Embed Size (px)
Citation preview

Innovative Approach to Working Innovative Approach to Working
with Families in Early Recoverywith Families in Early Recovery Innovative Approach to Working Innovative Approach to Working
with Families in Early Recoverywith Families in Early Recovery
Presented by:Presented by:
Santa Clara County Dependency Drug Santa Clara County Dependency Drug
Treatment Court (DDTC) and Treatment Court (DDTC) and
Santa Clara County DDTC Head Start ProgramSanta Clara County DDTC Head Start Program
Presented by:Presented by:
Santa Clara County Dependency Drug Santa Clara County Dependency Drug
Treatment Court (DDTC) and Treatment Court (DDTC) and
Santa Clara County DDTC Head Start ProgramSanta Clara County DDTC Head Start Program
Introductions• Frances Lewis-Johnese, Social Services Program
Manager III, Services Bureau C
• Joyce McEwen-Crawford, Supervisor of Drug
Court Unit
• Deborah Dohse, Social Work Coordinator for the
Santa Clara County DDTC Head Start Program
• Rosemary Tisch, Director of Prevention
Partnership International
Demographics of Santa Clara County
• The Sixth largest county in California.• In 2000, the total population was
1,682,585 persons according to the Census data.
• In 2000, 24.7% or 416,402 persons in Santa clara County were 0-17 years of age.
• Persons under the age of five years constituted 7.1% of the total population. Very close to the State average.

Where is Santa Clara County?

• Most ethnically diverse jurisdictions in the State.
• In year 2000, 34.1 % of the local residents were foreign born and 45.4 % of all resident a spoke a language other English in the home.
• Santa Clara County students speak more than 50 languages.
Santa Clara County Court Demographics
Judicial Caseload: • Number of new abuse/neglect
petitions filed in 2003 - 916. • Average judicial dependency
caseload for 2003 calendar year - 1,046 per judicial officer.
Note: All information was provided from the Status Report 2003 prepared by the Santa Clara County Juvenile Court, Santa Clara County Social Services
Agency, and Santa Clara County Office of the County Counsel
Breakdown of Race/Ethnicity in year 2000:
White -53.8%; Asian - 25.6 %; Hispanic - 24% Other - 12.1%, Two or more Races - 4.7% African-American - 2.8%,
American Indian/ Alaskan Indian - 0.7%
• The racial/ethnic distribution of the child population varied considerably from the adult with respect to persons of Hispanic origin.
• In the year 2000, 32.7% of all children, ages 0-
18, were Hispanic.
Santa Clara County Court Demographics
Number of Children in Care :• Percentage of children in out-of-home care
on 12/31/2002 - 80.6%• Number of abused/neglected children under
the jurisdiction of the Court on 12/31/2002 - 3,116
• Number of abused/neglected children under the jurisdiction of the Court on 12/31/2003 - 2,865
• Percentage of children in out-of-home care on 12/31/2003 - 76.5%
Santa Clara County Court Demographics
• ASFA Outcomes Snapshot in 2003
• Number of Children exiting court jurisdiction in 2003, number that achieved permanency as a result of:
• Reunification - 1,205• Adoption - 306• Legal Guardianship - 604• Number of Subsidized guardianships - 231
Santa Clara County Santa Clara County DDTC MovieDDTC Movie
Santa Clara County Santa Clara County DDTC MovieDDTC Movie
The Drug Court Team
• Judge Len Edwards, Department 67• Parent’s Attorneys
– Associate Dependency Attorneys– Dependency Legal Services
• Child’s Attorney, District Attorney• County Council• Social Workers• Drug and Alcohol Assessor• Other professionals on the team • Public Health Nurse• Mental Health Assessor• Domestic Violence Advocate• Cal-Works • Community Based Agency Representatives
such as Friends Outside
Getting into Drug Court
1. The client’s Attorney interviews their client and completes a referral packet
2. Client obtains a substance abuse assessment.
3. Attorney presents the client’s packet to the drug court team.
4. Client is accepted or rejected by the team.
5. If accepted the Drug Court Team creates a case plan for the Client.
6. The client meets the team and signs a contract.

Client Responsibility
• Obtain a substance abuse assessment.• Follow the case plan created by the
Drug Court Team• Remain Drug and Alcohol Free• If a relapse occurs;
•Report to the Treatment Provider
•Report to the Social Worker•Talk about it in Drug Court•You may have to be re-assessed.
Client Responsibility
• Be on time for all required meetings.
• Attend AA/NA or Health Realization (HR) meeting on a regular basis.
• Provide sign-in sheets from AA/NA/HR meetings as requested.
• Report any changes in living arrangements, employment or school to Social Worker.

Role of the Social Worker in Drug Court
• Collect information from treatment provider and all other parties involved in the clients drug court case plan and report information to Drug Court.
• Present client information to the Drug Court Team at the Drug Court Team meeting.
• Participates in a weekly case planning meeting prior to clients appearing in Drug Court.
(A copy of the agenda is attached in your handouts.)
• Parent focused: Only the issues pertaining to the drug court case plan are discussed;
• Non Adversarial: Attorney’s are team members.
• Therapeutic: Goal is to assist the parent through recovery, which may aid in the return of the children.
• Decisions are made and agreed upon by the Drug Court Team.
Difference between Drug Court and Dependency Court

Key Components of Drug Court
• Integrates the Child Welfare Services and Alcohol and Drug Services
• Non adversarial approach • Early identification through early
assessment• Early access to AOD services• Coordinated response to client
compliance• On-going judicial interaction• Intense monitoring and evaluation of
client participation.
Graduation vs. Completion• Completed 12 months• Consistent attendance• Complied with drug
court case plan.• 6 consecutive months
clean tests, prior to graduation.
• Complete an Exit Plan• In agreement with the
permanent plan
• Attended 12 months.
• Had intermittent relapses.
• Is no longer in Family Reunification or Family Maintenance and not in agreement with the permanent plan.

Philosophical Shift in FTDC Model
Philosophical Shift in FTDC Model
• Why the children should be the primary focus?
• Why assessments of children should occur early on?
• Why school readiness needs to be addressed prior to age five?
• Why the Head Start Model?• Why address parenting skills of parents?• Do you have better outcomes for the
children are involved in the classes?• Why address medical needs of parents?
Santa Clara County Family Treatment Drug Court (FTDC)Head Start Grant
• Serves 60 parents and 125 children annually. • It is a holistic approach to court mandated
treatment plan for reunification.• Parents will receive parent training and
modeling in a child-centered supervised visitation program based on a research based curriculum known as ‘Celebrating Families’.
• Children receive with extensive medical screening and assessments.
• This pilot program will help parents improve their parenting capabilities.
Why a Holistic Approach?• Many of the FTDC parents have not received sufficient
parenting themselves.
• Because of their substance abuse, a court mandated holistic and culturally competent parent training and child-centered Head Start Program with medical screening, assessments, and supervised visitations can improve the parenting capabilities of these parents.
• This historic groundbreaking pilot program will serve as a model to help families in other court systems obtain appropriate medical evaluations for themselves, their children, and receive parent education training.
Why a Holistic Approach?
• A child-centered Head Start Program can strengthen the county’s options for families who have lost custody, or at risk of losing custody of their children due to inadequate parenting capabilities and insufficient community-wide support channels to deter domestic violence.
Goals and Objectives
• To adequately assess parents’ medical needs and their children’s medical, developmental, and academic readiness for success in school;
• To help parents develop the culturally competent critical life
skills for supporting the development of their children’s health,
including children with neurological damage from prenatal
exposure to drugs and alcohol;
• To train parents on how to adequately support their children’s
academic readiness for school success; and
• To provide recovering parents and their children with ongoing
culturally competent support and life skills reinforcement
beyond the program cycle.
• 95% of the participating parents will complete medical exams
• 95% of the children will undergo medical, developmental, and academic screening and assessments. This will help parents and their children achieve health and academic success as demonstrated by assessment results, increased statements of feeling healthy, and increased academic performance.
• In addition, 80% of the participating parents will
demonstrate increased life skills in supporting the development of the children’s health, as observed by increased confidence in their ability to manage stress.
Goals and Objectives (con’t)
Program Objectives
• The participating parents will overcome conflict with their children, as demonstrated through parents’ classroom observations, homework behavior logs, feedback from teachers and social workers, and knowledge based surveys.
• Furthermore, 80% of the participating parents will adequately support their children’s academic readiness for school success as demonstrated through parents’ classroom observations, homework behavior logs, feedback from teachers and social workers, and knowledge based surveys.
• Ultimately, we estimate by September 30 of each program year, 50% of the recovering parents and their children will continue to participate in ongoing support and life skills reinforcement activities beyond the program cycle.

Major Components of the Grant
• Initial Screening and Assessment of Children
• Medical Assessment of Parents
• Integration of Head Start Program into FTDC Model
• Family Night Component
Initial Screening and Assessment of Children
• The child development-screening specialist who administers the FASNET screening tool documents each child’s results based on the following skill categories: physical findings, communication/language, socialization, behavior, AD/HD, and cognition.
• For each client, the professional documents areas of concern and strength, as well as a written summary and recommendations.
• Additionally, based on the screening results, children were referred to a variety of diverse programs geared to meet their needs.
• In the scoring of the Neurological Impairment Characteristic of Fetal Alcohol and Drug Exposure, if more than 50% of the items in any one category were marked true (positive result), then that category was considered a “high score” and is “flagged” for further assessment.

Medical Assessment of Parents
• Each parent is given a health screening questionnaire during the family night parenting class and are given medical resources in the community.
• In addition, all parents who reside in the transitional housing receives services from the public health nursing and are given medical resources in the community.

Integration of Head Start Program into FTDC Model
• Basic Principles of Head Start Program• Consistent with Child Welfare Outcomes• Early Acquisition of School Readiness
Skills• Parent Involvement on all levels• Strengthen the relationship between
children and their parents by providing a holistic, culturally competent program by the integration of both models.

Head Start Program
• Head Start/Early Head Start is a federally funded child development program for very low-income young children and their families.
• Since its inception in 1965, more than 20 million children and families nationally have benefited from Head Start’s comprehensive services.
• Statewide, this number is estimated to be in excess of 1,000,000 children and families.
• The primary target population for Project Head Start/Early Head Start is children between the ages of 0-5 and pregnant women from families living below the federal poverty line.

Head Start Program
• Head Start/Early Head Start programs are funded by the Federal Department of Health and Human Services directly to local community agencies.
• The Head Start/Early Head Start program is based on the premise that all children share certain needs, and that children from low-income families, in particular, can benefit from a comprehensive developmental program to meet those needs.
• Head Start/Early Head Start is a family-oriented, comprehensive, and community-based program to address developmental goals for children, support for parents in their work and child-rearing roles, and linkage with other service delivery systems.
Four Basic Principles of Head Start• A child can benefit most from a comprehensive,
interdisciplinary program to foster normal development and remedy problems.
• Parents are the primary educators of their children and must be directly involved in the program.
• The well-being of children is inextricably linked to the well-being of the entire family.
• Partnerships with other agencies and organizations in the community are essential to meeting family needs.

Family Night Component

Welcome toWelcome to

Celebrating Families!A 15 session education-support
group for families in early recovery
• Increases successful family reunification.
• Increases successful completion of Drug Court.
Of Of Celebrating Families!Celebrating Families!
HistoryHistory

Of Of Celebrating Families!Celebrating Families!
Research Research FoundationsFoundations

Research Foundations
• Brain chemistry.
• Healthy living skills.
• Risk and resiliency factors.
• Asset development.
CF! Incorporates current research on:CF! Incorporates current research on:
CF! Program Foundations
• Life Skills • Support
Group
• Family System

Of Of Celebrating Families!Celebrating Families!
The The SessionsSessions

Topics:
• Healthy Living
• Nutrition
• Communication
• Feelings
• Anger Management
• Facts about Alcohol/Tobacco and Other Drugs
• The Disease of Chemical Dependency
• How Chemical Dependency Affects the Whole Family
Topics: con’t
• Goal Setting
• Decision Making
• Boundaries
• Healthy Relationships
• Uniqueness

• Acts of Kindness
• WOW Moments
• Children’s Affirmations
• One-on-One Time with Kids
• Goal Setting
A Word About Homework!
This group is different – this is not
another parenting class. This is a
class on being a family.” From Parent Focus Group
“I now call my son twice a day. I used to think of calling him once a week. Now when I start to call a friend, I call him instead.”
Celebrating Families!Celebrating Families!

Celebrating Families!
Teaches
• Skill Building • Stress Reduction• Helping Others• Awareness of the
World• Value of spending
1-on-1 time with each child
• Telling children “I love you”.

Celebrating Families!Contacts
www.preventionpartnership.us Rosemary [email protected]
Deborah [email protected]
m

Medical and Health Screening Results

Medical and Health Screening Results
For all of the mothers and children who reside in Transitional Housing Units (THU), a health screening questionnaire is given to the parents.
• The questionnaire is used to assist in assessing their medical needs. The Child Health Disability Program (CHDP) follows up medical needs of the children under the foster care system.
• This health screen is a special project under the Public Health division. The services ensure children receive immunizations, assistance with TB testing for mothers, provide planning information and health related referrals for the mother and child.
Medical and Health Screening Results
• The ultimate goal of this program is to minimize or break barriers of fear and misunderstanding of the health system that some mothers often experience. The Public Health Nurse conducts Denver Development Assessments with the children and the data is maintained in a public health database.
• In addition, all parents where given a health survey in the Family Night parenting class and 95% of parents reported that they had been seen by a doctor in the last six months. Only 5% reported that they needed assistance in receiving medical care. Referrals and resources have been provided to those parents.
Initial Screening and
Assessment of Children
Initial Screening and Assessment of Children
The following results are from the Neurological Impairment screening process that was conducted on all children who participated in the Santa Clara County DDTC Head Start Program.
• During the first year, we successfully completed 85% of the initial screenings for all children involved in this program. The remaining 15% of children were not available to participate in the initial screening for various reasons.
• 71 completed clinical assessments of children out of 85 children.
Initial Screening and Assessment of Children
• Since this program started, out the 71 children that have been screened: 41% males and 59% females.
• Children were of all ages, from 6 months to 17 years
old. The predominant age group was children between one and five years of age.
• Individual children did score more than 50% in some of the skill categories.
• An analysis by age group showed a higher average scores were uncovered; thus further assessment
(for certain children) was needed.

Initial Screening and Assessment of Children
• 19 out of the 71 children between three and five years old showed higher average scores particularly in the areas of “Behavior,” “Communication,” and “AD/HD Symptoms.”
• 24 out of the 71 children between the ages of one and two had a highest average score in the area of “Communication”.
• 9 out of the 71 children between the ages of six and nine had a high average score in the area of “AD/HD symptoms”.
• 17 out of the children older than 10 years of age received lower average scores in most of their skill categories.
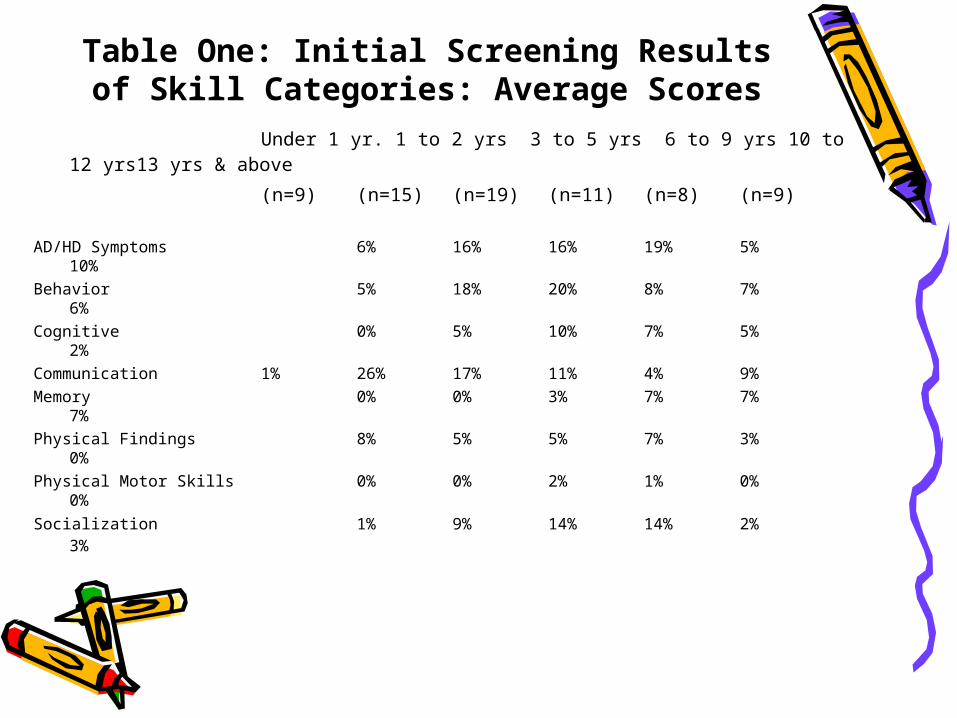
Table One: Initial Screening Results of Skill Categories: Average Scores
Under 1 yr. 1 to 2 yrs 3 to 5 yrs 6 to 9 yrs 10 to 12 yrs13 yrs & above
(n=9) (n=15) (n=19) (n=11) (n=8) (n=9)
AD/HD Symptoms 6% 16% 16% 19% 5% 10%
Behavior 5% 18% 20% 8% 7%6%
Cognitive 0% 5% 10% 7% 5%2%
Communication 1% 26% 17% 11% 4% 9%
Memory 0% 0% 3% 7% 7%7%
Physical Findings 8% 5% 5% 7% 3% 0%
Physical Motor Skills 0% 0% 2% 1% 0%0%
Socialization 1% 9% 14% 14% 2%3%
Head Start Program: 1st Year Results

• Most children have improved on their ability to complete puzzles in a timely manner; have learned the alphabet and can count fairly well from 1 to 20.
• Many Head Start age children continued to show an excellent ability in using their words during conflicts. Additionally, many show interest in reading and writing.
• Some children who had difficulties in communicating have made great efforts to verbalize their thoughts and feelings, they have also learned to ask questions.
• Most children have shown progress on counting, story
comprehension, and social skills with peers and teachers.
Head Start Program: 1st Year Results
This program uses the State Desired Results Developmental Profile (DRDP +) to assess children on their progress.
This assessment is completed every three months and includes:
• Child Desired Result 1: Children are personally and socially competent;
• Child Desired Result 2: Children are effective learners;
• Child Desired Result 3: Children show physical and motor competence; and
• Child Desired Result 4: Children are safe and healthy.
The DRDP has a list of “Performance Levels” for each measure including “Not Applicable,” “Not Observed,” “Not Yet,” “Emerging,” “Almost Mastered,” and “Fully Mastered.”
Desired Results Developmental Profile (DRDP +)

Desired Results Developmental Profile (DRDP +)
• Each child is assessed three times.
• Since the beginning of the program, 10 students have enrolled in the Head Start program.
• Fifty percent of these students are Hispanic, with 40% being White, and 10% other.
• The great majority of students are female (almost 80%).
• Teachers completed nine DRDP assessments (one additional assessment was completed in a different form, and it was excluded for this analysis)
• One child was assessed once and 8 were assessed twice.
Desired Results Developmental Profile (DRDP +)
The following is a comparison between assessment one and assessment two.
Assessment 1Desired Result 1: Children are personally and socially competent.
– Children were rated in all items as either “Emerging or “Almost Mastered.
– Children scored the highest (Almost Mastered) on the item “Child identifies self by categories of gender, age, or social group.”
Desired Result 2: Children are effective learners.– Head Start participants were rated as either “Emerging” or “Almost
Mastered” in most of the items in this category.– The following exception were: Child predicts outcomes in changes of
materials and cause and effect relationships based on past experiences; and Child writes three or more letters or numbers.
Desires Result 3: Children show physical and motor competence. – Under this category participant’s scores ranged from “Emerging” to
“Almost Mastered” to “Fully Mastered,” with the exception of: Child catches a large ball with two hands;
Desires Result 4: Children are Safe and Healthy. – These results for this category showed that all average rates were
between “Emerging” and “Almost Mastered.”
Assessment 2Desired Result 1: Children are personally and socially competent.
– In most items the children improved from “Almost Mastered” to “Fully Mastered” with the exception of one item where the ratings remained “Almost Mastered” in both assessments. This item is child exhibits impulse control and self-regulation, i.e. stay focused in the classroom.
Desired Result 2: Children are effective learners. – These Head Start participants showed improvement in each item
with the exception of: • Child observes and examines natural phenomena through
senses;• Child predicts outcomes in changes of materials and cause and
effect relationships based on past experiences; • Child uses measuring implements;• Child knows 10 or more letter name, especially those in their
own name; and• Child writes three or more letters or numbers.
Desires Result 3: Children show physical and motor competence. – All items improved for these children. They went from “Almost
Mastered” to “Fully Mastered,” with the exception of: • child catches a large ball with two hands; and • child skips or gallops.
Desires Result 4: Children are Safe and Healthy. – These youngsters improved in nearly all items from a rating
of “Almost Mastered” to “Fully Mastered,” with the exception of: Child listens to and understands English.

• C.A.L. Research developed a parent questionnaire.
• The purpose of this questionnaire is to better understand the parent’s perspective of how their children are benefiting from the Head Start program and thus helping them to prepare for school.
• The questionnaire includes 17 questions that measure how
parents perceive improvement in different areas of learning. The answers are measured on a scale from 1 to 4 with 4 =great, 3=some, 2=no improvement and 1=don’t know.
• We interviewed the parents of seven children; – Four of these parents had children currently attending
the Head Start program.– Four Head Start children were of different ages,
including (2) three year olds, (3) four year olds and (2) five year olds.
Head Start Parents Questionnaire

Head Start Parents Questionnaire
• The majority of parental responses were very positive with the average response for most questions being “some” and “great.”
• Statements that received positive responses included:– Your child’s interaction with adults;– Your child’s interaction with friends;– Your child’s interaction with other family members;– More confidence in his/her own ability to do things;– Understanding language;– Interest in learning;– Interest in playing with others;– How to solve puzzles;– Listen more carefully;– Learn how to count;– Write three or more letters or numbers;– His/her motor skills have improved (Hands, feet, etc.);– Knows first and last name;– Able to listen to and understand English; and– Speak English.

Head Start Parents Questionnaire
• The two questions that received the lowest average score, which included the responses of “some” or “no improvement” were in the following areas: improve reading skills; and communication with others”.
Open-ended Questions• The questionnaire also included five open-ended questions. • From analyzing these responses, it was found that parents were
very happy with the program and the teachers.
• All parents said that their children enjoyed the Head Start program and that they have made new friends.
• Additionally, some parents suggested an increase in the number of hours of the Head Start program, and only one parent said that she would like to see more program structure and a greater emphasis on academics instead of playtime.
Family Night 1st Year Results
Family Night Results : Parents
• To the statement “It is not important to recognize how we are feeling” (a false statement), 60% of participants said it was false at the pre-test while 100% said it was false at the post-test.
• To the statement “If someone does not start using alcohol until they are 18, they are less likely to become addicted,” (a true statement) 26% said it was true at the pre-test while 57% said it was true during the post-test.
• To the statement Men’s and women’s bodies react the same to alcohol, (a false statement), 60% said it was false at pre-test, while almost 80% said it was false at pos-test.
• .

Family Night Results : Parents
• To the statement “It‘s not important to tell your children that you love them,” (a false statement), 53% responded that it was a false statement at pre-test but 86% responded that it was a false statement at post-test.
• A great percentage of parents (87%) strongly agreed that they understand how to set goals for themselves. – Also eighty percent of them said that after the classes
they understand more about how chemical dependency has affected their children.
– Almost all parents said that now they regularly attend an organize group, like a support group where they feel respected and accepted
Parent Focus Groups• They learned "insights" into how children are affected by
drugs. Parents particularly liked role-playing because it helped them to see the children's points of view on drug issues.
• They also said that their children had learned to say "no" to drugs because they have a new understanding that giving into drugs will break families apart.
• Parents said that being with their children at the classes taught them how healthy family members should interact with each other.
• Some parents agreed that having dinner nightly with their children emphasized how important is to have a regular schedule. Being in touch with the daily lives of their children kept them in tune with how the children were doing each day.

Parent Focus Groups
• Parents also said that the classes taught them how to discipline kids in ways that are age-appropriate, without yelling.
• They also said they learned how to be consistent and loving parent and how to communicate better with other people who are important in their lives.
• Parents said they better understand how to motivate their kids and how to talk to them at their level.
• Another client said that she learned the importance of being consistent, that is giving the child a consistent schedule for meal times, games, and even play time.

Parent Focus Groups
Perhaps one of the greatest improvements was in their relationship with their children.
– For example, one client said that she is more patient in dealing with her children when they misbehave.
– Another client said that as a result of the classes, she knows how to give positive reinforcement to her kids and compliment them.
– Participants concurred that the classes provided them with tools to be "better moms".
– One person said that now she realizes that "I don't need drugs to help me get by now".
– Another commented: "I am able to make amends for things I have done wrong with my kids".
Family Night Results : Pre-teen/Adolescents• Most teens were successful in their ability to learn new
things.• Most teens were able to connect with healthy friends.• Adolescents and pre-adolescents completed a group
evaluation that showed high level of satisfaction with the classes.
• Responses regarding the most valuable from teens included:
– “I had the chance to discuss what happened through out my life”
– “It meant a lot because I learned how to deal with my
thoughts and feelings”
– “I had a chance to express myself and learn about things I did not know.”
Family Night Results : Pre-teen/Adolescents
• This group greatly improved in:
– Their understanding of their interest and talents;
– Their ability to communicate and to learn new things;
– Their ability to connect with others;
– Their attitude toward their community; and
– Their ability to control their anger.
Children: Ages 4 to 10
They completed a questionnaire addressing chemical dependency, feelings and healthy choices.
• They all agreed that chemical dependency is a disease.
• The results demonstrate that children were aware that chemical dependency hurts the whole family
• That there are a lot of other children like themselves whose parents who use drug and alcohol.
• All by one agreed that when parents drink or use drugs, they hurt the kids and everybody in the family.
• All of them said that it was O.K. to feel good about
themselves.
• They can make healthy choices for themselves.
Children: Ages 4 to 10• Seventy-one percent of these children said
that they got what they wanted from the program, and the same percentage said their leaders were helpful.
• A higher percentage (86%) said that they thought that it would be good for other kids like themselves to attend groups like that; and the same percentage said that the program made them feel better about themselves and their families and that the program help them to get along with adults.
• Overall, the children from this group learned how to avoid drugs, about chemical dependency, and about how to behave among other things.
Children: Ages 4 to 10
Group Leaders observed great improvements in the following areas:
• Ability to connect with healthy friends and with others;• Knowledge of the impact of alcohol and illegal drugs on
children and knowledge and use of coping skills to deal with stressful situations;
• Understanding of their interests and talents.
They were asked to describe one thing they have learned from the program. Responses included:
“Don’t use drugs no more”“Chemical dependency is a disease”
“I learned about drugs and that it is bad for you” “Kids can not smoke or use drugs, because it is bad”
Primary Knowledge Learned
• Know that parents’ addiction is not their fault;
that chemical dependency is a disease.
• They are not alone.
• They have an adult to talk with.
• Know how to choose and keep safe friends
Alcohol and other drug use even once in a while (for them) is
harmful.

Contacts
Rosemary Tisch(408) 406-0467
Email: [email protected]
.com
Frances Lewis-Johnese, SSPM III
(408) 975-5150
Email: [email protected]
Deborah Dohse(408) 975-5174(408) 829-1340
Email: [email protected]@cws.co.santa-clara.ca.us
Joyce McEwen-Crawford(408) 975-5197
Email: [email protected]
-clara.ca.us

The End





























