Embed Size (px)
Citation preview

Integrating Risk-based Care for Patients With CKD in the Community
Navdeep Tangri MD PhD FRCPC Associate Professor, Division of Nephrology Dept. of Medicine and Dept. of Community Health Sciences Seven Oaks General Hospital, University of Manitoba Adjunct Associate Professor, Division of Nephrology Tufts Medical Center, Tufts University

Background
• About 600,000 Canadians with Stage G3 CKD
• Most managed in primary care
• Some patients progress quickly
• In other, kidney function can remain stable for years

Background
• Low risk individuals
– Unnecessary anxiety – Burden of the chronic disease label – Psychological distress, absenteeism from work, & diminished quality of
life

Background
• Higher risk individuals who are under-recognized
– Limited opportunity to learn about CKD & take actions to control risk
factors & delay or prevent progression to kidney failure
– Less likely to choose home dialysis or a permanent vascular access
– Higher risk of hospitalizations & early mortality

Background
• Health system
– Increased wait times for urgent cases
– More rapid disease progression
– Inadequate preparation for dialysis and/or kidney transplant
Why Risk Prediction?
• Early & appropriate nephrology care
• Prognostic Information for patient & provider
• Clinical trial enrollment • Dialysis resource management

Kidney Failure Risk Equation (KFRE)
• The KFREs accurately predict the risk of kidney failure requiring dialysis in patients with CKD Stages 3-5 for up to 5 years
• Risk prediction is accurate across multiple countries & subpopulations
• The KFRE is simple & highly accurate, & can be integrated into clinical practice
• It is accessed online > 30,000 times a month

4 Variable Equation

Published Online First April 11, 2011
Available at
www.jama.com

Knowledge Translation
Risk Factor Units (Type Over Placeholder Values in
Each Cell) Notes Age years 50 Sex male (m) or female (f) m Estimated GFR ml/min/1.73 m2 30 Urine Albumin Creatinine Ratio mg/g 50 Calcium mg/dl 9.8 Phosphorous mg/dl 3.8 Albumin g/dl 4 Bicarbonate meq/l 26
Five year risk of kidney failure 10.7%
Knowledge Translation

Knowledge Translation - Output

Mayo Clinic Decision Aid
https://osteoporosisdecisionaid.mayoclinic.org/index.php/site/index




Research Question
Does providing patients (& their physicians) with information about their risk of kidney failure
improve quality of care, health literacy, & trust in the care they are receiving?

Study Objective
Design, implement, & evaluate a risk based CKD management pathway in primary care clinics
across Canada

Study Design
• National cluster randomized controlled trial in primary care clinics across Canada
• Clinics are part of the Canadian Primary Care Sentinel Surveillance Network (CPCSSN)

CPCSSN
• Network of primary care clinics – ˃800 physicians & nurse practitioners – Provide care to >1.5 million Canadians
• Report all data required to calculate major vascular & CKD risk
factors – eGFR, ACR, blood pressure, hemoglobin A1C, & quality indicators for
CKD care – Collected in a longitudinal fashion
• Allows for observation of changes over time
– Access via CPCSSN’s data extraction tools

CPCSSN
Study Design
• 134 CPCSSN primary care clinic clusters Canada-wide
• Randomization stratified by province
• Randomized 1:1
• 67 clinic clusters in each arm
Study Design
• Knowledge translation intervention
– Individualized information & tools explaining their risk factors (eGFR & albuminuria) & predicted risk for kidney failure
– Risk based management pathways for CKD & its underlying causes
Study Design
• Control – Usual care – No information on personalized risk or guidance for risk
based management
• All clinics will receive provincial summary documents
with existing guidelines for CKD care

Intervention
• Patients & providers receive individualized information about kidney failure risk & risk-based criteria for referral
• Intervention delivered over 12 months with 24 month follow
up

Intervention
• Integration of the KFRE in the CPCSSN DPT
– Low/medium/high risk of progression
– Links to management & referral guidelines, & clinical decision aids

Intervention
• Audit & feedback
– Feedback report with information about CKD, albuminuria, & ACEi/ARB use
– Information about clinic risk profile & % of patients meeting risk factor & referral targets

Intervention
• Medical detailing visit
– In-person visit from key opinion leader
– Discuss accuracy of the KFRE & guidance on the implementation of a risk based treatment pathway
– Share clinical decision aids (patient & provider infographics)
– Simulate the patient-provider discussion about the risk of CKD progression
– Identify a local champion to advocate for risk based care

Patient Infographic

Patient Infographic
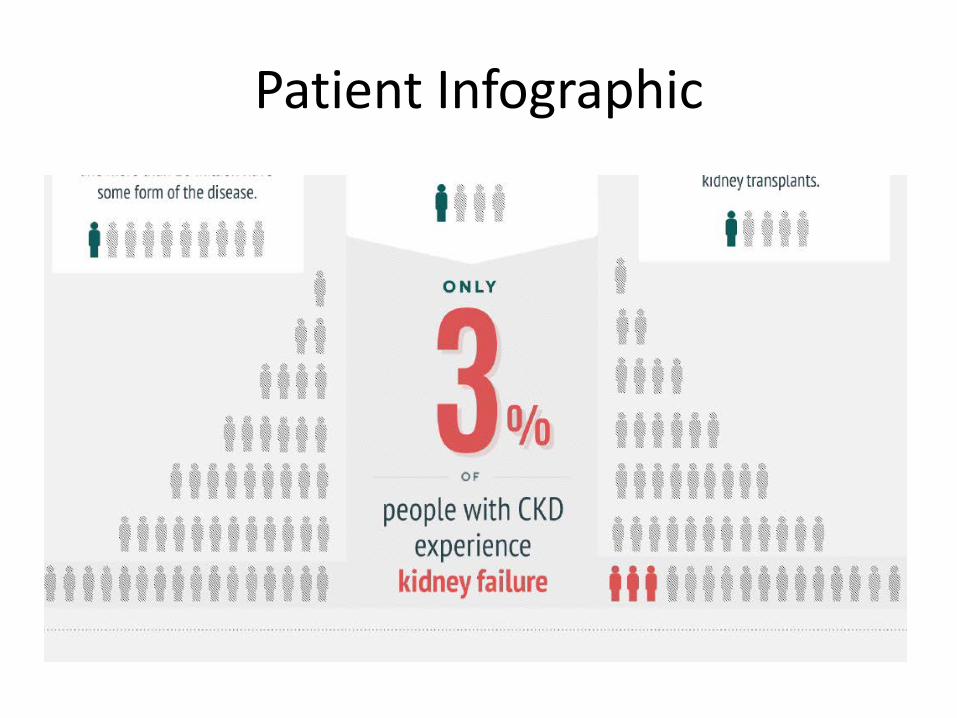
Patient Infographic

Risk Equation
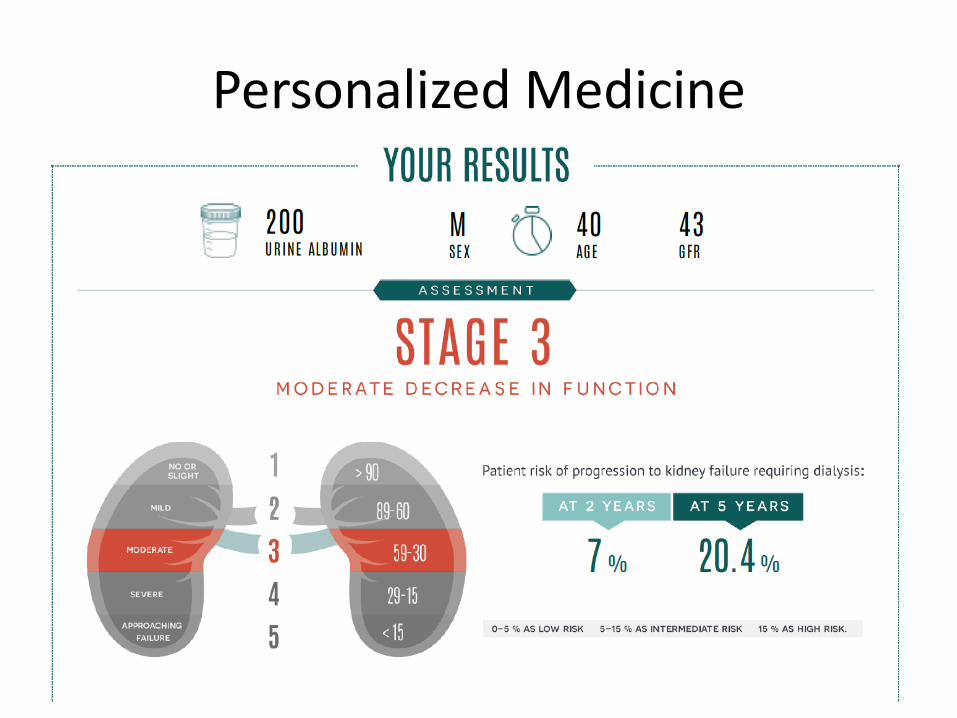
Personalized Medicine

Primary Outcomes
• Patient
– Albuminuria & ACEi/ARB • % of patients with albuminuria • % of patients with albuminuria on ACEi/ARB
– Management of diabetes • Hemoglobin A1C in target, < 8%
– Management of hypertension • Blood pressure (BP) in target, office BP < 130/80 for patients with diabetes, 140/90
for those without
– Decline in eGFR • 30% decline over 3 years of follow up

Primary Outcomes
• Health System
– Appropriate referral for patients at high risk for kidney failure
– Cost of CKD care
• Data from electronic medical records, comparison with provincial guidelines, & linkages with provincial administrative data

Secondary Outcomes
• Patient – CKD-specific health literacy – Trust in physician care
• Provider
– Satisfaction with the risk prediction tools & clinical decision aids
• Data from a sub-study using surveys & Likert scale
Patient Partner Involvement
• Study protocol refinement
• Clinical decision aid refinement
• Data analysis
• Interpretation of study findings
• Moving results to practice

Progress to Date
• Clinical decision aids developed
• Feasibility assessment completed – 461,383 patients with a measured eGFR – 146,224 with measured albuminuria – 65,021 have CKD Stage 3 or higher & would be impacted by our
intervention

Progress to Date
• CPCSSN Data Presentation Tool
– Available in all CPCSSN clinic electronic medical records
– Best platform for integration of the KFRE
– Clinicians can identify all patients with CKD Stage G3 or higher & rank them by risk of kidney failure using the KFRE
– Patients at high/low risk can be identified & targeted for further intervention

Impact
• Integration of the KFRE in primary care – Reduced anxiety – Improved health literacy – More appropriate referral
• Broader uptake
– Reduction in wait times – Improved access to specialist care for high risk patients

Thank you!
Questions or Comments?