Embed Size (px)
Citation preview

Integration of Emergency Management
into Healthcare
Paul D. Biddinger, M.D. F.A.C.E.P.
MGH Endowed Chair in Emergency Preparedness
Director, Center for Disaster Medicine and Vice Chairman for Emergency Preparedness,
Department of Emergency Medicine, Massachusetts General Hospital
Medical Director for Emergency Preparedness, MGH and Partners HealthcareDirector, Harvard T.H. Chan School of Public Health Emergency Preparedness Research, Evaluation and Practice
(EPREP) Program

Overview
• Review of disaster epidemiology
• Benefits of an emergency management
approach
• Key components of a hospital-based emergency
management program
@MGHDisasterMed 2

Disaster Events are Increasing
Source: The Economist https://www.economist.com/blogs/graphicdetail/2017/08/daily-chart-19

Global Terrorism
4Source: Global Terrorism Index 2015

Active Shooter Events
Source: FBI

Emerging Infectious Diseases - 1984
Anthony Fauci Testimony to Congress 1984

Emerging Infectious Diseases - 2004
The challenge of emerging and re-emerging infectious diseasesDavid M. Morens, Gregory K. Folkers & Anthony S. FauciNature 430, 242-249(8 July 2004)

Factors Driving Disaster Impacts
• Population is:– Growing
– Increasingly urban
– Increasingly coastal
• 1B people live in coastal areas at risk of flooding
• Climate change
• Violent conflicts
• Global travel
• Changes in animal farming
• Others….
Hugo Ahlenius, UNEP/GRID-Arendalhttp://www.grida.no/graphicslib/detail/human-impact-in-the-coastal-zones_80d7

Healthcare Sector Emergency
Preparedness
• Essential for preservation of life and health
• Differs substantially from traditional first responder preparedness and response– Public health infrastructure tremendously varied in the
US
– Health care is delivered in many very different venues (acute hospitals, clinics, rehabs, nursing homes, etc.)
– Nearly all hospitals are private entities
– Little or no intrinsic coordination of entities
– System is at (or beyond) capacity on a daily basis

Healthcare Sector Emergency
Preparedness
• Increasing in visibility and importance
– Study of previous events more rigorous
– Demonstration of differences in outcomes
– Public demand for accountability
Why Utilize an Emergency
Management Approach?
• Improved incident recognition
• Improved mobilization of resources
• Standardized planning and response
• Improved situational awareness
• Enhanced coordination
• Faster recovery
@MGHDisasterMed 11

Healthcare Emergency
Preparedness Capabilities
• Capability 1: Foundation for Health Care and Medical Readiness – Health care organizations have strong relationships, identify hazards and
risks, and prioritize and address gaps through planning, training, exercising, and managing resources.
• Capability 2: Health Care and Medical Response Coordination – Health care organizations plan and collaborate to share and analyze
information, manage and share resources, and coordinate strategies to deliver medical care to all populations during emergencies and planned events.
• Capability 3: Continuity of Health Care Service Delivery – Health care organizations provide uninterrupted, optimal medical care to all
populations in the face of damaged or disabled health care infrastructure. Simultaneous response and recovery operations result in a return to normal or, ideally, improved operations.
• Capability 4: Medical Surge – Health care organizations deliver timely and efficient care to their patients
even when the demand for health care services exceeds available supply.
November, 2016 ASPR Healthcare Preparedness Program Capabilities

CMS Requirements
• Effective as of 2017, CMS now has Emergency
Preparedness requirements for Medicare- and
Medicaid-participating providers and suppliers
• The rule establishes national emergency
preparedness requirements to plan adequately
for both natural and man-made disasters, and
coordinate with federal, state, tribal, regional,
and local emergency preparedness systems
13

CMS’ EP Rule
• Applies to 17 provider and supplier types who must meet four core elements:1. Emergency plan – Must have a detailed plan based on a
risk assessment and use “all-hazards” approach
2. Policies and procedures - Must develop and implement policies and procedures based on the emergency plan and risk assessment that are reviewed and updated at least annually.
3. Communication plan - Must maintain an emergency preparedness communication plan that coordinates communications within the facility, across healthcare providers, with state and local public health departments and emergency management systems
4. Training and testing program – Must be able to demonstrate that staff have knowledge of emergency procedures and receive training at least annually. Must conduct drills and exercises to test the emergency plan or participate in an actual incident that tests the plan
14
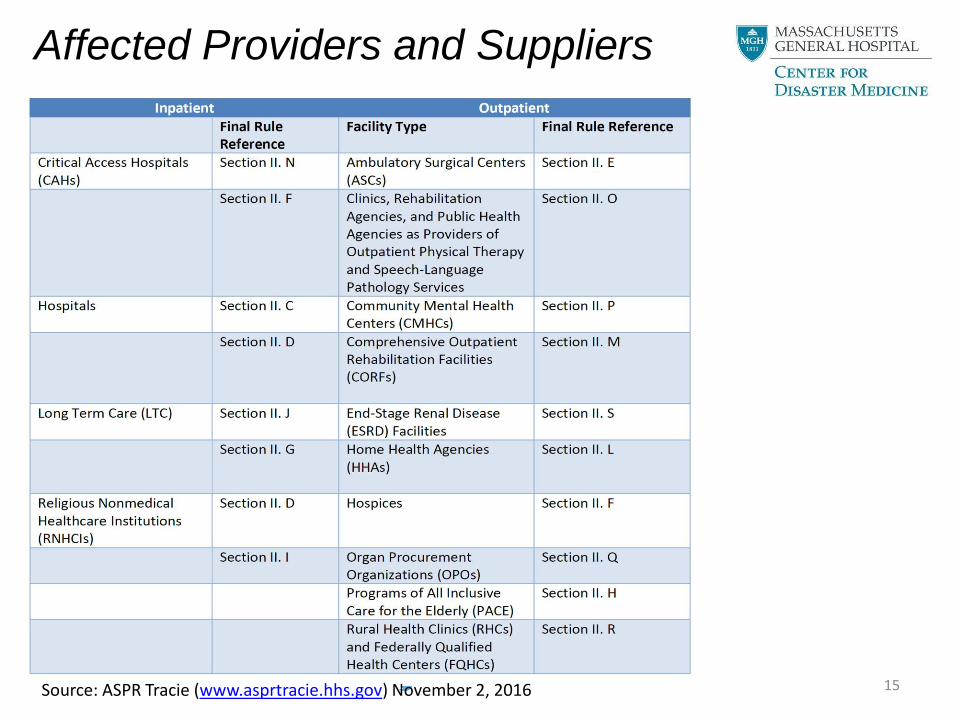
Affected Providers and Suppliers
15Source: ASPR Tracie (www.asprtracie.hhs.gov) November 2, 2016

The Disaster Management
Cycle
• Mitigation
• Preparation (planning)
• Response
• Recovery

Risk Assessment
• Effective emergency management depends on an a
hospital’s Hazard Vulnerability Analysis (HVA):
• A systematic approach to recognizing hazards that may
affect demand for the hospital’s services or its ability to
provide those services.
Probability Consequence Preparedness Risk

The Need for Evidence-Based
Planning
• Historically, disaster planning has often focused more
on “myths” and how we would like disasters to happen
rather than how they actually happen
– Auf der Heide, E. The Importance of Evidence-Based Disaster
Planning Annals of Emergency Medicine 2006 (47) 34-49
• When tragic events occur, lessons are often “learned”,
re-learned, and re-re-learned because they planners
were unaware of the science

Response
• By definition, disaster events start by overwhelming
capabilities and with chaos
• An ideal disaster response brings order to the chaos as
quickly as possible to make the best possible use of limited
capabilities
• To do this, a hospital needs:
1. A management system that best supports command
and control
2. Systems and technologies to support optimal situational
awareness
3. Efficient and interoperable mechanisms to integrate with
key partners in the response

The Incident Command
System
Incident Commander
Public Information Officer
Safety Officer
Liaison Officer
Medical Officer
Compliance OfficerChiefs of
Services
Biological Agent
Supervisor
Nuclear Agent
Supervisor
Chemical Agent
Supervisor
Optimum Care
Committee Consult
Logistics Section
Chief
Deputy
Logistics Sec.
Chief-Support
Deputy
Logistics Sec.
Chief-Service
Material
Supplies Unit
Leader
Information
Systems/
Technology
Unit Leader
Nutrition and
Food Services
Unit Leader
Planning Section
Chief
Workforce Unit
Leader
Nursing/Allied Health
Staff Emergency
Credentialing Manager
Physician Staff
Emergency
Credentialing
Manager
Situation Status
Unit Leader
Patient Tracking/
Capacity
Monitoring Unit
Leader
Finance Section
Chief
Time Unit
Leader
Compensation/
Claims Unit
Leader
Cost/
Procurement
Unit Leader
Inpatient Units
Division
Supervisor
Peri-Op Area
Division
Supervisor
ED Division
Supervisor
Psychological
Support Group
Supervisor
Ancillary
Services Group
Supervisor
Deputy Ops.
Sec. Chief-
Research
Adult Unit
Leader
Obstetrics Unit
Leader
Psych Unit
Leader
Critical Unit
Leader
Case
Management
Unit Leader
Operating
Room Unit
Leader
Post-
Anesthesia
Care Unit
Leader
Central Sterile
Processing Unit
Leader
ED Triage Unit
Leader
HazMat Unit
Leader
ED Minor Unit
Leader
ED Urgent Unit
Leader
ED Critical Unit
Leader
Respiratory
Care Unit
Leader
Pharmacy Unit
Leader
Radiology Unit
Leader
Laboratory Unit
Leader
Patient Support
Unit Leader
Family Support
Unit Leader
Police and
Security Unit
Leader
Biomedical
Engineering
Unit Leader
Security Advisor
Recovery/
Demobilization
Unit Leader
Infection
Control Unit
Leader
Staff Support
Unit Leader
Telecom Unit
Leader
Senior EM Advisor
Environmental
Services Unit
Leader
Outpatient
Adult Unit
Leader
Outpatient
Pediatric Unit
Leader
Offsite Unit
Leader
Outpatient
Procedural Unit
Leader
Cancer Center
& Procedural
Unit Leader
Operations
Section Chief
Employee
Services Group
Supervisor
Labor Pool
Manager
Volunteer/
Interpreter Services
Manager
Pediatric Unit
Leader
Facility Unit
Leader
Damage
Assessment
Manager
Facilities
Engineering
Manager
Transportation
Manager
Deputy Ops.
Sec. Chief-
Ambulatory
Outpatient
Psych Unit
Leader
Subject Matter Expert(s)
Documentation
Manager
Morgue Unit
Leader
Periop Services
Facilities Unit
Leader
Periop Services
MM Unit
Leader
20

Planning
• “…Plans are worthless, but planning is
everything. There is a very great distinction
because when you are planning for an
emergency you must start with this one thing:
the very definition of "emergency" is that it is
unexpected, therefore it is not going to happen
the way you are planning.”
Dwight D. Eisenhower. From a speech to the National Defense Executive Reserve Conference in Washington, D.C. (November 14, 1957)

“The Plan”
Well established processes for:
• Recognizing an “incident”
• Activation & notification
• Effective mobilization
• Rapidly achieving and maintaining situational awareness
• Timely and informed decision-making
• Effective implementation of decisions…
• Demobilization & return-to-readiness

MaHIMS Management Process
MANAGEMENT BY REACTION(Reactive)
Response Phase
Notification
MANAGEMENT BY OBJECTIVE(Proactive)
Response Phase
IncidentRecognized
First Response& initial
assessment
TacticalManagement
addressesimmediate needs
TransitionalMANAGEMENT
MEETING
establishesIncident Manager (IM)
& possiblyUnified Management (UM)
IM/UM sets overall
incident objectives& priorities
MANAGEMENT
MEETING
evaluates & revisesincident objectives
Assess progressutilizing measures
of effectivenessExecute AP &
initiate planningfor the next
Operational Period
Information processing²
& Supportive Plans³ development
OPERATIONS
BRIEFING
briefs theoperational
leaders on theAP
PLANNING
MEETING
develops incident strategy & tactics to
accomplish the incident objectives
The Planning
Cycle
Beginningof Operational
Period
Action Plan
(AP)¹
preparation
& approval
Figure adapted from: Planning Cycle, U.S. Coast Guard Incident Management Handbook,U.S. Coast Guard COMDTPUB P3120.17 April 2001
¹ ACTION PLAN (AP): A written description of the incident
objectives, strategies, tactics, and supporting plans for a
specific operational period.
² INFORMATION PROCESSING:
• Community health surveillance
• Patient tracking
• Resource status
• Boundary functions information
• Expert information
• Functional area reports
³ SUPPORTIVE PLANS:
• Health & Safety Plan
• Event Epidemiological Projection
• Alternative Strategies
• Contingency & Long-Range Planning
• Demobilization Planning

HCF A HCF CHCF B Healthcare Asset Management(EMP+EOP using incident management)
1st Tier
Medical Surge Capacity & Capability:
An Integrated Management System
2nd TierHealthcare “Coalition”(Mutual Aid & Support/Info Sharing/Coordination)
Jurisdiction I
(PH/EM/Public Safety)
Non-HCF
Providers
Medical
Support
3rd TierJurisdiction Incident Management(Medical IMS & Emergency Support-EOC)
4th Tier
Jurisdiction II
(PH/EM/Public Safety)
State Response & Coordination of Intrastate Jurisdictions
(Management coordination & support)
5th Tier
Federal Response(Support to State & locals) 6th Tier
Interstate Regional Coordination(Management coordination & Mutual
support)State A State B
Federal Response
(Regional & National)

Healthcare Coordinating Coalitions
@MGHDisasterMed 25

Specialty Responses
• Specialty annexes to the Emergency Operations Plan (EOP) must be developed to respond to unique situations that require special pre-planning and capabilities:– Mass casualty incidents (MCIs)
– Novel infectious disease outbreaks
– Hospital evacuation
– Active shooter/security threats
– Information systems downtime events
– Utility failures
– Chemical/hazmat events
– Nuclear/radiological events
– Inpatient and/or outpatient “surge”
– Fire
– Others

Anticipatable Challenges with
MCI Response
• The hospital’s notification interval will be very short, if it
exists at all
• Incident information will be inaccurate, incomplete, or
both
• The closest hospital is likely to be overwhelmed
• Patient distribution to other facilities may be uneven
• Patients will arrive by mechanisms other than EMS
• The ED and hospital will likely be full
• Triage must be brief, but must also be repeated
• Morbidity and mortality are likely to rise when the system
gets saturated
27

Hospital Actions Required
Within 5-10 Minutes
• Assess available information about the incident
• Notify hospital and departmental leadership
• Establish a command structure
• Secure the facility
• Communicate with on-site staff about the event
• Move existing patients out of the ED
– ED staff
– Admitting office
– Nursing supervisors
– Hospitalists/internists
– Patient transporters
• Prepare for MCI triage and patient tracking
28@MGHDisasterMed

Hospital Actions Required
Within 5-10 Minutes
• Mobilize maximal number of bedside staff to conduct multiple simultaneous resuscitations– Emergency medicine
– Trauma surgery
– Surgical subspecialists
– Anesthesia
– Others
• Mobilize sufficient supporting personnel, materials and resources – Imaging (X-ray, CT, others)
– Respiratory care
– Blood product support
– Lab evaluation
– Physical carts of resuscitation supplies
29

Essential Elements of a
Hospital MCI Protocol
1. Facility security
2. Triage
3. Patient registration
4. Patient tracking
5. Creation of immediate
ED capacity
6. Creation of
resuscitation teams
7. Creation of OR
capacity
8. Creation of support
capacity
• Blood bank
• Labs
• Imaging
• Morgue
9. Creation of inpatient
capacity
30@MGHDisasterMed

Training and Exercising
• Historically, the major focus of preparing clinical responders
for disasters has been via didactic education
• However, few clinicians remember much, if any, of this
training after 6-12 months
• Few also know specifically what their roles and responsibilities
in such events would be
• Robust disaster exercise programs are needed to find flaws
in plans and to train staff before the disaster occurs
• Performance in a disaster is highly correlated with having been
involved in a previous disaster

Special Tools to Support
Communication and Coordination
• Electronic notification systems– Private systems
– HHAN
• Web-based secure portals– WebEOC
• Alternative communications technologies– Radios
– Satellite phones
– HAMs
– Others…..

Persistent Challenges
• Access to disaster planning expertise
• Adequately supporting training and readiness
• Creating surge capacity
– Staff
– Stuff
– Space
• Funding

THANK YOU