Embed Size (px)
Citation preview

American Journal of Medical Genetics 103:252±254 (2001)
Letter to the Editor
Intermediate Form of Ablepharon±MacrostomiaSyndrome With CNS Abnormalities
To the Editor:
Ablepharon±macrostomia syndrome (AMS) (MIM200110) is a rare condition comprising de®ciency ofthe eyelids, macrostomia, absence of lanugo at birth,redundant skin, and abnormalities of the nose, ears,and genitalia. There is considerable phenotypic overlapwith Barber-Say syndrome [Barber et al., 1982] (BSS),and it has been suggested that the two conditions maybe allelic [Mazzanti et al., 1998]. A boy described byCesarino et al. [1988] also ®ts within this spectrum ofdisorders. Inheritance of AMS is unclear, but recently afamily was described with two sibs affected by AMS[Cruz et al., 2000]. The father had subtle abnormalitiesthat were restricted to the palpebral ®ssures and ears,suggesting autosomal dominant inheritance withmarked variable expressivity [Ferraz et al., 2000].We report a boy with AMS who exhibited a phenotypeof intermediate severity when compared with thepreviously reported cases of AMS [McCarthy and West,1977; Hornblass and Rei¯er, 1985; Markouizos et al.,1990; Price et al., 1991; Cruz et al., 1995, 2000;Pellegrino et al., 1996] and the possibly mildly affectedfather reported by Ferraz et al. [2000].
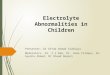
The boy was the second child of healthy nonconsan-guineous parents. There was no signi®cant familyhistory, and neither parent exhibited abnormal eye orear ®ndings. The boy was born at 41 weeks of gestationby vaginal delivery after a normal pregnancy. Therewas no exposure to tobacco, alcohol, or other drugs.Birth weight was 2,440 g and Apgar scores were 8 and10 at 1 and 5 minutes. The neonatal period was compli-cated by hypoglycemia, poor feeding and temperatureinstability, and an absence of lanugo hair, eyebrows,and eyelashes was noted. He was assessed in thegenetics clinic at age 4 months and again at age 6 yearsand 8 years. A number of dysmorphic features werenoted (Figs. 1 and 2). He had macrostomia with a milddegree of lateral clefting, abnormal ears with mildly
malformed helices and prominent earlobes, and arounded nasal tip with normally formed alae nasi.He had soft and redundant skin, ®ne hair, sparseeyebrows, hypoplastic nipples, and mild soft tissuesyndactyly of all ®ngers. The genitalia were normal,and there was no hypertelorism. Height was at thethird centile, with weight at the ®fth centile and headcircumference (occipital-frontal circumference) at thesecond centile. Karyotype was 46,XY (550-band level),in particular both chromosome 18s appeared normal.
Ophthalmologic assessment revealed prominentdeep-set eyes with abnormal shortening of both upperand lower eyelids associated with medial entropion
Fig. 1. The patient at age 8 months.
*Correspondence to: David J. Amor, Genetic Health ServicesVictoria, Flemington Rd, Parkville 3052, Australia.E-mail: [email protected]
Received 6 November 2000; Accepted 2 July 2001
DOI 10.1002/ajmg.1540
ß 2001 Wiley-Liss, Inc.

bilaterally. A corneal ulcer with secondary keratitisdeveloped at age 8 years, but reconstructive surgeryhas not yet been required. Visual acuity was mildlyreduced, and there was mild myopia and megalocornea.Audiology assessment was suggestive of a mixedconductive and sensory hearing loss.
Development was delayed. He walked at age 4 years,and at age 6 years he was assessed to be functioning atan 18-month level. At age 8 years, he was nonverbalbut could use simple signing. He displayed someautistic features including stereotypic play and poorsocialization. Neurologic examination showed general-ized hypotonia with normal re¯exes. His behavior waserratic, he slept poorly, and showed tactile sensitivity.Generalized seizures were present from age 2 years,and electroencephalography (EEG) showed frequentfocal epileptiform discharges in the left occipital andright posterior temporal regions. A magnetic resonanceimaging (MRI) scan was abnormal, with diffuse hypo-plasia of corpus callosum, mild prominence of the lateralventricles, and possible heterotopic gray matter relatedto the left lateral ventricle.
The pattern of malformations in this boy is consistentwith a diagnosis of AMS. His ophthalmologic, auri-
cular, and nasal manifestations are signi®cantly lesssevere, however, than early reports of this condition.Genital abnormalities and hypertelorism/telecanthus,both of which were present in 7 of 8 of previouslyreported cases, were also absent in this boy, raisingthe question of whether he has AMS or a separatedisorder (possibly allelic to AMS and BSS). The recentreport of a possibly mildly affected male with onlyeyelid and aural abnormalities supports the notion thatthe present case has an intermediate form of AMS[Ferraz et al., 2000].
Although delayed development has been described ina number of cases of AMS, the present case is onlythe second report of epilepsy and associated cen-tral nervous system (CNS) malformations in AMS.Pellegrino et al. [1996] reported a case of AMS withseizures, abnormal EEG, and MRI scan showingcerebral atrophy, abnormal myelination, underopercu-larization, and thinning of the corpus callosum. Thatcase also had a complex rearrangement of chromosome18q, and so it was unclear whether the CNS abnorm-alities should be considered part of AMS. The presentcase suggests that epilepsy and CNS abnormalitiesshould be included in the features of AMS.
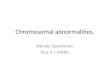
Fig. 2. Front (A) and side view (B) of patient at age 6 years.
Letter to the Editor 253

REFERENCES
Barber N, Say B, Bell R, Mervielle O. 1982. Macrostomia, ectropion,atrophic skin, hypertrichosis and growth retardation. Syndr Ident8:6±9.
Cesarino EJ, Pinheiro M, Freire-Maia N, Meira-Silva MC. 1988.Lid agenesis-macrostomia-psychomotor retardation-forehead hyper-trichosisÐa new syndrome? Am J Med Genet 31:299±304.
Cruz AA, Guimaraes FC, Obeid HN, Ferraz VE, Noce TR, Martinez FE.1995. Congenital shortening of the anterior lamella of all eyelids: theso-called ablepharon macrostomia syndrome. Ophthal Plast ReconstrSurg 11:284±287.
Cruz AA, Souza CA, Ferraz VE, Monteiro CA, Martins FA. 2000. Familialoccurrence of ablepharon-macrostomia syndrome: eyelid structure andsurgical considerations. Arch Ophthalmol 118:428±430.
Ferraz V, Melo D, Hansing S, Cruz A, Pina-Neto J. 2000. Ablepharon-macrostomia syndrome: ®rst report of familial occurrence. Am J MedGenet 94:281±283.
Hornblass A, Rei¯er DM. 1985. Ablepharon-macrostomia syndrome. Am JOphthalmol 99:552±556.
Markouizos D, Siddigi U, Siddigi S, Raziuddin K, Nangia B. 1990.Ablepharon macrostomia syndrome: report of a case and clinicaldelineation. Am J Hum Genet 47:A66.
Mazzanti L, Bergamaschi R, Neri I, Perri A, Patrizi A, Cacciari E,Forabosco A. 1998. Barber-Say syndrome: report of a new case. Am JMed Genet 78:188±191.
McCarthy GT, West CM. 1977. Ablepharon-macrostomia syndrome. DevMed Child Neurol 19:659±663.
Pellegrino JE, Schnur RE, Boghosian-Sell L, Strathdee G, Overhauser J,Spinner NB, Stump T, Grace K, Zackai EH. 1996. Ablepharon-macrostomia syndrome with associated cutis laxa: possible localizationto 18q. Hum Genet 97:532±536.
Price NJ, Pugh RE, Farndon PA, Willshaw HE. 1991. Ablepharon-macrostomia syndrome. Br J Ophthalmol 75:317±319.
David J. Amor*Ravi SavarirayanGenetic Health Services VictoriaRoyal Children's HospitalVictoria, Australia
Murdoch Childrens ResearchInstitute
Royal Children's HospitalVictoria, Australia
Department of PaediatricsUniversity of MelbourneVictoria, Australia
254 Amor and Savarirayan