Embed Size (px)
Citation preview

Interactive Videodisc and Compact Disc--Interactive for Ophthalmic Basic Science and Continuing Medical Education
Robert Folberg, MD, 1•2 Laura K. Dickinson, BA, 1 Robert A Christiansen, PhD, 1
Joan S. Huntley, PhD, 3 Daniel G. Lind, MS4
Background: The authors designed and implemented a complete curriculum in ophthalmic pathology using IBM- and Macintosh-based interactive videodisc (IVD) technology. They also redesigned a portion of this curriculum for a new television-based platform, compact disc-interactive (CD-I).
Methods: The following issues were addressed: curriculum design, instructional design, the assembly of illustrations and the ownership of such materials, the generation of computer-based medical art and animation, and programming. The issue of academic credit for faculty participating in this effort also was considered.
Results: The computer-based IVD program provides the following features: (1) rapid access to thousands of high-quality illustrations with the option of superimposing graphic labels and text directly over pictures; (2) the ability to view enlargements of photographs; (3) an online glossary to view definition of terms coupled with high-quality photographs; and (4) a dynamic introduction to pathophysiology using interactive animation sequences. The authors were able to incorporate the same interactive features into the CD-I version. High-quality medical illustrations can be used effectively on the CD-I platform.
Conclusions: Computer-based multimedia workstations are relatively expensive for personal use but may be useful if the equipment can be shared in a learning center or library. Compared with interactive computer-based solutions, consumer-oriented television-based technology such as CD-I is a relatively inexpensive vehicle for providing continuing medical education programs intended for use in the individual practitioner's office or home. Ophthalmology 1993;100:842-850
Originally received: November 5, 1992. Revision accepted: December 18, 1992.
In 1987, the University oflowa accepted an invitation to join the HealthCare Interactive Videodisc Consortium sponsored by the International Business Machines Corporation (IBM). 1 Each of the 17 medical educational institutions in this consortium developed five programs. Two of the five programs developed at the University of Iowa focused on ophthalmology: Basic Ophthalmology and Pathology of the Eye. 3 Basic Ophthalmology was designed to provide a core ophthalmic education to medical students, non-ophthalmic physicians (especially family practitioners and internists) and to paramedical personnel such as nurses and physician assistants. Most of the programs developed by this consortium were targeted to paramedical personnel and medical students who find computer-based educational programs challenging and interesting. 4
1 Department of Ophthalmology, University oflowa, Iowa City. 2 Department of Pathology, University of Iowa, Iowa City. 3 Weeg Computing Center, University oflowa, Iowa City. 4 University of Iowa Video Center, Iowa City.
Presented in part at Scientific Exhibits at the Annual Meetings of the American Academy of Ophthalmology from 1989 through 1992.
Supported in part through an unrestricted grant and a Senior Scientific Investigator Award (Dr. Folberg) from Research to Prevent Blindness, Inc, New York, New York, grants from IBM, Armonk, New York, Apple Computer, Cupertino, California, and 3M Corporation, St. Paul, Minnesota, Educational Development grants from the University of Iowa College of Medicine, and a grant from the University of Iowa Video Production Fund, Iowa City, Iowa.
None of the authors has an individual proprietary interest in any of the hardware or software products mentioned herein, but the University of Iowa Department of Ophthalmology has a financial interest in the programs, Pathology of the Eye and Basic Ophthalmology.
Reprint requests to Robert Folberg, MD, University oflowa, 100 Medical Research Center, Room 233, Iowa City, lA 52242-1182.
842
In contrast, Pathology of the Eye3 was written as a complete basic science course in ophthalmic pathology for residents and for use by practicing ophthalmologists

Folberg et al · Interactive Basic Science and Continuing Medical Education
as continuing medical education. For example, one of the modules in this program, a clinicopathologic approach to the diagnosis of eyelid lesions, was presented in a classroom format as a 2-hour course at two meetings of the American Academy of Ophthalmology (the content of the course was co-developed with Dr. David T. Tse, currently at the Bascom Palmer Eye Institute, University of Miami, Miami, FL). Other sections of Pathology of the Eye? have been presented in the classroom as continuing medical education courses and seminars. With Pathology ofthe Eye? as a frame of reference, we explain the rationale for using interactive media in ophthalmic basic science and continuing medical education curricula and describe the issues involved in program development. We also compare two different delivery platforms for interactive multimedia education: interactive videodisc (IVD) and compact disc-interactive (CD-I).
The topic of ophthalmic pathology was selected because ( 1) this subject is required in ophthalmic residencies, (2) ophthalmic practitioners show a high interest in reviewing this field as part of their continuing medical education, (3) there is a strong precedent for involving interactive technologies in pathology education, 1.4- 14 and (4) IVD is effective in teaching pathology. 12 It may be useful at this point to define and describe IVD and CD-I.
A 12-inch videodisc is a permanent medium: once pressed, no additions or changes may be made. Unlike a long-playing phonograph record, the videodisc is read by a laser instead of a stylus. The videodisc is therefore very durable and resistant to wear. Each side of a videodisc may hold up to 54,000 still images, 30 minutes of fullmotion video, or a combination of still images and fullmotion video. Two 30-minute sound tracks are available to accommodate multilingual instruction. The videodisc is an analog rather than a digital medium, which means that the signal from the videodisc player must either be displayed as a television picture on a computer monitor or must first be digitized before being displayed. Unfortunately, video standards are not uniform throughout the world and a videodisc manufactured for play in the United States under the NTSC standard will not play in most European countries which use the PAL video standard. A videodisc may be used at different levels. The levels of interactivity and the corresponding hardware and software requirements are summarized in Table 1. 15
Pathology of the Eye? is a level III IVD program. The image read by the videodisc player is transmitted to the microcomputer as a television signal. Hardware in the
microcomputer or its display apparatus integrates the television signal with text and graphics on the same screen (IBM Info Window display, Fig 1), or a graphics board in the microcomputer digitizes the analog television signal from the videodisc player and displays this image on the monitor along with text and graphics (IBM M-motion video adaptor). Full-screen, full-motion video may be used with existing hardware because the videodisc stores information in analog format.
In explaining the differences between IVD technology and CD-I, it also is helpful to describe CD-ROM. The CD-ROM disc measures approximately 5 inches in diameter. Unlike the videodisc, the CD-ROM disc stores audio and video data in digital rather than analog format. Images and audio, captured in digital form, may reside together with the program logic on this permanent medium. A CD-ROM player is either built into or is attached to a computer. Typically, the CD-ROM disc also stores the program logic together with text and graphics that may be integrated into the presentation, although the program that controls the access to and interaction with information on the disc also may reside on the computer's hard disc. The user interacts with the program through the computer. At this time, full-screen, full-motion video is not yet available for this platform. The appearance of the digitized images on the CD-ROM disc depends on a number of issues including the quality of the digitization and the ability of the microcomputer's graphics board to display high-resolution images. We are currently developing a CD-ROM version of Basic Ophthalmology.2
CD-I discs look like CD-ROM discs, are permanent and contain digital video and audio together with the program logic. However, the CD-I player is connected to a television set or monitor (Fig 2) instead of a computer; a user never directly interacts with a computer, although computer hardware is housed within the CD-I player. The CD-I user interacts with the programs by using a handheld remote-control device. A joystick, operated by the thumb (a "thumbstick"), moves a cursor on the television screen, and the user issues commands to the CD-I player by depressing (clicking) a button on the remote control device ("point and click" mode); there is no keyboard interface.
CD-ROM and CD-I discs are formatted differently and generally must be played in a machine designed for the specific format. Both CD-ROM and CD-I players can play audio COs. The quality of audio on a CD-I disc ranges from AM radio to high-quality stereo. A CD-I disc may
Table 1. Levels oflnteractivity for Videodiscs 15
Level
II
III
Hardware
Videodisc player connected to a monitor
Videodisc player connected to a monitor
Videodisc player connected to 1 or 2 monitors and a microcomputer
Program Control
None
Recorded on 1 of the audio tracks of the videodisc
Stored on floppy discs, the computer's hard disc, a removable storage device, or a CD-ROM disc
lnteractivity Permitted
Linear play, pause, stop, and search for specific frames on the videodisc
Interactivity is constrained by limited memory in the videodisc player
Permits complex branching, analysis of user responses, and integration of text and videodisc
843

Ophthalmology Volume 100, Number 6, June 1993
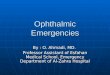
Figure 1. An IBM Info Window interactive videodisc unit. The videodisc player (black box to the left of the keyboard) is connected to the central processing unit of the computer (on the floor) and the monitor. An optional external disc drive rests on the videodisc player. The picture in the upper right corner of the screen is being displayed as a television signal from the videodisc player; all other screen elements are generated by the computer. With this configuration, users may interact with the program using the monitor's touchscreen, the mouse, or the keyboard.
hold up to 19 hours of low-quality audio; this makes it a rather convenient platform for multilingual instruction. Unlike videotapes and computer programs distributed on diskettes, CD-I programs cannot be duplicated (the actual software resides on the CD together with digitized audio, video, and graphics information). Full-motion video is not available on the CD-I platform at this time, although this feature is anticipated shortly. Compact disc-interactive discs are manufactured using an internationally recognized standard. Therefore, a properly designed CD-I disc can be played on any CD-I player and television set in the world. Recently, manufacturers have introduced portable CD-I players that are just slightly larger than portable audio CD players.
There are other interactive CD formats. Compact disc television from Commodore Computers (West Chester, PA) and the Video Information System from Tandy Corporation (Fort Worth, TX) also deliver interactive programs through television. The CD-I, CD television, and Video Information System formats are incompatible with each other. Photo-CD (Eastman Kodak, Rochester, NY) is compatible with CD-I. Photo-CD permits high-quality photographs to be encoded onto a CD for retrieval. The photographs stored on Photo-CO discs may be manipulated with specialized software.
Rationale for Using Interactive Technologies in Basic Science and Continuing Medical Education
One might argue that the combined use of text, graphics, and audio, sometimes designated as "multimedia," is not justified in medical education unless it can be shown that this technology either increases comprehension and retention or improves the efficiency oflearning (i.e., shortens the learning time). In fact, in one study, IVD substituted
844
for a portion of second-year medical student pathology lectures, and a comparison of pre-testing and post-testing showed a significant improvement, thus indicating that IVD could substitute for lectures. 12 However, the issue is not only whether new instructional technologies are superior to traditional methods, but also whether multimedia platforms such as lVD and CD-I offer opportunities for learning that are not otherwise available.
Comparison between Conventional Learning Tools and Interactive Multimedia
There is no one accepted definition of multimedia. Loosely defined, any technology that integrates different methods of transmitting data (text, audio, still photographs, static graphics, animations, full-motion video) uses "multimedia." Using this definition, a videotape on refraction techniques is multimedia (the tapes are narrated and frequently contain animations, motion pictures, and a variety of still images). With IVD, CD-ROM, or CD-I, a user can branch from one part of the presentation to another easily; the only interactions available to a videotape viewer are pause, fast forward, or reverse. To understand the advantages that interactive multimedia educational platforms offer, it is helpful to review the advantages and disadvantages of conventional teaching.
Books
Books are portable; they may be used nearly anywhere. Books can be interactive, in that the reader may skip from topic to topic, consult the index to look up a reference to related subject material, check citations to the scientific literature, and have access to illustrations that supplement the text. Unfortunately, most books do not provide feedback to help the reader determine whether the material studied is properly understood. Also, some features of a book may be inconvenient or awkward to use. For example, if the reader encounters an ambiguous term in a textbook, and if the reader is ambitious, the term must be found in the index and then located and studied before returning to the original place in the book.
It may be prohibitively expensive to publish large numbers of high-quality color photographs in books. Authors even disagree how to label the photographs. Some authors contend that pictures are best examined if they are unlabeled so the reader can study the illustration in its natural setting; by their very presence, labels and arrows call attention to important features. Providing illustrations with clear plastic overlays that may be flipped aside might solve this problem, but this is an expensive and impractical solution for large numbers of pictures. In Yanoff and Fine's16 extensive color atlas of ophthalmic pathology, sketches of the illustration appear next to the illustration itself. The sketch, not the original picture, is labeled. The reader must mentally superimpose the sketch over the illustration, but at least the illustration is presented without any interference by labels.
Finally, it is difficult to design book illustrations for teaching pathophysiology. Recently, some textbooks of systemic pathology have offered a series of color cartoons

Folberg et al · Interactive Basic Science and Continuing Medical Education
--
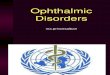
Figure 2. A television monitor rests on a CD-I player (Philips Consumer Electronics, Knoxville, TN). Users control CD-I programs with the handheld remote control device.
to illustrate changes in morphology or physiology over time. 16
•17 These cartoons depict static stages in a contin
uum of events, and the reader must reconstruct the connections between each stage.
Lectures and Courses Unless a teacher directly challenges an audience to participate in a lecture, the potential for a dynamic interchange between instructor and audience may be wasted. In the setting of continuing medical education, teachers may be reluctant to question seminar participants to avoid embarrassing a member of the audience. Likewise, few physicians ask questions at a lecture (even if the format of the presentation and time permit questions from the floor) for fear of exposing "ignorance" before a group of peers. Lectures are not only passive experiences, they are also linear: an individual in the audience must sit through portions of the subject matter that are already familiar (one cannot "fast forward"). Similarly, there is little opportunity for individuals in the audience to "replay" difficult material.
Lectures and courses must be scheduled at fixed times. It may be inconvenient for a physician to break away from practice to attend a continuing medical education seminar. Smaller courses are beginning to report a decrease in attendance. Not only is it expensive to attend a course, it is also expensive to pay staff to mind the office.
In addition, physicians who attend courses may be anxious because a "competitor" at home may care for their patients. At a large, well-attended conference, such as the Annual Meeting of the American Academy of Ophthalmology, several compelling presentations may compete at one time for the physician's attention. As the medical economic environment contracts, physicians may have to work harder to maintain their incomes and will have to budget time carefully to meet continuing medical education requirements.
Slide Sets
Instructional material can be packaged as 35-mm slides or, in the case of a pathology course, as glass histopathology slides. The printed material that may accompany a slide set presentation may ask questions of the user and provide written feedback (i.e., the correct answer). Therefore, slide set presentations may provide an active rather than passive learning experience. Although slide sets are not as portable as textbooks (slide sets require access to a projector or a microscope), the user can choose when to use the material, in contrast to the fixed schedule of a lecture. However, we have encountered three major drawbacks to the use of slidesets: ( 1) slides are frequently broken or lost and cannot be easily replaced, (2) no feedback is provided to the instructor concerning how well the material is mastered, and (3) no feedback is offered to the user.
Videotapes
Videotapes are well-suited for full-motion presentations such as operations. Watching a videotape, however, is largely a passive experience: the user can only interact by pausing, rewinding, or "fast-forwarding." No feedback is provided to either the curriculum designer or to the user. Although the distribution of videotapes is cost-effective, they can be easily reproduced and the developer's investment in developing a videotape curriculum may not be recovered because of unauthorized duplication. Although there is little or no profit from the development of medical educational materials, a medical educator who fails to recover some of the production expenses may not be capable of further educational productions. On the other hand, videodiscs, CD-ROM discs, and CD-I discs cannot be duplicated without considerable expense and effort.
Pathology of the Ey€? was designed to incorporate the best educational features of conventional learning methods (textbooks, lectures, slide sets, and videotapes) and to use interactive technologies to overcome many of their shortcomings.
Pathology of the Eye Interactive Videodisc Program: Hardware, Course Content, and Multimedia Features
Pathology of the Ey€? was designed to be a single-screen level III IVD program (i.e., information that controls interaction with the program is displayed on the same screen
845

Ophthalmology Volume 100, Number 6, June 1993
Inflammation Herpes Zoster
Note the prominent corneal nerves, a cl inical reflection of perineural inflammation.
Inflammation Herpes Zoster
Note the prominent · corneal nerves, a clinical reflection of perineural inflammation.
Top left, Figure 3. This figure and Figs 4 to 9 are screens from the Macintosh II version of Pathology of the Eye. 3 The composite illustration on the screen has been digitized by a board in the Macintosh. The buttons at the bottom of the screen control navigation through the program: the reverse arrow takes the user back one screen; the button labeled "M" takes the user to the previous menu; the button labeled "G" takes the user to the glossary to look up a term; buttons labeled "1-4" enlarge their respective pictures on the screen; buttons labeled "5-8" give more information about each picture, respectively; and the forward arrow advances to the next screen. In this screen, the cursor, in the shape of a hand, is over the "more information" button for the cornea pictured in the upper right.
Bottom left, Figure 4. This is the "more information" screen for the upper right screen image selected in Figure 3. If the user does not understand the information being displayed on the screen, selecting "more information" again would generate the screen shown in Figure 5.
Top right, Figure 5. By clicking over the button labeled "1," the user could enlarge this image (see Fig 6).
Bottom right, Figure 6. The outline of the nerve can be removed easily by clicking over the "more information" button again (see Fig 7).
as video and graphics information retrieved by the software, Fig l ). This program was originally written to run on IBM PS/2 computers equipped with either an Info Window (IBM) display or the IBM M-motion video adapter. The Info Window display offers the user the opportunity to interact with the program using a touchscreen. A keyboard or mouse also may be used with either an Info Window display or theM-motion video adapter. Although use of the touchscreen is optional, it does provide some interesting educational opportunities. For example, when a touchscreen is available, a user may press on a photograph of an eye with Vogt's striae in keratoconus: when the screen is touched, the striae fade, as if the user had pressed on the eye of a patient to accomplish the same effect.
846
Pathology of the Ey~ was redesigned to run on the Apple Macintosh II line of microcomputers (Cupertino, CA), equipped with a Videologic DV A-4000 video overlay board (Videologic Corporation, Cambridge, MA) (which, like the IBM M-motion video adapter, digitizes the analog television signal generated by the videodisc player). The text, graphics, pictures and special features are identical in each version of the program. The Macintosh version ofthe program features an icon-oriented interface.
Pathology of the Ey~ was designed as a complete course in ophthalmic pathology. Twelve subjects are covered in detail: a review of the general concepts of systemic pathology as they apply to the eye, surgical and non-surgical trauma, cornea, conjunctiva, eyelids, retina and vitreous, intraocular tumors, phakomatoses, lens, congenital

Folberg et al Interactive Basic Science and Continuing Medical Education
Top left, Figure 7. The outline of the nerve has been removed. By clicking over the arrow at the lower right corner, the user returns to the screen shown in Figure 3.
Bottom left, Figure 8. This is one screen from an interactive cartoon. In the program, this screen is followed by an actual photograph of the lesion.
Top right, Figure 9. This is a screen from a patient management section of the program. The user is asked to type in the answer.
Bottom right, Figure 10. Screen from the CD-I version of the section on the optic nerve that was redesigned from the videodisc program. The user is challenged to click over the nerve fiber layer infarct.
anomalies, orbit, and the optic nerve. Glaucoma is covered throughout the course. More than 35,000 still images appear on the videodisc, representing clinical photographs, gross pathology photographs, photomicrographs, ultrasonograms, radiologic studies including computed tomographic and magnetic resonance imaging scans, and transmission and scanning electron micrographs.
Interaction with the program is illustrated in Figures 3 to 6. Figure 3 shows a screen from the inflammation subsection on the fundamentals of pathology. The four illustrations provide clinicopathologic correlations for herpes zoster ophthalmicus. The user may elect to receive more information about any of these pictures. If the user wants information about the illustration in the upper right portion of the screen, the program would display the screen shown in Figure 4. The text that accompanies the picture points out the enlarged corneal nerve. If the user does not see the enlarged nerve, a graphic pointing out
the nerve may be pasted over the picture (Fig 5). The picture also may be enlarged (Fig 6) and the graphic toggled off (Fig 7) and on (Fig 6) as often as desired.
Other features include an online glossary that can be accessed directly from any screen in the course. If users are uncertain about the definition of a term, they need only select the highlighted term within the text and the program displays a definition of the term, coupled with an illustration and references to other places in the course which contain more information about the subject. When the user has finished consulting the glossary, the program returns the user to their original place. Users also may choose to browse through the illustrated list of 529 entities.
Clinicopathologic correlations and pathophysiology are taught by interactive animations (Fig 8). A variety of quizzes appears throughout the program as well. Users also are given the opportunity to apply their knowledge of pathology by managing patients (Fig 9).
847

Ophthalmology Volume 100, Number 6, june 1993
Development of the Program
The curriculum for Pathology of the Eye'3 was developed first for classroom presentations over a period of 6 years. The original text used in the program was derived from handouts distributed to students, and pictures used in the program were identical to those shown in the classroom. Developing the curriculum first for the classroom exposed us to difficulties that students were likely to experience in learning certain concepts. Also, the foils for quizzes (i.e., incorrect choices on multiple choice examinations) were taken directly from incorrect answers offered by students in classroom settings.
All of the illustrations used in the program were either in the public domain, or were donated by current or former faculty members of the Department of Ophthalmology at the University of Iowa. The program used no illustrations that had been copyrighted. To encourage the donation of photographic material, each donor of an illustration was assured that the picture might be used in subsequent publications. Material that first appeared on this videodisc has been used subsequently in scientific papers with proper acknowledgments. 18
The development team included instructional designers and graphic artists. All of the animations and medical art were original and commissioned for this program. A team of programmers spent 3.5 years developing and testing this program. The program was made available on both the IBM and Macintosh platforms as part of a research project both to determine the relative ease of development on these two major platforms and to reach as many potential users as possible. We discovered that there are no solutions that permit developers to "port" applications from one platform to another without some elements of redesign and reprogramming. The expense of producing Pathology of the Eye'3 for both the IBM and Macintosh platforms exceeded $100,000.
Acceptance of the Program for Continuing Medical Education
At the 1990 annual meeting of the American Academy of Ophthalmology, 36 individuals registered for one of three sessions, at which time they were permitted to browse through any portion of Pathology of the Eye3 for up to 3 hours. Twenty-three (65%) of these individuals were ophthalmic practitioners, taking the course for continuing medical education; the rest were residents. All of the registrants completed a detailed questionnaire concerning the suitability of the course for individualized continuing medical education. Most participants preferred the medium of interactive education to textbooks (62%), videotapes (68%), and lectures (72%). Most participants (89%) said that they would take another interactive course or would recommend this method of instruction to others.
Anecdotal comments suggested that the material might be "too easy." This criticism was surprising, because the same material, presented in classrooms as lectures or seminars, was often criticized as being "too difficult." Perhaps by permitting the user to control the pace and
848
order of the presentation in the videodisc presentation, "difficult" material became "easier"; the course content (text and illustrations) in both the classroom presentations and IVD program was identical. In the past 2 years, we have demonstrated this program to more than 200 physicians, many of whom were concerned about the cost of the required hardware. Also, although the programs themselves are easy to use, some expertise is required to install and configure the hardware.
Compact Disc .. Interactive for Continuing Medical Education
Our interviews with physicians who might use interactive technologies for continuing medical education disclosed that the "ideal" multimedia platform should be inexpensive to purchase, easy to operate, and available in the office or home. Currently, the CD-I player costs less than $600, requires no instruction to operate, and is easily connected to any television set. Currently, many commercial CD-I programs are available as games, for early childhood instruction, and as sources of information (e.g., a museum tour). Some medical educators were skeptical about using CD-I because they doubted that medical images could be displayed with fidelity on television, and because CD-I was considered to be suitable only for entertainment.
We redesigned a portion of the optic nerve segment from the videodisc version of Pathology of the Eye'3 for CD-I. The text that appeared in the IVD program was converted into a voice-over narration. This demonstration program was produced with both English and Spanish narration to demonstrate the potential for multilingual education. We were able to maintain all of the features of the computer-based IVD version (including hypertext, a glossary look-up function, and complex branching) in the CD-I version.
We demonstrated to our satisfaction that there is no significant degradation in the quality of photographs or illustrations on the CD-I platform. We also discovered that computer-based materials cannot be directly "ported" to CD-I. First, most computer-based teaching materials depend on the presentation of text. Most viewers would object to reading large quantities of text from a television screen. Also, most television viewers are accustomed to rapid changes in the composition of a television screen (many informational or instructional television programs feature some type of screen change as often as every 3 to 6 seconds). Therefore, although some principles of instructional design cross over from computer-based instruction to television-based instruction, attention must be paid to the medium of television when designing a CD-I program.
We were able to develop a highly interactive CD-I program. It is difficult to convey the impact of the simultaneous stimulation ofthe user's senses of sight and sound and the requirement that the user perform an action (manipulate the "thumbstick" and click a button) to make something happen on the screen. For example, at one point in our CD-I program, we challenge the user to find

Folberg et al · Interactive Basic Science and Continuing Medical Education
a nerve fiber layer infarct by clicking over the zone of pathology displayed on the television screen (Fig 10). If the user clicks to the left of the infarct, the narrator urges the user to "move to the right." If the user misses the infarct again by clicking too far to the left, the narrator responds, "move a bit more over to the right." The user gets the impression that there is a teacher built into the program.
We had the opportunity to allow physicians to compare the videodisc version of the optic nerve course to the CDI version of this material at the 1991 Annual Meeting of the American Academy of Ophthalmology, where both programs appeared side-by-side at a scientific exhibit. Of the more than 184 individuals who visited the exhibit, at least 20 viewed both the IVD program and the CD-I program; all but one preferred the CD-I version to the IVD. Some of the reasons for this preference may be related to the novelty of CD-I (many of the ophthalmologists had seen a computer-based tutorial, but none had ever seen a CD-I player because consumer versions of these players had not yet been made available to the public). However, the preference for CD-I as a vehicle for continuing medical education may be based on the method of presentation. Many of the ophthalmologists who compared the platforms volunteered that the IVD program was an interactive textbook, whereas the CD-I program was an interactive private tutorial with a teacher. The individual who preferred the IVD program to the CD-I presentation preferred textbooks to lectures.
Discussion
The fact that a program is interactive and uses multimedia does not make it an effective teaching tool. In the field of multimedia education, more attention is often directed to technologic issues (what platform is used, what special effects can be used) than to the effectiveness of these tools in educating the target audience.
Interactive videodisc, CD-ROM, and CD-I programs can be written as personalized teaching tools. In each platform, the individual who writes the scientific material controls the content while the user may control the order of the presentation, the pace of the program, and the amount of supplemental information that is viewed. Interactive programs present the opportunity for personalized instruction; they may be used either by small groups or by individuals. When used by individuals, interactive platforms such as IVD, CD-ROM, and CD-I can offer a private learning environment, free from the risks of public embarrassment. The subject matter itself may be personalized. For example, an interactive program on any platform might begin by asking a physician to enter a practice profile. A program on molecular genetics might provide a core curriculum suitable for all physicians, but might tailor the self-assessment problems to the subspecialty: ophthalmologists would "manage" patients with inherited retinal disorders, whereas internists might manage patients prone to some forms of cancer. Programs also could be designed to provide different levels of information within
a specialty, such as basic and advanced topics, and to provide feedback to the user.
Programs written for computer-based platforms such as IVD and CD-ROM may track a user's progress and record a user's answers to questions posed during the presentation. It is possible to track a user's progress through a CD-I program. Some versions of CD-I players are equipped with a floppy disc drive for this purpose, and some CD-I models are equipped with RS-232 ports, which makes it theoretically possible to link these players to remote sites through modems. Thus, it might be possible for an individual using a CD-I player to "log-in" (perhaps using a social security number), go through a CD-I course, and verify participation in continuing medical education by modem, although we are not aware of the implementation of these remote links using CD-I.
Medical students and residents may have easier access to computer-based IVD or CD-ROM programs in a library or learning center than practicing physicians. In the setting of a medical school or clinic, the cost of purchasing a multimedia computer can be partially justified by the large numbers of potential users served by the equipment. Some computer-based programs that use only digitized materials may be distributed across a network.
Placement of a multimedia computer with high-quality educational programs in a residency program may free faculty from teaching repetitive material (e.g., from offering the same introductory course each year). At the University of Iowa, we substitute the videodisc course, Pathology of the Eye, 3 for annual basic science lectures (it takes an average resident 25 to 35 hours to complete the videodisc course). Residents are expected to have completed the course before they start their ocular pathology rotation. Thus, they are well prepared for their laboratory experience, and the pathologist is free to concentrate on advanced, rather than basic, topics. These courses do not replace teachers; they free instructors to teach at a higher level.
To be fair, the interactive television-like features built into our CD-I demonstration program could have been implemented in our videodisc version. Why, then, produce programs for CD-I? Although computer-based multimedia platforms such as IVD and CD-ROM may occasionally be found in homes, CD-I players are mass marketed to individuals for use with their home television sets. In addition, a consumer-model CD-I player is currently priced at approximately 25% of the cost of a multimedia computer necessary to run IVD or CD-ROM programs. Finally, one need not know how to operate a computer to use a CD-I player (CD-I players are considerably easier to operate than videocassette recorders because there is nothing to program). A delivery platform, like CD-I, that is relatively affordable, that is designed for home use, and that is easy to operate may be an ideal vehicle for continuing medical education.
In selecting technology for the development of educational materials, the educator should first define the target audience. Will these materials be designed for and distributed to organizations with shared resources (e.g., residency programs) or to individuals? Organizations with shared resources might be able to afford computer-based
849

Ophthalmology Volume 100, Number 6, June 1993
technology, either analog (e.g., videodisc) or digital (CDROM). Individuals are more likely to be able to afford consumer-oriented technologies such as CD-I that offer all of the advantages of interactive multimedia education.
At this time, there are two major obstacles to the development of interactive programs for basic science and continuing medical education. First, the development cost of these programs is prohibitive and it is very difficult to obtain grants for their design and production. Second, some would argue that research in medical education is not really research. Yet, the development of a new method for medical education can be as time consuming as the formulation of a bench-research technique. Like the bench researcher who assumes risk in attempting to uncover new information, the educator assumes considerable academic risk in developing improved techniques to teach. Attention must be directed not only toward the use of new instructional technologies, but also toward the accuracy of the information being taught. Thus, the development and production of an interactive program is far more complex than authorship of a textbook. Nevertheless, many medical schools do not grant the same level of academic recognition to a research project in medical education as authorship of original journal articles or textbooks. Until institutions set into place a mechanism for the review of such new instructional techniques and programs and are prepared to grant academic recognition toward tenure for such efforts, junior faculty may consider the financial and academic risks of research in medical education to far outweigh its considerable rewards.
References
1. O'Neill PN. Developing videodisc instructions for the health sciences: a consortium approach. Acad Med 1990;65:624-7.
2. Farrell T A. Basic Ophthalmology: An Interactive Videodisc Program. Iowa City: Department of Ophthalmology, University of Iowa, 1991. Available from: The Department of Ophthalmology, University of Iowa, Iowa City, lA 52242.
3. Folberg R. Pathology of the Eye: An Interactive Videodisc Program. Iowa City: Department of Ophthalmology-Uni-
850
versity of Iowa, 1991. Available from: The Department of Ophthalmology, University of Iowa, Iowa City, lA 52242.
4. Xakellis GC, Gjerde C. Evaluation by second-year medical students of their computer-aided instruction. Acad Med 1990;65:23-6.
5. Templeton AC. Videodisc-computer technology in the teaching of pathology. Physiologist 1985;28:432-42.
6. Thursh DR, Mabry F, Levy AH. Computers and videodiscs in pathology education: ECLIPS as an example of one approach. Hum Pathol 1986; 17:216-8.
7. Mercer J, Pringle JH, Rae MJL, et a!. How do we teach pathology? The laser videodisc and computer-assisted learning. J Pathol 1988;156:83-9.
8. Woods JW, Jones RR, Schoultz TW, eta!. Teaching pathology in the 21st century. An experimental automated curriculum delivery system for basic pathology. Arch Pathol Lab Med 1988;112:852-6.
9. Jansen W, Baak JPA, Smeulders A WM, van Ginneken AM. A computer based handbook and atlas of pathology. Pathol Res Pract 1989; 185:652-6.
10. Levy AH, Thursh DR. The implementation of a knowledgebased Pathology Hypertext under HyperCard. J Med Syst 1989;13:321-9.
11. Valdes-Dapena M, Valdes-Dapena AM. A senior elective program in anatomic pathology. Arch Pathol Lab Med 1989;113:330-2.
12. Jones R, Schoultz T. Teaching pathology in the 21st century: assessment of required student use of interactive videodiscs designed to teach basic pathology. Hum Pathol 1990;21:6-10.
13. Kumar K, Hodgins M. Use of interactive videodisc for teaching of pathology laboratory cases. J Pathol 1990; 160: 145-9.
14. Nathwani BN, Heckerman DE, Horvitz EJ, Lincoln TL. Integrated expert systems and videodisc in surgical pathology: an overview. Hum Pathol 1990;21:11-27.
15. Ullmer EJ. Optical Disc Technology. [Bethesda, MD]: U.S. Dept. of Health and Human Services, 1990;9-10.
16. YanoffM, Fine BS. Ocular Pathology: A Color Atlas, 2nd ed. New York: Gower Medical, 1992.
17. Rubin E, Farber JL, eds. Pathology. Philadelphia: JB Lippincott, 1988.
18. Sneed SR, Weingeist TA. Management of siderosis bulbi due to a retained iron-containing intraocular foreign body. Ophthalmology 1990;97:375-9.