Embed Size (px)
Citation preview

204 Disasters and Emergency Planning
Disasters and Emergency PlanningJ Leaning, Harvard School of Public Health, Cambridge, MA, USA
ã 2008 Elsevier Inc. All rights reserved.
Introduction
Disasters have been part of human experience sincethe beginning of time. For centuries, people at risk ofdrought and famine or flood and heavy winds havemade individual or small group preparations to try toward off the worst effects. Agencies and systems dedicatedto disaster response have relatively recent origins,however, and can be traced, for most countries, to devel-opments during the nineteenth century and early twenti-eth centuries. These years saw governments deploymilitary units to help people affected by major naturaldisasters, urban authorities draw on fire departments toassist with emergencies other than fires, and civic organi-zations founded with the express purpose of taking careof the injured in war (the International Committee ofthe Red Cross) or the distressed at home (the nationalRed Cross and Red Crescent Societies). Private orreligious groups attended to people affected by emergen-cies or disaster, within their domestic jurisdictions orinternationally.
The formal field of disaster response developed in theyears during and after World War II. Many social, politi-cal, technological, and demographic factors contributedto this development. Relief agencies active during the warformed the core of what has now become a far-flungand international humanitarian network of nongovernmen-tal organizations. Governments came together to foundthe United Nations, which in turn established majorhumanitarian agencies with responsibilities for meetingemergency needs of vulnerable populations (UNHCR,UNICEF, WFP) and responding to major public healththreats (PAHO, WHO). The governments affected by theCold War set up civil defense planning bureaucracies thatsupported official and academic assessments of popula-tion response to natural disasters. Advances in scientificunderstanding and in technology (radar, satellites, com-puters) strengthened prediction and analysis of the geo-physical and technical parameters of natural andtechnological calamities. Population growth and acceler-ating population settlement in areas prone to hurricanes,earthquakes, and floods exposed greater numbers of peo-ple to the effects of these disasters. After major earth-quakes in Peru and Guatemala and serious hurricanes inthe United States, many local and national governmentscame under intensifying public pressure to improve theirdisaster response efforts. In 1980, the U.S. Governmentestablished the Federal Emergency Management Agency
and in 1983 PAHO set up its formal disaster response unit(Pan-American Health Organization, 1999).
The last 30 years have seen a marked expansion inknowledge on disasters themselves and the features ofeffective disaster response. Much of this knowledge basehas been built by practitioners and academics in what hasbecome a multidisciplinary enterprise, drawn from oper-ational sectors such as civil defense, fire-fighting, and thearmed forces as well as from fields of sociology, politicalscience, meteorology, engineering, psychology, emer-gency and trauma medicine, and public health.
Disasters
Disasters are complex phenomena that create extensiveconsequences for human populations. As such, all disas-ters can be seen as the sudden imposition of public healthcrises. An understanding of disasters in the context ofpublic health requires familiarity with issues of definition,incidence, data, and assessment. This understanding alsobuilds on recognizing features common to all disasters.
Definition
No standard case definition exists for disasters. The questfor an adequate definition reflects the underlying issuethat disasters are as much subjective as objective events.What is a disaster for a wealthy individual or group in ahighly developed society might not be perceived as suchby someone with far fewer resources in a communityorganized around lower levels of technology and capaci-ties, inured by chronic hardship to unexpected shocks.
The essence of what makes something a disaster, how-ever, has become a matter of general agreement: A disasteris an event that imposes severe and intense stress on acommunity and cannot be dealt with through deploymentof the ordinary resources of that community. Disasters areevents that require outside help.
Accepted definitions of disasters also include an ele-ment of time. Disasters are events that contain anticipa-tory warning signs (although often not observed or lookedfor) but impose a relatively abrupt impact. The conse-quences of that impact may persist for months or years.
Most disaster definitions are centered on human impactsand consequences. Natural events such as earthquakes orfloods that do not affect human populations (either in termsof direct casualties or more indirect economic, social, or

Disasters and Emergency Planning 205
psychological disruptions) are not usually registered as dis-asters and not counted in disaster databases.
Most disaster definitions also include an estimate ofeconomic costs, in terms of assets destroyed and fundsrequired to rebuilt and re-establish settlement and pre-disaster economic activity. Since thewealth of the developedworld derives in part from massive sustained investment ininfrastructure and technology, the measured economic costof a given disaster in rich countries is much higher than inpoor regions. As a result, disaster definitions that are basedon economic costs will introduce a bias toward events inwealthier countries.
Incidence
Calculating the annual incidence of disasters and trendlines over time is complicated by issues of ascertainmentas well as definition.
Disasters are not consistently or uniformly reported.Communities in poor and remote areas of the world donot have the resources to keep track of numbers of liveslost or economic assets destroyed. Transmitting these datato the media or a central data base also requires resourcesand time that are usually devoted to direct relief efforts.
In the last 30 years, however, as interest in the field ofdisasters has increased, there has been more outreach todisaster-affected communities. An apparent increase intrend lines may be simply the result of improved report-ing of events.
The accelerated worldwide population increase in thelast 60 years further complicates estimates of disaster inci-dence and trends. Since most definitions of disasters arebased on the numbers of people affected for a given event,an observed increase in the trend line for disaster incidencemight in fact be simply an artifact of population growth in agiven area.
Data
A number of organizations and academic centers havebeen tracking the incidence of disasters over the lastseveral decades and creating publicly available databaseson occurrences and trends.
One database used by many disaster experts has beendeveloped by the Brussels-basedCentre for Research on theEpidemiology of Disasters (CRED). The annual summaryof disaster statistics provided by CRED (2006) suggests thatdespite the acknowledged problems of definition and ascer-tainment, the incidence of disasters is increasing.
The CRED uses the following disaster definition:A disaster is
a situation or event, which overwhelms local capacity,
necessitating a request to national or international level
for external assistance; an unforeseen and often sudden
event that causes great damage, destruction and human
suffering (Centre for Research on the Epidemiology of
Disasters, 2007: 15).
In the CRED definition, disasters are categorized asnatural disasters (floods, windstorms, earthquakes, droughtand other extreme weather or meteorological events) andtechnological disasters (industrial, transport, and otherevents).
The threshold criteria (at least one must apply) for anevent to be included in the database are ten or morepeople reported killed; 100 or more people reportedaffected; a declaration of a state of emergency; and/or acall for emergency assistance.
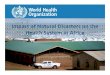
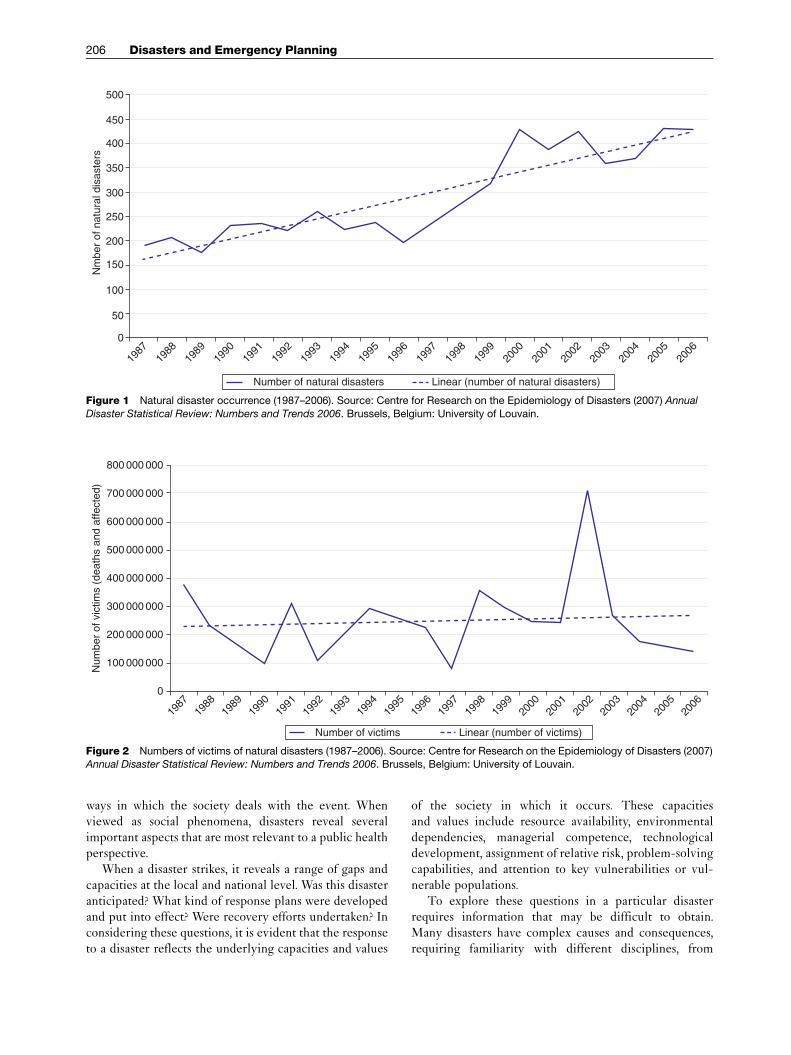
According to the latest (2006) CRED report, the trendline for natural disasters from 1987 to 2006 has shown anincrease in numbers of disasters as defined from justunder 200 disasters reported in 1987 to approximately450 disasters in 2006 (Figure 1). The numbers of peopleaffected (direct victims and people requiring immediateemergency assistance) have also increased over this timeframe, according to the CRED data on natural disasters(Figure 2). During this period, the annual numberof people affected ranged between 100 000 000 and300 000 000 for almost all years. The large peak in num-bers for 2002 is due primarily to four main events:A drought in India affecting 300million people, anotherin China affecting 60million people, a windstorm inChina affecting 100million people, and a flood in Chinaaffecting 60million people.
The economic costs of disasters are also recorded in theCRED database and an economic factor is used in deter-mining whether a given disaster is categorized as large.A large disaster in the CRED framework is one that causes50 deaths or more, affects 150 000 people or more, or exactscosts (in US$ 2003) of $200 million or more.
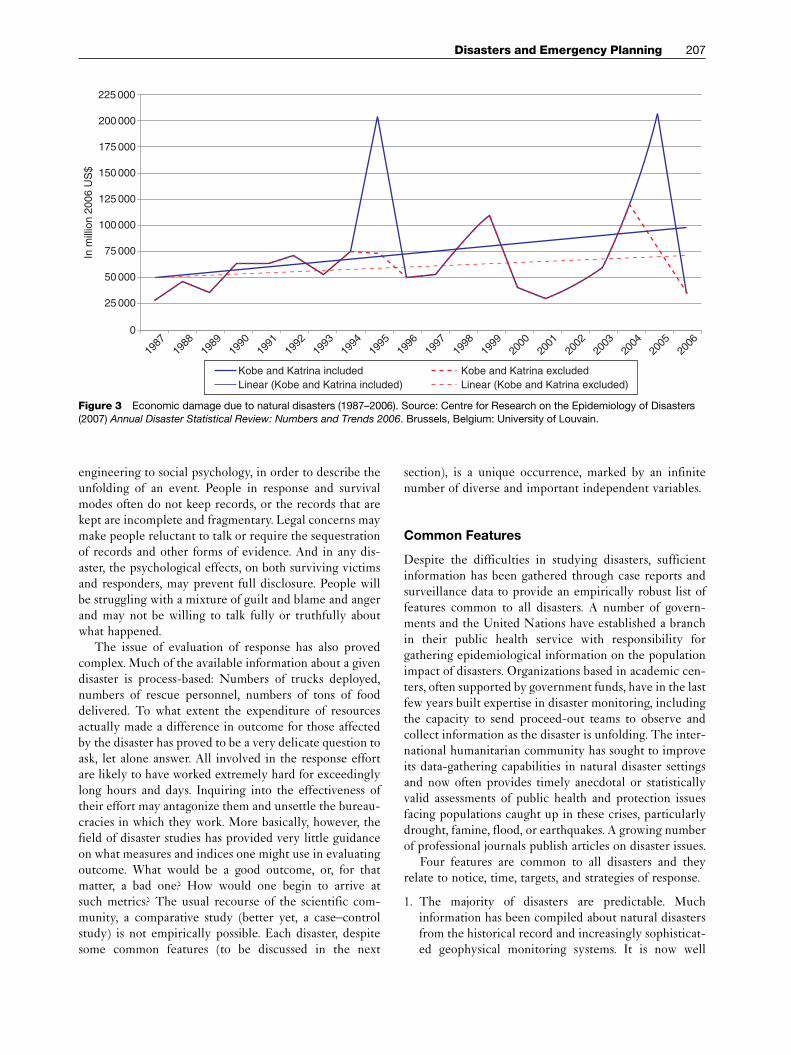
The economic costs of disasters, according to CREDdata, are also increasing (Figure 3; amount in 2006 US$).It is apparent that two major natural disasters, both occur-ring in the developed world, account for the recent majorpeaks: the 1995 earthquake (the Great Hanshin-AwajiEarthquake) in Kobe, Japan and the 2005 hurricane(Hurricane Katrina) in New Orleans, USA. The peak in2004–05 that is recorded with data from Kobe and Katrinaremoved is the sum of national and international costsrelating to the December 26, 2004 Asian Tsunami. Despiteits vast extent and extremely high death toll (approximately230 000 people killed in 14 affected countries), the AsianTsunami is dwarfed in first world economic terms becauseits impact was felt in less developed parts of the world.
Assessment
The study of disasters also requires examination of thesocial context in which a particular disaster occurs and the
100 000 000
0
200 000 000
300 000 000
400 000 000
500 000 000
600 000 000
700 000 000
800 000 000
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
Number of victims Linear (number of victims)
Num
ber
of v
ictim
s (d
eath
s an
d af
fect
ed)
Figure 2 Numbers of victims of natural disasters (1987–2006). Source: Centre for Research on the Epidemiology of Disasters (2007)Annual Disaster Statistical Review: Numbers and Trends 2006. Brussels, Belgium: University of Louvain.
Nm
ber
of n
atur
al d
isas
ters
0
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
50
100
150
200
250
300
350
400
450
500
Number of natural disasters Linear (number of natural disasters)
Figure 1 Natural disaster occurrence (1987–2006). Source: Centre for Research on the Epidemiology of Disasters (2007) Annual
Disaster Statistical Review: Numbers and Trends 2006. Brussels, Belgium: University of Louvain.
206 Disasters and Emergency Planning
ways in which the society deals with the event. Whenviewed as social phenomena, disasters reveal severalimportant aspects that are most relevant to a public healthperspective.
When a disaster strikes, it reveals a range of gaps andcapacities at the local and national level. Was this disasteranticipated? What kind of response plans were developedand put into effect? Were recovery efforts undertaken? Inconsidering these questions, it is evident that the responseto a disaster reflects the underlying capacities and values
of the society in which it occurs. These capacitiesand values include resource availability, environmentaldependencies, managerial competence, technologicaldevelopment, assignment of relative risk, problem-solvingcapabilities, and attention to key vulnerabilities or vul-nerable populations.
To explore these questions in a particular disasterrequires information that may be difficult to obtain.Many disasters have complex causes and consequences,requiring familiarity with different disciplines, from
225 000In
mill
ion
2006
US
$
200 000
175 000
150 000
125 000
100 000
75 000
50 000
25 000
0
2005
2004
2003
2002
2001
2000
1999
1998
1997
1996
1995
1994
1993
1992
1991
1990
1989
1988
1987
2006
Kobe and Katrina includedLinear (Kobe and Katrina included) Linear (Kobe and Katrina excluded)
Kobe and Katrina excluded
Figure 3 Economic damage due to natural disasters (1987–2006). Source: Centre for Research on the Epidemiology of Disasters(2007) Annual Disaster Statistical Review: Numbers and Trends 2006. Brussels, Belgium: University of Louvain.
Disasters and Emergency Planning 207
engineering to social psychology, in order to describe theunfolding of an event. People in response and survivalmodes often do not keep records, or the records that arekept are incomplete and fragmentary. Legal concerns maymake people reluctant to talk or require the sequestrationof records and other forms of evidence. And in any dis-aster, the psychological effects, on both surviving victimsand responders, may prevent full disclosure. People willbe struggling with a mixture of guilt and blame and angerand may not be willing to talk fully or truthfully aboutwhat happened.
The issue of evaluation of response has also provedcomplex. Much of the available information about a givendisaster is process-based: Numbers of trucks deployed,numbers of rescue personnel, numbers of tons of fooddelivered. To what extent the expenditure of resourcesactually made a difference in outcome for those affectedby the disaster has proved to be a very delicate question toask, let alone answer. All involved in the response effortare likely to have worked extremely hard for exceedinglylong hours and days. Inquiring into the effectiveness oftheir effort may antagonize them and unsettle the bureau-cracies in which they work. More basically, however, thefield of disaster studies has provided very little guidanceon what measures and indices one might use in evaluatingoutcome. What would be a good outcome, or, for thatmatter, a bad one? How would one begin to arrive atsuch metrics? The usual recourse of the scientific com-munity, a comparative study (better yet, a case–controlstudy) is not empirically possible. Each disaster, despitesome common features (to be discussed in the next
section), is a unique occurrence, marked by an infinitenumber of diverse and important independent variables.
Common Features
Despite the difficulties in studying disasters, sufficientinformation has been gathered through case reports andsurveillance data to provide an empirically robust list offeatures common to all disasters. A number of govern-ments and the United Nations have established a branchin their public health service with responsibility forgathering epidemiological information on the populationimpact of disasters. Organizations based in academic cen-ters, often supported by government funds, have in the lastfew years built expertise in disaster monitoring, includingthe capacity to send proceed-out teams to observe andcollect information as the disaster is unfolding. The inter-national humanitarian community has sought to improveits data-gathering capabilities in natural disaster settingsand now often provides timely anecdotal or statisticallyvalid assessments of public health and protection issuesfacing populations caught up in these crises, particularlydrought, famine, flood, or earthquakes. A growing numberof professional journals publish articles on disaster issues.
Four features are common to all disasters and theyrelate to notice, time, targets, and strategies of response.
1. The majority of disasters are predictable. Muchinformation has been compiled about natural disastersfrom the historical record and increasingly sophisticat-ed geophysical monitoring systems. It is now well

208 Disasters and Emergency Planning
understood that certain regions of the world lie inhigh-risk zones for earthquakes, windstorms, vastfloods, forest fires, and drought and famine. It is alsowell understood, with the exception of earthquakes,that these events have a seasonal periodicity andoccur in predictable annual cycles. Techniques arenow sufficiently advanced to warn at-risk populationsweeks in advance of the increased threat of impendingwindstorms and floods. As the situation unfolds, peoplecan be given 3–5 days of urgent warning regardingspecific geographic target areas. Large forest or scrubfires move quickly, but the assessment of rising risk isdeveloped over a period of at least several weeks, if notmonths. The pace of droughts is much slower, butmonitoring systems have become precisely calibratedto issue warning about phases of progressive droughtand population behavior (satellite imagery of cropfailure, change in market prices for food). If actedupon, these alerts can provide the time for govern-ments and the relief community to prepare a response.
In the case of technological disasters (such as minecollapse or explosion, chemical releases, building fail-ures, nuclear power plant events, transport calamities),a multidisciplinary science of risk assessment andstudy of interactions between humans and technicalsystems has developed. Experts in this field of techno-logical disasters find that it is usually possible to tracethe chain of system failure that produced the disasterevent and in many instances can arrive at graded esti-mates of probable risks of future failure.
2. All disasters occur in phases through time. Disasterexperts have identified three main phases (warning,impact, and consequences). Each of these phases variesin length of time depending on the nature of the dis-aster and the nature of the response. The names ap-plied to these phases may differ from country tocountry but the concept remains the same.
The warning phase begins with recognizing thatsome areas of the world or some technologies aremore at risk for certain kinds of disasters than othersand extends right up to sounding the alert at the actualmoment when the disaster event occurs. Often thatmoment is indeed measured in minutes or hours (aswith hurricanes and typhoons, or transport disasters).For other kinds of disasters (floods and forest fires, ortoxic chemical releases to the environment), the disas-ter event may build in magnitude and scope over aperiod of hours or days, so the warning phase for someadjacent geographic areas overlaps with the impactphase for those areas first affected.
The impact phase defines the period in time whenthe disaster in all its force has struck a geographic area.For earthquakes, the impact period is usually measuredin seconds and minutes, with after-shocks extendingfor hours and days at a diminished force. For floods, the
impact phase continues until the flood waters begin torecede from their high water mark. For industrial dis-asters, such as chemical explosions that release toxinsto the environment, the impact phase may persist for aslong as the contaminant is in contact with the affectedpopulation.
The consequences phase is often called the recoveryphase and refers to the longer-term issues that thedisaster has caused for the affected population, region-al environment, and society as a whole. These conse-quences range from death, injury, entrapment, orforced evacuation of human and animal populationsto extensive destruction of natural and built environ-ments, including infrastructure, assets, and livelihoods.Disasters can impose individual and population-scalepsychological distress and can affect the prevailingpolitical dynamics in a country or region. The conse-quences phase is always the most long-lasting andusually presents the greatest challenges to the disasterresponse community.
3. Disasters strike the vulnerable disproportionately. Vul-nerable in this context means those people who forreasons of socioeconomic status, political or socialmarginalization, or physical attributes are less wellprepared than others in the society to cope with theimpact of a given disaster. In many parts of the world,newly immigrant populations do not speak the officiallanguage in which warnings and instructions are issued.The physically disabled, medically ill, or mentallyimpaired are impeded from many forms of flight orsurvival maneuvers. Women, children, and the elderlyare in general less physically strong, so they will deriveless benefit from protection strategies that requirestrength and speed. In the developed world, it is thepoor who lack transport or second homes, makingevacuation in response to warning a less possibleoption.
Entire populations in the developing world are alsorendered vulnerable to hazards for reasons directlyrelated to poverty and population density. Populationgrowth over the last 50 years has disproportionatelyaffected the developing world. In the countryside, ac-cess to safe and productive land is becoming increas-ingly hard to attain, at the level of individual choiceand national policy. In rapidly urbanizing areas, peopleare crowded into poorly built structures that do notcomply with fire or earthquake codes. Hundreds ofmillions of people live on flood plains in China andIndia or in precarious hillsides and mountain areas orin unsafe slums and landfill sites not because they wantto do so but because they have no other choice.
Poverty at the level of the nation-state imposes anadditional vulnerability. To plan and prepare for dis-asters requires great investments of social capital andfinancial resources. Many developing nations have thin

Disasters and Emergency Planning 209
layers of managerial competence and cannot afford thetechnology to support substantial population-scale dis-aster response. In place of a network of interrelateddisaster bureaucracies that one sees in the developedworld, the countries of the developing world rely upontheir armed forces to organize response to major dis-asters when they strike. However, as effective as themilitary might be in the immediate postimpact phase,it is rare that military resources are devoted to robustefforts to protect and prepare the population in ad-vance of when disaster strikes. So poverty at the level ofthe national state constrains efforts at comprehensiveplanning to prevent and prepare for disasters, thusmaking their populations collectively more vulnerableto disaster impacts.
This point is tempered somewhat by the fact thatpeople in developing countries, particularly at the locallevel, may have access to traditional and innovativecoping strategies that make individuals and groupsvery good problem solvers in the face of regularlyoccurring disasters and resilient survivors in the faceof new threats.
A concluding note in this discussion of vulnerabilityrelates to the systematic exclusion of the vulnerable inmost efforts at disaster planning. Measures to protectpopulations are developed to suit the needs of themajority, and it takes a special effort to identify andmeet the concerns of the more socially and economi-cally marginalized groups. That effort is not usuallyundertaken, in rich as well as poor countries, until amajor disaster reveals this focal inadequacy.
4. Disasters are public health crises. They have direct andindirect effects on the health and well-being of largepopulations. They occur over time and alter the livingconditions and psychological mindsets of communitiesin the path of and adjacent to the direct disaster impactarea. Disasters require planning and response strategiesto address a wide range of human needs: Water, shelter,food, air quality, mobility, safety, medical care, psycho-logical support for dealing with loss, fear, grief, andanger. These strategies are focused on the needs ofpopulations, rather than individuals, and as such invokethe public health principles of prevention and popula-tion ethics.
Primary and secondary prevention is the publichealth strategy employed when the disease, condition,or event creates harm that cannot be rectified. Alldisasters entail serious and irretrievable loss of lifeand livelihoods. Comprehensive disaster strategiesfocus on a series of upstream issues, in terms of riskassessment and risk reduction, including warning, inorder to prevent a disaster from occurring or minimiz-ing its impact when it does strike. Comprehensive dis-aster strategies are also based on matching resources toneeds. Often, especially in the early phases after a
disaster has struck, the needs of the affected populationfar outstrip the resources available. This imbalance maypersist for weeks or months, depending on the magni-tude of the disaster and the resources that can be mar-shaled from outside. Consequently, disaster plannersand responders must organize the distribution ofgoods and services on the principle of emergency tri-age, which directs not only that those in greatest needare the priority targets for receipt of aid, but that scantresources must not be wasted on maximizing life for afew if by so doing the needs of many more people arecompromised or allowed to go unmet.
Emergency Planning and Disaster Response
These common features, identified through years ofobservation and analysis, provide the rationale, the logicalbasis, for the entire enterprise of emergency and disasterplanning. If disasters are in large measure predictable, if itis understood that they occur in phases, and if the patternof human impact and response is generally understood inadvance, then there is substantial justification for thedevelopment of an enterprise that can intervene in anygiven event with the aim of maximizing the chances thatas few people are adversely affected as possible.
Components of Disaster Planning andResponse
Disaster experts have over the years identified and cate-gorized disaster response strategies to match the threetime phases in which disasters take place: Warning,impact, and consequences. Disaster response strategiesalso occur in three main phases: Prevention, response,and recovery. These phases have subphases, such that anelement of prevention includes mitigation, the responsephase has an immediate postimpact component as well asa longer-term one, and the recovery phase extends intomany activities, including reconstruction, populationreturn, and resettlement (Table 1).
All these measures require policy development andimplementation, supported by appropriate regulatoryand legislative frameworks. These measures also dependon the efforts of disaster professionals, who come from awide range of backgrounds and training. The organizationof disaster response varies from country to country andoften within countries. In urban areas of the developedworld, a generic organizational model that is often used isthe Incident Command System (ICS), developed (asdescribed by Irwin, 1989) from U.S. experience fightingforest fires in California in the early 1970s. Disaster med-ical systems usually reflect the traditions of medical andtrauma care within a domestic jurisdiction. In the devel-oping world, disaster response often relies on the military.

Table 1 Key strategies in disaster response
Prevention/mitigation. Risk assessment (hazards and vulnerabilities). Risk elimination. Risk reduction. Risk protection. Monitoring and warning
Preparedness. Planning for all phases of disaster response. Planning for operational response during post impact and
recovery phases: Command, communications, coordination,
information. Resource mobilization and stockpiling. Setting up back-up systems and redundancies. Public education. Training and drills for disaster responders. Urgent warning and evacuation. Monitoring and evaluation
Response. Immediate post-impact (rescue). Short-term post-impact (recovery)Recovery. Reconstruction. Return. Resettlement
210 Disasters and Emergency Planning
Disasters of sweeping scope, entraining tens of thousandsif not millions of people, often enlist the efforts of theinternational humanitarian community, whose strategiesand programs are oriented to taking care of people whohave evacuated the area and gathered in large groups inorder to escape the direct effects of the event.
The work of prevention and mitigation is centered onassessment of risks, with priority placed on identificationand categorization of major and recurring threats to agiven population or geographic area. A refinement inrisk assessment is the capacity to specify by time andplace the real-time escalation scenario of a particulardisaster. This capacity is based on active monitoring ofprecursor conditions and permits increasingly early andspecific warning that a high-risk event is actually verylikely to occur.
For example, certain areas of the world are known tobe at high risk for windstorms accompanied by seriousflooding, such as the southeast and Gulf regions of theUnited States and the coastal zones of the Bay of Bengal(northeastern India and Bangladesh). This risk increasesdramatically during the hurricane and cyclone seasons(from June to November in the United States and fromApril to December in the Bay of Bengal). Meteorologicalfactors (such as fluctuations in ocean surface temperature)have been identified that indicate whether a particularhurricane or cyclone season is likely to be more or lesssevere. This information is used to accelerate prepared-ness and response planning for that season. Then, as theseason approaches, radar and satellite imaging permitclose inspection of brewing storms in the Atlantic or Bay
of Bengal. The increasingly intense and detailed depictionof an impending major windstorm provides the responsecommunity and the general public with more in-depth,targeted, and urgent information about when and whereto expect landfall.
This example highlights the way in which preventionmoves into mitigation. An aspect of prevention is elimina-tion of risk, which is not usually possible in the case ofvirtually all natural disasters and most technological ones.Reduction of risk, often termed mitigation, has acquireda major role in appropriate plans to address disaster threats.In the example of hurricanes or cyclones, mitigationefforts focus on providing early and effective warnings toresponders and the residents in the predicted impact zonein order to promote appropriate population responsesthat will reduce injury and loss of life (in this case, evacu-ation to stable structures at high ground). Mitigationefforts include measures to inspect and strengthen infra-structure (such as dams, bridges, buildings) and to moni-tor compliance with safety regulations and trainingpolicies relating to industries that are known to be risk-prone, such as mining, or industries in which a disasterwill have very costly consequences, such as air travel ornuclear power.
The work of preparedness is to ensure as fully aspossible that the response phase (immediate postimpactand somewhat longer term) is carried out with com-prehensive effectiveness. All preparedness activities aredesigned to support operations that must take place assoon as possible after the disaster impact. Efforts in thiscategory include planning for all phases, resource devel-opment, personnel training and practice drills, publiceducation, and development of technologies and systemsfor early warning, communication, coordination, andsocial mobilization.
In the example of hurricanes and cyclones, prepared-ness efforts focus on identifying main evacuation routesand safe destination sites, educating the public aboutwarning and evacuation procedures, including how toshore up and protect their homes in the event of evacua-tion, and making sure that everyone at risk from the windor the stormwater surge hears, sees, and heeds the instruc-tions contained in the warning and evacuation messages.
The concept of impact, as one phase in the evolution ofa disaster, is as noted above somewhat elastic in terms oftime. During the peak intensity of a storm or in the face ofrapidly rising flood waters, emergency response opera-tions are rarely undertaken. Instead, the response isinitiated as soon as is possible after the peak impact haspassed, in order not to expose disaster personnel toextreme danger. The first activities undertaken in theimmediate postimpact phase, termed the rescue phase,focus on finding, extricating, and stabilizing injured sur-vivors and providing emergency services to those in need.

Disasters and Emergency Planning 211
A slightly more delayed set of actions, still in the postim-pact response category, is called recovery. Recoveryoperations in this period are aimed at assessing damage,removing rubble, clearing streets and roads, repairingutilities, organizing primary care and instituting publichealth measures (such as vaccination), and establishingsecure temporary shelter and supply lines for evacuatedpopulations.
In terms of longer-term consequences, the responsestrategy is variously referred to as recovery, or recon-struction. Since the earlier postimpact tasks may takemonths, if not years to accomplish, often these two phasesoverlap in time and place. The main effort in the recovery/reconstruction phase is to return the affected population toits predisaster state of social and economic well-being. Theaim is to have early repairs and organization of servicescoincide with plans for the longer-term recovery phase.Such coherence in planning and operations is not alwaysachieved, in part because different actors are responsible forthese separate pieces of work and in part because the localleaders who could most directly inform the longer-termrecovery planning may be absent or ignored.
Public Health Impact of Specific Categoriesof Disasters
The greatest public health effects are caused by disasterswhose impact and consequences affect the largest numberof people. Usually the impact causes intense and wide-spread destruction and the extensive consequences areexperienced in the immediate or short-term aftermath.Disasters with this profile include floods, windstorms,earthquakes, drought/famine, and toxic contamination.These disasters often involve preimpact or postimpactpopulation movement (evacuation, flight), which in itselfcan cause significant harm and distress to large numbersof people.
In recent years, using analysis of case studies andcontemporaneous survey methodologies, epidemiologistshave advanced our knowledge of specific kinds of publichealth issues to anticipate in the wake of particular kindsof major disasters (Table 2). Philen et al. (1992), in theirepidemiological study of deaths from Hurricane Hugoin 1989, found that more people died from trauma thandrowning, including from self-help efforts in early clean-up (electrocution, heart attacks, and chain-saw trauma).This observation has been confirmed since in populationsgiven adequate warning for evacuation and has provensignificant in the design of preparedness and responseinterventions.
In many disasters, the correlation between numbers ofpeople directly affected and the public health impact isdirect, as can be seen in the evolving efforts to cope withthe consequences of the Asian Tsunami (December 2004)and Hurricane Katrina in the United States (August 2005).
If the concept of public health is expanded to include awide range of social and psychological factors, however,assignment of the public health impact of disasters doesnot always involve a straight numerical calculation relatedto immediate destruction and casualties. Certain kinds ofdisasters, particularly those involving toxic chemicals andradiation, or disasters that strike at pivotal historicalmoments, may inject disruptions with very long-lastingpolitical and psychosocial consequences. The enduringdynamics of some disasters, as noted by Erikson (1995),often carry implications for the health of the public thatare far out of proportion to the immediate observedeffects on infrastructure, environment, and human life.
For instance, the relatively low-level radiation leak atthe Three Mile Island nuclear power plant in Pennsylvaniain 1979, which caused no human casualties, caused suchfear in the general U.S. public that the subsequent dev-elopment of the nuclear industry was severely curtailed.The subsequent public health consequences includedthe national choice of oil and coal sources over nuclearenergy, with implications for environmental pollutionand geopolitics; increased regulation and scrutiny of thenuclear industry; and heightened psychological concernamong populations living adjacent to and downwind ofexisting nuclear power plants. This concern, sustained tothis day, also accelerated public anxiety throughout the1980s about the possible human consequences of nuclearwar and contributed to the campaign for nuclear armsreduction treaties.
Other disasters have had similarly far-reaching politi-cal, social, and psychological effects. The explosion andairborne release of methyl isocyanate over a sleepingpopulation in Bhopal (December 1984) resulted in anestimated 5 000 deaths but affected hundreds of thousandsof other people in the area because of the widespreadphysical and psychological morbidity caused by the lin-gering effects of chemical exposure and the loss of familymembers and livelihoods. The quest for ongoing medicalcare and for reparations has spawned the creation of neworganizations, new interest groups, and new national andinternational regulations relating to corporate responsi-bility and state liability for these major industrial events.The major nuclear power plant disaster at Chernobyl,USSR (April 1986), followed 2 years later by a very seri-ous earthquake in Soviet Armenia (December 1988), had asignificant influence on the Soviet policy of glasnost andthe international politics of the Cold War.
Lessons Learned
The duration of the recovery phase (the length of time ittakes before an affected community returns to its predisa-ster state) constitutes the main measure for assessing boththe magnitude of the disaster and the effectiveness of the
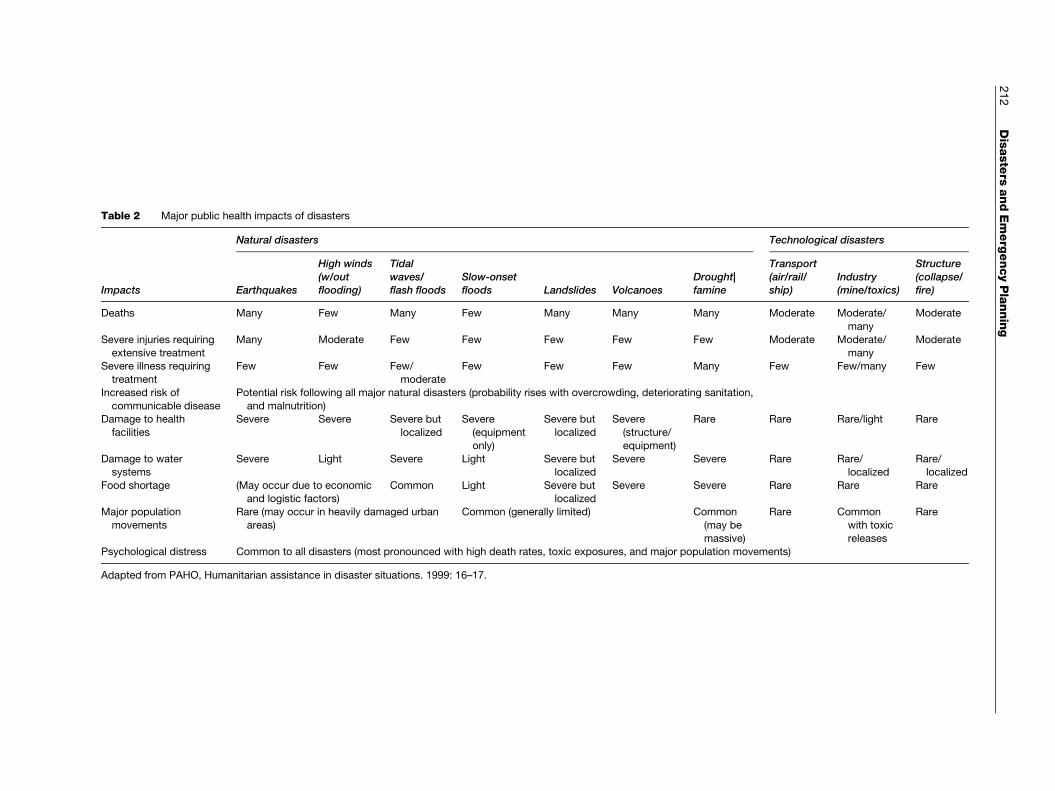
Table 2 Major public health impacts of disasters
Natural disasters Technological disasters
Impacts Earthquakes
High winds(w/outflooding)
Tidalwaves/flash floods
Slow-onsetfloods Landslides Volcanoes
Drought|famine
Transport(air/rail/ship)
Industry(mine/toxics)
Structure(collapse/fire)
Deaths Many Few Many Few Many Many Many Moderate Moderate/
many
Moderate
Severe injuries requiring
extensive treatment
Many Moderate Few Few Few Few Few Moderate Moderate/
many
Moderate
Severe illness requiring
treatment
Few Few Few/
moderate
Few Few Few Many Few Few/many Few
Increased risk of
communicable disease
Potential risk following all major natural disasters (probability rises with overcrowding, deteriorating sanitation,
and malnutrition)Damage to health
facilities
Severe Severe Severe but
localized
Severe
(equipment
only)
Severe but
localized
Severe
(structure/
equipment)
Rare Rare Rare/light Rare
Damage to watersystems
Severe Light Severe Light Severe butlocalized
Severe Severe Rare Rare/localized
Rare/localized
Food shortage (May occur due to economic
and logistic factors)
Common Light Severe but
localized
Severe Severe Rare Rare Rare
Major population
movements
Rare (may occur in heavily damaged urban
areas)
Common (generally limited) Common
(may be
massive)
Rare Common
with toxic
releases
Rare
Psychological distress Common to all disasters (most pronounced with high death rates, toxic exposures, and major population movements)
Adapted from PAHO, Humanitarian assistance in disaster situations. 1999: 16–17.
212
Disasters
andEmerg
encyPlanning

Disasters and Emergency Planning 213
response. Shortening that time period is a fundamental goalof the disaster response community. Technical competence(adequate warning, timely and appropriate interventions) isonlyone factor in achieving that goal. Experience has shownthat duration of recovery is measured as much in psycho-logical as in material terms. Experience has also shown thatthese public perceptions and psychological reactions areclosely related towhat actually happened, andwhen, duringall phases of the disaster experience.
When a disaster strikes, the expert community nowknows that their efforts will be evaluated not only in termsof what they did but also in terms of how people felt aboutthese actions. If people remember only that warningwas late and help was paltry, their ability to bounce backfrom the disaster and progress through recovery will bedelayed. Grievance and anger will cloud their perceptionsand intensify feelings of loss and sorrow. Themost enduringpsychological consequence of a disaster is based on socialmemoryandwhether people believe that the authorities dideverything possible to help them. In other words, a disasterresponse that not only is competent and humane but isperceived as such stands the best chance of shortening therecovery phase.
From this vantage point, a discussion of lessons learnedis as much a commentary on how to affect human psy-chological reactions as it is a list of key practical andtechnical inputs.
1. In the first 72 hours after a major natural disaster,all rescue efforts are undertaken by local survivors.The disaster itself usually creates conditions thatblock access from the outside. Consequently, peoplein disaster-prone areas must be educated to understandthat in the first few days after disaster impact theythemselves, within their own community, will needto search for survivors and find whatever food,shelter, and water they can. This understanding mustbe conveyed in advance of the disaster and be embed-ded in training about how to respond to official warn-ings and alerts about impending threats. Without suchadvance notice and education, people will be unpre-pared to help themselves initially and will tend toblame the authorities for this gap in outside reliefsupport.
2. Help from the outside must come after approximately72 h, or local people will begin to run out of sup-plies, will begin to be overcome by fatigue and grief,and will begin to lose trust in provincial, state, ornational authorities. In the face of major disasters,local people do cope, but only in the short run. As wehave noted, by definition a disaster is an event thatrequires outside assistance.
3. Outside responders must attend to issues of timing,appropriateness, and public perception in the delivery
of emergency supplies and services. The key priorities inthe immediate postimpact period must be undertakenrapidly with close attention to what the population actu-ally needs (tents and blankets rather than clothes) and toethical and fair methods of distribution.
4. Actions taken to protect populations and move themout of harm’s way (measures relating to security, shel-ter, evacuation, and temporary resettlement) are ladenwith psychosocial complexities. Inattention to thesecomplexities will give rise to significant negative con-sequences. Outside authorities should shore up law andorder without making local people more afraid. Theyshould try to avoid crowding people into mass settingswhere they have no personal space or privacy, sincevery high population densities raise the potential forepidemic disease and contribute to breakdown of in-ternal social order. Moving people far from home totemporary individual or group settlements may in-crease the likelihood that many will never return.
5. Disaster responders must recognize that to take care ofthe living is to take care of their dead. Urgent careof injured and desperate survivors should not distractauthorities from recognizing that disaster survivors aresuffused with attachment to the people they have lost.From the outset, in the phase of rescue as well asrecovery, survivors will expect the disaster respondersto devote careful attention to a sustained search for themissing and to appropriate retrieval and burial of thosewho have died.
6. The most complex phase of the disaster response is therecovery phase, in which a wide range of outside andlocal responders attempt to deal with the longer-termconsequences of the disaster. The Tsunami EvaluationSynthesis Report (Telford et al., 2006) offers lessonslearned from the response to the Asian Tsunami thatare applicable to many disasters much smaller in scopeand impact. A central finding is the importance ofsupporting local leaders and building local capacityin the communities. When the inevitable departure ofoutside resources and relief workers occurs, it is ineveryone’s interests that local actors are prepared totake charge of the remaining tasks of reconstruction.
7. Individuals as well as organizations and systems playmajor roles in disasters. Effective disaster leaders playsignificant roles in ensuring adherence to these lessonslearned and in guiding public perception and grouppsychology. The public face of leadership is usuallyprovided by the highest governmental authority for theaffected region, the senior officer in command of theresponse effort, and a corporate executive if a businessentity is involved. Disaster leaders must be able towork with the media and with the responders toevoke human resilience, maintain hope, and respondto psychological distress.

214 Disasters and Emergency Planning
Competent and compassionate personnel are alsocrucial to the disaster response operation. Psychologi-cal and physical support to alleviate disaster workerstress must be provided to ensure that the workforcecontinues to be able to provide for the needs of theaffected population.
Issues for the Future
The major issues facing the field of disasters and disasterresponse are:
1. The events themselves are affecting more people andprobably becoming more frequent.
2. Human interactions with technology and the environ-ment are contributing to these trends.
3. As a result, the demands on the disaster responsecommunity will only become more extensive and com-plex in the years ahead.
The predicted increases in disaster incidence and dis-aster severity arise from projections in observed trendsas well as from scientific assessments of global climatechange. Major concerns are increased incidence of hugewindstorms and floods, in earthquakes with massive pop-ulation consequences, and in widespread drought, leadingto significant famine.
Accelerating trends in human interaction with theenvironment, as well as global climate change, have beenidentified by the Intergovernmental Panel on GlobalClimate (Schneider et al., 2007) as contributing to theseincreases in disaster incidence and severity. These humaninteractions include policies relating to land use, popula-tion growth, population settlement, energy consumption,and economic development. These trends suggest that themajor threats for all populations in the world will comefrom the relationship of populations to environmentalhazards, particularly in terms of windstorms, floods,drought, and earthquakes. Reducing the vulnerability ofgrowing populations who are densely settled in high-riskcoastal or earthquake zones or who are residing in areas ofincreasing water scarcity must become an even higherpriority than it is today. These tasks of risk assessment andrisk reduction – the work of prevention and mitigation –have urgent relevance for rich societies as well as poor.
Yet regardless of improved efforts at prevention andmitigation in the years ahead, it is probable that an everlarger number of people will be caught up in major dis-asters, requiring an intensifying disaster capacity to pre-pare and respond appropriately when these events occur.This challenge may well bring closer alignment of thedomestic disaster response communities with agencieswho provide international humanitarian relief. In the
twenty-first century, disasters affecting one region mayprove more frequently to require outside help from therest of the world.
See also: Humanitarian Responses to Complex Emer-
gencies; Terrorism; Weapons of Mass Destruction.
Citations
Centre for Research on the Epidemiology of Disasters (2007) AnnualDisaster Statistical Review: Numbers and Trends 2006. Brussels,Belgium: University of Louvain.
Erikson KT (1995) New Species of Trouble: The Human Experience ofModern Disasters. New York: WW Norton.
Irwin RL (1989) The incident command system. In: Auf der Heide E (ed.)Disaster Response: Principles of Preparation and Coordination, pp.133–163. St. Louis, MO: Mosby.
Pan-American Health Organization (1999) Humanitarian assistance indisaster response. www.paho.org (accessed November 2007).
Philen RM, Combs DL, Miller L, Sanderson LM, Gibson Parrish R, andIng R (1992) Hurricane Hugo-related deaths: South Carolina andPuerto Rico, 1989. Disasters 16: 53–59.
Schneider SH, Semenov S, Patwardhan A, et al. (2007) Assessing keyvulnerabilities and the risk from climate change. In: Parry ML,Canziani OF, Palutikof JP and Hansen CE (eds.) Climate Change2007: Impacts, Adaptation and Vulnerability, pp. 777–810.Contribution of Working group II to the Fourth Assessment Report ofthe Intergovernmental Panel on Climate Change. Cambridge, UK:Cambridge University Press.
Telford J, Cosgrave J, and Houghton R (2006) Joint Evaluationof theInternational Response to the Indian Ocean Tsunami: SynthesisReport. London: Tsunami Evaluation Coalition.
Further Reading
Auf der Heide E (1989) Disaster Response: Principles of Preparation andCoordination. St. Louis, MO: Mosby.
Barton AH (1970) Communities in Disaster: A Sociological Analysis ofCollective Stress Situations. Garden City, NY: Doubleday Anchor.
Bignell V, Peters G, and Pym C (1978) Catastrophic Failures. MiltonKeynes, UK: The Open University Press.
Cohen RE and Ahearn FL (1980) Handbook for Mental Health Care ofDisaster Victims. Baltimore, MD: Johns Hopkins University Press.
Cuny FC (1993) Introduction to disaster management, lesson 5:Technologies of disaster management. Prehospital DisasterMedicine 6: 372–374.
Daniels RJ, Kettl DF and Kunreuther H (eds.) (2006) On Risk andDisaster: Lessons from Hurricane Katrina. Philadelphia, PA:University of Pennsylvania Press.
Gist R and Lubin B (eds.) (1989) Psychological Aspects of Disaster.New York: John Wiley & Sons.
Hogan DE and Burstein JL (eds.) (2002) Disaster Medicine. Philadelphia,PA: Lippincott Williams and Wilkins.
Mileti DS (1999) Disasters by Design: A Reassessment of NaturalHazards in the United States. Washington, DC: Joseph Henry Press.
Noji EK (ed.) (1997) The Public Health Consequences of Disasters.New York: Oxford University Press.
Perrow C (1984) Normal Accidents: Living with High-risk Technologies.New York: Basic Books.
Waeckerle JF (1991) Disaster planning and response. New EnglandJournal of Medicine 324: 815–821.
World Health Organization (1999) Community EmergencyPreparedness: A Manual for Managers and Policy-makers. Geneva,Switzerland: WHO.

Disease Classification 215
Relevant Websites
http://www.southasiadisasters.net – All India Disaster Mitigation Institute.http://www.adpc.net – Asian Disaster Preparedness Center.http://www.cdc.gov – Centers for Disease Control and
Prevention (CDC).http://www.cred.be – Centre for Research on the Epidemiology of
Disasters (CRED).http://www.climate.noaa.gov – Climate Program Office (CPO) of the
National Oceanic and Atmospheric Administration (NOAA),Washington DC.
http://www.emi-megacities.org – Earthquakes and MegacitiesInitiative (EMI).
http://www.ema.gov.au – Emergency Management Australia.http://ec.europa.eu/echo – European Commission Humanitarian Aid
department (ECHO).http://www.fews.net – Famine Early Warning System Network (FEWS)
(from USAID).http://www.fema.gov – Federal Emergency Management
Agency (FEMA).http://www.geohaz.org – GeoHazards International (GHI).http://www.state.gov/s/inr/hiu – Humanitarian Information Unit.http://www.ipcc.ch – Intergovernmental Panel on Global Climate
Change.
Disease ClassificationR Jakob, World Health Organization, Geneva, Switzerland
ã 2008 WHO. Published by Elsevier Inc. All rights reserved.
Classifications are essential for science, as they define theuniverse of entities that are studied and highlight the rele-vant aspects of these entities. Internationally endorsed clas-sifications facilitate the storage, retrieval, analysis, andinterpretation of data and their comparison within popula-tions over time and between populations at the same pointin time, as well as the compilation of internationally consis-tent data. Populations may be nations, states and territories,regions, minority groups, or other specified groups.
In many areas of the world, a large proportion of thepopulation has no access to health care provided by medi-cally qualified personnel. In these areas, health care is oftenprovided by lay or paramedical personnel and is based ontraditional methods or elementary medical training. Thesesame personnel also must produce the health informationneeded to indicate the existence of a health problem or tofacilitate the management of health-care systems.
Use
The purpose of classifying diseases is manifold. In epide-miology and prevention, a classification of diseases is usedto alert the health authorities to the emergence of a health
http://www.icrc.org – International Committee of the Red Cross (ICRC).http://www.ifrc.org – International Federation of Red Cross and Red
Crescent Societies (IFRC).http://www.itc.nl – International Institute for Geo-Information Science
and Earth Observation (ITC).http://www.noaa.gov – National Oceanic and Atmospheric
Administration (NOAA).http://www.ntsb.gov – National Transportation Safety Board (NTSB).http://www.colorado.edu/hazards – Natural Hazards Center at the
University of Colorado at Boulder.http://www.paho.org – Pan American Health Organization (PAHO).http://www.reliefweb.int – ReliefWeb.http://www.unisdr.org – United Nations International Strategy for
Disaster Reduction (UNISDR).http://ochaonline.un.org – United Nations Office for the Coordination of
Humanitarian Affairs (OCHA).http://www.udel.edu/DRC – University of Delaware Disaster Research
Center.http://dmc.engr.wisc.edu – University of Wisconsin Disaster
Management Center.http://www.usfa.dhs.gov – U.S. Fire Administration.http://www.usgs.gov – US Geological Survey Service.http://www.who.int – World Health Organization (WHO).http://www.wssi.org – World Seismic Safety Initiative (WSSI).
problem (for example, an increase in cases of an infectiousdisease indicating the possible start of an epidemic).
Management of health depends on information aboutdisease frequency for planning, operations, or evaluation.Knowledge is needed regarding diseases that cause highmortality and morbidity to allocate health-care workers,medications, devices, and facilities needed for treatmentand prevention.
Available funds for providing health-care services andimproving health are always limited. Statistics that arecompiled with the aid of a classification of diseases allowspending the money in the most useful way for the popu-lation health. Prevention and health programs can beimproved, for example, by analyzing differences betweentwo regions in terms of maternal deaths.
There are many different diseases. In order to under-stand the disease pattern of a population, one needs tohave a unique classification system so that the resultscan be displayed and reported in a systematic way. Agree-ing on how to classify (group) diseases at a regional,national, and international level enables comparing resultsand merging such information into larger-scale statis-tics ( Jakob et al., 2007; WHO, International Classifica-tions, 2007).