Embed Size (px)
Citation preview
Intersectoral Nutrition Strategy Sindh
Striving for Intersectoral
solution of Malnutrition
to have Healthy Children and
Mother


Careful management of the well-being of population is the essence of good government. Health is always a
provincial priority and government’s prime responsibility. Nutrition is an integral part of social sector development and improvement in its indicators would promote the much desired economic development through a healthy population.
Targets of MDGs strongly warrant that we must take some strategic steps and make efforts towards improved results. Therefore Planning and Development department has embarked on a historical achievement of formulating an Intersectoral Nutrition strategy for the Province of Sindh involving all the concerned departments, academia, Civil Society and Development Partners, a milestone in itself. We all know that both resources and skill are there, but what is lacking is a whole hearted effort. There is a need for proper utilization of all that is available, by competent and dedicated people.
Government of Sindh will provide full administrative support for implementation of this Strategy. The aim would be improvement of nutrition and socio- economic status of the people of province. Simply put, better nutrition advances human development, and poor nutrition constrains it. The former is obvious choice.
I am assured that Intersectoral Nutrition Strategy for Sindh not only provides a clear direction for all stakeholders and serves as a framework for consensus and convergence but also provides basis for
sustainable results and actions to address malnutrition.
I hope this Strategy will contribute to the socio economic & health status of poor masses of province. It should provide a base line to build upon leading towards progress. I also wish success to all the program personnel in the achievement of the goals set out for them in this effort.
Syed Qaim Ali ShahChief Minister
Mr. Arif Ahmad KhanAdditional Chief SecretaryPlanning & Development
It is a recognized fact that population of Sindh province especially women & children suffer from some of the
highest rates of malnutrition in the country. There is also an undeniable link between malnutrition and human development.
In the context of malnutrition the underlying causes are the prevalent poverty in the Sindh (about 31% of population lives below the poverty line), landlessness, food insecurity, gender imbalances and level of woman empowerment. These factors place Sindh at a serious disadvantage to meet the Millennium Development Goals (MDGs).
The National Nutrition Survey (NNS) 2011 reveals alarming malnutrition rates in Sindh. Natural disasters coupled with insufficient public sector investment; and limited awareness among individuals, families, policy makers and communities has a major impact on the current nutritional status. Responding to malnutrition requires a multisectoral approach to tackle these short comings.
An issue like this needs a very precise intersectoral strategy to arrest the malnutrition situation in the province. Therefore, development of a robust strategic plan with involvement and recognition from all line departments is a major challenge for Government. We appreciate the efforts of UNICEF for its support in formulation of this vital document together with the hard work put in by relevant officers of Planning & Development Department.
This Strategy has been formulated after a comprehensive and participatory approach.
Technical inputs have been obtained from all stakeholders i.e. the departments of health, population welfare, education, agriculture, food, livestock, women development and social welfare. Development partners, academia and civil society organizations have also made significant contribution.
I expect that the Government of Sindh’s policy makers and executives would benefit from this document and undertake rational and practical implementation plans to achieve the intended objectives.

Ms Rehana Ghulam Ali MemonSecretary (Development)
Malnutrition is an obstacle to human development, and without much more elective interventions it will
continue to inflict irreversible damage to individuals, early in life and large economic and social losses on countries for years to come.
Although, MDGs gave us direction with sequential milestones, for improving significant demographic, health and social indicators, yet for want of allocative efficiency and smart planning, we are terribly far away from reaching our targets to promote sustainable development and protecting the most vulnerable and disadvantaged segments from the disturbing effects. Therefore, it is strongly warranted that we must take more determined steps to achieve the targets of MDGs.
Evidence shows that fragmented actions, governance, financing and weak capacities are the core issues in Public Sector. Increasing budgetary allocations have not borne the desired outcomes unless we have clear strategic direction to trounce these issues.
The Intersectoral Nutrition Strategy has been formulated, based on Policy Guidance Notes prepared earlier. The hard work and strong commitment of Planning and Development Officials and focal person on nutrition made this incredible task tangible.
This strategy on nutrition has been developed through a consultative process by the Steering Committee and Technical Working Group on Nutrition, which includes representatives from line departments, academia, civil society and
development partners under the lead role of Planning and Development Department and aegis of UNICEF.
Intersectoral Nutrition Strategy proposes approaches, to address the major nutrition problems in the province. It aims to support in establishing and implementing action in accordance with current situation and resources.
This strategy emphasizes support for the most vulnerable groups, and alleviation of poverty and hunger, the root causes of malnutrition. Every effort has been made to direct the focus of all stakeholders for results on ground; particularly in health and nutrition system strengthening; and to support the leadership of government to achieve the Millennium Development Goals.
Intersectoral Nutritional Strategy For Sindh
Table of contentsAcronyms .............................................................................................................................................0
Overview
Introduction ...........................................................................................................................................1
Background information........................................................................................................................ 1
Overview of the nutrition status in Sindh .............................................................................................. 2
Review of the past initiatives ................................................................................................................ 4
Causality framework .............................................................................................................................5
Intervention framework ......................................................................................................................... 6
Goal of the INSS...................................................................................................................................8
Operational objectives .......................................................................................................................... 8
Underlying assumptions ....................................................................................................................... 8
The guiding principles........................................................................................................................... 8
Target group .......................................................................................................................................10
Rationale for the investment in nutrition ............................................................................................. 11
Organization analysis ........................................................................................................................ 11
Oversight coordination, monitoring and evaluation ............................................................................ 19
AnnexuresAnnexure one: Logical framework presentation .................................................................................. i
Annexure two: Sectoral recommendations
Health Sector ........................................................................................................................................ ii
Education sector .................................................................................................................................. ix
Agriculture/Fisheries/Livestocks .........................................................................................................xiii
WASH and PHED ...............................................................................................................................xix
Cross Sectoral RecommendationCSO .................................................................................................................................................. xxiii
BISP ..................................................................................................................................................xxv
Women Development Department ...................................................................................................xxix
Annexure three: maps of high risk districts for malnutrition ........................................................... xxxii
AcronymsADP Annual Development ProgramBCC Behavior Change CommunicationBHU Basic Health UnitCBA Child Bearing AgeCBO Community Based OrganizationCCT Conditional Cash TransferCHWs Community Health WorkersCMAM Community-based Management of Acute MalnutritionCMWs Community MidwivesDHIS District Health Information SystemDOH Department of HealthEPI Expanded Program on ImmunizationFANS Flood Affected Nutrition SurveyGAIN Global Alliance for Improved NutritionGAM General Acute MalnutritionGDP Gross Domestic ProductGoS Government of SindIDA Iron Deficiency Anemia IMR Infant Mortality RateIYCF Infant and Young Child FeedingLBW Low Birth WeightLHW Lady Health WorkerM&E Monitoring and EvaluationMAM Moderately Acute MalnutritionMI Micronutrient InitiativeMNCH Maternal, Neonatal and Child HealthMOU Memorandum of UnderstandingMTDF Medium Term Development FrameworkNGO Non-Governmental OrganizationNIDs National Immunization DaysNNS National Nutrition SurveyNPS Nutrition Program for SindNWFFP National Wheat Flour Fortification ProjectPC-1 Planning Commission-pro forma 1PDHS Pakistan Demographic and Health SurveyPHC Primary Health CarePLW Pregnant and Lactating WomenPSLSM Pakistan Social and Living Standards MeasurementRUTF Ready to Use Therapeutic FoodSAM Severely Acute MalnutritionSC Stabilization CenterSFP Supplementary Feeding ProgramTORs Terms of ReferencesWFP World Food ProgramWHO World Health Organization***
0
1
Sindh – Intersectoral Nutritional Strategy1. IntroductionNational nutritional survey has highlighted alarmingly high level of malnutrition in Pakistan. One fourth of the population (24%) is undernourished and two out of every five children malnourished. The national stunting prevalence among children under five is 43.7%1,2. The findings indicate that Pakistan has the second highest number of severely wasted children next to India3. According to the most recent esti-mates by the United Nations Food and Agriculture Organization (FAO) 37.5 million people in Pakistan are not receiving proper nourishment4.
Nutritional status has huge implications at individual and societal level. At individual level, poor nutrition affects health and survival, physical and cognitive functioning, and work capacity thus decreasing the income of households and national economy. According to the United Nations Standing Committee on Nutrition’s5 (SCN) fifth report on the world nutrition situation, just three types of malnutrition are respon-sible for 3-4 percent of GDP loss in Pakistan in any given year.
Under-nutrition has huge implications for women and children as is evident from the high rates of infant and maternal mortality which is reported as 87 per 1000 live births for infants (Sindh MICS 2009-10.) and 314 maternal deaths per 100,000 live births (Sindh PDHS 2006-07) for mothers in Sindh.
In order to respond to this grave and urgent situation, Government of Pakistan and developmental partners have committed to address the issue of malnutrition on war footing. Following document is the output of the long series of dialogues and consultations and inputs by various partners.
2. Sindh – Background InformationSindh is the 2nd largest province of Pakistan and is divided into 23 districts, 113 talukas/ tehsils and 1,703 Union Councils with current estimated population of 43 million in 2011 (Sindh HSS Report). Sindh’s growth rate is highest in the country6. Population demographic analysis indicates 15% of the population under five years of age. Sindh’s contribution to the national economy has been substantial – between 30 and 33 percentage of the country’s GDP with a population that is nearly 50% urban. The province’s GDP per capita is roughly three times that of the country as a whole. The rural population of Sindh is scattered over large distances and infrastructure is poor. Rural households face livelihood issues due to decreasing agricultural productivity and heavy devasta-tion caused by recent floods7.
According to the Benazir Income Support Program (BISP), 45.7 percent people (Approximately 82 mil-lion) in Pakistan are living below the poverty line. And out of these 45.7 percent people 36.5 percent (Approximately 65 million) of the total population are living in chronic poverty8. The rural-urban poverty
1 All data is from the Pakistan National Nutrition Survey (NSS), 2011 unless otherwise indicated. The 2011 survey is the first to provide repre-sentative data for each of the provinces.2 By comparison, India = 48%; Nepal = 45%; Bangladesh = 43%; D.R. Congo = 43%; Sri Lanka = 17%3 Policy guidance notes Sindh4 http://www.tbl.com.pk/malnutrition-in-pakistan-the-hidden-hunger/5 United Nations Standing Committee on Nutrition (SCN). Fifth Report on the World Nutrition Situation: Nutrition for Improved Development Outcomes, March 2004.6 Pakistan Economic Survey of 2011-12 7 TRF (2011). Situational analysis for post devolution health sector strategy of Sindh province. November, quoted in Road Map for Health systems strengthening in Sindh province Province to support USAID/Pakistan’s RMNCH programs in Pakistan. DRAFT, October 2012, USAID8 Adnan M.Crossing the poverty line. “The News” Sunday, 10th June 2012, Islamabad
2
gap in Sindh is high compared to the other provinces. Women and children (out-of-school/work), dis-abled, and the elderly, are the most vulnerable groups.
Sindh has a large network of primary, secondary, diagnostic, pharmacy and ambulance services being provided in many parts in collaboration with private sector. Around 22% of public sector offers tertiary care services to low income groups. Issues of staff retention particularly of female staff, frequent drug stock-outs and poor maintenance of building and equipment are major challenges faced by the public health sector. MNCH, LHW program, EPI and other vertical programs operate under the rubric of the Department of Health. Population welfare department is separate but aims to work very closely with the health sector. The districts that present most challenging health profiles are Thatta, Tharpakar, Jacoba-bad, Badin, Mirpurkhas, Kambar and Kashmore. Karachi, Hyderabad and Sukkur are comparatively the most developed districts while other districts of Sindh are middle ranking. Almost one third of mothers in Sindh have had six or more pregnancies. Sindh has a very low literacy rate of 46%9 with female literacy level of only 12%10. 73% of urban compared to 50% rural have ever attended school.
NNS indicates that a very small proportion (32%) of the population in Sindh have access to pipe water. In addition, according to NNS, 85 percent respondents stated that they “never treat water in any way to make it safer for drinking”. The situation in rural area is even more alarming where 92% population never treated water. One-third of the population of Pakistan defecates openly in the fields. In rural Sindh, the people are poor and lack sanitation facilities. .According to PSLM 2010-2011, 62% house-hold in Sindh have flush toilet facility compared to 66% national. There are a lot of disparities with in the districts (7% for Tharparkar Vs. 97% for Karachi).
Women in Sindh have low social status as evident from the poor education and literacy indicators in females (46% females compared to 71% for males).The society is patriarchal with fathers and brothers responsible for decision regarding women’s health, marriage and family size. It is a cultural norm to serve meal to men first (NNS 2011).
Sindh has successful models of public private partnership for health care delivery such as People’s Primary Health Care Initiative which is now operational in 21 districts of Sindh. The Basic Health Units, Dispensaries, Mother and Child Healthcare Centers have been transferred to PPHI, Sindh. PPHI is now looking after 1137 facilities which include 647 BHUs, 9 RHCs, 34 MCHs, 435 dispensaries and 12 others (Unani Shifa Khana)11.
3. Overview Of Nutrition Status In Sindh National Nutrition Survey 2011 highlights that, directly or indirectly, “the concurrent vicious life cycle of malnutrition contributes to almost 35 per cent of all under-five deaths in the country”. It argues that over the past 20 years, “there has been little change in the prevalence of malnutrition in the population”, despite greater food availability and an overall increase in caloric intake per capita12.
Analysis of NNS 2011 indicates that Sindh is the most food deprived province of Pakistan where only 28 percent households are food secure (21.1% food insecure without hunger, 33.8% food insecure with moderate hunger and 16.8% food insecure with severe hunger).
The survey indicates that unlike many other areas in South Asia, there are no significant differences in the nutritional status of young girls and boys. . Problems emerge for females however in adolescence and adulthood. Only 52.5% of women in Sindh have body mass index which is normal, while 23.7% are underweight and 24.0% are overweight or obese.
9 Pakistan economic survey 201110 Policy analysis of education in Sindh, UNESCO, 201111 Monthly bulletin PPHI Sindh, monthy performance review, Dec 2012 , vol 1 , issue 3, pg # 1 and 1012 Situation analysis of children and women in Pakistan, 2012
3
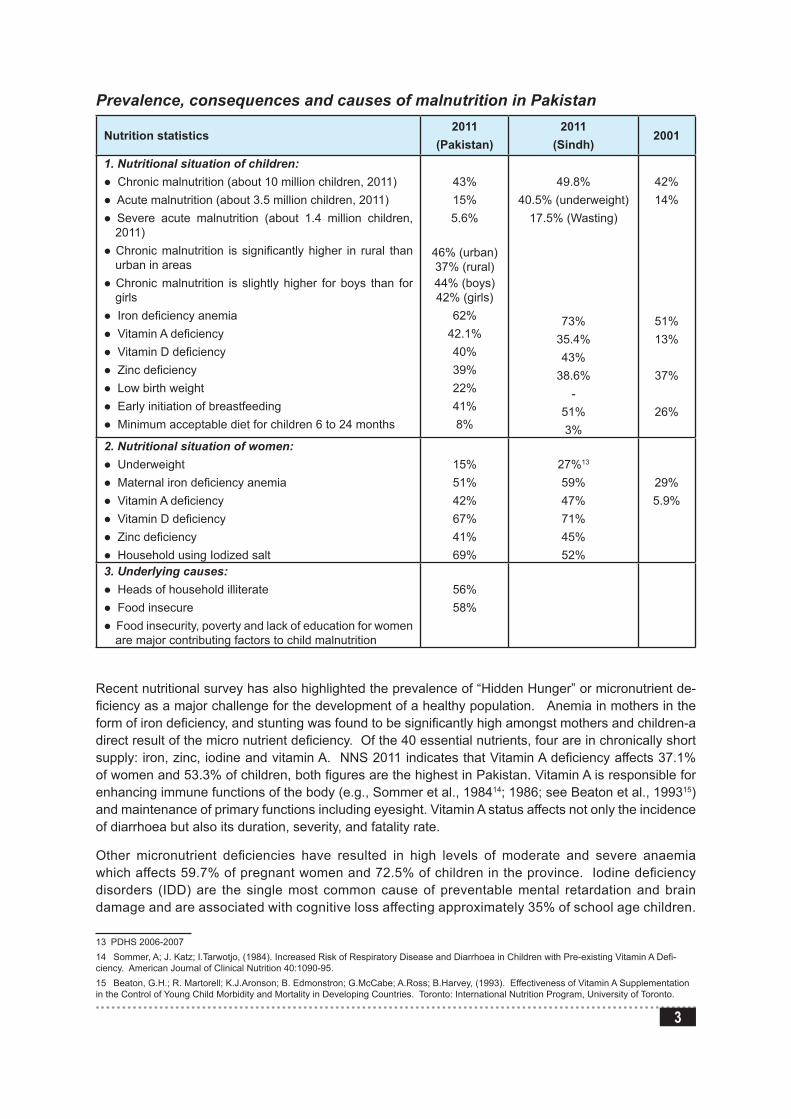
Prevalence, consequences and causes of malnutrition in Pakistan
Nutrition statistics2011
(Pakistan)2011
(Sindh)2001
1. Nutritional situation of children:l Chronic malnutrition (about 10 million children, 2011)l Acute malnutrition (about 3.5 million children, 2011)l Severe acute malnutrition (about 1.4 million children,
2011)l Chronic malnutrition is significantly higher in rural than
urban in areasl Chronic malnutrition is slightly higher for boys than for
girlsl Iron deficiency anemial Vitamin A deficiencyl Vitamin D deficiencyl Zinc deficiencyl Low birth weightl Early initiation of breastfeedingl Minimum acceptable diet for children 6 to 24 months
43%15%5.6%
46% (urban) 37% (rural)44% (boys) 42% (girls)
62%42.1%40%39%22%41%8%
49.8%40.5% (underweight)
17.5% (Wasting)
73%35.4%43%
38.6%-
51%3%
42%14%
51%13%
37%
26%
2. Nutritional situation of women:l Underweightl Maternal iron deficiency anemial Vitamin A deficiencyl Vitamin D deficiencyl Zinc deficiencyl Household using Iodized salt
15%51%42%67%41%69%
27%13
59%47%71%45%52%
29%5.9%
3. Underlying causes:l Heads of household illiteratel Food insecurel Food insecurity, poverty and lack of education for women
are major contributing factors to child malnutrition
56%58%
13
Recent nutritional survey has also highlighted the prevalence of “Hidden Hunger” or micronutrient de-ficiency as a major challenge for the development of a healthy population. Anemia in mothers in the form of iron deficiency, and stunting was found to be significantly high amongst mothers and children-a direct result of the micro nutrient deficiency. Of the 40 essential nutrients, four are in chronically short supply: iron, zinc, iodine and vitamin A. NNS 2011 indicates that Vitamin A deficiency affects 37.1% of women and 53.3% of children, both figures are the highest in Pakistan. Vitamin A is responsible for enhancing immune functions of the body (e.g., Sommer et al., 198414; 1986; see Beaton et al., 199315) and maintenance of primary functions including eyesight. Vitamin A status affects not only the incidence of diarrhoea but also its duration, severity, and fatality rate.
Other micronutrient deficiencies have resulted in high levels of moderate and severe anaemia which affects 59.7% of pregnant women and 72.5% of children in the province. Iodine deficiency disorders (IDD) are the single most common cause of preventable mental retardation and brain damage and are associated with cognitive loss affecting approximately 35% of school age children.
13 PDHS 2006-200714 Sommer, A; J. Katz; I.Tarwotjo, (1984). Increased Risk of Respiratory Disease and Diarrhoea in Children with Pre-existing Vitamin A Defi-ciency. American Journal of Clinical Nutrition 40:1090-95.15 Beaton, G.H.; R. Martorell; K.J.Aronson; B. Edmonstron; G.McCabe; A.Ross; B.Harvey, (1993). Effectiveness of Vitamin A Supplementation in the Control of Young Child Morbidity and Mortality in Developing Countries. Toronto: International Nutrition Program, University of Toronto.

4
Only 52% of the households use iodized salt in the province. The survey also underscored the fact that although stunting is significantly higher in food insecure households; it is not uncommon in food secure households.
Review Of The Past InitiativesReview of the past initiatives indicates a general tendency towards developing “nutrition specific” interven-tion mostly in health sector indicating the general perception that nutrition is the mandate of the health sector. Review also indicates that within the health sector, primary focus has been on implementing CMAM activities which is probably in response to onslaught of cases that ascended to surface after flood that struck the Sindh province. On the prevention and promotion side, health sector has been active in implementing IYCF and preventing micro-nutrient deficiency through initiatives like Wheat Flour Fortification and Universal salt iodization. 125 Wheat Flour Fortification plants were successfully built. In the absence of legislation to restrict sale of unfortified products in the markets, the micronutrient fortification initiatives always faced prob-lem of sustainability. Health sector has successfully integrated nutrition and breast feeding counseling in the curriculum of LHWs and CMWs; these components would however benefit from more focus on competency building for managing the cases of malnutrition and problems faced during breast feeding. Models of baby friendly hospitals have also been instituted but these also failed to get institutionalized in the absence of leg-islation. Analysis of MIS reports indicated that it is mostly department specific such as nutrition, MNCH, EPI. There is a tremendous opportunity to harmonize the information to develop a comprehensive understanding of the nutrition situation In Sindh.
Malnutrition is a multidimensional issue. The recognition of the role of other sectors has been nebulous and hardly any model of inter-sectoral action is available for analysis. Hence, while social protection packages such as Bailtul Maal and Benazir income support program have been introduced, opportunities to use its database to reach out to the ultra-poor population with social development interventions have not been exploited; while agriculture sector showed remarkable success in increasing agriculture produce, it did not delve into food security issues or invested significant efforts in exploring ways to augment bio-diversity and bio-availability of the crops. Similarly, harmful effects of bio-engineered seeds and chemical pesticide and its impact on the nutrient quality have not been raised as a concern to the extent needed. Similarly, in the livestock sector, focus has been on producing more milk or meat without enough understanding and hence control measure to discourage use of hormones did not receive much attention.
Inter-sectoral action is critical to addressing nutritional problem but there is a serious dearth of any suc-cessful inter-sectoral initiative even for demonstration or piloting purpose in the country. In the social protection arena, the country has introduced cash transfers to families through BISP but the opportuni-ties to synchronize this activity with other sectors have not been fully exploited. TAWANA – a model of school feeding programs strived to adopt inter-sectoral approach by striking a tripartite agreement between ministry of social welfare, ministry of education and ministry of women development. TAWANA however faced a lot of problems and failed to achieve its desired outcomes. Analysis of the underlying reasons for this tendency to work vertically can be categorized into the following:
a) Vertical nature of the program funding that lacked any incentive to work horizontally in inter-sectoral approach;
b) Lack of vertical integration as a result of centrally controlled organizational structure;c) Lack of political will to establish coordinating bodies to provide space for inter-sectoral action;d) Lack of donor harmonization that resulted in fragmentation of initiatives;e) Lack of human resources capacity to unfold the technical aspect of the issue and build capacity to
address the issue using inter-sectoral approach.
INSS has strived to learn from the past experience within the country and international experience documented in “scaling up nutrition intervention”. A series of consultation and inputs have guided the INSS developmental proves.
5
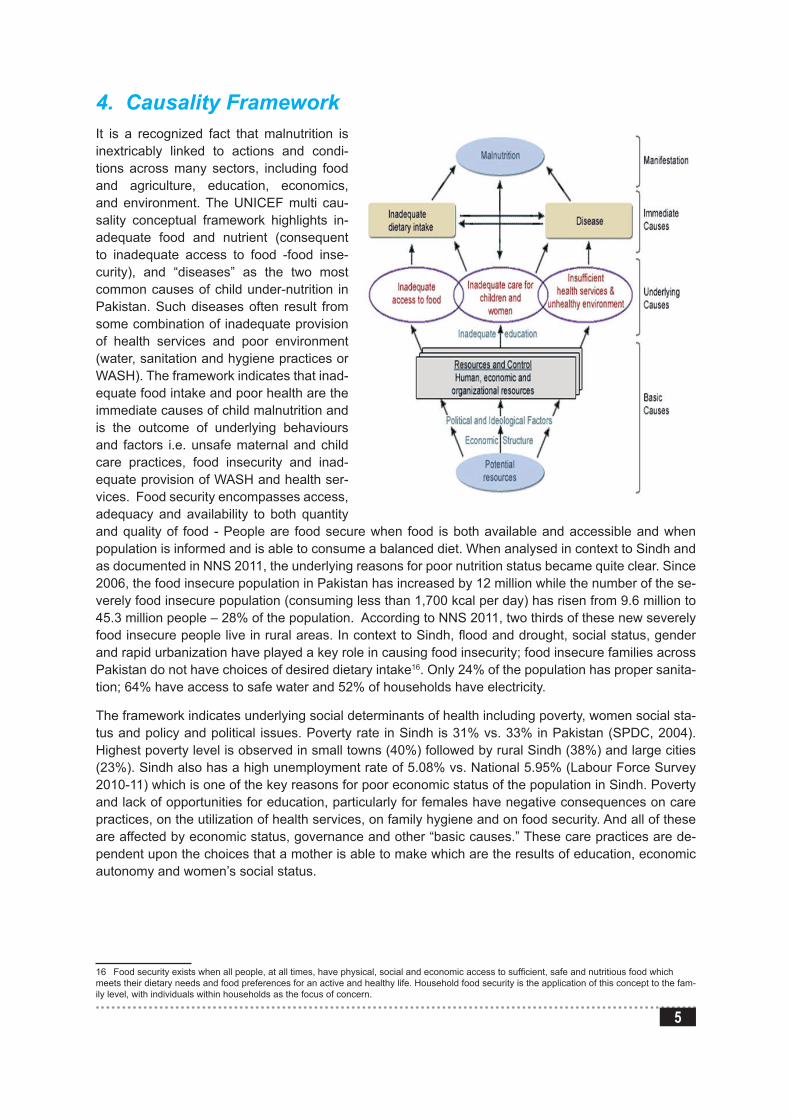
4. Causality Framework It is a recognized fact that malnutrition is inextricably linked to actions and condi-tions across many sectors, including food and agriculture, education, economics, and environment. The UNICEF multi cau-sality conceptual framework highlights in-adequate food and nutrient (consequent to inadequate access to food -food inse-curity), and “diseases” as the two most common causes of child under-nutrition in Pakistan. Such diseases often result from some combination of inadequate provision of health services and poor environment (water, sanitation and hygiene practices or WASH). The framework indicates that inad-equate food intake and poor health are the immediate causes of child malnutrition and is the outcome of underlying behaviours and factors i.e. unsafe maternal and child care practices, food insecurity and inad-equate provision of WASH and health ser-vices. Food security encompasses access, adequacy and availability to both quantity and quality of food - People are food secure when food is both available and accessible and when population is informed and is able to consume a balanced diet. When analysed in context to Sindh and as documented in NNS 2011, the underlying reasons for poor nutrition status became quite clear. Since 2006, the food insecure population in Pakistan has increased by 12 million while the number of the se-verely food insecure population (consuming less than 1,700 kcal per day) has risen from 9.6 million to 45.3 million people – 28% of the population. According to NNS 2011, two thirds of these new severely food insecure people live in rural areas. In context to Sindh, flood and drought, social status, gender and rapid urbanization have played a key role in causing food insecurity; food insecure families across Pakistan do not have choices of desired dietary intake16. Only 24% of the population has proper sanita-tion; 64% have access to safe water and 52% of households have electricity.
The framework indicates underlying social determinants of health including poverty, women social sta-tus and policy and political issues. Poverty rate in Sindh is 31% vs. 33% in Pakistan (SPDC, 2004). Highest poverty level is observed in small towns (40%) followed by rural Sindh (38%) and large cities (23%). Sindh also has a high unemployment rate of 5.08% vs. National 5.95% (Labour Force Survey 2010-11) which is one of the key reasons for poor economic status of the population in Sindh. Poverty and lack of opportunities for education, particularly for females have negative consequences on care practices, on the utilization of health services, on family hygiene and on food security. And all of these are affected by economic status, governance and other “basic causes.” These care practices are de-pendent upon the choices that a mother is able to make which are the results of education, economic autonomy and women’s social status.
16 Food security exists when all people, at all times, have physical, social and economic access to sufficient, safe and nutritious food which meets their dietary needs and food preferences for an active and healthy life. Household food security is the application of this concept to the fam-ily level, with individuals within households as the focus of concern.
6
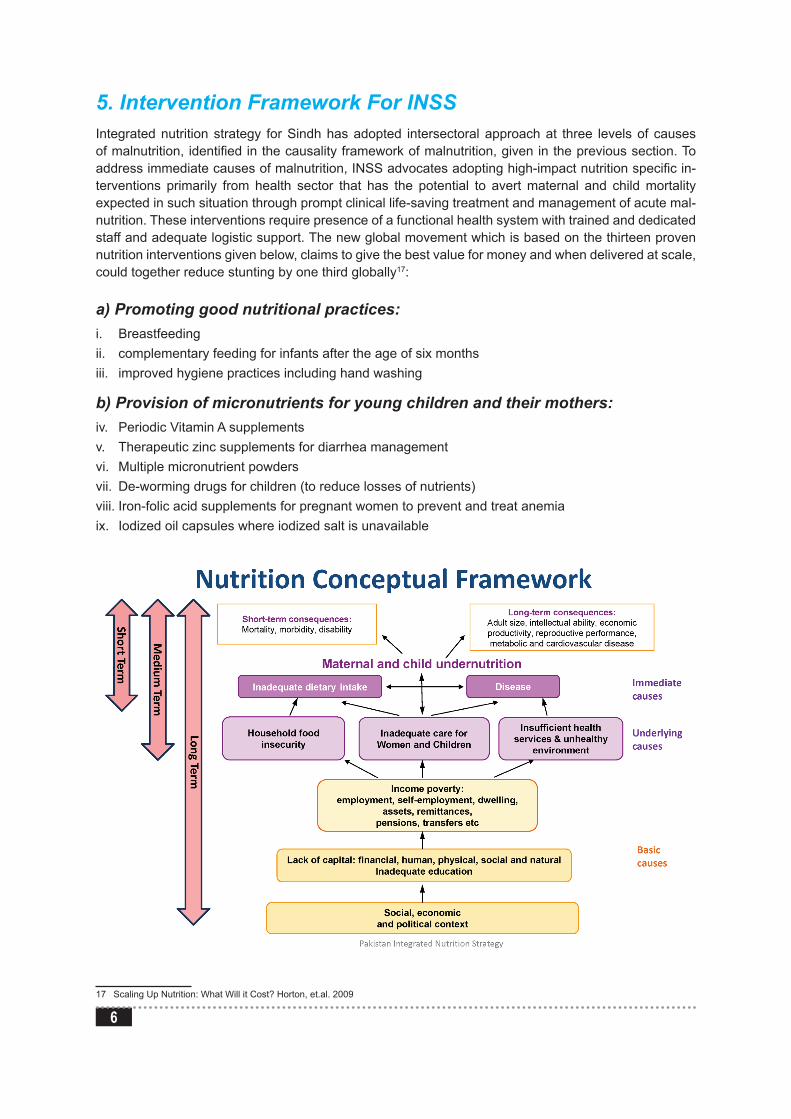
5. Intervention Framework For INSSIntegrated nutrition strategy for Sindh has adopted intersectoral approach at three levels of causes of malnutrition, identified in the causality framework of malnutrition, given in the previous section. To address immediate causes of malnutrition, INSS advocates adopting high-impact nutrition specific in-terventions primarily from health sector that has the potential to avert maternal and child mortality expected in such situation through prompt clinical life-saving treatment and management of acute mal-nutrition. These interventions require presence of a functional health system with trained and dedicated staff and adequate logistic support. The new global movement which is based on the thirteen proven nutrition interventions given below, claims to give the best value for money and when delivered at scale, could together reduce stunting by one third globally17:
a) Promoting good nutritional practices:i. Breastfeedingii. complementary feeding for infants after the age of six monthsiii. improved hygiene practices including hand washing
b) Provision of micronutrients for young children and their mothers:iv. Periodic Vitamin A supplementsv. Therapeutic zinc supplements for diarrhea managementvi. Multiple micronutrient powdersvii. De-worming drugs for children (to reduce losses of nutrients) viii. Iron-folic acid supplements for pregnant women to prevent and treat anemiaix. Iodized oil capsules where iodized salt is unavailable
17 Scaling Up Nutrition: What Will it Cost? Horton, et.al. 2009
7
c) Provision of micronutrients through food fortification for all:x. Salt iodizationxi. Iron fortification of staple foods
d) Therapeutic feeding for malnourished children with special foods:xii. Prevention or treatment for moderate under nutritionxiii. Treatment of severe under nutrition (“severe acute malnutrition”) with ready-to-use therapeutic
foods RUTF). Through these interventions the strategy will aim to reach more adolescent girls, pregnant women and children under five years of age. Community mobilization activities through LHWs to identify and treat severe acute malnutrition through clinical lifesaving interventions are vital for ensuring successful uptake of such intervention. In addition, the strategy envisages sectors to upscale and revitalize vari-ous models present on ground such as Infant and young child feeding program (IYCF), promotion of hygiene behaviors, Vitamin A supplementation and micronutrients and food fortification (wheat with iron and salt with iodine). Most of these interventions emanate out of the 2008 Lancet Series on Maternal and Child Under-nutrition and the revised interventions (Lancet Maternal and Child Nutrition series 2013).
In order to address underlying causes of malnutrition, INSS will adopt medium term strategies proposed in the malnutrition intervention framework. Potential areas of actions include:
i) continue to enhance research and access to bio-diversification and bio-fortified food through house-hold education,
ii) incorporate nutrition interventions in small holder agriculture and rural farmers for encouraging pro-duction of homestead food production and get access to livelihood support– e.g. food for training, food voucher scheme, micro-credit, etc.);
iii) Enhance production, availability and access to fortified food such as fortified flour, oil and other food items as well as access to and micronutrient powders through legislative measures, enforcement of legislation through civil society and Quality assurance department (PSQC) and incentivising private markets and sectors;
iv) improve access and use of safe drinking water and sanitation through the provision of water purifi-cation tablets, containers, soap and hygiene education) and iv) increase access to functional public and private health services in the rural areas to provide access vaccination, PHC, ANC, obstetric and new-born care
In order to address the basic causes, every sector has reviewed their existing sectoral policies and strategies and has identified the areas of synergies. The sectors will also identify the areas of policy coherence and identify and address any unintended negative consequence on nutrition of the popula-tion. The departments and P and D have committed to reassess their existing PC1s to ensure these are gender sensitive, nutrition sensitive and address the need to reach out to those most affected by the issues.
8
6. Goal Of The Intersectoral Nutrition InterventionIntersectoral nutrition strategy for Sindh aims to reduce chronic malnutrition in children aged 0-24 months by 10 percentage points (from an estimated 49.8% to 39.8% by the end of 2016.)18 iron de-ficiency anaemia in children from 73% to 62% and maternal anaemia from 59% to 49% by the end of 2016 through sustainable, effective and inter-sectoral interventions.
6.1. Operational objectivesi. Improve nutritional outcomes in the Sindh province with a focus on sustainable, effective intersec-
toral interventionsii. Strengthen the provincial capacity for developing, mobilizing and stewarding intersectoral interven-
tion developed through public private partnership;iii. Integration and mainstreaming of nutrition in agricultural education, agriculture services and com-
munity development programs;iv. Promote nutrition health of women and children through linking mother and child health with social
protection, and food security interventions to produce long term sustained results; v. Promote programmatic complementarities and geographical convergence through coordinating the
strategic sectoral plan vi. Provide a broad Monitoring and Evaluation Framework for monitoring of nutrition sector strategy by
DOH and partners
6.2. Underlying assumption1. There is commitment to rapidly scale up both domestic and external investment for intersectoral
nutrition intervention;2. Development partners will harmonize their external assistance and will aim to reduce fragmentation
and enhance mutual accountability;3. Government, non-governmental sector and elected representatives will own the strategy;4. There is readiness to move towards one integrated provincial and district level monitoring and
evaluation system;5. Key sectors i.e. health, agriculture, food/ livestock/poultry and water and sanitation are committed to
coordinate and collaborate intersectorally and cross sectorally to make their interventions pro-poor, gender and nutrition supportive.
7. The Guiding Principles
Principle One: Recognition of Right to foodThe right to food is the first fundamental principle underlying this strategy. It is defined as:
“The right to have regular, permanent and unrestricted access, either directly or by means of financial purchases, to quantitatively and qualitatively adequate and sufficient food corresponding to the cultural traditions of the people to which the consumer belongs, and which ensure a physical and mental, indi-vidual and collective, fulfilling and dignified life free of fear.”
Principle two: Evidence based interventionsNutrition interventions instituted globally with right policies and interventions have shown remarkably
18 Given that weight data on infants in the first months of life will also offer insights on the prevalence of low birth weight, the indicator as a whole can serve as a measure of nutritional status in the first 1000 days.
9
reduction in the rates of under-nutrition. In designing the strategy, the country experience will be studied by the stakeholders. There is much that Pakistan can learn from neighboring countries like Bangladesh where appropriate policies, strategies and evidence based interventions have reduced malnutrition. In Bangladesh, from 1996 to 2006, there was 20 % reduction in stunting and 10 % reduction in under-weight.
Principle three: Geographical convergenceSindh has 23 districts however the situation of chronic malnutrition varies across districts. Even within districts, there are UCs which are more deprived then the other where social determinants of malnutri-tion are to a great extent lacking. It is proposed that the strategy focuses on district levels and further on high risk UCs within those districts and other districts for implementation in a phase wise manner. It is also proposed that such districts become priority districts for all the sectors and the coherent plan of implementation is adopted. The maps of high risk districts have been given in Annexure III.
Principle four: Gender empowermentThe status of women and women has a direct role on reduction in under-nutrition. One study19 that shows improving the status of women in South Asia would reduce the level of underweight children un-der three years of age by approximately 12%. According to World Bank giving 100 girls one additional year of primary education would prevent roughly 60 infant deaths and three maternal deaths, while averting some 500 births.
Principle five: Plan inter-sectorally and implement sectorally The strategy advocates inter-sectoral actions. Each sector will analyze their sectoral strategies using nutrition lens. These multiple sectors through their combined and coordinate actions will reduce vulner-ability to malnutrition through preventing illness and promoting health by creating an enabling environ-ment for actions. The strategy although will adopt an intersectoral approach but for implementation will focus sectorally and improving their current operations. The strategy proposes an oversight planning committee at the provincial level and an intersectoral district level committee to ensure coherent inter-sectoral interventions.
Principle six: Encourage involvement of the civil societyThe strategy envisions a critical and constructive role of the civil society and non state actors. The study envisages encouraging civil society stakeholders to actively participate in social mobilization, gover-nance, service delivery, research, monitoring and advocacy for nutrition promoting actions.
Principle seven: Common targets and indicators Common targets and indicators will be instituted with an aim to reduce prevalence of child stunting and micronutrient deficiency in women and children. It is proposed that a oversight project monitoring structure be formed to ensure that the nutrition outcomes are showing improvement through carrying out mid-term and end term evaluation. The strategy recommends development of a common inter-department reporting format to be implemented at the UC levels. The reports would be submitted to the district level and then the provincial level inter-ministerial group for monitoring of the progress.
19 L. Smith, U. Ramakrishnan,A. Ndiaye, L. Haddad, and R. Martorell, The Importance of Women’s Status for Child Nutrition in Developing Countries,Research Report 131, IFPRI, 2003

10
8. Target Group For Nutrition Intervention
1000 days plus approach (Preconception, conception, pregnancy and lactating women)Maternal nutritional status is a determinant of chronic and acute nutritional status in children under 5 years old. Scientific evidence indicates that first 1,000 days after conception is the most critical period of a child development. However the boundaries are inexact and in particular, the critical importance of the preconception period is being recognized. Both the size and age of women at the time of conception as well as nutrition during pregnancy are important. Many children are born undernourished because their mothers have a poor nutrition status. Through this route the disadvantages incurred by poor nutrition are passed between generations20. The data from Pakistan indicates that a significant proportion of children are already stunted at six months of age indicating the critical contribution of fetal malnutrition and small for gestational age. When mothers are breastfeeding they require extra energy which they can get from the reserves they have built up during pregnancy and from eating extra food after birth. The data indicates that a significant proportion, almost half by some estimates, of growth faltering oc-curs between the ages of six and 24 months when the child is no longer protected by exclusive breast feeding and critically dependent on appropriate complementary foods for nutritional needs. In addition effects of under-nutrition are irreversible if intervention is delayed until the child is two years old. Even a child adequately nourished after 24 months of age is unlikely to recover growth ‘lost’ in the first two years as a result of malnutrition.
Childhood (2-5years): Poor diet and repeated episodes of infectious disease and parasites affects the nutritional status of 2-9 year old children. Vitamin A supplementation is unlikely to affect linear growth, but has an impact of diarrheal disease burden and morbidity21. Zinc supplementation has an impact on linear growth and the effect is greatest among children between 12-36 months of age at risk of zinc deficiency. Psychological development may improve with a combined preschool nutrition and stimula-tion intervention. While improved weight gain has been demonstrated among school age children after deworming, there is no evidence of benefits on linear growth in children under 5. Malaria control using bed nets can reducethe prevalence of anaemia in young children and improve growth.
20 Scaling Up Nutrition: The UK’s position paper on under nutrition, September 201121 Strategies, Policies and Programs to Improve the Nutrition ... - FANTAwww.fantaproject.org/.../StrategiesPoliciesPrograms_Nestel.pdf
11
Adolescent age groups Adolescent boys and girls are both the target for the INSS. This age group is particularly important for girls because of their reproductive role, impact it has on the baby and inferior social status needs priority attention. INSS aims to give priority to adolescents in both education and health sector. Evi-dence suggest that adolescents should be considered separately as two groups22 for programmatic purpose: the younger ones (10-14 years), when 80% of the growth takes place and need for nutrients is very high; and the older ones (15-19 years), whose rate of growth has slowed down but for whom micronutrient deficiency control, especially Iron deficiency anemia (IDA control), is important. Adoles-cent girls in the age group of 10-14 years can be reached through school if they are able to attend the secondary. 15-19 years of age group is very important because in rural communities girls are often married at a younger age and a therefore a poor pre-pregnancy nutritional status and iron stores have a greater effect on pregnancy outcomes than anything taking place during pregnancy. Girls in the later age group can be reached through preconception counseling. Community based outreach workers from various sectors can play a critical role in influencing family behavior towards nutrition in girls in this age group.
Rationale For Investment In Nutrition In Sindh“Nutrition Policy Guidance Notes for Sindh” very clearly indicates that malnutrition in the province re-sults in direct loss to the economy of 2.7 to 4.1% of GDP annually and places constraints on economic and social development in the province through three tier pathways:
l Direct losses in productivity from impaired physical status –l Indirect losses from poor cognitive function l Losses emanating from increased health costs resulting when malnutrition reduces immune re-
sponse to infection. The report has outlined in detail about the impact of malnutrition as a direct consequence of prevalence rate of stunting (under 5), wasting (under 5), IDD in school age children, Anaemia in under 5 year old children and Vitamin A deficiency (under 5)23.
9. Organization And Sector Analysis And Proposed Inputs
I. Planning and Development (P and D)Planning and Development Department has a key role in policy planning, coordination between provincial and federal governments and donor agencies, coordination of foreign aid and technical assistance from abroad through Economic Affairs Division. P and D Dept. process PC-1 for different departments; finalize Annual Development Plan and 5 years Development Plan for different departments in the province.
Headed by Additional Chief Secretary (ACS), Sindh P&D Dept. is manned by about 200 officers in vari-ous technical and administration sections. P &D has 4 wings and every wing has its own role, technical, administrative, development and procurement. P and D has a technical committee which is headed by the chief economist and initially approves projects to be further sent to Provincial Development Working Party (PDWP) for approval. P and D has a monitoring evaluation cell and (TPM) which performs the role of the third party monitoring cell as well.
After 18th amendment budget given by Federal Govt. is now with Provincial Govt. and channelized through provincial finance dept. on demand basis and according to agreed ADP to respective dept. If
22 Adolescent Nutrition: A Review of the Situation in Selected South-East Asian Countries23 Nutrition policy guidance notes Sindh, P and D, Government of Sindh.
12
any project’ budget crosses 1000 million it goes to ECNEC for approval and then to Federal Govt. ap-proval through Central Development Working Party (CDWP). Once approved from Federal CDWP then Sindh Govt. releases administrative approval.
Potential role in INSS:i. P&D is currently reviewing following PC1s which will have tremendous impact on improving nutri-
tional status of the population:a) PC1 –NPS on agriculture development of farmers through micro credit loans, improving the ir-
rigation system and building safe capacity for grain storage. b) PC1 for nutrition (NPS) is in its finalizing stages and focuses primarily on improving the nutri-
tional status of children under five years and pregnant/ lactating women. ii. Sindh P and D department has adopted leadership role in bringing together different sectors un-
der the aegis of steering committee chaired by ACS development and secretaries of relevant de-partments as members. Steering committee has technical working group that comprises of focal persons from department of health, education, women development, agriculture, food, livestock, fishery and social welfare.
iii. The secretariat of the inter-sectoral strategy implementation will be based in the P and D.
II. Health SectorHealth sector plays a key role in addressing the nutrition issue mostly through addressing immediate causes of malnutrition. Like other vertical department, health department has also been devolved. De-volution in principle is meant to empower provinces upto district level. Lack of adequate funding has compromised the provinces to achieve desired level of effectiveness of the program. In addition lack of proper preparation and provincial capacity has restricted the province from taking a full benefit of the change and maximize on the synergy that would have been an outcome of this change.
Following sub sectors of health are directly involved in nutrition activities:
Lady Health Workers (LHW): LHW program currently operates in 23 districts of Sindh. LHWs are responsible for screening babies with moderate to severe malnutrition using MUAC approach and administration of iron, folic acid to pregnant women (during the house visit) and administer deworming tablets to children. LHWs play a critical role in community awareness raising around the issue. The LHW collects information about nutritional status of the children in the community but there is limited sharing of this information with other subsectors of health.
MNCH Program: MNCH program aims to reduce maternal and neonatal mortality through promoting skilled birth delivery, safe delivery practices, exclusive breast feeding and complimentary feeding in hard-to-reach areas as well as to support BEMONC & CEMONC 24/7 at all levels as per WHO proto-cols. MNCH activities are focussed at expectant mother and children of less than 5 years of age with no or little
Access to health services24 (USAID report). Role of CMW in nutrition program is limited to distribution of vitamins and supplements, Iron & folic acid, Calcium, Vitamin D and Multi vitamins to women during pregnancy and after delivery.
EPI/Polio Program: EPI program primarily focuses on immunization of children up to 15 months of age. Polio eradication program is not under the umbrella of EPI but is an important initiative from nutri-tion perspective. Vitamin A supplements are administered to children up to 5 years during the campaign. When the Polio program is rolled up and Pakistan achieves “Polio free Pakistan” status, new strategies will be designed for continuation of administration of Vitamin A.
24 Road Map for Health, Systems Strengthening in Sindh Province to support USAID/Pakistan’s RMNCH programs in Pakistan. DRAFT, Octo-ber 2012
13
Health Education Units, Structure and FunctionsPresently, the Health Education Officers (HEOs) and health education service units are present at the provincial and district levels but these are weak and not functioning properly because of shortage of staff. Support staff is also not available in any health education service unit to carry out health educa-tion-related field activities. A proposal is under consideration to establish service structure, organiza-tional structure and operational funding for health education and cadre of HEOs and required support staff. With enhanced capacity, health education cell can play a key role in standardizing health education and communication messages to be promoted from different sectors
Nutrition Program Cell: Sindh has a provincial nutrition program cell which is headed by a Pro-vincial Nutrition manager along with two deputy program managers. The program relies completely on district health officers of various programs and CBOs for program implementation. It is being imple-menting following four components:
i. Community outreachii. Supplementary Feeding Programme (SFP)iii. Outpatient Therapeutic programme: for children suffering with SAM iv. Inpatient Care for malnourished children
Nutrition Support Programme Sindh (NPS) NSP envisaged for 2013 to 2016 will target 09 districts of Sindh. Its PC-1 is in its finalizing stages and focuses primarily on improving the nutritional status of children under five years and pregnant/ lactating women. The PC1 will be executed by Health Department, GoS with financial support by the World Bank and ADP allocation of Govt. of Sindh. The Provincial Nutrition Support Program and Health Department will be responsible for the operationalization of the PC1. The Nutrition Cell, Health Department will act as Program Implementation Unit (PIU) and provide oversight and leadership for effective implementa-tion of the programme at provincial and district level. Nutrition cell of the project will be responsible for ensuring regular program monitoring, annual assessments, mid and end term evaluations of the inter-ventions. NSP framework has been developed with reference to Medium Term Development Frame-work and MDGs1, 4, & 5. Project will be implemented by the provincial department of health at the Provincial level and will be implemented through District health office of health at the District levels esp. the service delivery part primarily through the Lady Health Workers, of the National Program for Family Planning and Primary Health Care, services of PPHI
The main focus of the NPS is on the following:
l Addressing malnutrition in Children (06 – 59 months) and Pregnant & Lactating Women through IYCF and CMAM services esp. to the rural areas
l Addressing Micronutrient Deficiency through provision of micronutrient powders (through LHWs and CMWs), iron folic acid tablets to pregnant women, vitamin A supplementation (EPI Program), supply of Zinc and ORS
l Communication for Development and Behaviour Change; l Strengthening Institutional Capacity, Research and M&E Systemsl Focus on micronutrient deficiency through Vitamin A campaigns, IFA supplements and counselling
of PLWs, ensuring continuous supply of Zinc and ORS and training of health workers to address de-worming of male and female children with a focus on poor and disadvantaged through UNICEF support
l Advocacy for fortified foods. NPS aims to advocate for enacting of law for fortification of foods, in-cluding salt and wheat flour, advocacy with private salt processors for expansion of salt iodization program and with policy makers and private industry for expansion of the wheat flour fortification program along with capacity building for monitoring and demand creation, system of sustainable supply of KIO3 (iodine fortification),etc.

14
l In country production of high density diet for treatment of severely malnourished children.
III. Sindh Education And Literacy SectorThe vision of the Education and Literacy Department25, Govt. of Sindh is “to instil moral values and pro-vide education to all citizens irrespective of gender, caste, creed, or race. The basic thrust of the reform agenda is to remove illiteracy and provide free and compulsory primary and secondary education to all within minimum possible period.”
Sindh has 49,605 institutions from primary till higher secondary level. The share of various sectors is as follows: primary – 90.8%; Middle – 5.4%; Secondary – 3.3% and higher secondary – 0.5%26. There are 4.5 million children at these various levels with bulk (62%) going to primary. There is huge decline in middle sector enrolment compared with primary and if the transition gets improved serious efforts would be needed to provide physical space and teachers for increased enrolment. Across all the levels, the student-teacher ratio stand at 1:30; student-school ratio stand at 1:147 and student classroom ratio stand at 1:44.
In accordance with the 18th amendment, the functions of federal education ministry has been devolved to the provinces which on one hand present many opportunities but on the other hand, also pose some challenges because of the lack of capacity to deal with this change. Sindh, does not have a formal poli-cy document available at the provincial level, there is discussion within the provincial education ministry on the issues of education policy and curriculum in post 18th Amendment scenario27.
The ideology of Pakistan lays down upon the Government the obligation to make education acces-sible to all citizens. Sindh already had Sindh Compulsory Primary Education Ordinance of 2001 in place without much impact on enrollment as evident from various surveys. On February 13th, 2013 Sindh has legislated compulsory free education free and compulsory for children between five and 16 years. Enforcement of the ordinance and legislation will pose huge challenge for the DoE. Under the new law, all private schools will be bound to reserve 10 percent admissions for disadvantaged and terrorism-affected children. Under the “Sindh Right of Children to Free and Compulsory Education Act, 2013”, children will fall into the disadvantaged criterion if their parents’ monthly income is less than the minimum wage – Rs8,000 – fixed by the government. The law also makes it compulsory for parents or guardians to send their children to school.
AGPES is the PC1 for fourth phase of “assistance to girls primary education in Sindh (AGPES)” with a major focus on school feeding as a means to increase girls enrolment has been approved for the period from July 2013 to 30th June 2014 with a budget of Rs. 780 million. Under this project, 500 Government Girls Primary Schools in five districts i.e. Jamshoro, Thatta, Badin, Dadu and Tharparkar has been targeted to increase the low enrolment ratio in these districts. The project is within the framework of Education for all (EFA)”.
Sector IV: Department Of Agriculture / Food / Livestock / Poultry And Fisheries Agriculture contributes to over 21% of GDP, and employment to 45% of the country’s labour force be-sides contributing to substantially to the country’s exports. Four major crops (wheat, rice, cotton, and sugarcane) on average, contribute 29 percent to the value added in overall agriculture and 6.0 percent to GDP28. The livestock sector contributes 11% of the country’s GDP, with an estimated 42 billion liters of milk produced per annum.Since the 18th Amendment to the Constitution of 1973, Ministry of Food
25 http://www.sindheducation.gov.pk/26 Policy Analysis of Education in Sindh, UNESCO, Pakistan27 Dr Eshya Mujahid-Mukhtar. “Situation Analysis of the education sector”. UNESCO.28 Agriculture - Ministry of Finance available on www.finance.gov.pk/survey/chapter_12/02-Agriculture.pdf
15
and Agriculture and federal ministry of livestock and dairy development have been devolved to prov-inces. In spite of this change, issues such as the import and export of agricultural inputs and products, price setting, standardization and quarantine issues, national research and inter provincial issues i.e. rehabilitation, operation and maintenance of primary irrigation structure come under the nexus of the Federal Government.
Dairy Industry And Livestock: On average a dairy animal in Pakistan yields 6-8 times less milk than a dairy animal of the developed world29; Small average animal holding herd size of 3 per household in the country is posing a major barrier to developing the dairy farming sector.30 Dairy farmers are therefore not motivated to feed their animals, good quality fodder or practice good farm management.
Development Of Livestock Sector: Livestock and fisheries play an important role in poverty reduc-tion in the rural areas particularly from women perspective and has been described as a priority area of investment strategy of the government of Sindh. Government in its future plan has undertaken a project to set up a dairy village and animal meat processing zones in district Thatta on a public private partnership basis which will have direct impact on the meat and dairy product enhancement which will reduce poverty as well as availability of nutrition food.
Development Of Fishery Sector: Development of fishery sector will have impact upon the poverty reduction and availability of nutritious food. Rs. 1.065 billion has been allocated for 10 schemes in fisheries sector, in which 5 are ongoing schemes and 5 schemes are new projects which are be implemented in the next fiscal year. A model village has been planned for fisherman at Hawks-bay, Zero Point Badin, Munchhar Lake and Keenjhar LakeThatta. Budget also incorporates introduction of culture of High value Brackish Water fish in Sindh, rehabilitation of Pilot Shrimp Farm Garho as Training & Research Centre.
Sector V: Water, Sanitation Hygeine And PHED DepartmentsBefore promulgation of Sindh Local Government Ordinance (SLGO) 2001, the local Government was declared a department under rule 1979 for providing and maintaining the water supply and sanitation services throughout the province through Metropolitan corporations, Municipal committees, town com-mittees and union councils. After promulgation of Sindh Local Government Ordinance (SLGO) 2001, sanitation functions have been devolved to taluka/town level and a body designated as taluka/town Mu-nicipal Administration (TMA) has been set up, to provide municipal services at a taluka/town level under the Department of Local Government in the provincial administration. Prior to the SLGO, the water sup-ply and sanitation facilities for rural and urban areas were provided through Public Health Engineering Department [PHED] including its operation and maintenance.
Public Health Eng. Department was initially created by Government of Sindh (GOS) as a Project Directorate in mid-sixties and worked as a wing of local Govt. Department. PHE was upgraded in mid-seventies as a department with restricted mandate for only construction of water and drainage schemes throughout the province except two cities i.e Karachi and Hyderabad for which KWSB & WASA got the mandate.
Sindh Government has issued “Sindh Sanitation Strategy (SSS)” in 201131 which is currently more hardware focussed. The strategy can be reviewed to promote health and hygiene practices in context to both rural and urban areas of the province through behavioural change approaches and adoption of innovative technologies under the rubric of National Sanitation Policy (NSP).
“Municipal Services Delivery Program” (MSDP) Sindh is a program initiated by Sindh Government in collaboration with USAID with an aim to provide safe drinking water, improved sanitation and solid
29 Dairy Industry of Pakistan at www.iiste.org/Journals/index.php/EJBM/article/.../326530 Dairy Industry of Pakistan, available on www.iiste.org/ Journals/ index.php/ EJBM/ article/.../326531 http://202.83.164.25/wps/wcm/connect/1354e5804189d3a695fb9f71b08de1d3/Draft+Sindh+Sanitation+Strategy+June+18+2008.pdf?MOD=AJPERES&CACHEID=1354e5804189d3a695fb9f71b08de1d3&CACHEID=1354e5804189d3a695fb9f71b08de1d3

16
waste management system. The project upon completion will be reduce the incidence of diarrhoea and other water related diseases in selected secondary cities/ towns in the province
Sindh Cities Improvement Program (SCIP) is a Government of Sindh and Asian Development Bank (ADB) $400 million program focussed on improving the urban infrastructure & services, urban en-vironment and public health. SCIP has the potential to reduce the incidence of diarrhoea and other water borne and water related for an estimated 4-5 million residents in participating secondary cities in Sindh.
Operation and Management is a vital element of any water and sanitation scheme. The responsibility of O&M for urban schemes was entrusted to Municipal committees and the understanding continues to date. Unfortunately, the issue of Operation and Management (O and M) for rural schemes persists to pose a challenge as no clear policy could be devised. This is reflected in the figures received from WASH sector that reveals that more than 80% of water and sanitation schemes in urban areas (Popula-tion more than 5000 persons) are functional. While dwellers of urban area have access to water, this is not necessarily safe clean drinking water if assessed on the internationally recommended criteria. In contrast in the rural areas, proportion of functional scheme is less than 25%.Most of the rural population does not have access to water.
Cross Cutting Sectors
I. Social Welfare And Social Protection ProgramPoverty and under-nutrition are very closely interlinked and is indeed been defined as a cross sec-toral agenda. Poverty-Nutrition Cycle is vicious in nature and lead to a very complex inter-relationship between the poverty-related causes and consequences of malnutrition. The conceptual framework of the United Nations Children’s Fund (UNICEF 1990) identifies poverty as an important basic cause of under-nutrition.
Pakistan has adopted National Social Protection Strategy (2007) that provides a unique oppor-tunity to strengthen its social protection. Consistent with the Poverty Reduction Strategy and Pakistan Vision 2030, the Strategy provides a sectoral framework to address poverty allevia-tion. Since 18th amendment in the constitution, social welfare has now been fully devolved to the provinces. Even though coordination of programs within each province is likely to improve as a re-sult of the devolution, it is feared that in the absence of a central, coordinating body, coordination among provinces might deteriorate. Provincial capacity to manage this portfolio is also questionable. In 2009, as a key element of this strategy, Pakistan introduced a national safety net program, the Benazir Income Support Program (BISP). The primary mandate of Benazir Income Support Program (BISP) is poverty alleviation. BISP has immense potential to reach out to poor women and children by making cash transfer conditional to certain health behavior which may ultimately improve the nutritional status of the target group.
In recent past 90 percent of Zakat funds were diverted to BISP. Enrolled families are paid cash assis-tance @ Rs.1000 per month on quarterly basis; apart from benefits provided under graduation strategy like: long term interest free returnable financial assistance, vocational & technical training, health & life insurance coverage. In 2010, about 7% of the country’s population was benefiting from the transfers. The BISP also includes microcredit financial assistance, and is pilot testing health and life insurance coverage and vocational skills training32
32 Channa A, 2012. Background Paper Social Protection in Pakistan: A Profile of Existing Programs and an Assessment of Data Available for Analysis, Asia Research Centre, London School of Economics.
17
BISP has also established a small Social Policy Research Unit in order to strengthen research activities related to social policy social protection and cash transfers.
Special initiatives of BISP include:
a. Waseela-e-Haq: To promote self-employment among women beneficiaries (or their nominees as in Balochistan, trainees are usually men to improve their livelihood. Soft loan of PKR 300,000 on 15 years terms for business+10 days fully covered training on entrepreneurship and business manage-ment are being offered.
b. Waseela-e-Rozgar: To empower female beneficiary or her nominee through acquiring a skill; be-come economically independent by acquiring vocational training through dynamic and Intersectoral technical education and vocational training service
Beneficiaries are given vocational training in one of 52 different trades (check for nutrition relevant!)
c. Waseela-e-Sehat: Health Insurance program with an annual maximum limit of Rs. 25,000 per family through Benazir Sehat cards , Conditional Social Transfers
BISP has also established a small Social Policy Research Unit in order to strengthen research activities related to social policy social protection and cash transfers.
Proposed Action
a) BISP is planning to expand its coverage to rural areas- an excellent opportunity to address basic cause of under-nutrition;
b) Education sector has proposed working with BISP to encourage daughters of BISP beneficiaries to enrol in schools which access to mid-day meal program
c) The BISP database is an immense resource and can be used to map out social welfare for women and disabled as it captures nationwide segment of the ultra-poor population. Through microfinance loans and waseela-e rozgar, BISP has expressed readiness to encourage small level food and mi-cronutrient products stores in rural areas that can provide access to diverse source of food at low cost upon showing BISP card or vouchers, e.g. multi-micronutrient powders, soap, water purifiers;
d) Health awareness around nutrition can be promoted through utilization of cell phones (owned by 56% of BISP’s beneficiaries) to provide/reinforce key information tailored to pregnancy or early childhood as appropriate.
e) BISP has expressed its commitment to work with agriculture and PHED program to assist skill de-velopment program in rural communities using expertise available for food processing and opera-tion and management of the water and sanitation network.
f) Other social safety net programmes with cash or food transfers to extremely poor households will be promoted
II. Women Development Department Women Development Cell was established in the Planning & Development Department, Government of Sindh in 1979. The objective of this cell was to address women’s issues through an institutionalized sys-tem in planning and development of Sindh. In 1995 a separate Women Development Department was formed with a broader scope than the previously established cell within the P&DD. However in 1998 the Department was merged with the Social Welfare Department at the secretariat level. In 2001 the Directorate of Women Development was abolished and a Women Development Wing was established under Directorate of Social Welfare. It was later put under the control of Population Welfare Depart-
18
ment. In 2003 a separate Women Development Department was re-established with a strong mandate focused towards women’s empowerment and gender equality. WDD aspires to enhance the status of women to promote women’s rights, ensure their active participation in national life at all levels on the basis of gender equality and to serve as an agent of change in the society, improved legal to economic resources and employment access.
The Women Development Department will achieve these role as a catalyst, lobbyist and advocate for gender related issues by providing a platform for women in anticipation. After the devolution of Ministry of Women Development , Government of Pakistan, responsibility and role of Women Development Department, Government of Sindh have been extensively enhanced. The Women Development De-partment, Government of Sindh comprises a Secretariat/Administrative department and a Directorate headed by a Secretary. Following are the roles of the WDD:
1. Formation of public policies and laws to meet special needs of women.
2. Protection and promotion of Women’s rights, gender equity and equality in public sector or in par-ticular and society in general.
3. Discharge of responsibilities with regard to status of women and girls.
4. Development projects for providing special facilities for women such at strategic initiative, innova-tions and special equalizing projects.
5. Coordination of women’s welfare programs with other concerned departments and agencies at District and local level for making conductive and safe work environment for working women and conducting research/surveys in the regard.
6. Improvement of working conditions of female labour both in urban and rural areas.
7. Promotion of cottage industry with special preference to participation of women in such industry.
8. Maintenance of a database of all women parliamentarians, councillors and members of civil society organizations working on gender issues.
9. Setting up of community/mohallah Schools and training centres for women on the basis of self-help community development.
10. Setting up of advisory legal centres to provide legal aid to women and to review laws considered to be discriminatory against women and formulate recommendations in respect thereof.
11. Implementation of National Women’s Welfare Policy as applicable to the Province of Sindh.
12. Registration and assistance of women Organizations.
13. Promotion and under taking of training and research on the condition and problem of women
14. Service matters, except those entrusted to the Services, General Administration and Coordination Department.
Civil Society Organizations Civil society is “an umbrella term for a range of non-state and non-market citizen organizations and ini-tiatives, networks and alliances operating in a broad spectrum of social, economic, and cultural fields. These include formal institutions, non-governmental organizations, trade unions, professional asso-ciations, philanthropies, academia, independent pressure groups, think tanks, and traditional informal formations, such as faith-based organizations, shrines, seminaries, and neighborhood associations.” Since the 1980s, health-related CSOs have proliferated in type, number and functions they perform, a development largely seen in positive terms. NGOs have mushroomed, however legal framework for recognizing CSO role is still absent. The CSOs with their independent transparent role will strengthen the governance and monitoring role during the implementation of intersectoral nutrition intervention
19
plan. In addition CSOs with technical expertise will extend their support in the research, documentation social mobilization activities.
l Internationally there are several examples available which indicates that with CSOs participation, advocacy objectives are rapidly adopted e.g. HIV, youth issues etc. With the devolution and district based health service delivery, the environment has become more supportive for CSO participation. Participation of CSOs is viewed as manifestation of democratic society
l During crises situation and emergency response, CSOs and NGOs have emerged as a powerful player in the Government for resource mobilization and for strengthening service delivery;
l Experience from other countries indicates that CSOs often are more effective in ensuring corporate role through appropriate regulation.
l In Pakistan, CSOs and NGOs have been actively involved in undertaking series of research and surveys particularly around issues of nutrition including anthropometric surveys.
“Pakistan Health and immunization CSO coalition” is an important platform that currently has a constitu-ency of 51 members and is planning to broaden itself. The coalition has expanded itself into an orga-nized platform and is working to strengthen Government in many social change agenda like vaccina-tion, social mobilization and strengthening service delivery in hard to reach population. Initially funded by GAVI, the platform today represents CSOs in NITAG and other dialogue fora. The coalition has plans to expand health, agriculture, environment and other sectors are organized under the rubric of coalition and on creating social awareness on various aspects of nutrition. CSO will also support Women devel-opment department and Social welfare in carrying out advocacy and social change activities
10. Oversight Coordination, Monitoring And Evaluation
10.1 Provincial Inter-Sectoral Nutrition Program Oversight CommitteeIntersectoral nutrition strategy is the first strategy which involves working across many departments working under the GoS. In order to have successful implementation of the strategy, it is important to establish an oversight “Provincial inter inter-sectoral committee” harmonizes plans and takes decisions to ensure implementation of coordinated and geographically convergent actions, tracks implementation of sectoral commitment, address any emerging red flag problems and limiting factors quickly and efficiently, and to assure accountability for results. It is proposed that the committee be chaired by Chief secretary or Additional chief secretary. Following departments will represent on the committee.
l Department of agriculture/ food/ livestock /poultry and fisheries
l Department of education (DoE)
l Department of health (DoH) and population welfare
l Public health engineering department (PHED) and local government
l Women Development Department (WDD) and social welfare
l Finance department P and D
l M and E Department
The committee would also have representation from following departments and sectors:
l Department of social welfare
20
l Women development department
l CSO coalition
ToR Of The Provincial Intersectoral Nutrition Committee:
a) Ensure that various departments are able to work in a coherent and coordinated manner;
b) Ensure the annual district based work plans have been produced in consultation with other sectoral partners;
c) Provide oversight during implementation to ensure that the province achieves its targeted objec-tives and activities;
d) Carry out arbitration and mediation role in case of any conflict and differences between various sec-tors
e) Ensure that an overarching, intersectoral MIS has been developed that reports key performance indicators by all sectors on a quarterly basis;
f) Provides support and approval for mid-term and end term evaluation.
g) Provide policy guidance and support in case it is needed.
g) Performing any other functions assigned to the intersectoral nutrition committee by Chief or assis-tant chief secretary.
10.2. District Based Inter-Sectoral Nutrition Program CommitteeDevolution has provided a unique opportunity to Pakistan and Sindh in particular to operationalize a “district based intersectoral nutrition program committee”. The committee would be responsible for identifying UCs for phase wise intersectoral implementation. The committee will have the representa-tion of various departments and will be guided by the strategic plan approved at the provincial level. A mechanism / platform called “inter-sectoral district nutrition group (IDNG)” or implementation of inter-sectoral nutrition intervention would be established in each district.
The DINPC will have representation from different departments. Following are the terms of reference of DINPC
Terms Of Reference Of District Based Intersectoral Nutrition Program Committee (DINPC)
DIPNC will be responsible for:
i. Prioritizing UCs in each high risk districts for phase wise introduction of the program;
ii. Ensure development and reporting of monitoring indicators for UC level inter-sectoral nutrition ac-tivities;
iii. To oversee the development of micro plans for implementation at the UC level;
iv. To resolve any red flag issue if it arises.

21
Financing Mechanisml A Nutrition section should be established in the province that will provide guidance, support, coordi-
nation and processing of nutrition sensitive intervention across all the sectors.
l Inter-sectoral strategy will be the central tool and will have the monitoring indicators to see progress on the nutrition status
n Every department will make their plans which are nutrition sensitive preferably using policy notes
n Every department will also review their existing plans in pipeline and will aim to make these nutrition sensitive
n P and D will ensure that every plan that is approved is nutrition sensitive
n Plans will be funded either by ADP or foreign assistance
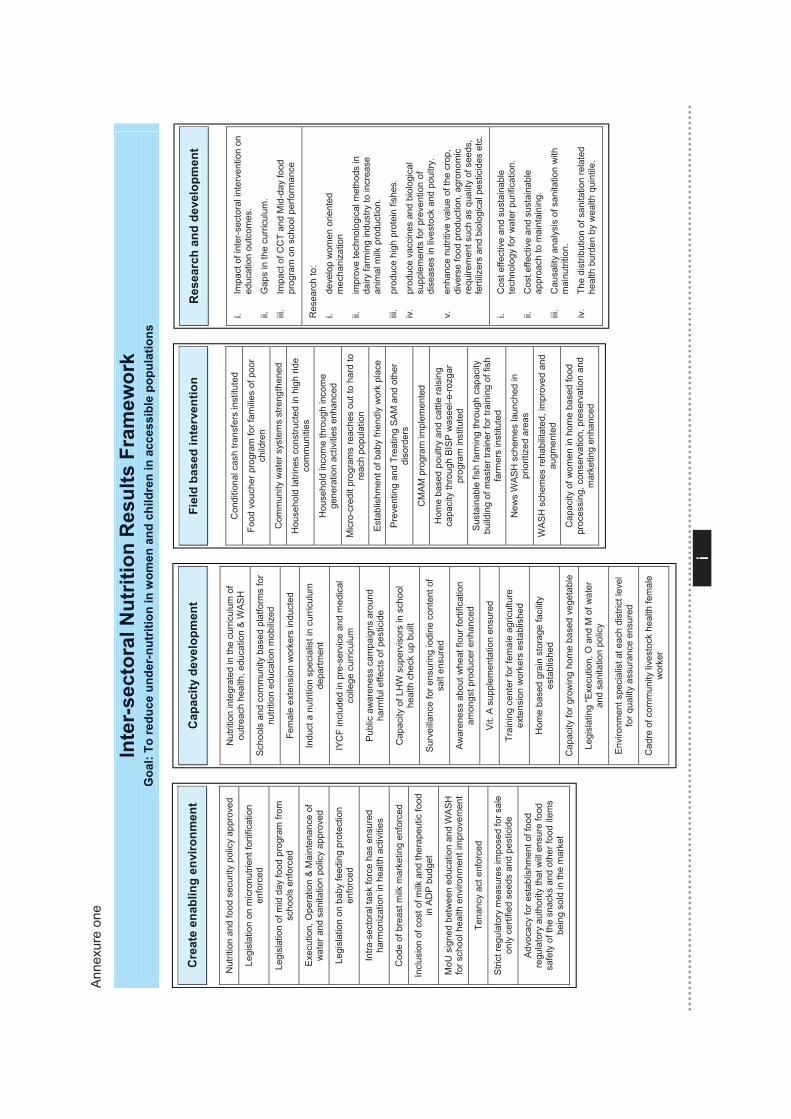
i
i
Ann
exur
e on
e
Cre
ate
enab
ling
envi
ronm
ent
Nut
ritio
n an
d fo
od s
ecur
ity p
olic
y ap
prov
ed
Legi
slat
ion
on m
icro
nutri
ent f
ortif
icat
ion
enfo
rced
Legi
slat
ion
of m
id d
ay fo
od p
rogr
am fr
om
scho
ols
enfo
rced
Exe
cutio
n, O
pera
tion
& M
aint
enan
ce o
f w
ater
and
san
itatio
n po
licy
appr
oved
Legi
slat
ion
on b
aby
feed
ing
prot
ectio
n en
forc
ed
Intra
-sec
tora
l tas
k fo
rce
has
ensu
red
harm
oniz
atio
n in
hea
lth a
ctiv
ities
Cod
e of
bre
ast m
ilk m
arke
ting
enfo
rced
Incl
usio
n of
cos
t of m
ilk a
nd th
erap
eutic
food
in
AD
P b
udge
t
MoU
sig
ned
betw
een
educ
atio
n an
d W
AS
H
for s
choo
l hea
lth e
nviro
nmen
t im
prov
emen
t
Tena
ncy
act e
nfor
ced
Stri
ct re
gula
tory
mea
sure
s im
pose
d fo
r sal
e on
ly c
ertif
ied
seed
s an
d pe
stic
ide
Adv
ocac
y fo
r est
ablis
hmen
t of f
ood
regu
lato
ry a
utho
rity
that
will
ens
ure
food
sa
fety
of t
he s
nack
s an
d ot
her f
ood
item
s be
ing
sold
in th
e m
arke
t
Cap
acity
dev
elop
men
t
Nut
ritio
n in
tegr
ated
in th
e cu
rric
ulum
of
outre
ach
heal
th, e
duca
tion
& W
AS
H
Sch
ools
and
com
mun
ity b
ased
pla
tform
s fo
r nu
tritio
n ed
ucat
ion
mob
ilize
d
Fem
ale
exte
nsio
n w
orke
rs in
duct
ed
Indu
ct a
nut
ritio
n sp
ecia
list i
n cu
rric
ulum
de
partm
ent
IYC
F in
clud
ed in
pre
-ser
vice
and
med
ical
co
llege
cur
ricul
um
Pub
lic a
war
enes
s ca
mpa
igns
aro
und
harm
ful e
ffect
s of
pes
ticid
e
Cap
acity
of L
HW
sup
ervi
sors
in s
choo
l he
alth
che
ck u
p bu
ilt
Sur
veill
ance
for e
nsur
ing
iodi
ne c
onte
nt o
f sa
lt en
sure
d
Aw
aren
ess
abou
t whe
at fl
our f
ortif
icat
ion
amon
gst p
rodu
cer e
nhan
ced
Vit.
A s
uppl
emen
tatio
n en
sure
d
Trai
ning
cen
ter f
or fe
mal
e ag
ricul
ture
ex
tens
ion
wor
kers
est
ablis
hed
Hom
e ba
sed
grai
n st
orag
e fa
cilit
y es
tabl
ishe
d
Cap
acity
for g
row
ing
hom
e ba
sed
vege
tabl
e
Legi
slat
ing
“Exe
cutio
n, O
and
M o
f wat
er
and
sani
tatio
n po
licy
Env
ironm
ent s
peci
alis
t at e
ach
dist
rict l
evel
fo
r qua
lity
assu
ranc
e en
sure
d
Cad
re o
f com
mun
ity li
vest
ock
heal
th fe
mal
e w
orke
r
Fiel
d ba
sed
inte
rven
tion
Con
ditio
nal c
ash
trans
fers
inst
itute
d
Food
vou
cher
pro
gram
for f
amili
es o
f poo
r ch
ildre
n
Com
mun
ity w
ater
sys
tem
s st
reng
then
ed
Hou
seho
ld la
trine
s co
nstru
cted
in h
igh
ride
com
mun
ities
Hou
seho
ld in
com
e th
roug
h in
com
e ge
nera
tion
activ
ities
enh
ance
d
Mic
ro-c
redi
t pro
gram
s re
ache
s ou
t to
hard
to
reac
h po
pula
tion
Est
ablis
hmen
t of b
aby
frien
dly
wor
k pl
ace
Pre
vent
ing
and
Trea
ting
SA
M a
nd o
ther
di
sord
ers
CM
AM
pro
gram
impl
emen
ted
Hom
e ba
sed
poul
try a
nd c
attle
rais
ing
capa
city
thro
ugh
BIS
P w
asee
l-e-ro
zgar
pr
ogra
m in
stitu
ted
Sus
tain
able
fish
farm
ing
thro
ugh
capa
city
bu
ildin
g of
mas
ter t
rain
er fo
r tra
inin
g of
fish
fa
rmer
s in
stitu
ted
New
s W
AS
H s
chem
es la
unch
ed in
pr
iorit
ized
are
as
WA
SH
sch
emes
reha
bilit
ated
, im
prov
ed a
nd
augm
ente
d
Cap
acity
of w
omen
in h
ome
base
d fo
od
proc
essi
ng, c
onse
rvat
ion,
pre
serv
atio
n an
d m
arke
ting
enha
nced
Res
earc
h an
d de
velo
pmen
t
i. Im
pact
of i
nter
-sec
tora
l int
erve
ntio
n on
ed
ucat
ion
outc
omes
.
ii.
Gap
s in
the
curr
icul
um.
iii.
Impa
ct o
f CC
T an
d M
id-d
ay fo
od
prog
ram
on
scho
ol p
erfo
rman
ce
Res
earc
h to
:
i. de
velo
p w
omen
orie
nted
m
echa
niza
tion
ii.
impr
ove
tech
nolo
gica
l met
hods
in
dairy
farm
ing
indu
stry
to in
crea
se
anim
al m
ilk p
rodu
ctio
n.
iii.
prod
uce
high
pro
tein
fish
es.
iv.
prod
uce
vacc
ines
and
bio
logi
cal
supp
lem
ents
for p
reve
ntio
n of
di
seas
es in
live
stoc
k an
d po
ultry
.
v.
enha
nce
nutri
tive
valu
e of
the
crop
, di
vers
e fo
od p
rodu
ctio
n, a
gron
omic
re
quire
men
t suc
h as
qua
lity
of s
eeds
, fe
rtiliz
ers
and
biol
ogic
al p
estic
ides
etc
.
i. C
ost e
ffect
ive
and
sust
aina
ble
tech
nolo
gy fo
r wat
er p
urifi
catio
n.
ii.
Cos
t effe
ctiv
e an
d su
stai
nabl
e ap
proa
ch to
mai
ntai
ning
.
iii.
Cau
salit
y an
alys
is o
f san
itatio
n w
ith
mal
nutri
tion.
iv.
The
dist
ribut
ion
of s
anita
tion
rela
ted
heal
th b
urde
n by
wea
lth q
uint
ile.
Inte
r-se
ctor
al N
utrit
ion
Res
ults
Fra
mew
ork
Goa
l: To
redu
ce u
nder
-nut
ritio
n in
wom
en a
nd c
hild
ren
in a
cces
sibl
e po
pula
tions
In
ter-
sect
oral
Nut
ritio
n R
esul
ts F
ram
ewor
k G
oal:
To re
duce
und
er-n
utrit
ion
in w
omen
and
chi
ldre
n in
acc
essi
ble
popu
latio
ns
Res
earc
h an
d de
velo
pmen
t Fi
eld
base
d in
terv
entio
n C
apac
ity d
evel
opm
ent
Cre
ate
enab
ling
envi
ronm
ent
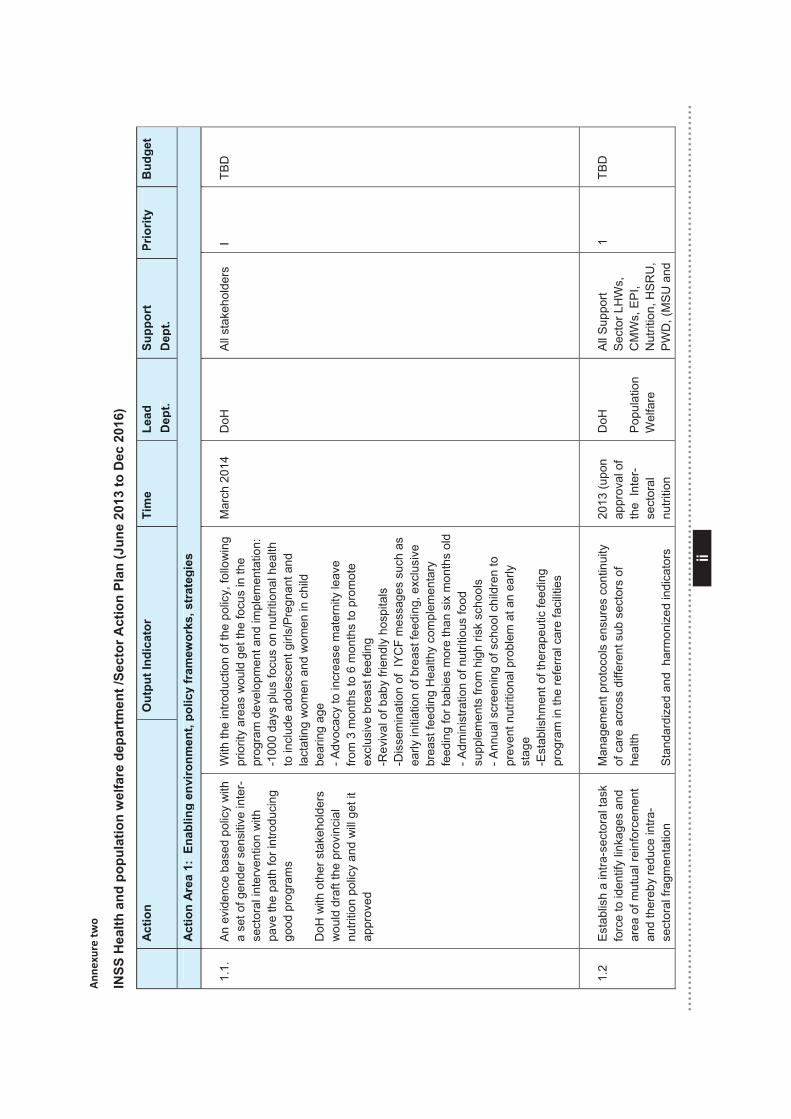
ii
ii
Ann
exure tw
o
INSS
Hea
lth a
nd p
opul
atio
n w
elfa
re d
epar
tmen
t /Se
ctor
Act
ion
Plan
(Jun
e 20
13 to
Dec
201
6)
A
ctio
n O
utpu
t Ind
icat
or
Tim
e Le
ad
Dep
t.
Supp
ort
Dep
t. Pr
iorit
y
Bud
get
A
ctio
n A
rea
1: E
nabl
ing
envi
ronm
ent,
polic
y fr
amew
orks
, str
ateg
ies
1.1.
An
evi
denc
e ba
sed
polic
y w
ith
a se
t of g
ende
r sen
sitiv
e in
ter-
sect
oral
inte
rven
tion
with
pa
ve th
e pa
th fo
r int
rodu
cing
go
od p
rogr
ams
DoH
with
oth
er s
take
hold
ers
wou
ld d
raft
the
prov
inci
al
nutri
tion
polic
y an
d w
ill g
et it
ap
prov
ed
With
the
intro
duct
ion
of th
e po
licy,
follo
win
g pr
iorit
y ar
eas
wou
ld g
et th
e fo
cus
in th
e pr
ogra
m d
evel
opm
ent a
nd im
plem
enta
tion:
-1
000
days
plu
s fo
cus
on n
utrit
iona
l hea
lth
to in
clud
e ad
oles
cent
girl
s/P
regn
ant a
nd
lact
atin
g w
omen
and
wom
en in
chi
ld
bear
ing
age
- Adv
ocac
y to
incr
ease
mat
erni
ty le
ave
from
3 m
onth
s to
6 m
onth
s to
pro
mot
e ex
clus
ive
brea
st fe
edin
g -R
eviv
al o
f bab
y fri
endl
y ho
spita
ls
-Dis
sem
inat
ion
of I
YC
F m
essa
ges
such
as
early
initi
atio
n of
bre
ast f
eedi
ng, e
xclu
sive
br
east
feed
ing
Hea
lthy
com
plem
enta
ry
feed
ing
for b
abie
s m
ore
than
six
mon
ths
old
- Adm
inis
tratio
n of
nut
ritio
us fo
od
supp
lem
ents
from
hig
h ris
k sc
hool
s - A
nnua
l scr
eeni
ng o
f sch
ool c
hild
ren
to
prev
ent n
utrit
iona
l pro
blem
at a
n ea
rly
stag
e -E
stab
lishm
ent o
f the
rape
utic
feed
ing
prog
ram
in th
e re
ferra
l car
e fa
cilit
ies
Mar
ch 2
014
DoH
Al
l sta
keho
lder
s I
TBD
1.2
Est
ablis
h a
intra
-sec
tora
l tas
k fo
rce
to id
entif
y lin
kage
s an
d
area
of m
utua
l rei
nfor
cem
ent
and
ther
eby
redu
ce in
tra-
sect
oral
frag
men
tatio
n
Man
agem
ent p
roto
cols
ens
ures
con
tinui
ty
of c
are
acro
ss d
iffer
ent s
ub s
ecto
rs o
f he
alth
Stan
dard
ized
and
har
mon
ized
indi
cato
rs
2013
(upo
n ap
prov
al o
f th
e In
ter-
sect
oral
nu
tritio
n
DoH
Popu
latio
n W
elfa
re
All
Sup
port
Sec
tor L
HW
s,
CM
Ws,
EP
I, N
utrit
ion,
HS
RU
, P
WD
, (M
SU
and
1 TB
D
A
ctio
n O
utpu
t Ind
icat
or
Tim
e Le
ad
Dep
t.
Supp
ort
Dep
t. Pr
iorit
y
Bud
get
A
ctio
n A
rea
1: E
nabl
ing
envi
ronm
ent,
polic
y fr
amew
orks
, str
ateg
ies
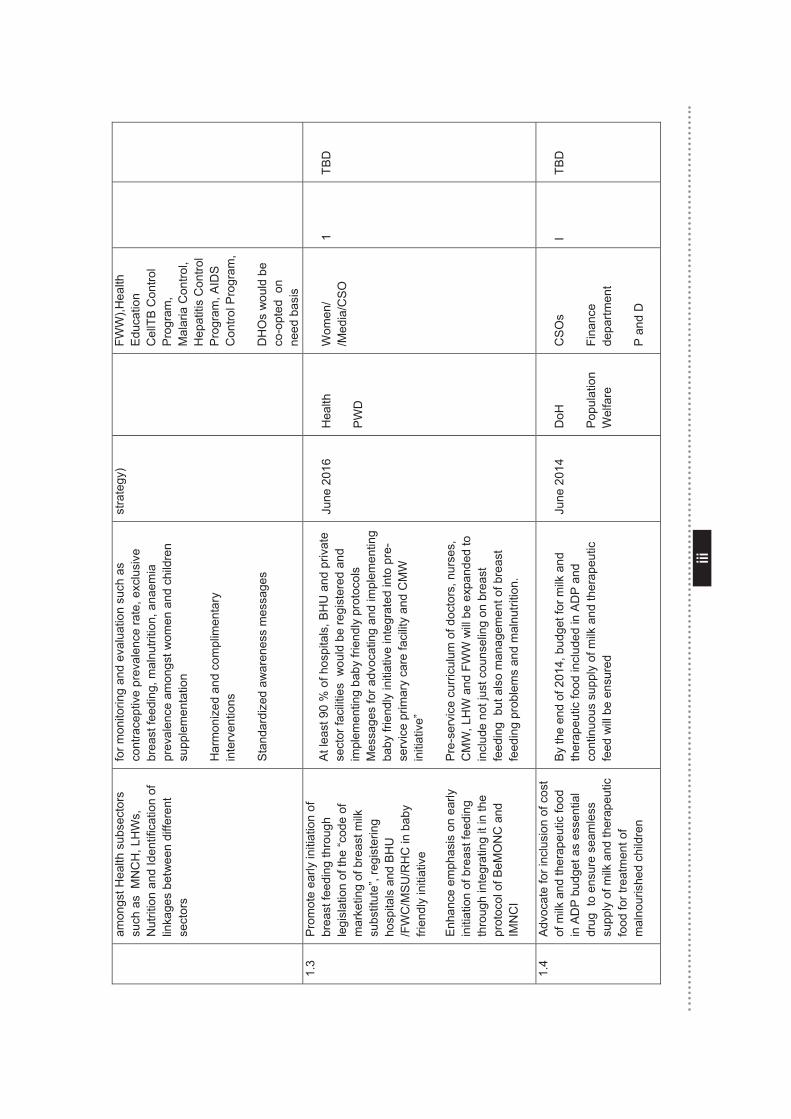
iii
iii
amon
gst H
ealth
sub
sect
ors
such
as
MN
CH
, LH
Ws,
N
utrit
ion
and
Iden
tific
atio
n of
lin
kage
s be
twee
n di
ffere
nt
sect
ors
for m
onito
ring
and
eval
uatio
n su
ch a
s co
ntra
cept
ive
prev
alen
ce ra
te, e
xclu
sive
br
east
feed
ing,
mal
nutri
tion,
ana
emia
pr
eval
ence
am
ongs
t wom
en a
nd c
hild
ren
supp
lem
enta
tion
Har
mon
ized
and
com
plim
enta
ry
inte
rven
tions
Stan
dard
ized
aw
aren
ess
mes
sage
s
stra
tegy
) FW
W),H
ealth
Ed
ucat
ion
Cel
lTB
Con
trol
Pro
gram
, M
alar
ia C
ontro
l, H
epat
itis
Con
trol
Pro
gram
, AID
S
Con
trol P
rogr
am,
DH
Os
wou
ld b
e co
-opt
ed o
n ne
ed b
asis
1.
3 P
rom
ote
early
initi
atio
n of
br
east
feed
ing
thro
ugh
legi
slat
ion
of th
e “c
ode
of
mar
ketin
g of
bre
ast m
ilk
subs
titut
e”, r
egis
terin
g ho
spita
ls a
nd B
HU
/F
WC
/MS
U/R
HC
in b
aby
frien
dly
initi
ativ
e
Enha
nce
emph
asis
on
early
in
itiat
ion
of b
reas
t fee
ding
th
roug
h in
tegr
atin
g it
in th
e pr
otoc
ol o
f BeM
ON
C a
nd
IMN
CI
At l
east
90
% o
f hos
pita
ls, B
HU
and
priv
ate
sect
or fa
cilit
ies
wou
ld b
e re
gist
ered
and
im
plem
entin
g ba
by fr
iend
ly p
roto
cols
M
essa
ges
for a
dvoc
atin
g an
d im
plem
entin
g ba
by fr
iend
ly in
itiat
ive
inte
grat
ed in
to p
re-
serv
ice
prim
ary
care
faci
lity
and
CM
W
initi
ativ
e”
Pre
-ser
vice
cur
ricul
um o
f doc
tors
, nur
ses,
C
MW
, LH
W a
nd F
WW
will
be
expa
nded
to
incl
ude
not j
ust c
ouns
elin
g on
bre
ast
feed
ing
but
als
o m
anag
emen
t of b
reas
t fe
edin
g pr
oble
ms
and
mal
nutri
tion.
June
201
6 H
ealth
PW
D
Wom
en/
/Med
ia/C
SO
1
TBD
1.4
Adv
ocat
e fo
r inc
lusi
on o
f cos
t of
milk
and
ther
apeu
tic fo
od
in A
DP
bud
get a
s es
sent
ial
drug
to
ensu
re s
eam
less
su
pply
of m
ilk a
nd th
erap
eutic
fo
od fo
r tre
atm
ent o
f m
alno
uris
hed
child
ren
By
the
end
of 2
014,
bud
get f
or m
ilk a
nd
ther
apeu
tic fo
od in
clud
ed in
AD
P a
nd
cont
inuo
us s
uppl
y of
milk
and
ther
apeu
tic
feed
will
be
ensu
red
June
201
4
DoH
Popu
latio
n W
elfa
re
CS
Os
Fina
nce
depa
rtmen
t
P an
d D
I TB
D
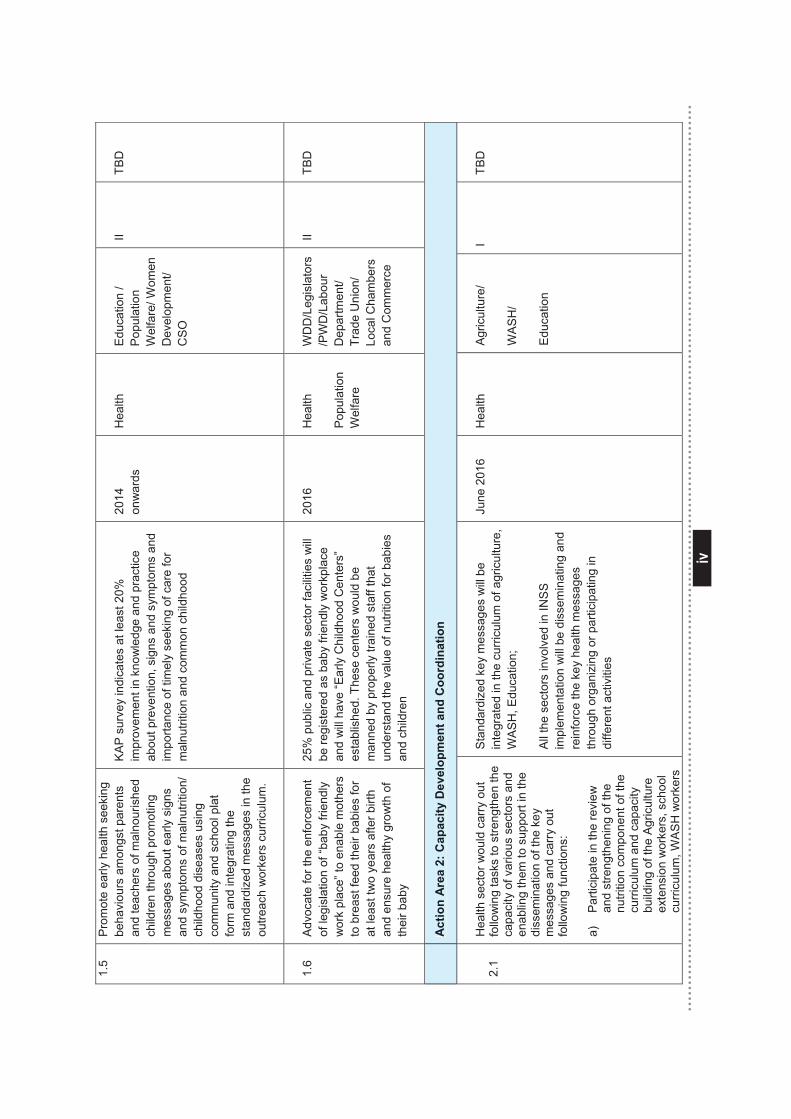
iv
iv
1.5
Prom
ote
early
hea
lth s
eeki
ng
beha
viou
rs a
mon
gst p
aren
ts
and
teac
hers
of m
alno
uris
hed
child
ren
thro
ugh
prom
otin
g m
essa
ges
abou
t ear
ly s
igns
an
d sy
mpt
oms
of m
alnu
tritio
n/
child
hood
dis
ease
s us
ing
com
mun
ity a
nd s
choo
l pla
t fo
rm a
nd in
tegr
atin
g th
e st
anda
rdiz
ed m
essa
ges
in th
e ou
treac
h w
orke
rs c
urric
ulum
.
KA
P s
urve
y in
dica
tes
at le
ast 2
0%
impr
ovem
ent i
n kn
owle
dge
and
prac
tice
abou
t pre
vent
ion,
sig
ns a
nd s
ympt
oms
and
impo
rtanc
e of
tim
ely
seek
ing
of c
are
for
mal
nutri
tion
and
com
mon
chi
ldho
od
2014
on
war
ds
Hea
lth
Edu
catio
n /
Popu
latio
n W
elfa
re/ W
omen
D
evel
opm
ent/
CS
O
II TB
D
1.6
Adv
ocat
e fo
r the
enf
orce
men
t of
legi
slat
ion
of “b
aby
frien
dly
wor
k pl
ace”
to e
nabl
e m
othe
rs
to b
reas
t fee
d th
eir b
abie
s fo
r at
leas
t tw
o ye
ars
afte
r birt
h an
d en
sure
hea
lthy
grow
th o
f th
eir b
aby
25%
pub
lic a
nd p
rivat
e se
ctor
faci
litie
s w
ill
be re
gist
ered
as
baby
frie
ndly
wor
kpla
ce
and
will
hav
e “E
arly
Chi
ldho
od C
ente
rs”
esta
blis
hed.
The
se c
ente
rs w
ould
be
man
ned
by p
rope
rly tr
aine
d st
aff t
hat
unde
rsta
nd th
e va
lue
of n
utrit
ion
for b
abie
s an
d ch
ildre
n
2016
H
ealth
Popu
latio
n W
elfa
re
WD
D/L
egis
lato
rs/P
WD
/Lab
our
Dep
artm
ent/
Trad
e U
nion
/ Lo
cal C
ham
bers
an
d C
omm
erce
II TB
D
A
ctio
n A
rea
2: C
apac
ity D
evel
opm
ent a
nd C
oord
inat
ion
2.1
Hea
lth s
ecto
r wou
ld c
arry
out
fo
llow
ing
task
s to
stre
ngth
en th
e ca
paci
ty o
f var
ious
sec
tors
and
en
ablin
g th
em to
sup
port
in th
e di
ssem
inat
ion
of th
e ke
y m
essa
ges
and
carr
y ou
t fo
llow
ing
func
tions
:
a)
Par
ticip
ate
in th
e re
view
an
d st
reng
then
ing
of th
e nu
tritio
n co
mpo
nent
of t
he
curri
culu
m a
nd c
apac
ity
build
ing
of th
e Ag
ricul
ture
ex
tens
ion
wor
kers
, sch
ool
curr
icul
um, W
AS
H w
orke
rs
Stan
dard
ized
key
mes
sage
s w
ill b
e in
tegr
ated
in th
e cu
rricu
lum
of a
gric
ultu
re,
WA
SH
, Edu
catio
n;
All
the
sect
ors
invo
lved
in IN
SS
im
plem
enta
tion
will
be
diss
emin
atin
g an
d re
info
rce
the
key
heal
th m
essa
ges
thro
ugh
orga
nizi
ng o
r par
ticip
atin
g in
di
ffere
nt a
ctiv
ities
June
201
6 H
ealth
Ag
ricul
ture
/
WA
SH
/
Edu
catio
n
I TB
D
Act
ion
Are
a 2:
Cap
acity
Dev
elop
men
t and
Coo
rdin
atio
n
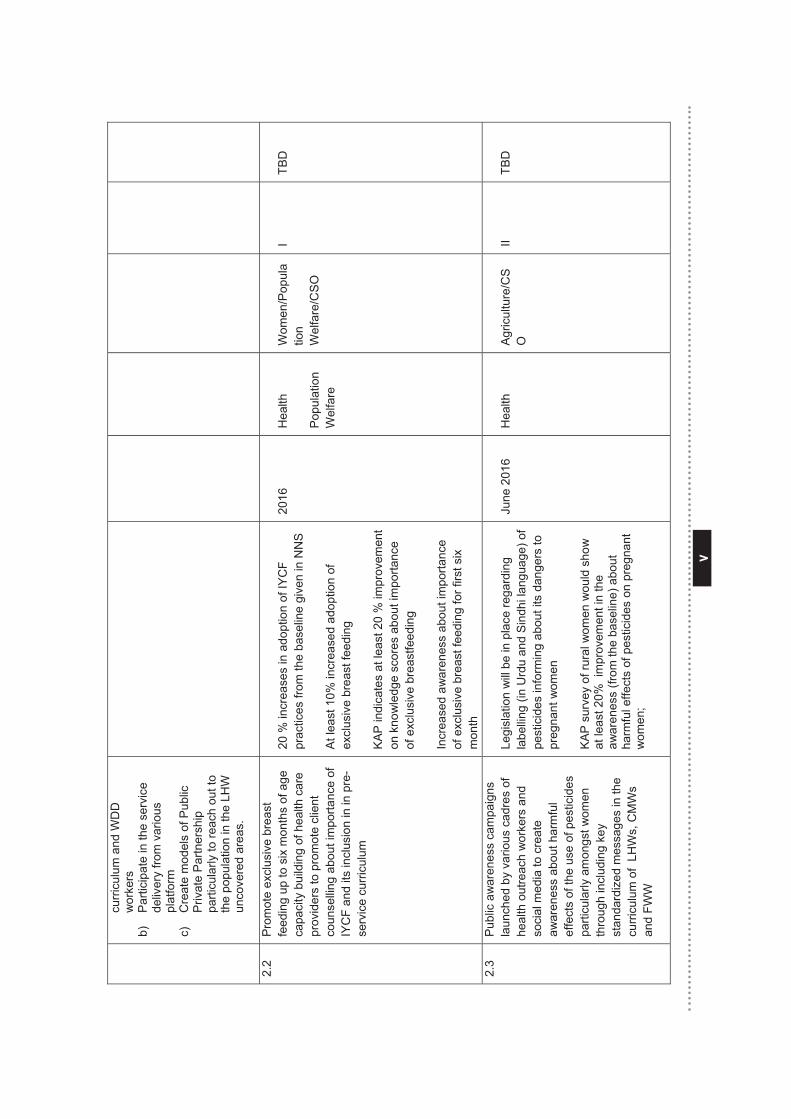
v
v
curr
icul
um a
nd W
DD
w
orke
rs
b)
Par
ticip
ate
in th
e se
rvic
e de
liver
y fro
m v
ario
us
plat
form
c)
C
reat
e m
odel
s of
Pub
lic
Priv
ate
Par
tner
ship
pa
rticu
larly
to re
ach
out t
o th
e po
pula
tion
in th
e LH
W
unco
vere
d ar
eas.
2.2
Pro
mot
e ex
clus
ive
brea
st
feed
ing
up to
six
mon
ths
of a
ge
capa
city
bui
ldin
g of
hea
lth c
are
prov
ider
s to
pro
mot
e cl
ient
co
unse
lling
abo
ut im
porta
nce
of
IYC
F an
d its
incl
usio
n in
in p
re-
serv
ice
curri
culu
m
20 %
incr
ease
s in
ado
ptio
n of
IYC
F pr
actic
es fr
om th
e ba
selin
e gi
ven
in N
NS
At l
east
10%
incr
ease
d ad
optio
n of
ex
clus
ive
brea
st fe
edin
g
KA
P in
dica
tes
at le
ast 2
0 %
impr
ovem
ent
on k
now
ledg
e sc
ores
abo
ut im
porta
nce
of e
xclu
sive
bre
astfe
edin
g
Incr
ease
d aw
aren
ess
abou
t im
porta
nce
of e
xclu
sive
bre
ast f
eedi
ng fo
r firs
t six
m
onth
2016
H
ealth
Popu
latio
n W
elfa
re
Wom
en/P
opul
atio
n W
elfa
re/C
SO
I TB
D
2.3
Publ
ic a
war
enes
s ca
mpa
igns
la
unch
ed b
y va
rious
cad
res
of
heal
th o
utre
ach
wor
kers
and
so
cial
med
ia to
cre
ate
awar
enes
s ab
out h
arm
ful
effe
cts
of th
e us
e of
pes
ticid
es
parti
cula
rly a
mon
gst w
omen
th
roug
h in
clud
ing
key
stan
dard
ized
mes
sage
s in
the
curr
icul
um o
f LH
Ws,
CM
Ws
and
FWW
Legi
slat
ion
will
be
in p
lace
rega
rdin
g la
belli
ng (i
n U
rdu
and
Sind
hi la
ngua
ge) o
f pe
stic
ides
info
rmin
g ab
out i
ts d
ange
rs to
pr
egna
nt w
omen
KA
P s
urve
y of
rura
l wom
en w
ould
sho
w
at le
ast 2
0% i
mpr
ovem
ent i
n th
e aw
aren
ess
(from
the
base
line)
abo
ut
harm
ful e
ffect
s of
pes
ticid
es o
n pr
egna
nt
wom
en;
June
201
6 H
ealth
Ag
ricul
ture
/CS
O
II TB
D
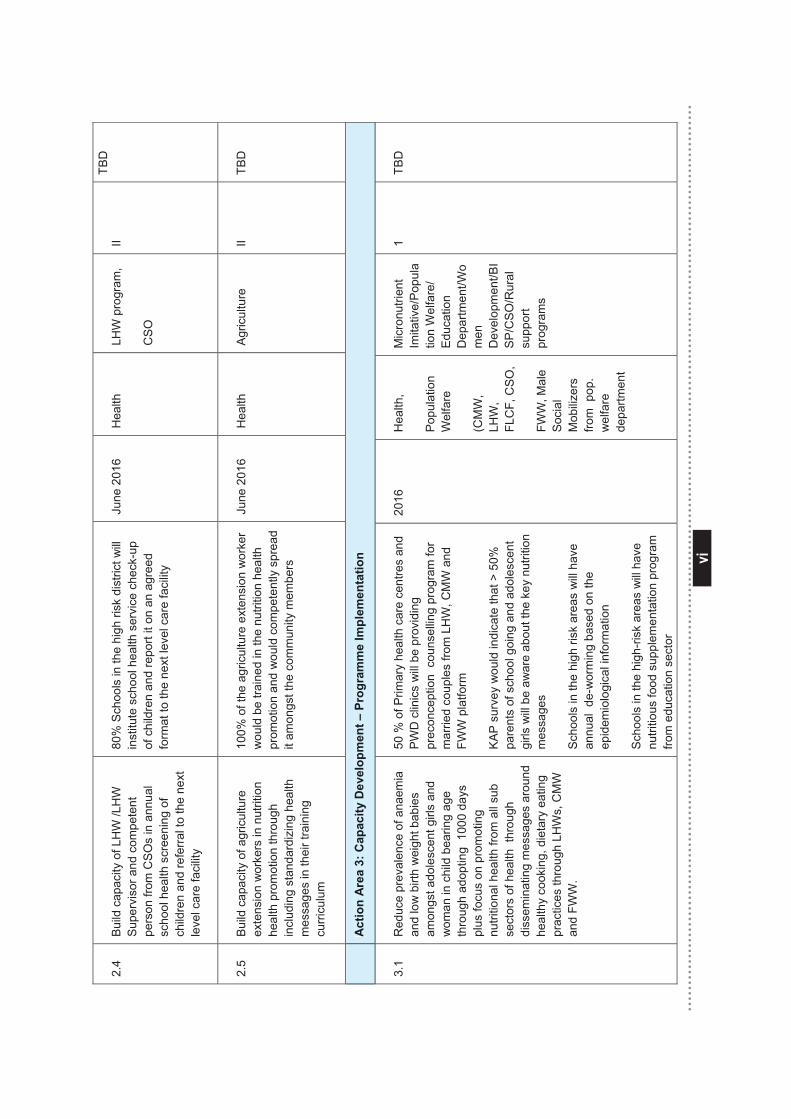
vi
vi
2.4
Build
cap
acity
of L
HW
/LH
W
Sup
ervi
sor a
nd c
ompe
tent
pe
rson
from
CS
Os
in a
nnua
l sc
hool
hea
lth s
cree
ning
of
child
ren
and
refe
rral t
o th
e ne
xt
leve
l car
e fa
cilit
y
80%
Sch
ools
in th
e hi
gh ri
sk d
istri
ct w
ill
inst
itute
sch
ool h
ealth
ser
vice
che
ck-u
p of
chi
ldre
n an
d re
port
it on
an
agre
ed
form
at to
the
next
leve
l car
e fa
cilit
y
June
201
6 H
ealth
LH
W p
rogr
am,
CS
O
II TB
D
2.5
Bui
ld c
apac
ity o
f agr
icul
ture
ex
tens
ion
wor
kers
in n
utrit
ion
heal
th p
rom
otio
n th
roug
h in
clud
ing
stan
dard
izin
g he
alth
m
essa
ges
in th
eir t
rain
ing
curri
culu
m
100%
of t
he a
gric
ultu
re e
xten
sion
wor
ker
wou
ld b
e tra
ined
in th
e nu
tritio
n he
alth
pr
omot
ion
and
wou
ld c
ompe
tent
ly s
prea
d it
amon
gst t
he c
omm
unity
mem
bers
June
201
6 H
ealth
Ag
ricul
ture
II
TBD
A
ctio
n A
rea
3: C
apac
ity D
evel
opm
ent –
Pro
gram
me
Impl
emen
tatio
n
3.1
Red
uce
prev
alen
ce o
f ana
emia
an
d lo
w b
irth
wei
ght b
abie
s am
ongs
t ado
lesc
ent g
irls
and
wom
an in
chi
ld b
earin
g ag
e th
roug
h ad
optin
g 1
000
days
pl
us fo
cus
on p
rom
otin
g nu
tritio
nal h
ealth
from
all
sub
sect
ors
of h
ealth
thr
ough
di
ssem
inat
ing
mes
sage
s ar
ound
he
alth
y co
okin
g, d
ieta
ry e
atin
g pr
actic
es th
roug
h LH
Ws,
CM
W
and
FWW
.
50 %
of P
rimar
y he
alth
car
e ce
ntre
s an
d PW
D c
linic
s w
ill b
e pr
ovid
ing
pr
econ
cept
ion
cou
nsel
ling
prog
ram
for
mar
ried
coup
les
from
LH
W, C
MW
and
FW
W p
latfo
rm
KA
P s
urve
y w
ould
indi
cate
that
> 5
0%
pare
nts
of s
choo
l goi
ng a
nd a
dole
scen
t gi
rls w
ill b
e aw
are
abou
t the
key
nut
ritio
n m
essa
ges
Sch
ools
in th
e hi
gh ri
sk a
reas
will
hav
e an
nual
de-
wor
min
g ba
sed
on th
e ep
idem
iolo
gica
l inf
orm
atio
n
Sch
ools
in th
e hi
gh-ri
sk a
reas
will
hav
e nu
tritio
us fo
od s
uppl
emen
tatio
n pr
ogra
m
from
edu
catio
n se
ctor
2016
Hea
lth,
Popu
latio
n W
elfa
re
(CM
W,
LHW
, FL
CF,
CS
O,
FWW
, Mal
e S
ocia
l M
obili
zers
fro
m p
op.
wel
fare
de
partm
ent
Mic
ronu
trien
t Im
itativ
e/P
opul
atio
n W
elfa
re/
Educ
atio
n D
epar
tmen
t/Wo
men
D
evel
opm
ent/B
IS
P/C
SO
/Rur
al
supp
ort
prog
ram
s
1 TB
D
Act
ion
Are
a 3:
Cap
acity
Dev
elop
men
t – P
rogr
amm
e Im
plem
enta
tion
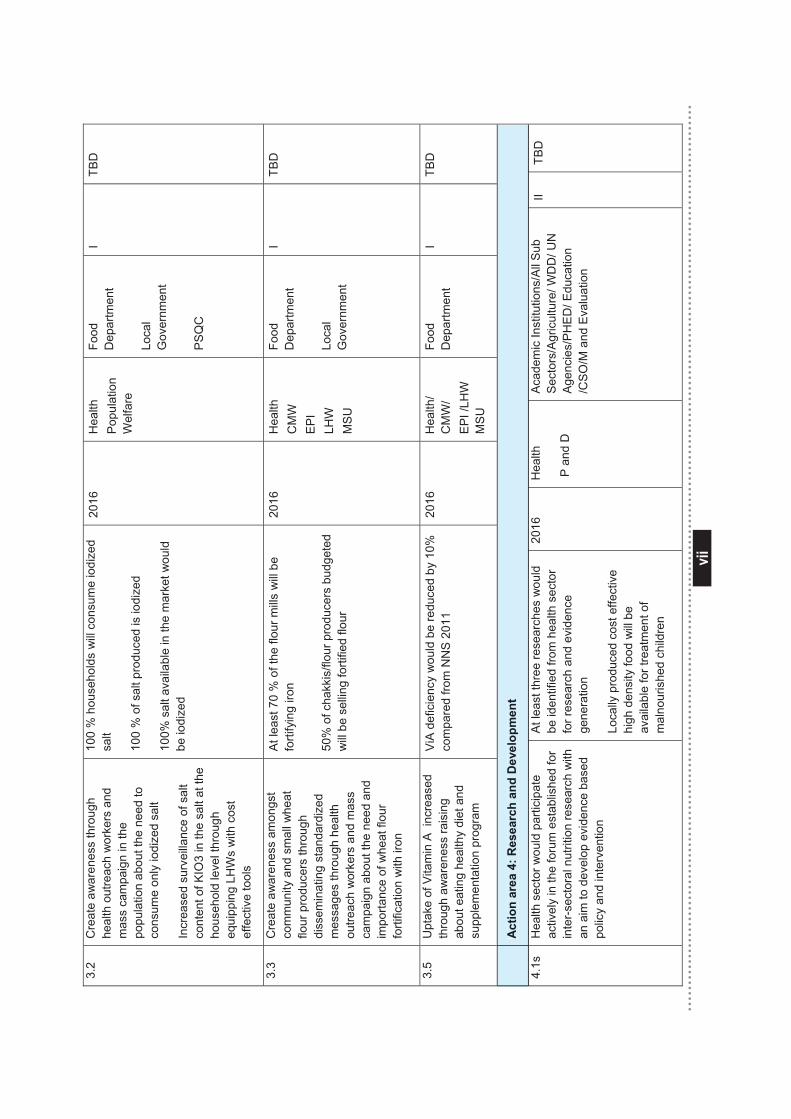
vii
vii
3.2
Cre
ate
awar
enes
s th
roug
h he
alth
out
reac
h w
orke
rs a
nd
mas
s ca
mpa
ign
in th
e po
pula
tion
abou
t the
nee
d to
co
nsum
e on
ly io
dize
d sa
lt
Incr
ease
d su
rvei
llanc
e of
sal
t co
nten
t of K
IO3
in th
e sa
lt at
the
hous
ehol
d le
vel t
hrou
gh
equi
ppin
g LH
Ws
with
cos
t ef
fect
ive
tool
s
100
% h
ouse
hold
s w
ill c
onsu
me
iodi
zed
salt
100
% o
f sal
t pro
duce
d is
iodi
zed
100%
sal
t ava
ilabl
e in
the
mar
ket w
ould
be
iodi
zed
2016
H
ealth
Po
pula
tion
Wel
fare
Food
D
epar
tmen
t Lo
cal
Gov
ernm
ent
PS
QC
I TB
D
3.3
Cre
ate
awar
enes
s am
ongs
t co
mm
unity
and
sm
all w
heat
flo
ur p
rodu
cers
thro
ugh
diss
emin
atin
g st
anda
rdiz
ed
mes
sage
s th
roug
h he
alth
ou
treac
h w
orke
rs a
nd m
ass
cam
paig
n ab
out t
he n
eed
and
impo
rtanc
e of
whe
at fl
our
forti
ficat
ion
with
iron
At l
east
70
% o
f the
flou
r mills
will
be
forti
fyin
g iro
n
50%
of c
hakk
is/fl
our p
rodu
cers
bud
gete
d w
ill b
e se
lling
forti
fied
flour
2016
H
ealth
C
MW
E
PI
LHW
M
SU
Food
D
epar
tmen
t Lo
cal
Gov
ernm
ent
I TB
D
3.5
Upt
ake
of V
itam
in A
inc
reas
ed
thro
ugh
awar
enes
s ra
isin
g ab
out e
atin
g he
alth
y di
et a
nd
supp
lem
enta
tion
prog
ram
ViA
defic
ienc
y w
ould
be
redu
ced
by 1
0%
com
pare
d fro
m N
NS
201
1 20
16
Hea
lth/
CM
W/
EP
I /LH
W
MS
U
Food
D
epar
tmen
t
I TB
D
A
ctio
n ar
ea 4
: Res
earc
h an
d D
evel
opm
ent
4.1s
H
ealth
sec
tor w
ould
par
ticip
ate
activ
ely
in th
e fo
rum
est
ablis
hed
for
inte
r-sec
tora
l nut
ritio
n re
sear
ch w
ith
an a
im to
dev
elop
evi
denc
e ba
sed
polic
y an
d in
terv
entio
n
At l
east
thre
e re
sear
ches
wou
ld
be id
entif
ied
from
hea
lth s
ecto
r fo
r res
earc
h an
d ev
iden
ce
gene
ratio
n
Loca
lly p
rodu
ced
cost
effe
ctiv
e hi
gh d
ensi
ty fo
od w
ill b
e av
aila
ble
for t
reat
men
t of
mal
nour
ishe
d ch
ildre
n
2016
H
ealth
P a
nd D
Aca
dem
ic In
stitu
tions
/All
Sub
S
ecto
rs/A
gric
ultu
re/ W
DD
/ UN
A
genc
ies/
PH
ED
/ Edu
catio
n /C
SO
/M a
nd E
valu
atio
n
II TB
D
Act
ion
area
4: R
esea
rch
and
Dev
elop
men
t
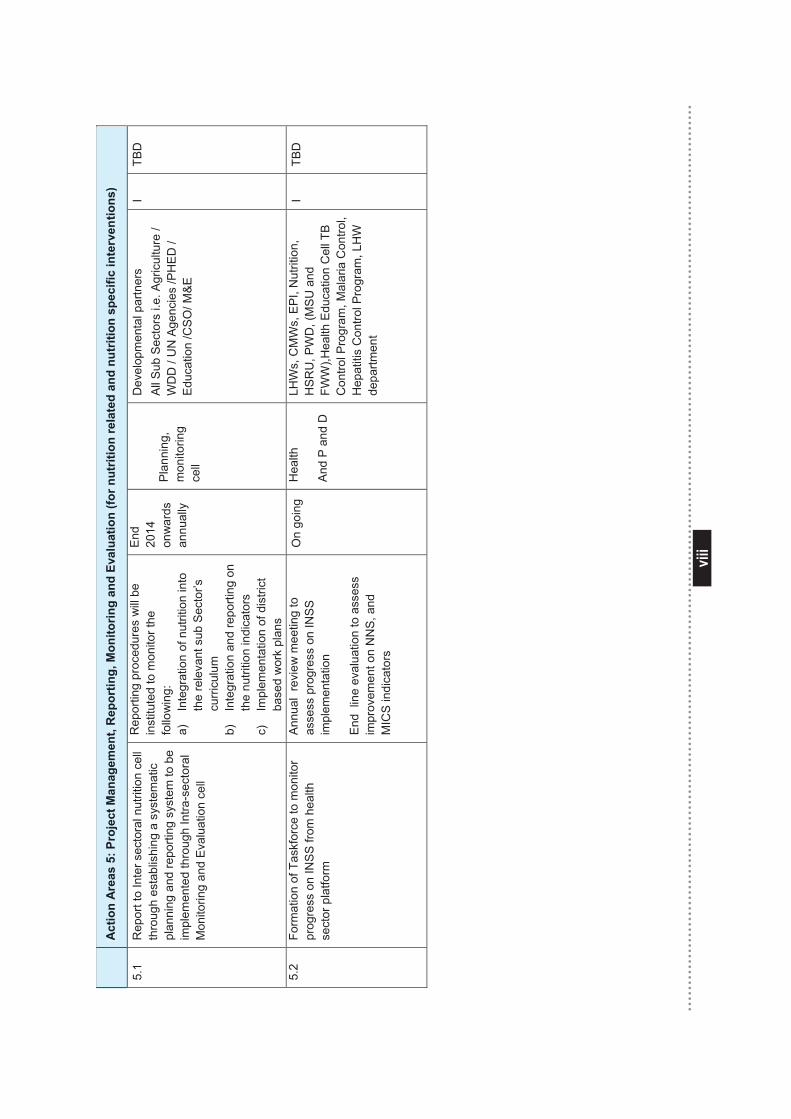
viii
viii
A
ctio
n A
reas
5: P
roje
ct M
anag
emen
t, R
epor
ting,
Mon
itorin
g an
d Ev
alua
tion
(for n
utrit
ion
rela
ted
and
nutr
ition
spe
cific
inte
rven
tions
)
5.1
Rep
ort t
o In
ter s
ecto
ral n
utrit
ion
cell
thro
ugh
esta
blis
hing
a s
yste
mat
ic
plan
ning
and
repo
rting
sys
tem
to b
e im
plem
ente
d th
roug
h In
tra-s
ecto
ral
Mon
itorin
g an
d Ev
alua
tion
cell
Rep
ortin
g pr
oced
ures
will
be
inst
itute
d to
mon
itor t
he
follo
win
g:
a)
Inte
grat
ion
of n
utrit
ion
into
th
e re
leva
nt s
ub S
ecto
r’s
curri
culu
m
b)
Inte
grat
ion
and
repo
rting
on
the
nutri
tion
indi
cato
rs
c)
Impl
emen
tatio
n of
dis
trict
ba
sed
wor
k pl
ans
End
2014
on
war
ds
annu
ally
Pla
nnin
g,
mon
itorin
g ce
ll
Dev
elop
men
tal p
artn
ers
All
Sub
Sec
tors
i.e.
Agr
icul
ture
/ W
DD
/ U
N A
genc
ies
/PH
ED
/ E
duca
tion
/CS
O/ M
&E
I TB
D
5.2
Form
atio
n of
Tas
kfor
ce to
mon
itor
prog
ress
on
INS
S fr
om h
ealth
se
ctor
pla
tform
Ann
ual
revi
ew m
eetin
g to
as
sess
pro
gres
s on
INS
S
impl
emen
tatio
n
End
lin
e ev
alua
tion
to a
sses
s im
prov
emen
t on
NN
S, a
nd
MIC
S in
dica
tors
On
goin
g H
ealth
And
P an
d D
LHW
s, C
MW
s, E
PI,
Nut
ritio
n,
HS
RU
, PW
D, (
MS
U a
nd
FWW
),Hea
lth E
duca
tion
Cel
l TB
Con
trol P
rogr
am, M
alar
ia C
ontro
l, H
epat
itis
Con
trol P
rogr
am, L
HW
de
partm
ent
I TB
D
Act
ion
Are
as 5
: Pro
ject
Man
agem
ent,
Rep
ortin
g, M
onito
ring
and
Eval
uatio
n (fo
r nut
ritio
n re
late
d an
d nu
triti
on s
peci
fic in
terv
entio
ns)
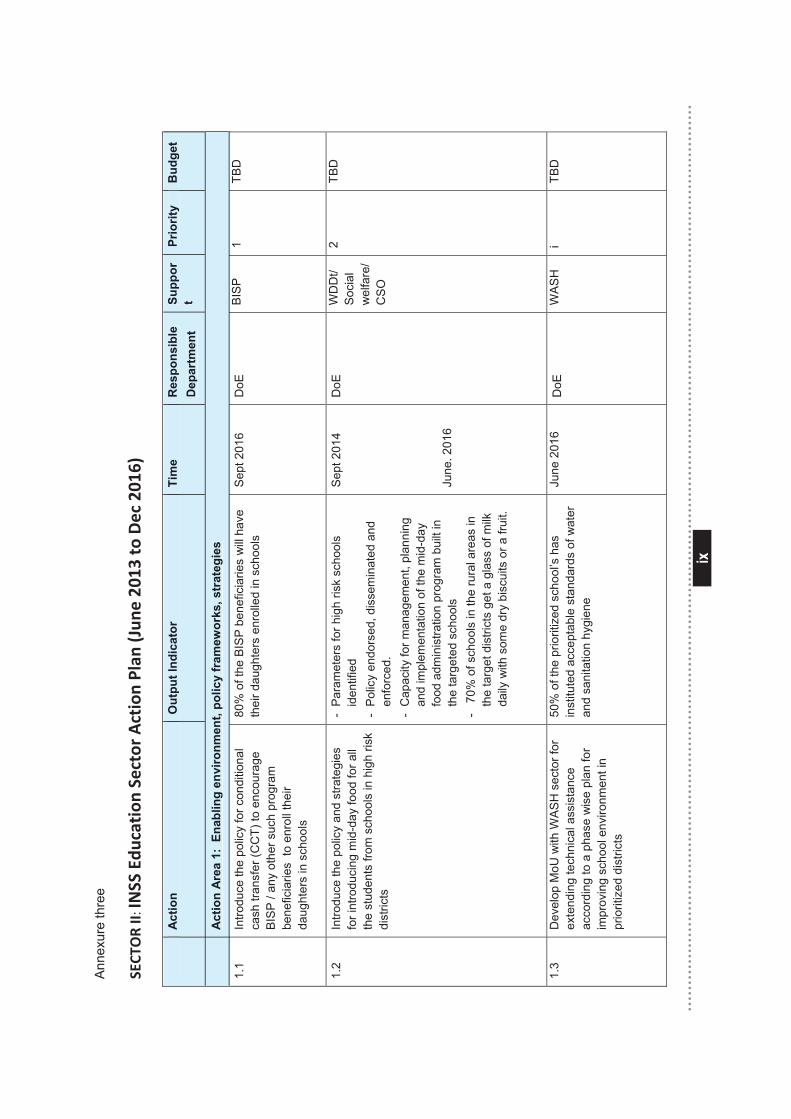
ix
ix
Ann
exur
e th
ree
SECT
OR II: IN
SS Edu
cation
Sector Action Plan
(Jun
e 20
13 to Dec 201
6)
A
ctio
n O
utpu
t Ind
icat
or
Tim
e R
espo
nsib
le
Dep
artm
ent
Supp
ort
Prio
rity
B
udge
t
A
ctio
n A
rea
1: E
nabl
ing
envi
ronm
ent,
polic
y fr
amew
orks
, str
ateg
ies
1.1
Intro
duce
the
polic
y fo
r con
ditio
nal
cash
tran
sfer
(CC
T) to
enc
oura
ge
BIS
P /
any
othe
r suc
h pr
ogra
m
bene
ficia
ries
to e
nrol
l the
ir da
ught
ers
in s
choo
ls
80%
of t
he B
ISP
ben
efic
iarie
s w
ill h
ave
thei
r dau
ghte
rs e
nrol
led
in s
choo
ls
Sep
t 201
6 D
oE
BIS
P
1 TB
D
1.2
Intro
duce
the
polic
y an
d st
rate
gies
fo
r int
rodu
cing
mid
-day
food
for a
ll th
e st
uden
ts fr
om s
choo
ls in
hig
h ris
k di
stric
ts
- P
aram
eter
s fo
r hig
h ris
k sc
hool
s id
entif
ied
- Po
licy
endo
rsed
, dis
sem
inat
ed a
nd
enfo
rced
. -
Cap
acity
for m
anag
emen
t, pl
anni
ng
and
impl
emen
tatio
n of
the
mid
-day
fo
od a
dmin
istra
tion
prog
ram
bui
lt in
th
e ta
rget
ed s
choo
ls
- 7
0% o
f sch
ools
in th
e ru
ral a
reas
in
the
targ
et d
istri
cts
get a
gla
ss o
f milk
da
ily w
ith s
ome
dry
bisc
uits
or a
frui
t.
Sep
t 201
4 Ju
ne. 2
016
DoE
WD
Dt/
Soc
ial
wel
fare
/ C
SO
2 TB
D
1.3
Dev
elop
MoU
with
WA
SH
sec
tor f
or
exte
ndin
g te
chni
cal a
ssis
tanc
e ac
cord
ing
to a
pha
se w
ise
plan
for
impr
ovin
g sc
hool
env
ironm
ent i
n pr
iorit
ized
dis
trict
s
50%
of t
he p
riorit
ized
sch
ool’s
has
in
stitu
ted
acce
ptab
le s
tand
ards
of w
ater
an
d sa
nita
tion
hygi
ene
June
201
6 D
oE
WA
SH
i
TBD
A
ctio
n O
utpu
t Ind
icat
or
Tim
e R
espo
nsib
le
Dep
artm
ent
Supp
ort
Prio
rity
B
udge
t
Act
ion
Are
a 1:
Ena
blin
g en
viro
nmen
t, po
licy
fram
ewor
ks, s
trat
egie
s
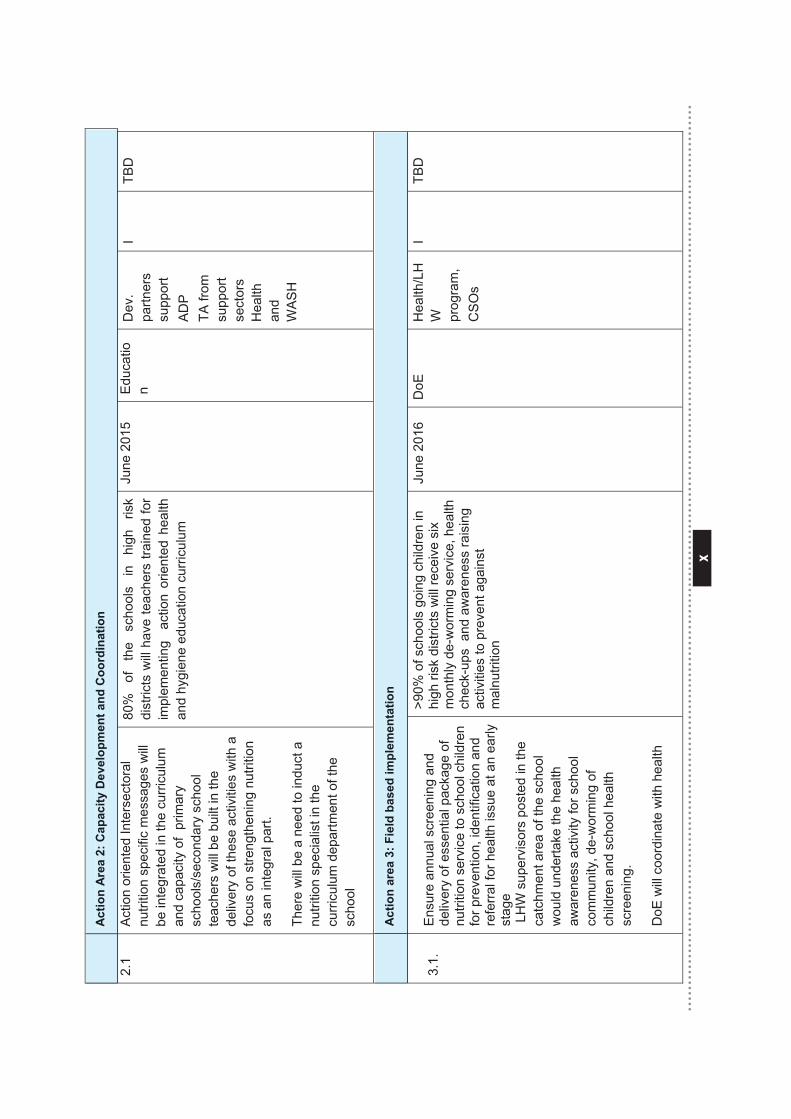
x
x
A
ctio
n A
rea
2: C
apac
ity D
evel
opm
ent a
nd C
oord
inat
ion
2.1
Act
ion
orie
nted
Inte
rsec
tora
l nu
tritio
n sp
ecifi
c m
essa
ges
will
be in
tegr
ated
in th
e cu
rric
ulum
an
d ca
paci
ty o
f pr
imar
y sc
hool
s/se
cond
ary
scho
ol
teac
hers
will
be b
uilt
in th
e de
liver
y of
thes
e ac
tiviti
es w
ith a
fo
cus
on s
treng
then
ing
nutri
tion
as a
n in
tegr
al p
art.
Ther
e w
ill b
e a
need
to in
duct
a
nutri
tion
spec
ialis
t in
the
curr
icul
um d
epar
tmen
t of t
he
scho
ol
80%
of
th
e sc
hool
s in
hi
gh
risk
dist
ricts
will
hav
e te
ache
rs tr
aine
d fo
r im
plem
entin
g a
ctio
n or
ient
ed h
ealth
an
d hy
gien
e ed
ucat
ion
curr
icul
um
June
201
5 E
duca
tion
Dev
. pa
rtner
s su
ppor
t A
DP
TA
from
su
ppor
t se
ctor
s H
ealth
an
d W
ASH
I TB
D
A
ctio
n ar
ea 3
: Fie
ld b
ased
impl
emen
tatio
n
3.1.
E
nsur
e an
nual
scr
eeni
ng a
nd
deliv
ery
of e
ssen
tial p
acka
ge o
f nu
tritio
n se
rvic
e to
sch
ool c
hild
ren
for p
reve
ntio
n, id
entif
icat
ion
and
refe
rral
for h
ealth
issu
e at
an
early
st
age
LH
W s
uper
viso
rs p
oste
d in
the
catc
hmen
t are
a of
the
scho
ol
wou
ld u
nder
take
the
heal
th
awar
enes
s ac
tivity
for s
choo
l co
mm
unity
, de-
wor
min
g of
ch
ildre
n an
d sc
hool
hea
lth
scre
enin
g.
DoE
will
coor
dina
te w
ith h
ealth
>90%
of s
choo
ls g
oing
chi
ldre
n in
hi
gh ri
sk d
istri
cts
will
rece
ive
six
mon
thly
de-
wor
min
g se
rvic
e, h
ealth
ch
eck-
ups
and
aw
aren
ess
rais
ing
activ
ities
to p
reve
nt a
gain
st
mal
nutri
tion
June
201
6 D
oE
Hea
lth/L
HW
pr
ogra
m,
CS
Os
I TB
D
Act
ion
Are
a 2:
Cap
acity
Dev
elop
men
t and
Coo
rdin
atio
n
Act
ion
area
3: F
ield
bas
ed im
plem
enta
tion
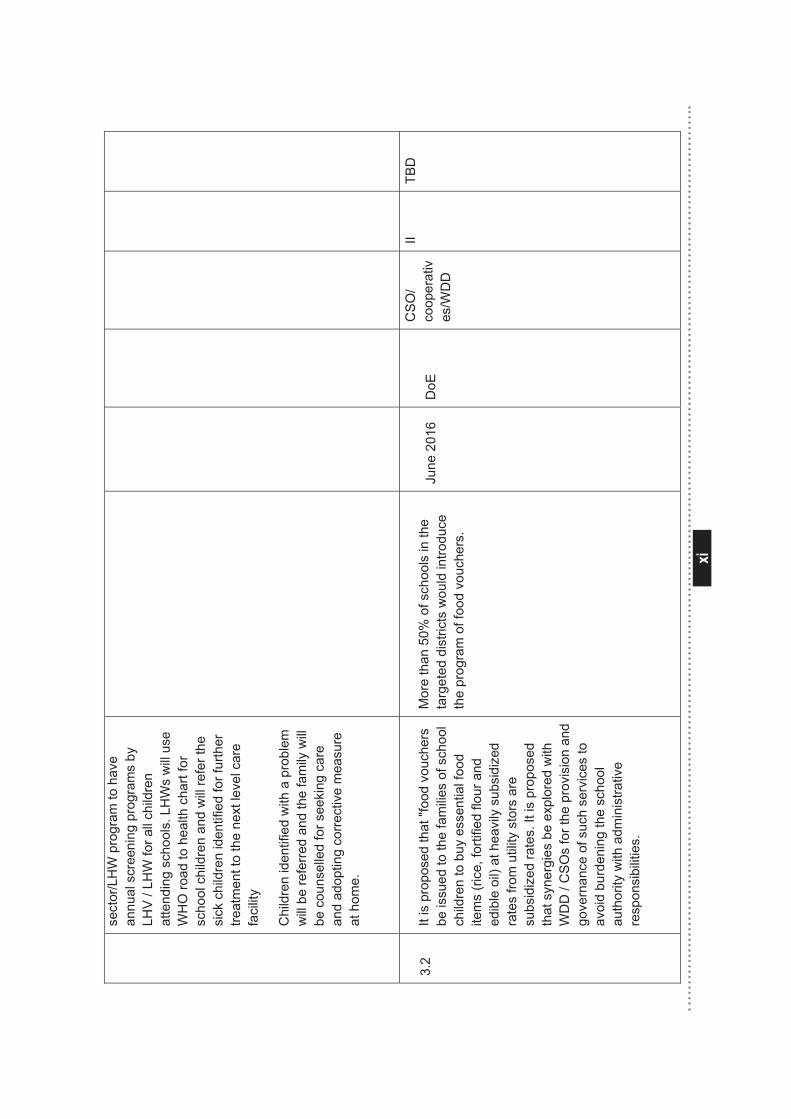
xi
xi
sect
or/L
HW
pro
gram
to h
ave
annu
al s
cree
ning
pro
gram
s by
LH
V /
LHW
for a
ll ch
ildre
n at
tend
ing
scho
ols.
LH
Ws
will
use
W
HO
road
to h
ealth
cha
rt fo
r sc
hool
chi
ldre
n an
d w
ill re
fer t
he
sick
chi
ldre
n id
entif
ied
for f
urth
er
treat
men
t to
the
next
leve
l car
e fa
cilit
y
Chi
ldre
n id
entif
ied
with
a p
robl
em
will
be
refe
rred
and
the
fam
ily w
ill
be c
ouns
elle
d fo
r see
king
car
e an
d ad
optin
g co
rrec
tive
mea
sure
at
hom
e.
3.
2 It
is p
ropo
sed
that
"foo
d vo
uche
rs
be is
sued
to th
e fa
mili
es o
f sch
ool
child
ren
to b
uy e
ssen
tial f
ood
item
s (r
ice,
forti
fied
flour
and
ed
ible
oil)
at h
eavi
ly s
ubsi
dize
d ra
tes
from
util
ity s
tors
are
su
bsid
ized
rate
s. It
is p
ropo
sed
that
syn
ergi
es b
e ex
plor
ed w
ith
WD
D /
CS
Os
for t
he p
rovi
sion
and
go
vern
ance
of s
uch
serv
ices
to
avoi
d bu
rden
ing
the
scho
ol
auth
ority
with
adm
inis
trativ
e re
spon
sibi
litie
s.
Mor
e th
an 5
0% o
f sch
ools
in th
e ta
rget
ed d
istri
cts
wou
ld in
trodu
ce
the
prog
ram
of f
ood
vouc
hers
.
June
201
6 D
oE
CS
O/
coop
erat
ives
/WD
D
II TB
D
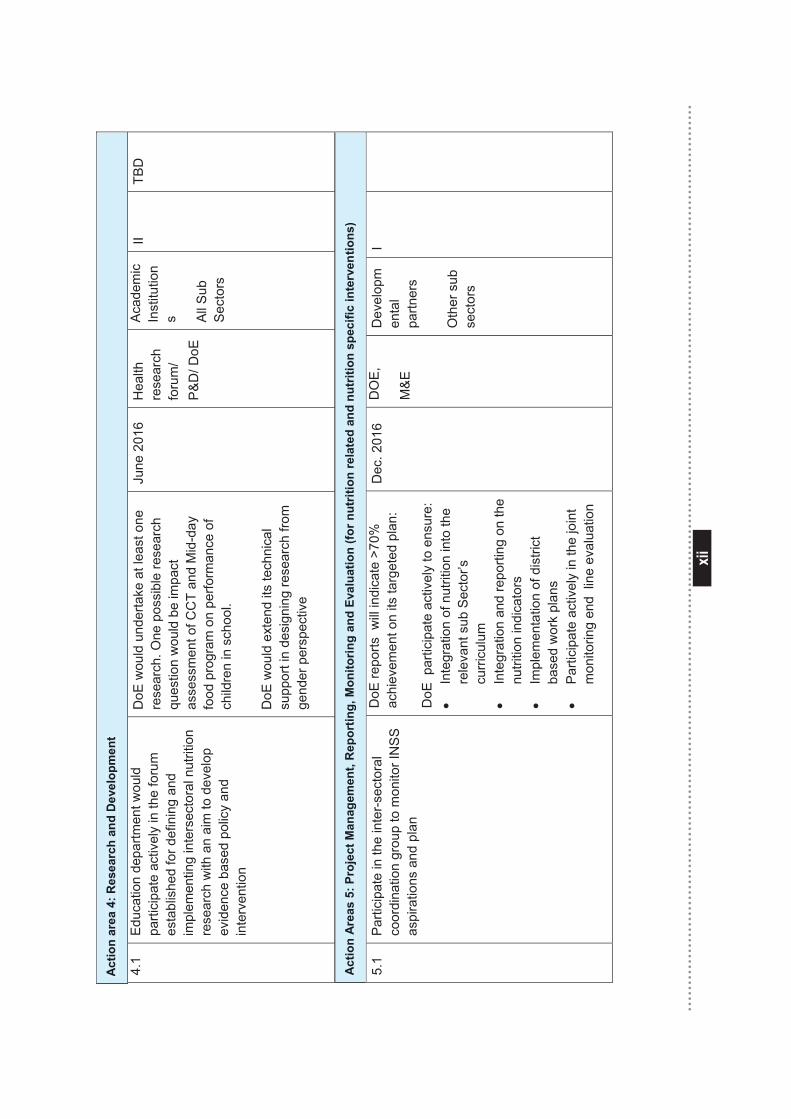
xii
xii
Act
ion
area
4: R
esea
rch
and
Dev
elop
men
t
4.1
Edu
catio
n de
partm
ent w
ould
pa
rtici
pate
act
ivel
y in
the
foru
m
esta
blis
hed
for d
efin
ing
and
impl
emen
ting
inte
rsec
tora
l nut
ritio
n re
sear
ch w
ith a
n ai
m to
dev
elop
ev
iden
ce b
ased
pol
icy
and
inte
rven
tion
DoE
wou
ld u
nder
take
at l
east
one
re
sear
ch. O
ne p
ossi
ble
rese
arch
qu
estio
n w
ould
be
impa
ct
asse
ssm
ent o
f CC
T an
d M
id-d
ay
food
pro
gram
on
perfo
rman
ce o
f ch
ildre
n in
sch
ool.
DoE
wou
ld e
xten
d its
tech
nica
l su
ppor
t in
desi
gnin
g re
sear
ch fr
om
gend
er p
ersp
ectiv
e
June
201
6 H
ealth
re
sear
ch
foru
m/
P&
D/ D
oE
Aca
dem
ic
Inst
itutio
ns A
ll S
ub
Sect
ors
II TB
D
Act
ion
Are
as 5
: Pro
ject
Man
agem
ent,
Rep
ortin
g, M
onito
ring
and
Eval
uatio
n (fo
r nut
ritio
n re
late
d an
d nu
triti
on s
peci
fic in
terv
entio
ns)
5.1
Par
ticip
ate
in th
e in
ter-
sect
oral
co
ordi
natio
n gr
oup
to m
onito
r IN
SS
as
pira
tions
and
pla
n
DoE
repo
rts w
ill in
dica
te >
70%
ac
hiev
emen
t on
its ta
rget
ed p
lan:
D
oE p
artic
ipat
e ac
tivel
y to
ens
ure:
•
Inte
grat
ion
of n
utrit
ion
into
the
rele
vant
sub
Sec
tor’s
cu
rric
ulum
•
Inte
grat
ion
and
repo
rting
on
the
nutri
tion
indi
cato
rs
• Im
plem
enta
tion
of d
istri
ct
base
d w
ork
plan
s •
Par
ticip
ate
activ
ely
in th
e jo
int
mon
itorin
g en
d li
ne e
valu
atio
n
Dec
. 201
6 D
OE
,
M&E
Dev
elop
men
tal
partn
ers
Oth
er s
ub
sect
ors
I
Act
ion
area
4: R
esea
rch
and
Dev
elop
men
t
Act
ion
Are
as 5
: Pro
ject
Man
agem
ent,
Rep
ortin
g, M
onito
ring
and
Eval
uatio
n (fo
r nut
ritio
n re
late
d an
d nu
triti
on s
peci
fic in
terv
entio
ns)
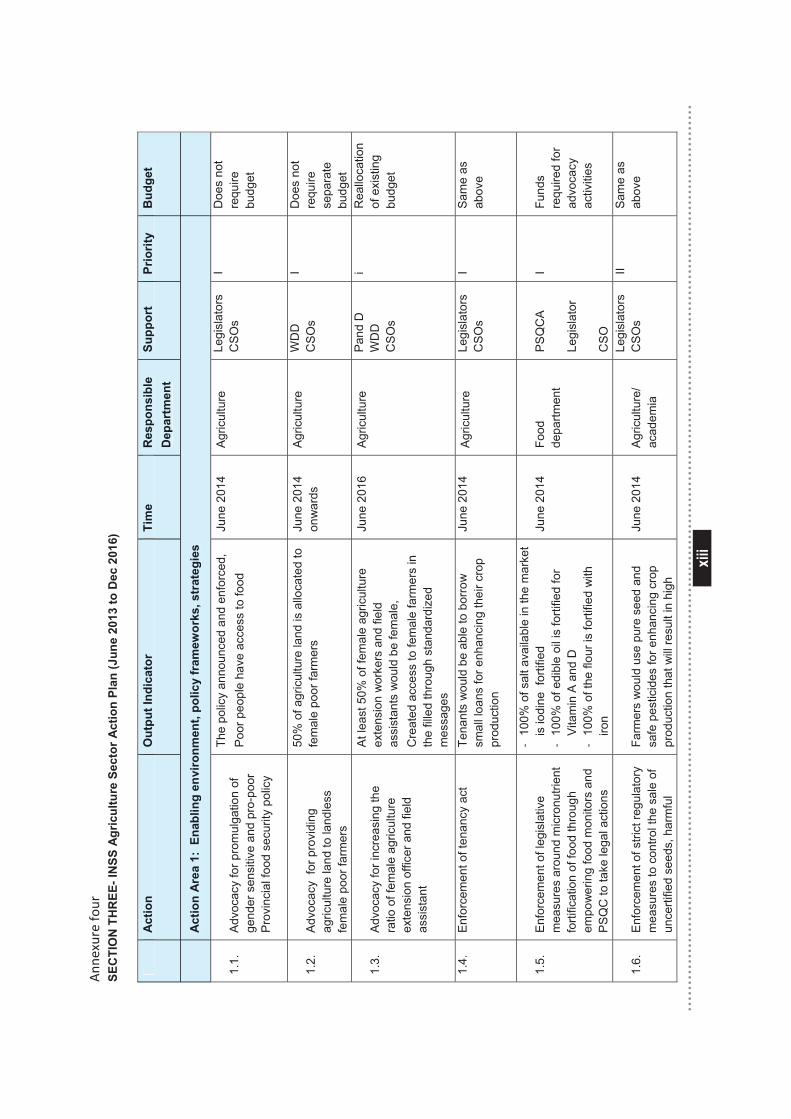
xiii
xiii
Ann
exure four
SEC
TIO
N T
HR
EE- I
NSS
Agr
icul
ture
Sec
tor A
ctio
n Pl
an (J
une
2013
to D
ec 2
016)
Act
ion
Out
put I
ndic
ator
Ti
me
Res
pons
ible
D
epar
tmen
t Su
ppor
t Pr
iorit
y
Bud
get
A
ctio
n A
rea
1: E
nabl
ing
envi
ronm
ent,
polic
y fr
amew
orks
, str
ateg
ies
1.1.
A
dvoc
acy
for p
rom
ulga
tion
of
gend
er s
ensi
tive
and
pro-
poor
P
rovi
ncia
l foo
d se
curit
y po
licy
The
polic
y an
noun
ced
and
enfo
rced
, P
oor p
eopl
e ha
ve a
cces
s to
food
Ju
ne 2
014
Agric
ultu
re
Legi
slat
ors
CS
Os
I D
oes
not
requ
ire
budg
et
1.2.
A
dvoc
acy
for p
rovi
ding
ag
ricul
ture
land
to la
ndle
ss
fem
ale
poor
farm
ers
50%
of a
gric
ultu
re la
nd is
allo
cate
d to
fe
mal
e po
or fa
rmer
s Ju
ne 2
014
onw
ards
Ag
ricul
ture
W
DD
C
SO
s I
Doe
s no
t re
quire
se
para
te
budg
et
1.3.
A
dvoc
acy
for i
ncre
asin
g th
e ra
tio o
f fem
ale
agric
ultu
re
exte
nsio
n of
ficer
and
fiel
d as
sist
ant
At l
east
50%
of f
emal
e ag
ricul
ture
ex
tens
ion
wor
kers
and
fiel
d as
sist
ants
wou
ld b
e fe
mal
e,
Cre
ated
acc
ess
to fe
mal
e fa
rmer
s in
th
e fil
led
thro
ugh
stan
dard
ized
m
essa
ges
June
201
6 Ag
ricul
ture
Pa
nd D
W
DD
C
SO
s
i R
eallo
catio
n of
exi
stin
g bu
dget
1.4.
E
nfor
cem
ent o
f ten
ancy
act
Te
nant
s w
ould
be
able
to b
orro
w
smal
l loa
ns fo
r enh
anci
ng th
eir c
rop
prod
uctio
n
June
201
4 A
gric
ultu
re
Legi
slat
ors
CS
Os
I S
ame
as
abov
e
1.5.
E
nfor
cem
ent o
f leg
isla
tive
mea
sure
s ar
ound
mic
ronu
trien
t fo
rtific
atio
n of
food
thro
ugh
empo
wer
ing
food
mon
itors
and
P
SQ
C to
take
lega
l act
ions
‐ 10
0% o
f sal
t ava
ilabl
e in
the
mar
ket
is io
dine
for
tifie
d
‐ 10
0% o
f edi
ble
oil i
s fo
rtifie
d fo
r Vi
tam
in A
and
D
‐ 10
0% o
f the
flou
r is
forti
fied
with
iro
n
June
201
4 Fo
od
depa
rtmen
t P
SQ
CA
Legi
slat
or
CS
O
I Fu
nds
requ
ired
for
advo
cacy
ac
tiviti
es
1.6.
E
nfor
cem
ent o
f stri
ct re
gula
tory
m
easu
res
to c
ontro
l the
sal
e of
un
certi
fied
seed
s, h
arm
ful
Farm
ers
wou
ld u
se p
ure
seed
and
sa
fe p
estic
ides
for e
nhan
cing
cro
p pr
oduc
tion
that
will
resu
lt in
hig
h
June
201
4 Ag
ricul
ture
/ ac
adem
ia
Legi
slat
ors
CS
Os
II S
ame
as
abov
e
A
ctio
n O
utpu
t Ind
icat
or
Tim
e R
espo
nsib
le
Dep
artm
ent
Supp
ort
Prio
rity
B
udge
t
Act
ion
Are
a 1:
Ena
blin
g en
viro
nmen
t, po
licy
fram
ewor
ks, s
trat
egie
s
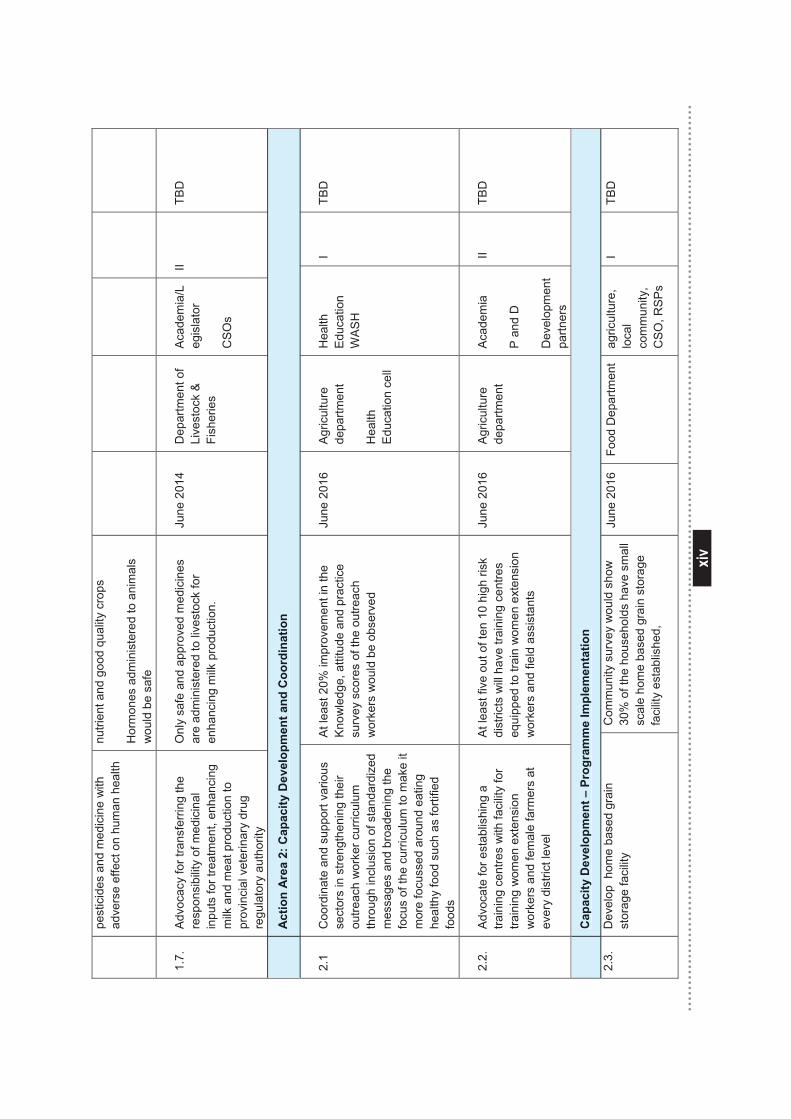
xiv
xiv
pest
icid
es a
nd m
edic
ine
with
ad
vers
e ef
fect
on
hum
an h
ealth
nu
trien
t and
goo
d qu
ality
cro
ps
Hor
mon
es a
dmin
iste
red
to a
nim
als
wou
ld b
e sa
fe
1.7.
A
dvoc
acy
for t
rans
ferri
ng th
e re
spon
sibi
lity
of m
edic
inal
in
puts
for t
reat
men
t, en
hanc
ing
milk
and
mea
t pro
duct
ion
to
prov
inci
al v
eter
inar
y dr
ug
regu
lato
ry a
utho
rity
Onl
y sa
fe a
nd a
ppro
ved
med
icin
es
are
adm
inis
tere
d to
live
stoc
k fo
r en
hanc
ing
milk
pro
duct
ion.
June
201
4 D
epar
tmen
t of
Live
stoc
k &
Fi
sher
ies
Aca
dem
ia/L
egis
lato
r
CS
Os
II TB
D
A
ctio
n A
rea
2: C
apac
ity D
evel
opm
ent a
nd C
oord
inat
ion
2.1
Coo
rdin
ate
and
supp
ort v
ario
us
sect
ors
in s
treng
then
ing
thei
r ou
treac
h w
orke
r cur
ricul
um
thro
ugh
incl
usio
n of
sta
ndar
dize
d m
essa
ges
and
broa
deni
ng th
e fo
cus
of th
e cu
rric
ulum
to m
ake
it m
ore
focu
ssed
aro
und
eatin
g he
alth
y fo
od s
uch
as fo
rtifie
d fo
ods
At l
east
20%
impr
ovem
ent i
n th
e K
now
ledg
e, a
ttitu
de a
nd p
ract
ice
surv
ey s
core
s of
the
outre
ach
wor
kers
wou
ld b
e ob
serv
ed
June
201
6 Ag
ricul
ture
de
partm
ent
Hea
lth
Educ
atio
n ce
ll
Hea
lth
Edu
catio
n W
AS
H
I TB
D
2.2.
A
dvoc
ate
for e
stab
lishi
ng a
tra
inin
g ce
ntre
s w
ith fa
cilit
y fo
r tra
inin
g w
omen
ext
ensi
on
wor
kers
and
fem
ale
farm
ers
at
ever
y di
stric
t lev
el
At l
east
five
out
of t
en 1
0 hi
gh ri
sk
dist
ricts
will
hav
e tra
inin
g ce
ntre
s eq
uipp
ed to
trai
n w
omen
ext
ensi
on
wor
kers
and
fiel
d as
sist
ants
June
201
6 Ag
ricul
ture
de
partm
ent
Acad
emia
P an
d D
Dev
elop
men
t pa
rtner
s
II TB
D
C
apac
ity D
evel
opm
ent –
Pro
gram
me
Impl
emen
tatio
n
2.3.
D
evel
op h
ome
base
d gr
ain
stor
age
faci
lity
Com
mun
ity s
urve
y w
ould
sho
w
30%
of t
he h
ouse
hold
s ha
ve s
mal
l sc
ale
hom
e ba
sed
grai
n st
orag
e fa
cilit
y es
tabl
ishe
d,
June
201
6 Fo
od D
epar
tmen
t ag
ricul
ture
, lo
cal
com
mun
ity,
CS
O, R
SP
s
I TB
D
Act
ion
Are
a 2:
Cap
acity
Dev
elop
men
t and
Coo
rdin
atio
n
Cap
acity
Dev
elop
men
t – P
rogr
amm
e Im
plem
enta
tion
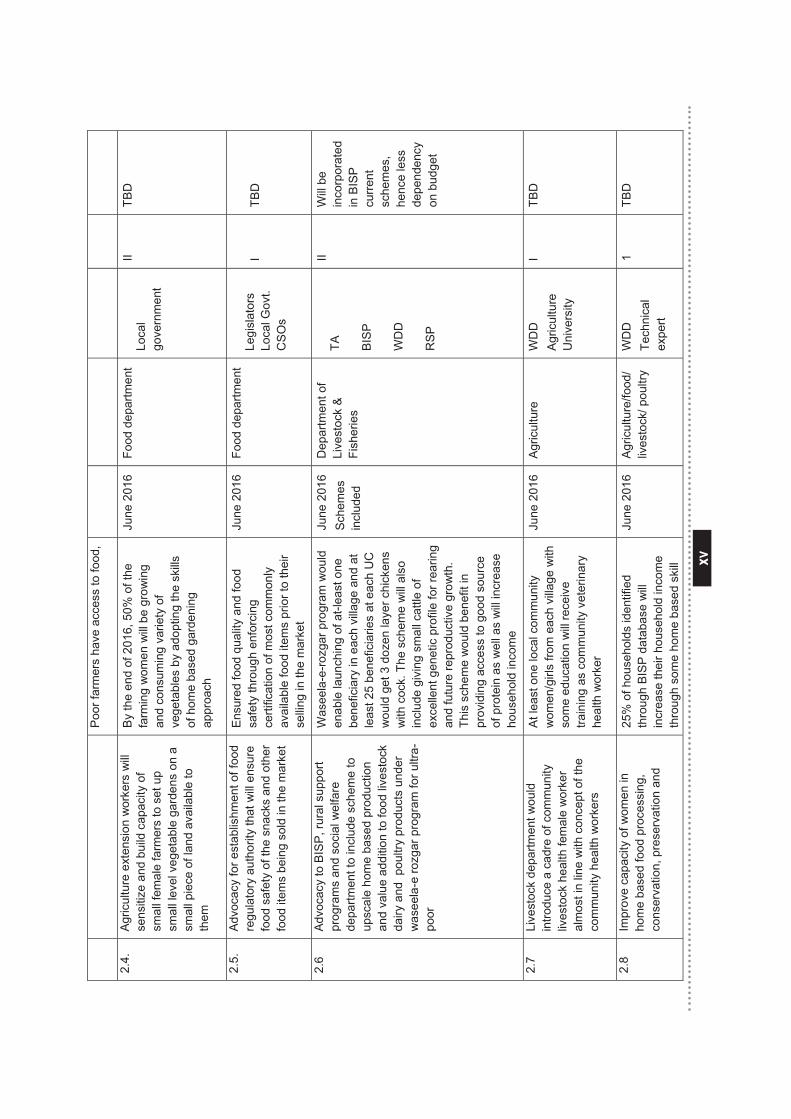
xv
xv
Poo
r far
mer
s ha
ve a
cces
s to
food
,
2.4.
Ag
ricul
ture
ext
ensi
on w
orke
rs w
ill
sens
itize
and
bui
ld c
apac
ity o
f sm
all f
emal
e fa
rmer
s to
set
up
smal
l lev
el v
eget
able
gar
dens
on
a sm
all p
iece
of l
and
avai
labl
e to
th
em
By
the
end
of 2
016,
50%
of t
he
farm
ing
wom
en w
ill b
e gr
owin
g an
d co
nsum
ing
varie
ty o
f ve
geta
bles
by
adop
ting
the
skills
of
hom
e ba
sed
gard
enin
g ap
proa
ch
June
201
6 Fo
od d
epar
tmen
t Lo
cal
gove
rnm
ent
II TB
D
2.5.
A
dvoc
acy
for e
stab
lishm
ent o
f foo
d re
gula
tory
aut
horit
y th
at w
ill e
nsur
e fo
od s
afet
y of
the
snac
ks a
nd o
ther
fo
od it
ems
bein
g so
ld in
the
mar
ket
Ensu
red
food
qua
lity
and
food
sa
fety
thro
ugh
enfo
rcin
g ce
rtific
atio
n of
mos
t com
mon
ly
avai
labl
e fo
od it
ems
prio
r to
thei
r se
lling
in th
e m
arke
t
June
201
6 Fo
od d
epar
tmen
t Le
gisl
ator
s Lo
cal G
ovt.
CS
Os
I TB
D
2.6
Adv
ocac
y to
BIS
P, r
ural
sup
port
prog
ram
s an
d so
cial
wel
fare
de
partm
ent t
o in
clud
e sc
hem
e to
up
scal
e ho
me
base
d pr
oduc
tion
and
valu
e ad
ditio
n to
food
live
stoc
k da
iry a
nd p
oultr
y pr
oduc
ts u
nder
w
asee
la-e
rozg
ar p
rogr
am fo
r ultr
a-po
or
Was
eela
-e-ro
zgar
pro
gram
wou
ld
enab
le la
unch
ing
of a
t-lea
st o
ne
bene
ficia
ry in
eac
h vi
llage
and
at
leas
t 25
bene
ficia
ries
at e
ach
UC
w
ould
get
3 d
ozen
laye
r chi
cken
s w
ith c
ock.
The
sch
eme
will
als
o in
clud
e gi
ving
sm
all c
attle
of
exce
llent
gen
etic
pro
file
for r
earin
g an
d fu
ture
repr
oduc
tive
grow
th.
This
sch
eme
wou
ld b
enef
it in
pr
ovid
ing
acce
ss to
goo
d so
urce
of
pro
tein
as
wel
l as
will
incr
ease
ho
useh
old
inco
me
June
201
6 S
chem
es
incl
uded
Dep
artm
ent o
f Li
vest
ock
&
Fish
erie
s TA
BIS
P
WD
D
RS
P
II W
ill be
in
corp
orat
ed
in B
ISP
cu
rrent
sc
hem
es,
henc
e le
ss
depe
nden
cy
on b
udge
t
2.7
Live
stoc
k de
partm
ent w
ould
in
trodu
ce a
cad
re o
f com
mun
ity
lives
tock
hea
lth fe
mal
e w
orke
r al
mos
t in
line
with
con
cept
of t
he
com
mun
ity h
ealth
wor
kers
At l
east
one
loca
l com
mun
ity
wom
en/g
irls
from
eac
h vi
llage
with
so
me
educ
atio
n w
ill re
ceiv
e tra
inin
g as
com
mun
ity v
eter
inar
y he
alth
wor
ker
June
201
6 Ag
ricul
ture
W
DD
Ag
ricul
ture
U
nive
rsity
I TB
D
2.8
Impr
ove
capa
city
of w
omen
in
hom
e ba
sed
food
pro
cess
ing,
co
nser
vatio
n, p
rese
rvat
ion
and
25%
of h
ouse
hold
s id
entif
ied
thro
ugh
BISP
dat
abas
e w
ill
incr
ease
thei
r hou
seho
ld in
com
e th
roug
h so
me
hom
e ba
sed
skill
June
201
6 A
gric
ultu
re/fo
od/
lives
tock
/ pou
ltry
WD
D
Tech
nica
l ex
pert
1 TB
D
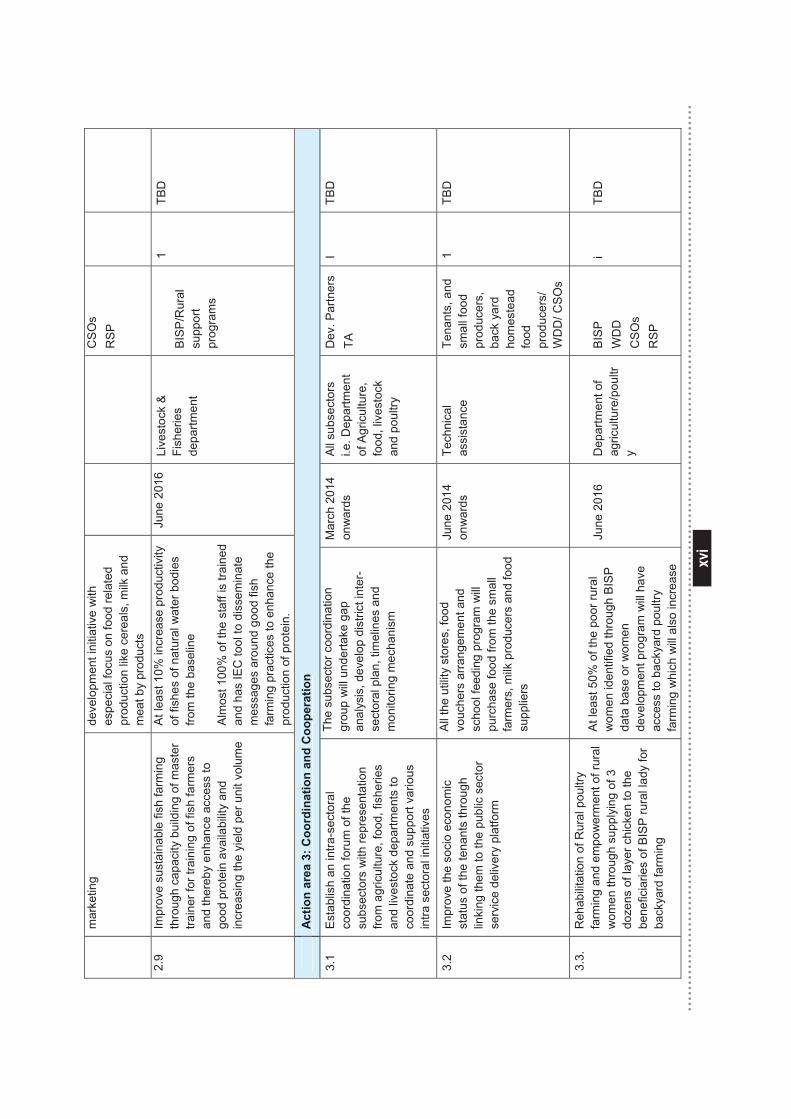
xvi
xvi
mar
ketin
g de
velo
pmen
t ini
tiativ
e w
ith
espe
cial
focu
s on
food
rela
ted
prod
uctio
n lik
e ce
real
s, m
ilk a
nd
mea
t by
prod
ucts
CS
Os
RS
P
2.9
Impr
ove
sust
aina
ble
fish
farm
ing
thro
ugh
capa
city
bui
ldin
g of
mas
ter
train
er fo
r tra
inin
g of
fish
farm
ers
and
ther
eby
enha
nce
acce
ss to
go
od p
rote
in a
vaila
bilit
y an
d in
crea
sing
the
yiel
d pe
r uni
t vol
ume
At l
east
10%
incr
ease
pro
duct
ivity
of
fish
es o
f nat
ural
wat
er b
odie
s fro
m th
e ba
selin
e A
lmos
t 100
% o
f the
sta
ff is
trai
ned
and
has
IEC
tool
to d
isse
min
ate
mes
sage
s ar
ound
goo
d fis
h fa
rmin
g pr
actic
es to
enh
ance
the
prod
uctio
n of
pro
tein
.
June
201
6 Li
vest
ock
&
Fish
erie
s de
partm
ent
BIS
P/R
ural
su
ppor
t pr
ogra
ms
1 TB
D
A
ctio
n ar
ea 3
: Coo
rdin
atio
n an
d C
oope
ratio
n
3.1
Est
ablis
h an
intra
-sec
tora
l co
ordi
natio
n fo
rum
of t
he
subs
ecto
rs w
ith re
pres
enta
tion
from
agr
icul
ture
, foo
d, fi
sher
ies
and
lives
tock
dep
artm
ents
to
coor
dina
te a
nd s
uppo
rt va
rious
in
tra s
ecto
ral i
nitia
tives
The
subs
ecto
r coo
rdin
atio
n gr
oup
will
und
erta
ke g
ap
anal
ysis
, dev
elop
dis
trict
inte
r-se
ctor
al p
lan,
tim
elin
es a
nd
mon
itorin
g m
echa
nism
Mar
ch 2
014
onw
ards
A
ll su
bsec
tors
i.e
. Dep
artm
ent
of A
gric
ultu
re,
food
, liv
esto
ck
and
poul
try
Dev
. Par
tner
s TA
I
TBD
3.2
Impr
ove
the
soci
o ec
onom
ic
stat
us o
f the
tena
nts
thro
ugh
linki
ng th
em to
the
publ
ic s
ecto
r se
rvic
e de
liver
y pl
atfo
rm
All
the
utili
ty s
tore
s, fo
od
vouc
hers
arra
ngem
ent a
nd
scho
ol fe
edin
g pr
ogra
m w
ill pu
rcha
se fo
od fr
om th
e sm
all
farm
ers,
milk
pro
duce
rs a
nd fo
od
supp
liers
June
201
4 on
war
ds
Tech
nica
l as
sist
ance
Te
nant
s, a
nd
smal
l foo
d pr
oduc
ers,
ba
ck y
ard
hom
este
ad
food
pr
oduc
ers/
W
DD
/ CS
Os
1 TB
D
3.3.
R
ehab
ilita
tion
of R
ural
pou
ltry
farm
ing
and
empo
wer
men
t of r
ural
w
omen
thro
ugh
supp
lyin
g of
3
doze
ns o
f lay
er c
hick
en to
the
bene
ficia
ries
of B
ISP
rura
l lad
y fo
r ba
ckya
rd fa
rmin
g
At l
east
50%
of t
he p
oor r
ural
w
omen
iden
tifie
d th
roug
h B
ISP
da
ta b
ase
or w
omen
de
velo
pmen
t pro
gram
will
hav
e ac
cess
to b
acky
ard
poul
try
farm
ing
whi
ch w
ill a
lso
incr
ease
June
201
6 D
epar
tmen
t of
agric
ultu
re/p
oultr
y
BIS
P
WD
D
CS
Os
RS
P
i TB
D
A
ctio
n ar
ea 3
: Coo
rdin
atio
n an
d C
oope
ratio
n
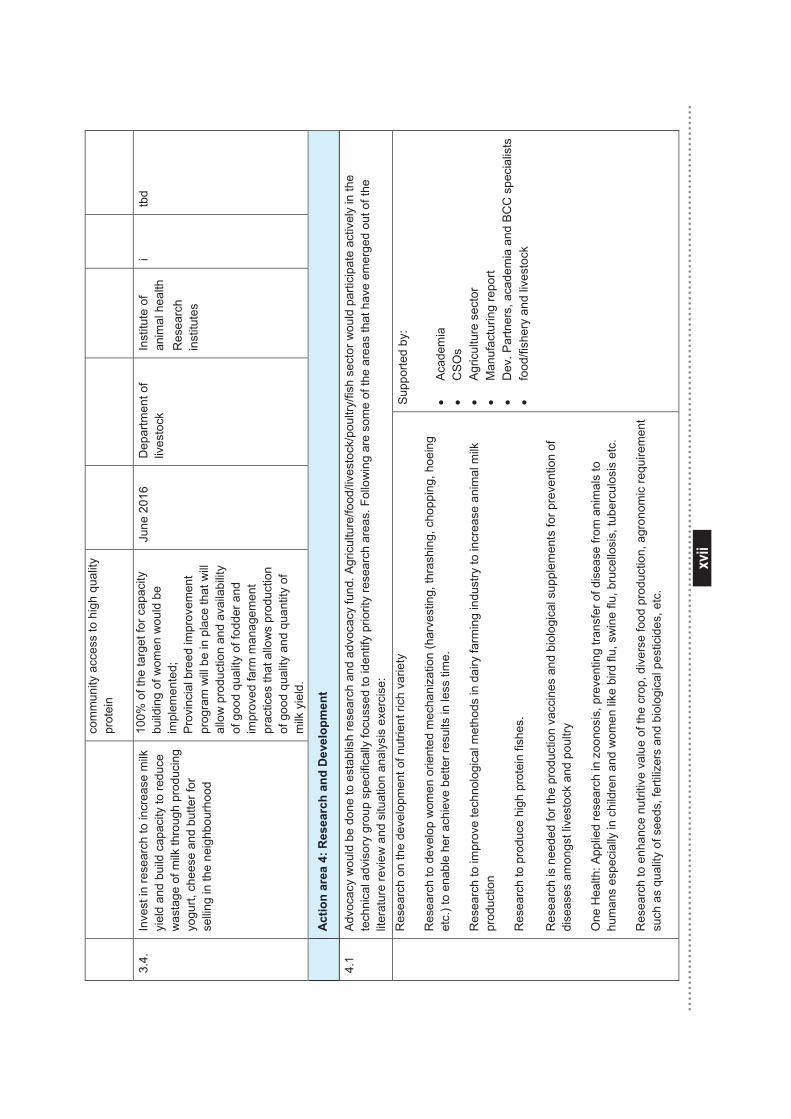
xvii
xvii
com
mun
ity a
cces
s to
hig
h qu
ality
pr
otei
n
3.4.
In
vest
in re
sear
ch to
incr
ease
milk
yi
eld
and
build
cap
acity
to re
duce
w
asta
ge o
f milk
thro
ugh
prod
ucin
g yo
gurt,
che
ese
and
butte
r for
se
lling
in th
e ne
ighb
ourh
ood
100%
of t
he ta
rget
for c
apac
ity
build
ing
of w
omen
wou
ld b
e im
plem
ente
d;
Prov
inci
al b
reed
impr
ovem
ent
prog
ram
will
be in
pla
ce th
at w
ill al
low
pro
duct
ion
and
avai
labi
lity
of g
ood
qual
ity o
f fod
der a
nd
impr
oved
farm
man
agem
ent
prac
tices
that
allo
ws
prod
uctio
n of
goo
d qu
ality
and
qua
ntity
of
milk
yie
ld.
June
201
6 D
epar
tmen
t of
lives
tock
In
stitu
te o
f an
imal
hea
lth
Res
earc
h in
stitu
tes
i tb
d
A
ctio
n ar
ea 4
: Res
earc
h an
d D
evel
opm
ent
4.1
Advo
cacy
wou
ld b
e do
ne to
est
ablis
h re
sear
ch a
nd a
dvoc
acy
fund
. Agr
icul
ture
/food
/live
stoc
k/po
ultry
/fish
sec
tor w
ould
par
ticip
ate
activ
ely
in th
e te
chni
cal a
dvis
ory
grou
p sp
ecifi
cally
focu
ssed
to id
entif
y pr
iorit
y re
sear
ch a
reas
. Fol
low
ing
are
som
e of
the
area
s th
at h
ave
emer
ged
out o
f the
lit
erat
ure
revi
ew a
nd s
ituat
ion
anal
ysis
exe
rcis
e:
R
esea
rch
on th
e de
velo
pmen
t of n
utrie
nt ri
ch v
arie
ty
Res
earc
h to
dev
elop
wom
en o
rient
ed m
echa
niza
tion
(har
vest
ing,
thra
shin
g, c
hopp
ing,
hoe
ing
etc.
) to
enab
le h
er a
chie
ve b
ette
r res
ults
in le
ss ti
me.
Res
earc
h to
impr
ove
tech
nolo
gica
l met
hods
in d
airy
farm
ing
indu
stry
to in
crea
se a
nim
al m
ilk
prod
uctio
n
Res
earc
h to
pro
duce
hig
h pr
otei
n fis
hes.
R
esea
rch
is n
eede
d fo
r the
pro
duct
ion
vacc
ines
and
bio
logi
cal s
uppl
emen
ts fo
r pre
vent
ion
of
dise
ases
am
ongs
t liv
esto
ck a
nd p
oultr
y
One
Hea
lth: A
pplie
d re
sear
ch in
zoo
nosi
s, p
reve
ntin
g tra
nsfe
r of d
isea
se fr
om a
nim
als
to
hum
ans
espe
cial
ly in
chi
ldre
n an
d w
omen
like
bird
flu,
sw
ine
flu, b
ruce
llosi
s, tu
berc
ulos
is e
tc.
Res
earc
h to
enh
ance
nut
ritiv
e va
lue
of th
e cr
op, d
iver
se fo
od p
rodu
ctio
n, a
gron
omic
requ
irem
ent
such
as
qual
ity o
f see
ds, f
ertil
izer
s an
d bi
olog
ical
pes
ticid
es, e
tc.
Supp
orte
d by
: •
Acad
emia
•
CS
Os
• Ag
ricul
ture
sec
tor
• M
anuf
actu
ring
repo
rt •
Dev
. Par
tner
s, a
cade
mia
and
BC
C s
peci
alis
ts
• fo
od/fi
sher
y an
d liv
esto
ck
A
ctio
n ar
ea 4
: Res
earc
h an
d D
evel
opm
ent
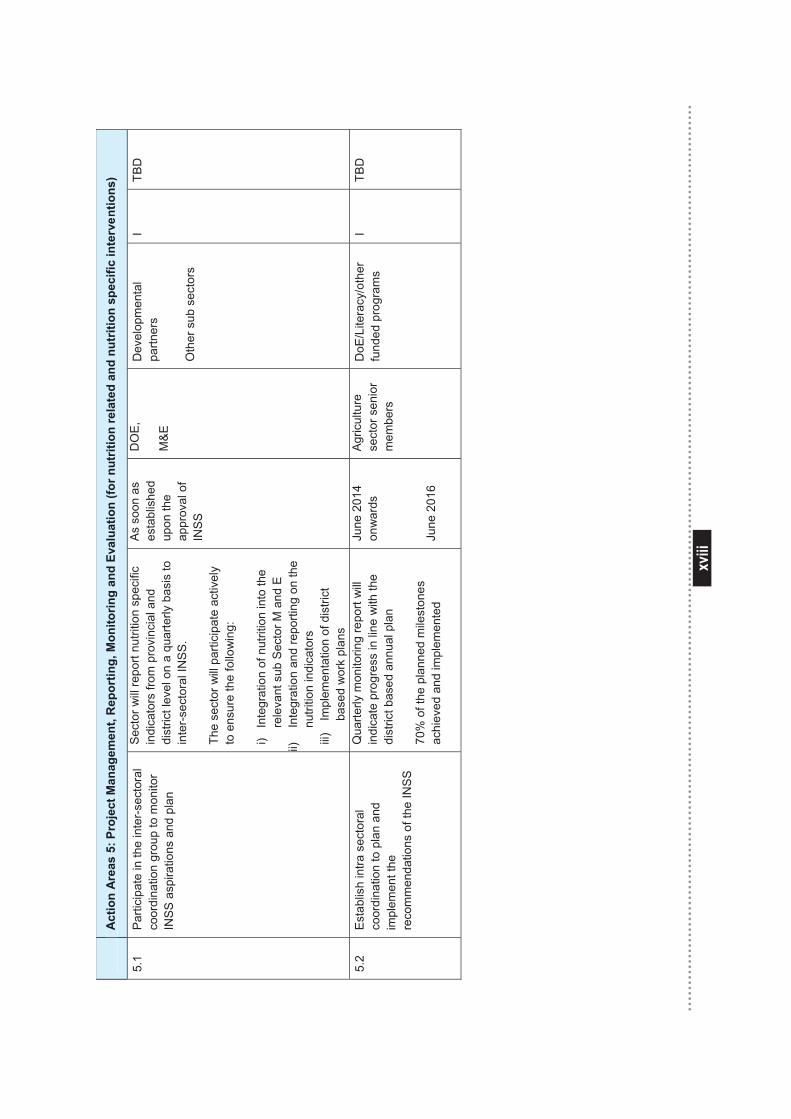
xviii
xviii
A
ctio
n A
reas
5: P
roje
ct M
anag
emen
t, R
epor
ting,
Mon
itorin
g an
d Ev
alua
tion
(for n
utrit
ion
rela
ted
and
nutr
ition
spe
cific
inte
rven
tions
)
5.1
Par
ticip
ate
in th
e in
ter-s
ecto
ral
coor
dina
tion
grou
p to
mon
itor
INS
S a
spira
tions
and
pla
n
Sec
tor w
ill re
port
nutri
tion
spec
ific
indi
cato
rs fr
om p
rovi
ncia
l and
di
stric
t lev
el o
n a
quar
terly
bas
is to
in
ter-
sect
oral
INS
S.
Th
e se
ctor
will
par
ticip
ate
activ
ely
to e
nsur
e th
e fo
llow
ing:
i)
Inte
grat
ion
of n
utrit
ion
into
the
rele
vant
sub
Sec
tor M
and
E
ii)
Inte
grat
ion
and
repo
rting
on
the
nutri
tion
indi
cato
rs
iii)
Impl
emen
tatio
n of
dis
trict
ba
sed
wor
k pl
ans
As
soon
as
esta
blis
hed
upon
the
appr
oval
of
INS
S
DO
E,
M&
E
Dev
elop
men
tal
partn
ers
Oth
er s
ub s
ecto
rs
I TB
D
5.2
Est
ablis
h in
tra s
ecto
ral
coor
dina
tion
to p
lan
and
impl
emen
t the
re
com
men
datio
ns o
f the
INS
S
Qua
rterly
mon
itorin
g re
port
will
in
dica
te p
rogr
ess
in li
ne w
ith th
e di
stric
t bas
ed a
nnua
l pla
n 70
% o
f the
pla
nned
mile
ston
es
achi
eved
and
impl
emen
ted
June
201
4 on
war
ds
June
201
6
Agric
ultu
re
sect
or s
enio
r m
embe
rs
DoE
/Lite
racy
/oth
er
fund
ed p
rogr
ams
I TB
D
A
ctio
n A
reas
5: P
roje
ct M
anag
emen
t, R
epor
ting,
Mon
itorin
g an
d Ev
alua
tion
(for n
utrit
ion
rela
ted
and
nutr
ition
spe
cific
inte
rven
tions
)
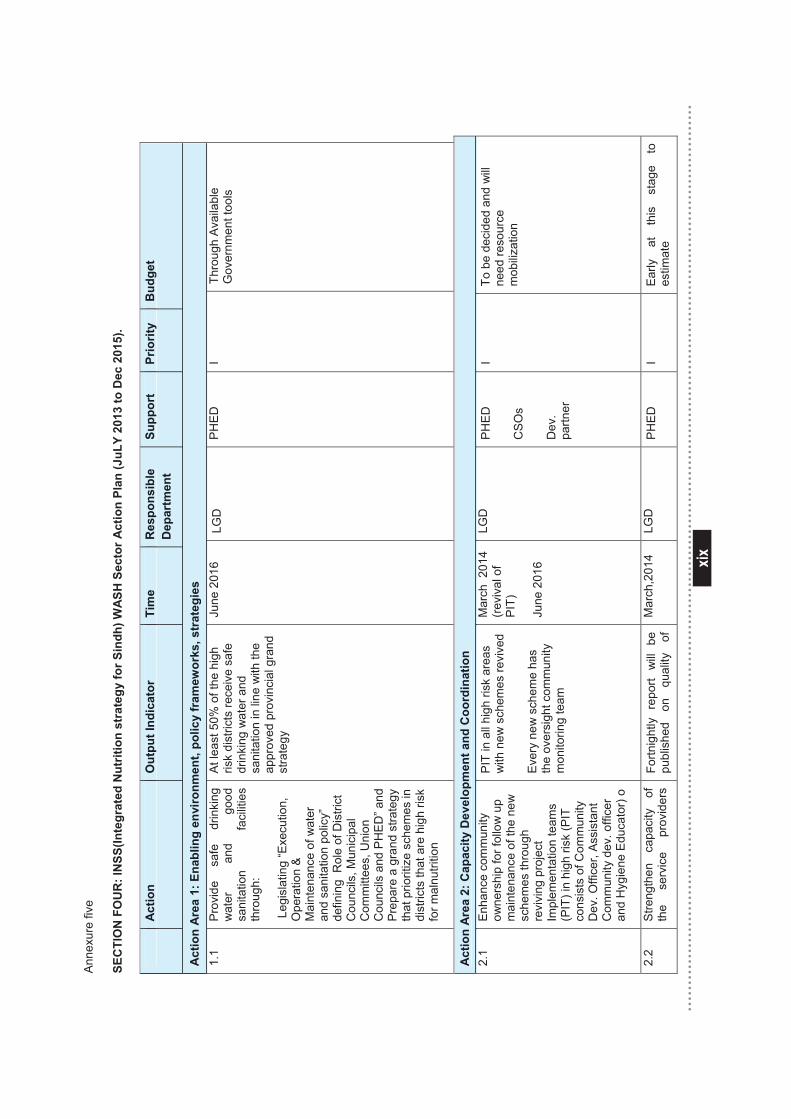
xix
xix
Ann
exur
e fiv
e
SEC
TIO
N F
OU
R: I
NSS
(Inte
grat
ed N
utrit
ion
stra
tegy
for S
indh
) WA
SH S
ecto
r Act
ion
Plan
(JuL
Y 20
13 to
Dec
201
5).
A
ctio
n O
utpu
t Ind
icat
or
Tim
e R
espo
nsib
le
Dep
artm
ent
Supp
ort
Prio
rity
B
udge
t
Act
ion
Are
a 1:
Ena
blin
g en
viro
nmen
t, po
licy
fram
ewor
ks, s
trat
egie
s 1.
1 P
rovi
de
safe
dr
inki
ng
wat
er
and
good
sa
nita
tion
faci
litie
s th
roug
h:
Leg
isla
ting
“Exe
cutio
n,
Ope
ratio
n &
M
aint
enan
ce o
f wat
er
and
sani
tatio
n po
licy”
de
finin
g R
ole
of D
istri
ct
Cou
ncils
, Mun
icip
al
Com
mitt
ees,
Uni
on
Cou
ncils
and
PH
ED” a
nd
Pre
pare
a g
rand
stra
tegy
th
at p
riorit
ize
sche
mes
in
dist
ricts
that
are
hig
h ris
k fo
r mal
nutri
tion
At l
east
50%
of t
he h
igh
risk
dist
ricts
rece
ive
safe
dr
inki
ng w
ater
and
sa
nita
tion
in li
ne w
ith th
e ap
prov
ed p
rovi
ncia
l gra
nd
stra
tegy
June
201
6 LG
D
P
HE
D
I Th
roug
h Av
aila
ble
Gov
ernm
ent t
ools
Act
ion
Are
a 2:
Cap
acity
Dev
elop
men
t and
Coo
rdin
atio
n 2.
1 En
hanc
e co
mm
unity
ow
ners
hip
for f
ollo
w u
p m
aint
enan
ce o
f the
new
sc
hem
es th
roug
h re
vivi
ng p
roje
ct
Impl
emen
tatio
n te
ams
(PIT
) in
high
risk
(PIT
co
nsis
ts o
f Com
mun
ity
Dev
. Offi
cer,
Assi
stan
t C
omm
unity
dev
. offi
cer
and
Hyg
iene
Edu
cato
r) o
PIT
in a
ll hi
gh ri
sk a
reas
w
ith n
ew s
chem
es re
vive
d E
very
new
sch
eme
has
th
e ov
ersi
ght c
omm
unity
m
onito
ring
team
Mar
ch 2
014
(revi
val o
f PI
T)
June
201
6
LGD
P
HE
D
CS
Os
Dev
. pa
rtner
I To
be
deci
ded
and
will
ne
ed re
sour
ce
mob
iliza
tion
2.2
Stre
ngth
en
capa
city
of
th
e s
ervi
ce
prov
ider
s Fo
rtnig
htly
re
port
will
be
pu
blis
hed
on
qual
ity
of
Mar
ch,2
014
LGD
P
HE
D
I
Early
at
th
is
stag
e to
es
timat
e
A
ctio
n O
utpu
t Ind
icat
or
Tim
e R
espo
nsib
le
Dep
artm
ent
Supp
ort
Prio
rity
B
udge
t
Act
ion
Are
a 1:
Ena
blin
g en
viro
nmen
t, po
licy
fram
ewor
ks, s
trat
egie
s
Act
ion
Are
a 2:
Cap
acity
Dev
elop
men
t and
Coo
rdin
atio
n
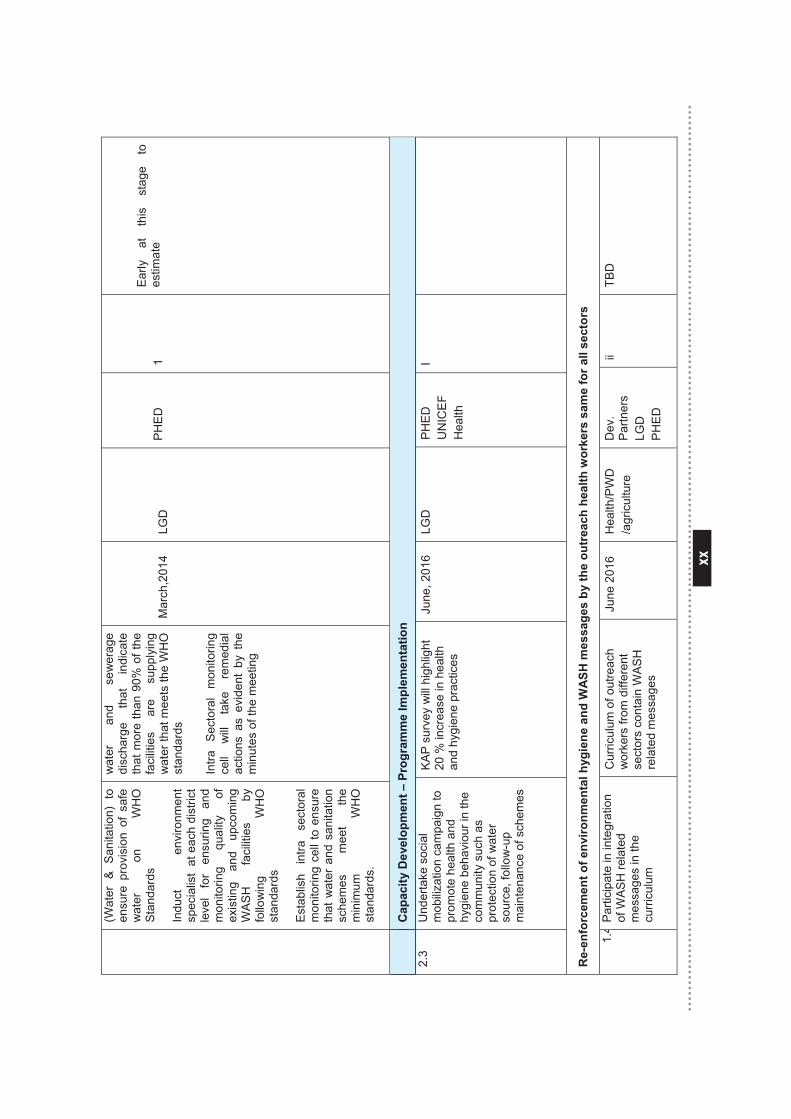
xx
xx
(Wat
er &
San
itatio
n) t
o en
sure
pro
visi
on o
f sa
fe
wat
er
on
WH
O
Stan
dard
s
Indu
ct
envi
ronm
ent
spec
ialis
t at
eac
h di
stric
t le
vel
for
ensu
ring
and
mon
itorin
g qu
ality
of
ex
istin
g an
d up
com
ing
WA
SH
fa
cilit
ies
by
follo
win
g W
HO
st
anda
rds
Est
ablis
h in
tra
sect
oral
m
onito
ring
cell
to e
nsur
e th
at w
ater
and
san
itatio
n sc
hem
es
mee
t th
e m
inim
um
WH
O
stan
dard
s.
wat
er
and
sew
erag
e di
scha
rge
that
in
dica
te
that
mor
e th
an 9
0% o
f the
fa
cilit
ies
are
supp
lyin
g w
ater
that
mee
ts th
e W
HO
st
anda
rds
In
tra
Sec
tora
l m
onito
ring
cell
will
ta
ke
rem
edia
l ac
tions
as
evid
ent
by t
he
min
utes
of t
he m
eetin
g
Mar
ch,2
014
LGD
PH
ED
1
Early
at
th
is
stag
e to
es
timat
e
C
apac
ity D
evel
opm
ent –
Pro
gram
me
Impl
emen
tatio
n
2.3
U
nder
take
soc
ial
mob
iliza
tion
cam
paig
n to
pr
omot
e he
alth
and
hy
gien
e be
havi
our i
n th
e co
mm
unity
suc
h as
pr
otec
tion
of w
ater
so
urce
, fol
low
-up
mai
nten
ance
of s
chem
es
KA
P s
urve
y w
ill h
ighl
ight
20
% in
crea
se in
hea
lth
and
hygi
ene
prac
tices
June
, 201
6 LG
D
PH
ED
U
NIC
EF
Hea
lth
I
Re-
enfo
rcem
ent o
f env
ironm
enta
l hyg
iene
and
WA
SH m
essa
ges
by th
e ou
trea
ch h
ealth
wor
kers
sam
e fo
r all
sect
ors
1.4
Par
ticip
ate
in in
tegr
atio
n of
WA
SH
rela
ted
mes
sage
s in
the
curri
culu
m
Cur
ricul
um o
f out
reac
h w
orke
rs fr
om d
iffer
ent
sect
ors
cont
ain
WA
SH
re
late
d m
essa
ges
June
201
6 H
ealth
/PW
D
/agr
icul
ture
D
ev.
Par
tner
s LG
D
PH
ED
ii TB
D
C
apac
ity D
evel
opm
ent –
Pro
gram
me
Impl
emen
tatio
n
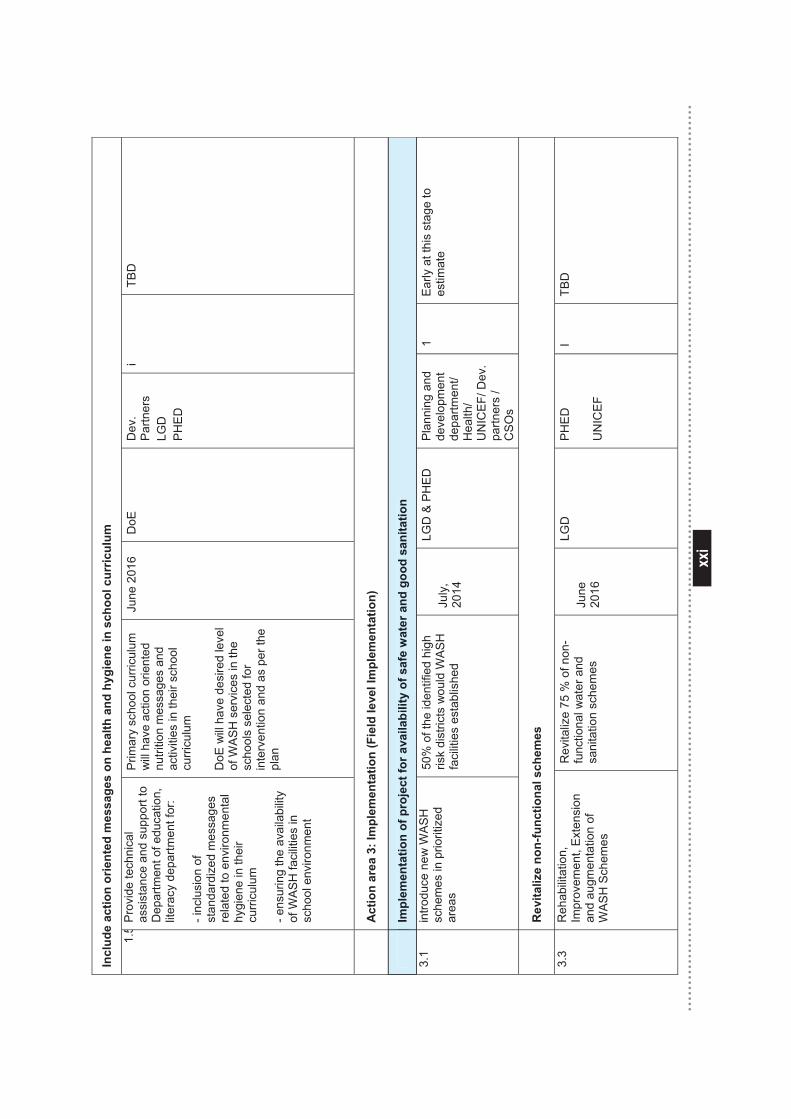
xxi
xxi
Incl
ude
actio
n or
ient
ed m
essa
ges
on h
ealth
and
hyg
iene
in s
choo
l cur
ricul
um
1.5
Prov
ide
tech
nica
l as
sist
ance
and
sup
port
to
Dep
artm
ent o
f edu
catio
n,
liter
acy
depa
rtmen
t for
:
- inc
lusi
on o
f st
anda
rdiz
ed m
essa
ges
rela
ted
to e
nviro
nmen
tal
hygi
ene
in th
eir
curri
culu
m
- ens
urin
g th
e av
aila
bilit
y of
WA
SH
faci
litie
s in
sc
hool
env
ironm
ent
Prim
ary
scho
ol c
urric
ulum
w
ill h
ave
actio
n or
ient
ed
nutri
tion
mes
sage
s an
d ac
tiviti
es in
thei
r sch
ool
curri
culu
m
DoE
will
hav
e de
sire
d le
vel
of W
AS
H s
ervi
ces
in th
e sc
hool
s se
lect
ed fo
r in
terv
entio
n an
d as
per
the
plan
June
201
6 D
oE
Dev
. P
artn
ers
LGD
P
HE
D
i TB
D
A
ctio
n ar
ea 3
: Im
plem
enta
tion
(Fie
ld le
vel I
mpl
emen
tatio
n)
Im
plem
enta
tion
of p
roje
ct fo
r ava
ilabi
lity
of s
afe
wat
er a
nd g
ood
sani
tatio
n
3.1
intro
duce
new
WA
SH
sc
hem
es in
prio
ritiz
ed
area
s
50%
of t
he id
entif
ied
high
ris
k di
stric
ts w
ould
WA
SH
fa
cilit
ies
esta
blis
hed
July
, 20
14
LGD
& P
HE
D
Plan
ning
and
de
velo
pmen
t de
partm
ent/
Hea
lth/
UN
ICE
F/ D
ev.
partn
ers
/ C
SO
s
1 E
arly
at t
his
stag
e to
es
timat
e
R
evita
lize
non-
func
tiona
l sch
emes
3.3
Reh
abili
tatio
n,
Impr
ovem
ent,
Ext
ensi
on
and
augm
enta
tion
of
WA
SH
Sch
emes
Rev
italiz
e 75
% o
f non
-fu
nctio
nal w
ater
and
sa
nita
tion
sche
mes
June
20
16
LGD
P
HE
D
UN
ICE
F
I TB
D
Im
plem
enta
tion
of p
roje
ct fo
r ava
ilabi
lity
of s
afe
wat
er a
nd g
ood
sani
tatio
n
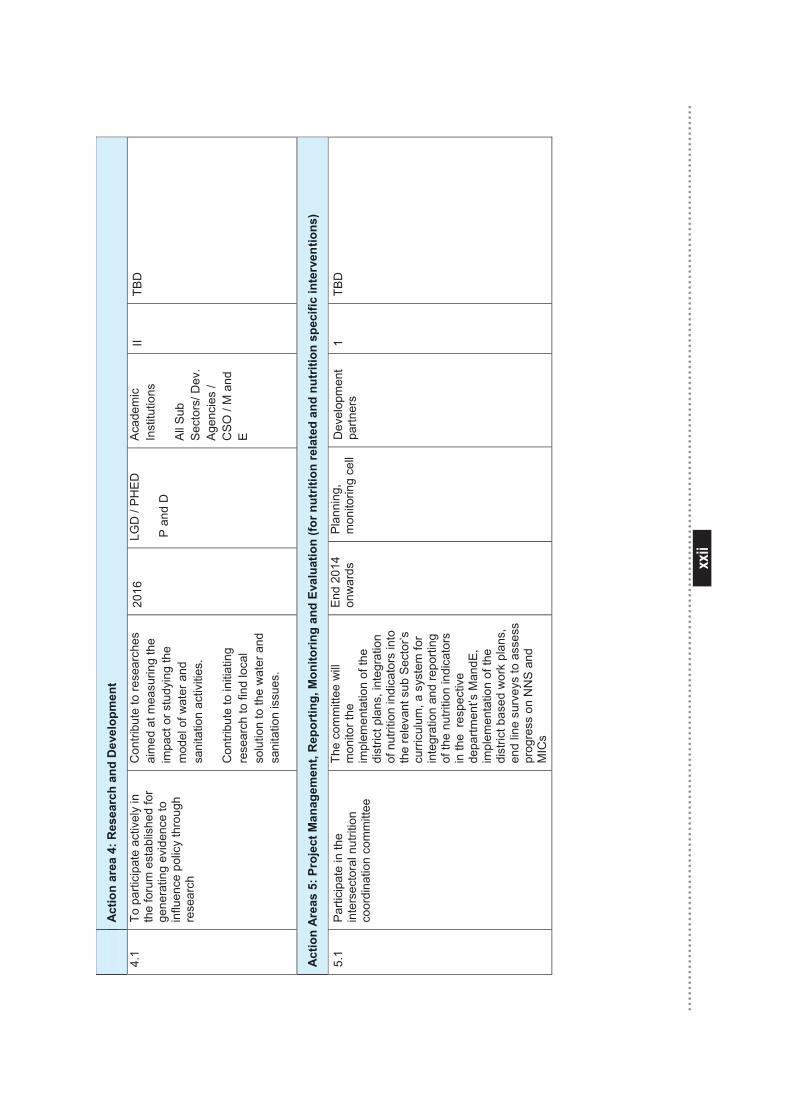
xxii
xxii
A
ctio
n ar
ea 4
: Res
earc
h an
d D
evel
opm
ent
4.1
To p
artic
ipat
e ac
tivel
y in
th
e fo
rum
est
ablis
hed
for
gene
ratin
g ev
iden
ce to
in
fluen
ce p
olic
y th
roug
h re
sear
ch
Con
tribu
te to
rese
arch
es
aim
ed a
t mea
surin
g th
e im
pact
or s
tudy
ing
the
mod
el o
f wat
er a
nd
sani
tatio
n ac
tiviti
es.
Con
tribu
te to
initi
atin
g re
sear
ch to
find
loca
l so
lutio
n to
the
wat
er a
nd
sani
tatio
n is
sues
.
2016
LG
D /
PH
ED
P a
nd D
Acad
emic
In
stitu
tions
All S
ub
Sec
tors
/ Dev
. A
genc
ies
/ C
SO
/ M
and
E
II TB
D
Act
ion
Are
as 5
: Pro
ject
Man
agem
ent,
Rep
ortin
g, M
onito
ring
and
Eval
uatio
n (fo
r nut
ritio
n re
late
d an
d nu
triti
on s
peci
fic in
terv
entio
ns)
5.1
Par
ticip
ate
in th
e in
ters
ecto
ral n
utrit
ion
coor
dina
tion
com
mitt
ee
The
com
mitt
ee w
ill
mon
itor t
he
impl
emen
tatio
n of
the
dist
rict p
lans
, int
egra
tion
of n
utrit
ion
indi
cato
rs in
to
the
rele
vant
sub
Sec
tor’s
cu
rric
ulum
, a s
yste
m fo
r in
tegr
atio
n an
d re
porti
ng
of th
e nu
tritio
n in
dica
tors
in
the
resp
ectiv
e de
partm
ent’s
Man
dE,
impl
emen
tatio
n of
the
dist
rict b
ased
wor
k pl
ans,
en
d lin
e su
rvey
s to
ass
ess
prog
ress
on
NN
S an
d M
ICs
End
2014
on
war
ds
Pla
nnin
g,
mon
itorin
g ce
ll
Dev
elop
men
t pa
rtner
s 1
TBD
A
ctio
n ar
ea 4
: Res
earc
h an
d D
evel
opm
ent
Act
ion
Are
as 5
: Pro
ject
Man
agem
ent,
Rep
ortin
g, M
onito
ring
and
Eval
uatio
n (fo
r nut
ritio
n re
late
d an
d nu
triti
on s
peci
fic in
terv
entio
ns)
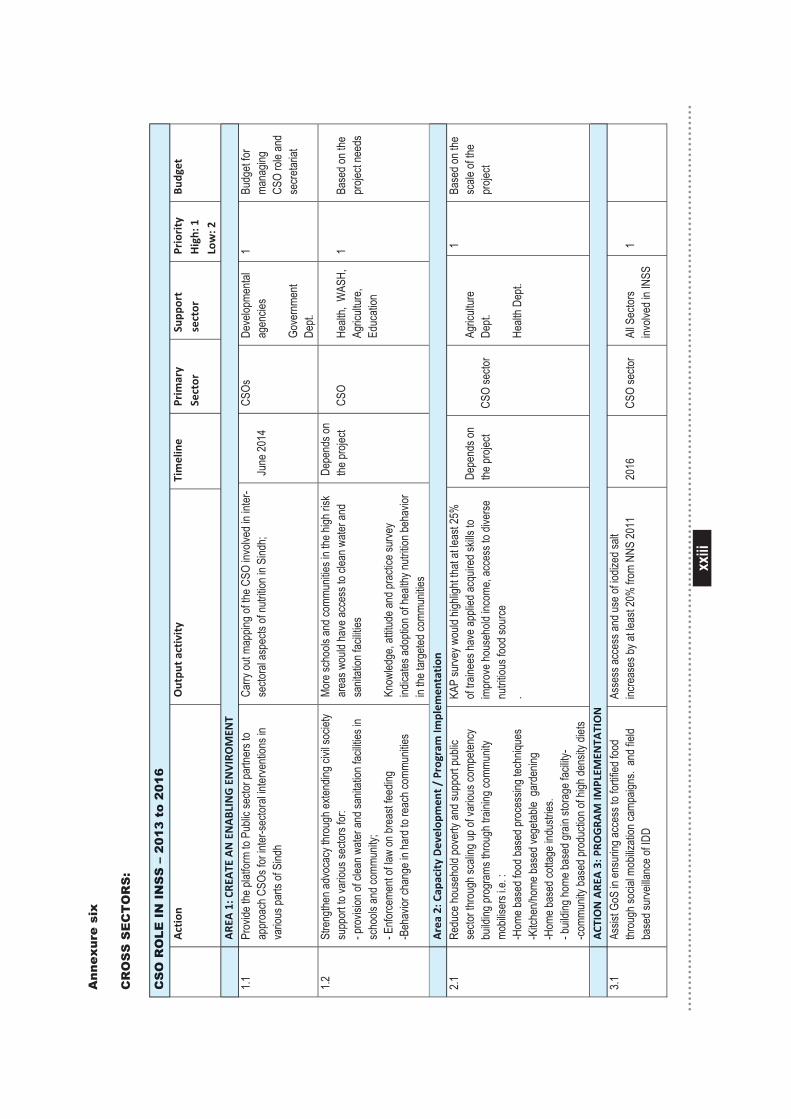
xxiii
xxiii
Ann
exur
e si
x
CR
OS
S S
EC
TO
RS
:
CS
O R
OLE
IN
IN
SS
– 2
013
to 2
016
Action
Outpu
t activity
Timeline
Prim
ary
Sector
Supp
ort
sector
Priority
High: 1
Low: 2
Budg
et
ARE
A 1: C
REATE
AN ENABLING ENVIROMEN
T 1.1
Pr
ovide
the p
latfor
m to
Publi
c sec
tor pa
rtner
s to
appr
oach
CSO
s for
inter
-secto
ral in
terve
ntion
s in
vario
us pa
rts of
Sind
h
Carry
out m
appin
g of th
e CSO
invo
lved i
n inte
r- se
ctora
l asp
ects
of nu
trition
in S
indh;
Ju
ne 20
14
CSOs
Deve
lopme
ntal
agen
cies
Gove
rnme
nt De
pt.
1 Bu
dget
for
mana
ging
CSO
role
and
secre
tariat
1.2
Stre
ngthe
n adv
ocac
y thr
ough
exten
ding c
ivil s
ociet
y su
ppor
t to va
rious
secto
rs for
: - p
rovis
ion of
clea
n wate
r and
sanit
ation
facil
ities i
n sc
hools
and c
ommu
nity;
- Enfo
rceme
nt of
law on
brea
st fee
ding
-Beh
avior
chan
ge in
hard
to re
ach c
ommu
nities
More
scho
ols an
d com
munit
ies in
the h
igh ris
k ar
eas w
ould
have
acce
ss to
clea
n wate
r and
sa
nitati
on fa
cilitie
s Kn
owled
ge, a
ttitud
e and
prac
tice s
urve
y ind
icates
adop
tion o
f hea
lthy n
utritio
n beh
avior
in
the ta
rgete
d com
munit
ies
Depe
nds o
n the
proje
ct CS
O He
alth,
WAS
H,
Agric
ultur
e, Ed
ucati
on
1 Ba
sed o
n the
pr
oject
need
s
Area 2: Cap
acity Develop
men
t / Program Im
plem
entation
2.1
Re
duce
hous
ehold
pove
rty an
d sup
port
publi
c se
ctor t
hrou
gh sc
aling
up of
vario
us co
mpete
ncy
build
ing pr
ogra
ms th
roug
h tra
ining
comm
unity
mo
bilise
rs i.e
. : -H
ome b
ased
food
base
d pro
cess
ing te
chniq
ues
-Kitc
hen/h
ome b
ased
vege
table
gard
ening
-H
ome b
ased
cotta
ge in
dustr
ies.
- buil
ding h
ome b
ased
grain
stor
age f
acilit
y-
-comm
unity
base
d pro
ducti
on of
high
dens
ity di
ets
KAP
surve
y wou
ld hig
hligh
t that
at lea
st 25
%
of tra
inees
have
appli
ed ac
quire
d skil
ls to
impr
ove h
ouse
hold
incom
e, ac
cess
to di
verse
nu
tritiou
s foo
d sou
rce
.
Depe
nds o
n the
proje
ct
CSO
secto
r
Agric
ultur
e De
pt.
Healt
h Dep
t.
1 Ba
sed o
n the
sc
ale of
the
proje
ct
ACT
ION ARE
A 3: P
ROGRA
M IM
PLEM
ENTA
TION
3.1
Assis
t GoS
in en
surin
g acc
ess t
o for
tified
food
thr
ough
socia
l mob
ilizati
on ca
mpaig
ns. a
nd fie
ld ba
sed s
urve
illanc
e of ID
D
Asse
ss ac
cess
and u
se of
iodiz
ed sa
lt inc
reas
es by
at le
ast 2
0% fr
om N
NS 20
11
2016
CS
O se
ctor
All S
ector
s inv
olved
in IN
SS
1
CS
O R
OLE
IN
IN
SS
– 2
013
to 2
016
ARE
A1:CR
EATE
ANEN
ABLINGEN
VIROMEN
T
Area2:Ca
pacity
Develop
men
t/Program
Implem
entation
ACT
IONARE
A3:PR
OGRA
MIM
PLEM
ENTA
TION
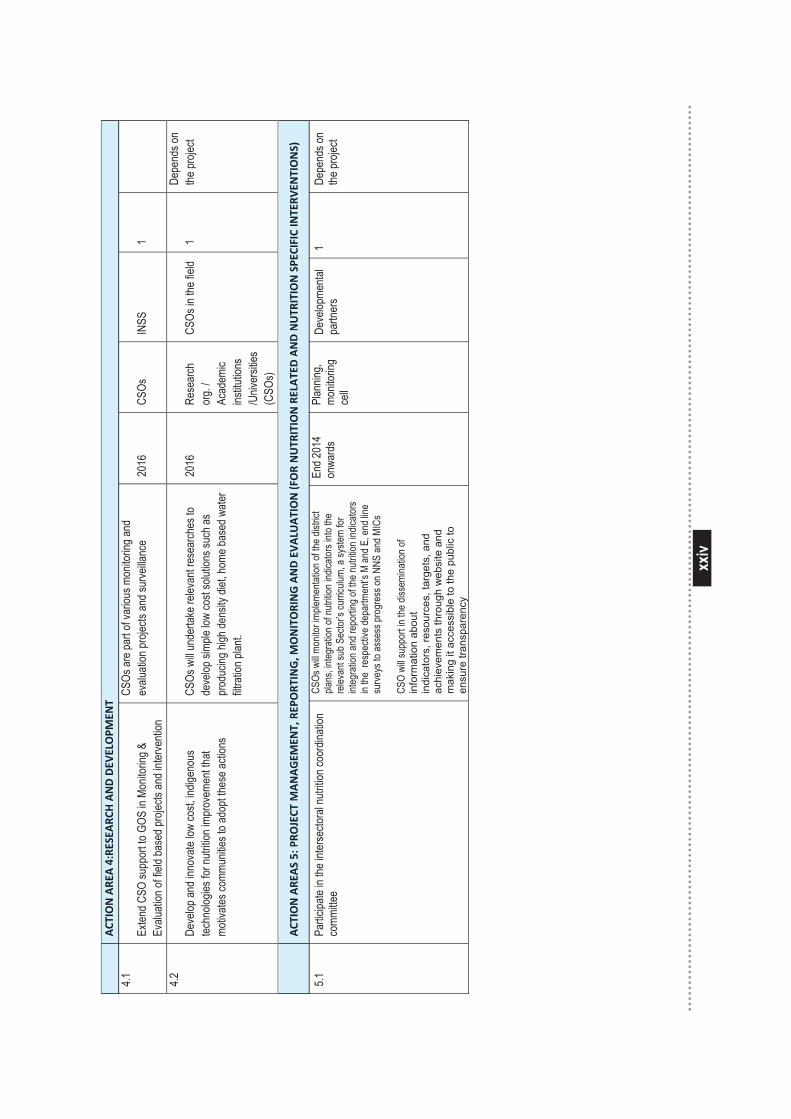
xxiv
xxiv
ACT
ION ARE
A 4:RESEA
RCH AND DEV
ELOPM
ENT
4.1
Exten
d CSO
supp
ort to
GOS
in M
onito
ring &
Ev
aluati
on of
field
base
d pro
jects
and i
nterve
ntion
CSOs
are p
art o
f var
ious m
onito
ring a
nd
evalu
ation
proje
cts an
d sur
veilla
nce
2016
CS
Os
INSS
1
4.2
Deve
lop an
d inn
ovate
low
cost,
indig
enou
s tec
hnolo
gies f
or nu
trition
impr
ovem
ent th
at mo
tivate
s com
munit
ies to
adop
t thes
e acti
ons
CSOs
will
unde
rtake
relev
ant r
esea
rches
to
deve
lop si
mple
low co
st so
lution
s suc
h as
prod
ucing
high
dens
ity di
et, ho
me ba
sed w
ater
filtra
tion p
lant.
2016
Re
sear
ch
org.
/ Ac
adem
ic ins
titutio
ns
/Univ
ersit
ies
(CSO
s)
CSOs
in th
e fiel
d 1
Depe
nds o
n the
proje
ct
ACT
ION ARE
AS 5: PRO
JECT
MANAGEM
ENT, REP
ORT
ING, M
ONITORING AND EVALU
ATION (FOR NUTR
ITION RELATED AND NUTR
ITION SPE
CIFIC INTERV
ENTIONS)
5.1
Partic
ipate
in the
inter
secto
ral n
utritio
n coo
rdina
tion
comm
ittee
CSOs
will
monit
or im
pleme
ntatio
n of th
e dist
rict
plans
, integ
ratio
n of n
utritio
n ind
icator
s into
the
relev
ant s
ub S
ector
’s cu
rricu
lum, a
syste
m for
int
egra
tion a
nd re
portin
g of th
e nutr
ition i
ndica
tors
in the
res
pecti
ve de
partm
ent’s
M an
d E, e
nd lin
e su
rveys
to as
sess
prog
ress
on N
NS an
d MIC
s CS
O wi
ll sup
port
in th
e diss
emina
tion o
f in
form
atio
n ab
out
indi
cato
rs, r
esou
rces
, tar
gets
, and
ac
hiev
emen
ts th
roug
h w
ebsi
te a
nd
mak
ing
it ac
cess
ible
to th
e pu
blic
to
ensu
re tr
ansp
aren
cy
End 2
014
onwa
rds
Plan
ning,
monit
oring
ce
ll
Deve
lopme
ntal
partn
ers
1 De
pend
s on
the pr
oject
ACT
IONARE
A4:RE
SEARC
HANDDEV
ELOPM
ENT
ACT
IONARE
AS5:PR
OJECT
MANAGEM
ENT,RE
PORT
ING,M
ONITORINGANDEV
ALU
ATION(FORNUTR
ITIONRE
LATEDANDNUTR
ITIONSPEC
IFIC
INTERV
ENTIONS)
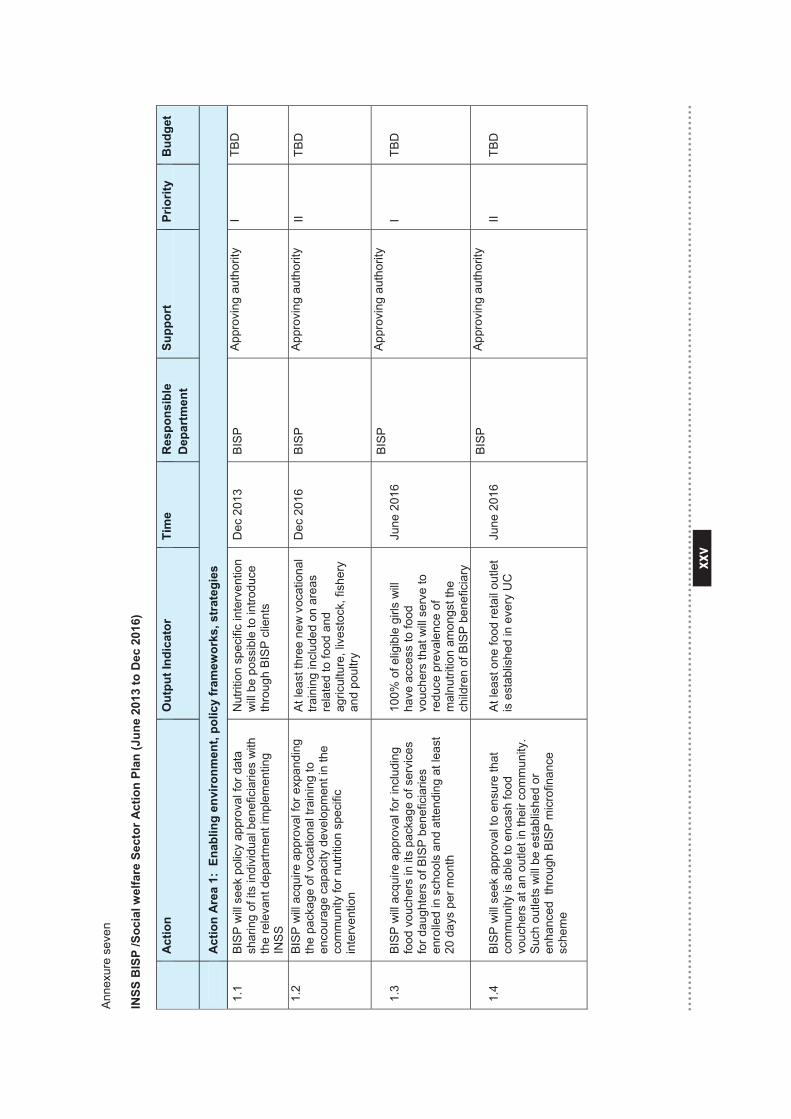
xxv
xxv
Anne
xure
sev
en
INSS
BIS
P /S
ocia
l wel
fare
Sec
tor A
ctio
n Pl
an (J
une
2013
to D
ec 2
016)
Act
ion
Out
put I
ndic
ator
Ti
me
Res
pons
ible
D
epar
tmen
t Su
ppor
t Pr
iorit
y
Bud
get
A
ctio
n A
rea
1: E
nabl
ing
envi
ronm
ent,
polic
y fr
amew
orks
, str
ateg
ies
1.1
BISP
will
see
k po
licy
appr
oval
for d
ata
shar
ing
of it
s in
divi
dual
ben
efic
iarie
s w
ith
the
rele
vant
dep
artm
ent i
mpl
emen
ting
INS
S
Nut
ritio
n sp
ecifi
c in
terv
entio
n w
ill b
e po
ssib
le to
intro
duce
th
roug
h B
ISP
clie
nts
Dec
201
3 B
ISP
A
ppro
ving
aut
horit
y I
TBD
1.2
BIS
P w
ill a
cqui
re a
ppro
val f
or e
xpan
ding
th
e pa
ckag
e of
voc
atio
nal t
rain
ing
to
enco
urag
e ca
paci
ty d
evel
opm
ent i
n th
e co
mm
unity
for n
utrit
ion
spec
ific
inte
rven
tion
At l
east
thre
e ne
w v
ocat
iona
l tra
inin
g in
clud
ed o
n ar
eas
rela
ted
to fo
od a
nd
agric
ultu
re, l
ives
tock
, fis
hery
an
d po
ultry
Dec
201
6 B
ISP
Ap
prov
ing
auth
ority
II
TBD
1.3
BIS
P w
ill a
cqui
re a
ppro
val f
or in
clud
ing
food
vou
cher
s in
its
pack
age
of s
ervi
ces
for d
augh
ters
of B
ISP
ben
efic
iarie
s en
rolle
d in
sch
ools
and
atte
ndin
g at
leas
t 20
day
s pe
r mon
th
100%
of e
ligib
le g
irls
will
ha
ve a
cces
s to
food
vo
uche
rs th
at w
ill s
erve
to
redu
ce p
reva
lenc
e of
m
alnu
tritio
n am
ongs
t the
ch
ildre
n of
BIS
P b
enef
icia
ry
June
201
6 B
ISP
Ap
prov
ing
auth
ority
I
TBD
1.4
BIS
P w
ill s
eek
appr
oval
to e
nsur
e th
at
com
mun
ity is
abl
e to
enc
ash
food
vo
uche
rs a
t an
outle
t in
thei
r com
mun
ity.
Suc
h ou
tlets
will
be
esta
blis
hed
or
enha
nced
thr
ough
BIS
P m
icro
finan
ce
sche
me
At l
east
one
food
reta
il ou
tlet
is e
stab
lishe
d in
eve
ry U
C
June
201
6 B
ISP
Ap
prov
ing
auth
ority
II
TBD
A
ctio
n O
utpu
t Ind
icat
or
Tim
e R
espo
nsib
le
Dep
artm
ent
Supp
ort
Prio
rity
B
udge
t
A
ctio
n A
rea
1: E
nabl
ing
envi
ronm
ent,
polic
y fr
amew
orks
, str
ateg
ies
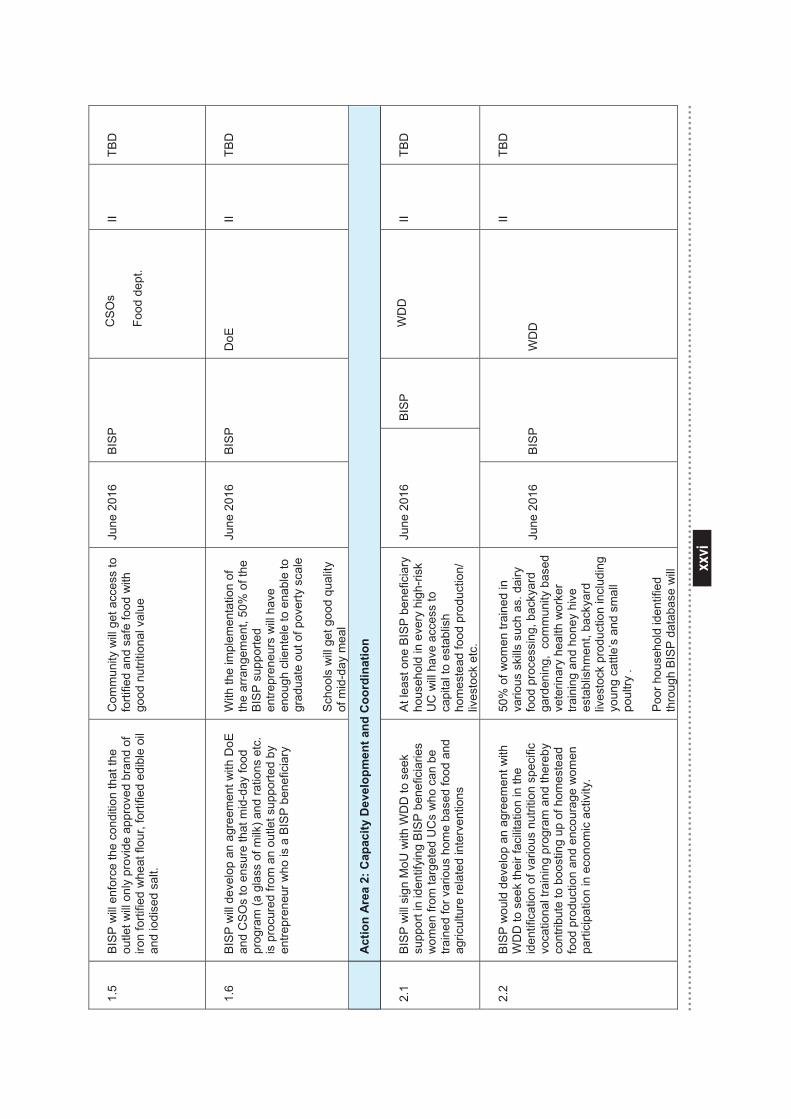
xxvi
xxvi
1.5
BIS
P w
ill e
nfor
ce th
e co
nditi
on th
at th
e ou
tlet w
ill o
nly
prov
ide
appr
oved
bra
nd o
f iro
n fo
rtifie
d w
heat
flou
r, fo
rtifie
d ed
ible
oil
and
iodi
sed
salt.
Com
mun
ity w
ill g
et a
cces
s to
fo
rtifie
d an
d sa
fe fo
od w
ith
good
nut
ritio
nal v
alue
June
201
6 B
ISP
C
SO
s Fo
od d
ept.
II TB
D
1.6
BIS
P w
ill d
evel
op a
n ag
reem
ent w
ith D
oE
and
CS
Os
to e
nsur
e th
at m
id-d
ay fo
od
prog
ram
(a g
lass
of m
ilk) a
nd ra
tions
etc
. is
pro
cure
d fro
m a
n ou
tlet s
uppo
rted
by
entre
pren
eur w
ho is
a B
ISP
bene
ficia
ry
With
the
impl
emen
tatio
n of
th
e ar
rang
emen
t, 50
% o
f the
B
ISP
sup
porte
d en
trepr
eneu
rs w
ill h
ave
enou
gh c
lient
ele
to e
nabl
e to
gr
adua
te o
ut o
f pov
erty
sca
le
Scho
ols
will
get
goo
d qu
ality
of
mid
-day
mea
l
June
201
6 B
ISP
D
oE
II TB
D
A
ctio
n A
rea
2: C
apac
ity D
evel
opm
ent a
nd C
oord
inat
ion
2.1
BIS
P w
ill si
gn M
oU w
ith W
DD
to s
eek
supp
ort i
n id
entif
ying
BIS
P b
enef
icia
ries
wom
en fr
om ta
rget
ed U
Cs
who
can
be
train
ed fo
r var
ious
hom
e ba
sed
food
and
ag
ricul
ture
rela
ted
inte
rven
tions
At l
east
one
BIS
P b
enef
icia
ry
hous
ehol
d in
eve
ry h
igh-
risk
UC
will
have
acc
ess
to
capi
tal t
o es
tabl
ish
hom
este
ad fo
od p
rodu
ctio
n/
lives
tock
etc
.
June
201
6 B
ISP
W
DD
II
TBD
2.2
BIS
P w
ould
dev
elop
an
agre
emen
t with
W
DD
to s
eek
thei
r fac
ilita
tion
in th
e id
entif
icat
ion
of v
ario
us n
utrit
ion
spec
ific
voca
tiona
l tra
inin
g pr
ogra
m a
nd th
ereb
y co
ntrib
ute
to b
oost
ing
up o
f hom
este
ad
food
pro
duct
ion
and
enco
urag
e w
omen
pa
rtici
patio
n in
eco
nom
ic a
ctiv
ity.
50%
of w
omen
trai
ned
in
vario
us s
kills
suc
h as
. dai
ry
food
pro
cess
ing,
bac
kyar
d ga
rden
ing,
com
mun
ity b
ased
ve
terin
ary
heal
th w
orke
r tra
inin
g an
d ho
ney
hive
es
tabl
ishm
ent,
back
yard
liv
esto
ck p
rodu
ctio
n in
clud
ing
youn
g ca
ttle’
s an
d sm
all
poul
try .
Poor
hou
seho
ld id
entif
ied
thro
ugh
BISP
dat
abas
e w
ill
June
201
6
BIS
P
WD
D
II TB
D
Act
ion
Are
a 2:
Cap
acity
Dev
elop
men
t and
Coo
rdin
atio
n
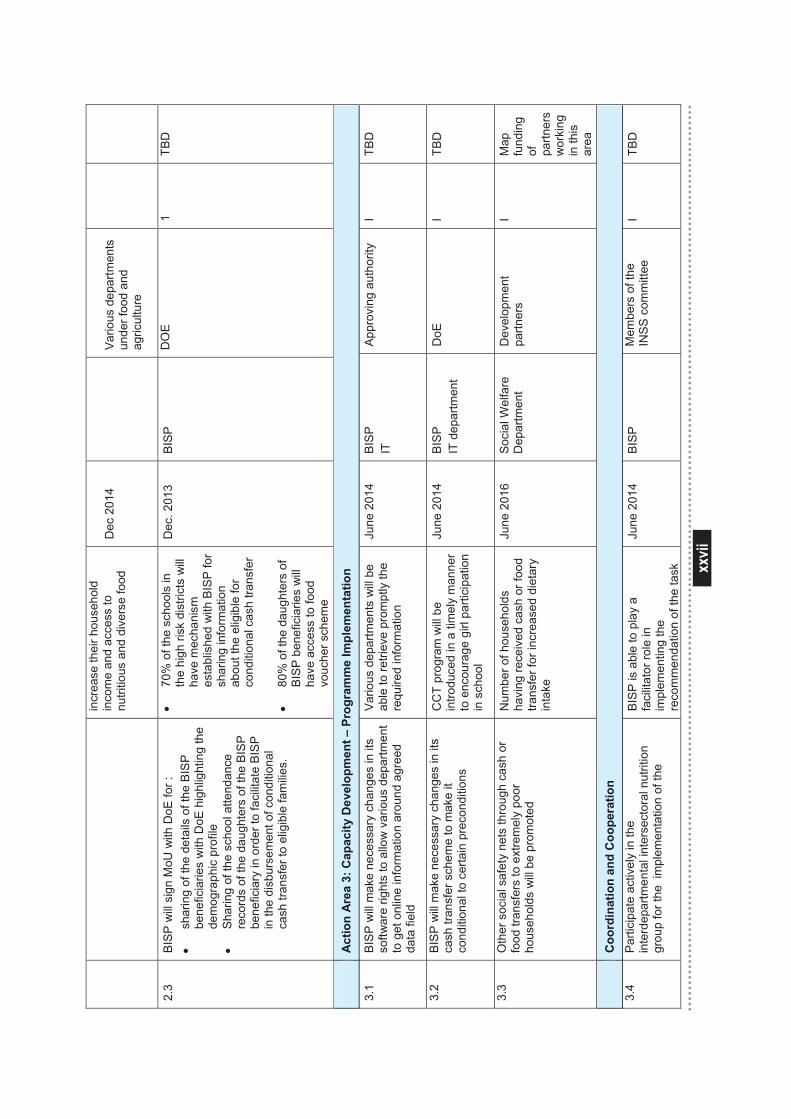
xxvii
xxvii
incr
ease
thei
r hou
seho
ld
inco
me
and
acce
ss to
nu
tritio
us a
nd d
iver
se fo
od
Dec
201
4 Va
rious
dep
artm
ents
un
der f
ood
and
agric
ultu
re
2.3
BIS
P w
ill s
ign
MoU
with
DoE
for :
•
shar
ing
of th
e de
tails
of t
he B
ISP
be
nefic
iarie
s w
ith D
oE h
ighl
ight
ing
the
dem
ogra
phic
pro
file
•
Sha
ring
of th
e sc
hool
atte
ndan
ce
reco
rds
of th
e da
ught
ers
of th
e B
ISP
be
nefic
iary
in o
rder
to fa
cilit
ate
BIS
P
in th
e di
sbur
sem
ent o
f con
ditio
nal
cash
tran
sfer
to e
ligib
le fa
mili
es.
• 70
% o
f the
sch
ools
in
the
high
risk
dis
trict
s w
ill ha
ve m
echa
nism
es
tabl
ishe
d w
ith B
ISP
for
shar
ing
info
rmat
ion
abou
t the
elig
ible
for
cond
ition
al c
ash
trans
fer
• 80
% o
f the
dau
ghte
rs o
f B
ISP
ben
efic
iarie
s w
ill
have
acc
ess
to fo
od
vouc
her s
chem
e
Dec
. 201
3 B
ISP
D
OE
1
TBD
A
ctio
n A
rea
3: C
apac
ity D
evel
opm
ent –
Pro
gram
me
Impl
emen
tatio
n
3.1
BIS
P w
ill m
ake
nece
ssar
y ch
ange
s in
its
softw
are
right
s to
allo
w v
ario
us d
epar
tmen
t to
get
onl
ine
info
rmat
ion
arou
nd a
gree
d da
ta fi
eld
Vario
us d
epar
tmen
ts w
ill b
e ab
le to
retri
eve
prom
ptly
the
requ
ired
info
rmat
ion
June
201
4 B
ISP
IT
A
ppro
ving
aut
horit
y I
TBD
3.2
BIS
P w
ill m
ake
nece
ssar
y ch
ange
s in
its
cash
tran
sfer
sch
eme
to m
ake
it co
nditi
onal
to c
erta
in p
reco
nditi
ons
CC
T pr
ogra
m w
ill b
e in
trodu
ced
in a
tim
ely
man
ner
to e
ncou
rage
girl
par
ticip
atio
n in
sch
ool
June
201
4 B
ISP
IT
dep
artm
ent
DoE
I
TBD
3.3
Oth
er s
ocia
l saf
ety
nets
thro
ugh
cash
or
food
tran
sfer
s to
ext
rem
ely
poor
ho
useh
olds
will
be
prom
oted
Num
ber o
f hou
seho
lds
havi
ng re
ceiv
ed c
ash
or fo
od
trans
fer f
or in
crea
sed
diet
ary
inta
ke
June
201
6 S
ocia
l Wel
fare
D
epar
tmen
t D
evel
opm
ent
partn
ers
I M
ap
fund
ing
of
partn
ers
wor
king
in
this
ar
ea
C
oord
inat
ion
and
Coo
pera
tion
3.4
Par
ticip
ate
activ
ely
in th
e in
terd
epar
tmen
tal i
nter
sect
oral
nut
ritio
n gr
oup
for t
he i
mpl
emen
tatio
n of
the
BIS
P is
abl
e to
pla
y a
faci
litat
or ro
le in
im
plem
entin
g th
e re
com
men
datio
n of
the
task
June
201
4
BIS
P
Mem
bers
of t
he
INS
S c
omm
ittee
I
TBD
A
ctio
n A
rea
3: C
apac
ity D
evel
opm
ent –
Pro
gram
me
Impl
emen
tatio
n
C
oord
inat
ion
and
Coo
pera
tion
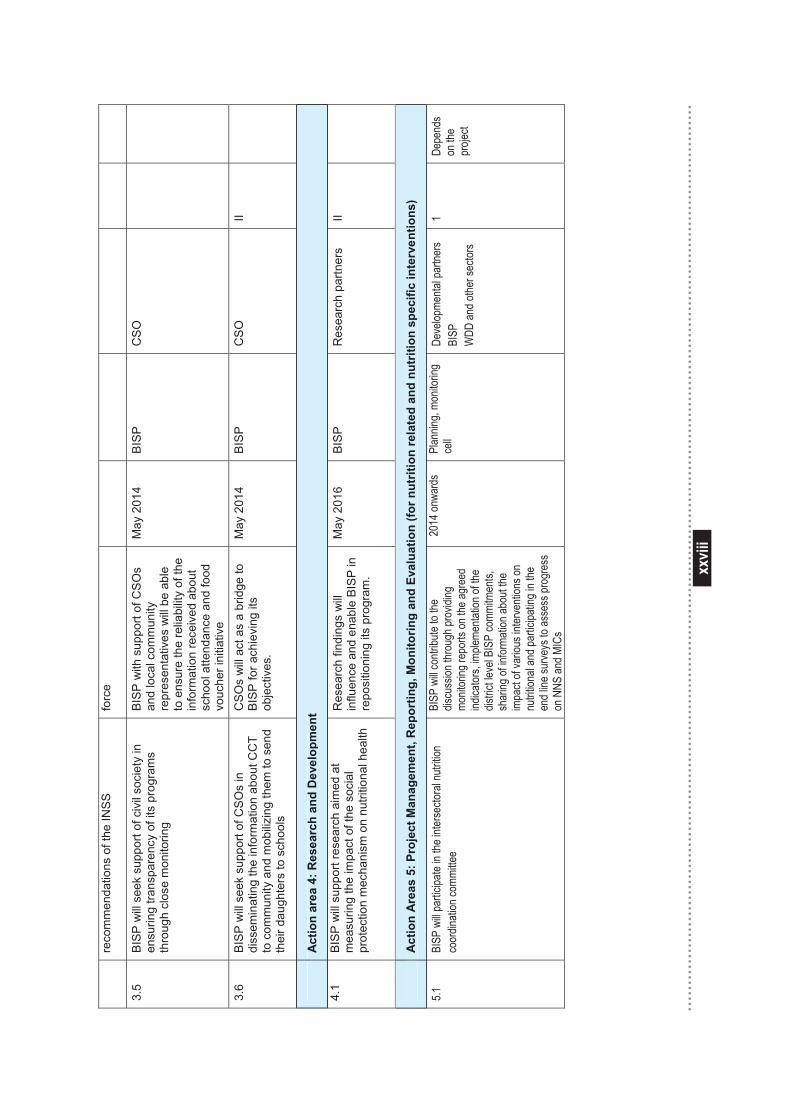
xxvii
i
xxviii
reco
mm
enda
tions
of t
he IN
SS
fo
rce
3.5
BIS
P w
ill s
eek
supp
ort o
f civ
il so
ciet
y in
en
surin
g tra
nspa
renc
y of
its
prog
ram
s th
roug
h cl
ose
mon
itorin
g
BIS
P w
ith s
uppo
rt of
CS
Os
and
loca
l com
mun
ity
repr
esen
tativ
es w
ill b
e ab
le
to e
nsur
e th
e re
liabi
lity
of th
e in
form
atio
n re
ceiv
ed a
bout
sc
hool
atte
ndan
ce a
nd fo
od
vouc
her i
nitia
tive
May
201
4 B
ISP
C
SO
3.6
BIS
P w
ill s
eek
supp
ort o
f CS
Os
in
diss
emin
atin
g th
e in
form
atio
n ab
out C
CT
to c
omm
unity
and
mob
ilizin
g th
em to
sen
d th
eir d
augh
ters
to s
choo
ls
CS
Os
will
act
as
a br
idge
to
BIS
P fo
r ach
ievi
ng it
s ob
ject
ives
.
May
201
4 B
ISP
C
SO
II
A
ctio
n ar
ea 4
: Res
earc
h an
d D
evel
opm
ent
4.1
BIS
P w
ill s
uppo
rt re
sear
ch a
imed
at
mea
surin
g th
e im
pact
of t
he s
ocia
l pr
otec
tion
mec
hani
sm o
n nu
tritio
nal h
ealth
Res
earc
h fin
ding
s w
ill
influ
ence
and
ena
ble
BISP
in
repo
sitio
ning
its
prog
ram
.
May
201
6 B
ISP
R
esea
rch
partn
ers
II
A
ctio
n A
reas
5: P
roje
ct M
anag
emen
t, R
epor
ting,
Mon
itorin
g an
d Ev
alua
tion
(for n
utrit
ion
rela
ted
and
nutr
ition
spe
cific
inte
rven
tions
)
5.1
BISP
will
partic
ipate
in the
inter
secto
ral n
utritio
n co
ordin
ation
comm
ittee
BISP
will
contr
ibute
to the
dis
cuss
ion th
roug
h pro
viding
mo
nitor
ing re
ports
on th
e agr
eed
indica
tors,
imple
menta
tion o
f the
distric
t leve
l BIS
P co
mmitm
ents,
sh
aring
of in
forma
tion a
bout
the
impa
ct of
vario
us in
terve
ntion
s on
nutrit
ional
and p
artic
ipatin
g in t
he
end l
ine su
rveys
to as
sess
prog
ress
on
NNS
and M
ICs
2014
onwa
rds
Plan
ning,
monit
oring
ce
ll
Deve
lopme
ntal p
artne
rs BI
SP
WDD
and o
ther s
ector
s
1 De
pend
s on
the
proje
ct
A
ctio
n ar
ea 4
: Res
earc
h an
d D
evel
opm
ent
A
ctio
n A
reas
5: P
roje
ct M
anag
emen
t, R
epor
ting,
Mon
itorin
g an
d Ev
alua
tion
(for n
utrit
ion
rela
ted
and
nutr
ition
spe
cific
inte
rven
tions
)
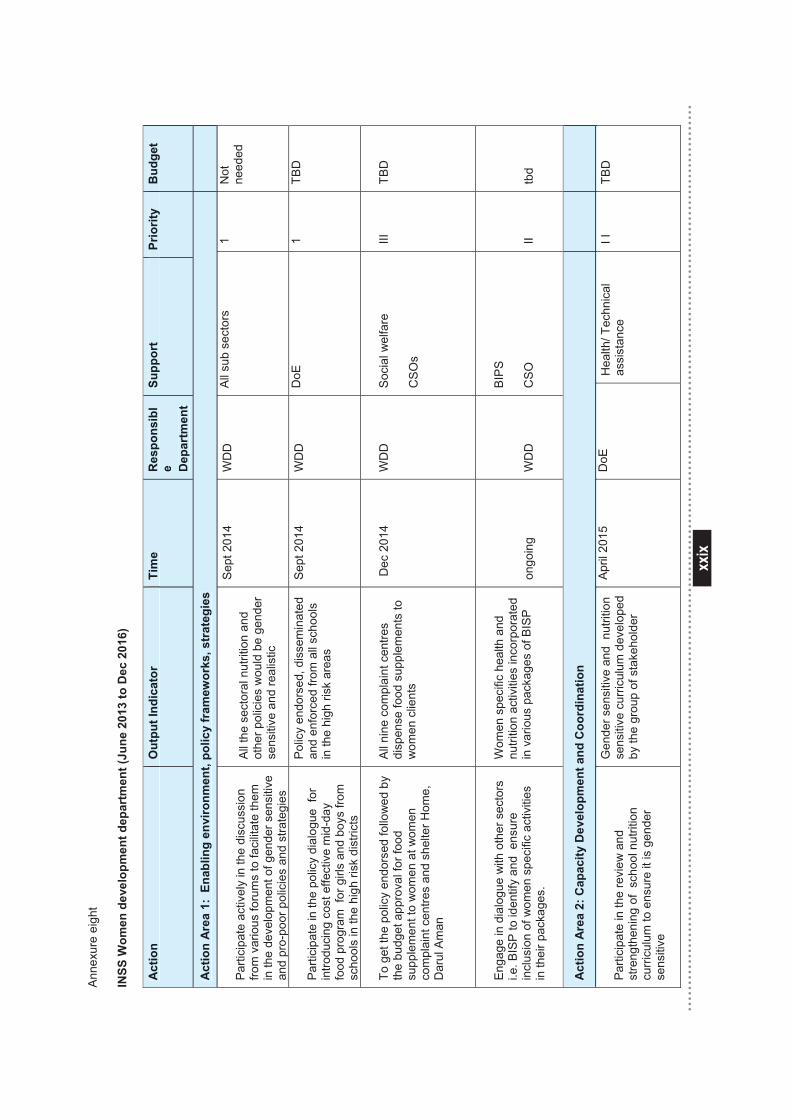
xxix
xxix
Anne
xure
eig
ht
INSS
Wom
en d
evel
opm
ent d
epar
tmen
t (Ju
ne 2
013
to D
ec 2
016)
A
ctio
n O
utpu
t Ind
icat
or
Tim
e R
espo
nsib
le D
epar
tmen
t
Supp
ort
Prio
rity
B
udge
t
Act
ion
Are
a 1:
Ena
blin
g en
viro
nmen
t, po
licy
fram
ewor
ks, s
trat
egie
s
Par
ticip
ate
activ
ely
in th
e di
scus
sion
fro
m v
ario
us fo
rum
s to
faci
litat
e th
em
in th
e de
velo
pmen
t of g
ende
r sen
sitiv
e an
d pr
o-po
or p
olic
ies
and
stra
tegi
es
All
the
sect
oral
nut
ritio
n an
d ot
her p
olic
ies
wou
ld b
e ge
nder
se
nsiti
ve a
nd re
alis
tic
Sep
t 201
4 W
DD
A
ll su
b se
ctor
s 1
Not
ne
eded
Parti
cipa
te in
the
polic
y di
alog
ue f
or
intro
duci
ng c
ost e
ffect
ive
mid
-day
fo
od p
rogr
am f
or g
irls
and
boys
from
sc
hool
s in
the
high
risk
dis
trict
s
Polic
y en
dors
ed, d
isse
min
ated
an
d en
forc
ed fr
om a
ll sc
hool
s in
the
high
risk
are
as
Sep
t 201
4 W
DD
D
oE
1 TB
D
To g
et th
e po
licy
endo
rsed
follo
wed
by
the
budg
et a
ppro
val f
or fo
od
supp
lem
ent t
o w
omen
at w
omen
co
mpl
aint
cen
tres
and
shel
ter H
ome,
D
arul
Am
an
All
nine
com
plai
nt c
entre
s di
spen
se fo
od s
uppl
emen
ts to
w
omen
clie
nts
Dec
201
4 W
DD
S
ocia
l wel
fare
CS
Os
III
TBD
Eng
age
in d
ialo
gue
with
oth
er s
ecto
rs
i.e. B
ISP
to id
entif
y an
d e
nsur
e in
clus
ion
of w
omen
spe
cific
act
iviti
es
in th
eir p
acka
ges.
Wom
en s
peci
fic h
ealth
and
nu
tritio
n ac
tiviti
es in
corp
orat
ed
in v
ario
us p
acka
ges
of B
ISP
ongo
ing
WD
D
BIP
S
CS
O
II
tbd
Act
ion
Are
a 2:
Cap
acity
Dev
elop
men
t and
Coo
rdin
atio
n
Par
ticip
ate
in th
e re
view
and
st
reng
then
ing
of s
choo
l nut
ritio
n cu
rric
ulum
to e
nsur
e it
is g
ende
r se
nsiti
ve
Gen
der s
ensi
tive
and
nut
ritio
n se
nsiti
ve c
urric
ulum
dev
elop
ed
by th
e gr
oup
of s
take
hold
er
April
201
5
DoE
H
ealth
/ Tec
hnic
al
assi
stan
ce
I I
TBD
Act
ion
Out
put I
ndic
ator
Ti
me
Res
pons
ibl
e Dep
artm
ent
Supp
ort
Prio
rity
B
udge
t
Act
ion
Are
a 1:
Ena
blin
g en
viro
nmen
t, po
licy
fram
ewor
ks, s
trat
egie
s
Act
ion
Are
a 2:
Cap
acity
Dev
elop
men
t and
Coo
rdin
atio
n
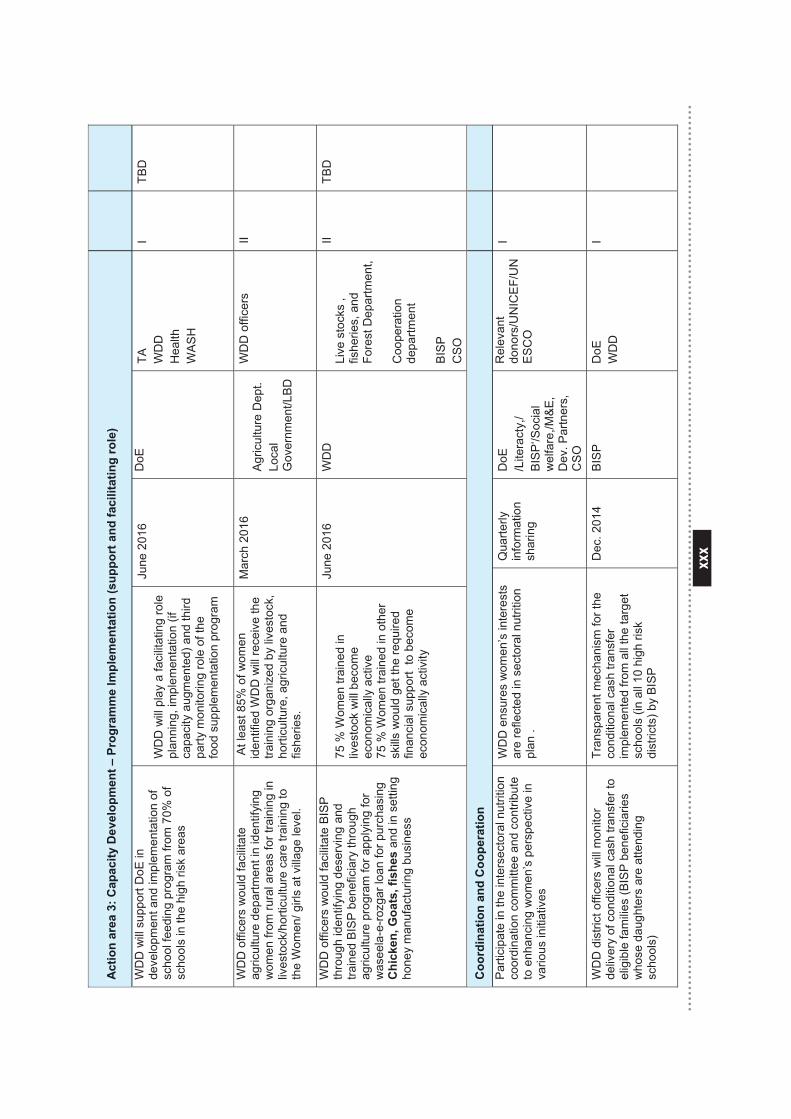
xxx
xxx
Act
ion
area
3: C
apac
ity D
evel
opm
ent –
Pro
gram
me
Impl
emen
tatio
n (s
uppo
rt a
nd fa
cilit
atin
g ro
le)
WD
D w
ill s
uppo
rt D
oE in
de
velo
pmen
t and
impl
emen
tatio
n of
sc
hool
feed
ing
prog
ram
from
70%
of
scho
ols
in th
e hi
gh ri
sk a
reas
WD
D w
ill p
lay
a fa
cilit
atin
g ro
le
plan
ning
, im
plem
enta
tion
(if
capa
city
aug
men
ted)
and
third
pa
rty m
onito
ring
role
of t
he
food
sup
plem
enta
tion
prog
ram
June
201
6 D
oE
TA
WD
D
Hea
lth
WA
SH
I TB
D
WD
D o
ffice
rs w
ould
faci
litat
e ag
ricul
ture
dep
artm
ent i
n id
entif
ying
w
omen
from
rura
l are
as fo
r tra
inin
g in
liv
esto
ck/h
ortic
ultu
re c
are
train
ing
to
the
Wom
en/ g
irls
at v
illage
leve
l.
At l
east
85%
of w
omen
id
entif
ied
WD
D w
ill re
ceiv
e th
e tra
inin
g or
gani
zed
by li
vest
ock,
ho
rticu
lture
, agr
icul
ture
and
fis
herie
s.
Mar
ch 2
016
Agr
icul
ture
Dep
t.
Loca
l G
over
nmen
t/LB
D
WD
D o
ffice
rs
II
WD
D o
ffice
rs w
ould
faci
litat
e B
ISP
th
roug
h id
entif
ying
des
ervi
ng a
nd
train
ed B
ISP
ben
efic
iary
thro
ugh
agric
ultu
re p
rogr
am fo
r app
lyin
g fo
r
was
eela
-e-ro
zgar
loan
for p
urch
asin
g
Chi
cken
, Goa
ts, f
ishe
s an
d in
set
ting
hone
y m
anuf
actu
ring
busi
ness
75 %
Wom
en tr
aine
d in
liv
esto
ck w
ill b
ecom
e ec
onom
ical
ly a
ctiv
e 75
% W
omen
trai
ned
in o
ther
sk
ills w
ould
get
the
requ
ired
finan
cial
sup
port
to b
ecom
e ec
onom
ical
ly a
ctiv
ity
June
201
6 W
DD
Li
ve s
tock
s ,
fishe
ries,
and
Fo
rest
Dep
artm
ent,
Coo
pera
tion
depa
rtmen
t
BIS
P
CS
O
II TB
D
Coo
rdin
atio
n an
d C
oope
ratio
n
Par
ticip
ate
in th
e in
ters
ecto
ral n
utrit
ion
coor
dina
tion
com
mitt
ee a
nd c
ontri
bute
to
enh
anci
ng w
omen
’s p
ersp
ectiv
e in
va
rious
initi
ativ
es
WD
D e
nsur
es w
omen
’s in
tere
sts
are
refle
cted
in s
ecto
ral n
utrit
ion
plan
.
Qua
rterly
in
form
atio
n sh
arin
g
DoE
/L
itera
cty,
/ B
ISP
‘/Soc
ial
wel
fare
,/M&
E,
Dev
. Par
tner
s,
CS
O
Rel
evan
t do
nors
/UN
ICE
F/U
NE
SC
O
I
WD
D d
istri
ct o
ffice
rs w
ill m
onito
r de
liver
y of
con
ditio
nal c
ash
trans
fer t
o el
igib
le fa
mili
es (B
ISP
ben
efic
iarie
s w
hose
dau
ghte
rs a
re a
ttend
ing
scho
ols)
Tran
spar
ent m
echa
nism
for t
he
cond
ition
al c
ash
trans
fer
impl
emen
ted
from
all
the
targ
et
scho
ols
(in a
ll 10
hig
h ris
k di
stric
ts) b
y B
ISP
Dec
. 201
4 B
ISP
D
oE
WD
D
I
Act
ion
area
3: C
apac
ity D
evel
opm
ent –
Pro
gram
me
Impl
emen
tatio
n (s
uppo
rt a
nd fa
cilit
atin
g ro
le)
Coo
rdin
atio
n an
d C
oope
ratio
n
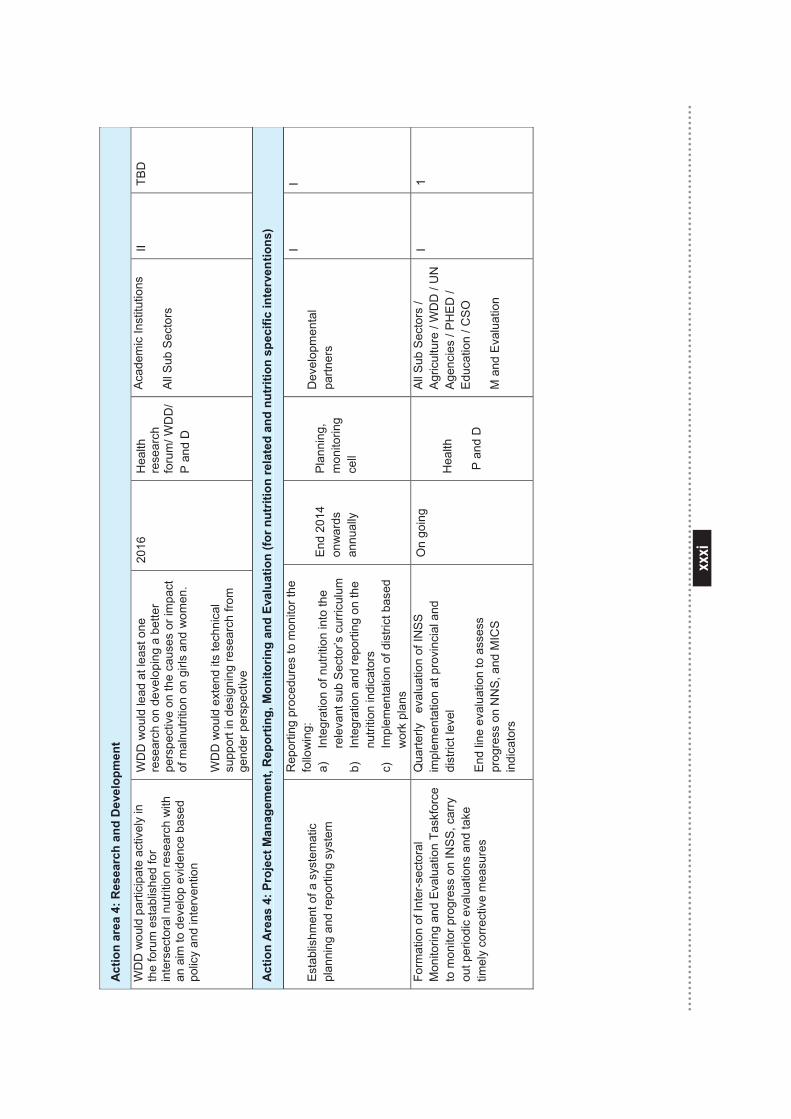
xxxi
xxxi
Act
ion
area
4: R
esea
rch
and
Dev
elop
men
t
WD
D w
ould
par
ticip
ate
activ
ely
in
the
foru
m e
stab
lishe
d fo
r in
ters
ecto
ral n
utrit
ion
rese
arch
with
an
aim
to d
evel
op e
vide
nce
base
d po
licy
and
inte
rven
tion
WD
D w
ould
lead
at l
east
one
re
sear
ch o
n de
velo
ping
a b
ette
r pe
rspe
ctiv
e on
the
caus
es o
r im
pact
of
mal
nutri
tion
on g
irls
and
wom
en.
WD
D w
ould
ext
end
its te
chni
cal
supp
ort i
n de
sign
ing
rese
arch
from
ge
nder
per
spec
tive
2016
H
ealth
re
sear
ch
foru
m/ W
DD
/ P
and
D
Aca
dem
ic In
stitu
tions
All
Sub
Sec
tors
II TB
D
Act
ion
Are
as 4
: Pro
ject
Man
agem
ent,
Rep
ortin
g, M
onito
ring
and
Eval
uatio
n (fo
r nut
ritio
n re
late
d an
d nu
triti
on s
peci
fic in
terv
entio
ns)
Est
ablis
hmen
t of a
sys
tem
atic
pl
anni
ng a
nd re
porti
ng s
yste
m
Rep
ortin
g pr
oced
ures
to m
onito
r the
fo
llow
ing:
a)
In
tegr
atio
n of
nut
ritio
n in
to th
e re
leva
nt s
ub S
ecto
r’s c
urric
ulum
b)
In
tegr
atio
n an
d re
porti
ng o
n th
e nu
tritio
n in
dica
tors
c)
Im
plem
enta
tion
of d
istri
ct b
ased
w
ork
plan
s
End
2014
on
war
ds
annu
ally
Pla
nnin
g,
mon
itorin
g ce
ll
Dev
elop
men
tal
partn
ers
I I
Form
atio
n of
Inte
r-sec
tora
l M
onito
ring
and
Eva
luat
ion
Task
forc
e to
mon
itor p
rogr
ess
on IN
SS
, car
ry
out p
erio
dic
eval
uatio
ns a
nd ta
ke
timel
y co
rrect
ive
mea
sure
s
Qua
rterly
ev
alua
tion
of IN
SS
im
plem
enta
tion
at p
rovi
ncia
l and
di
stric
t lev
el
End
line
eval
uatio
n to
ass
ess
prog
ress
on
NN
S, a
nd M
ICS
in
dica
tors
On
goin
g H
ealth
P a
nd D
All
Sub
Sec
tors
/ A
gric
ultu
re /
WD
D /
UN
A
genc
ies
/ PH
ED
/ E
duca
tion
/ CS
O
M a
nd E
valu
atio
n
I 1
Act
ion
area
4: R
esea
rch
and
Dev
elop
men
t
Act
ion
Are
as 4
: Pro
ject
Man
agem
ent,
Rep
ortin
g, M
onito
ring
and
Eval
uatio
n (fo
r nut
ritio
n re
late
d an
d nu
triti
on s
peci
fic in
terv
entio
ns)