Embed Size (px)
Citation preview
November 25, 2013
Intermountain Med Staff NewsDecember 12, 2013
Dear Colleagues,
We believe the most important thing we can do to improve the relationship between Intermountain and physicians is communicate, openly and honestly. With that in mind, please see the following Med Staff News update, which has important information for you and your practice.
Please let us know if you think this update is a worthwhile effort. If there is something you want more information about, let us know. If you have questions, comments or concerns, don’t hesitate to contact either of us.
Thank you for all that you do in support of Intermountain Healthcare and patients you serve.
Sincerely,
Brent Wallace, MD Susan DuBois Chief Medical Officer Assistant Vice PresidentIntermountain Healthcare Physician Relations and [email protected] Medical Affairs (801) 442-3866 [email protected] (801) 442-2840
Table of Contents
Cerner Update for Physicians
Shared Accountability
Clinical Program and Service Line Updates
Cardiovascular
Behavioral Health
Intensive Medicine
Pediatric
Primary Care
Women and Newborn
Influenza
Intermountain Labs
Screenings vs. Diagnostics
SelectHealth UpdateDischarge Review Program
M-Tech
Regulatory Compliance New ICD-10 Codes
CME Program Update
New CMS Payments Program
Physician-Owned Entities
Fitness Feature Sitting is the New Smoking
2Continued on next page
INTERMOUNTAIN ANNOUNCED IN OCTOBER THAT IT SELECTED CERNER AS A NEW EMR
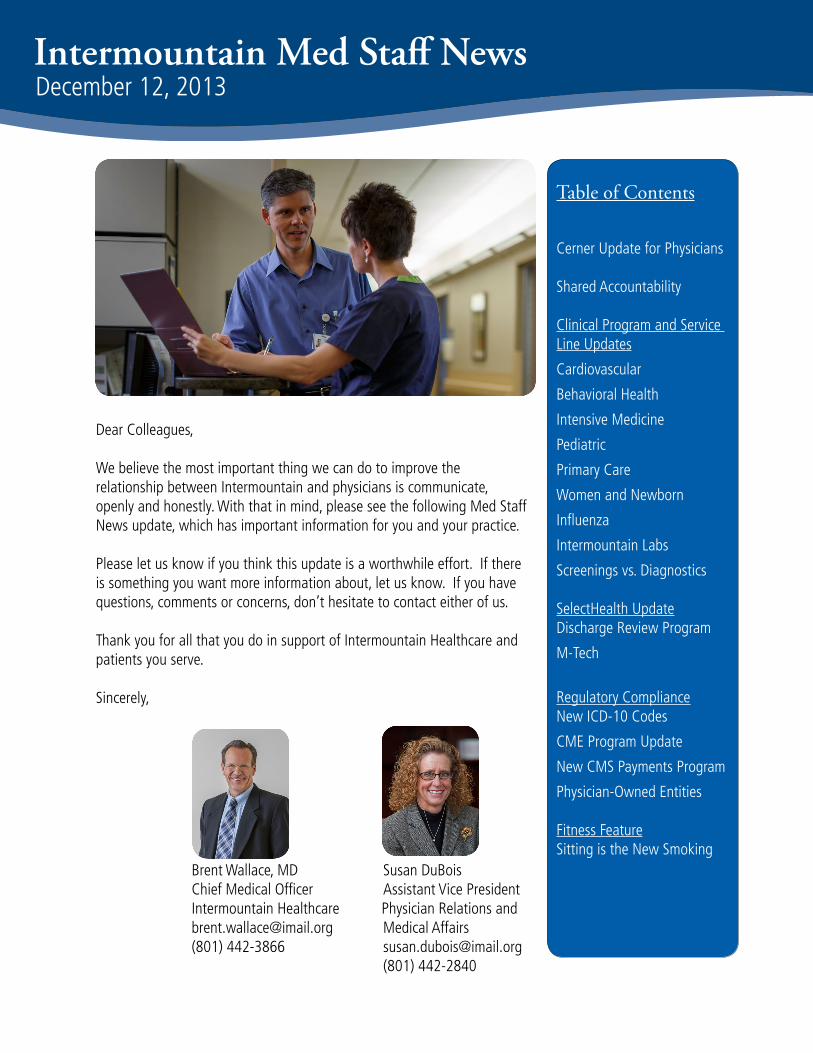
GOVERNANCE STRUCTUREThe Executive Committee, led by Mark Briesacher, MD, began meeting the first week of December and is responsible for providing governance for all aspects of the relationship between Intermountain and Cerner in a timely and efficient manner, including the following work:
ITERATIVE DESIGN PROCESSIn October, teams from Cerner performed observation walkthroughs in many Intermountain hospitals and clinics to interview leaders and staff about clinical and revenue cycle processes, workflows and clinician/user experiences.
Following these visits, Cerner teams began planning how to build the Intermountain “Model System,” a working Cerner prototype that uses Intermountain’s data and processes to show functionality from beginning to end. It allows Intermountain teams to view the most recent improvements and to provide real-world feedback to Cerner.
Using an iterative design process, Intermountain’s Model System will be continually tested and refined throughout the configuration process. During this time, Intermountain and Cerner teams will be able to develop features, review changes and confirm clinical, practice management and revenue cycle requirements on a continual basis. AFFILIATED PHySICIAN STRATEGyOne early focus is on our affiliated physician partners. As key members of our hospital medical staffs and SelectHealth insurance panels, we will work with Cerner to provide different levels of integration with each of our affiliated physician practices. Early work has focused on putting a leadership team together for this work and answering questions from affiliated clinics and practices.
DATA MIGRATION STRATEGyIntermountain has begun working with Cerner on the data migration strategy, and teams of engineers and medical informaticists are evaluating options for bringing data into the new system. The goal is to make the data transition as easy as possible for clinicians, and Intermountain-Cerner project teams and leaders will keep clinicians up-to-date on this important work.
If you have questions or comments about the Cerner project, please contact Mark Briesacher, MD at [email protected], or Craig Jacobsen, AVP, Information Systems, at [email protected].
Cerner UpdaTe for physiCians
Executive CommitteeChaired by Dr. Mark Briesacher
Model System Steering CommitteeConfiguration and implementation
of Cerner’s HIT platform
Affiliated Physicians Strategy Group
Integration of our HIT with our affiliated physicians and clinics
Innovation Steering CommitteeCo-development and innovation
of our HIT
Cerner Update

3Continued on next page
shared accountability Update
intermountain’s shared accountability strategyShared Accountability—Intermountain Healthcare’s approach to providing better care, improving population health, and keeping costs sustainable in the nation’s changing healthcare environment—is moving from the development stage to implementation in many arenas. Most of the Shared Accountability strategy is on track for full implementation by 2016.
Shared Accountability’s three key strategies include: redesigning care, engaging patients and physicians, and aligning financial incentives. Here is a summary of what is happening in each of these areas:
REDESIGNING CAREIntermountain continues to apply evidence-based care standards to define the right care for patients. Current focuses include: 1) A Utilization Management strategic plan, and 2) Integrated Care Management (ICM) pilot programs coordinating high-risk patient needs across providers and settings. A new Assistant Vice President for Integrated Care Management, Teresa Garrett, started in December. PHySICIAN AND PATIENT ENGAGEMENTThe Medical Group and SelectHealth continue to roll out Personalized Primary Care (with Intermountain Medical Group clinics) and Advanced Primary Care (with affiliated physician clinics). This is Intermountain’s version of the patient-centered “Medical Home” concept for care coordination services for chronic medical conditions and high-risk patients. All Medical Group clinics will be participating in Personalized Primary Care by 2014. Current objectives include Total Cost of Care measurement, high-risk patients, and children with special needs.
Pilots of three Shared Decision-Making tools (EMMI Solutions, Health Dialog, and Archimedes IndiGO) are moving forward at select Medical Group clinics with plans for future expansion.
Work is moving forward to develop shared-risk networks with Intermountain Healthcare and SelectHealth. A health benefit design strategic plan was approved this month. Benefit design addresses the way health benefits are structured and used by subscribers. The plan addresses health plan product design, employer/employee compacts, health promotion and wellness structure, disease-management requirements, and value-based benefit design.
The Health Education and Health Literacy Guidance Council is streamlining and improving patient education materials. The council is developing metrics to evaluate the impact of standardized patient education, starting with pre-diabetes prevention and diabetes management.

4Continued on next page
ALIGNING FINANCIAL INCENTIVESHealthcare is gradually moving from a fee-for-service environment, which incentivizes volumes, to a population health management environment that rewards both productivity and best outcomes for groups of individuals. Over time, financial risk will move from health plans to healthcare systems. Intermountain is working with physicians and other stakeholders to develop a model to bear and manage risk in this environment.
Intermountain is providing more transparency for patients through the development of system pricing models. Pharmacy and imaging pricing strategy and DRG-based rate proposals were approved earlier this year. Intermountain is negotiating with payers to transition to DRG contracts and streamline reimbursements.
A physician payment model beta test has launched with a limited number of Medical Group and affiliated physician clinics and a subset of patients. The model pays for care provided, plus a significant performance-based payment for meeting quality, service, and cost goals. The beta will be in data-gathering mode until summer 2014, with the at-risk payment portion scheduled to go live late summer 2014. To provide more transparency for physicians, analytics tools have been created supporting the physician payment beta. This will provide physicians with actionable data to improve patient care.
Intermountain and SelectHealth are finishing our first full year administering shared-risk Medicare and Medicaid products. SelectHealth Community Care, our managed care Medicaid plan, covers medical and pharmacy benefits to about 77,000 members. SelectHealth Advantage, our Medicare Advantage product, covers over 4,300 members. Under these plans:
• Intermountain’s delivery system bears the risk • Governmental entities establish non-negotiable payment rates and have significant additional compliance and reporting requirements• These populations are generally high-risk or “at-risk” with social, cultural, and economic needs that are quite different from commercially insured populations
In 2014, we will develop and implement formal structures to manage the care of these members in an integrated manner across the continuum of care.
If you have questions, please contact Brent Wallace, MD, at [email protected].
shared accountability Update
SHARED ACCOUNTABILITy UPDATE – continued

Clinical Program and Service Line Updates
5Continued on next page
The Cardiovascular Clinical Program (CVCP) board goal is to improve best practices for patients who are at risk for heart failure. This is a three-year board goal, and already we’ve achieved this year’s portion by implementing inpatient heart failure identification and risk stratification notifications, along with many other enhancements. We’ll continue to make significant improvements across the continuum of care of these patients. Details can be viewed at https://my.intermountain.net/clinical/cv/Pages/Home.aspx.
If you have any questions, please contact Donald Lappe, MD, at [email protected], orColleen Roberts at [email protected].
Cardiovascular Clinical program

Clinical Program and Service Line Updates
6Continued on next page
Behavioral health Clinical programThe Fifth Edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) was released by the American Psychiatric Association’s Annual meeting in May 2013 and replaces the DXM-IV-TR.
A few new diagnoses were added and others moved to new groupings. More information can be obtained from www.dsm5.org. The Behavioral Health Clinical Program has recommended that Intermountain providers begin to use the new DSM-5 beginning January 1, 2014.
If you have any questions, please contact Mark Foote, MD, at [email protected], or Carolyn Tometich at [email protected].

Clinical Program and Service Line Updates
7Continued on next page
intensive Medicine Clinical programThe Intensive Medicine Clinical Program 2013 Board Goal pursued the hypothesis that higher reliable use of order sets could improve compliance with care process models by building into the orders defaults to the appropriate care processes. We selected three diagnosis-specific order sets approved for enterprise-wide use:
• Severe sepsis• Pneumonia• Ischemic stroke
Our goal was to achieve utilization of the identified order sets 30% of the time for patients admitted with sepsis, pneumonia, or ischemic stroke. Between July 1 and November 25, 2013, the order sets were used 1,608 times achieving a rate of 50% for the targeted population.
This process was an important confirmation that the best way to create safe, effective and usable order sets is to evolve them as they are used in the clinical environment. The order sets were created by experts in the knowledge domain and reviewed by various committees including pharmacy, compliance, lab, revenue cycle and clinical programs. This initial review process worked well, but it was only when the order sets were used in the real clinical environment that we got the feedback needed to make them even safer, usable, acceptable and effective. To capitalize on this experience, we are now encouraging physicians in all departments to use the available CPOE order sets in HELP2 and give feedback for further improvement.
Soon, order sets will be programed into Cerner and modeled using the current HELP2 CPOE order set content. The better and more robust the HELP2 order set, the better the Cerner order set will be. When Cerner is installed, all orders will be electronically generated and handwritten and preprinted orders will disappear. We have the opportunity now to make the order set content robust, acceptable and effective by getting as much experience with them now in the HELP2 modules.
For those who are not familiar with access to or use of the order sets, access this self-learning teaching slide set by selecting “order sets” on the left hand menu, and pulling down the screen until you see a PowerPoint presentation called “Physician Orientation to Order Sets.”
If you have any questions, please contact Terry Clemmer, MD, at [email protected].

Clinical Program and Service Line Updates
8Continued on next page
pediatric Clinical programRespiratory season is knocking on our doors now. The numbers of positive viral tests are increasing. If you are interested in seeing our recently updated GermWatch content, please go to www.germwatch.org. Here you will find information about what viruses are circulating — including great information you can use with your patients and their parents.
A word about collection of specimens for viral respiratory testing — we have for years collected specimens via NP suctioning and this was the preferred method until flocked swabs became an option. The microbiology supervisor at Primary Children’s Hospital states the advantage of flocked swabs over suction is a better amount of cell recovery, since suction tends to contain lots of respiratory mucous. Flocked swabs collect less mucous initially and the UTM or M4 that they are transported in helps dissolve the mucous. Of course better cell recovery means a higher chance of detecting virus if it is there. The swabs are also less invasive and quicker to collect.
If you have any questions, please contact Edward Clark, MD, at [email protected], or Carolyn Reynolds at [email protected].

Clinical Program and Service Line Updates
9Continued on next page
primary Care Clinical programThe Primary Care Clinical Program launched an Affiliate Guidance Council to:
• Describe the current environment at Intermountain with regard to Shared Accountability initiatives • Provide an avenue for communication with affiliated practices that will improve the Clinical Program’s ability to support affiliated practices • Engage affiliated practices in efforts to improve health and reduce waste
The group meets every other month. As a part of these meetings, we have discussed a variety of clinical measures including the diabetes and asthma bundles which are required for HEDIS and the SelectHealth Primary Care Incentive.
The Primary Care Clinical Program has recently rolled out two new care process models: • Eating Disorders • Lifestyle and Weight Management In collaboration with the University of Utah, both Intermountain and affiliated providers will be participating in the evaluation of the Asthma Tracker. Providers interested in participating in the evaluation should contact Flory Nikoy at [email protected] or Bernhard Fassl at [email protected].
If you have any questions, please contact Wayne Cannon, MD, at [email protected], or Sharon Hamilton at [email protected].
Clinical Program and Service Line Updates
10Continued on next page
Women and newborn Clinical programBoth CMS and the Joint Commission have identified inappropriate, early elective delivery <39 weeks as a nationally-reported measure. CMS also has delineated appropriate medical indications for delivery prior to 39 weeks, e.g., preeclampsia or diabetes.
The Women and Newborn Clinical Program believes that more stringent adherence to guidelines will be enforced by CMS in the near future and that the Joint Commission may link hospital accreditation to complying with guidelines that proscribe inappropriate, early delivery <39 weeks. Intermountain started reporting inappropriate, early elective deliveries to CMS in January 2013, and the information is a matter of public record. For these reasons, Intermountain Healthcare’s Women and Newborn Clinical Program is recommending that all facilities and providers adhere to CMS guidelines defining appropriate early deliveries <39 weeks. Moreover, the Clinical Program can no longer accept “corrections” for early deliveries that do not meet CMS guidelines. To assist with this process, we have updated the Intermountain-allowed medical indications for delivery to meet the CMS indications.
The above notwithstanding, the Clinical Program recognizes that a few patients or circumstances not defined by CMS will need early delivery for unusual reasons. We are implementing a program to accurately document the medical rationale for these infrequent early deliveries that fall outside of CMS guidelines. All such deliveries will require regional MFM approval, and the MFM physician will document the medical rationale in the chart. MFM consultation is available in each region.
Also, beginning in January 2014, hospitals with more than 1,100 deliveries a year will begin reporting to the Joint Commission along with the other perinatal variables as part of the Perinatal Core Measure Set. Many measures will require accurate provider documentation. More information will follow on this requirement early next year. The Perinatal Core Measure Set variables are listed below. For more details on these variables, click here.
PC-01 Elective DeliveryPC-02 Cesarean section rate in low-risk first birthsPC-03 Antenatal steroid administrationPC-04 Health care-associated blood stream infections in newbornsPC-05 Exclusion breast milk feeding
If you have any questions, please contact Ware Branch, MD, at [email protected], or Teri Kiehn at [email protected].

Clinical Program and Service Line Updates
11Continued on next page
The influenza season is now upon us with 86 documented cases of flu confirmed by Intermountain laboratories as of December 12. Twelve of these patients have been hospitalized, with six in an ICU setting. All regions in the system and all age groups have been affected. Most of the diagnosed cases to date have been Influenza A (H1N1). Connect to GermWatch for up to date information on respiratory viruses throughout the year. All strains of influenza to date have been sensitive to oseltamivir, of which we have an abundant supply.
New for this season is the availability at some sites of a new CLIA-waived rapid influenza test, the BD Veritor. This test has a sensitivity of roughly 90% for Influenza A strains (including H1N1), and a sensitivity of roughly 80% for Influenza B strains. Specificity for this test is 98% for both A and B strains. The sensitivity of this test, though good, is much less than PCR-based techniques in which sensitivity is 99%. In cases where there is a strong suspicion of Influenza or in patients at high risk of complications, you should follow up a negative rapid test with a more reliable PCR-based test.
Vaccination remains the single best way to prevent influenza acquisition and transmission. Since the advent of mandatory influenza vaccination at Intermountain, we have experienced very high rates of vaccination by Intermountain physicians and staff. Individuals who have received medical or religious exemption from vaccination are required to wear a mask while in clinical venues during periods of high influenza activity in order to prevent nosocomial transmission of influenza to our vulnerable patients.
If you have any questions, please contact Douglas L. Smith, MD, at [email protected].
influenza Update

Clinical Program and Service Line Updates
12Continued on next page
NOTICE TO EVERyONE WHO ORDERS CHEMISTRy TESTS:All laboratories throughout Intermountain Healthcare will change from Ortho VITROS to Abbott ARCHI-TECT chemistry analyzers beginning in December 2013. Because of the new instruments, some tests will have new reference ranges and the laboratories’ test menus will change slightly.
A summary of what will change• Reference ranges for LDH and lipase changed
drastically throughout Intermountain Healthcare on Wednesday, December 4, 2013. The new reference ranges for LDH and lipase will be 55% and 75% lower, respectively, than current ranges.
• Reference ranges for AST, CO2, phosphorus, and TIBC will change slightly as of December 4. Reference range changes will be noted on patient reports.
• Chemistry analyzers will be exchanged during December, January, and February.
• Conjugated Bilirubin, Unconjugated Bilirubin, and Neonatal Bilirubin will be replaced by Direct, Indirect, and Total Bilirubin. Neonatal Bilirubin Fractionation will be discontinued. (Note: Direct and Conjugated Bilirubin are not identical.)
• Total Iron Binding Capacity (TIBC) will be calculated from transferrin.• The same CRP test will apply to all ages. Neonatal CRP will be discontinued.
How to order lab tests:
Before the changeover• Order the same tests you have been ordering. The Lab will keep track of which instrument is in use
at which site.
After the changeover (the Lab will announce when it is finished)• Order Direct Bilirubin instead of Conjugated Bilirubin. • Order Total Bilirubin or Bilirubin Fractionation for all ages of patients including neonates. • Order CMP, HFP, and CRP for all ages of patients. As always, order high-sensitivity CRP (hsCRP)
only for cardiovascular risk assessment in adults.
If you have questions or need further information, contact your hospital’s laboratory director, or Sarah Ilstrup, MD, at 801-507-2146 or [email protected], Phil Bach, PhD, at 801-507-2287, 801-662-2180, or [email protected], or Brian Davis, MT(ASCP), at 801-357-4180 or [email protected], or contact Steve Mikkelsen at [email protected].
intermountain Laboratories prepare for Change

Clinical Program and Service Line Updates
13Continued on next page
The Affordable Care Act requires that Medicare and private plans provide all US Preventive Services Task Force (USPSTF) recommended preventive services with no cost sharing, including screenings (e.g., colorectal cancer screening and breast cancer mammography). According to the ICD-9-CM Official Guidelines for Coding and Reporting and the Medicare Claims Processing manual, a screening is the testing for disease or disease precursors in seemingly well individuals, so that early detection and treatment can be provided for those who test positive for the disease.
The testing of a person to rule out or confirm a suspected diagnosis is not a screening. It is a diagnostic examination. Diagnostic procedures do have cost sharing. Patients with signs or symptoms should not be scheduled as screenings and should be informed that they may have a co-pay.
Some Intermountain patients have understood that their procedures will be billed as screenings although they have documented signs and/or symptoms. Health Information Management
(HIM) must code these procedures as diagnostic procedures, not screenings, based on the documentation of a sign and/or symptom. These patients are filing complaints because they feel that Intermountain is billing them unjustly.
Please inform your patients that if they have signs or symptoms and will be receiving a test to rule out or confirm the diagnosis, they may be sharing the cost of the procedure through a copayment or coinsurance.
Furthermore, HIM will always code the testing for disease or disease precursors in seemingly well individuals as a screening. If a finding (e.g., polyp, diverticulosis, etc.) is detected by the screening, it will be assigned as a secondary diagnosis code. If an intervention is conducted during a screening, the CPT procedure code assigned by HIM will only change through the addition of a modifier. This modifier indicates that the exam began as a screening, but required intervention.
If you have any questions, please contact Neil Nokes, PhD, MPH/HAS, at [email protected].
screenings vs. diagnostic examinations

14Continued on next page
Beginning January 1, 2014, SelectHealth will launch a Readmission Avoidance program for SelectHealth Advantage (Medicare) and SelectHealth Community Care (Medicaid) patients who are discharged from an inpatient facility. Upon discharge, all SelectHealth Medicare or Medicaid patients will be reviewed by a SelectHealth care manager to determine their risk of readmission, using LACE criteria.
Patients found to have greater than 10% risk of readmission will receive a call from a SelectHealth care manager to assess whether they have the resources to manage their illness and avoid a readmission. If the SelectHealth care manager determines that the patient’s resources are not optimal, a nurse home visit will be completed through a request from SelectHealth by Intermountain Home Care to address concerns and provide education for the patient. Information obtained through the home visit then will be shared with SelectHealth Care Management and the patient’s PCP to help the patient and the provider team manage the patient’s condition(s).
The Readmission Avoidance Home Visit is primarily for the purpose of care management, and it will be separate from any other home health services that have been ordered by a physician. The request for these services will originate from the SelectHealth Care Management team, and it will be coordinated with other case management initiatives within Intermountain and the patient’s primary care provider. The visit will be for care management purposes to prevent readmissions, and it will not include an assessment to diagnose or assess new conditions. It is also not intended to replace any care provided by physicians, home health, or other providers.
If you have questions or concerns about the SelectHealth Readmission Avoidance Quality Improvement Plan or an associated home visit for your SelectHealth Advantage or SelectHealth Community Care patient, please call the SelectHealth Care Management Manager at 801-442-7913. For general questions, please contact Dot Verbrugge, MD, at [email protected].
selecthealth readmission avoidance Quality improvement program
(SelectHealth Advantage Chronic Care Improvement Program)
selecthealth Update

15Continued on next page
M-Tech is SelectHealth’s formal process for reviewing emerging health care technologies (procedures, devices, tests and biologics) for the purpose of establishing coverage benefits. Existing technologies are, at times, also examined through this process. These determinations are then developed into published medical policies which outline coverage and any limitations to any specific technologies.
All SelectHealth medical policies and technology assessments can be viewed on our website. Go to www.selecthealth.org, click on the “Provider” tab (upper right corner), enter your log in information, click on “Policies and Procedures” (left side of page), click “Agree” to the terms and conditions and you will then be directed to the Policies & Procedures page.
The most recent technologies assessments topics with their completion dates, coverage determination and associated medical policies are as follows:
Subcutaneous Mastectomy for Fibrocystic Breast Disease (11-5-13)Cover in limited circumstances. Currently there is very little evidence to support the safety and efficacy of subcutaneous mastectomy for the treatment of fibrocystic breast disease. However, as this is typically and rarely used as a last resort treatment for patients experience intractable pain, the committee agreed to allow coverage in limited circumstances after conservative therapies have been exhausted. Medical policy is being drafted.
Oncotype DX Prostate for Prostate Cancer Outcome Prognosis (11-5-13)Deny as investigational. As no literature has been published to validate the accuracy of this test or establish the clinical utility, the M-Tech committee agreed to deny this as investigational. Medical policy is being drafted.
T:slim Insulin Pump (9-17-13)Cover as medically necessary. Though current evidence regarding the clinical utility of the t:slim pump is lacking, it is FDA cleared with predicate devices being other insulin devices suggesting it has demonstrated similar functionality and that its performance on health outcomes should be similar. See Medical Policy #133.
Hereditary Cancer Syndrome Multiplex Gene Panels (9-17-13)Cover genetic panels for oncology in limited circumstances. Current evidence suggests that BROCA, BreastNext and ColoNext are clinically relevant options in limited circumstances. Medical policy is being drafted.
selecthealth Technology assessment (M-Tech)
Ozurdex for Branch/Central Retinal Vein Occlusion and Uveitis (7-30-13)Cover according to FDA labeling. Current evidence suggests that Ozurdex treatment is a reasonable option for select patient populations consistent with their FDA approved indications. See Medical Policy #435.
Hypothermia for Neonatal Hypoxic-Ischemic Encephalopathy (7-30-13)Cover as medically necessary. Current evidence strongly supports the efficacy and safety of hypothermia therapy for hypoxic-ischemic encephalopathy in full term infants with the benefits far out weighing the risks. See Medical Policy #536.
Bronchial Thermoplasty for Asthma (7-30-13)Cover for in limited circumstances. Current evidence suggests that bronchial thermoplasty is a reasonable treatment option for patients who have failed conservative therapies. See Medical Policy #379.
Genetic Testing for Indeterminate Thyroid Biopsy (7-30-13)Cover as medically necessary. Current evidence tends to support the clinical validity and utility of the Veracyte Afirma Thyroid FNA analysis test. Further, given the lack of adequate evidence to draw conclusions regarding alternative tests used to assess indeterminate thyroid biopsies, at present, we further recommend denial of coverage of alternative genetic testing for indeterminate thyroid biopsies. See Medical Policy #538.
If you have any questions, please contact Ken Schaecher, MD, FACP, CPC, at [email protected].
selecthealth Update

16Continued on next page
Intermountain Healthcare is committed to adopting the use of ICD-10 codes by October 1, 2014 as mandated by the Centers for Medicare and Medicaid Services (CMS). Significant preparation for this adoption has been underway for many months, and you can expect to see many communications about ICD-10 and Intermountain’s adoption plans over the next year.
Support resources for physicians are being coordinated through the ICD-10 Implementation Team, Physician Relations, and the regional IPAS representatives. Depending on your role at Intermountain, you will hear directly from one of these groups in the near future.
Additional information about Intermountain’s ICD-10 adoption plans can be found on Intermountain.net and Intermountainphysician.org.
Providers may also contact their regional IPAS representatives for more information about Intermountain’s adoption of ICD-10.
If you have any questions, please contact Ken Marrott at [email protected].
regulatory Compliance

17Continued on next page
The Intermountain CME Program has a variety of newly announced live courses on their 2014 schedule. For more information, please check the schedule at https://intermountainphysician.org/intermountaincme/Pages/Course-Schedule.aspx.
It is likely you recently received an email from DOPL regarding mandatory opioid education due by January 31, 2016. Intermountain Healthcare will be releasing this training in 2014, so please watch this newsletter and the Intermountain CME website for more information.
If you have any questions, please contact SarahAnn Whitbeck at [email protected] or 801-442-3934.
Continuing Medical education
18Continued on next page
Open Payments is a CMS program to increase public awareness of financial relationships between healthcare industry and physicians by collecting and making public any payments or transfers of value between drug and device manufacturers and physicians or teaching hospitals. CMS requires drug and medical device manufacturers to collect information about payments or other transfers of value they make to physicians and teaching hospitals and submit the data annually to CMS. These data will be made publicly available and searchable.
The types of payments or transfers of value that are reportable by industry include: consulting fees, speaker fees, honoraria, gifts, entertainment, food and beverage, travel and lodging, education, research activities, charitable contributions, royalties or licenses, current or prospective ownership or investment interest and grants. Payments or transfers of value made both directly and indirectly through a third party will be reported, as will payments to a physician that are subsequently passed to a third party, such as a charity. CMS will allow for disputing reports prior to publication, so physicians should keep track of financial interactions with industry to ensure that the reports are accurate.
Physicians can sign up at go.cms.gov/openpayments to receive email updates about the program. Additional information is available at http://www4a.cms.gov/Regulations-and-Guidance/Legislation/National-Physician-Payment-Transparency-Program/Physicians.html. Education on the program that grants CME credit can be accessed at http://www.medscape.org/viewarticle/780900?src=cmsaca and http://www.medscape.org/viewarticle/807771.
If you have any questions, please contact Brad Nokes at [email protected].
CMs open payments (aka “sunshine act”)
regulatory Compliance
19
intermountain’s position on physician-owned entitiesIn March 2013, the OIG issued a “Special Fraud Alert: Physician-Owned Entities.” The Fraud Alert addresses physician-owned entities (POEs) that derive revenue from “selling, or arranging for the sale of, implantable medical devices” and “includes physician-owned entities that purport to design or manufacture, typically under contractual arrangements, their own medical devices or instrumentation.” The Fraud Alert suggests heightened concern about POEs, which the OIG describes as “inherently suspect under the anti-kickback statute.” Although the Fraud Alert specifically addresses implantable medical devices provided by physician-owned distributorships (PODs), the OIG noted that the same principles would apply to other types of POEs.
In response, Intermountain has adopted an updated policy regarding contracting with POEs. The basic position of the policy is quite simple: Intermountain will no longer contract with POEs, and will also be discontinuing purchases from existing POEs. Under the policy, a POE includes any entity that is owned in any part by a physician or an immediate family member of a physician. “Ownership” can mean shares, partnership units, bonds and other forms of debt, or royalties based on purchases by the ordering physician, and has no minimum percentage of ownership to trigger the prohibition. The policy, however, limits the scope of the prohibition to those POEs whose physician-owners are in a position to generate business for Intermountain, as determined by the Intermountain Anti-Kickback Statute Committee.
Under the policy, Intermountain recognizes that some products are unique to a particular manufacturer and do not have an equivalent produced by a non-POE. Consequently, an exception to the POE policy can be made for “disruptive technologies.” If you believe a product is unique and potentially groundbreaking from a therapeutic perspective, then contact your hospital administrator to begin the process to seek a disruptive technologies exemption for that product.
For more information, reference: OIG Special Fraud Alert: http://oig.hhs.gov/fraud/docs/alertsandbulletins/2013/POD_Special_Fraud_Alert.pdf
Physician Owned Entities Financial Arrangements Policy:https://kr.ihc.com/kr/Dcmnt?ncid=522595208&vrsn=&tfrm=default
Disruptive Technologies Exception Guideline:https://kr.ihc.com/kr/Dcmnt?ncid=522595212&vrsn=&tfrm=default
If you have any questions, please contact Brad Nokes at [email protected].
regulatory Compliance

20Continued on next page
sitting is the new smoking
By: Liz Joy, MD, MPH We are fortunate in Utah to have the lowest smoking rate in the nation – 10.2% compared to the national rate of 20.4%. Likewise, the percentage of adults who report doing no physical activity or exercise (such as running, calisthenics, golf, gardening or walking) other than their regular job in the last 30 days was 19% in Utah, compared to a national average of 26%.
Despite these positives, the fact that nearly 1 in 5 Utah adults gets no regular exercise is concerning. This figure doesn’t take into account the number of hours many adults spend with their backsides firmly planted in a chair. It is estimated that the average US adult spends 7.7 hours a day sitting. Several long-term longitudinal cohort studies have found that time spent sitting (on average > 6 hours/day) is an independent risk factor for premature mortality from all causes. A paper published in The Lancet in July 2012 compared global deaths per year attributed to both smoking and sitting, and found them to be nearly equivalent.
Our nation’s first physical activity guidelines were published in 2008, and recommend that adults accumulate a minimum of 150 minutes/week of moderate intensity exercise, in addition to muscle strength training at least 2 times per week. However, given the research findings since the guidelines were published, the NEW “physical activity prescription” should be 150 minutes a week of moderate intensity activity in addition to activity throughout the day to avoid prolonged sitting. Physical activity has been shown time and time again to be a key (perhaps THE key) lifestyle attribute associated with improved health and longevity.
We need to assess physical activity like any other vital sign, and utilize resources such as the Intermountain Lifestyle and Weight Management Care Process Model, and the LiVe Well Program to help ourselves, our patients, and our families move more.
If you have any questions, please contact Liz Joy, MD, MPH, at [email protected].
“It is estimated that the average US adult spends 7.7 hours a day sitting.”
fitness feature by Liz Joy, MD, MPH