Embed Size (px)
Citation preview

Innovationsin
‘Omnineuromodulation’TM
Innovationsin
‘Omnineuromodulation’TM
May 2006May 2006

2
Introduction
• Present a scientific validation for cannabinoids (CBs) asserting their therapeutic effects through ‘Omnineuromodulation’TM
CBs are CB1 agonists that activate presynaptic CB1 endocannabinoid receptors, which are omnipresent throughout the Central Nervous System (CNS)
Action on these receptors modulates neuronal signaling in important brain areas, including those that mediate nausea/vomiting, appetite, and neuropathic pain
• Review evidence showing how omnineuromodulation underlies the therapeutic role of CBs in the management of Chemotherapy-Induced Nausea and Vomiting (CINV), Cachexia, and Neuropathic Pain (NP)
3
The Ubiquitous CB1
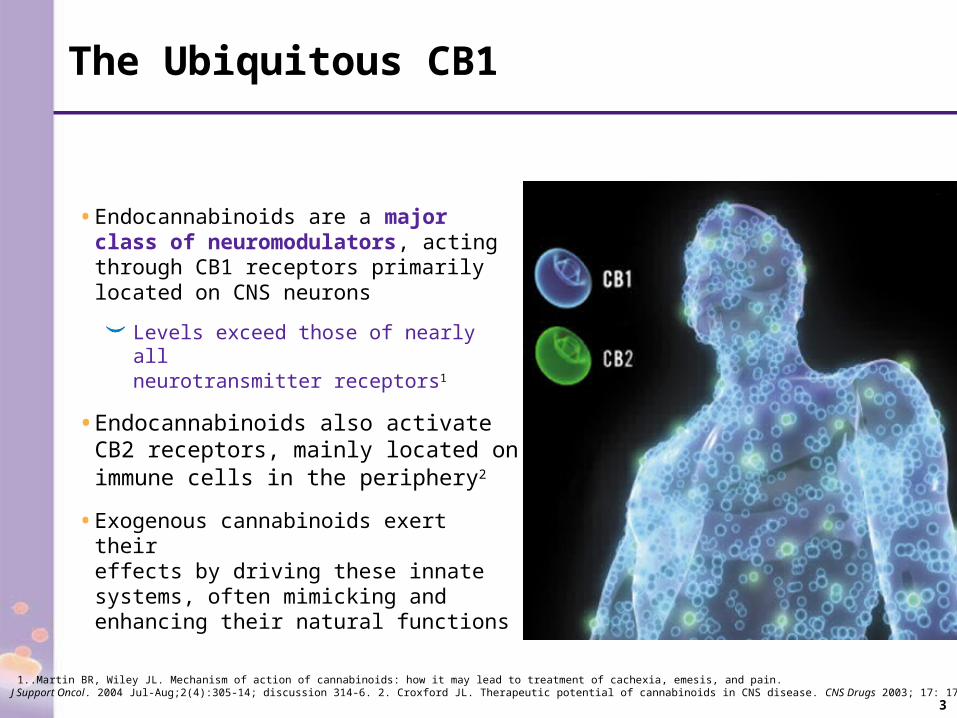
• Endocannabinoids are a major class of neuromodulators, acting through CB1 receptors primarily located on CNS neurons
Levels exceed those of nearly all neurotransmitter receptors1
• Endocannabinoids also activate CB2 receptors, mainly located on immune cells in the periphery2
• Exogenous cannabinoids exert their effects by driving these innate systems, often mimicking and enhancing their natural functions
1..Martin BR, Wiley JL. Mechanism of action of cannabinoids: how it may lead to treatment of cachexia, emesis, and pain. J Support Oncol. 2004 Jul-Aug;2(4):305-14; discussion 314-6. 2. Croxford JL. Therapeutic potential of cannabinoids in CNS disease. CNS Drugs 2003; 17: 179-202.
4
The Ubiquitous CB1
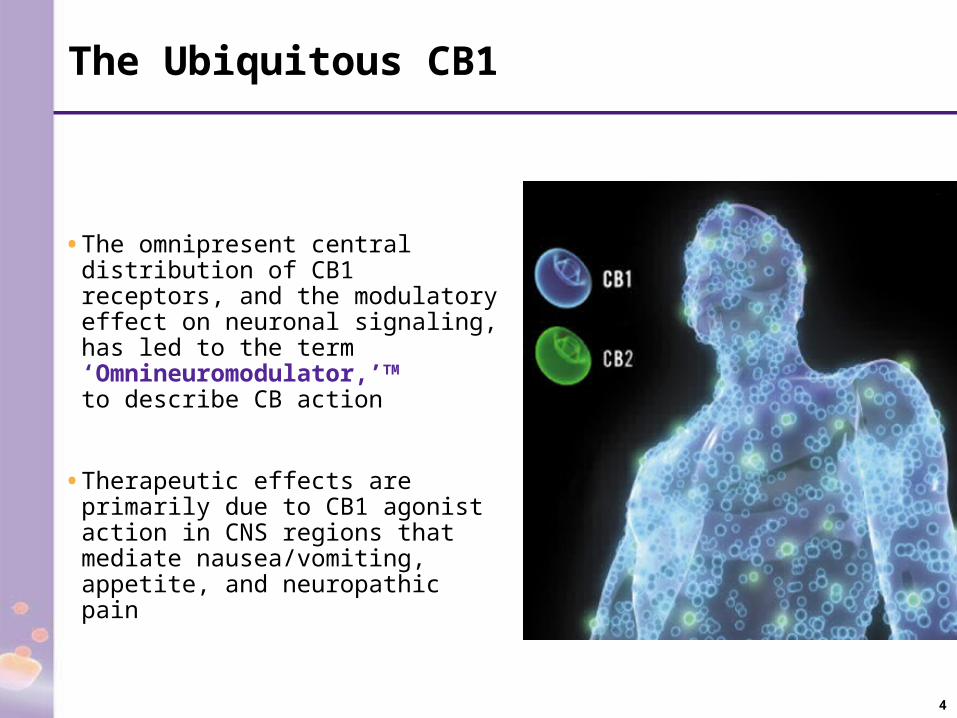
• The omnipresent central distribution of CB1 receptors, and the modulatory effect on neuronal signaling, has led to the term ‘Omnineuromodulator,’TM to describe CB action
• Therapeutic effects are primarily due to CB1 agonist action in CNS regions that mediate nausea/vomiting, appetite, and neuropathic pain

5
Omnineuromodulation
• CBs, such as CESAMET™ (nabilone), act on presynaptic CB1 receptors, similar to innate or “endo”-cannabinoids
Inhibits the release of excitatory (e.g., glutamate) and inhibitory (e.g., GABA) neurotransmitters
• The primary effect on neuronal signaling appears to be inhibitory, but network effects may be complex and, hence, modulatory in nature
• Endocannabinoids act in reverse from classical neurotransmitters by serving as retrograde synaptic messengers
A Sequential Overview of Omnineuromodulation
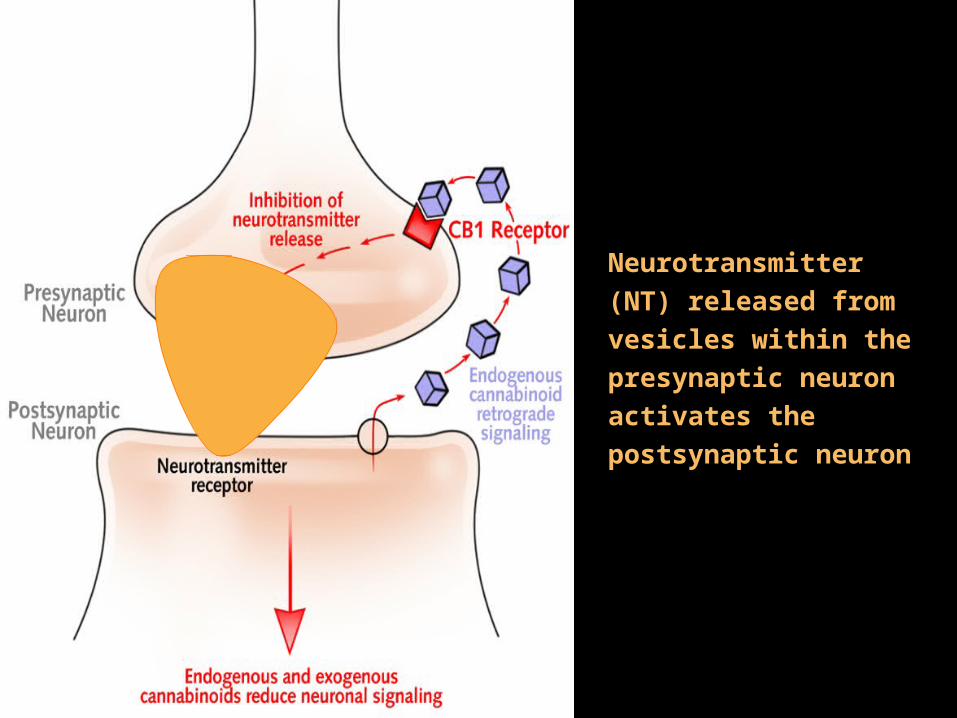
Neurotransmitter (NT) released from vesicles within the presynaptic neuron activates the postsynaptic neuron
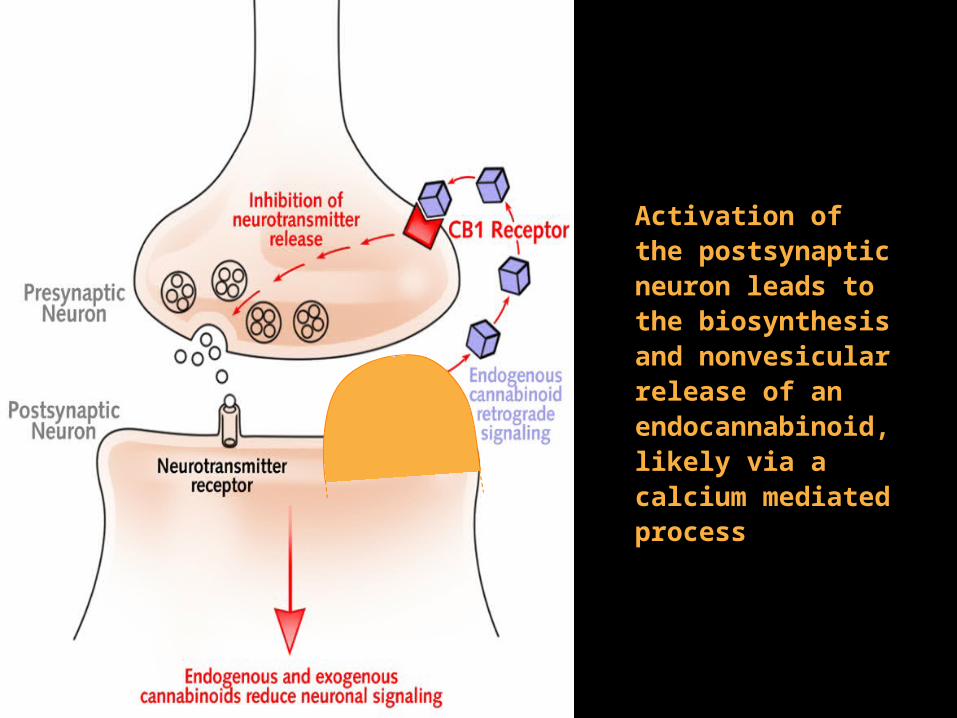
Activation of the postsynaptic neuron leads to the biosynthesis and nonvesicular release of an endocannabinoid, likely via a calcium mediated process

The endocannabinoid diffuses back to and binds to the presynaptic CB1 receptor

The CB1 receptor activates a G protein which can lead to a number of presynaptic downstream events (e.g., effects on ion currents) that result in the inhibition of neurotransmitter release
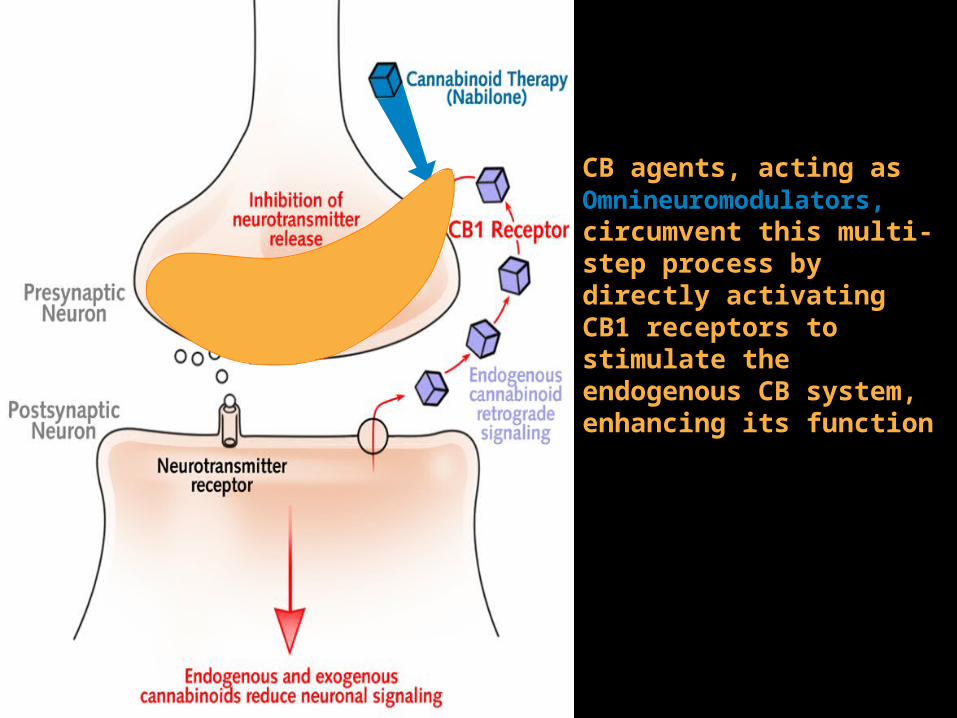
CB agents, acting as Omnineuromodulators, circumvent this multi-step process by directly activating CB1 receptors to stimulate the endogenous CB system, enhancing its function

Anti-emetic, Anti-nausea Effects of Cannabinoids

Causes of nausea and vomiting/emesis: Viral illness Cancer Chemotherapy Radiotherapy

• The Nucleus of the Solitary Tract (NTS) in the DVC receives information about:
Blood-borne emetics via the brainstem (BS) “Chemo-receptor Trigger Zone” Abdominal irritants via vagal afferents
• NTS neurons, in turn, project to a BS central pattern generator, which coordinates vomiting behavior
Dorsal Vagal Complex (DVC)
- NTS
Dorsal Vagal Complex (DVC)
- NTS

Higher cortical and limbic regions (governing taste, smell, sight, pain, memory and emotion) can suppress or stimulate nausea/vomiting through descending connections to the BS emetic circuitry
Cortex Limbic System
Cortex Limbic System
Brainstem Emetic Circuitry
Brainstem Emetic Circuitry
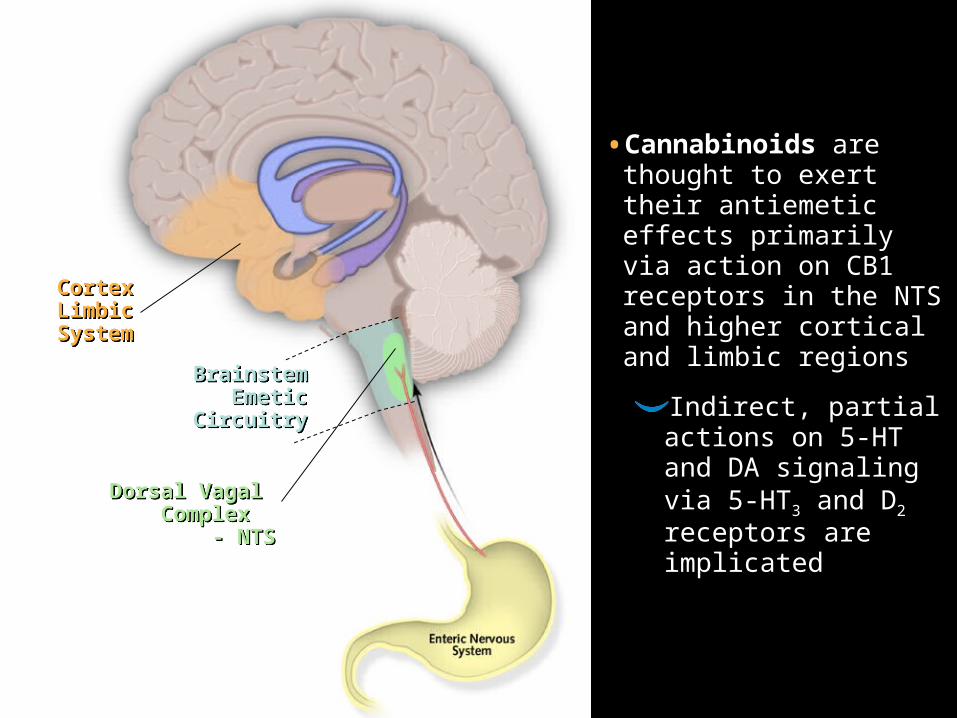
• Cannabinoids are thought to exert their antiemetic effects primarily via action on CB1 receptors in the NTS and higher cortical and limbic regions
Indirect, partial actions on 5-HT and DA signaling via 5-HT3 and D2 receptors are implicated Dorsal Vagal
Complex - NTS
Dorsal Vagal Complex
- NTS
Brainstem Emetic
Circuitry
Brainstem Emetic
Circuitry
Cortex Limbic System
Cortex Limbic System
Potential Action of Cannabinoids in Cachexia
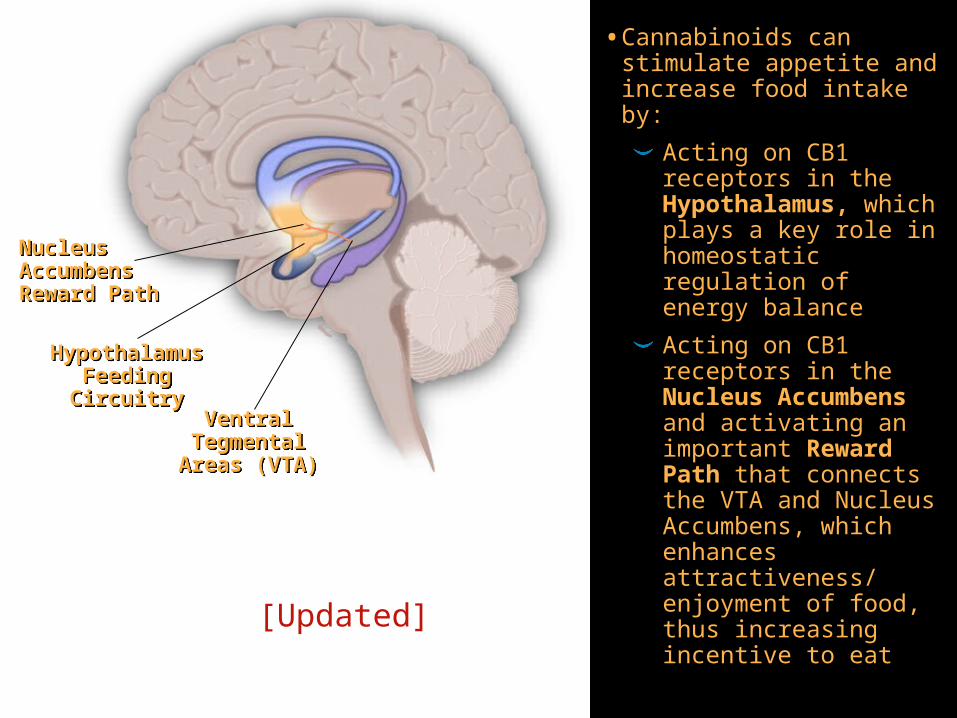
• Cannabinoids can stimulate appetite and increase food intake by:
Acting on CB1 receptors in the Hypothalamus, which plays a key role in homeostatic regulation of energy balance
Acting on CB1 receptors in the Nucleus Accumbens and activating an important Reward Path that connects the VTA and Nucleus Accumbens, which enhances attractiveness/ enjoyment of food, thus increasing incentive to eat
Hypothalamus Feeding Circuitry
Hypothalamus Feeding Circuitry
Nucleus Accumbens Reward Path
Nucleus Accumbens Reward Path
Ventral Tegmental
Areas (VTA)
Ventral Tegmental
Areas (VTA)
[Updated]

Hypothalamus Feeding Circuitry
Hypothalamus Feeding Circuitry
Nucleus Accumbens Reward Path
Nucleus Accumbens Reward Path
Ventral Tegmental Area (VTA)
Ventral Tegmental Area (VTA)
Leptin HormoneLeptin Hormone
• CBs drive the innate cannabinoid system in the hypothalamus to stimulate feeding, and circumvent the partial negative control of the circulating satiety factor leptin hormone1-2
• CBs also increase motivation to eat through interaction with the dopamine and opioid systems in the Reward Path1,3
1. Cota et al, 20032. Harrold and Williams, 20033. Fride et al, 2005

CBs may also promote feeding by acting on CB1 receptors in the Enteric Nervous System to modulate gut-derived satiety signals, such as the peptide cholecystokinin (CCK)
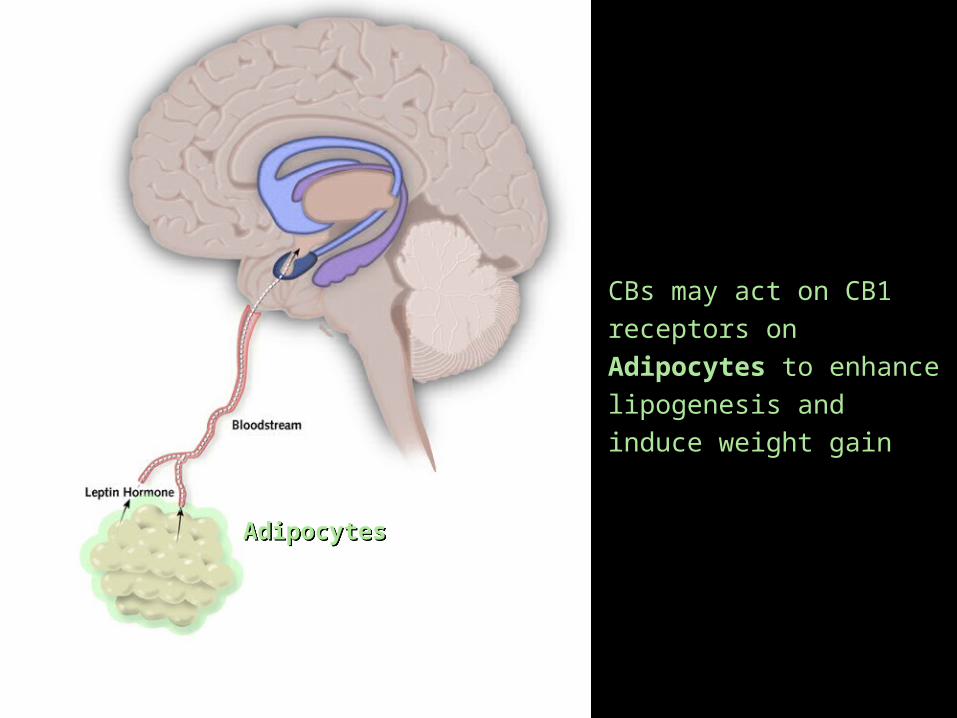
CBs may act on CB1 receptors on Adipocytes to enhance lipogenesis and induce weight gain
AdipocytesAdipocytes
Potential Action of Cannabinoids
in Neuropathic Pain (NP)
23
What is NP?
• NP is caused by primary lesion or dysfunction of the nervous system
Generally chronic
Highly unresponsive to traditional analgesics
Hallmark symptoms include hyperalgesia and allodynia
• Peripheral and central pathophysiological mechanisms may be involved, including an overstimulation and hyperexcitability of nerve paths
• Given the multiple pathologic mechanisms underlying NP and multiple targeting of CBs, CB agents represent a promising potential therapy
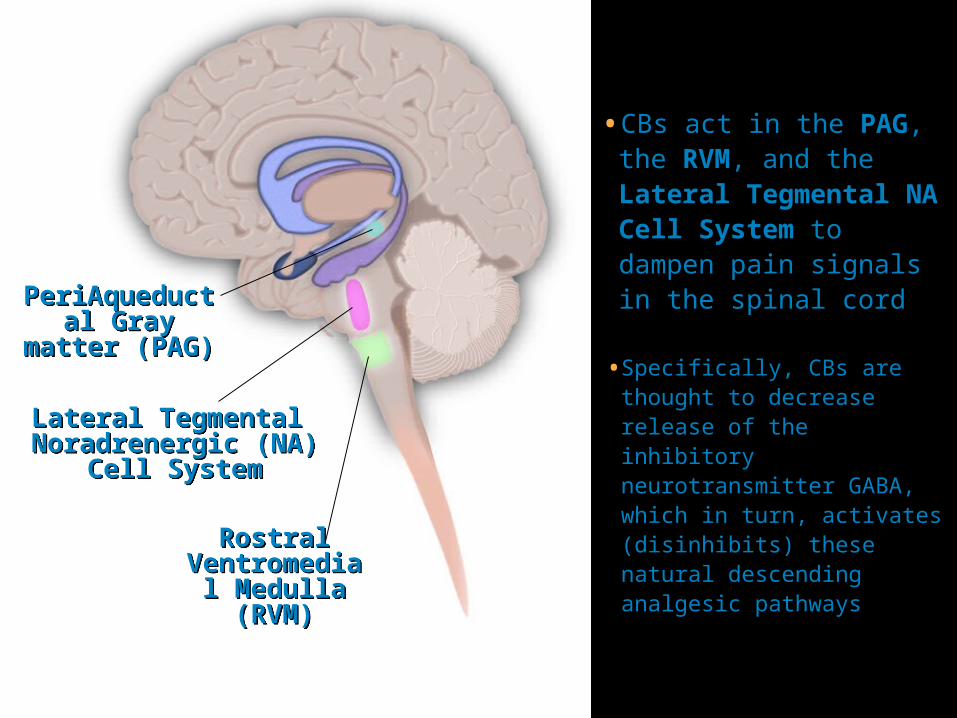
PeriAqueductal Gray matter
(PAG)
PeriAqueductal Gray matter
(PAG)
• CBs act in the PAG, the RVM, and the Lateral Tegmental NA Cell System to dampen pain signals in the spinal cord
Rostral Ventromedial
Medulla (RVM)
Rostral Ventromedial
Medulla (RVM)
• Specifically, CBs are thought to decrease release of the inhibitory neurotransmitter GABA, which in turn, activates (disinhibits) these natural descending analgesic pathways
Lateral Tegmental Noradrenergic (NA)
Cell System
Lateral Tegmental Noradrenergic (NA)
Cell System

CBs weaken ascending pain messages by suppressing noxious stimulus-evoked activity in the VPL of the Thalamus, and are thereby thought to decrease pain sensitivity
Ventral Posterolateral Nucleus (VPL)
Ventral Posterolateral Nucleus (VPL)

Amygdala-mediated analgesic effects of CBs may diminish the unpleasant emotional experience that is a component of pain
Amygdala(Emotion)Amygdala(Emotion)

• CBs produce antinociception in the SC by modulating evoked responses of primary sensory fibers (nociceptors) in the Dorsal Horn, via a presynaptic action on DRG neurons
• CBs act on CB1 receptors to inhibit glutamate release from nociceptors in the SC, reducing excitatory signaling (via NMDA) that mediates the central sensitization of pain
Dorsal Root Ganglion
(DRG)
Dorsal Root Ganglion
(DRG)
Spinal Cord (SC)
Spinal Cord (SC)

• CBs may act on CB1 receptors located on the peripheral terminals of Primary Sensory Neurons (Nociceptors) to inhibit pain transmission
• CBs may also act on CB2 receptors on surrounding immune cells to decrease inflammation and nociceptor excitation, reducing pain sensitivity
Nociceptor Peripheral Terminals
Nociceptor Peripheral Terminals
29
Cannabinoid and Opioid Synergism
• Combination therapy with CB agents and opioids may be an effective approach for NP
• CB and opioid systems appear to work synergistically to reduce pain, by producing analgesic effects in converging brain pathways via different mechanisms
E.g., both activate the descending analgesic pathway in the RVM and PAG by blocking inhibitory GABA inputs
• Opioid analgesics are considered less effective for NP than inflammatory pain, possibly due to depletion of opioid receptors in the spinal cord following peripheral nerve injury
In contrast, there is an upregulation of CB1 receptors in the thalamus which may increase analgesic efficacy of CBs in chronic pain conditions

30
Summary
• CB agonists act as Omnineuromodulators—a term that describes their role in activating CB1 endocannabinoid receptors, which are omnipresent throughout the CNS and modulate neuronal signaling
• Evidence shows that Omnineuromodulation underlies the therapeutic role of CB agents in the treatment of CINV, Cachexia, and NP
• Given potential synergy between CB and opioid systems, combination therapy for NP may be a more effective approach

31
Approved for the treatment of nausea and vomiting associated with cancer chemotherapy in patients who
have failed to respond adequately to conventional antiemetic treatments

32
• CESAMET™ delivers:1
Convenient BID dosing: The usual adult dosage is 1 or 2 mg BID
Predictable pharmacokinetics: Peak plasma concentrations occur within 2 hours following oral administration
Long acting: 8 to 12 hour duration of action
Not detected by the EMIT test2
• In anti-emetic phase III studies, involving 316 cancer patients receiving a variety of chemotherapeutics (including cisplatin), CESAMET™ was shown to be superior in efficacy to placebo, as well as to prochlorperazine, in:1
Reduction of vomiting episodes
Reduction of nausea severity
Improvement in appetite
Investigators’ global impression of efficacy3





























