Embed Size (px)
Citation preview

Inside-outside technique for posterior occipitocervical spineinstrumentation and stabilization: preliminary results
T. GLENN PAIT, M.D., OSSAMA AL-MEFTY, M.D., FREDERICK A. Boop, M.D.,KENAN I. ARNAUTOVIC, M.D., SALIM RAHMAN, M.D., AND WADE CEOLA, M.D.
Department of Neurosurgery, University ofArkansas for Medical Sciences, Little Rock, Arkansas
Object. The authors present a series of 16 patients who underwent inside-outside occipital and posterior cervicalspine stabilization.
Methods. In this technique, the screw was placed from the inside of the occiput to the outside. An articular (lateral) mass plate was contoured to the shape of the occipital bone and the cervical spine and affixed to the occiputwith a flat-headed screw or stud placed through a burr hole in the calvaria with the flat head of the screw in theepidural space and the threads facing outward. The bone plate was then secured with a nut to the occipital screwand the cervical plate was attached to the spine with a bone screw that coursed through the plate and into the articular pillar. Our series included six children and 10 adults. In five patients, previous fusion had failed; in two patientsspinal instability was secondary to Down's syndrome; two patients' instability was related to developmental anomalies; and in five patients spinal instability was due to the presence of tumor. One patient with rheumatoid arthritishad undergone a transoral procedure. Two patients had suffered traumatic fracture. Three patients died of causesunrelated to the procedure, one patient died of metastatic cancer, and one patient died in a long term care facility ofcardiopulmonary complications. One patient with renal failure suffered a hemorrhage from an arteriovenous fistula after being treated with dialysis. In one child, a nut backed off after 3 months. The nut was reseated, and a maturing arthrodesis was present.
Conclusions. The authors conclude that the inside-outside occipitocervical fixation is an effective technique forstabilizing the cervical spine.
KEyWORDS
wire fixationocciput • cervical spine • posterior spinal instrumentation
• screw fixation • inside-outside technique • screw
OCCIPITOCERVICAL fixation procedures have alwayspresented a challenge to the neurosurgeon becausethe anatomical complexity in this area requires
a thorough understanding of the important bony andsoft-tissue elements. Any type ofinst11lmentation must accommodate the anatomical structures and satisfy the biomechanical needs and the kinematics of the craniovertebral junction. To meet such demands, occipitocervicalstabilization techniques have undergone continuous refinement. Early techniques in which only bone grafts wereused demonstrated a high rate of failure. 15.32-34.46 Wiresecuring techniques, which secure the bone struts withsuboccipital and sublaminar wires, became popular because of their ease of use and low cost. These procedures are a better alternative to the bone graft methods; however, failure rates still range between 5% and30%.15.16,19,30.32.33.41.53,54
Wire-securing procedures often failed to provide therigid fixation needed to promote long-term arthrosis,and advancements in metallic fixtures (cables, pins, rods,screws, and plates) have since provided a more successful,rigid craniocervical system.5,6,9,11.13.14,17,21-24,26,39.40,42-45,47.48.50
Plates have been affixed with screws to the occiput andcervical spine;S.6.9,11,14,21.23,42-44,48-50 however, these screwsmust be placed from the outside to the inside of the occiput, and the surgeon must be careful to avoid intraduralpenetration of the screws, To help prevent screw penetration, we have developed a technique of placing the screwfrom the inside of the occiput to the outside.
Clinical Material and Methods
For this technique, an articular mass (lateral mass) plateis contoured to fit the shape of the occipital bone and thecervical spine, and the plate is affixed to the occiput bymeans of a flat-headed screw or stud placed through a burrhole in the calvaria so that the head of the screw is in theepidural space and the threads face outward. The boneplate is then secured with a nut to the occipital screw. Thecervical plate is attached to the spine with a bone screwthat courses through the plate and into the articular pillar(lateral rnass).S,14.35,36.43,48 Such stabilization provides imme-diate rigid fixation for bone fusion.
All 16 patients (10 adults, six children) underwent post-

T. G. Pait, et al.
TABLE l
History and outcome data in 16 patients who underwent inside-outside occipitocervical stabilization
AgeCase (yrs),No. Sex Prefixation History
FollowUp
(mas) Outcome
18 returned to school & active lifestyle
14 returned to school; solid fusion after reseatingloosened nut; active lifestyle
II stabilization achieved; no further episodes ofquadriparesis
6 completed proton beam therapy; returned to school
3 4, M Down's syndrome; repeated episodes of transient quadriparesis
9, F osteoblastoma in skull base & CI-3; pro: pos excision & stabilization presection via ant approach
2 7, F dev defects, suboccipital craniectomy, failed fusion
died of cardiopulmonary complications in longterm care facility
improved
died of primary disease
gait improved; walking independently & resumedactivities at home
treated in rehab; home, anticipating return toschool
completed school & entered workforce
undergoing rehab
died of rare aneurysmal hemorrhage at arteriovenous dialysis shunt site
transferred to long-term care facilitypain decreased; undergoing oncological therapypain decreased; at home, resumed daily activities
pain decreased; wearing collar, anticipating returnto work
gait disturbance; chordoma in CVJ; pro: transcondylar resection & halo brace
upper thoracic pain, Chiari malformation, large syrinx wI other dev anomalies; 4pos fossa exploration, dural closure wI graft, 10 fixation, & transoral approachto resect basilar invagination
Down's syndrome; 1st pro: transcondylar odontoidectomy, continued instability; 182nd pro: OC onlay bone fusion wI wire fixation, still unstable
severe neck pain, breast cancer metastasis at C-2 wI ant comp; pro: ant C-2carpectomy
diffuse ossification of PLL, myelopathy; unable to walk; 1st pro: multilevel de- 14compression wI arthrodesis & ant plate, halo placed; pseudarthrosis & platemigration; myelopathy worse, CT shows continued compression; 2nd pro: antplate & strut graft removed; 3rd pro: pos cervical laminectomies & 10 fixation
severe incomplete SCI from OA dislocation, slight movement in rt arm 3
rheumatoid arthritis; progressive weakness due to ant compressive lesion at C 1-2; 10pro: transoral approach for decompression
renal failure on dialysis, diabetes, cervical spondylosis; 1st pro: multi ant & poscervical pros for spondylosis; fall wI type II odontoid fracture; 2nd pro: posatlantoaxial stabilization wI Brooks pro, failed fusion wI continued instability
obese, multi trauma wI pulmonary complications, type Il odontoid fracture & 6multi cervical spine fractures
chordoma in skull base; extended transmaxillary resection, halo brace 4multi myeloma involving C-2, severe pain, prior radio- & chemotherapy 4type II odontoid fracture; pro: Sonntag pos atlantoaxial wire & bone graft 3
(transarticular C 1-2 fixation not possible due to VA locations), followed byhard cervical collar & rehab, failed fusion
os odontoideum, failed fusion after OC fusion wI Luque rectangle; C 1-2 fixatio 2not possible due to distorted anatomy
4 12, M
5 14,M
6 18, F
7 59,F
8 57,F
9 36, F
10 60, F
II 70, M
12 81, F
13 22,F14 73, M15 58, F
l6 51, M
. * Ant = anterior; comp = compression; CT = computerized tomography; CVJ = craniovertebral junction; dev = developmental; 10 = inside-outside fixatIOn; multi = multiple; OA =occlpltoatlantal; OC = occipitocervical; PLL = posterior longitudinal ligament; pos = posterior; pro = procedure; rehab = rehabIlitatIOn; SCI = spll1al cord Injury; VA = vertebral artery.
operative anteroposterior and lateral radiography with dynumic st\1lJi s to \/al\\~\t for an)1 motion s gIn nt ahnormalities and for screw fixation and cervical spine alignment. Over a period of 18 months, (July 1996 throughDecember 1997), all patients underwent inside-outsideoccipitocervicaJ fusion. Data on patient history and treatment are shown in Table 1.
Surgical Technique
For this procedure, the patient was placed prone withgel cushions under the chest, the head was fixed in theMayfield headrest, and alignment of the cervical spinewas monitored by fluoroscopy. If we anticipated having touse transarticular screw fixation, the cervical spine wasflexed under an image intensifier to provide the best anglefor the drill to enter. The back the patient's head and neckwere shaved and prepared, and the posterior occipitocervical spine was exposed via a standard midline incision.
The median skin incision extended from two fingers' breadth above the external occipital protuberanceto the level of fusion. The nuchal ligament was divided in
the midline, and the occipital and cervical muscles werestripped from their bony attachments through subperiosteal dissection. The suboccipital and cervical paraspinous muscles were retracted laterally to expose the underlying bony architecture. Gentle operative technique wasused so as not to disturb important anatomical structuresor move unstable bone. The posterior tubercle of the atlas was palpated, its midline defined, and the muscles attached to it were gently swept laterally.
The dissection was continued laterally, maintainingbone contact to prevent injury to the horizontal segmentof the vertebral artery that is cushioned in the suboccipitalcavernous sinus. Any bleeding from the suboccipital cavernous sinus was stopped with Gelfoam and thrombin.2
The atlantoccipital membranes, ligamentum flavum, andvertebral arches were exposed with curettes and dissectors. The articular masses (lateral cervical masses) ofthe lower cervical vertebrae were cleaned of soft tissue inpreparation for screw fixation. 35.361f transarticular screwswere to be placed or C-2 pars interatticularis fixation wasto be performed, the pars, ganglion, and nerve of C-2 weredefined.
2

Inside-outside spine instrumentation and stabilization
~
"J ~' ~I(; ,.,
o
t,
G
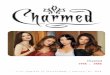
FIG. 1. Artist's illustrations (A-G) and photograph (H) demonstrating the involved surgical procedures in the inside-outside technique. A: With the template in position, the sites for cervicalspine screw fixation and the occipital exit are marked. B: Theentry hole is marked above the exit site either medially or laterally.Using a drill, a hole is made at the entry site and the keyway is cutfrom the burr (entry) hole to the marked exit site. C: The inside-outside screw is attached to a guide rod and inserted into theentry site. D: The reconstruction plate is placed over the inside-outside screw, and the nut is loosely attached to the screw.The epidural location of the inside-outside screw is appreciated.E: The cervical spine fixation screws are secured. F: The inside-outside screw is secured and sublaminar wires, if needed, aretightened. A screwdriver is inserted through the socket wrench andinto the hex of the inside-outside screw to provide countettorque.
G: The rib grafts are secured to the plate with wire fixation. H: Intraoperative photograph demonstrating the inside-outside screw and spinescrews after tightening and the rib grafts after being secured with sutures.
After the occiput and cervical spine were exposed, theoperative field was prepared for instrumentation. We describe the surgical procedures in 10 steps.
Step 1: Marking the Occiput and Cervical SpineWith a Template
A malleable template is placed over the occiput and cervical spine and contoured to the correct shape (Fig. 1A).The sites of cervical screw fixation determine the entryand exit points of the inside-outside occipital screw. Thereconstruction template is positioned over the articular(lateral cervical) masses; the holes of the template must bepositioned to allow the proper angle for the drill to enter.Transarticular Cl-2 or C-2 pars fixation sites are the firstto be determined; the C-2 screw site is not as adjustable as
the occipital and articular (lateral cervical) masses. Afterthe C-2 site has been determined, the template is adjustedover the articular (lateral cervical) masses to allow thescrew to enter the superior lateral quadrant (the safe quadrant).5,23.35.36 With the template in position, the hole overthe occiput, which corresponds to the correct cervicalposition, is marked with a colored pen. This hole will bethe exit site of the inside-outside screw (Fig. lA). Theentry site is marked above the exit site either laterally ormedially,
Step 2: Creating the Entry Site
With a craniotome, a burr hole is made at the markedentry site. This point can also be made with a surgical drill(Fig. 18). Bone dust from the drilling is saved to be used
3

T. G. Pait, et al.
FIG. 2. Left: Preoperative sagittal computerized tomography scan obtained in a 9-year-old girl with osteoblastoma (asterisk). Right:Postoperative sagittal computerized tomography scan obtamed after tumor resectIOn. Note the positIOn of the construct (soltd arrows), andbone graft (open arrows).
to fill the entry hole. The occipital hole is cleaned, the durais exposed, and the dura is separated from the inner tableof the skull.
Step 3: Establishing the Keyway
The keyway, which is cut with either rongeurs or a surgical drill with a fraise (footplate), extends to the markedexit site. The entry and exit sites are enlarged to allow safeand easy passage of the inside--()utside screw (Fig. lB).
Step 4: Positioning the lnside-Outside Screw With theGuide Rod
The inside-outside screw is attached to the guide rod(Dyna-Lok T-bolt and Nut; Sofamor Danek, Memphis,TN) and then carefully placed epidurally into the entry siteand guided to the exit site (Fig. lC).
Step 5: Checking the Template
The template is placed over the inside--()utside screwand the contour of the plate is checked. The template isagain aligned to allow for correct cervical screw fixation.
Step 6: Placing the Reconstruction Plate
The reconstruction plate (Axis System; Sofamor Danek, Memphis, TN; and AO/Synthes Posterior CervicalPlating System; Synthes Spine, Paoli, PA) is bent to matchthe template. The surgeon must be careful not to twist theplate while bending it. If the plate is twisted, it may notrest tlatly on the bony surfaces, and the holes for the penetrating screws may be misaligned; in addition, the fit ofthe implant and bone interfaces may also be affected. Partof the lamina of C-2 may need to be drilled down to allowbetter surface-to-surface contact between the plate andbone.
Step 7: Anchoring the Articular Mass Screw andEstablishing Transarticular or C-2 Parslnterarticularis Fixation
The transarticular or C-2 pars interarticularis fixation isthe first site of the cervical spine to be anchored to the
4
reconstmction plate. The bony morphology of the atlasand axis are carefully studied on computerized tomography scans. Subluxations of CI-2 are. reduc.ed to a~low
correct alignment. The vertebral artery IS studied on eitherstandard angiograms or magnetic resonance angiogramsobtained in patients with tumors.
The neurovascular elements coursing over the pars ofC-2 are defined a second time. Using a bone awl, a purchase site is placed approximately 2 to 3 mm lateral to themedial border of the C-2 pars. The trajectory of the drill ischecked fluoroscopically, and the drill is directed towardthe dorsal cortex of the anterior arch of C-l. The screwlength needed is determined from the drill and checkedafter the drill is tapped. The cervical spine screws areplaced into the superior lateral quadrant of the articular(lateral) masses. 35 .36
Step 8: Preparing the Cross Link (Optional)
In one patient, we used a cross-linked plate to achievegreater stabilization of an occipitoatlantal dislocation. Todevelop a linking unit, a small inside-outside screw (stud)is placed under and through the axial reconstmction plate.This placement allows another plate to be secured to theprimary plate.
Step 9: Attaching the Reconstruction Plate to thelnside-Outside Screw and lnserting the Cervical SpineScrews or Sublaminar Cables
The reconstmction plate is placed over the inside-outside screw and a nut is then placed and tightened slightly with a socket wrench, although the nut is not securedfirmly at this stage in the procedure (Fig. 10). The plate isthen positioned over the entry site of the C-2 screw, andthe transarticular screw is directed into the prepared bone.Advancement of the screw is closely monitored on continuous fluoroscopy. Like the nut on the inside-outsidescrew, this screw is not completely tightened. The nextscrew is placed in the most caudal site and is the last screwof the construct. The remaining fixation points are thensecured (Fig. IE).
The inside-outside screw is firmly tightened, and any

Inside-outside spine instrumentation and stabilization
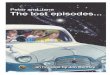
FIG. 3. Left: Preoperative sagittal magnetic resonance image showing a chordoma (asterisk) in a 12-year-old boy.Center: Postoperative sagittal magnetic resonance image showing radical tumor resection. Note the fat graft (asterisk) inthe site of the resected tumor. Right: Postoperative lateral x-ray film showing the posterior stabilization construct.
sublaminar cables or wires are secured to the plate. Ascrewdriver is inserted through the socket wrench into thehex in the inside-outside screw to provide countertorque(Fig. IF).
Step 10: Finishing the Arthrodesis
The arthrodesis is completed with a rib or bone takenfrom the iliac crest. The occiput and cervical spine surfaces are decorticated, and the rib is secured to the platewith sutures or wire for good surface-to-surface contact(Fig. IG and IH). The keyway is then filled with bone.The operative field is amply inigated, and the incision isclosed in layers. Antibiotics are administered throughoutthe surgical procedure.
Results
Six children and 10 adults (aged 4-81 years) underwentinside-outside occipitocervical fixation and fusion. Thefollow-up period ranged from 1 to 18 months. We used theAxis system for plate fixation in all adult patients,S butbecause it is too wide to be used in children, the narrowerAO system, which better matches the smaller articularmasses, was used in the six children.
In patients with tumors, we could not perform atlantoaxial fixation because the lesions had destroyedbone. Patients with developmental anomalies could notundergo screw fixation because the bone had maturedpoorly.
One child who was placed in a halo brace postoperatively was the only patient to have one nut loosen from theinside-outside screw (after 3 months). This nut had beenplaced without the use of countertorque. During a secondsurgery in which the nut was reseated without difficulty,the bone fusion was noted to be maturing. The patient wasthen placed in a firm collar and has since returned to normal levels of activity. All other children were placedin firm collars and showed no radiological evidenceof instrument movement or failure. A 9-year-old girl whounderwent anterior resection of an osteoblastoma has returned to school (Fig. 2). A 12-year-old boy has completed a course of proton radiation therapy for a chordoma
(Fig. 3). A 14-year-old boy with a Chiari malformationunderwent transoral resection of the odontoid. The othertwo children also improved and are living actively. An18-year-old woman with Down's syndrome was initially placed in a firm collar. Because of her vigorous headmovements, however, her chin became chafed and theskin around the inion abraded. She was placed in a halofor approximately 6 weeks. At follow-up examination,solid fusion mass was confirmed without evidence of apseudarthrosis. She finished school and is now employed.
One woman with ossification of the posterior longitudinal ligament no longer requires a wheelchair and iswalking without assistance. A patient who sustained anoccipitoatlantal dislocation died of cardiopulmonary complications after being transferred to a long-term care facility. One patient died of cancer that metastasized to thespine. A third patient with renal disease died of a hemorrhage after undergoing dialysis for a rare aneurysm in anarteriovenous fistula in his arm. An 81-year-old woman, amUltiple trauma victim with an odontoid fracture, wastransferred to a rehabilitation center. One 22-year-oldwoman with an aggressive chordoma developed bacterialmeningitis after her first surgery; when she was medicallystable, she underwent occipitocervical fixation and wastransferred to a long-term sUPPOtt facility. A man withmultiple myeloma is undergoing further treatment for hisdisease, but he can hold his head erect without pain. A 58year-old woman, who suffered multiple injuries from anautomobile accident, returned home and resumed dailyactivities; she can walk with assistance. A 51-year-oldman in whom a CI-2 fusion failed was discharged homewearing a collar; his pain has improved, he is becomingmore active, and he anticipates returning to work.
The inside-outside instrument was the only type of occipital fixation needed. No other types of adjuvant fixationsuch as wire or other screws were utilized. Because werecognized the thinness of the occipital bone prior to treatment in the children, there was never need to abandon theoperation. In such a situation, the inside-outside screwdiameter was increased to accommodate the thinness ofthe bone. In addition, there were no fractures of the occipital bone during screw tightening. We found no evidence
5

of screw migration through the keyhole. The dura in theelderly patients also did not cause any problem. We had nodural tears or cerebrospinal fluid leaks.
Discussion
Occipitocervical instability may be caused by tumor,inflammation, trauma (bone or ligamentous injury), congenital anomalies, and degenerative lesions.2,4,7,10,18,25,27,28.35,37,51.52 Because radiological methods of diagnosis haveimproved, these abnormalities have been identified earlier. Increasing appreciation of the anatomical defectsand better ways to determine spinal stability or instabilityprompted the refinement of surgical techniques used tocure these lesions. 1,3,6,9, II ,13, 14,16, 19,21 ,22,24,26,29-33.38-40,42-48,50,53,54 In-ternal fixation and fusion procedures for the treatmentof occipitocervical instability have undergone numerouschanges.6,9, 11,1 3, 14, 16, 19,21 ,22,24,26,30,32,33,39,40-48,50,53,54 Improvementsin metallurgy and a better understanding of biomechanicshave helped surgeons to improve occipitospinal stabilization techniques. 12,20,38
In any occipitocervical fixation procedure, the surgeonmust address the complex bony anatomy of the region,namely the occiput, the occipital condyles, C-l, and C-2.The occiput does not easily accommodate instrumentation. In fact, the area available for the fixation of implantsis limited. Bone thickness is also of concern when anyinternal fixation is needed, Traditional "outside-inside"screws can be anchored laterally into only a shallow shelfof bone or into the thicker midline keel. When suchscrews are used, the thickness of the occiput must be measured to assess the anticipated screw length and preventinjury to the underlying cerebellum,21 In this type of fixation the surgeon relies on radiological images to confirmthat the screws did not inadvertently penetrate the brain. Ina series in which occipitocervical fusion was performedusing internal fixation, Heywood and colleagues21 did notencounter cerebral complications, but they avoided penetration of the inner table.
The Geschwend method of occipitocervical fixationinvolves placing a wide-headed, flat screw from the outside to the inside of the occiput. A wire is then placedaround the necks of both screws, passed under the arch ofC-l, and secured around a spinous process.32 As with thestandard outside-inside technique, the strength of the construct greatly depends on the bone purchase achieved withthe occipital screws. A similar pullout problem is encountered when wire is used for fixation or for attaching posterior instrumentation. Wire or cables may easily pull orcut through the occipital bone. Because of the thin bone inchildren, this problem becomes particularly worrisome.
The inside-outside method for the provision of occipitocervical fixation offers several advantages over the outside-inside techniques. Screws are not placed in a blinded fashion. The surgeon sees the entire screw; in fact,the screw points toward the surgeon. The flat surface ofthe screw head, not the threads, is next to the dura. Furthermore, the surgeon need not be concerned about thethickness of the occiput when determining screw length.The inside-outside screw avoids the hazards of the cuttingeffect of wire or cable, If articular mass (lateral mass)screw fixation cannot be perfonned in the spine, sublaminar wires can be attached to the reconstruction plate.
6
T. G. Pait, et al.
Conclusions
We have used the inside-outside technique for the treatment of occipitocervical instability in 16 patients. The instrumentation has remained well seated in all but onepatient. One patient, whose fixation device demonstratedloosening of the nut, was the only patient placed in a halobrace immediately after surgery. Any stabilization technique should be simple and safe. The instrumentationshould be designed to prevent injury to nearby structureswhile providing maximum stabilization and promotingsolid maturation of the arthrodesis. Inside-outside occipitocervical fixation fulfills these demands.
Acknowledgments
The authors thank Julie Yamamoto for her editorial assistanceand excellent suggestions, We are indebted to Kim Vognet, R.N"for gathering patient data and records, We are grateful to JamieTillman, Graphic Artist, for the artistic illustrations, and to RonTribell, Chief Medical Illustrator, for his invaluable assistance inpreparing figures for this paper. We are also grateful for the typingtalents of Betty Patterson and Amy Keeland in prepm1ng this manuscript.
References
I. AI-Mefty 0, Borba LA, Aoki N, et al: The transcondylar approach to extradural nonneoplastic lesions of the cranioveltebral junction. J Neurosurg 84: 1-6, 1996
2, Arnautovic Kl, AI-Mefty 0, Pait TG, et al: The suboccipitalcavernous sinus, J Neurosurg 86:252-262, 1997
3, Benzel EC: Complex instrumentation constructs and force applications, in Benzel EC (ed): Biomechanics of Spine Stabilization: Principles and Clinical Practice. New York: McGraw-Hill, 1995, pp 25-31,221-245
4. Bettalanffy H, Seeger W: The dorsolateral, suboccipital, transcondylar approach to the lower clivus and anterior portion ofthe craniocervical junction, Neurosurgery 29:815-821, 1991
5, Brattstrom H: Surgery in atlanto-axial dislocation in rheumatoidarthritis. Reconstr Surg TraumatoI18:16--29, 1981
6, Bryan WJ, Inglis AE, Sculco TP, et al: Methylmethacrylate stabilization for enhancement of posterior cervical arthrodesis inrheumatoid arthritis. J Bone Joint Surg (Am) 64:1045-1050,1982
7, Bucholz RW, Burkhead WZ: The pathological anatomy of fatal atlanto-occipital dislocations, J Bone Joint Surg (Am) 61:248-250, 1979
8, Cherny WB, Sonntag VK, Douglas RA: Lateral mass posterior plating and facet fusion for cervical spine instability, BNIQuart 7:2-11, 1991
9. Cregan JC: Internal fixation of the unstable rheumatoid cervicalspine. Ann Rheum Dis 25:242-252, 1966
10, Crockard HA, Essigman WK, Stevens JM, et al: Surgical treatment of cervical cord compression in rheumatoid arthritis, AnnRheum Dis 44:809-816,1985
11, Dickman CA, Sonntag VK, Marcotte PJ: Techniques of screwfixation of the cervical spine. BNI Quart 8:9-26, 1992
12, Dunn EJ, Anas PP: The management of tumors of the upper cervical spine. Orthop Clin North Am 9: I065-1080, 1978
13. Ellis PM, Findlay JM: Craniocervical fusion with contouredLuque rod and autogeneic bone graft. Can J Surg 37:50-54,1994
14. FehJings MG, Errico T, Cooper P, et al: Occipitocervical fusionwith a five-millimeter malleable rod and segmental fixation,Neurosurgery 32:198-207,1993
15. Fielding JW, Hawkins RJ, Ratzan SA: Spine fusion for atlantoaxial instability. J Bone Joint Surg (Am) 58:400-407, 1976

Inside-outside spine instrumentation and stabilization
16. Grantham SA, Dick HM, Thompson RC Jr, et al: Occipitocervical arthrodesis: indications, technique, and results. ClinOrthop 65:118-129,1969
17. Grob D, Dvorak J, Panjabi M, et al: Posterior occipitocervicalfusion: a preliminary report of a new technique. Spine 16(SuppI3):17-24,1991
18. Hakuba A, Komiyama M, Tsujimoto T, et al: Transuncodiscalapproach to dumbbell tumors of the cervical spinal canal. JNeurosurg 61:1100-1106, 1984
19. Hamblen DL: Occipito-cervical fusion: indications, technique,and results. J Bone Joint Surg 49:33-45, 1967
20. Harrington KD: Current concepts review. Metastatic disease ofthe spine. J Bone Joint Surg (Am) 68: 1110-1115,1986
21. Heywood AW, Learmonth rD, Thomas M: Internal fixation foroccipito-cervical fusion. J Bone Joint Surg (Br) 70:708-711,1988
22. Itoh T, Tsuji H, Katoh Y, et al: Occipito-cervical fusion reinforced by Luque's segmental spinal instrumentation for rheumatoid diseases. Spine 13:1234-1238,1988
23. Kerschbaumer F: Rheumatoid instability, in Bauer R, Kerschbaumer F, Poisel S (eds): Atlas of Spinal Operations. NewYork: Thieme, 1993, pp 347-376
24. MacKenzie AI, Uttley D, Marsh HT, et al: Craniocervical stabilization using Luque/Hartshill rectangles. Neurosurgery 26:32-36, 1990
25. McWhorter JM, Alexander E, Davis CH, et al: Posterior cervical fusion in children. J Neurosurg 45:211-215, 1976
26. Menezes AH: Congenital and acquired abnormalities of the craniovertebral junction, in Youmans JR (ed): Neurological Surgery: a Comprehensive Reference Guide to the Diagnosisand Management of Neurosurgical Problems, ed 4. Philadelphia: WE Saunders, 1996, pp 1035-1089
27. Menezes AH, Muhonen M: Management of occipito-cervicalinstability, in Cooper PR (ed): Management of PosttraumaticSpinal Instability. Park Ridge, IL: American Association ofNeurological Surgeons, 1990, pp 65-76
28. Menezes AH, VanGilder JC: Transoral-transpharyngeal approach to the anterior craniocervical junction: ten-year experience with 72 patients. J Neurosurg 69:895-903, 1988
29. Menezes AH, VanGilder JC, Clark CR, et al: Odontoid upwardmigration in rheumatoid arthritis: an analysis of 45 patientswith "cranial settJing." J Neurosurg 63:500-509, 1985
30. Menezes AH, VanGilder IC, Graf CI, et al: Craniocervica1abnormalities: a comprehensive surgical approach. J Neurosurg 53:444-455, 1980
31. Miller JD, A1-Mefty 0, Middleton TH III: Synovial cyst at thecraniovertebra1 junction. Surg Neurol 31:239-242, 1989
32. Murphy MJ, Southwick WO: Posterior approaches and fusions,in Cervical Spine Research Society (ed): The Cervical Spine.Philadelphia: JB Lippincott, 1983, pp 496-513
33. Murphy MJ, Southwick WO: Posterior approaches and fusions,in Cervical Spine Research Society (ed): The Cervical Spine,ed 2. Philadelphia: JB Lippincott, 1989, pp 775-791
34. Newman P, Sweetnam R: Occipito-cervical fusion: an operativetechnique and its indications. J Bone Joint Surg 51:423-431,1969
35. Pait TG, Borba LAB: Stabilization of the cervical spine (C3C7) with articular mass (lateral mass) plate and screws, in LongD (ed): Atlas of Operative Neurosurgical Technique. Baltimore: Williams & Wilkins, 1996, Vol 5, pp 91-100
36. Pait TG, McAllister PV, Kaufman HH: Quadrant anatomy ofthe articular pillars (lateral cervical mass) of the cervical spine.J Neurosurg 82: 1011-1014, 1995
37. Pang D, Wi1berger IE Jr: Traumatic atlanto-occipital dislocation with survival: case report and review. Neurosurgery 7:503-508, 1980
38. Panjabi M, Dvorak J, Duranceau J, et al: Tlu'ee-dimensionalmovements of the upper cervical spine. Spine 13:726-730,1988
39. Papadopoulos SM, Dickman CA, Sonntag VK, et al: Traumaticatlanto-occipital dislocation with survival. Neurosurgery 28:574-579, 1991
40. Ransford AO, Crockard HA, Pozo JL, et al: Craniocervical instability treated by contoured loop fixation. J Bone Joint Surg(Br) 68:73-177,1986
41. Robinson RA, Southwick WO: Surgical approaches to the cervical spine, in American Academy of Orthopedic Surgeons(ed): Instructional Course Lectures. SI. Louis: CV Mosby,1960, Vol 17, pp 299-330
42. Roy-Camille R, Mazel C: Stabilization of the cervical spinewith posterior plates and screws, in Camins MB, O'Leary PF(eds): Disorders of the Cervical Spine. Baltimore: Williams &Wilkins, 1992, pp 577-591
43. Roy-Camille R, Mazel C, Saillant G, et al: Rationale and techniques of internal fixation in trauma of the cervical spine, inErrico TJ, Bauer RD, Waugh T (eds): Spinal Trauma. Philadelphia: JB Lippincott, 1991, 163-191
44. Roy-Cam.ille R, Saillant G, Mazel C: Internal fixation ofthe unstable cervical spine by a posterior osteosynthesis withplates and screws, in Cervical Spine Research Society (ed):The Cervical Spine, ed 2. Philadelphia: JB Lippincott, 1989,390-403
45. Sakou T, Kawajda H, Morizono S, et al: Occipitoatlantoaxialfusion utilizing a rectangular rod. Clin Orthop Rei Res 239:136-144, 1989
46. Sherk HH, Snyder B: Posterior fusions of the upper cervical spine: indications, techniques and prognosis. Orthop ClinNorth Am 9:1091-1099,1978
47. Songer MN, Spencer DL, Meyer PR Jr, et al: The use of sublaminar cables to replace Luque wires. Spine 16 (Suppl):418-421, 1991
48. Sonntag VK, Dickman CA: Craniocervical stabilization. ClinNeurosurg 40:243-272, 1993
49. SorU1tag VK, Dickman CA: Occipitocervical instrumentation, in Hitchon PW, Traynelis VC, Rengachary SS (eds):Techniques in Spinal Fusion and Stabilization. New York:Thieme, 1995, pp 107-121
50. Sumi M, Kataoka 0, Ikeda M, et al: Atlantoaxial dislocation: afollow-up study of surgical results. Spine 22:759-764, 1997
51. Sutterlin CE TIl: Axis fixation system for posterior cervicalreconstruction, in Hitchon PW, Traynelis VC, Rengachary SS(eds): Techniques in Spinal Fusion and Stabilization. NewYork: Thieme, 1995, pp 159-169
52. Traynelis VC, Marano GD, Dunker RO, et al: Traumaticatlanto-occipital dislocation. Case report. J Neurosurg 65:863-870, 1986
53. Wertheim SB, Bohlman HH: Occipitocervical fusion: indications, technique, and long-term results in thirteen patients. JBone Joint Surg (Am) 69:833-836, 1987
54. Yashon D: Surgical management of trauma to the spine, inSchmidek HH, Sweet WH (eds): Operative NeurosurgicalTechniques: Indications, Methods, and Results, ed 2. Orlando: Grune & Stratton, 1988, Vol 2, pp 1449-1469
Manuscript received February 3, 1998.Accepted in final form July 17, 1998.Address reprint requests to: T. Glenn Pait, M.D., Department of
Neurosurgery, University of Arkansas for Medical Sciences, 4301West Markham Street, Slot 507, Little Rock, Arkansas 72205-7199.
7