Embed Size (px)
Citation preview

REVIEW ARTICLE Abhijit et.al / IJIPSR / 3 (6), 2015, 663-687
Department of Pharmaceutical Technology ISSN (online) 2347-2154
Available online: www.ijipsr.com June Issue 663
PATHOPHYSIOLOGICAL BASIS OF ERECTILE
DYSFUNCTION IN DIABETES MELLITUS: A REVIEW
1Abhijit De*,
2Mamta Farswan Singh,
3Vinod Singh,
2Veerma Ram,
2Shradha Bisht
1Department of Pharmaceutical Technology, Bengal School of Technology, Sugandha,
West Bengal, INDIA 2Department of Pharmacy, SBS PG Institute of Biomedical Sciences, Balawala, Dehradun,
INDIA 3Faculty of Pharmacy, Gurukul Kangri University, Haridwar, INDIA
Corresponding Author
Abhijit De
Assistant Professor, Dept. of Pharmaceutical Technology
Bengal School of Technology, Sugandha, West Bengal, INDIA
Email: [email protected]
Phone: +91 8274847571
International Journal of Innovative
Pharmaceutical Sciences and Research www.ijipsr.com
Abstract
Erectile dysfunction is a common complication of diabetes mellitus and also is the first symptom of as yet
undiagnosed diabetes. The Massachusetts Male Aging Study (MMAS) was the first major epidemiological
investigation to study the prevalence of ED in diabetes. According to MMAC the incidence of ED was correlated
with glycemic control and increases with increasing age, duration of diabetes and deteriorating metabolic control,
and was higher in individuals with type 2 diabetes than those with type 1 diabetes. The pathophysiology of ED in
diabetes is multifactorial including vascular and neural factors being equally implicated. In diabetic men,
peripheral vasculopathy and neuropathy are intimately involved in the development of ED. Diabetic patients
associated with insufficient control of glycemic level extremely suffer from disruption of endothelial functions,
generation of increased level of free radicals, loss of control in the parasympathetic and non adrenergenic non
cholinergic nerves (NANC). In diabetic patients hypogonadism, autonomic neuropathy, arterial insufficiency, low
testosterone, changes in expression of protein kinase C, RhoA-Rho kinase Ca2+
-sensitization pathway results in
vascular damages of penile smooth muscle which are more or less related to erectile dysfunction. Penile tissue
from diabetic men with ED demonstrates impaired neurogenic and endothelium-mediated relaxation of smooth
muscle, increased accumulation of advanced glycation end products (AGEs) and upregulation of arginase which
lead to decrease in the level of NO in corpora cavernosa. Still there is a need to understand the pathophysiology of
ED in diabetic patients and to make an effort to diagnose and treat ED for improving the quality of life of the
patients of diabetes. This review aimed to provide an update of the normal physiology of penile erection and the
pathophysiological mechanisms of erectile dysfunction (ED) in diabetes patients.
Keywords: Diabetes Mellitus, Erectile dysfunction, Oxidative stress, Advanced glycation end products,
Arginase, Rho Kinase, Tumor Necrosis Factor.
REVIEW ARTICLE Abhijit et.al / IJIPSR / 3 (6), 2015, 663-687
Department of Pharmaceutical Technology ISSN (online) 2347-2154
Available online: www.ijipsr.com June Issue 664
INTRODUCTION
Diabetes mellitus is one of the major risk factor for cardiovascular mortality and morbidity.
Diabetes mellitus has been shown to be an important risk factor for ED in several studies [1].
Based on the types of diabetes whether type I or type II, still it is a controversial point that which
type of diabetes actually play a vital role in altering sexual behavior of human. Male sexual
dysfunction among diabetic patients can include disorders of libido, ejaculatory problems, and
erectile dysfunction (ED) [2,3,4]. In diabetes mellitus erectile dysfunction is mainly associated
with increasing age and time of evolution of diabetes [5,6,7,8]. Chronic hyperglycemia in diabetic
patients may lead to micro- and macrovasculopathy, including endothelial dysfunction [9,10].
DM is responsible for several biochemical and homeostasis alterations that may result in male
subfertility and or infertility [11].
Hypogonadism, autonomic neuropathy, and arterial insufficiency are associated with a higher
likelihood of ED in cross-sectional and longitudinal studies of men with diabetes [12,13,14].
Androgen deficiency in diabetic rats is associated with downregulation of the neuronal isoforms
of nitric oxide synthase, suggesting a trophic effect of testosterone on peripheral erectile tissues.
Relaxation of penile tissue requires nitric oxide from nonadrenergic-noncholinergic neurons and
the endothelium [15]. Penile tissue from diabetic men with ED demonstrates impaired neurogenic
and endothelium-mediated relaxation of smooth muscle, [16] increased accumulation of advanced
glycation end products (AGEs),[17] and upregulation of arginase, a competitor with nitric oxide
synthase for its substrate L-arginine [18]. Erectile dysfunction is defined as the ability of the male
to attain and maintain penile erection which is sufficient to permit sexual intercourse upto
satisfactory level [19]. Epidemiological data focused that majority of men with DM is prone to
ED. In a study done in 541 DM men aged 20-59 years, 35% of ED was reported [20]. This
condition has been estimated to affect 150 million individuals worldwide and data from the
ENIGMA study in 2004 suggested that the condition is prevalent in approximately 17% of all
European men [21,22].
Approximately 20–30 million men in the United States and approximately 0.5 million men in the
UK have ED of varying severity. According to the Massachusetts Male Aging Study, 52% of men
in the United States between the ages of 40 and 70 years have ED [23].
The incidence is approximately 32% in the United Kingdom, 26% in Japan and 19% in Denmark
[24,25,26]. In the same study, it was found that the risk of cardiovascular complication was higher

REVIEW ARTICLE Abhijit et.al / IJIPSR / 3 (6), 2015, 663-687
Department of Pharmaceutical Technology ISSN (online) 2347-2154
Available online: www.ijipsr.com June Issue 665
in patients with non-insulin dependent diabetes that suffered from ED compared with the diabetic
patients who did not have ED [27].
In this article, we will discuss the factors and
pathophysiological mechanisms responsible for erectile dysfunction in diabetic patients.
BASIC PHYSIOLOGY OF PENILE ERECTION
Erection is a neurovascular event that involves spinal and supra spinal pathways. Penile erection
can arise from various stimuli include tactile stimuli to penis leading to reflex erection, the second
mechanism include erotic stimuli, whether visual, auditory, olfactory or imaginative also produce
erection through the stimulation of paraventricular nucleus and medial preoptic area of the
hypothalamus and the third mechanism involved in the production of nocturnal erection during
REM sleep [28]. The final common pathway involves the release of nitric oxide (NO) from both
endothelial cells and neurons, which acts as a vasodilator causing penile engorgement and
erection. Studies over the past years supports the vital role of endothelial-derived NO from eNOS
in the regulation of penile erection both in normal physiology and in pathological disease states.
Penile erection is elicited by neural signals from the spinal cord, which increases nNOS activity
and the production of NO from NANC nerves, thereby causing an increase in blood flow to the
cavernosal tissue [29,30]. eNOS is then activated by increased blood flow from the arteries
supplying the corpora and expansion of the sinusoidal spaces of the corpora and thereby causing
penile erection REF. Hurt and colleagues (2002), by using selective pharmacological inhibitors
and eNOS knockout mice, showed that penile erection-dependent processes to cavernosal nerve
stimulation and drug-induced relaxation of the corpus cavernosum are mediated by
phosphatidylinositol 3-kinase (PI3-kinase) and activation of the serine/ threonine protein kinase
Akt [31].
This pathway phosphorylates eNOS to increase endothelial-derived NO [32].
The use of pharmacological inhibitors of PI3- kinase in the penis of rats demonstrated that these
inhibitors were able to reduce erections to electrical nerve stimulation. This signaling pathway
was furthermore shown to be responsible for sustained NO production via a PI3 kinase/ Akt-
dependent activation of eNOS with subsequent increases in the release of endothelial-derived NO.
NO then diffuses to the underlying smooth muscle cells where it activates the soluble form of
guanylate cyclase and elevates intracellular levels of cGMP and the activity of cGKI protein
kinase. The NO/cGMP-signaling cascade reduces contractile activity and promotes cavernosal
smooth muscle relaxation REF.
REVIEW ARTICLE Abhijit et.al / IJIPSR / 3 (6), 2015, 663-687
Department of Pharmaceutical Technology ISSN (online) 2347-2154
Available online: www.ijipsr.com June Issue 666
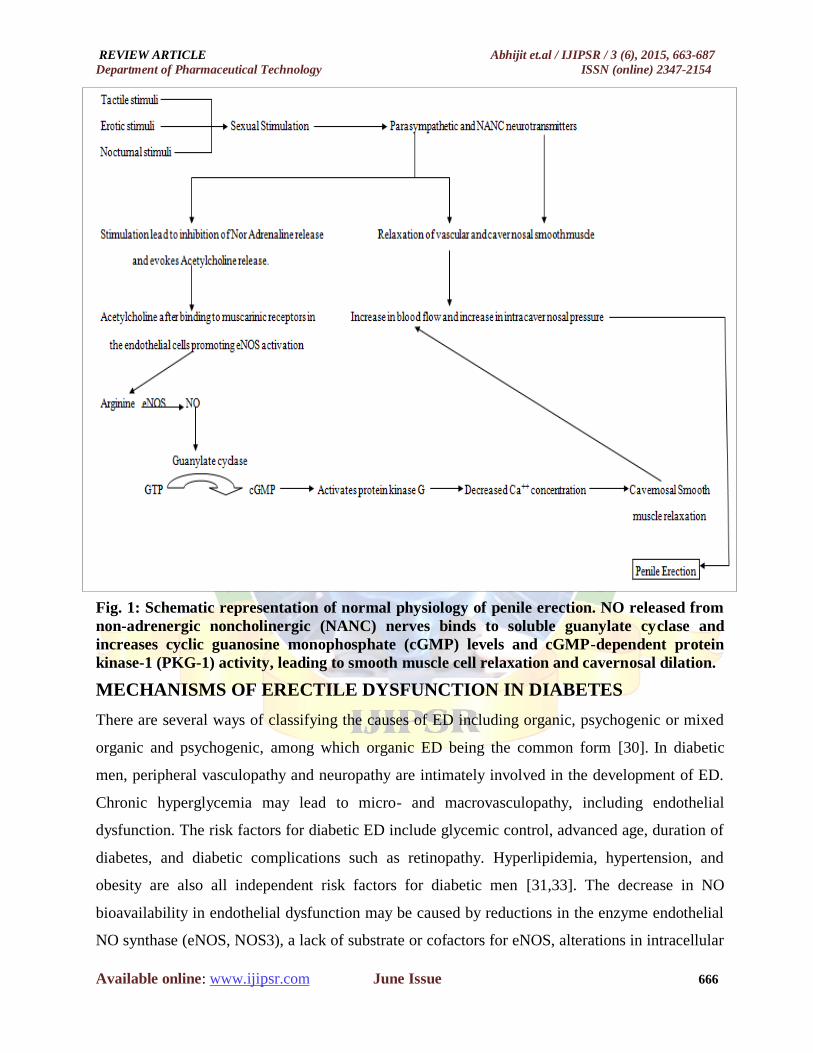
Fig. 1: Schematic representation of normal physiology of penile erection. NO released from
non-adrenergic noncholinergic (NANC) nerves binds to soluble guanylate cyclase and
increases cyclic guanosine monophosphate (cGMP) levels and cGMP-dependent protein
kinase-1 (PKG-1) activity, leading to smooth muscle cell relaxation and cavernosal dilation.
MECHANISMS OF ERECTILE DYSFUNCTION IN DIABETES
There are several ways of classifying the causes of ED including organic, psychogenic or mixed
organic and psychogenic, among which organic ED being the common form [30]. In diabetic
men, peripheral vasculopathy and neuropathy are intimately involved in the development of ED.
Chronic hyperglycemia may lead to micro- and macrovasculopathy, including endothelial
dysfunction. The risk factors for diabetic ED include glycemic control, advanced age, duration of
diabetes, and diabetic complications such as retinopathy. Hyperlipidemia, hypertension, and
obesity are also all independent risk factors for diabetic men [31,33]. The decrease in NO
bioavailability in endothelial dysfunction may be caused by reductions in the enzyme endothelial
NO synthase (eNOS, NOS3), a lack of substrate or cofactors for eNOS, alterations in intracellular

REVIEW ARTICLE Abhijit et.al / IJIPSR / 3 (6), 2015, 663-687
Department of Pharmaceutical Technology ISSN (online) 2347-2154
Available online: www.ijipsr.com June Issue 667
signaling such that eNOS is not appropriately activated or uncoupled or accelerated degradation
of NO by reactive oxygen species (ROS), such as superoxide anion. Endothelial dysfunctions,
venous occlusion, decrease in nitric oxide level, failure of mechanisms of vasodilation and
formation of advanced glycation end products can be contributing factor for diabetes induced ED
[34].
DIABETES AND ENDOTHELIAL DYSFUNCTION
The term Endothelial dysfunction refers to a condition in which the healthy endothelial monolayer
diminishes its physiologic properties and impair dilatory mechanism by shifting towards a
vasoconstrictor and proinflammatory state [35].
The importance of endothelium was first
identified by its effect in limiting the vascular tone [36]. Various vasoconstricted and vasodilated
agents are involved in the physiology of penile erection. Cavernosal smooth muscle cells in the
penis are predominately found in the contracted state with minimal blood flowing through the
cavernous sinuses. The balance between known contractile systems (RhoA/Rho-kinase, a-
adrenergic, endothelin, angiotensin, thromboxane A2) and vasodilatory second-messenger
systems (adenylate cyclase-cyclic AMP and guanylate cyclase-cyclic GMP) determines the
overall tone of corpora cavernosa smooth muscle of the penis [37,38]. Damaged to endothelial-
dependent vasoreactivity has been demonstrated in various animal models. Various studies
performed on human and animal models indicates that in diabetes upregulation of endothelin 1
and Ag-II takes place which further causes contraction of the smooth muscles of corpora
cavernosa and flaccidity of penis. Jesmin et al observed a decrease of the immunofluroscent
staining of e NOS and the expression of this enzyme in the penile tissue of obese rats with respect
to controls [39]. Three contributing sources to endothelial dysfunction in diabetes include
alteration of endothelial function directly by hyperglycemia and its biochemical product,
alteration of endothelial function by high glucose through the synthesis of growth factors and
vasoactive agents in other cells which then alter the vascular permeability and alteration of
endothelial function by components of metabolic syndrome [40]. Endothelial dysfunction is
mainly related to decreased expression or activity of eNOS which results in decreased
bioavailability of NO and associated signaling molecules such as protein kinase C. Various
molecules are involved in the pathogenesis of endothelial dysfunction in diabetes such as free
radicals, arginase, NO, Rho-rho kinase, protein kinase C, tumour necrosis factor - α (TNF- α) and
advanced glycation end products.
REVIEW ARTICLE Abhijit et.al / IJIPSR / 3 (6), 2015, 663-687
Department of Pharmaceutical Technology ISSN (online) 2347-2154
Available online: www.ijipsr.com June Issue 668
OXIDATIVE STRESS AND ERECTILE DYSFUNCTION
ROS may modify endothelial function directly by activating several transcription factors leading
to the upregulation of adhesion molecules to platelets and leukocytes and decreasing the
bioavailability of NO or indirectly by increasing the formation of advanced glycation end
products (AGEs) or increasing oxidation of low density lipoprotein [41,42].
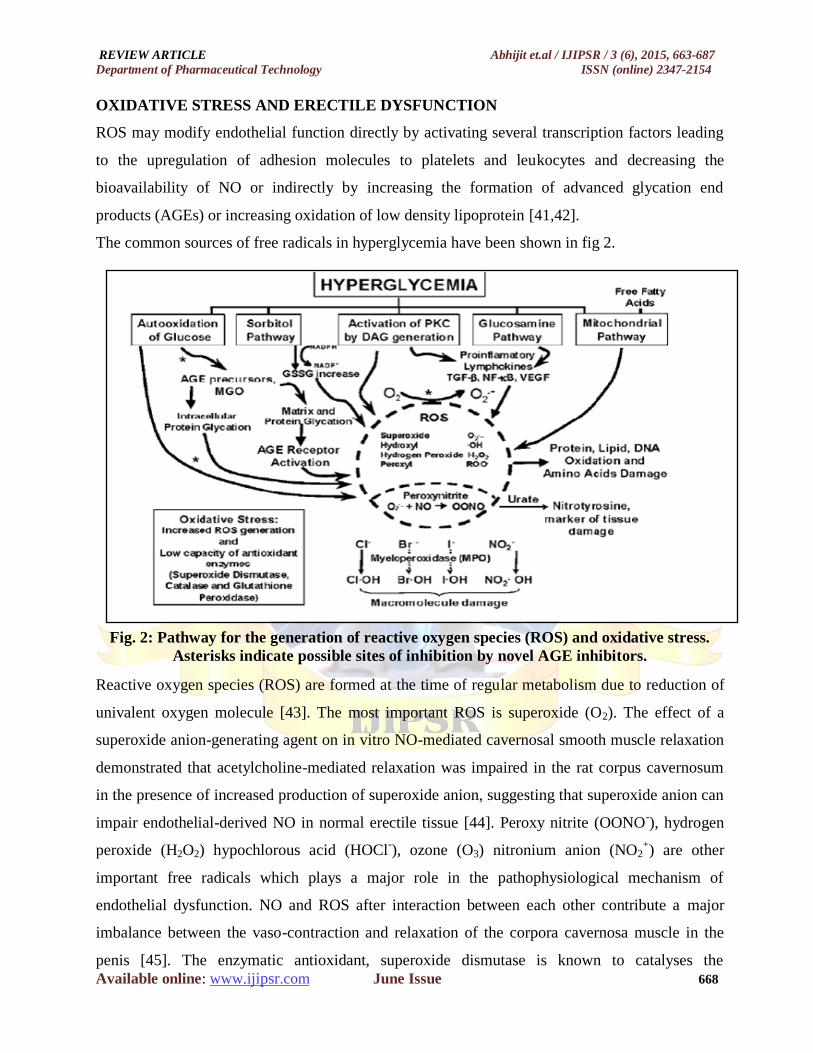
The common sources of free radicals in hyperglycemia have been shown in fig 2.
Fig. 2: Pathway for the generation of reactive oxygen species (ROS) and oxidative stress.
Asterisks indicate possible sites of inhibition by novel AGE inhibitors.
Reactive oxygen species (ROS) are formed at the time of regular metabolism due to reduction of
univalent oxygen molecule [43]. The most important ROS is superoxide (O2). The effect of a
superoxide anion-generating agent on in vitro NO-mediated cavernosal smooth muscle relaxation
demonstrated that acetylcholine-mediated relaxation was impaired in the rat corpus cavernosum
in the presence of increased production of superoxide anion, suggesting that superoxide anion can
impair endothelial-derived NO in normal erectile tissue [44]. Peroxy nitrite (OONO-), hydrogen
peroxide (H2O2) hypochlorous acid (HOCl-), ozone (O3) nitronium anion (NO2
+) are other
important free radicals which plays a major role in the pathophysiological mechanism of
endothelial dysfunction. NO and ROS after interaction between each other contribute a major
imbalance between the vaso-contraction and relaxation of the corpora cavernosa muscle in the
penis [45]. The enzymatic antioxidant, superoxide dismutase is known to catalyses the

REVIEW ARTICLE Abhijit et.al / IJIPSR / 3 (6), 2015, 663-687
Department of Pharmaceutical Technology ISSN (online) 2347-2154
Available online: www.ijipsr.com June Issue 669
dismutation of superoxide to hydrogen peroxide and oxygen. This enzyme mainly involves in the
removal of superoxide radicals from the human body and hence prevents the adverse effects of
superoxide in vasculature. It was hypothesized that the administration of the superoxide dismutase
(SOD) mimetic Tempol (4- hydroxy-2, 2, 6, 6-tetramethylpiperidine 1-oxyl) may reverse
diabetes-induced erectile dysfunction. To test this hypothesis, reactive oxygen species-related
genes (SOD1, SOD2, GP-1, CAT, NOS2, and NOS3) were tested and erectile functional studies
and immunohistochemical analysis were carried out in diabetic rats treated with or without
Tempol [46,47]. A decrease in CAT mRNA expression was observed in diabetes but there was no
change in CAT protein levels between control and diabetes whereas NOS2 (iNOS) mRNA and
protein levels were increased in diabetic rats [48]. Administration of Tempol to diabetic rats
inhibited superoxide overproduction. It also reversed the increase of iNOS mRNA expression in
rat crura and release of nitric oxide from endothelial cells leading to decreased formation of
peroxynitrite. Hyperglycemia in diabetes also favors increased expression of iNOS (NOS2)
through the activation of stress sensitive pathways such as NF-eˆB, which can increase the
generation of NO [49]. Superoxide immediately interacts with NO, generating cytotoxic
peroxynitrite (OONO-), thereby reducing the efficacy of the potent endothelium-derived
vasodilator system that participates in the homeostatic regulation of the vasculature [50,51].
Pathophysiologially peroxynitrite after reacting with tyrosyl residue of proteins inactivates SOD
which further leads to increased level of superoxide. Moreover superoxide and peroxynitrite
combinely play a major role in the apoptosis of the endothelium causes reduction in the
availability of NO. This reduced NO concentration promotes the adhesion of neutrophils to
platelets as well as endothelium by the expression of co-adhesion molecules. Peroxynitrite also
act as a driving force for more adhesion of platelets and neutrophils which causes release of
vasoconstricting substances such as serotonin and thromboxane A2 and vasculopathic erectile
dysfunction [52]. It was reported that antioxidants mainly alpha tocopherol and melatonin
improved the DM induced sexual impairment in male rats [53]. The corpus cavernosa of diabetic
rats and men with ED possess lipid peroxidation quantitatively in a high level along with up
regulation of superoxide anion and reduced antioxidants levels [54]. ROS have also been
implicated in over expression of arginase activity which further causes uncoupling of eNOS by
suppressing L-arginine [55]. This uncoupled eNOS utilizes molecular oxygen to generate
superoxide and increasing ROS formation [56]. In diabetics ROS also causes the overexpression
of Rho kinase which contributes a promising role in ED.

REVIEW ARTICLE Abhijit et.al / IJIPSR / 3 (6), 2015, 663-687
Department of Pharmaceutical Technology ISSN (online) 2347-2154
Available online: www.ijipsr.com June Issue 670
ROLE OF ARGINASE AND NO IN ERECTILE DYSFUNCTION
L-Arginine is a cationic, semi essential amino acid that is necessary precursor for the synthesis of
L-proline, L-orthinine, polyamines and proteins [57,58] L-Arginine requires the arginase enzyme
and it is also a substrate for production of NO through eNOS activation. Arginase catalyzes the
divalent cation dependent hydrolysis of L-Arginine to form orthinine and urea and exists in two
major isoforms: Arginase I and Arginase II [59,60]. Arginase I, a cytosolic enzyme abundantly
expressed in the liver which control the majority of total body arginase activity but arginase II is a
mitochondrial protein mainly expressed in wide variety of tissue, mostly expressed in the kidney
and prostrate and poorly expressed in the liver [61,62]. L-Arginine acts as a common substrate
which induces competition between arginase and eNOS [63]. In DM increased arginase activity
lead to eNOS dysfunction [64]. Experimentally it had been showed that vascular arginase activity
was increased in diabetic rats and TNF acts as a mediator to promote arginase activity [64,65]. In
diabetic patients, increased arginase expression in the penis reduces the availability of L-arginine
as substrate which further decreases the coupling of NOS and causes less release of NO. The
decreased bioavailability of NO contributes to vasculopathic erectile dysfunction. Studies have
demonstrated that animals with chemically induced and genetic diabetes have significant
decreases in penile eNOS and nNOS protein/gene expression and cavernosal cGMP levels which
is responsible for impaired mating behavior [66,67,68,69,70,71]. Interestingly, endothelium-
independent cavernosal smooth muscle relaxation is also impaired in animal models of diabetes
which suggests that diabetes attenuates endothelial and neurogenic- NO neurotransmission but
may also affect smooth muscle reactivity and the downstream second messengers like soluble
guanylate cyclase, cGMP, or protein kinase cGKI [72]. Impairment in NO biosynthesis can be
potentiated by the fact that long-term oral administration of L-arginine to rabbits with diabetes
increased endothelium-dependent corporal smooth muscle relaxation by increasing the
availability of substrate L-arginine for conversion to L-citrulline and NO. In the presence of
ABH, an arginase inhibitor, the calcium-dependent conversion of L-arginine to L-citrulline was
increased significantly in diabetic cavernosal tissue. These data may suggest that the elevated
arginase expression/activity reduces eNOS activity by competing the eNOS for L-arginine, and
that inhibition of arginase by ABH shifts the availability of L-arginine to eNOS, thus resulting in
increased conversion of the substrate to NO. It has been shown in the rats that sodium nitrite
(NaNO2) administered intra-cutaneously increases ICP and decreases systemic arterial pressure.
REVIEW ARTICLE Abhijit et.al / IJIPSR / 3 (6), 2015, 663-687
Department of Pharmaceutical Technology ISSN (online) 2347-2154
Available online: www.ijipsr.com June Issue 671
The ability of nitrite to enhance erectile activity suggests further investigation in the use of nitrite
as a therapeutic agent for ED.
ROLE OF RHO KINASE
Flaccidity of penis is due to contraction of cavernosal smooth muscles [73]. Contraction of
cavernosal smooth muscle is primarily mediated by the Ca21- dependent activation of MLC
kinase, resulting in the phosphorylation of MLC, and subsequent actin/myosin cross-bridge
formation. In addition, recent evidence has established the important role of myosin phosphatase
in regulating the MLC mediated smooth muscle contraction. Myosin phosphatase by
phosphorylating MLCK prevents the phosphorylation of MLC and thereby contributes to smooth
muscle relaxation. A principle regulator of MLC phosphatase activity is the serine/threonine
kinase, Rho-kinase. Although the role of RhoA/Rho-kinase has been well outlined in numerous
forms of smooth muscle, recent evidence has demonstrated its importance in the regulation of
cavernosal smooth muscle tone [74,75,76,77]. Rho kinase by phosphorylating inactivates myosin
phosphatase and thereby causes smooth muscle contraction. In diabetic patients upregulation of
Rho Kinase causes more inactivation of myosin phosphatase and leads to more contraction of
cavernosal muscles and erectile dysfunction. In diabetic patients RhoA activation also leads to
increased arginase activity. Under physiological conditions NO by inhibiting Rho Kinase causes
MLCK phosphorylation and smooth muscle relaxation. However in diabetic patients decrease in
the level of NO is not able to regulate the activity of Rho kinase and therefore leads to muscle
contraction. It was proposed that NO can inhibit the RhoA/ Rho-kinase pathway in the normal
physiology of erectile response [78,79,80].
Rats with STZ-induced diabetes also have an
increased level of RhoA and Rho-kinase in diabetic corpus cavernosum at a time when eNOS
protein and activity is reduced [81]. Role of Rho-kinase in the maintenance of cavernosal smooth
muscle vasoconstriction has been supported by the evidence that administration of the Rho kinase
inhibitor, Y-27632, directly into the cavernosal sinuses of rats caused dose-dependent increase in
intracavernosal pressure [74]. Y-27632, a Rho kinase inhibitor when given intracutaneously
along with pretreatment with NOS inhibitors (L-NMA and L-NAME) or sGC inhibitor
(Methylene blue) in rats resulted in increased erectile activity due to nerve stimulation,
independent of NO [82]. Bivalacqua et al found that erectile activity, cGMP levels, constitutive
NOS activity and cavernosal eNOS protein were restored to normal level when the diabetic
animals were transfected with a dominant negative RhoA mutant [83]. Fasudil, a Rho kinase
inhibitor after chronic administration was shown to treat vasculogenic erectile dysfunction [84]. A

REVIEW ARTICLE Abhijit et.al / IJIPSR / 3 (6), 2015, 663-687
Department of Pharmaceutical Technology ISSN (online) 2347-2154
Available online: www.ijipsr.com June Issue 672
most recent study concluded that diabetes associated erectile dysfunction enhances Akt activity
due to upregulation of RhoA/ Rho-kinase pathway, which directly leads to apoptosis of
cavernosal tissue [85]. In a study of diabetes induced erectile dysfunction by streptozotocin or
alloxan in rats and rabbits, Rho kinase inhibitor SAR407899 was found to cause relaxation of
corpora cavernosa invivo [86].
ROLE OF PROTEIN KINASE C AND TNF-ALPHA
Protein kinase C is an enzyme mainly activated by high glucose concentration and high TNF [87].
DM causes de novo synthesis of diacylglycerol which leads to the PKC activation [88]. Diabetes
induced translocation of PKC-alpha to renal membrane was associated with increased
nicotinamide adenine dinucleotide phosphate oxidase-dependent superoxide generation and
kidney damage [89]. Of the various isoforms PKC in vascular cells, it is found by immunoblotting
studies that the PKC β and δ isoforms in the aorta and heart of diabetic rats get activated on
exposure to high glucose [90,91]. Hyperglycemia in DM generates Tumor Necrosis Factor (TNF)
and then the cytokine upregulates the endothelial arginase activity [92,93]. TNF binds to different
receptors TNF-R1 (soluble TNF has the highest affinity) and TNF-R2 (Membrane bound TNF has
the highest affinity) [94,95]. Except TNF-R2, TNF-R1 consists of death domain which gets
activated during apoptosis signal [96]. TNF-R2 though not carry death domain is involved in
regulation of apoptosis in micro vascular endothelial cells [97]. Up regulation of TNF in diabetics
decreases eNOS expression and thus affect NO production [98]. It also promotes ROS production
in endothelial cells through NADPH oxidase and uncoupled NOS [99,100,101]. Moreover, PKC
activation leads to TNF mediated increase in permeability of endothelial monolayers and
endothelial dysfunctions [102]. TNF-α levels are increased in serum of patients with moderate to
severe ED [103,104,105] and
TNF-α is inversely associated with sexual performance [103].
Experimental studies have demonstrated that TNF-α knockout mouse exhibited changes in
cavernosal reactivity that would facilitate erectile responses, decreased responses to adrenergic
nerve stimulation and increased NANC and endothelium-dependent relaxation that are associated
with increased corporal eNOS and nNOS protein levels [106]. The penile smooth muscle cells
synthesizes endothelin-1 (ET-1), its converting enzyme (ECE-1), and both ETA and ETB receptor
subtypes [107,108,109]. ET-1 induces vasoconstriction and also stimulates the expression of
adhesion molecules and activates transcriptional factors responsible for the coordinated increase
in the expression of many cytokines and enzymes, which can in turn lead to the production of
inflammatory mediators [110,111]. Angiotensin II, ET-1 and other inflammatory mediators have
REVIEW ARTICLE Abhijit et.al / IJIPSR / 3 (6), 2015, 663-687
Department of Pharmaceutical Technology ISSN (online) 2347-2154
Available online: www.ijipsr.com June Issue 673
been shown to increase TNF-α levels [112,113,114,115]. However further studies are essential to
determine whether TNF-α plays a detrimental role in ED associated with CVD such as
hypertension, diabetes, CAD, and heart failure. Finally, a key role for TNF-α in mediating smooth
muscle and endothelial dysfunction is of interest not only because markedly elevated serum levels
of TNF-α have been documented in patients with ED, but also because we now have access to
targeted anti-TNF-α therapies.
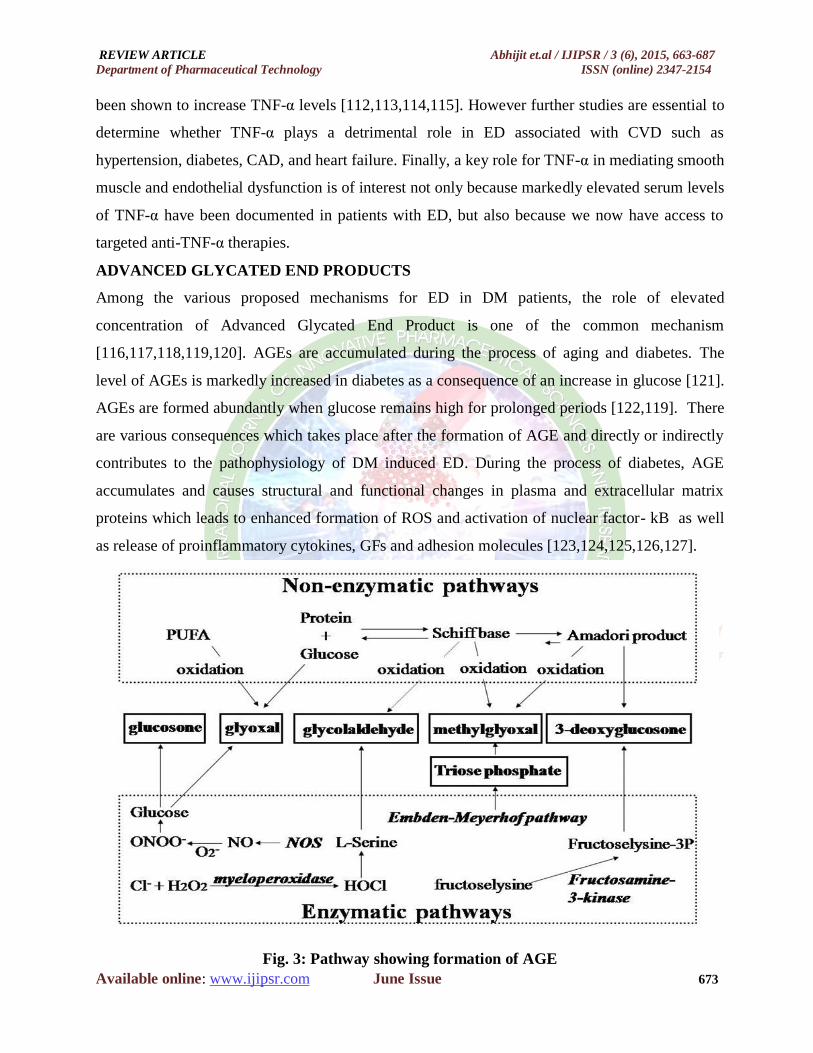
ADVANCED GLYCATED END PRODUCTS
Among the various proposed mechanisms for ED in DM patients, the role of elevated
concentration of Advanced Glycated End Product is one of the common mechanism
[116,117,118,119,120]. AGEs are accumulated during the process of aging and diabetes. The
level of AGEs is markedly increased in diabetes as a consequence of an increase in glucose [121].
AGEs are formed abundantly when glucose remains high for prolonged periods [122,119]. There
are various consequences which takes place after the formation of AGE and directly or indirectly
contributes to the pathophysiology of DM induced ED. During the process of diabetes, AGE
accumulates and causes structural and functional changes in plasma and extracellular matrix
proteins which leads to enhanced formation of ROS and activation of nuclear factor- kB as well
as release of proinflammatory cytokines, GFs and adhesion molecules [123,124,125,126,127].
Fig. 3: Pathway showing formation of AGE

REVIEW ARTICLE Abhijit et.al / IJIPSR / 3 (6), 2015, 663-687
Department of Pharmaceutical Technology ISSN (online) 2347-2154
Available online: www.ijipsr.com June Issue 674
In diabetes through the process of glycation, glucose reacts with amino groups producing Schiff
base, which is modified to form more stable amadori products [128]. AGE acts through surface
receptors such as Receptor for AGE (RAGE), 80 kH phosphoprotein (R-2), scavenger receptor II,
lactoferrin like polypeptide and CD-36 [129]. AGE can also form covalent bonds with vascular
collagen which leads to thickening of blood vessels, decreased elasticity, endothelial dysfunction
and atherosclerosis. AGE at the molecular level acts on various channels and receptors in
cavernosal smooth muscle cells especially on k+ channel which help in the release of intracellular
Ca++
ion and cause cavernosal smooth muscle relaxation. AGE damages this physiology of K+ ion
channel and thus disrupting the relaxation capacity of cavernosal smooth muscle and leads to
early onset of DM induced ED [130]. AGE also increases the expression of major
vasoconstrictors such as ET1 and VEGF [131]. Along with AGE, receptor for advanced glycated
end product (RAGE) also contribute the overexpression of ET1 in the cavernosal tissue [132]. It
has been proposed that AGEs through the generation of ROS and cell damage decrease the level
of cGMP which affect the smooth muscle relaxation [133,134]. AGEs accumulate in endothelial
and smooth muscle cells and cause sustained cellular activation of various proteins and generation
of oxygen- derived free radicals. It is now proposed that AGE inhibitors can repair the
vasoconstrictory mechanism of cavernosal smooth muscle by various mechanisms as depicted
possibly in fig 2. Aminoguanidine, a novel inhibitor of AGE formation and ALT-711, a
compound that breaks down AGE, has been demonstrated to play a major role in treating DM
induced ED and observed that there is a major improvement in the endothelium-dependent
cavernosal smooth muscle relaxation in vitro and erectile responses in vivo [132,134].
Additionally, aminoguanidine also prevent diabetes-induced changes in the connective tissue
composition of the microvascular wall of the arterioles supplying the penis, thus improving
arterial inflow to the penis. Taken together, the deleterious effects of AGEs seem to be involved
in the pathogenesis of endothelial dysfunction as it relates to diabetes.
CONCLUSION
Normal penile erection is dependent on the integrity of the endothelium. Endothelial-derived NO
plays an important role in the physiological mechanism of erection. Alteration in the
concentration of NO due to damage to endothelium or due to increased destruction appears to be
the most important causes for ED. Diabetes Mellitus is a most important risk for the development
of erectile dysfunction. A major factor contributing to diabetic ED in human corporal tissue is a
REVIEW ARTICLE Abhijit et.al / IJIPSR / 3 (6), 2015, 663-687
Department of Pharmaceutical Technology ISSN (online) 2347-2154
Available online: www.ijipsr.com June Issue 675
reduction in the number of nitrergic NOS containing nerve fibers, constitutive NOS activity, and
impaired endothelial and neurogenic mediated smooth muscle relaxation. The detectable changes
in diabetes associated with ED are endothelial abnormality which causes loss of the normal
homeostatic mechanisms. Hyperglycemia in diabetes collectively induces endothelial
dysfunction, oxidative stress, disturbance in NANC pathway, formation of advanced glycated end
products, over expression of arginase enzyme and TNF-alpha, activation of protein kinase C and
endothelin1 which ultimately leads to ED as consequence. Various animal and human
experimental data have demonstrated that diabetic vasculopathy and neuropathy contribute
significantly to diabetes-associated ED. Impairments in endothelium-dependent and NANC-
mediated cavernosal smooth muscle relaxation are well established in diabetic corpus cavernosum
in vitro and in vivo. Recent evidence suggests that oxidative stress may play a major role in
diabetic endothelial dysfunction of the penile vascular bed. Studies on the use of a Rho Kinase
inhibitor for treatment of STZ induced ED also indicate the involvement of Rho Kinase in
diabetic erectile dysfunction. The correlation among these molecules has revealed the most
possible mechanism underlying diabetes induced ED. Discovery of the pathophysiological
mechanisms involved in disease associated ED will undoubtedly lead to prevention strategies and
new therapies for ED. Still researches are going on investigating the proper treatment targeting
these molecules which may lead to novel strategies for curing ED in the future.
REFERENCES
1. K. Kohei, “Pathophysiology of type II diabetes and its treatment policy,” Japanese Medical
Association Journal, vol. 53, no. 1, pp. 41-46, 2010.
2. R. Lucas, R. Caldwell, and G. Yang, “Novel mechanisms of endothelial dysfunction in
diabetes.” Journal of Cardiovascular Disease Research, vol. 1, no. 2, pp. 117-119, 2010.
3. P.J. Grant, “Diabetes Mellitus as a prothrombotic condition”. Journal of Internal Medicine,
vol. 262, no. 2, pp. 152-157, 2007.
4. D.D. Eulises, “Erectile dysfunction: A chronic complication of diabetes mellitus”.
Complementary and Alternative Medicine, pp. 69-78, 2012.
5. R. Klein, B.E. Klein, K.E. Lee, S.E. Moss, and K.J. Cruickshanks, “Prevalence of self
reported erectile dysfunction in people with long term IDDM”. Diabetes care, vol. 19, no. 2,
pp. 135-141, 1996.

REVIEW ARTICLE Abhijit et.al / IJIPSR / 3 (6), 2015, 663-687
Department of Pharmaceutical Technology ISSN (online) 2347-2154
Available online: www.ijipsr.com June Issue 676
6. D. Fedele, C. Coscelli, D. Cucinotta, G. Forti, F. Santeusanio et al., “Incidence of erectile
dysfunction in Italian men with diabetes”. Journal of Urology, vol. 166, no. 4, pp. 1368-1371,
2001.
7. D.K. McCulloch, I.W. Campbell, F.C. Wu, R.J. Prescott, and B.F. Clarke, “The prevalence of
diabetic impotence”. Diabetologia, vol.18, no. 4, pp. 279-283, 1980.
8. A. Roth, O. Kalter-Leibovici, Y. Kerbis, J. Chen, T. Sobol et al., “Prevalence and risk factors
for erectile dysfunction in men with diabetes, hypertension or both diseases: a community
survey among 1,412 Israeli men”. Clinical Cardiology, vol. 26, no. 1, pp. 25-30, 2003.
9. K.P. Kleinman, H.A. Feldman, C.B. Johannes, C.A. Derby, and J.B. McKinlay, “A new
surrogate variable for erectile dysfunction status in the Massachusetts male aging study”.
Journal of Clinical Epidemiology, vol. 53, no. 1, pp. 71-78, 2000.
10. J.H. Romeo, A.D. Seftel, Z.T. Madhun, and D.C. Aron, “Sexual function in men with diabetes
type 2: association with glycemic control”. Journal of Urology, vol. 163, no. 3, pp. 788-791,
2000.
11. R. Leite, “Targets for the treatment of erectile dysfunction is NO/c GMP still the answer?”
Recent Patents on Cardiovascular Drug Discovery, vol. 2, no. 2, pp. 119-132, 2007.
12. B.L. Meena, D.K. Kochar, T.D. Aggarwal, R. Chaudhary, and A. Kochar, “Association
between erectile dysfunction and cardiovascular risk in individuals with type 2 diabetes
without overt cardiovascular disease”. International Journal of Diabetes in Developing
Countries, vol. 29, no. 4, pp. 150-154, 2009.
13. NIH Consensus Conference. Impotence. The Journal of the American Medical Association,
vol. 270, no. 1, pp. 83-90, 1993.
14. I. Eardley, “Pathophisiology of erectile dysfunction”. The British Journal of Diabetes and
Vascular Disease, vol. 2, no. 4, pp. 272-276, 2002.
15. R. Maas, E. Schwedhelm, J. Albsmeier, and B.H. Boger, “The pathophysiology of erectile
dysfunction related to endothelial dysfunction and mediators of vascular functions”. Vascular
Medicine, vol. 7, no. 3, pp. 213-225, 2002.
16. Z. Colakoglu, E. Kutluay, C. Ertekin, B. Altay, R. Killi et al., “Autonomic nerve involvement
and venous leakage in diabetic men with impotence”. International Journal of Urology, vol.
83, no. 4, pp. 453-456, 1999.
17. M.A. Potenza, S. Gagliardis, and C. Nacci, “Endothelial dysfunction in diabetes: from
mechanism to therapeutics targets”. Current Medical Chemistry, vol. 16, pp. 94-112, 2009.

REVIEW ARTICLE Abhijit et.al / IJIPSR / 3 (6), 2015, 663-687
Department of Pharmaceutical Technology ISSN (online) 2347-2154
Available online: www.ijipsr.com June Issue 677
18. J.E. Deanfield, J.P. Halcox, and T.J. Rabelink, “Endothelial function and dysfunction: testing
and clinical relevance”. Circulation, vol. 115, pp. 1285-1295, 2007.
19. S. Jesmin, I. Sakuma, and K. Nonomura, “Diminished penile expression of vascular
endothelial growth factor and its receptor at the insulin-resistant stage of a type II diabetic rat
model: a possible cause of erectile dysfunction in diabetes”. Journal of Molecular
Endocrinology, vol. 31, no. 3, pp. 401-418, 2003.
20. C.G. Schalkwijk, and C.D. Stehouwer, “Vascular complications in diabetes mellitus: the role
of endothelial dysfunction”. Clinical Science London, vol. 109, no. 2, pp. 143-59, 2005.
21. S. Rahbar, and J.L. Figarola, “Novel inhibitors of advanced glycated end products. Archives
of Biochemistry & Biophysics, vol. 419, no. 1, pp. 63-79, 2003.
22. J.S. Beckman, and W.H. Koppenol, “Nitric oxide, superoxide and peroxynitrite: the good, the
bad, and ugly”. American Journal of Physiology, vol. 271, pp. 1424-1437, 1996.
23. J.Y. Jeremy, G.D. Angelini, M. Khan, D.P. Mikhailidis, and C.S. Thopson, “Platelets, oxidant
stress and erectile dysfunction, an hypothesis”. Cardiovascular Research, vol. 46, no. 1, pp.
50-54, 2000.
24. A.S. De Vreise, T.J. Verbeuren, J. Van de Voorde, N.H. Lameire, and P.M. Vanhoutte,
“Endothelial dysfunction in diabetes”. British Journal of Pharmacology, vol. 130, no. 5, pp.
963-974, 2000.
25. F. Fiordaliso, I. Cuccovillo, R. Bianchi, A. Bai, M. Doni, and M. Salio, “Cardiovascular
oxidative stressis reduced by an ACE inhibitor in a rat model of streptozotocin induced
diabetes”. Life Science, vol. 79, pp. 121-129, 2006.
26. H.E. Tawfik, A.B. Remessy, S. Matragoon, G. Ma, R.B. Caldwell, and R.W. Caldwell,
“Simvastatin improves diabetes induced coronary endothelial dysfunction. Journal of
Pharmacology and Experimental Therapeutics, vol. 319, no. 1, pp. 386-395, 2006.
27. A. Ceriello, “Oxidative stress and diabetes associated complications”. Endocrine Practice, vol.
12, no. 1, pp. 60-62, 2006.
28. Z.T. Bloomgarden, “American Diabetes Association Annual Meeting. Endothelial
dysfunction, neuropathy and the diabetic foot, diabetic mastopathy, and erectile dysfunction”.
Diabetes Care, vol. 21, pp. 83-89, 1998.
29. R.B. Moreland, G. Hsieh, M. Nakane, and J.D. Brioni, “The biochemical and neurologic basis
for the treatment of male erectile dysfunction”. Journal of Pharmacology and Experimental
Therapeutics, vol. 296, no. 2, pp. 225-234, 2001.

REVIEW ARTICLE Abhijit et.al / IJIPSR / 3 (6), 2015, 663-687
Department of Pharmaceutical Technology ISSN (online) 2347-2154
Available online: www.ijipsr.com June Issue 678
30. S.K. Agarwal, A. Prakash, and N.P. Singh, “Erectile dysfunction in diabetes mellitus: Novel
treatments”. International Journal of Diabetes in Developing Countries, vol. 23, pp. 94-98,
2003.
31. K.J. Hurt, B. Musicki, M.A. Palese, J.K. Crone, R.E. Becker, J.L. Moriarity, S.H. Snyder, and
A.L. Burnett, “Akt-dependent phosphorylation of endothelial nitric-oxide synthase mediates
penile erection”. Proceedings of the National Academy of Sciences of the United State of
America, vol. 99, no. 6, pp. 4061-4066, 2002.
32. B.J. Michell, J.E. Griffiths, and K.I. Mitchelhill et al., “The Akt kinase signals directly to
endothelial nitric oxide synthase”. Current Biology, vol. 9, no. 15, pp. 845-848, 1999.
33. K. Paskaloglu, G. Sener, and G. Ayanoglu-Dulger, “Melatonin treatment protects against
diabetes –induced functional and biochemical changes in rat aorta and corpus cavernosum”.
European Journal of Pharmacology, vol. 499, pp. 345-354.
34. T.J. Bivalacqua, M.F. Usta, M. Kendirci, L. Pradhan, X. Alvarez, H.C. Champion, P.J.
Kadowitz, and W.J. Hellstrom, “Superoxide anion production in the rat penis impairs erectile
function in diabetes: influence of in vivo extracellular superoxide dismutase gene therapy”.
The Journal of Sexual Medicine, vol. 2, no. 2, pp. 187-197, 2005.
35. H. Tsubouchi, T. Inoguchi, T. Sato, N. Sato et al., “Statin attenuates high glucose induced and
diabetes induced oxidative stress in vitro and in vivo evaluated by electron spin resonance
measurement”. Free Radical Biology and Medicine, vol. 39, no. 4, pp. 444-452, 2005.
36. S. Kimura, G.X. Zhang, T. Shokoji, I. Yao, Y.Y. Fan et al., “Role of NAD(P)H oxidase and
mitochondria derived reactive oxygen species in cardioprotection of ischemic reperfusion
injury by angiotensin II”. Hypertension, vol. 45, pp. 860-866.
37. K.E. Andersson, “Neurophysiology/pharmacology of erection”. International Journal of
Impotence Research, vol. 13(suppl 3), pp. S8-S17, 2001.
38. T.M. Mills, K. Chitaley, R.W. Lewis, and R.C. Webb, “Nitric oxide inhibits RhoA/ Rho-
kinase signaling to cause penile erection”. European Journal of Pharmacology, vol. 439, no. 1,
pp. 173-174, 2002.
39. B. Barbul, “Arginine: biochemistry, physiology, and therapeutic implications”. Journal of
Parenteral and Enteral Nutrition, vol. 10, pp. 227-238, 1986.
40. G. Wu, and S.M. Morris, “Arginine metabolism: NO and beyond”. Biochemical Journal, vol.
336, no. 1, pp. 1-17, 1998.
REVIEW ARTICLE Abhijit et.al / IJIPSR / 3 (6), 2015, 663-687
Department of Pharmaceutical Technology ISSN (online) 2347-2154
Available online: www.ijipsr.com June Issue 679
41. E. David, “Arginine metabolism: Enzymology, Nutrition and Clinical Significance”.
American Society of Nutritional Science, 2004.
42. W. Zhang, B. Baban, M. Rojas, S. Tofigh, C. Patel et al., “Arginase activity mediates retinal
inflammation in endotoxin induced uveitis”. American Journal of Pathology, vol. 175, pp.
891-902, 2009.
43. J.G. Vockley, C.P. Jenkinson, H. Shukla, and R.M. Kern, “Cloning and characterization of
human type II human arginase gene”. Genomics, vol. 38, no. 2, pp. 118-123, 1996.
44. J.J. Cartledge, I. Eardley, and J.F. Morrison, “Impairment of corpus cavernosal smooth
muscle relaxation by glycosylated human haemoglobin”. British Journal of Urology
International, vol. 85, no. 6, pp. 735-741, 2000.
45. S.M. Morris, and D. Bhamidipati, “Human type II arginase: sequence analysis and tissue
specific expression”. Gene, vol. 193, no. 2, pp. 157-161, 1997.
46. A. Ceriello, “New insights on oxidative stress and diabetic complications may lead to a
„causal‟ antioxidant therapy”. Diabetes Care, vol. 26, no. 5, pp. 1589-1596, 2003.
47. M.M. Spitaler, and W.F. Graier, “Vascular targets of redox signaling in diabetes mellitus”.
Diabetologia, vol. 45, pp. 476-494, 2002.
48. F.G. Soriano, L. Virag, P. Jagtap, E. Szabo, J.G. Mabley, and L. Liaudet, “Diabetic
endothelial dysfunction: the role of poly (ADP-ribose) polymerase activation”. Nature
Medicine, vol. 7, pp. 108-113, 2001.
49. M.F. Usta, T.J. Bivalacqua, D.Y. Yang, A. Ramanitharan, D.R. Sell, and A. Viswanathan et
al., “The protective effect of aminoguanidine on erectile function in streptozotocin diabetic
rats”. Journal of Urology, vol. 170, no. 4, pp. 1437-1442, 2003.
50. A.R. White, S. Ryoo, H.C. Champion, J. Steppan, D. Wang et al., “Knockdown of arginase I
restores NO signaling in the vasculature of old rats”. Hypertension, vol. 47, no. 2, pp. 245-
251, 2006.
51. M.J. Romero, and R.B. Caldwell, “Does elevated arginase activity contributes to diabetes-
induced endothelial dysfunction”. Federation of American Societies for Experimental
Biology, vol. 20, pp. 1125-1129, 2006.
52. M.J. Romero, D.H. Platt, H.E. Tawfik, and M. Bartoli, “Diabetes induced coronary vascular
dysfunction involves increased arginase activity”. Circulation Research, vol. 102, pp. 95-102,
2008.
REVIEW ARTICLE Abhijit et.al / IJIPSR / 3 (6), 2015, 663-687
Department of Pharmaceutical Technology ISSN (online) 2347-2154
Available online: www.ijipsr.com June Issue 680
53. X. Gao, X. Xu, S. Belmandi, Y. Park, Z. Tang et al., “TNF alpha Contributes to the
endothelial dysfunction by upregulating arginase in ischaemia/ reperfusion injury”.
Arteriosclerosis, Thrombosis and Vascular Biology, vol. 27, pp. 1269- 1275, 2007.
54. K.E. Andersson, and G. Wagner, “Physiology of penile erection”. Physiological Reviews, vol.
75, no. 1, pp. 191-236, 1995.
55. M.P. Walsh, “The Ayerst Award Lecture 1990. Calcium dependent mechanisms of regulation
of smooth muscle contraction”. Biochemistry and Cell Biology, vol. 69, pp. 771-800, 1991.
56. A.P. Somlyo, and A.V. Somlyo, “Signal transduction by G-proteins, Rho-kinase and protein
phosphatase to smooth muscle and non-muscle myosin II”. Journal of Physiology, vol. 522,
no. 2, pp. 177-185, 2000.
57. R.W. Rees, T. Zeissen, D.J. Ralph, P. Kell, S. Moneada et al., “Human and rabbit cavernosal
smooth muscle cells express Rho-kinase”. International Journal of Impotence Research, vol.
14, no. 1, pp. 1-7, 2002.
58. H. Wang, M. Eto, W.D. Steers, A.P. Somlyo, and A.V. Somlyo, “RhoA mediated Ca2+
sensitization in erectile function”. The Journal of Biological Chemistry, vol. 277, no. 34, pp.
14-21, 2002.
59. K. Chitaley, R.C. Webb, T.M. Mills et al., “RhoA/Rhokinase: a novel player in the regulation
of penile erection”. International Journal of Impotence Research, vol. 13, pp. 67-72, 2001.
60. T.M. Mills, K. Chitaley, R.W. Lewis, and R.C. Webb, “Nitric oxide inhibits RhoA/Rho-
kinase signaling to cause penile erection”. European Journal of Pharmacology, vol. 439, no.1 ,
pp. 173-174, 2002.
61. K. Chitaley, C.J. Wingard, R. Clinton et al., “Antagonism of Rho-kinase stimulates rat penile
erection via a nitric oxide-independent pathway”. Nature Medicine, vol. 7, no. 1, pp. 119-122,
2001.
62. T.G. Bivalacqua, T.C. Champion, M.F. Usta et al., “RhoA/Rho-kinase suppresses endothelial
nitric oxide synthase in the penis: a mechanism for diabetes-associated erectile dysfunction”.
Proceedings of the National Academy of Sciences of the United States of America, vol. 101,
no. 24, pp. 9121-9126, 2004.
63. K. Park, S.W. Kim, S.W. Rhu, and J.S. Paick, “Chronic administration of an oral Rho Kinase
inhibitor prevents the development of vasculogenic erectile dysfunction in a rat model”. The
Journal of Sexual Medicine, vol. 3, no. 6, pp. 996-1003, 2006.
REVIEW ARTICLE Abhijit et.al / IJIPSR / 3 (6), 2015, 663-687
Department of Pharmaceutical Technology ISSN (online) 2347-2154
Available online: www.ijipsr.com June Issue 681
64. W.J. Li, K. Park, J.S. Paick, and S.W. Kim, “Chronic treatment with an oral Rho-kinase
inhibitor restores erectile function by suppressing corporal apoptosis in diabetic rats”. The
Journal of Sexual Medicine, vol. 8, no. 2, pp. 400-410, 2011.
65. M. Uehata, T. Ishizaki, H. Satoh, J. Ono, T. Kawahara et al., “Calcium sensitization of smooth
muscle mediated by a Rho-associated protein kinase in hypertension”. Nature, vol. 389, pp.
990-994, 1997.
66. G. Ari, Y. Vardi, and J.P. Finberg, “Nitric oxide and penile erection in streptozotocin-diabetic
rats”. Clinical Science London, vol. 96, pp. 365-371, 1999.
67. A.I. El-Sakka, C.S. Lin, R.M. Chui, R. Dahiya, and T.F. Lue, “Effects of diabetes on nitric
oxide synthase and growth factor genes and protein expression in an animal model”.
International Journal of Impotence Research, vol. 11, no. 3, pp. 123-132, 1999.
68. A.G. Akingba, and A.L. Burnett, “Endothelial nitric oxide synthase protein expression,
localization, and activity in the penis of the alloxan-induced diabetic rat”. Molecular Urology,
vol. 5, no. 4, pp. 189-197, 2001.
69. C.S. Thompson, F.H. Mumtaz, M.A. Khan, R.M. Wallis, D.P. Mikhailidis, R.J. Morgan, G.D.
Angelini, and J.Y. Jeremy, “The effect of sildenafil on corpus cavernosal smooth muscle
relaxation and cyclic GMP formation in the diabetic rabbit”. European Journal of
Pharmacology, vol. 425, no. 1, pp. 57-64, 2001.
70. A. Escrig, R. Marin, P. Abreu, J.L. Gonzalez-Mora, and M. Mas, “Changes in mating
behavior, erectile function, and nitric oxide levels in penile corpora cavernosa in
streptozotocin-diabetic rats”. Biology of Reproduction, vol. 66, no. 1, pp. 185-189, 2002.
71. T.J. Bivalacqua, M.F. Usta, H.C. Champion, D. Adams, D.B. Namara, A.B. Abdel- Mageed,
P.J. Kadowitz, and W.J. Hellstrom, “Gene transfer of endothelial nitric oxide synthase
partially restores nitric oxide synthesis and erectile function in streptozotocin diabetic rats”.
Journal of Urology, vol. 169, no. 5, pp. 1911-1917, 2003.
72. K.J Way, and J.J. Reid, “The effects of diabetes on nitric oxide-mediated responses in rat
corpus cavernosum”. European Journal of Pharmacology, vol. 376, no. 1, pp.73-82, 1999.
73. A.P. Somlyo, and A.V. Somlyo, “Signal transducing by G-proteins, Rho-kinase and protein
phosphatase to smooth muscle and non muscle myosin II”. Journal of Physiology, vol. 522,
no. 2, pp. 177-185, 2000..

REVIEW ARTICLE Abhijit et.al / IJIPSR / 3 (6), 2015, 663-687
Department of Pharmaceutical Technology ISSN (online) 2347-2154
Available online: www.ijipsr.com June Issue 682
74. K. Chitaley, C.J. Wingard, R.W. Clinton, H. Branam, V.S. Stopper, R.W. Lewis, and T.M.
Mills, “Antagonism of Rho-kinase stimulates rat penile erection via a nitric oxide-independent
pathway”. Nature Medicine, vol. 7, no. 1, pp. 119-122, 2001.
75. K. Chitaley, R.C. Webb, and T.M. Mills, “The ups and downs of Rho-kinase and penile
erection: upstream regulators and downstream substrates of rho-kinase and their potential role
in the erectile response”. International Journal of Impotence Research, vol. 15, pp. 105-109,
2003.
76. T.M. Mills, K. Chitaley, and R.W. Lewis, “Vasoconstrictors in erectile physiology”.
International Journal of Impotence Research, vol. 13, no. 5, pp. 29-34, 2001.
77. R.W. Rees, D.J. Ralph, M. Royle, S. Moncada, and S. Cellek S, “Y-27632, an inhibitor of
Rho-kinase, antagonizes noradrenergic contractions in the rabbit and human penile corpus
cavernosum”. British Journal of Pharmacology, vol. 133, no. 4, pp. 455-458, 2001.
78. F. Guagnini, M. Ferazzini, M. Grasso, S. Blanco, and T. Croci, “Erectile properties of the
Rho-kinase inhibitor SAR407899 in diabetic animals and human isolated corpora cavernosa”.
Journal of Translational Medicine, vol. 10, pp. 1-11, 2012.
79. M.B. Ganz, and A. Seftel, “Glucose induced changes in protein kinase C and nitric oxide are
prevented by Vit E”. American Journal of Preventive Medicine, vol. 278, pp. 146-152, 2000.
80. X.F. Ming, H. Viswambharan, C. Barandier, J. Ruffieux, K. Kaibuchi, S. Rusconi, and Z.
Yang, “Rho GTPase/Rho kinase negatively regulates endothelial nitric oxide synthase
phosphorylation through the inhibition of protein kinase B/Akt in human endothelial cells”.
Molecular and Cellular Biology, vol. 22, no. 24, pp. 8467-8477, 2002.
81. T.J Bivalacqua, M.F. Usta, K. Chitaley, H.C. Champion, R.C. Webb, R.W. Lewis, T.M. Mills,
and W. Hellstrom, “Adeno-associated viral gene transfer of dominant negative RhoA
improves erectile function in streptozotocin diabetic rats [abstract]”. Journal of Urology, vol.
169, pp. 1198, 2003.
82. P.A. Craven, R.K. Studer, and H. Negrete, “Protein kinase C in diabetic nephropathy”.
Journal of Diabetes and Its Complications, vol. 9, no. 4, pp. 241-245, 1995.
83. T. Bonke, S.R. Thorpe, M.T. Coughlan, K. Fukami, F.Y. Yap et al., “Inhibition of NADPH
oxidase prevents AGE product mediated damage in diabetic nephropathy through a protein
kinase C alpha dependent pathway”. Diabetes, vol. 57, no. 2, pp. 460-469, 2008.

REVIEW ARTICLE Abhijit et.al / IJIPSR / 3 (6), 2015, 663-687
Department of Pharmaceutical Technology ISSN (online) 2347-2154
Available online: www.ijipsr.com June Issue 683
84. T. Shiba, T. Ionguchi, J.R. Sportsman, W. Health, S. Bursella et al., “Correlation of
diacylglycerol and PKC activity in rat retina circulation”. American Journal of Physiology,
vol. 235, no. 5, pp. 783-793, 1993.
85. T. Inoguchi, R. Battan, E. Handler, J.R. Sportsman, W. Health et al., “Preferential elevation of
protein kinase C isoform and diacylglycerol levels in the aorta and heart of diabetic rats,
differential reversibility to glycemic control by islet cell transplantation”. Proceedings of
National Academy of Sciences United State of America, vol. 89, pp. 11059-11063, 1992.
86. M. Kunisaki, S.E. Bursell, F. Umeda, H. Nawata, and G.L. King, “Normalization of DAG-
Protein kinase C activation by Vit E in aorta of diabetic rats and cultured rat smooth muscle
cells exposed to elevated glucose levels”. Diabetes, vol. 43, no. 11, pp. 1372-1377, 1994.
87. D. Wallach, E.E. Varfolomeer, N.L. Malinin, Y.V. Goltser, A.V. Kovalenko et al., “Tumour
necrosis factor receptor and FAS signaling mechanisms”. Annual Review of Immunology,
vol. 17, pp. 331-367, 1999.
88. M. Grell, H. Wajant, G. Zimmermann, and P. Scheurich, “The type I receptor (CD120a) is the
high affinity receptor and FAS signaling mechanisms”. Annual Review of Immunology, vol.
17, pp. 331-367, 1999.
89. R. Lucas, I. Garica, Y.R. Donati, M. Hribar, S.J. Mandriota et al., “Uromodulin (Tamm-
Horsfall glycoprotein): a renal ligand for lymphokines”. Science, vol. 237, pp. 1479-1484,
1987.
90. K.L Mac Naul, and N.I. Hutchinson, “Differential expression of iNOS and cNOS mRNA in
human vascular smooth muscle cells and endothelial cells under normal and inflammatory
conditions”. Biochemical and Biophysical Research Communications, vol. 196, no. 3, pp.
1330-1334, 1993.
91. D. Sorescu, and K.K. Griendling, “ROS, mitochondria, amd NADPH oxidases in the
development and progression of heart failure”. Congestive Heart Failure, vol. 8, no. 3, pp.
132-140, 2002.
92. J.M. Downey, B. Omar, and H. Ooiwa, “SOD therapy for myocardial ischemia”. Free Radical
Research Communications, vol. 12, pp. 703-720, 1991.
93. K.A. Pritchard, L. Groszek, D.M. Smalley, W.C. Sessa, M. Wu et al., “Native LDL increases
endothelial cell NO synthase generation of superoxide anion”. Circulation Research, vol. 77,
no. 3, pp. 510-518, 1995.

REVIEW ARTICLE Abhijit et.al / IJIPSR / 3 (6), 2015, 663-687
Department of Pharmaceutical Technology ISSN (online) 2347-2154
Available online: www.ijipsr.com June Issue 684
94. T. Ferro, P. Neumann, N. Gertzberg, R. Clements, and A. Johnson, “Protein kinase C alpha
mediates endothelial barrier dysfunction induced by TNF alpha”. American Journal of
Physiology Lung Cellular and Molecular Physiology, vol. 278, pp. 1107-1117, 2000.
95. K. Daisuke, and K. George, “Protein kinase C activation and development of diabetic
complications”. Diabetes, vol. 47, pp. 121-125, 1998.
96. D.B. Jiaan, A.D. Seftel, J. Forarty, N. Hampel, W. Cruz et al., “Age related increase in AGE
in penile tissue”. World Journal of Urology, vol. 13, pp. 369-375, 1995.
97. C.R. Moore, and R. Wang, “Pathophysiology and treatment of diabetic erectile dysfunction”.
Asian Journal of Andrology, vol. 8, no. 6, pp. 675-684, 2006.
98. M.E. Sullivan, M.R. Dashwood, C.S. Thompson, J.R. Muddle, D.P. Mikhailidis et al.,
“Alterations in endothelin B receptor sites in cavernosal tissue of diabetic rabbits: potential
relevance to the pathogenesis of erectile dysfunction”. Journal of Urology, vol. 158, no. 5, pp.
1966-1972, 1997.
99. V.S. Thore, A.D. Kshirsagar, N.S. Vyawahare, V.S. Joshi, K.G. Ingale et al., “Diabetes
induced Erectile dysfunction: epidemiology, pathophysiology and management”. Journal of
Diabetes and Its Complications, vol. 25, pp. 129-136, 2011.
100. L.C. Maillard LC, “Action des acides amines sur les sacres, formation des melanoidines par
voie methodique”. Proceedings of the Academy of Sciences, vol. 154, no. 2, pp. 66-68, 1912.
101. R. Nagai, T. Mori, Y. Yamamoto, Y. Kaji, and Y. Yonei, “Significance of advanced
glycated end products in aging-related disease”. Japanese Society of Anti-aging Medicine,
vol. 7, no. 10, pp. 112-119, 2010.
102. M. Brownlee, A. Cerami, and H. Vlassara, “Advanced glycosylation end products in tissue
and the biochemical basis of diabetic complications”. The New England Journal of Medicine,
vol. 318, no. 20, pp. 1315-1321, 1988.
103. C. Vlachopoulos, K. Aznaouridis, N. Ioakeimidis, K. Rokkas, C. Vasiliadou, N.
Alexopoulos, E. Stefanadi, A. Askitis, and C. Stefanadis, “Unfavourable endothelial and
inflammatory state in erectile dysfunction patients with or without coronary artery disease”.
European Heart Journal, vol. 27, pp. 2640-2648, 2006.
104. C. Vlachopoulos, K. Rokkas, N. Ioakeimidis, and C. Stefanadis, “Inflammation, metabolic
syndrome, erectile dysfunction, and coronary artery disease: Common links”. European
Urology, vol. 52, pp. 1590-1600, 2007.

REVIEW ARTICLE Abhijit et.al / IJIPSR / 3 (6), 2015, 663-687
Department of Pharmaceutical Technology ISSN (online) 2347-2154
Available online: www.ijipsr.com June Issue 685
105. C.B. Johannes, A.B. Araujo, H.A. Feldman, C.A. Derby, K.P. Kleinman, and J.B.
McKinlay, “Incidence of erectile dysfunction in men 40–69 years old: Longitudinal results
from the Massachusetts male aging study”. Journal of Urology, vol. 163, no. 2, pp. 460-463,
2000.
106. F.S. Carneiro, L.C. Sturgis, F.R. Giachini, Z.N. Carneiro, V.V Lima, B.M. Wynne, S. San
Martin, M.W. Brands, R.C. Tostes, and R.C. Webb, “TNF-alpha knockout mice have
increased corpora cavernosa relaxation”. The Journal of Sexual Medicine, vol. 6, no. 1, pp.
115-125, 2009.
107. I. Kifor, G.H. Williams, M.A. Vickers, M.P. Sullivan, P. Jodbert, and R.G. Dluhy, “Tissue
angiotensin II as a modulator of erectile function, Angiotensin peptide content, secretion and
effects in the corpus cavernosum”. Journal of Urology, vol. 157, pp. 1920-1925, 1997.
108. E.L. Schiffrin, and R.M. Touyz, “From bedside to bench to bedside: Role of renin-
angiotensin-aldosterone system in remodeling of resistance arteries in hypertension”.
American Journal of Physiology- Heart and Circulatory Physiology, vol. 287, pp. 435-446,
2004.
109. S. Granchi, G.B. Vannelli, L. Vignozzi, C. Crescioli, P. Ferruzzi, R. Mancina, M.C. Vinci, G.
Forti, S. Filippi, M. Luconi, F. Ledda, and M. Maggi, “Expression and regulation of
endothelin-1 and its receptors in human penile smooth muscle cells”. Molecular Human
Reproduction, vol. 8, no. 12, pp. 1053-1064, 2002.
110. E.L. Schiffrin, “Vascular endothelin in hypertension”. Vascular Pharmacology, vol. 43, pp.
19-29, 2005.
111. R.C. Tostes, and M.N. Muscara, “Endothelin receptor antagonists: Another potential
alternative for cardiovascular diseases”. Current Drug Targets- Cardiovascular and
Hematological Disorders, vol. 5, pp. 287-301, 2005.
112. P.A. Marsden, and B.M Brenner, “Transcriptional regulation of the endothelin-1 gene by
TNF-alpha”. American Journal of Physiology, vol. 262, pp. 854-861, 1992.
113. N.R. Ferreri, Y. Zhao, H. Takizawa, J.C. McGiff, “Tumor necrosis factor-alpha-angiotensin
interactions and regulation of blood pressure”. Journal of Hypertension, vol. 15, no. 12, pp.
1481-1484, 1997.
114. B. Luo, L. Liu, L. Tang, J. Zhang, Y. Ling, and M.B. Fallon, “ET-1 and TNF-alpha in HPS:
Analysis in prehepatic portal hypertension and biliary and nonbiliary cirrhosis in rats”.
REVIEW ARTICLE Abhijit et.al / IJIPSR / 3 (6), 2015, 663-687
Department of Pharmaceutical Technology ISSN (online) 2347-2154
Available online: www.ijipsr.com June Issue 686
American Journal of Physiology- Gastrointestinal and Liver Physiology, vol. 286, no. 2, pp.
294-303, 2004.
115. T. Kagawa, T. Takao, T. Horino, R. Matsumoto, K. Inoue, T. Morita, and K. Hashimoto,
“Angiotensin II receptor blocker inhibits tumour necrosis factor-alpha-induced cell damage in
human renal proximal tubular epithelial cells”. Nephrology (Carlton), vol. 13, no. 4, pp. 309-
315, 2008.
116. M. Cardenas-Leon, E. Diaz-Diaz, R. Arguelles-Medina, P. Sanchez-Canales, V. Diaz-
Sanchez et al., “Glycation and protein crosslinking in the diabetes and ageing pathogenesis”.
Revista de Investigacion Clinica, vol. 61, pp. 505-520, 2009.
117. J.J Cartledge, I. Eardley, and J.F. Morrison, “Nitric oxide mediated corpus cavernosal
smooth muscle relaxation is impaired in ageing and diabetes”. British Journal of Urology
International, vol. 87, pp. 394-401, 2001.
118. G. Basta, A.M. Schimidt, C. De, “Advanced glycation end products and vascular
inflammation: implications for accelerated atherosclerosis in diabetes”. Cardiovascular
Research, vol. 63, no. 4, pp. 582-592, 2004.
119. R. Bucala, K.J. Tracey, and A. Cerami, “Advanced glycosylation products quench nitric
oxide and mediate defective endothelium-dependent vasodilatation in experimental diabetes”.
Journal of Clinical Investigation, vol. 87, no. 2, pp. 432-438, 1991.
120. M. Brownlee, “Biochemistry and molecular cell biology of diabetic complications”. Nature,
vol. 414, no. 6865, pp. 813-820, 2001.
121. D.B. Jiaan, A.D. Seftel, J. Fogarty, N. Hampel, W. Cruz, J. Pomerantz, and M. Zuik, and
V.M. Monnier, “Age-related increase in an advanced glycation end product in penile tissue”.
World Journal of Urology, vol. 13, no. 6, pp. 369-375, 1995.
122. A.D. Seftel, N.D. Vaziri, Z. Ni et al., “Advanced glycation end products in human penis:
elevation in diabetic tissue, site of deposition, and possible effect through iNOS or eNOS”.
Urology, vol. 50, pp. 1016-1026, 1997.
123. R. Lehmann, and E.D. Schleicher, “Evaluation of glutathione S-transferase P1 genetic
variants affecting type-2 diabetes susceptibility and glycemic control”. Clinica Chimica Acta,
vol. 297, pp. 135-144, 2000.
124. A. Heidland, K. Sebekova, and R. Schinzel, “Advanced glycation end products and the
progresive course of renal disease”. American Journal of Kidney Diseases, vol. 38, no. 4, pp.
100-106, 2001.

REVIEW ARTICLE Abhijit et.al / IJIPSR / 3 (6), 2015, 663-687
Department of Pharmaceutical Technology ISSN (online) 2347-2154
Available online: www.ijipsr.com June Issue 687
125. H. Vlassara, J. Cai, T. Crandal, R. Goldberg, and V. Oberstein, “Inflammatory markers are
induced by dietary glycotoxins: A pathway for accelerated atherosclerosis in diabetes”.
Proceedings of National Academic Sciences, vol. 99, no. 24, pp. 15596-15601, 2002.
126. R. Singh, A. Barden, T. Mori, and L. Beilin, “Advanced glycated end products: a review”.
Diabetologia, vol. 44, pp. 129-145, 2001.
127. T.J. Bivalacqua, M.F. Usta, M. Kendirci, L. Pradhan, and X. Alvarez, “Superoxide anion
production in rat penis impairs erectile function in diabetes: influence of in vivo extracellular
superoxide dismutase gene therapy”. The Journal of Sexual Medicine, vol.2, pp. 187-197,
2005.
128. J.J. Cartledge, I. Eardley, and J.F. Morrison, “Advanced glycation end-products are
responsible for the impairment of corpus cavernosal smooth muscle relaxation seen in
diabetes”. British Journal of Urology International, vol. 87, no.4, pp. 402-407, 2001.
129. R.A. Costabile, “Optimizing treatment for diabetes mellitus induced erectile dysfunction”.
Journal of Urology, vol. 170, pp. 35-39, 2003.
130. S. Morano, “Pathophysiology of diabetic sexual dysfunction”. Journal of Endocrinological
Investigation, vol. 26, pp. 65-69, 2003.
131. D. Chen, Y.X. Shan, and Y.T. Dai, “Advanced glycation end products and their receptors
elevate the activity of endothelin-1 in rat cavernosum”. Zhonghua Nan Ke Xue, vol. 14, pp.
110-115, 2008.
132. S. Cellek, J. Rodrigo, E. Lobos, P. Fernandez, J. Serrano et al., “Selective nitrergic
neurodegeneration in diabetes mellitus- a nitric oxide-dependent phenomenon”. British
Journal of Pharmacology, vol. 128, no. 8, pp. 1804-1812, 1999.
133. H. Vlassara, “The AGE-receptor in the pathogenesis of diabetic complications”. Diabetes/
Metabolism Research and Reviews, vol. 17, pp. 436-443, 2001.
134. M.F. Usta, M. Kendirci, S. Gur, N.A. Foxwell, T.J. Bivalacqua et al., “The breakdown of
preformed advanced glycation end products reverses erectile dysfunction in streptozotocin-
induced diabetic rats: preventive versus curative treatment”. The Journal of Sexual Medicine,
vol. 3, pp. 242-250, 2006.










![International Journal of Innovative Pharmaceutical ...ijipsr.com/sites/default/files/articles/IJIPSRMNR-274.pdfA new series of 1-(1, 3 dioxoisoindolin 2 yl) 3 [(Z) substitutedbenzylidene]](https://img.dokumen.tips/doc/110x75/60680d55de1fbf78b2080514/international-journal-of-innovative-pharmaceutical-a-new-series-of-1-1-3-dioxoisoindolin.jpg)


















![International Journal of Innovative Pharmaceutical ...ijipsr.com/sites/default/files/articles/IJIPSRMN-27.pdf · pharmaceutical industry [1]. This is due to the fact that even trace](https://img.dokumen.tips/doc/110x75/5e9da1a75adc43534019cc63/international-journal-of-innovative-pharmaceutical-pharmaceutical-industry-1.jpg)