 2.9% in the first 6-mo period of observation to 82.7% in the last 6 mo. Theuse of stents increased strikingly over a 36-mo period, from 6% to 46% of all procedures.The majority of implantations were performed either for an ‘‘off-label’’ unapproved indica-tion or with an unapproved device. Cathet. Cardiovasc. Diagn. 40:133–138, 1997.r 1997 Wiley-Liss, Inc.
Key words: intracoronary stents; interventional cardiology; percutaneous angioplasty
INTRODUCTION
Intracoronary stents have had a major effect on thepractice of interventional cardiology. Two stents havebeen approved by the Food and Drug Administration(FDA), one for the treatment of abrupt or threatenedclosure (the Cook Flex Stenty), and one for the preven-tion of restenosis in de novo native coronary arterystenosis (the Palmaz-Schatzy coronary stent). These tworelatively limited approved indications do not account forthe dramatic increase in stent implantation procedures,estimated to be 50,000–100,000 in 1995 in the UnitedStates alone. It is apparent that many patients haveintracoronary stents placed for indications other thanthose approved by the FDA. This increased usage hasimportant implications for patient health care delivery,because some patients who receive stents require in-creased hospital stay for anticoagulation, supply costs forthe procedures are initially increased, and reimbursement
becomes an issue for nonapproved devices. This in-creased utilization also has potential legal ramificationsbecause of lack of FDA approval for many of the currentindications. The purposes of this paper are to documentthe change in stent usage in a single interventionalcardiology practice over time, and to study the relativefrequency of ‘‘off-label’’ compared with FDA-approvedindications.
From the 1Division of Cardiovascular Diseases and InternalMedicine, Mayo Clinic and Mayo Foundation, Rochester,Minnesota2Section of Biostatistics, Mayo Clinic and Mayo Foundation,Rochester, Minnesota3Mayo Graduate School, Mayo Clinic and Mayo Foundation,Rochester, Minnesota
*Correspondence to: Dr. David R. Holmes, Jr., Mayo Clinic, 200 FirstStreet SW, Rochester, MN 55905.
Received 26 September 1996; Revision accepted 2 October 1996
Catheterization and Cardiovascular Diagnosis 40:133–138 (1997)
r 1997 Wiley-Liss, Inc.

MATERIALS AND METHODS
All patients undergoing percutaneous coronary revascu-larization at the Mayo Clinic are entered into a data baseregistry study approved by our Institutional ReviewBoard. Patients undergo treatment after consultation withtheir individual referring physicians and after givinginformed consent. This study included all consecutivepatients being treated with percutaneous coronary inter-vention techniques from January 1993–December 1995.The patient demographics, coronary anatomy, and rea-sons for revascularization were prospectively entered.Four stents were used during the duration of this study:
the Gianturco-Roubiny stent (Cook, Inc., Bloomington,IN), the Palmaz-Schatz Johnson & Johnson Interven-tional Systems (JJIS) coronary stent (New Brunswick,NJ), the JJIS biliary stent, and the Wiktory stent(Medtronic, Inc., Minneapolis, MN). Two stents wereapproved for use by the FDA: the Cook Flex Stent 20-mmstent was approved for the treatment of acute or threat-ened closure (June 4, 1993), and the Johnson & JohnsonPalmaz-Schatz stent was approved for the prevention ofrestenosis in de novo native coronary arterial lesions(August 2, 1994). The remaining stents were used forunapproved indications (biliary stent), or were under aninvestigational device exemption protocol (Wiktor, Au-gust 28, 1991–April 25, 1994).The indication for stent placement was identified
prospectively and coded by the operator. For this study,each stent implantation was categorized by indication(Table I). As mentioned, only two stents were approvedfor use by the FDA during this time; for the remainder ofthe indications, several different types of stents wereused. Use of approved stents for unapproved indicationsor use of investigational stents depended on specificprotocols, device availability, and operator preference.Successful stent implantation was defined as successfuldelivery of the stent and no in-hospital deaths, Q-wavemyocardial infarctions, or coronary bypass graft surger-ies.
Patient Group Assignment
Patients were divided into eight groups, depending onindication for stent placement. Some were placed in morethan one group because of multiple indications.
Group A: Treatment of abrupt or threatened clo-sure using an approved stent.These patients receivedstents as treatment for acute or threatened closure compli-cating coronary intervention. Abrupt closure was definedas thrombolysis in myocardial infarction (TIMI) 0 or Iflow in a previously patent coronary vascular segment;threatened closure was defined as a reduction in TIMIflow by one category or more, usually associated withischemic symptoms or electrocardiographic abnormali-
ties. Currently, the only FDA-approved device for thisindication is the Cook Flex Stent.Group B: Prevention of restenosis in native coro-
nary arteries with primary (de novo) atheromatouslesions using an approved stent.These patients receivedstents electively in an effort to reduce the probability ofrestenosis. In this group, stents were planned regardlessof the initial results of intervention. For this indication,the only FDA-approved device is the Palmaz-Schatz JJIScoronary stent.Group C: Treatment of restenotic lesions.These
patients received stents as treatment of restenosis develop-ing after an initially successful intervention. All four stenttypes were used, even though none of them is approvedfor this indication.Group D: Treatment of vein graft disease.These
patients received stents electively to treat primary athero-matous or restenotic lesions in saphenous vein grafts.Although the Cook Flex Stent is approved for treatmentof failed angioplasty of saphenous vein grafts, no stent iscurrently approved for elective placement in vein graftlesions. All four types of stents were used, depending onspecific features of the vein graft disease.Group E: High-risk lesions. High-risk lesions were
defined by each operator after review of the baselinecoronary angiogram. High-risk lesions included, among
TABLE I. Indication for Stent Implantation, Stent Type, andStatus of Food and Drug Administration (FDA) Approval *
Group Indication Stent design
Indicationapprovedby FDA
A Treatment of abrupt orthreatened closure
Cook Flex StentTM Yes
B Prevention of restenosis inde novo native coronaryarterial stenosis
Palmaz-SchatzTM
coronary stentaYes
C Treatment of restenoticlesions
JJIS, Cook Flex StentTM,WiktorTM, biliary stenta
No
D Treatment of vein graftdisease
Biliary stent, WiktorTM,JJIS, Gianturco-RoubinTM
No
E Prophylactic treatment ofhigh-risk lesions
Biliary stent, WiktorTM,Palmaz-SchatzTM
coronary stent, CookFlex StentTM
No
F Treatment of suboptimalresults
WiktorTM, biliary stent No
G Treatment of abrupt orthreatened closure(other stents)
JJIS, WiktorTM, biliarystent
No
H Prevention of restenosis inde novo native coronaryarterial stenosis (otherstents)
Cook Flex StentTM,WiktorTM
No
*JJIS, Johnson & Johnson Interventional Systems.aFrom Johnson & Johnson Interventional Systems.
134 Holmes et al.

other characteristics, marked angulation, severe eccen-tric, large, irregular atheroma, or other properties thoughtto be associated with an increased risk of suboptimalresult or complications with conventional dilatation.Elective stent use was planned in the patients beforeangioplasty was begun, and the decision to place a stentdid not depend on the initial results of intervention. Nostent is currently approved for this indication.Group F: Treatment of suboptimal results. These
patients received stents in an elective but unplannedfashion for a suboptimal result after initial percutaneoustransluminal coronary angioplasty (PTCA). This wasconsidered present when a residual stenosis of$50%remained after treatment with an appropriately sizedballoon, laser, or atherectomy device. All four stents wereused.Group G: Treatment of abrupt or threatened clo-
sure with a nonapproved stent. The indication forstenting in this group is similar to that in group A, but thepatients were treated with Palmaz-Schatz coronary, Wik-tor, and biliary stents.Group H: Prevention of restenosis in primary
atheromatous (do novo) native coronary arterial steno-ses with unapproved stents.This group is similar togroup B, but consists of patients treated with Cook FlexStents. In some patients, lesions may have had more thanone indication for stent implantation, in which case theinitial indication was used as the primary indication forstent implantation.
Adjunctive Therapy
During the course of this study, the use of anticoagu-lant therapy to accompany stent implantation evolved.Both of the approved devices (the Cook Flex Stent andthe Palmaz-Schatz coronary stent) include labeling indica-tions specifying the use of intense anticoagulation (warfa-rin [Coumadin]) as well as antiplatelet regimens (dipyri-damole [Persantine] and aspirin). This anticoagulantregimen consisted of the use of these drugs for 1–3-moafter stent implantation. Given that the use of warfarin,aspirin, and dipyridamole is a labeling indication, allother regimens that did not specifically include warfarinwere also considered ‘‘off-label.’’The study period was divided into 6-mo intervals
beginning in January 1993 and extending through Decem-ber 1995. Within each period, the total number of stentsimplanted, the specific indication for stenting, and thetotal number of percutaneous interventions were deter-mined. In addition, the use of warfarin or other anticoagu-lant regimens was recorded.Statistical assessment was carried out byx2 testing for
discrete variables. Assessment of changes in indicationfor stenting over time was analyzed, using the Armitagelinear trend test for proportions [1].
RESULTS
From January 1993–December 1995, a total of 2,994patients underwent an attempted percutaneous interven-tion. In these patients, a total of 3,614 procedures wasperformed. In 689 patients (23%), at least one stent wasplaced; the average number of stents per patient was 1.55(range, 1–6).Demographics of patients can be seen in Table II; the
characteristics of patients treated in our laboratory with-out the use of coronary stents during the study period arealso displayed. Most patients were male. A history ofprior myocardial infarction was noted in 53.5% and59.2% of patients receiving a stent and those treatedwithout a stent, respectively. Most patients had unstableangina. The frequency of prior coronary bypass graftsurgery was greater in patients receiving a stent (29.9%)than in those not receiving one (19.6%;P, 0.001).The proportion of patients treated with coronary stents
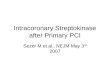
increased throughout the study period (Fig. 1). Stent usedoubled during the first two periods and then continued toincrease rapidly at each interval. During the last 12-moperiod, beginning on January 1, 1995, the number of pro-cedures receiving stents increased from 42.9% to 46.3%.The indications for stent implantation changed during
the period of observation (Table III). During the initialtime period (January 1993–June 1993), an approvedindication for implantation was used in 48.6% of allprocedures involving stents (group A). Treatment ofrestenotic lesions (37.1%), vein graft disease (31.4%),and suboptimal results of PTCA (25.7%) were alsofrequent indications for stent placement. The treatment ofabrupt closure by a device approved for that indication(i.e., the Cook Flex Stent) declined from 48.6% to 18.5%in the last 6-mo period (P5 0.001). A device approvedfor prevention of restenosis first became available for usein this institution in the period beginning July 1994.During that initial 6-mo period, only 8.4% of procedures
TABLE II. Characteristics of 2,962 Patients Receiving and NotReceiving Coronary Stents *
Stents (%) No stents (%) P
Patients 689 2,305Procedures 919 2,695Male 675 (73.5) 1,892 (70.2) 0.06Prior myocardial infarction 492 (53.5) 1,596 (59.2) 0.003Unstable angina 694 (87.5) 1,984 (90.2) 0.086History of congestive heart
failure 130 (14.2) 380 (14.1) 0.970Coronary artery disease 0.410One-vessel 280 (32.4) 819 (31.6)Two-vessel 354 (41.0) 1,018 (39.3)Three-vessel 230 (26.6) 755 (29.1)
Prior CABG 275 (29.9) 527 (19.6) ,0.001
*CABG, coronary artery bypass graft surgery.
Change in Intracoronary Stent Practice 135

had a stent implanted for prevention of restenosis as theindication. This indication increased slightly (P5 0.11)but still remained relatively low in the last observationperiod, during which only 14.9% of procedures had thatas a primary indication. The second most commonindication in the last period remained treatment of arestenotic lesion (23.8%), an unapproved indication, andthis was followed by treatment of an abrupt or threatenedclosure using a stent not approved for that indication(19.8%). During the final 6-mo period of observation,when stents were used in 46.3% of patients treated in thecatheterization laboratory, 59.4% of all stent procedureswere for non-FDA-approved indications.Irrespective of specific indications, success rates over
the entire 36 mo of observation were excellent, rangingfrom 90.7–98.0% (Table IV). Q-wave myocardial infarc-tion for the total patient cohort was 1.3%, ranging from0–2.6% of patients. Coronary bypass surgery was alsorequired infrequently: 2.9% for the entire group and only5.1% for patients with acute or threatened closure.All-cause in-hospital mortality varied among groups, butaveraged 2.1%.There were striking changes in the utilization of
intense anticoagulation regimens with warfarin. As canbe seen (Fig. 2), the number of procedures in whichwarfarin was not used increased from 2.9% during thefirst observation interval to 82.7% during the last 6 mo.
DISCUSSION
This paper documents the marked change in thepractice pattern of stent implantation at a tertiary carecenter with a large interventional cardiology practice.Over a 36-mo period beginning in January 1993 andending in December 1995, the use of stents in interven-tional cases increased from 6.2% of cases up to 46.3% ofall procedures, an eightfold increase. Most cases involvedeither an unapproved device or an unapproved indication;
during the final 6-mo period, an unapproved device orunapproved indication constituted 59.4% of all stentimplantations. In addition, the use of the non-FDA-approved adjunctive treatment regimen without warfarinincreased from 2.9% in the first 6-mo period to 82.7% inthe last 6-mo period.The issues of approved vs. ‘‘off-label’’ indications and
the use of approved vs. nonapproved devices havereceived considerable attention in cardiovascular disease.Concern has been raised about the discrepancy and lagbetween the development of new technology and itsapproval by regulatory agencies. The use of approvedstents for treatment of ‘‘off-label’’ indications, or the useof unapproved stents, is associated with multiple poten-tial problems, including legal ramifications, which maybe substantial if complications occur, and reimbursementissues. The latter have come under increasing scrutiny bythe federal government and are now part of an investiga-tion by the Office of the Inspector General in Medicarepatients. The potential benefits to patients are substantial,however, because newer technology can be made avail-able; for example, biliary stents can be used to treat verylarge vein grafts with focal stenoses, avoiding the needfor repeat surgery [2]. Without randomized clinical trials,it is unclear whether such newer technology improvesoutcome. In coronary stenting, a large number of observa-tional studies in a variety of patient and angiographicsubsets, e.g., vein graft disease or treatment of suboptimalresults of conventional PTCA, have documented that theoutcome does indeed appear to be improved over that inhistorical cohorts of patients [3–13]. These observationalstudies, however, do not provide the conclusive scientificevidence of efficacy that can be demonstrated in rigor-ously controlled randomized trials.The use of stents has dramatically changed the practice
of interventional cardiology. This change has been mostmarked since the documentation by two randomized trialsthat stents used for de novo lesions in native coronaryarteries can decrease angiographic restenosis and moder-ately decrease clinical restenosis (the Stent RestenosisStudy [STRESS] and the Balloon Expandable StentImplantation study [BENESTENT]) [14,15]. The translat-ability from a reduction in restenosis with stents placedfor de novo native coronary lesions to other angiographicsubsets is not certain. Initial information suggests thattreatment of restenotic lesions with stents may not beassociated with markedly improved outcome comparedwith conventional PTCA, although more data fromrandomized trials will be required [11,12]. It is known,however, that the final angiographic stenosis is the mostimportant determinant of long-term outcome and thatoptimal stent implantation can yield a residual stenosis of,10% [16,17]. The increase in stent implantation hasalso been the result of the observational data that stents
Fig. 1. Proportion of interventional cases receiving stents overthe time of the study.
136 Holmes et al.

can effectively decrease the complications of acute orthreatened closure after conventional dilatation [7,8].Stent practice based on these observations and in tworandomized trials, however, did not account for the greatincrease in stent usage at this single institution. Instead,the increase was related more to the application ofapproved devices for nonapproved indications, e.g., treat-ment of restenotic lesions or treatment of suboptimalresults of PTCA, and of nonapproved devices, e.g., theWiktory stent, which currently account for 59.4% of allstent procedures.
The success rate for this entire 36-mo experience ofconsecutive patients was excellent, at 93.7%. Although itvaried among the different indications, the numbers ineach group and the variability were limited. The overallincidences of Q-wave myocardial infarction (1.3%), needfor coronary bypass surgery (2.9%), vascular surgery(2.5%), and in-hospital all-cause mortality (2.1%) werelow, irrespective of the indication for stent implantation.One of the most dramatic changes in practice was the
use of nonapproved adjunctive drug regimens; the num-bers of patients treated with ‘‘off-label’’ drug regimensincreased significantly. In the most recent 6-mo cohort ofpatients, 82.7% were treated without warfarin, whereas inthe initial 6-mo cohort, only 2.9% were treated withoutwarfarin. This change has been documented at otherinstitutions [18].This dramatic change in stent use has important
implications. In-hospital charges associated with stentsare increased compared with those for conventionalballoon angioplasty [19–21]. At present, this issue is alsoaggravated by the fact that there is no specific diagnosis-related group for stent implantation, although in thefuture this may change. In addition, as previously docu-mented, the translatability from approved indicationsubsets of patients to nonapproved indication subsets ofpatients in terms of short- and long-term outcomes is lesscertain. Outcomes in multiple published series, however,
TABLE III. Number of Procedures With Each Indication for Stenting by Time Period †
January 1993–June 1993 (%)
July 1993–December 1993 (%)
January 1994–June 1994 (%)
July 1994–December 1994 (%)
January 1995–June 1995 (%)
July 1995–December 1995 (%) P*
ApprovedGroup A 17 (48.6) 31 (44.9) 34 (40.0) 59 (35.1) 77 (28.3) 56 (18.5) ,0.001Group B 13 (8.4) 44 (16.2) 45 (14.9) 0.115
UnapprovedGroup C 13 (37.1) 34 (49.3) 32 (37.7) 60 (38.7) 65 (23.9) 72 (23.8) ,0.001Group D 11 (36.4) 14 (20.3) 24 (28.2) 34 (21.9) 40 (14.7) 45 (14.9) ,0.001Group E 1 (2.9) 3 (4.4) 5 (5.9) 9 (5.8) 23 (8.5) 53 (17.5) ,0.001Group F 9 (25.7) 9 (13.0) 9 (10.6) 24 (15.5) 53 (19.5) 58 (19.1) 0.268Group G 3 (8.6) 8 (11.6) 6 (7.1) 9 (5.8) 44 (16.2) 60 (19.8) ,0.001Group H 1 (1.5) 5 (5.1) 11 (7.1) 13 (4.8) 21 (6.9) 0.235
Total number of procedures 35 69 85 155 272 303
*Statistical assessment used the Armitage linear trend test for proportions [1].†Patients often had more than one indication for stenting, so that the total number of indications is greater than the total number of procedures.
TABLE IV. In-Hospital Outcome for Patient Groups Treated *
Totalcohort
Group
A B C D E F G H
Number 919 273 103 276 168 93 160 129 51Success (%) 93.7 91.2 97.1 94.9 94.6 93.5 94.4 90.7 98.0Q-wave MI (%) 1.3 2.6 1.0 0.7 1.2 1.1 0.6 2.3 0Any CABG (%) 2.9 5.1 1.0 3.3 0 1.1 1.9 7.0 0Vascular surgery (%) 2.5 4.4 4.9 2.9 3.0 4.3 1.3 2.3 0Death (%) 2.1 1.5 0 1.1 3.6 5.4 3.1 2.3 0
*CABG, coronary artery bypass graft; MI, myocardial infarction.
Fig. 2. Change in stent practice, with increasing percentage ofpatients not treated with warfarin.
Change in Intracoronary Stent Practice 137

appear to show improved longer-term success. Thesenonapproved indications remain problematic for third-party payers and the federal government, who are inter-ested in ‘‘proven’’ treatment approaches.Without random-ized clinical trials, proven clinical benefit is substantiallyharder to document.
CONCLUSIONS
Use of intracoronary stents strikingly increased in a36-mo period, from 6% to 46% of all procedures. Mostimplantations were performed either for an ‘‘off-label’’unapproved indication or with an unapproved device. Inaddition, in the last 6 mo of observation, 82.7% ofpatients were treated without warfarin, an unapproved‘‘off-label’’ practice.
REFERENCES
1. Armitage P: Test for linear trend in proportions and frequencies.Biometrics 11:375–386, 1955.
2. Wong SC, Popma JJ, Pichard AD, et al.: Comparison of clinicaland angiographic outcomes after saphenous vein graft angioplastyusing coronary versus ‘‘biliary’’ tubular slotted stents. Circulation91:339–350, 1995.
3. Strauss BH, Serruys PW, Bertrand ME, et al.: Quantitativeangiographic follow-up of the coronary Wallstent in native vesselsand bypass grafts (European experience—March 1986 to March1990). Am J Cardiol 69:475–481, 1992.
4. Schatz RA, Baim DS, Lean M, et al.: Clinical experience with thePalmaz-Schatz coronary stent. Initial results of a multicenter study.Circulation 83:148–161, 1991.
5. Carrozza JP Jr, Kuntz RE, Levine MJ, et al.: Angiographic andclinical outcome of intracoronary stenting: Immediate and long-term results from a large single-center experience. J Am CollCardiol 20:328–337, 1992.
6. Savage MP, Fischman DL, Schatz RA, et al.: Long-term angio-graphic and clinical outcome after implantation of a balloon-expandable stent in the native coronary circulation: Palmaz-SchatzStent Study Group. J Am Coll Cardiol 24:1207–1212, 1994.
7. Roubin GS, Cannon AD, Agrawal SK, et al.: Intracoronarystenting for acute and threatened closure complicating percutane-ous transluminal coronary angioplasty. Circulation 85:916–927,1992.
8. Herrmann HC, Buchbinder M, Clemen MW, et al.: Emergent useof balloon-expandable coronary artery stenting for failed percuta-neous transluminal coronary angioplasty. Circulation 86:812–819,1992.
9. Sutton JM, Ellis SG, Roubin GS, et al.: Major clinical events aftercoronary stenting. The multicenter registry of acute and electiveGianturco-Roubin stent placement. The Gianturco-Roubin Intra-coronary Stent Investigator Group. Circulation 89:1126–1137,1994.
10. Dean LS, Roubin GS, Lembo NJ, et al.: Initial experience andin-hospital outcome in patients receiving the Cook flexible coilintra-coronary stent. A report from the New Approaches toCoronary Intervention Registry. Circulation 86:373, 1992.
11. Fenton SH, Fischman DL, Savage MP, et al.: Long-term angio-graphic and clinical outcome after implantation of balloon-expandable stents in aortocoronary saphenous vein grafts. Am JCardiol 74:1187–1191, 1994.
12. Piana RN, Moscucci M, Cohen DJ, et al.: Palmaz-Schatz stentingfor treatment of focal vein graft stenosis: Immediate results andlong-term outcome. J Am Coll Cardiol 23:1296–1304, 1994.
13. Maiello L, Colombo A, Gianrossi R, Goldenberg S, Martini G,Finci L: Favourable results of treatment of narrowed saphenousvein grafts with Palmaz-Schatz stent implantation. Eur Heart J15:1212–1216, 1994.
14. Fischman DL, Leon MB, Baim DS, et al.: A randomized compari-son of coronary-stent placement and balloon angioplasty in thetreatment of coronary artery disease. Stent Restenosis StudyInvestigators. N Engl J Med 331:496–501, 1994.
15. Serruys PW, De Jaegere P, Kiemeneij F, et al.: A comparison ofballoon-expandable-stent implantation with balloon angioplasty inpatients with coronary artery disease. N Engl J Med 331:489–495,1994.
16. Kuntz RE, Safian RD, Carrozza JP, Fishman RF, Mansour M,Baim DS: The importance of acute luminal diameter in determin-ing restenosis after coronary atherectomy or stenting. Circulation86:1827–1835, 1992.
17. Kuntz RE, Safian RD, Levine MJ, Reis GJ, Diver DJ, Baim DS:Novel approach to the analysis of restenosis after the use of threenew coronary devices. J Am Coll Cardiol 19:1493–1499, 1992.
18. Colombo A, Hall P, Nakamura S, et al.: Intracoronary stentingwithout anticoagulation accomplished with intravascular ultra-sound guidance. Circulation 91:1676–1688, 1995.
19. Dick RJ, Popma JJ, Muller DW, Burek KA, Topol EJ: In-hospitalcosts associated with new percutaneous devices. Am J Cardiol68:879–885, 1995.
20. Cohen DJ, Krumholz HM, Sukin CA, et al.: In-hospital andone-year economic outcomes after coronary stenting or balloonangioplasty—Results from a randomized clinical trial. Circulation92:2480–2487, 1995.
21. Cohen DJ, Breall JA, Ho KKL, et al.: The economics of electivecoronary revascularization: Comparison of costs and charges forconventional angioplasty, directional atherectomy, stenting andbypass surgery. J Am Coll Cardiol 22:1052–1059, 1993.
138 Holmes et al.