Embed Size (px)
Citation preview
Using data to save money and
improve performance
Annalisa Trama
Fondazione IRCCS Istituto Nazionale dei Tumori, Milan (Italy)
International Conference Improving Outcomes in Cancer
13 November 2015 - Parliament of the Republic of Lithuania
www.eurocare.it
Survival measure
health care system effectiveness

Objectives
• Describe differences in cancer survival across
European countries
• Discuss contributing factors for interpreting survival
differences
– Macroeconomic indicators
– Quality of care/pattern of care
DATA: population-based cancer registries
EUROCARE 5
21 million cancer diagnoses
116 Cancer Registries
30 European countries

EUROCARE 5
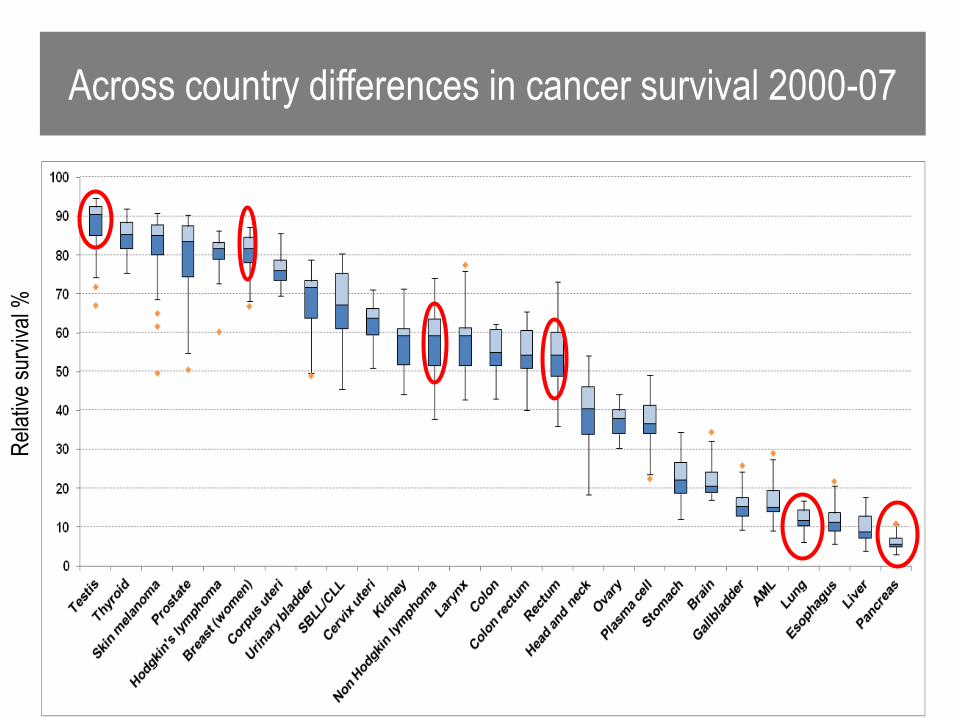
Across country differences in cancer survival 2000-07
Rel
ativ
e su
rviv
al %

0 20 40 60 80 100
Denmark
Finland
Iceland
Norway
Sweden
Ireland
UK-England
UK-Northern Ireland
UK-Scotland
UK-Wales
Austria
Belgium
France
Germany
Switzerland
The Netherlands
Croatia
Italy
Malta
Portugal
Slovenia
Spain
Bulgaria
Czech Rep
Estonia
Latvia
Lithuania
Poland
Slovakia
European Average
0 20 40 60 80 100
Denmark
Finland
Iceland
Norway
Sweden
Ireland
UK-England
UK-Northern Ireland
UK-Scotland
UK-Wales
Austria
Belgium
France
Germany
Switzerland
The Netherlands
Croatia
Italy
Malta
Portugal
Slovenia
Spain
Bulgaria
Czech Rep
Estonia
Latvia
Lithuania
Poland
Slovakia
European Average
Rectal
Five-year relative survival 2000-07Breast 0 20 40 60 80 100
Denmark
Finland
Iceland
Norway
Sweden
Ireland
UK-England
UK-Northern Ireland
UK-Scotland
UK-Wales
Austria
Belgium
France
Germany
Switzerland
The Netherlands
Croatia
Italy
Malta
Portugal
Slovenia
Spain
Bulgaria
Czech Rep
Estonia
Latvia
Lithuania
Poland
Slovakia
European Average
NH lymphoma

Five-year survival for all cancers combined
diagnosed in 2000–07 in children, by country

Time trend in age and case-mix standardised
5-year relative survival by European region and gender
Source: Baili et al, EJC, 2015

Macro economic
indicators

Relationship between gross domestic product (GDP), expressed
as parity purchasing power (PPP, US$), and the 5-year age- and cancer
site-adjusted relative survival in the EUROCARE-3 countries
GDP (PPP,US$)Source: Micheli at al, Annals of Oncology, 2003
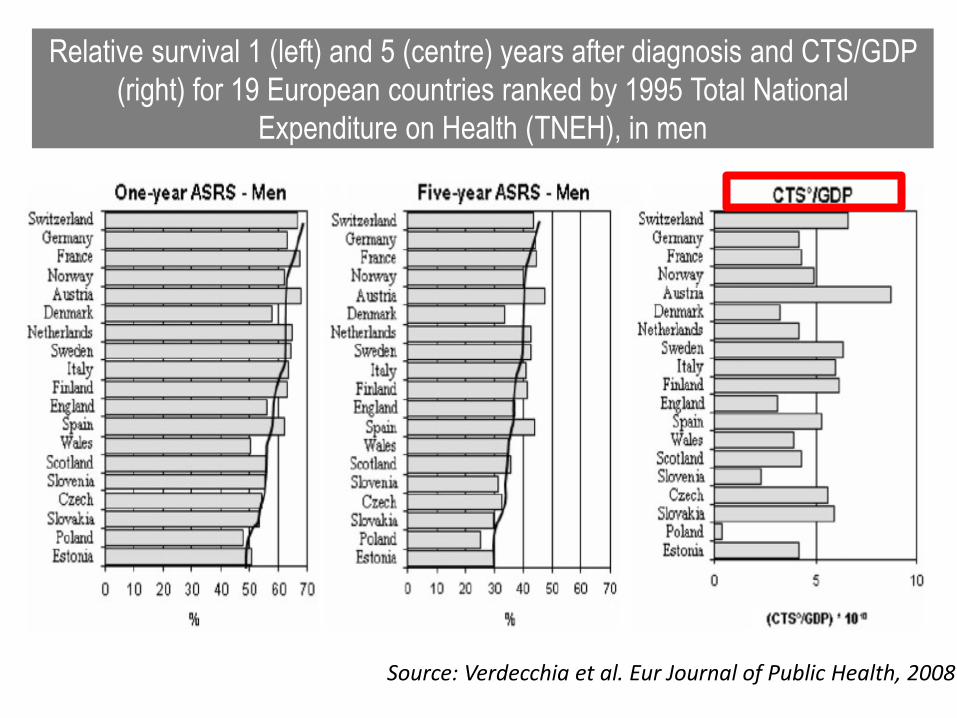
Relative survival 1 (left) and 5 (centre) years after diagnosis and CTS/GDP
(right) for 19 European countries ranked by 1995 Total National
Expenditure on Health (TNEH), in men
Source: Verdecchia et al. Eur Journal of Public Health, 2008

Five-year age- and case-mix-standardised relative survival
for all cases diagnosed in 2000–2007 ranked by Total NationalExpenditure on Health (TNEH)
Source: Baili et al, EJC, 2015

• all cancer survival differences between richer
countries mainly depend on CTS/GDP (index of
technological investment in cancer in relation to
available prosperity)
• survival differences between poorer countries
mainly depend on TNEH— general level of health
investment
Source: Verdecchia et al. Eur Journal of Public Health, 2008

Relationship between total national expenditure on health (TNEH),
(US$PPP), and the 5-year age-adjusted relative all-cancer survival (%)
(period 2000-2002) by country and national health-care system organization
National health services vs social security system
Survival : 55.2 vs 55.6
TNEH: 2500 US$PPP vs 3000 US$PPP
Source: Gatta et al, JNCI, No. 46, 2013

Quality of care

www.rarecarenet.eu

198 rare cancers (incidence rate < 6 per 100,000)
22% of all new cancer in Europe
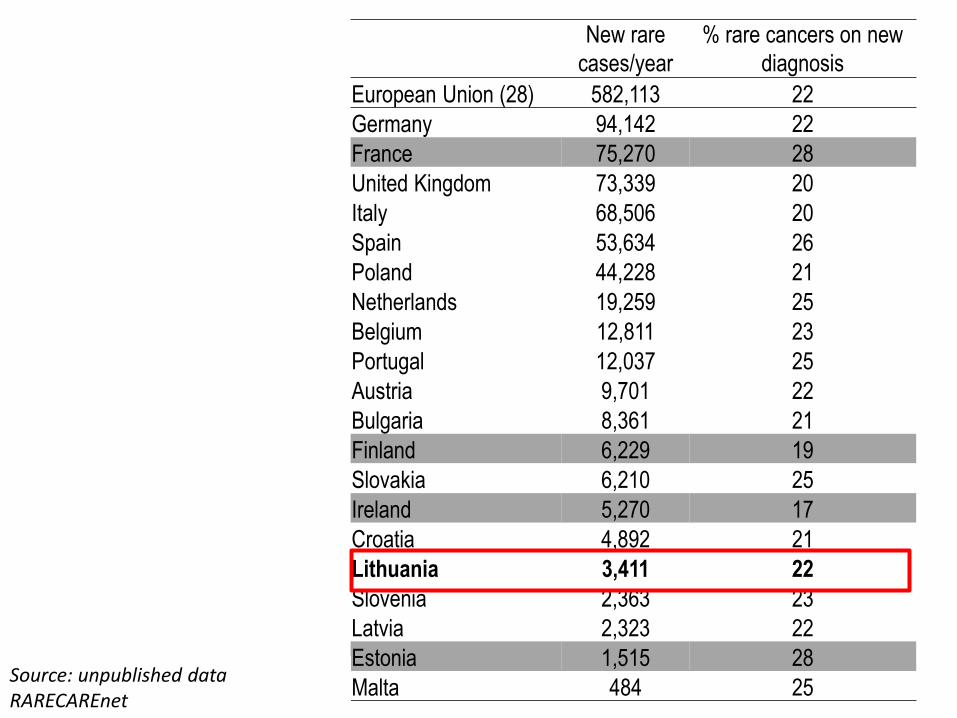
New rare
cases/year
% rare cancers on new
diagnosis
European Union (28) 582,113 22
Germany 94,142 22
France 75,270 28
United Kingdom 73,339 20
Italy 68,506 20
Spain 53,634 26
Poland 44,228 21
Netherlands 19,259 25
Belgium 12,811 23
Portugal 12,037 25
Austria 9,701 22
Bulgaria 8,361 21
Finland 6,229 19
Slovakia 6,210 25
Ireland 5,270 17
Croatia 4,892 21
Lithuania 3,411 22
Slovenia 2,363 23
Latvia 2,323 22
Estonia 1,515 28
Malta 484 25Source: unpublished data RARECAREnet

Time variation in 5 year relative survival 1999-2007 (age standardised)
%
Source: unpublished data RARECAREnet
0
10
20
30
40
50
60
70
80
1999-2001 2002-2004 2005-2007
rare
common

OBJECTIVES1. to collect and disseminate information on health care pathways for rare cancers and on updated
epidemiological indicators
2.to identify the qualification criteria for centres of expertise for rare cancer
3. to identify and disseminate information on centres of expertise (CoE) for rare cancers
4. to produce and disseminate information on diagnosis and management of rare cancer
5. to develop a clinical data base on very rare cancer (situations for which clinical trials are difficult to perform)
6. to develop and disseminate information for patients and patients’ association

RARE CANCERS
Rare skin cancers including non
cutaneous melanoma
Thoracic - rare cancers
Male genital and urogenital rare
Female genital rare
Neuroendocrine tumours
Tumours of the endocrine organs
Central Nervous System tumours
Sarcomas
Digestive rare
Haematological
Head and neck cancers
Pediatric cancers
198 rare cancers General criteria for CoE
Cancer specific criteria
-Soft tissue sarcoma
-Head and neck cancers
- Neuroendocrine tumours
-Testicular cancers

Evidenced based

European experience

Country level experience
Germany
The Netherland
UK
France
Belgium

European Society Medical Oncology
European Society for Radiation oncology
European Society of Surgical Oncology
European Society of Pathology
European association of head and neck cancers
European neuroendocrine tumor society
European association of urology
ESMO working group on sarcoma
European Organisation for Research and Treatment of Cancer
Organisation European Cancer Institutes
Joint action on rare diseases
European School of Oncology
WHO?

HOW?1. Consensus meeting on quality criteria for Centres of expertise
2. High resolution studies with population-based cancer registries
3. Consensus meeting for the definitive validation of the list of criteria

High resolution studiesYears of diagnosis: 2009-2011
* 10 cancer registries
GEP-NET sarcomas of
limbs
head and neck
cancers(larynx, oral cavity,
oropharynx,hypopharynx)
testicular
cancers
Total
Ireland 334 122 1,330 506 2,293
Netherlands 1,381 722 6,382 2,135 10,620
Bulgary 141 252 978 564 1,935
Finland _ 152 _ 385 537
Belgium 733 280 _ 615 1,628
Slovenia _ 63 219 198 480
Italy* _ 332 646 976
Head and neck
cancers

1. Timely start of treatment
• Time to start treatment (time between definitive pathological diagnosis and beginning of surgery or radiotherapy)
• Time in starting postoperative radiotherapy or concomitant chemo-radiotherapy
2. Stage at diagnosis
3. Adherence to clinical guidelines (ESMO guidelines for squamous cell carcinoma of the head and neck)
• Proportion of patients with early stage I and II referred for either surgery or radiotherapy
• Proportion of patients with locally advanced stage III and IV referred for surgery plus postoperative radiotherapy or post-operative chemo-radiotherapy or combined concomitant chemoradiation
4. Quality of surgery and radiotherapy
• Complete tumour resection (histological verification of tumour free margins after surgery)
• Readmission, re operation within 30 days from main surgery
• Grade 3 or more late toxicities (more than 3 months after radiotherapy)
• % of patients receiving intensity-modulated radiation therapy (IMRT) vs % receiving 3D conformal
radiation therapy
• All type of surgery should be available (CoE should ensure, when appropriate, minimal invasive surgery). Reconstructive surgery is very important too
5. Quality of pathology reports after surgery
• Proportion of pathology reports on cancer resections with a full set of core data items recorded (site and laterality of the carcinoma, maximum diameter of tumour, maximum depth of invasion, histological type of carcinoma, degree of differentiation (grade), pattern of invasion, lymphnode involvement)
6. Involvement in clinical-translational research
7. Availability of formalised multidisciplinary decision (with member experts on head and neck cancers)
Head and neck cancers

Across country differences in cancer survival 2000-07
Rel
ativ
e su
rviv
al %

Time to start treatment From histological verification to treatment (radiotherapy or surgery)
< 1 month > 1 month Number
Ireland 39% 61% 1,159
Netherlands 37% 63% 5,186
Slovenia 40% 60% 205
Italy 56% 44% 672
Breast in Italy * Number %
< 15 days 2,515 66
16-31 days 602 16
>1 month 655 17
unknown 19 1
Total 3,791 100
*data kindly provided by the Italian high resolution study on breast, P. Minicozzi
Head and neck cancers

What matter? (1)
TreatmentIreland Slovenia Netherlands
> 1month > 1 month > 1month
N % N % N %
surgery 227 32 14 11 1,572 48
radiotherapy 480 68 110 89 1,686 52
Total 706 100 124 100 3,258 100
Time to start treatment
Head and neck cancers

hospital volume cases/year
<20 20-50 >100
n % n % n %
> 1 monthlarynx 71 54% 101 65% 166 78%
other sites 92 45% 147 55% 129 68%
< 1 monthlarynx 60 45% 54 35% 46 22%
other sites 112 85% 119 77% 60 28%
Advanced stage 39% 49% 59%
Time to start treatment
Head and neck cancers
What matter? (2)
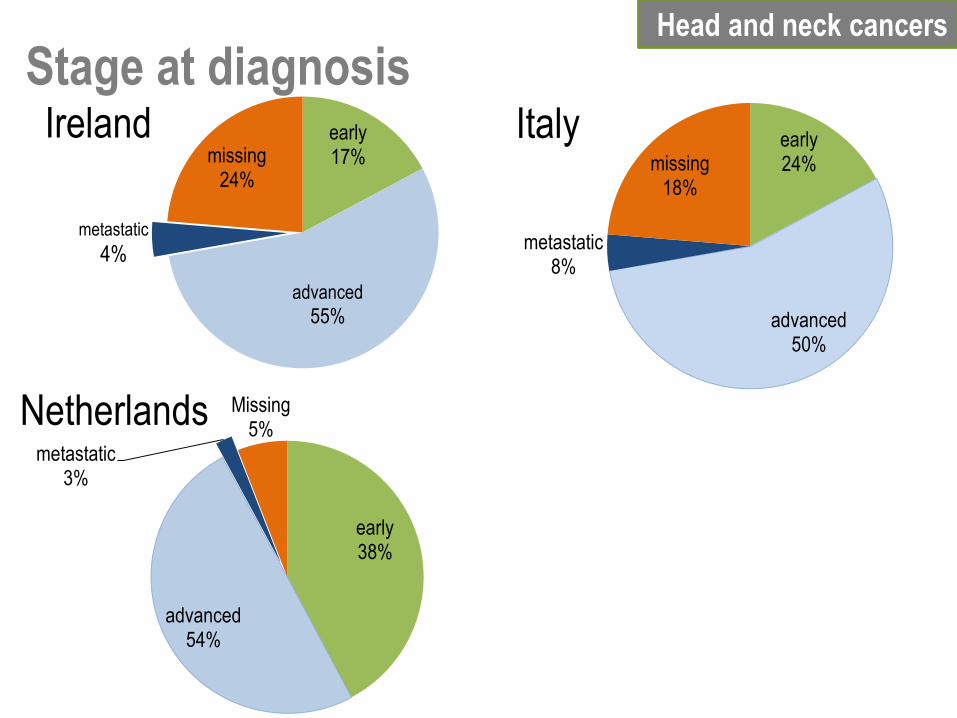
Head and neck cancers
Stage at diagnosisearly24%
advanced50%
metastatic8%
missing18%
Italy
early38%
advanced54%
metastatic3%
Missing5%
Netherlands
early17%
advanced
55%
metastatic
4%
missing24%
Ireland

http://makesensecampaign.eu/

Head and neck cancers
Quality of pathological report
Ireland* Slovenia Netherlands* Italy
N % N % N % N %
site and laterality of the carcinoma 50 100 64 100 120 83 399 91
histological type of carcinoma 50 100 64 100 133 92 404 92
degree of differentiation (grade) 44 88 61 95 105 73 394 90
lymphnode involvement (cases N+) 11 100 24 92 34 24 101 78
margin status 50 100 50 78 106 74 363 83
maximum diameter of tumour 50 100 36 56 99 69 335 76
maximum depth of invasion 0 0 35 55 86 60 233 53
pattern of invasion 0 0 4 6 85 59 269 61
*Data on a sample of cases
Slovenia Netherlands Italy
N % N % N %
All information 28 31 42 27 154 35
Hospital volume

Netherlands
0
20
40
60
80
100
120
140
160
180
200
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35
Volume of radiotherapy treatment
0
20
40
60
80
100
120
1 4 7 10 13 16 19 22 25 28 31 34 37 40 43 46 49 52 55 58 61 64 67 70 73 76 79
Volume of surgery
0
20
40
60
80
100
120
140
1 2 3 4 5 6 7 8 9 10111213141516171819202122232425262728
Volume of radiotherapy treatment
0
10
20
30
40
50
60
70
1 6
11
16
21
26
31
36
41
46
51
56
61
66
71
76
81
86
91
96
10
1
10
6
11
1Volume of surgery
Belgium

Head and neck cancers 5-year relative survival
in selected countries, 2000-2007

Centralisation?
Centres of Expertise?
European reference Network?
Imagine if the best specialists
from across Europe could join
their efforts to tackle complex
or rare medical conditions
that require highly specialised
healthcare and a concentration
of knowledge and resources.
That's the purpose of the
European Reference
Networks and it's becoming a
reality.
http://ec.europa.eu/health/ern/policy/index_en.htm

Conclusions
• We do have good data to support health care organisation
• Population based cancer registries are important for planning and monitoring cancer control strategies

Thank you to all cancer registries participating in EUROCARE
and RARECAREnet and to you all for the attention!
The RARECAREnet project is supported by the Executive Agency for Health and Consumers (EAHC) of the European Commision






























