Embed Size (px)
Citation preview

Intersection of Policy and Politics in State Coverage Expansion
Campaigns
Walter ZelmanProfessor, Director, Health Science ProgramCalifornia State University, Los [email protected] 323. 343.4635

Study Goals
Better understand the political dimension of coverage expansions
Provide value to those seeking such expansions
Increase research interest in that dimension, and provide starting points for more political analysis

Scratching the Surface
Study involves 5 states and multiple issues, options, and variables
Many could be the focus of a full study Given limited number of states, often
unclear what is an exception and what is trend
Result: Findings here as likely to be questions as answers
Study Methods and Sources
Review of public information:– Monitored newspapers– Web sites of interests and others– Reports, press releases, and other publicly
available documents
Interview about 5 individuals per state: participants and observers
Outline of Presentation
I Systemic Factors
II Processes of Policy Development
III Financing Reform and Cost Control
IV The Interests
V Strategy
VI Leadership

Systemic Factors: Complexity and Interconnectedness
The redistricting analogy: interrelated nature of the parts
Public and private sector connections Multiple interests, major economic
impacts likely to be involved in almost any issue
Hard to take one issue or opponent at a time

System Factors: the Institutions and the rules
Supermajority votes: the California problem 60 votes in the US Senate Political Science 101: the Madisonian model Rules may favor the status quo, especially
when interests are numerous and powerful: Thumbs on the checkerboard
Unlimited need for campaign funds, mostly from the interests

Systemic Factors: Federal Issues and Funding
ERISA Federal financing: Medicare, Medicaid,
SCHIP, disproportionate share, tax code, etc
Do states have tools to limit cost growth, and especially the major technological drivers?

Systemic Factors: Economic Cycles and Budgets
Best opportunities for reform may come when capacity to address the problem is low
Hard economic times raise visibility of the issue, but put pressure on state budgets: higher spending, lower revenues

Concerns and Economic Opportunity
High concern about costs and/or coverage
Low concern about costs and/or coverage
Strong or recovering economy
1993-94 1996-2001
Weak economy Current situation for states
?

Policy Development: Private Processes
Governors and private processes– Good staff talent– Largely private– Appreciation of complexity: led to expanded
concepts to reform, more focus on cost Romney: came to individual mandate Rendell: moved from fed to state focus and more
focus on small business and economy Schwarzenegger: all connected Spitzer: need to move incrementally: kids first

Policy Development: Public Processes
Varieties of public processes and outputs– Road maps: MA, NY– Task forces: hearings, reports, differently
constituted: IL, PA, NY– All states except California– Varied purposes and value:
May reflect emphasis on search for evidence-based, consensus solutions
Financing Options: Employer Requirements
Trend may be to modest levels: – Low percentage requirements– Perhaps a sliding scale
Demands on employers may be limited by concerns about economic impacts– Particularly true for small employers who
barely seem to even need organized lobbying power: others use them to make the case

Financing Options: Employer Requirements
Final or Pending Position
Notes
California 1-6% fee on non-offering employers
Compromise between Gov (4%) and Dems (7.5%)
Illinois 3% assessment on employers spending <4%
Remains unchanged; measure likely to fail
Massachusetts $295 per year per ee on non-insuring employers
Compromise between no tax and House leadership
Pennsylvania No pay or play requirement
Gov proposed 3% tax for non-insuring employers

Financing Options: Employers
Chambers, like most associations, may continue to reflect lowest-common denominator positions
There is evidence of some employer willingness to accept some “shared responsibility”
– But, support may require protection in out –years– Apparent, sizable reluctance to break ranks
Individual business supporters or coalitions can reduce appearance of across-the-board business opposition
May even be possible to win appearance of small business support

Financing: Individual Mandate
Logic for mandate seems strong: May increase number of offering employers Probably needed to fix individual market Politically, may required to win business, insurer
support Is possible to protect low-income families Eventually accepted in MA; limited version in CA; IL
task force accepted it

Financing: Individual Mandate
But opposition still considerable: All states Slippery slope away from employer
responsibility: Uncertainty trumps economics Large deductibles may make it affordable, but
also less attractive It is a hard sell for unions and to consumers Politically, support may require imposition of
requirements on employers

Financing: Federal Funds
State reform as federal reform All states report funding as the central
challenge: especially in lean years States still wary of imposing broad taxes Successful state efforts will probably
require more access to federal funds States with great disproportionate share
funds may have greater capacity

Percent who say they would support a universal health insurance system even if it…
Let’s Not Forget… Public Debates Matter
35%
33%
28%
18%
Limited their choice of doctors
Meant some treatments currently covered would no longer be covered
Meant there were waiting lines for non-emergency treatments
Meant they would pay either higher premiums or more taxes
Source: ABC News/Kaiser Family Foundation/USA Today Health in America Survey (conducted September 7-12, 2006)
Percent who support a universal health insurance system, in which everyone
is covered by a program like Medicare that is gov’t-run
and financed by taxpayers
56% 40%
Percent who support the current system, in which most people are covered through private employers, but some people have no insurance

Financing: Cost Control
Policymakers clearly see tie they once did not see: costs rising faster than wages
Public concern on costs also high Some see cost control, improving system,
as key to framing: not uninsured But public appears unwilling to deal with
hard choices here

Pennsylvania’s Employees and Businesses Cannot Keep Up with Health Care Inflation
% Increase in Family Health Insurance Premiums vs. Inflation and Increase in Median Wages in PA Between 2000 and 2006
13.3%
17.0%
75.5%
Increase in Median Income
Inflation
Increase in Premiums
WalterZelman Presentations

Projected Average Annual Growth in Illinois Health Care Spending Without Reform,
Gross State Product and Wages 2005 - 2015
7.50%
4.80%
3.20%
0%
2%
4%
6%
8%
Wages Gross StateProduct
Health Care
Av
era
ge
An
nu
al G
row
th 2
00
5-2
01
5
WalterZelman Presentations

American Views on Most Important Issue for Government:
% Saying Issue is One of Two Most Important
43
34
1511
83
05
101520253035404550
Costs Access forUninsured
Medi/Rx Quality Gov Role IllegalImmigration
Source: AP, 2006

Factors seen as “Very Important” Reasons for Health Cost Increases
6560 57
46
36
0
10
20
30
40
50
60
70
Drug /ins profit Was te/fraud C os t of Unins Malprac L aw New tec h/pro.
Ca Field Poll Jan 2007

Financing: Cost Control
Two conflicting themes Cannot achieve or sustain reform without
cost control Cannot achieve reform with cost control Conflict: easiest way to reduce interest
group opposition is expanding, not contracting the pie

The Interests: Organized Labor
Much of labor may lack enthusiasm for centrist approaches
Traditional labor position: employer required to pay 80% of defined benefit
Mixed reports on labor support in 2007-08– Issues with labor in MA, IL, CA– SEIU more supportive than AFL: health care
workers, lower wage workers AFL more concerned on costs than SEIU Purchaser, provider conflict?
The Interests: Organized Labor
Concerns about individual mandate and slippery slopes
Concerns about level playing fields Concerns about loss of union benefits as a
recruiting tool Concerns about paying higher costs/taxes so
that non-union employers can get subsidized coverage

Hospitals
Provider and leader in business community Have been important supporters: Mass, Ill Can be major force for reform: sees benefits,
can lead in some business communities Ideal interest group: a leader in virtually
every district; Boards are who’s who of community

Hospitals
Multiple problems in hospital leadership Trade associations may not lead: reform may
produce winners and losers Safety net, DSH hospitals will demand
protection even as fewer dollars are needed Multiple concerns about changes, reductions
in revenue streams Support of hospitals may require a larger pie

Physicians
Not reported to be playing major roles Negative in some states: insignificant in
others Specialty associations may be drawing
more members Primary care and family physicians
different; can they fill the void?

Health Plans
Some supportive of coverage expansions: Can be sizable business asset– If insurance model unchallenged, regulatory
elements limited and market rules acceptable
Support may require individual mandate Those with underwriting models may be
vigorous opponents
Consumers
Need much more study Broad coalitions appear effective: but
capacity to mobilize public may be limited Role of labor in these coalitions needs
study Religious ties effective in several cases:
produce real credibility

Consumers
Little evidence of significant public pressure – Public attention to state issues way below that
of federal Single payer leverage down: consumer
groups support it, but more in theory than practice– But may still maintain capacity to undermine
other reform efforts (California)

Strategies: Partisan and Centrist
Consensus-building strategies seem dominant: – Republican votes rare; but Democrats need
business and provider allies– Public, stakeholder processes may reflect that
perceived need
Cost control now central to strategy

Leadership: Some Findings
Systemic forces may be most important in long run, but leadership and specific decisions matter
Many leaders made major efforts But many reports of major animosity between
key players: NY, CA, ILL Significant input re Governors not
maintaining positive, respectful relations with legislators

Leadership in Massachusetts
More recognition of leaders and leadership in Massachusetts?– Is it just the result of success?– Or, did leadership really emerge and why?
Greater perception of shared need to succeed

Five States: a Positive View
Massachusetts succeeded Illinois has made progress, might have
made more: tax proposal hurt, Governor’s relations with Speaker hostile
Pennsylvania: some progress made, issue still in doubt
California: came close New York: has potential

Five States: an Alternative View
Massachusetts Unique No new successes in 2007 Obstacles vary, but always substantial: costs,
complexity, multiple interests Primary problem is finding a political coalition
that will support the cost reductions or new financing needed
Creating, sustaining state reforms may require major federal assistance

Some Future Research Needs
Analysis of interest group positions. What might change, what won’t: hospitals, labor, physicians
Processes for seeking input and building support: on costs and coverage

Premiums and Poverty Levels2000 2007 Percent
Increase
250% of PovertyFamily of Four
44,007 51,625 17
HMO Family Premium
5,844 11,879 103
Premium as % of 250% of Poverty
13.2 22.9

What is Affordable?
Need to subsidize to higher levels of poverty
Cap on family spending 15% of income Premium is $11,879 Income needed: $79,193 % of poverty: 383
WalterZelman Presentations

A Tale of Two States
Massachusetts California
Percent of non-elderly population uninsured
11 19
Percent of non-elderly adults under 200% of poverty
29 39
Percent of those adults uninsured
23 44
WalterZelman Presentations

A Centrist Strategy: Core Premises
Must minimize widespread interest group opposition
Accept coverage before effective cost control
Accept up-front, additional cost: consider use of incentives for additional federal $
Primary reliance on expansions of federal programs for new dollars

A Centrist Strategy: Core Elements
Modest, individual mandate with adequate protections on affordability– Coverage would have to be broad: deductibles
or co-pays might be middle range Modest, scaled employer mandate (ERISA
flexibility or safe harbors may be required)– Some mechanism to protect against near-
automatic increases in employer fee

A Centrist Strategy: Core Elements
Reliance on expansions of federal programs for additional state funds– May need to include higher provider payments– Builds on current programs– Does not create new programs– Assumes a national strategy: federal
requirements with state flexibility

A Centrist Strategy: Core Elements
Connector, pool, FEHB-type mechanism to ease subsidy, individual market, and “pay” employee mechanisms– Capacity of pool to expand may prove critical– Potential to gain single payer support
Framing: security (keep what you like, won’t lose insurance), affordability, prevention
Revenue: federal tax exclusion change?

A Centrist Strategy: Core Elements
Visible public process to seek input from stakeholders and public and craft policy– Runs counter to traditional honeymoon strategy:
right choice may depend on margin of victory
High level commitment or commission to address long-term strategy for cost control
Alliances with sub-groups of major interests: Physicians, large and small employers, insurers

Let’s Not Forget… Agreement On Goals Easy, Solutions Hard
Percent who FAVOR
88%
37%
74%
73%
70%
80%
Tax credits for businesses
Requiring businesses to offer insurance to employees
Expanding state government programs such as Medicaid
Tax credits for individuals
Expanding Medicare to people under age 65
When forced to choose…
Percent who say “MOST preferred option”
National single-payer plan
23%
15%
13%
17%
12%
17%
Source: Kaiser Family Foundation/Harvard Health Care Agenda for the New Congress Survey November, 2004

Let’s Not Forget… Personal Status Quo = Not So Bad, Change = Scary
Source: ABC News/Kaiser Family Foundation/USA Today Health Care in America Survey (conducted September 7-12, 2006)
15%
15%
20%
26%
16%
17%
19%
20%
Percent saying that a universal health insurance system would make each of the following better…
Cost of your/your family’s health care
Availability of treatment to you/your family
Quality of your/your family’s health care
Your/your family’s choice of doctors & hospitals
Amount you pay for medical care
Your choice of doctors
Quality of care available to you
You personally
Percent saying the Clinton Health Care Reform Plan would have a positive effect on…
Source: Gallup/CNN/USA Today Poll, April 1994

Percent who say they would support a universal health insurance system even if it…
Let’s Not Forget… Public Debates Matter
35%
33%
28%
18%
Limited their choice of doctors
Meant some treatments currently covered would no longer be covered
Meant there were waiting lines for non-emergency treatments
Meant they would pay either higher premiums or more taxes
Source: ABC News/Kaiser Family Foundation/USA Today Health in America Survey (conducted September 7-12, 2006)
Percent who support a universal health insurance
system, in which everyone is covered by a program like
Medicare that is gov’t-run and financed by taxpayers
56% 40%
Percent who support the current system, in which most people are covered through private employers, but some people have no insurance

Sources of Influence
Electoral power Direct Lobbying Indirect lobbying, including grass roots Campaign contributions Influence over, access to one key player, committee or process Access to free media Direct to public advertising Community Support Public Credibility Limited, focused agenda Internal agreement on policy options

Key Interests and Sources of Power
Physicians Lobbying, campaign $, access to media, public credibility
Hospitals Lobbying, campaign dollars, community support
Health Plans Lobbying, campaign $, direct advertising
Pharmaceutical companies Direct advertising, lobbying, campaign $
Consumer groups Access to media, public credibility
Chiropractors Campaign dollars, focused agenda
Seniors/Medicare Electoral power, grass roots/indirect lobbying, volunteerism

Lobbying Expenditures by Industry
California, in Thousands
Health $11,490
Manufacturing/Industrial $9,904
Education $8,864
Finance and Insurance $8,649
Utilities $8,458
Source: California Secretary of State

Lobbying Expenditures, 2002
California Medical Assn $568,000
California Healthcare Assn $686,000
California Assn of Health Plans $128,000
Ca Assn of Physician Groups $102,000
PHRMA $151,000
Source: California Secretary of State

Number of Contributions MadeJanuary-June, 2003
California Medical Assn 125
California Healthcare Assn 114
California Association of Health Plans 57

Contributions of the California Medical Assn, One Committee, 2001-2002
Governor Davis $100,000
Senator John Burton c. $26,000
Assemblyman Sam Aanestad c. $72,000
Assemblywoman Charlene Zettel c. $37,000
Assembly candidate Nakanishi c. $53,000
Attorney General Lockyer c. $12,000
Total to all candidates c. $1,300,000

Systemic Environment: Traditional and Unique obstacles
Traditional obstacles of fragmented government, limited mandates, supermajority votes, dependence of policymakers on special interest campaign financing
Unique obstacles: interrelatedness of parts, inability to separate issues, face “one enemy at a time.”
Framing in the States
Plight of uninsured still the cause But is clearly an effort to link this problem to
a larger problem that is causing harm to all Shared responsibility is popular, positive
construct: But may not lead to breakthrough policy agreement
Cost and coverage clearly linked

Framing
Some framing issue as “broken system:” Coverage as part of larger problem that must be addressed as a whole
Cost and coverage problem linked to affordability for business and drain on economy
Hidden taxes, emergency rooms, all paying for the uninsured

Framing: Old and New ideas
President Clinton security theme in less evidence: might be cleaner than more complex “broken system” frames
Given rising economic concerns, advocates, candidates may wish to consider framing health problem as part of economic downturn

Two Strategies
Centrist/Bipartisan Democratic Partisan
Cost Coverage
Limit the opposition Build the base
Business/economic case Moral case
Public process Mobilization of support
Risks low-energy support Risks interest group opposition, narrow base
Shared responsibility Primarily Employer/Gov financed, no indiv mandate
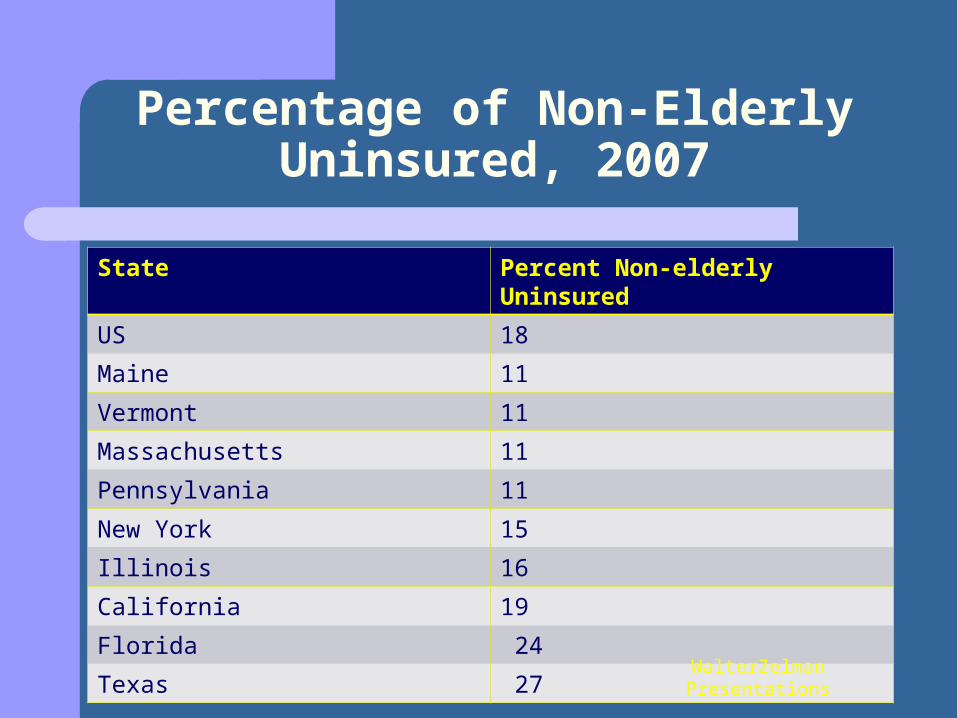
Percentage of Non-Elderly Uninsured, 2007
State Percent Non-elderly Uninsured
US 18
Maine 11
Vermont 11
Massachusetts 11
Pennsylvania 11
New York 15
Illinois 16
California 19
Florida 24
Texas 27WalterZelman Presentations

A Centrist strategy: Core Premises
Must minimize widespread interest group opposition Accept coverage before effective cost control
--Public still uncomfortable with trade-offs
--Provider opposition likely
--Public unrealistic on real issues
--Significant reductions in benefits not acceptable to Dems and support groups

Areas of interest
Systemic factors: Rules of the game, largely beyond control of state policymakers
Matters of process: policy development Major Interest groups; their goals and
perceived impacts of various policies on them
The toughest policy issue: Sources of funding

Areas of Interest
Strategy and framing Political leadership Options for going forward

Conclusions and Suggestions:Massachusetts as Unique
Low number of uninsured High per capita income Financial imperative Network of players One-party legislature
Still: effort came close to failure

Processes: Lessons
Need to pursue appearances if not reality of listening to public and stakeholder concerns– May reflect emphasis on search for evidence-
based, consensus solutions– Partisan, non-consensus approach probably would
not do this Process leads to greater awareness of linkage of
the parts, broader reform Reform may take time: to pursue a process, work
out differences, negotiate






























