Embed Size (px)
Citation preview

Interest Circle CallJune 3, 2010
1
OverviewWhat is a Managed Care Entity (MCE)? How is behavioral health structured in an
MCE?What do MCE’s do? What is the difference in roles between the
MCE and the state purchaser of MCE services?
What does all this mean for Parity and HCR?
2

Definition of a Managed Care Entity An organization responsible for a system of
health care delivery that influences utilization , cost, quality of services, and measures performance. The goal is a system that delivers value by giving people access to quality, cost-effective health care.
3

Structure Managed care takes various forms/names:
Managed Care Entity (MCE)Managed Care Organization (MCO) Primary Care Clinician Model (PCCM)- primary
care as gatekeeper)Pre-Paid Inpatient Health Plan (PIHP) Health Management Organization (HMO)Administrative Service Organization*Integrated plan Carve-out plan
4* ASO may retain responsibility for only partial list of described activities
Structure (cont) Need to know how the MCE manages the
behavioral health benefit
Is it:Integrated within one planSubcontracted to another organizationCarved-out from any physical health
management
5

Structure (cont)MCE approaches to BH
6
ImplicationsSubstance use disorders/addiction impacts and
requires strategies that address both physical health and behavioral health
It sits at the intersection of the MCE and its’ operations
Substance use disorders predispose people to PH problems, complicate existing PH conditions, co-exist with other BH issues, and impact self-care
MCE structures that are not geared to look “across” the health of individuals, may under-recognize, under-report and under-prepare to support this population
7

Implications MCE structure will inform how behavioral
health –specific information is used by the MCE Physical “side” is larger than BH “side” –
inadvertent competition for resources Depth of knowledge about substance
use/addiction How incentives are aligned (or not) to address
SA Ability to access/use data to guide action
8

MCE Key Responsibilities 4 Major Activities:
Utilization Management (UM)Quality Management (QM)Network Management (NM)Rates & Claims Payment
These activities are inter-dependent and are not separate activities
9
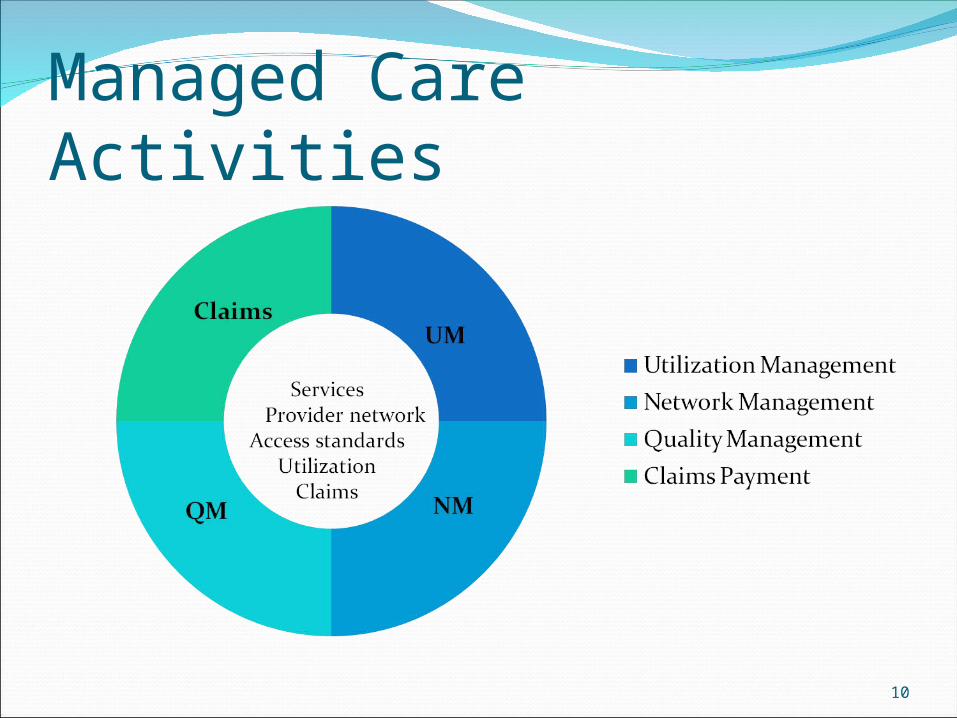
Managed Care Activities
10
Utilization Management (UM)Processes that address under and over utilization
Covered servicesCriteria for access to a covered service
Medical necessity criteria Initial, concurrent, and discharge criteria
Care Management ( and/or disease management)Authorization--amount, duration, scope &
processes used Clinical reviewsAppeals
11

Network Management (NM)Types of activities include:
Provider credentials for each covered serviceEnsuring that providers can meet access
standards set by federal or state requirements: Ex: language, geography/travel time, choice
Ensuring that providers deliver services according to service definitions and clinical/practice standards (also tied to QM)
12

Quality Management (QM)Types of activities include:
Evidenced-based practices (also tied to UM and covered services)
Outcome measuresPerformance or service delivery process
measuresPay-for-performance
13
Rates & Claims PaymentTypes of activities include:
Establishing rates for servicesPaying “clean” claimsPursuing any other insurance available for an
MCE covered memberFraud and abuse monitoring
14

ImplicationsMCE processes may or may not be geared to
address unique aspects of substance abuse/addiction
Approaches to QM, UM or NM may pose barriers
MCE ‘s use of provider and consumer input
15

Differences between MCE and State Purchaser rolesImportant to know when a state purchaser
has authority over an issue, when it is the purview of an MCE, and when it is shared by both
16

Differences between MCE and State Purchaser roles*
State Purchaser
MCE
Defining covered services
Use of evidenced-based practices
Defining access standards (Ex: geography, language, choice)
Ensuring standards are met by providers
Strategies used to manage utilization
Establishing provider credentialing
Establishing performance measures
Setting rates and paying claims
Use of data to improve quality and control costs
17* Numerous federal requirements guide both state purchaser and MCE activities

ImplicationsState purchaser of MCE services may /may not be
substance abuse authority for the state/level of knowledge of SA
MCE may/may not be knowledgeable about SAGathering information and advocating for
changes may require discussions with the MCE, the state purchaser or both
Timing of changes in contract between state and MCE
18
Current Political ContextWellstone-Domenici Mental Health Parity and
Addictions Equity Act effective 1/1/10Health Care ReformPayment reformHIT Private insurers and coverage Controlling costsIntegrating careImproving quality
19

Political Context (cont)Medicaid Cost Containment
Medicaid Enrollment
Services
Rates
Utilization
20

Implications of Parity and HCRState purchasers and MCE’s scrambling to
assess impact and implement changes Party Act is in effect but time lag on full
implementation of contracts, procedures, etcParity and HCR have changed how state level
Medicaid programs can control their costs No longer can use the same “levers” of
enrollment, services and rates Reliance on managed care to keep utilization
in check will increase 21

SummaryThe community expertise on SA is essentialOpportunities to partner with MCE Opportunities to partner with state purchaser Use of data
22