Embed Size (px)
Citation preview

RESEARCH ARTICLE Open Access
Interference with work in fibromyalgia - effect oftreatment with pregabalin and relation to painresponseSebastian Straube1*, R Andrew Moore2, Jocelyn Paine3, Sheena Derry2, Ceri J Phillips4, Ernst Hallier1 andHenry J McQuay2
Abstract
Background: Clinical trials in chronic pain often collect information about interference with work as answers tocomponent questions of commonly used questionnaires but these data are not normally analysed separately.
Methods: We performed a meta-analysis of individual patient data from four large trials of pregabalin forfibromyalgia lasting 8-14 weeks. We analysed data on interference with work, inferred from answers to componentquestions of Fibromyalgia Impact Questionnaire (FIQ), Short Form 36 Health Survey, Sheehan Disability Scale, andMultidimensional Assessment of Fatigue, including “How many days in the past week did you miss work, includinghousework, because of fibromyalgia?” from FIQ. Analyses were performed according to randomised treatmentgroup (pregabalin 150-600 mg daily or placebo), pain improvement (0-10 numerical pain rating scale scores at trialbeginning vs. end), and end of trial pain state (100 mm visual analogue pain scale [VAS]).
Results: Comparing treatment group average outcomes revealed modest improvement over the duration of thetrials, more so with active treatment than with placebo. For the ‘work missed’ question from FIQ the change forpatients on placebo was from 2.2 (standard deviation [SD] 2.3) days of work lost per week at trial beginning to 1.9(SD 2.1) days lost at trial end (p < 0.01). For patients on 600 mg pregabalin the change was from 2.1 (SD 2.2) daysto 1.6 (SD 2.0) days (p < 0.001). However, the change in days of work lost was substantial in patients with a goodpain response: from 2.0 (SD 2.2) days to 0.97 (SD 1.6) days (p < 0.0001) for those experiencing >/= 50% painimprovement and from 1.9 (SD 2.2) days to 0.73 (SD 1.4) days (p < 0.0001) for those achieving a low level of painat trial end (<30 mm on the VAS). Patients achieving both >/= 50% pain improvement and a pain score <30 mmon the VAS had the largest improvement, from 2.0 (SD 2.2) days to 0.60 (SD 1.3) days (p < 0.0001). Analysinganswers to the other questions yielded qualitatively similar results.
Conclusions: Effective pain treatment goes along with benefit regarding work. A reduction in time off work >1day per week can be achieved in patients with good pain responses.
BackgroundFibromyalgia is a common chronic pain condition. Itoccurs in 1-2% of the population, more often in womenthan in men [1-3]. Chronic pain conditions such asfibromyalgia have profound effects on quality of life[4-6] and lead to interference with work and loss of pro-ductivity [7-13].
In clinical trials of treatments for chronic painful con-ditions - including trials in fibromyalgia - data on timeoff work and interference with work are typically col-lected as answers to component questions of commonlyused questionnaires. Answers from these componentquestions are used to calculate overall scores of thequestionnaires, but are not usually analysed separatelyand specifically with regard to work-related outcomes.Such an analysis - though not originally intended by theinventors of the questionnaires or the triallists who usedthem - nonetheless has the potential to provide useful
* Correspondence: [email protected] of Occupational, Social and Environmental Medicine, UniversityMedical Center Göttingen, Göttingen, GermanyFull list of author information is available at the end of the article
Straube et al. BMC Musculoskeletal Disorders 2011, 12:125http://www.biomedcentral.com/1471-2474/12/125
© 2011 Straube et al; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative CommonsAttribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction inany medium, provided the original work is properly cited.

insights into the outcomes associated with pain treat-ment: Do the patients with the greatest improvement inpain scores over the duration of the trial and those whohave the lowest levels of pain at trial end also have thelargest benefit with regard to work? How large is thebenefit? Do patients with no or little pain improvementand high end of trial pain scores achieve any meaningfulbenefit regarding work?We have recently addressed the question whether ben-
efit in chronic pain trials across different domains of lifeoccurs in the same patients, using a large set of indivi-dual patient data from randomised controlled trials(RCTs) of pregabalin in fibromyalgia [14]. We foundthat those patients with the largest pain improvement(difference in pain intensity at trial beginning vs. end)also had the largest benefit with regard to quality of lifeand time off work. The study presented here builds onour previous results. Using the same dataset we presentnew analyses specifically relating to work. We investi-gated time off work and interference with work inpatients with fibromyalgia based on data from work-related component questions from commonly usedquestionnaires. Analyses were conducted by randomisedtreatment group (pregabalin at doses of 150-600 mg perday or placebo), pain improvement (comparing painintensity at the beginning and the end of trials), andfinal (end of trial) pain state.We analysed answers to work-related component
questions from different questionnaires commonly usedin chronic pain trials all addressing work but using dif-ferent wording and assessment scales. Our aims werethreefold: first, to illuminate the relationship betweenpain treatment, pain response, and work; second, toinvestigate the comparability of answers to work-relatedquestions from different questionnaires; and, third, toprovide a framework for future analyses of data onwork-related outcomes collected in clinical trials inchronic painful conditions.
MethodsWe performed a meta-analysis of individual patient datafrom four large trials of pregabalin for fibromyalgia last-ing 8-14 weeks, analysing data on interference withwork, inferred from answers to component questions ofFibromyalgia Impact Questionnaire (FIQ), Short Form36 Health Survey (SF-36), Sheehan Disability Scale(SDS), and Multidimensional Assessment of Fatigue(MAF), including “How many days in the past week didyou miss work, including housework, because of fibro-myalgia?” from FIQ. Analyses were performed accordingto randomised treatment group (pregabalin at 150-600mg daily or placebo), pain improvement (comparing 0-10 numerical pain rating scale scores at trial beginning
and end), and end of trial pain state (100 mm visualanalogue pain scale [VAS]).Pfizer Inc. provided Excel files containing individual
patient data from four RCTs of pregabalin (Lyrica) inthe treatment of fibromyalgia along with PDF files ofthe corresponding clinical trial reports. Pfizer study IDnumbers of these trials and ClinicalTrials.gov identifiernumbers (where available) were as follows:
• 1008-105 [15]• A0081056, NCT00645398 [16]• A0081077, NCT00230776 [17]• A0081100, NCT00333866 [18]
An enriched enrolment randomised withdrawal trial,the “FREEDOM trial” [19], was not included in our ana-lysis because it was of fundamentally different trialdesign [20].Patients in the four included trials were at least 18
years old, fulfilling American College of Rheumatologyclassification criteria for fibromyalgia (1990 classificationcriteria) and with pain scores of ≥40 mm on the 100mm VAS after stopping any relevant pain or sleep medi-cation. Patients were randomised to receive pregabalin(150 mg, 300 mg, 450 mg, or 600 mg per day), or pla-cebo, predominantly with a 2-week dose escalationphase followed by fixed dosing for up to 14 weeks oftotal trial duration. The minimum requirement forinclusion in this individual patient meta-analysis wasthat trials had to be both randomised and double blind.Trial and patient characteristics are detailed in Addi-
tional file 1. In the four trials 2757 patients agedbetween 18 and 82 years were treated with pregabalinor placebo. More than 90% of trial participants werewomen. One trial lasted 8 weeks (trial 1008-105); theothers lasted 13 or 14 weeks. Pregabalin doses of 300mg (685 patients) and 450 mg (687 patients) were usedin all four trials, 600 mg (564 patients) in three, and 150mg (132 patients) in one trial; placebo was given to 689patients. Trial quality was assessed using the OxfordQuality Scale [21]. Validity was scored using the OxfordPain Validity Scale [22]. All trials obtained the maxi-mum scores of 5/5 and 16/16 on these scales, indicatinghigh trial quality and validity.We analysed individual patient data on pain scores
and time off work or interference with work obtained atthe beginning of the trials (baseline measurements) andat the end of trials. Data on time off work or interfer-ence with work were compared
• according to randomised treatment group (placeboor pregabalin at doses of 150, 300, 450, or 600 mgper day),
Straube et al. BMC Musculoskeletal Disorders 2011, 12:125http://www.biomedcentral.com/1471-2474/12/125
Page 2 of 9

• according to pain improvement, as described bythe comparison of baseline numerical pain ratingscores (scale 0-10) with end of trial numerical painrating scores (assessed after 8 weeks of treatment intrial 1008-105 and after 12 weeks of treatment inthe three other trials), and• according to pain state at end of trial, as assessedby the VAS pain score on a 0-100 mm scale.
Not all questionnaires were used in all trials and notall patients had usable individual patient data available.Therefore the number of patients contributing to indivi-dual analyses differed. Numbers of patients contributingare given in Tables 1-2 and Figures 1-2.Cut-off levels for pain improvement and end of trial
pain state were chosen with clinical relevance in mindand were based on published evidence. The Initiativeon Methods, Measurement, and Pain Assessment inClinical Trials (IMMPACT) defined benchmarks forinterpreting change in chronic pain clinical trial out-come measures [23]: a ‘minimally important’ improve-ment was defined as a 10-20% decrease in painintensity, a ‘moderately important’ improvement wasdefined as at least 30% decrease, and a ‘substantial’improvement equated to at least 50% decrease in painintensity. This formed the basis for our approach toclassify improvement in pain intensity as 0-<15%, 15-<30%, 30-<50%, ≥50%, or worsening. Furthermore,pain greater than about 30 mm on a 100 mm VAS is
equivalent to ‘moderate’ or greater pain [24,25] andtherefore a pain level below 30 mm appears to be asuitable clinical target. Hence 0-30 mm was chosen asthe strictest category of end of trial pain state andwas compared with the pain states >30-50 mm and>50 mm.We also analysed time off work and interference with
work according to whether patients achieved the statusof a ‘state responder’ (end of trial VAS pain score of 30mm or less), ‘improvement responder’ (at least 50%improvement in numerical pain rating scale score overthe duration of the trials), ‘double responder’ (state andimprovement responder), or ‘non-responder’ (neitherstate nor improvement responder).This approach was applied to the following five com-
ponent questions from four commonly used question-naires:
• “How many days in the past week did you misswork, including housework, because of fibromyal-gia?” (scale 0-7) from the FIQ;• “When you worked, how much did pain or otherfibromyalgia symptoms interfere with your ability todo your work, including housework?” (scale 0-10)from the FIQ;• “During the past 4 weeks, how much did paininterfere with your normal work (including bothwork outside the home and housework)?” (scale 1-5)from the SF-36;
Table 1 Days of work missed
Mean number (SD) of days of work missed perweek at trial beginning
Mean number (SD) of days of work missedper week at trial end
Statisticalsignificance
Pregabalin dose (n)
Placebo (557) 2.2 (2.3) 1.9 (2.1) **
300 mg (547) 2.4 (2.3) 1.9 (2.1) ****
450 mg (553) 2.1 (2.2) 1.7 (2.0) ***
600 mg (561) 2.1 (2.2) 1.6 (2.0) ***
Pain improvement(n)
Pain worse (221) 1.9 (2.1) 1.9 (2.1) NS
0-15% (281) 2.5 (2.4) 2.2 (2.2) NS
15-30% (233) 2.4 (2.2) 1.7 (2.0) ***
30-50% (319) 2.1 (2.2) 1.1 (1.7) ****
≥50% (435) 2.0 (2.2) 0.97 (1.6) ****
VAS pain score attrial end (n)
>50 mm (1042) 2.4 (2.3) 2.1 (2.1) *
>30-50 mm (340) 1.9 (2.0) 1.1 (1.7) ****
0-30 mm (436) 1.9 (2.2) 0.73 (1.4) ****
Days of work missed per week at the beginning and end of trials as assessed by the question “How many days in the past week did you miss work, includinghousework, because of fibromyalgia?” from the Fibromyalgia Impact Questionnaire (FIQ). Data are presented according to daily pregabalin dose, according toimprovement in pain intensity scores over the course of the trials, and according to pain state at end of the trials; statistical significance for the comparison oftrial end vs. beginning: * p < 0.05, ** p < 0.01, *** p < 0.001, **** p < 0.0001, NS - no significant difference. FIQ data were not available for trial 105, the only trialwith a 150 mg pregabalin group. Therefore no data for participants treated with 150 mg pregabalin are presented here.
Straube et al. BMC Musculoskeletal Disorders 2011, 12:125http://www.biomedcentral.com/1471-2474/12/125
Page 3 of 9

Table 2 Interference with work
Mean score (SD) at trial beginning Mean score (SD) at trial end Statistical significance
Pregabalin dose (n)
Placebo (556) 6.8 (2.1) 5.6 (2.6) ****
300 mg (551) 6.7 (2.1) 5.5 (2.6) ****
450 mg (553) 6.7 (2.1) 5.3 (2.6) ****
600 mg (562) 6.7 (2.1) 5.5 (2.7) ****
Pain improvement (n)
Pain worse (221) 6.3 (2.2) 6.1 (2.2) NS
0-15% (282) 7.2 (1.9) 6.5 (2.2) ****
15-30% (233) 6.8 (2.1) 5.7 (2.3) ****
30-50% (319) 6.6 (1.9) 4.2 (2.3) ****
≥50% (435) 6.6 (2.2) 3.5 (2.6) ****
VAS pain score at trial end (n)
>50 mm (1046) 7.0 (2.0) 6.5 (2.1) ****
>30-50 mm (326) 6.3 (2.1) 4.5 (2.0) ****
0-30 mm (387) 6.3 (2.2) 2.8 (2.3) ****
Interference with work as assessed by the question “When you worked, how much did pain or other fibromyalgia symptoms interfere with your ability to doyour work, including housework?” (scale 0-10) from the Fibromyalgia Impact Questionnaire. Data are presented according to daily pregabalin dose, according toimprovement in pain intensity scores over the course of the trials, and according to pain state at end of the trials; abbreviations as in Table 1.
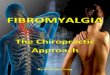
Figure 1 Days of work missed. Days of work missed per week at the beginning and end of trials as assessed by the question “How many daysin the past week did you miss work, including housework, because of fibromyalgia?” from the Fibromyalgia Impact Questionnaire (FIQ). Data arepresented as a comparison of ‘state’ and ‘improvement’ responders; ‘non-responders’ are neither state nor improvement responders; ‘doubleresponders’ are both. ** p < 0.01, *** p < 0.001, **** p < 0.0001, NS - no significant difference, SD - standard deviation. FIQ data were notavailable for trial 105, the only trial with a 150 mg pregabalin group. Therefore no data for participants treated with 150 mg pregabalin arepresented here.
Straube et al. BMC Musculoskeletal Disorders 2011, 12:125http://www.biomedcentral.com/1471-2474/12/125
Page 4 of 9

• “The symptoms have disrupted your work/schoolwork” (scale 0-10) from the SDS;• “In the past week, to what degree has fatigue inter-fered with your ability to work?” (scale 1-10) fromthe MAF.
Spreadsheet calculations from the individual patientdata were performed independently of Pfizer by one ofthe authors: Jocelyn Paine from the commercial spread-sheet calculating and programming service ‘SpreadsheetFactory’ [26]. The statistical significance of differences inmean values at the beginning and end of trials wasestablished with the t test using ‘QuickCalcs’ [27].
ResultsDays of work lost per weekBased on response data from the question “How manydays in the past week did you miss work, includinghousework, because of fibromyalgia?” from the FIQ wecompared placebo and pregabalin treatment arms of thetrials (Table 1). There was statistically significantimprovement at trial end (compared with the baselinevalues at trial beginning) in all treatment arms, includ-ing in the patients treated with placebo, though greaterimprovement occurred with pregabalin treatment.While the analysis of patients according to rando-
mised treatment group (and irrespective of pain
response) reveal only modest average improvementswhen trial beginning and end were compared, analysingpatients according to pain improvement revealed sub-stantial differences. Those patients with the largest painimprovements (changes in 0-10 numerical pain ratingscale score from trial baseline to trial end) also had thelargest changes in days off work. Those with at least50% pain improvement gained about one day of workper week (Table 1).Analysing days off work by end of trial pain state (100
mm VAS score) likewise revealed a close relationshipbetween pain experience and time off work. While therewas little difference in time off work in those with afinal VAS pain state >50 mm, those with a pain state>30-50 mm benefited substantially, and patients with afinal pain state of 0-30 mm benefited extensively, gain-ing about 1.3 days of work per week (Table 1).Next we analysed time off work according to status as
a ‘state responder’, ‘improvement responder’, ‘doubleresponder’ or ‘non-responder’ (Figure 1). Patients whowere neither state nor improvement responders had theleast benefit in term of gaining time at work. Patientswho were improvement but not state responders bene-fited more and those who were state but not improve-ment responders had even more benefit. Doubleresponders had the largest benefit, with an average of1.4 more days of work per week
Figure 2 Interference with work. Interference with work as assessed by the question “When you worked, how much did pain or otherfibromyalgia symptoms interfere with your ability to do your work, including housework?” from the Fibromyalgia Impact Questionnaire;responder categories and abbreviations as in Figure 1.
Straube et al. BMC Musculoskeletal Disorders 2011, 12:125http://www.biomedcentral.com/1471-2474/12/125
Page 5 of 9

Interference with work as assessed from the FIQWe analysed answers to the question “When youworked, how much did pain or other fibromyalgia symp-toms interfere with your ability to do your work, includ-ing housework?” from the FIQ in an analogous mannerto answers to the question about days of work missed.Our findings were similar: Analysing all patients inde-pendently of pain outcomes there was improvementwith regard to work over the duration of the trials inevery treatment group, more so with pregabalin thanwith placebo, though the differences were not large.Those with the most pain improvement and the leastend of trial pain scores had the best outcome in termsof experiencing less interference with work, while thosewith little pain improvement and high end of trial painscores had little benefit (Table 2). Double-respondershad the largest benefit with a 67% reduction in averagework interference, followed by state only responders(55%), improvement only responders (27%), and non-responders (12%; Figure 2).
Other questions about interference with workThe answers to the component questions about interfer-ence with work from the other questionnaires produceda similar picture. Categorising patients by randomisedtreatment group (pregabalin 150, 300, 450, or 600 mg orplacebo) revealed modest improvement when trialbeginning and end were compared, somewhat more soin the pregabalin groups than with placebo (data notshown).Analyses of state and improvement responders like-
wise yielded qualitatively similar results. We investigatedbetween-question similarity by calculating the percentimprovement in answers to the different work-relatedquestions, in each case comparing responses at trialbeginning and end. We performed these analysesaccording to pain improvement over the duration of thetrials (Table 3) and according to end of trial pain state(Table 4). For example, patients in the category of ≥50%improvement in pain score had a 52% improvement inthe score for the FIQ question about days of workmissed and 47% improvement in work interference as
assessed from the FIQ question; those in the category of30-50% pain improvement had an improvement in theanswers to those questions of 47% and 36% respectively.Lower levels of pain benefit were associated with smallerreductions in work interference, and patients withoutpain improvement had no meaningful improvementeither with regard to days of work missed or with regardto interference with work in any question (Table 3). Thepattern of higher levels of pain intensity reduction beingassociated with greater reductions in work interferencewas found for questions from all four questionnaires(FIQ, SF-36, SDS, and MAF). The degree of benefit wassimilar in the three questionnaires using a 0-10 or 1-10scale (FIQ, SDS, and MAF), with somewhat less benefitfor SF-36, using a five-point scale.Patients with an end of trial pain state of 30 mm or
less on the 0-100 mm VAS had an improvement in thescore for the FIQ questions about days of work missedand work interference of 61% and 56%, respectively.Those with a final VAS score >50 mm only had minimalimprovement in days of work lost and work interference(Table 4). Again, less pain was associated with greaterimprovement in work interference for all questions, andthe degree of benefit was similar in the three question-naires using a 0-10 or 1-10 scale (FIQ, SDS, and MAF),with somewhat less apparent benefit for SF-36 where afive-point scale was used.
DiscussionAnalysis of data at the level of the individual patient canreveal insights over and above those that can beobtained from the analysis of group mean values but itis only possible when trial data are made available at thelevel of the individual patient. We had such data forpregabalin trials in fibromyalgia, but not for pregabalinin other painful conditions, nor for other drugs in fibro-myalgia or other painful conditions. The availability ofclinical trial data at the level of the individual patient isuncommon, especially where trials have consistentlyused several different assessment scales permitting ana-lysis of the relationship between treatment success asmeasured by pain relief and work interference.
Table 3 Improvement in answers to work-related questions according to pain improvement
Painimprovement
FIQ (days of workmissed)
FIQ (interference withwork)
SF-36 (interference withwork)
SDS (interference withwork)
MAF (interference withwork)
≥ 50% 52 47 33 62 57
30 - <50% 47 36 23 42 35
15 - <30% 28 16 16 28 28
0 - <15% 12 10 8.2 12 0.95
<0% -1.0 2.8 1.8 -6.9 -10
Percent improvement in answers to work-related questions over the duration of the trials; patients were categorised by pain improvement (based on the 0-10numerical pain rating scale comparing trial beginning and end); FIQ - Fibromyalgia Impact Questionnaire, SF-36 - Short Form 36 Health Survey, SDS - SheehanDisability Scale, MAF - Multidimensional Assessment of Fatigue.
Straube et al. BMC Musculoskeletal Disorders 2011, 12:125http://www.biomedcentral.com/1471-2474/12/125
Page 6 of 9

This study demonstrated that most benefit regardingwork in trials of pregabalin for fibromyalgia is obtainedby patients who have large improvements in pain inten-sity, achieve a low level of pain after treatment, andespecially if they achieve both of these outcomes. Com-paring treatment groups irrespective of pain outcomesreveals a picture of only modest average benefit of activetreatment when compared with placebo. However, sub-stantial benefit in work-related outcomes can be demon-strated in those for whom treatment ‘works’ in the sensethat it leads to a reduction in pain or a low end of trialpain state. Relationships between higher levels of painand increased disability and interference with activitieshave been shown for a variety of conditions includingcancer pain, phantom limb pain, back pain, and carpaltunnel syndrome [28-30], but improvements in work-related endpoints on return to a low pain state are lesswell described.The point that fibromyalgia leads to substantial inter-
ference with work is well worth making. The status offibromyalgia as a valid disease entity, let alone one witha substantial impact on a variety of domains of life, haslong been in question because a clear physical correlateof the disease could not be demonstrated. Not surpris-ingly, in the face of such scepticism the diagnosis offibromyalgia is often delayed [13]. Recently, however,evidence pointing to objective changes is accumulating[31]. A link between elevated intrinsic brain connectivityand spontaneous pain intensity in fibromyalgia has beenshown [32], as has an association between cerebralblood flow and response to treatment with gabapentin[33]. Along with the emerging evidence of a physicalcorrelate comes the insight that fibromyalgia has realand profound impact across different domains of lifeincluding work [8-10,12,13] and that the economic bur-den associated with fibromyalgia is substantial, alsobecause of a high prevalence of co-morbidities [34]. Dis-ease state and interference with work are linked in fibro-myalgia, as the present and other studies demonstrate.Temporary work disability in fibromyalgia patients hasbeen associated with a worse clinical situation andworse functional capacity [35]. A narrative interviewstudy uncovered that severe pain and fatigue, together
with a demanding life situation and ageing, seemed tocause substantial interference with work and functioning[36]. Remaining at work despite fibromyalgia requires ‘aconstant struggle’ against the symptoms and conse-quences of the disease [37]. Increased awareness offibromyalgia as a genuine condition along with practice-oriented diagnostic criteria and a scale for the assess-ments of symptom severity [38], will hopefully lead tomore prompt diagnosis and adequate treatment.The IMMPACT group suggested that 50% improve-
ment in pain intensity is ‘substantial improvement’ [23].Other evidence suggests that 30 mm is a suitable cut-offto determine a target pain state [24,25]. Our findings ontime off work and interference with work underline theusefulness of these suggested cut-offs in clinical practice.Our analysis provides further evidence that benefit
due to treatment of fibromyalgia with pregabalin acrossdifferent domains of life occurs largely in the samepatients, as we previously suggested [14]. Those patientswith the lowest end of trial pain levels and the mostpain improvements had the largest benefits regardingwork. This underlines the point that effective pain treat-ment should be sought, both from a patient perspectiveand also from an economic perspective [39], and thatpain outcomes are linked with outcomes in otherdomains of life. Achieving the state of effective paincontrol will probably involve changing therapy in a sub-stantial number of patients because no therapy workswell in more than half the patients with fibromyalgia[40-42]. Therefore, always using just one drug for treat-ing this complex and varied condition, even if it appearsbest on a population level, is unlikely to deliver the bestoutcomes for the most patients.We found that data from several questions about time
off work and interference with work with somewhat dif-ferent wording and from different questionnaires yieldedoverall similar results, though when expressed as per-cent improvement in scores (comparing trial beginningand end, Tables 3 and 4) there were differences in themagnitude of the improvement. Caution is thereforeneeded when data from different work-related questionsare compared. The preliminary findings here wouldindicate that questionnaires with 0-10 or 1-10 scales
Table 4 Improvement in answers to work-related questions according to pain state
Pain state (VASscore)
FIQ (days of workmissed)
FIQ (interference withwork)
SF-36 (interference withwork)
SDS (interference withwork)
MAF (interference withwork)
≤ 30 mm 61 56 41 68 58
30 - 50 mm 41 28 22 46 37
> 50 mm 9.9 7.1 5.9 12 6.2
Percent improvement in answers to work-related questions over the duration of the trials; patients were categorised according to pain state (0-100 mm VASscore) at the end of trial; FIQ - Fibromyalgia Impact Questionnaire, SF-36 - Short Form 36 Health Survey, SDS - Sheehan Disability Scale, MAF - MultidimensionalAssessment of Fatigue.
Straube et al. BMC Musculoskeletal Disorders 2011, 12:125http://www.biomedcentral.com/1471-2474/12/125
Page 7 of 9

measuring work interference are associated with biggerimprovements in work interference measures than aquestionnaire with a 1-5 scale. This may be an effect ofthe scales, because the maximum possible reductionthat can be attained on a 1-5 scale is 80%, while it is90% on a 1-10 scale and 100% on a 0-10 scale.Despite the large number of patients studied in four
high quality randomised trials, the analysis presentedhere has important limitations, not least being a retro-spective analysis that is only hypothesis-generating. Asmentioned previously, using component questions ofquestionnaires in this way was not intended by thedevelopers of the questionnaires, and the question-naires have therefore not been validated for this use.Furthermore, the wording of the questions addressing‘interference with work’ does not allow a differentia-tion into what kind of ‘interference’ (absenteeism, pre-senteeism) is present. We had no objective records oftime at work or time off work on which to base ouranalysis; nor did we have a detailed description of thetype of occupation. This would have been interestingbecause different kinds of occupation may be differ-ently affected by pain and its treatment. Moreover, weonly used data from four trials of pregabalin in fibro-myalgia where we had individual data available; otherchronic pain conditions and treatments might producedifferent results.These limitations determine the agenda for future
research: The first step would be a repetition of thistype of analysis for different work-related questions,different treatments and different chronic pain condi-tions to determine whether or not our findings aregeneral. Because data on time off work and interfer-ence with work are commonly collected in chronicpain trials, this is primarily a question of obtainingaccess to the data and performing the analyses. Thesecond step will be more difficult: to collect moredetailed information on occupation and objective dataon time off work as part of clinical trials in chronicpain. We hope that raising the awareness of theseissues will lead to such data being collected in chronicpain trials in the future.
ConclusionsThis meta-analysis of individual patient data from fourtrials of pregabalin for fibromyalgia demonstrates thateffective pain treatment, described in terms of painimprovement over the course of the trials and end oftrial pain state, is linked with benefit regarding work. Areduction in time off work of more than one day perweek can be achieved in patients with good painresponses. Analysing answers to work-related compo-nent questions from different questionnaires yields qua-litatively similar results.
Additional material
Additional file 1: Study and patient characteristics. The studies areidentified by their Pfizer study ID numbers, the ClinicalTrials.gov identifiernumbers (where available), and references to publications.
AbbreviationsFIQ: Fibromyalgia Impact Questionnaire; IMMPACT: Initiative on Methods,Measurement, and Pain Assessment in Clinical Trials; MAF: MultidimensionalAssessment of Fatigue; NS: no significant difference; RCT: randomisedcontrolled trial; SD: standard deviation; SDS: Sheehan Disability Scale; SF-36:Short Form 36 Health Survey; VAS: visual analogue scale
AcknowledgementsWe are grateful to Pfizer Inc. for providing us with the data. This project wassupported by a grant to S.S. from Research program, Faculty of Medicine,Georg-August-University Göttingen. Other funding was from Pain Researchfunds of the Oxford Pain Relief Trust and institutional funds of the NuffieldDivision of Anaesthetics, University of Oxford. Financial support for severalassociated projects was provided by Pfizer Inc., but this analysis wasadditional to and outside the scope of the funded work. R.A.M. is funded byNIHR Biomedical Research Centre Programme.
Author details1Department of Occupational, Social and Environmental Medicine, UniversityMedical Center Göttingen, Göttingen, Germany. 2Pain Research, NuffieldDivision of Anaesthetics, Nuffield Department of Clinical Neurosciences,University of Oxford, Churchill Hospital, Oxford, UK. 3Spreadsheet Factory,Stratfield Road, Oxford, UK. 4School of Human and Health Sciences, SwanseaUniversity, Swansea, UK.
Authors’ contributionsSS and RAM were involved with the original concept, planning the study,writing it, analysis, and preparing a manuscript; JP performed the calculation;SD, CJP, EH, and HJM. were involved with planning, and writing. All authorsread and approved the final manuscript.
Competing interestsSS received research support and grants from charities, Bandolier, ReckittBenckiser, and Georg-August-University Göttingen and received lecture feesfrom University Children’s Hospital Zurich and Oxford Medical Knowledge.RAM received lecture fees from Merck, Pfizer, Menarini, Lundbeck,AstraZeneca; served as a consultant for Merck, Pfizer, Eli Lilly, Flynn, Futura,Altana, Fujisawa, GSK, Shire, Sanofi-Aventis, Grünenthal, Organon, ZARS;received research grants from Merck, Pfizer, Abbott, AstraZeneca, Menarini,GSK, Aspreva, Janssen-Cilag. CJP received lecture fees from Merck, Gileadand Lundbeck in the past year, served as a consultant for Merck, Pfizer andSanofi-Aventis in the past year and received a departmental grant fromNapp in the past year. SD received research support from UK governmentand charities. HJM received lecture or consultancy fees in the past year fromMenarini, Esteve, Grünenthal, Pfizer, Reckitt Benckiser, IMS and Archimedes.
Received: 4 February 2011 Accepted: 3 June 2011Published: 3 June 2011
References1. McNalley JD, Matheson DA, Bakowshy VS: The epidemiology of self-
reported fibromyalgia in Canada. Chronic Dis Can 2006, 27:9-16.2. Mas AJ, Carmona L, Valverde M, Ribas B, EPISER Study Group: Prevalence
and impact of fibromyalgia on function and quality of life in individualsfrom the general population: results from a nationwide study in Spain.Clin Exp Rheumatol 2008, 26:519-526.
3. Bannwarth B, Blotman F, Roué-Le Lay K, Caubère JP, André E, Taïeb C:Fibromyalgia syndrome in the general population of France: Aprevalence study. Joint Bone Spine 2009, 76:184-187.
4. Hawley DJ, Wolfe F: Pain, disability, and pain/disability relationships inseven rheumatic disorders: a study of 1,522 patients. J Rheumatol 1991,18:1552-1557.
Straube et al. BMC Musculoskeletal Disorders 2011, 12:125http://www.biomedcentral.com/1471-2474/12/125
Page 8 of 9

5. Martinez JE, Ferraz MB, Sato EI, Atra E: Fibromyalgia versus rheumatoidarthritis: a longitudinal comparison of the quality of life. J Rheumatol1995, 22:270-274.
6. Sprangers MA, de Regt EB, Andries F, van Agt HM, Bijl RV, de Boer JB,Foets M, Hoeymans N, Jacobs AE, Kempen GI, Miedema HS, Tijhuis MA, deHaes HC: Which chronic conditions are associated with better or poorerquality of life? J Clin Epidemiol 2000, 53:895-907.
7. Stewart WF, Ricci JA, Chee E, Morganstein D, Lipton R: Lost productivetime and cost due to common pain conditions in the US Workforce.JAMA 2003, 290:2443-2454.
8. Henriksson CM, Liedberg GM, Gerdle B: Women with fibromyalgia: workand rehabilitation. Disabil Rehabil 2005, 27:685-694.
9. Al-Allaf AW: Work disability and health system utilization in patients withfibromyalgia syndrome. J Clin Rheumatol 2007, 13:199-201.
10. White KP, Speechley M, Harth M, Ostbye T: Comparing self-reportedfunction and work disability in 100 community cases of fibromyalgiasyndrome versus controls in London, Ontario: the London FibromyalgiaEpidemiology Study. Arthritis Rheum 1999, 42:76-83.
11. White AG, Birnbaum HG, Mareva MN, Henckler AE, Grossman P, Mallett DA:Economic burden of illness for employees with painful conditions. JOccup Environ Med 2005, 47:884-892.
12. White LA, Birnbaum HG, Kaltenboeck A, Tang J, Mallett D, Robinson RL:Employees with fibromyalgia: medical comorbidity, healthcare costs,and work loss. J Occup Environ Med 2008, 50:13-24.
13. Choy E, Perrot S, Leon T, Kaplan J, Petersel D, Ginovker A, Kramer E: Apatient survey of the impact of fibromyalgia and the journey todiagnosis. BMC Health Serv Res 2010, 10:102.
14. Moore RA, Straube S, Paine J, Phillips CJ, Derry S, McQuay HJ: Fibromyalgia:Moderate and substantial pain intensity reduction predicts improvementin other outcomes and substantial quality of life gain. Pain 2010,149:360-364.
15. Crofford LJ, Rowbotham MC, Mease PJ, Russell IJ, Dworkin RH, Corbin AE,Young JP Jr, LaMoreaux LK, Martin SA, Sharma U, Pregabalin 1008-105Study Group: Pregabalin for the treatment of fibromyalgia syndrome:results of a randomized, double-blind, placebo-controlled trial. ArthritisRheum 2005, 52:1264-1273.
16. Mease PJ, Russell IJ, Arnold LM, Florian H, Young JP Jr, Martin SA, Sharma U:A randomized, double-blind, placebo-controlled, phase III trial ofpregabalin in the treatment of patients with fibromyalgia. J Rheumatol2008, 35:502-514.
17. Arnold LM, Russell IJ, Diri EW, Duan WR, Young JP Jr, Sharma U, Martin SA,Barrett JA, Haig G: A 14-week, randomized, double-blinded, placebo-controlled monotherapy trial of pregabalin in patients with fibromyalgia.J Pain 2008, 9:792-805.
18. Pauer L, Danneskiold-Samsoe B, Jespersen A: Pregabalin for themanagement of Fibromyalgia (FM): A 14-week, randomised, double-blind, placebo controlled, monotherapy trial (Study A0081100). AnnRheum Dis 2008, 67(Suppl):256.
19. Crofford LJ, Mease PJ, Simpson SL, Young JP Jr, Martin SA, Haig GM,Sharma U: Fibromyalgia relapse evaluation and efficacy for durability ofmeaningful relief (FREEDOM): a 6-month, double-blind, placebo-controlled trial with pregabalin. Pain 2008, 136:419-431.
20. McQuay HJ, Derry S, Moore RA, Poulain P, Legout V: Enriched enrolmentwith randomised withdrawal (EERW): Time for a new look at clinical trialdesign in chronic pain. Pain 2008, 135:217-220.
21. Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ,McQuay HJ: Assessing the quality of reports of randomized clinical trials:is blinding necessary? Control Clin Trials 1996, 17:1-12.
22. Smith LA, Oldman AD, McQuay HJ, Moore RA: Teasing apart quality andvalidity in systematic reviews: an example from acupuncture trials inchronic neck and back pain. Pain 2000, 86:119-132.
23. Dworkin RH, Turk DC, Wyrwich KW, Beaton D, Cleeland CS, Farrar JT,Haythornthwaite JA, Jensen MP, Kerns RD, Ader DN, Brandenburg N,Burke LB, Cella D, Chandler J, Cowan P, Dimitrova R, Dionne R, Hertz S,Jadad AR, Katz NP, Kehlet H, Kramer LD, Manning DC, McCormick C,McDermott MP, McQuay HJ, Patel S, Porter L, Quessy S, Rappaport BA,Rauschkolb C, Revicki DA, Rothman M, Schmader KE, Stacey BR, Stauffer JW,von Stein T, White RE, Witter J, Zavisic S: Interpreting the clinicalimportance of treatment outcomes in chronic pain clinical trials:IMMPACT recommendations. J Pain 2008, 9:105-121.
24. Collins SL, Moore RA, McQuay HJ: The visual analogue pain intensityscale: what is moderate pain in millimetres? Pain 1997, 72:95-97.
25. Tubach F, Ravaud P, Baron G, Falissard B, Logeart I, Bellamy N,Bombardier C, Felson D, Hochberg M, van D, Dougados M: Evaluation ofclinically relevant states in patient reported outcomes in knee and hiposteoarthritis: the patient acceptable symptom state. Ann Rheum Dis2005, 64:34-37.
26. Spreadsheet Factory. [http://www.spreadsheet-factory.com].27. QuickCalcs. [http://www.graphpad.com/quickcalcs].28. Serlin RC, Mendoza TR, Nakamura Y, Edwards KR, Cleeland CS: When is
cancer pain mild, moderate or severe? Grading pain severity by itsinterference with function. Pain 1995, 61:277-284.
29. Jensen MP, Smith DG, Ehde DM, Robinsin LR: Pain site and the effects ofamputation pain: further clarification of the meaning of mild, moderate,and severe pain. Pain 2001, 91:317-322.
30. Turner JA, Franklin G, Heagerty PJ, Wu R, Egan K, Fulton-Kehoe D, Gluck JV,Wickizer TM: The association between pain and disability. Pain 2004,112:307-314.
31. Harris RE, Clauw DJ: How do we know that the pain in fibromyalgia is‘real’? Curr Pain Headache Rep 2006, 10:403-407.
32. Napadow V, Lacount L, Park K, As-Sanie S, Clauw DJ, Harris RE: Intrinsicbrain connectivity in fibromyalgia is associated with chronic painintensity. Arthritis Rheum 2010, 62:2545-2555.
33. Usui C, Hatta K, Doi N, Nakanishi A, Nakamura H, Nishioka K, Arai H: Brainperfusion in fibromyalgia patients and its differences betweenresponders and poor responders to gabapentin. Arthritis Res Ther 2010,12:R64.
34. Lachaine J, Beauchemin C, Landry PA: Clinical and economiccharacteristics of patients with fibromyalgia syndrome. Clin J Pain 2010,26:284-290.
35. Rivera J, Esteve-Vives J, Vallejo MA, Rejas J, Grupo ICAF: Factors associatedwith temporary work disability in patients with fibromyalgia. RheumatolInt 2010.
36. Sallinen M, Kukkurainen ML, Peltokallio L, Mikkelsson M: Women’snarratives on experiences of work ability and functioning infibromyalgia. Musculoskeletal Care 2010, 8:18-26.
37. Löfgren M, Ekholm J, Ohman A: ’A constant struggle’: successfulstrategies of women in work despite fibromyalgia. Disabil Rehabil 2006,28:447-455.
38. Wolfe F, Clauw DJ, Fitzcharles MA, Goldenberg DL, Katz RS, Mease P,Russell AS, Russell IJ, Winfield JB, Yunus MB: The American College ofRheumatology preliminary diagnostic criteria for fibromyalgia andmeasurement of symptom severity. Arthritis Care Res (Hoboken) 2010,62:600-610.
39. Phillips C, Main C, Buck R, Aylward M, Wynne-Jones G, Farr A: Prioritisingpain in policy making: the need for a whole systems perspective. HealthPolicy 2008, 88:166-175.
40. Bennett RM, Kamin M, Karim R, Rosenthal N: Tramadol andacetaminophen combination tablets in the treatment of fibromyalgiapain: a double-blind, randomized, placebo-controlled study. Am J Med2003, 114:537-545.
41. Sultan A, Gaskell H, Derry S, Moore RA: Duloxetine for painful diabeticneuropathy and fibromyalgia pain: systematic review of randomisedtrials. BMC Neurol 2008, 8:29.
42. Straube S, Derry S, Moore RA, McQuay HJ: Pregabalin in fibromyalgia:meta-analysis of efficacy and safety from company clinical trial reports.Rheumatology (Oxford) 2010, 49:706-715.
Pre-publication historyThe pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2474/12/125/prepub
doi:10.1186/1471-2474-12-125Cite this article as: Straube et al.: Interference with work in fibromyalgia- effect of treatment with pregabalin and relation to pain response.BMC Musculoskeletal Disorders 2011 12:125.
Straube et al. BMC Musculoskeletal Disorders 2011, 12:125http://www.biomedcentral.com/1471-2474/12/125
Page 9 of 9









![Perioperative Pregabalin & Ketamine as Multimodal …...Source: Lyrica ® (Pregabalin) [Package Insert]. Pfizer Pharmaceuticals LLC. Vega Baja, PR: 2011 Pregabalin Adverse Effects](https://img.dokumen.tips/doc/110x75/5f64d8667e802371ab4d10a5/perioperative-pregabalin-ketamine-as-multimodal-source-lyrica-pregabalin.jpg)