Embed Size (px)
Citation preview

1
Artificial pancreas device systems in development for the closed-loop control
of type 1 diabetes
Horizon Scanning Centre
March 2015

2
The National Institute for Health Research Horizon Scanning Centre (NIHR HSC) is based at the University of Birmingham in the UK. The NIHR HSC aims to supply timely information to key health policy and decision-makers and research funders within the NHS about emerging health technologies that may have a significant impact on patients or the provision of health services in the near future. The scope of our activity includes pharmaceuticals, medical devices and equipment, diagnostic tests and procedures, therapeutic interventions, rehabilitation and therapy, and public health activities. Horizon Scanning Centre reports can be accessed via our website at: www.hsc.nihr.ac.uk, and the centre can be followed on Twitter at: @OfficialNHSC.
This report presents independent research funded by the National Institute for Health Research (NIHR). The views expressed in this publication are those of the author(s)
and not necessarily those of the NHS, the NIHR or the Department of Health.
The NIHR Horizon Scanning Centre, University of Birmingham, United Kingdom
[email protected] http://www.hsc.nihr.ac.uk/
Copyright © University of Birmingham 2015

3
CONTENTS
EXECUTIVE SUMMARY ................................................................................................................................. 5
ACKNOWLEDGEMENTS ............................................................................................................................... 6
1. INTRODUCTION ....................................................................................................................................... 7
1.1 TYPE 1 DIABETES ................................................................................................................................ 7
1.1.1 Overview of the condition .......................................................................................................... 7
1.1.2 How common is type 1 diabetes? .............................................................................................. 8
1.1.3 The management of type 1 diabetes ......................................................................................... 8
1.2 ARTIFICIAL PANCREAS DEVICE SYSTEMS ......................................................................................... 11
1.2.1 About the technology ............................................................................................................... 11
1.2.2 Different types of systems ........................................................................................................ 12
1.2.3 Stage of development .............................................................................................................. 15
1.2.4 Potential benefits ..................................................................................................................... 17
2. METHODS .............................................................................................................................................. 18
2.1 TECHNOLOGY TYPES INCLUDED ...................................................................................................... 18
2.2 REVIEW STRATEGY ........................................................................................................................... 18
2.2.1 Technology identification ......................................................................................................... 18
2.2.2 Healthcare professionals’ perspective ..................................................................................... 18
2.2.3 Potential users’ perspective ..................................................................................................... 19
3. RESULTS ................................................................................................................................................. 21
3.1 ARTIFICIAL PANCREAS DEVICE SYSTEMS IDENTIFIED ...................................................................... 21
3.1.1 Timeframe to availability .......................................................................................................... 22
3.1.2 Current research setting ........................................................................................................... 22
3.1.3 Level of automation.................................................................................................................. 22
3.1.4 Control algorithm ..................................................................................................................... 22
3.1.5 Glycaemic control strategy ....................................................................................................... 22
3.2 HEALTHCARE PROFESSIONALS’ PERSPECTIVE ................................................................................. 23
3.2.1 Clinical need ............................................................................................................................. 23
3.2.2 Potential benefits ..................................................................................................................... 23
3.2.3 Who might benefit? .................................................................................................................. 24
3.2.4 User-friendly features .............................................................................................................. 24
3.2.5 Perceived interest from potential users ................................................................................... 25
3.2.6 Concerns ................................................................................................................................... 25
3.2.7 Potential barriers to adoption .................................................................................................. 26
3.2.8 Evidence base ........................................................................................................................... 26

4
3.3 POTENTIAL USERS’ PERSPECTIVE .................................................................................................... 27
3.3.1 Physical properties of the controller device ............................................................................. 29
3.3.2 Controller functionality ............................................................................................................ 28
3.3.3 System configuration ................................................................................................................ 30
3.3.4 Use in real life ........................................................................................................................... 31
3.3.5 Potential impact on health and wellbeing ............................................................................... 32
3.3.6 Adoption issues ........................................................................................................................ 33
4. DISCUSSION ........................................................................................................................................... 35
APPENDICES ............................................................................................................................................... 38
Appendix 1 Glossary of terms ............................................................................................................... 38
Appendix 2. Identification sources and search terms ........................................................................... 44
Appendix 3. List of developers identified .............................................................................................. 46
Appendix 4. Technical questionnaire sent to developers ..................................................................... 47
Appendix 5. Healthcare professionals’ questionnaire .......................................................................... 48
Appendix 6. Potential users’ questionnaire .......................................................................................... 50
Appendix 7. Artificial pancreas device (APD) systems identified .......................................................... 52
Appendix 8. Further information on the APD systems identified ......................................................... 64
REFERENCES .............................................................................................................................................. 73

5
EXECUTIVE SUMMARY Type 1 diabetes is a life-long condition that usually begins in childhood and accounts for around 10-15% of all people with diabetes. There is currently no way of preventing its onset, and no cure. The condition is managed on a daily basis by regular self-testing and insulin therapy. For many of those affected, type 1 diabetes can have a negative impact on health and quality of life. A variety of new and emerging technologies are being developed to improve the ways in which type 1 diabetes can be managed. In this report, we focus on one of these new areas of research: externally-worn closed-loop artificial pancreas device (APD) systems. We sought to identify the systems that were being developed by searching online sources of information (such as clinical trial and bibliographic databases, and the medical media) and the NIHR Horizon Scanning Centre database of technologies. We approached the developers to obtain further information about the identified systems. We also involved healthcare professionals and people with type 1 diabetes to find out about their perspectives on this new technology. A total of 18 APD systems were identified and are presented in this report. They were all being tested in clinical research studies. Six of them were being tested in the home environment, while the others were being tested in more formal research settings. The report provides an overview of the levels of automation that the systems were capable of and the different types of control algorithm and strategies that they used to achieve glycaemic regulation. Most of the technologies were still in relatively early stages of development, and the first fully automated commercial APD systems were expected to appear on the market from late 2016 onwards. The report also summarises the views expressed by the healthcare professionals and members of the public with type 1 diabetes who we engaged with to provide input. These include comments about what benefits they think this new form of technology might bring, what the key issues will be concerning their use and adoption into the healthcare system, and the important features that they would like to see in commercial products when they become available. People with type 1 diabetes were very interested in the idea of APD systems and thought they could potentially improve their health and quality of life. In addition to emphasising the importance of safety, reliability and accuracy, preferences were expressed about the physical design, characteristics and functionality that these systems should have if they are to be acceptable to users.
We would welcome your views on this report.
Please take our brief online survey at this link:
https://www.surveymonkey.com/s/X7WW6QX

6
ACKNOWLEDGEMENTS NIHR Horizon Scanning Centre review team Dr Sara Trevitt Senior Analyst Dr Sue Simpson Associate Director Dr Annette Wood Medical Advisor. Healthcare professionals The following clinical experts gave us their advice and views on APD technology:
• Dr Kenneth Robertson, Consultant Paediatrician, Royal Hospital for Sick Children, Glasgow.
• Freya Brown, Diabetes Clinical Nurse Specialist - Paediatrics, Children and Young Patients Diabetes Team, University College London Hospitals NHS Foundation Trust, London.
• Dr Nick Oliver, Consultant Physician and Honorary Clinical Senior Lecturer, Imperial College, London
• Barbara Hudson, Clinical Nurse Specialist in Diabetes (Adult), Queen Elizabeth Hospitals Birmingham NHS Foundation Trust, Birmingham.
Statement of potential conflict of interest: Dr Nick Oliver is lead clinical researcher for one of the technologies presented in this report. Members of the public affected by type 1 diabetes The following people and their organisations enabled us to involve 26 members of the public who gave us their views on APD technology:
• Mr Martin Lodemore, Senior Public Involvement Advisor at INVOLVE, and a member of the NIHR Clinical Research Network Coordinating Centre Patient and Public Involvement and Engagement (PPIE) team.
• Ms Rachel Connor, Head of Research Communications, JDRF UK (formerly known as the Juvenile Diabetes Research Foundation).
The NIHR Horizon Scanning Centre is grateful to all those who helped us to include both a healthcare professionals’ and potential users’ perspective in this report. We thank them for their time and valuable contributions.

7
1. INTRODUCTION
Artificial pancreas device systems According to the diabetes charity JDRF ‘artificial pancreas systems will be the most revolutionary advance in diabetes care since the discovery of insulin’1,2. Although artificial pancreas device (APD) systems will not be a cure for type 1 diabetes, they could offer users a largely hands-off way of managing their condition more easily and effectively in the near future. This horizon scanning report provides: (a) An overview of what this emerging technology is and what benefits it might bring to
people affected by type 1 diabetes. (b) Information about the individual systems that are being developed. (c) A summary of views expressed by healthcare professionals and potential users. A glossary of terms is provided (Appendix 1).
1.1 TYPE 1 DIABETES The human body keeps a constant control over the levels of glucose circulating in the blood. The pancreas senses minute changes in blood glucose levels. It responds by quickly adjusting the levels of hormones that it produces, including insulin and glucagon. These hormones work to regulate the level of blood glucose, and keep it within a healthy range.
1.1.1 Overview of the condition Type 1 diabetes mellitus (also known as type 1 diabetes, T1DM and T1D) is a lifelong autoimmune condition in which the normal mechanism for controlling blood glucose levels does not work3. The term type 1 diabetes has replaced older terms for the same condition, including insulin-dependent diabetes, juvenile onset diabetes, early-onset diabetes, and Insulin-Dependent Diabetes Mellitus (IDDM). It usually develops before the age of 40 (although it can start at any age), and the peak age for diagnosis is in children aged between 10 and 14 years4. Type 1 diabetes is caused by the body's immune system attacking and destroying the pancreatic cells that produce insulin. It is not yet known exactly what makes this happen, although it is thought that a combination of genetic and environmental factors may increase the risk of developing the condition5. It is treated using daily insulin replacement therapy. People with type 1 diabetes need to carefully adjust their insulin doses, particularly when they eat and/or exercise. Other factors can also affect the amount of insulin needed including alcohol consumption, hormonal changes, growth in

8
children, stress and illness. For many people affected by type 1 diabetes, managing the condition can have an impact on their lifestyle and quality of life. Insulin therapy is not a cure for the condition, and even with careful management it is possible for people with type 1 diabetes to spend parts of the day or night with blood glucose levels above or below the recommended healthy range. Short-term complications can occur if blood glucose levels go too low or too high. One such complication is hypoglycaemia (often referred to as a hypo). This is where blood glucose levels fall to a level that could potentially cause harm and initially causes symptoms such as tiredness, weakness, confusion, and increased pulse rate. Severe hypoglycaemia is more serious and the person affected requires urgent assistance. It can cause fits, loss of consciousness, coma, and even death. It is estimated that people with type 1 diabetes in the UK may experience up to ten hypos a week6 and that nearly half of people with type 1 diabetes will experience a severe hypo every year7. If diabetes is not closely managed over long periods of time, there may be a risk of developing long-term complications such as heart disease, nerve damage (sometimes leading to amputation), and sight problems. In the UK, having type 1 diabetes typically reduces the life expectancy of those affected by 20 years8.9. Type 1 diabetes differs from the other more common kind of diabetes, called type 2 diabetes (T2D), where some insulin-producing cells still remain, but either not enough insulin is produced or what is produced does not work properly10. Unlike type 1 diabetes, type 2 diabetes is linked to being overweight and usually affects people aged over 40. It is treated mainly with lifestyle changes (e.g. healthy eating and physical activity) as well as oral medications, insulin, or other injectable medications.
1.1.2 How common is type 1 diabetes? In 2014, around 3.8 million people in the UK had diabetes11. About 10-15% of people with diabetes have type 1 diabetes9,12,13,14, which equates to approximately 380,000-570,000 people in the UK. Recent estimates by NICE put the number of people in the UK with type 1 diabetes somewhat lower than this at 250,00015. More males have the condition than females: 56% compared to 44%16. For children and young people under the age of 19, the estimated UK prevalence of the condition is one in every 430-530 of the population of that age. In 2014, there were approximately 32,550 children and young people with type 1 diabetes in the UK14. The incidence of type 1 diabetes is rising, with the greatest increase being seen in children younger than five years15. In 2011/12, 8,952 people were diagnosed with the condition in the UK, of whom 77% were aged 40 or under at the time17. The incidence for type 1 diabetes in children under 14 years is 24.5 per 100,00018. The NHS spends around £1 billion a year on type 1 diabetes, and 80% of the public money that is spent on diabetes overall goes towards dealing with complications arising from the condition19.
1.1.3 The management of type 1 diabetes Type 1 diabetes is managed on an ongoing daily basis by the person themselves or with the help of someone in a caring role. It involves regularly testing blood glucose levels and injecting insulin as and when needed to keep them within target range. For

9
adults the target range currently recommended by NICE is 4-7mmol/L before meals and <9mmol/L two hours after meals, and for children it is 4-8mmol/L before meals and <10mmol/L two hours after meals8. In 2011/2012, around 6.5% of people with type 1 diabetes were meeting recommended targets for HbA1c (glycated haemoglobin)18. Blood glucose testing Testing blood glucose levels regularly during the day helps people with type 1 diabetes to make informed decisions about diet, activity and insulin dose requirements20. For people with type 1 diabetes the conventional testing method is to use a portable device called a blood glucose meter. First, the side of a finger is pricked using a small gadget called a lancet to draw a small drop of blood. This is then transferred to the test strip in the blood glucose meter, which gives the result within 10 seconds. Devices that can check blood glucose levels continuously and automatically are also available. These are called ‘continuous glucose monitors’ (CGM) or RT-CGM (Real-time CGM). The device is attached just below the skin. The rates of CGM usage are generally low and discontinuation rates are high21,22. Examples of commercially available RT-CGMs include:
• Dexcom G4 PLATINUM system. • Medtronic Diabetes Guardian Real Time system. • Medtronic Diabetes 530G with Enlite Sensor. • Abbott Freestyle Navigator 2.
Insulin therapy • Multiple dose injection (MDI) Type 1 diabetes is treated by injecting insulin to replace the natural hormone. Most people with the condition inject insulin using either an injection ‘pen’ (also called an insulin pen) or a syringe, at least two to four times a day. This manual method is known as multiple dose injection (MDI). Some people with type 1 diabetes prefer this method, as they find that it meets their needs and suits their lifestyle. • Continuous Subcutaneous Insulin Infusion therapy (CSII) An alternative way for people with type 1 diabetes to deliver their insulin is by CSII. This method is becoming more widely used. It involves wearing a battery-powered insulin pump (which is about the size of a small mobile phone) throughout the day and night. The pump delivers a continuous flow of rapid-acting insulin through a very small tube inserted just beneath the skin (called the infusion set) located somewhere on the abdomen, buttock, upper arm or thigh. An insulin reservoir needs to be replenished every two or three days, and the insertion site also needs to be moved regularly. Pre-programmed, personalised basal rates of insulin are delivered, and can be adjusted by the user in real-time to match dynamic changes in insulin requirements, e.g. for meals.

10
Commercially available insulin pumps include:
• Accu-Chek Insight Insulin Pump System. • Cellnovo Insulin Pump System. • DANA Diabecare R Insulin Pump. • Lifescan Animas Vibe Insulin Pump. • Medtronic Paradigm Veo Pump (replaced by MiniMed 640G system, 2015a). • mylife Omnipod insulin pump.
The advantages of CSII over the MDI method are that fewer injections are needed, it can offer a more flexible lifestyle, it reduces the total amount of insulin needed, and potentially enables the user to manage their condition more effectively23. The evidence base for pump therapy (and the NICE guidance) suggests that the benefits are in reduced frequency and severity of hypoglycaemia, and reduced HbA1c; pump therapy achieves this with a neutral impact on weight and can improve quality of lifeb. The disadvantages of CSII include having to test blood glucose levels more often, and an increased risk of infection and scarring at insertion sites. Insulin pumps can be supplied to people with type 1 diabetes by the NHS if they meet the criteria laid down by NICE24. Otherwise, CSII systems can be purchased privately for around £2,000-£2,500, with essential disposables costing a further £1,500 per year. Currently in the UK, around 6% of adults and 19% of children aged under 18 years with type1 diabetes are using insulin pumps25,26. This is somewhat below the 15-20% level for adults who would meet the NICE criteria for insulin pump therapy. Individual choice, suitability and other factors may mean that pump therapy is not appropriate for many of these peopleb. The UK figure of 6% for adults is lower than for other European countries (where pump usage is more than 15%) and the USA (where it is 40%). Reported rates of discontinuation of insulin pump use are high21,27. A UK service level audit of insulin pump therapy usage in adults reported that 93% of the insulin pump centres that took part did not report any barriers in obtaining funding for people who fulfilled NICE criteria, but the audit did identify a significant shortfall in the funding of healthcare professionals required to deliver insulin pump services28. The most advanced kind of insulin pump on the market is called an integrated ‘sensor-augmented pump’ (SAP) system, where the pump includes glucose sensors which report continuous glucose data from a subcutaneous sensor. Examples of devices that have this kind of added functionality include:
• MiniMed Paradigm Veo System (Medtronic) • Vibe (Animas, part of Johnson & Johnson) • G4 PLATINUM CGM (Dexcom).
However, SAPs are not yet widely used and are not currently funded by the NHS. NICE is conducting an appraisal of this technology, and guidance on its use in the NHS is expected in October 201515. a Expert personal communication. b Expert opinion - personal communication.

11
Smartphone applications are being developed to help with day-to-day diabetes management29. Personal digital assistants (PDAs) can help with postprandial (after-meal) glucose control for those who have to calculate their meal boluses. Automated bolus calculators (ABCs) can help with pre-meal insulin dosing for those using insulin without pumps30. Examples of ABCs include Accu-Chek Expert and FreeStyle InsuLinx blood glucose monitoring systems.
1.2 ARTIFICIAL PANCREAS DEVICE SYSTEMS
1.2.1 About the technology What is it? An artificial pancreas device system (also known as an APD system, AP or APDS) is a small, portable medical device that is being designed to carry out the function of a healthy pancreas in controlling blood glucose levels. It uses digital communication technology to automate insulin delivery31. An APD system is worn externally on the body, and is made up of three functional components:
1. A continuous glucose monitor (CGM). 2. A digital controller. 3. An insulin pump (CSII).
As described earlier, two of these three components are already available (CGMs and insulin pumps), and are being used routinely by some people with type 1 diabetes. What is new? The new feature of APD systems is that the CGM and insulin pump are linked together for the first time by a digital controller device (the ‘brain’ or ‘control centre’) containing a control algorithm. An algorithm is a set of rules by which information can be quickly processed through a series of steps to arrive at a logical decision about what needs to be done next. Algorithms are usually written out as a set of mathematical equations, and are used quite widely in medicine to help healthcare professionals reach logical and consistent decisions about patient care when the information going into that decision is complex. How does it work? The control algorithm rapidly analyses information from the CGM and uses it to automatically control the insulin pump to regulate blood glucose levels. Because the controller connects up the other two functions (monitoring and insulin delivery) this is known as ‘closed loop’ control. This will provide a largely hands-free system that can function around the clock much like a non-diabetic pancreas, although it would involve using up to three devices (or even four, if two pumps are needed).

12
What will it look and feel like? At this point in time, the look, feel and functionality of APD systems is not clear, as most systems are still at a prototype stage of development rather than being finished products. For each commercial product, the three functions performed by an APD system (monitoring, control, and insulin delivery) will need to be configured into the form of physical devices in some way. Possible APD system configurations might include:
(a) The control function is performed by a bespoke mobile controller device, which connects wirelessly to the CGM and insulin pump (the controller is carried by the user while the CGM and pump are worn on the body). The controller device would probably look similar to a modified smartphone, but only function for this purpose. In this scenario, one additional device would need to be carried to make the transition from CGM/pump-use to APD systemc.
(b) The control function is integrated into the insulin pump device (or CGM), with a
smartphone or smartwatch application (app) possibly providing a user interface with the controller. In this scenario, no separate device would need to be carried to make the transition from CGM/pump-use to APD system, if the user carried a smartphone or smartwatch anywayc. If they did not, then a smartphone or smartwatch might need to be carried.
(c) The control function takes the form of an app installed on a regular smartphone
or smartwatch. The APD control app would run alongside all the other functions performed by such technologies. Commercial smartphones have been used in research studies, but security concerns have meant that in many cases the normal phone function had to be disabled and other apps removed during testingd. In this scenario, no separate device would need to be carried to make the transition from CGM/pump-use to APD system, if the user carried a smartphone or smartwatch anywayc. If they did not, then a smartphone or smartwatch would need to be carried.
According to an expert, it is most likely that the algorithm will be incorporated into the pump in due course (configuration b). There are huge issues around integrating it into smartphones (configuration c) in that apps may be able to provide some simple levels of functionality, but will probably not be able to run the main control algorithm for quite some time yete.
1.2.2 Different types of systems APD systems can be classified into several different types according to (a) the type of control algorithm that they use, and (b) the type of strategy that they use to achieve glycaemic control. These different types of system can be summarised as follows.
c If the APD system requires two pumps or a second ‘backup’ CGM, then the total number of devices would increase accordingly. d Expert personal communication. e Expert opinion - personal communication.

13
Control algorithm There are four main types of algorithm being used in the development of APD systems and some systems use a combination of these:
1. Model Predictive Control (MPC) MPC is a proactive type of algorithm: it predicts glucose levels at a specific time point in the near future. It can also ‘learn’ about the user’s routine, enabling it to deliver insulin in a more individualised way32.
2. Proportional Integral Derivative (PID)
PID is a reactive type of algorithm: it responds to measured glucose levels. Some user input can make PID systems work even better, and in many systems an insulin feedback (IFB) function is added to detect the insulin on board and help prevent hypoglycaemia32.
3. Fuzzy Logic (FL)
The fuzzy logic type of algorithm (also known as ‘expert rules’) is different from both PID and MPC algorithms in that instead of trying to replicate the actions of natural biological processes, it calculates insulin dose based on how a clinical expert would make real-time adjustments using the information coming in from the CGM – working rather like a ‘virtual’ doctor.
4. Bio-inspired
A bio-inspired form of control is based on a mathematical model of how pancreatic beta cells produce insulin in response to changes in blood glucose levels.
As well as using CGM data, some systems use (or ‘learn’ from) how biometric/physiological factors fluctuate in the individual (e.g. galvanic skin response measured by a special armband during exercise). These systems are called ‘multivariable’ or ‘adaptive’ systems33. In addition to these main approaches, some research teams are developing systems based on artificial neural networks34. MPC and PID algorithms have been the most widely studied: there have been 14 clinical trials of MPC systems and six trials of PID systems35. In these studies, MPC controllers have been associated with slightly fewer episodes of hypoglycaemia per person, and PID controllers achieved a slightly longer time within range. However, there is no evidence from direct head-to-head comparisons of the various types of algorithm that suggests that any of them is better or worse than any othersf. The differences between the various types of control algorithm are very technical and because they are still at the prototype stage there is little publically accessible information available about them. It is therefore too early to be able to comment on what practical advantages they might offer if, and when, they turn into commercial products.
f Expert personal communication.

14
For some APD systems, data could potentially be sent to a cloud-based computing server and shared if ongoing monitoring or support is needed. This would possibly mean that carers could access real-time data remotely, which may be an important feature for some, such as the parents of young children. However, for others this might give rise to potential privacy issues. Glycaemic control strategies • Treat-to-Range or Treat-to-Target In functional terms, APD systems can be classified according to the two different objectives that one might want to achieve in regulating blood glucose:
1. Treat-to-Range (TTR) The objective is to keep blood glucose levels within a personalised window (e.g. between 5-8mmol/L). When the user is within range, the system is quiet and runs on its pre-programmed basal rates. As soon as blood glucose falls below the lower limits of the range, the controller suspends insulin delivery, and if they go up above the top of the range it delivers more insulin. TTR is also as known as Control-to-Range (CTR).
2. Treat-to-Target (TTT) The objective here is to keep levels as close as possible to a specific glucose value (e.g. 6mmol/L). TTT is also known as Control-to-Target (CTT).
• Insulin only or bi-hormonal APD systems can also be classified according to the hormones that are used to achieve glycaemic control.
1. Insulin only Single hormone systems restore the insulin deficiency of type 1 diabetes. However, because there can be delays in sensing changes in glucose levels and in subcutaneous insulin absorption, tight control can be difficult to achieve using insulin alone as the risk of hypoglycaemia increases.
2. Bi-hormonal
Because people with type 1 diabetes often have reduced glucagon production, several research teams are now using a ‘bi-hormonal’ (‘dual’, or ‘multi’-hormonal) approach, in which insulin is used to lower blood glucose while glucagon is used to raise it.
Bi-hormonal control might offer a way of achieving tighter glycaemic control, and be better at avoiding hypoglycaemia. However, glucagon is unstable in solution and needs to be replaced every eight hoursg. The other practical issue is that dual infusion pumps have not been developed yet, so at the moment bi-hormonal APD systems use two separate pumps and two infusion sets, which may not be attractive to users. In the g Expert personal communication.

15
future, there may be other hormones that can be used in bi- or multi-hormonal systems, for example glucagon-like molecules based on islet associated polypeptide (IAPP) and glucagon-like peptide 1 (GLP-1), or prescription drugs such as pramlintide.
1.2.3 Stage of development The international research effort The reason why APD systems are topical at the moment is that the three key components have reached a level of sophistication and practicality that can be combined to create a functional unit. This has led to a concerted push to bring this new technology to market as quickly as possible. Several international research initiatives have been set up to help make this happen, including: • The JDRF Artificial Pancreas Project (APP) Consortium.
This is an international collaboration between 24 centres around the world, which is working to develop around eight different APD systems.
• The Artificial Pancreas@home (AP@home) project.
This is a research programme funded by the European Union, which completed recently having developed a prototype APD system. The project aims were: (a) to create a new improved two-port APD system (i.e. two points of entry into the body) based on well-established components for optimisation, verification and validation of current preliminary algorithms in clinical studies, and (b) to develop and validate a single-port system.
• The Diabetes wiREless Artificial Pancreas ConsortiuM (DREAM). This is an international collaboration between three centres in Israel, Slovenia and Germany, which is developing an APD system.
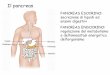
Levels of automation Complex new technologies are typically developed through a series of small progressive steps, a process that can take years or even decades. JDRF has defined six incremental stages on the basis of what the APD technology is capable of doing (Figure 1).

16
Figure 1. The six stages of development towards an artificial pancreas device system36
Two first-generation APD systems (both from Medtronic Diabetes) have been approved and are available for clinical use in the EU37,38,39,40:
1. The threshold suspend MiniMed® 530G with Enlite® sensor system. 2. The predictive Minimed™ 640G with SmartGuard® system.
Clinical research phase The focus of this report is the generational stages 4, 5 and 6 (i.e. closed-loop systems). At the moment, there are several of these progressing through phase 1 and phase 2 clinical research35,41,42,43 (Appendix 1: Glossary for description of clinical trial phases). Moving from inpatient to community settings APD systems are being tested in a number of research settings to see how they perform under different conditions. The most closely controlled setting is to use the device in clinics or hospitals (i.e. inpatient settings). So far, more than 30 inpatient studies have been completed44. Several research teams are now testing APD systems outside of the clinic, in more real-life situations (i.e. outpatient settings)45. As an example, in some studies participants are out and about during the day but sleep in specialist diabetes camps or hotels at night, so that researchers can keep a close check on their glucose levels. A small number of research teams are now testing APD systems in people’s own homes. The level of medical supervision varies from direct monitoring (with the researcher there with the person), to remote monitoring (e.g. they are connected via internet link), to unsupervised use with very careful training and support available at all times. The duration of monitoring may be all the time that the APD system is being used, or just at night. During 2014, the first results from home-use studies were published46,47,48,49,50. In these, people with type 1 diabetes (both adults and adolescents) used APD systems without direct supervision in their own homes for short periods of time. There are currently several APD systems being tested in the home setting in clinical trials; the number of participants in these studies is increasing, as is the duration that the systems

17
are being used for. In order to be sure that APD systems are safe, effective and reliable enough for everyday use, more research of this kind will be needed. The technology will need to work for users with varied needs and lifestyles, and as time goes by different systems may be developed to meet the needs of specific user-groups. There is good evidence that APD systems can work well when used for short periods of time in outpatient settings, especially for night time use51,52,53, and that they can lead to more time being spent within target glycaemic range and a lowered risk of hypoglycaemia51. There are ongoing research studies that will help find out whether such systems can work around the clock for longer periods of time (e.g. several months), and what health and quality of life benefits they may offer to users. When will the technology become available? The first closed-loop APD systems (second or third generation) are expected to appear on the market from late 2016 onwards. However, further testing still needs to be done to find out whether such APD systems can deal safely with all that real life entails, for example in addition to meals, snacks, and physical exercise, factors such as alcohol consumption, stress, and hormonal changes. Developers will not only need to demonstrate that these systems are extremely safe, reliable and effective, but also make sure that their products appeal to users in terms of their design, functionality and connectivity54, and that they are practical for long-term use.
1.2.4 Potential benefits An APD system is not a cure for type 1 diabetes. However, for many people affected by the condition it might provide a new option for managing their condition, as it works automatically for days at a time and is intended to provide more finely-tuned glycaemic control than is possible using current technology. The size of the controller device has been reducing as research progresses, from laptop, to tablet, and now on to smaller wireless smartphone-sized devices. A review in 2014 concluded that APD systems appear to be better than CSII therapy alone in terms of (a) increased time within target blood glucose range, (b) reduced frequency of hypoglycaemia, and (c) better overnight control55. A published survey of people who had personal experience of using APD systems in research studies, found that the main reasons given for using them were personal benefit, convenience, perceived usefulness, and perceived ease of use35,56.

18
2. METHODS
2.1 TECHNOLOGY TYPES INCLUDED Exclusion and Inclusion criteria In this review we include APD systems that are wearable (i.e. externally worn), intended for use in the closed-loop control of type 1 diabetes, currently being tested in human subjects (i.e. in clinical stage research) and classified as second or third generation systems (Figure 1).
The review does not include first generation APD systems (stages 1-3), or biological types of artificial pancreas technologies such as implantable bioengineered systems or gene therapy57.
2.2 REVIEW STRATEGY
2.2.1 Technology identification We identified emerging APD systems for type 1 diabetes by systematically searching a wide range of sources including:
• Technology databases, e.g. the in-house NIHR Horizon Scanning Centre database, and international horizon scanning databases, e.g. EuroScan.
• Research in progress, e.g. clinical trial registries such as ClinicalTrials.gov. • Published research, e.g. bibliographic databases such as MedLine. • Relevant conference reports and abstracts. • Review articles and commentaries in relevant specialist journals. • Websites and publications of relevant organisations and developers.
This was supplemented by searching more general sources of information, such as Google, health media reports, review articles and industry news. The search process took place between July and September 2014. A full list of identification sources and search terms used is provided (Appendix 2). Results from the searches were collated, and each of the developers identified (Appendix 3) were contacted. A technical questionnaire was sent to each of them to request further information, so that we could establish whether or not a technology met the review’s inclusion criteria (Appendix 4). The information obtained helped us to filter the long-list of technologies down to a final short-list, and to organise our results according to the type and stage of development of each technology.
2.2.2 Healthcare professionals’ perspective Four healthcare professionals who specialise in type 1 diabetes were identified and invited to provide expert advice. These experts included both doctors and nurses, and had specific expertise in the care of both adults and children (paediatrics). We sent

19
them a questionnaire which asked for their general views about APD systems and for any specific comments on the individual systems that we had identified (Appendix 5). They were also asked to provide information on any additional technologies they were aware of that had not been identified.
2.2.3 Potential users’ perspective In order to identify some of the key issues about APD technology from a potential users’ perspective we involved members of the public with type 1 diabetes and their carers. User involvement We collaborated with two organisations in order to engage with people affected by type 1 diabetes who were interested in giving us their views about APD technology. The type 1 diabetes charity JDRF posted a short advertisement on their Facebook page, which invited anyone interested in completing our questionnaire to contact the project lead at the NIHR HSC. In addition, the NIHR Clinical Research Network (NIHR CRN) Patient and Public Involvement and Engagement (PPIE) team, who work closely with Diabetes UK, invited a group of their existing contacts who are affected by type 1 diabetes to complete our questionnaire. The team emailed our questionnaire to the people who agreed to be involved. The questionnaire A questionnaire for potential users was developed with input from the PPIE team and an experienced patient advocate with type 1 diabetes (Appendix 6). We invited everyone to complete Part A of the questionnaire (the ‘general views’ section). Part B (about the specific systems being developed) was optional, for those who wished to comment on this. We also provided a list of further information about APD systems. Everyone was given two weeks to return their completed questionnaires to the HSC by email. Analysis of questionnaires The comments received from the questionnaires were analysed using Framework Analysis58. The comments were analysed in two ways: (a) general comments made about APD systems as a new form of technology, and (b) device-specific comments made about the individual APD systems that had been identified. General comments These were first sorted as direct quotes into ‘themes’, e.g. the size of the controller device, its weight, how discrete or bulky it is, etc. Next, to get a clearer picture of the balance of opinion, each theme was sub-divided into:
• Positive ‘likes and wish lists’. • Negative ‘concerns and dislikes’. • Neutral ‘comments’.

20
The direct quotes were placed into the relevant boxes in the matrix (Table 1). Table 1. Thematic matrix used for general comments Theme Likes and wish lists Concerns and dislikes Neutral comments
Theme 1 • Survey quote 1 • Survey quote 2 • Survey quote 3 Theme 2 • Survey quote 4
• Survey quote 5 • Survey quote 6
Theme 3 • Survey quote 7 • Survey quote 8 etc … Device-specific comments The device-specific comments were first sorted as direct quotes by technology name, and then sub-divided according to whether they were positive, negative or neutral, and placed into the relevant boxes in the matrix as follows: Table 2. Thematic matrix used for device-specific comments Device name Likes and wish
lists Concerns and dislikes
Neutral comments
Technology name 1 • Survey quote 1 • Survey quote 2 • Survey quote 3 Technology name 2 • Survey quote 4
• Survey quote 5 • Survey quote 6
Technology name 3 • Survey quote 7 • Survey quote 8 etc . . . Once the two thematic matrices had been completed, the main themes were identified. The comments that related to each main theme or specific technology are summarised in the results section, with direct quotes (presented in italic text) included for illustration.

21
3. RESULTS
3.1 ARTIFICIAL PANCREAS DEVICE SYSTEMS IDENTIFIED A total of 18 APD systems were identified (Table 3). Table 3. Summary of APD systems identified Tech no.
Name of APD system Generation & stage of development
1 Inreda’s artificial pancreas Generation 3 - stage 6 2 Bionic Pancreas Generation 3 - stage 6 3 GlucoSitter Generation 2 - stages 4 or 5 4 Florence Generation 2 - stage 4 5 Diabetes Assistant (DiAs) Generation 2 - stage 4 6 Closed Loop Glucose-Sensing Insulin-
Delivery System Generation 2 - stage 5
7 Closed-Loop Assessment (CLASS) Generation 2/3 - stage 5 + 6 8 Zone-MPC Generation 2 - stage 5 9 Portable Artificial Pancreas System (pAPS) Generation 2 - stage 5 10 Medtronic artificial pancreas system
(product name not known) Generation 2 - stage 4
11 Artificial Pancreas Control Software (APC) Generation 3 - stage 6 (unconfirmed) 12 Bio-inspired Artificial Pancreas Generation 2 - stage 5
(+ capability to work as generation 3, stage 6)
13 Integrated Multivariable Adaptive Artificial Pancreas (MAAP)
Generation 2 - stage 5 (+ capability to work as generation 3, stage 6)
14 Dose Safety Controller (DSC) Generation 2 - stage 5 15 Physiologic Insulin Delivery with Adaptive
Basal (PIDAB) Generation 2 - stage 5
16 ClosedLoop4MealControls (CL4M) Generation 2 - stage 5 17 Predictive Rule-Based Algorithm (pRBA) Generation 2 - stage 4 18 DIABELOOP Generation 2 - stage 4
Appendix 7 provides further details of each of the identified APD systems. Information including links to news articles, recent research publications and ongoing clinical trials for individual APD systems is also presented (Appendix 8).

22
3.1.1 Timeframe to availability An approximate timeframe for when a system may become commercially available in the EU was only publically available for one of the 18 systems (technology 1: end of 2016). Several of the systems are at the prototype stage and the information about them is limited. Of the 18 APD systems identified, five are currently being developed by commercial companies (technologies 1, 3, 10, 11 and 14). Five of the 18 developers were willing to give us very provisional indications of their timeframe to product launch (four of these as ‘confidential’ information). Based on this information we estimate that two systems may become commercially available by the end of 2016, one during 2017, and two more by the end of 2018. Timeframe information on the other 13 systems was not available.
3.1.2 Current research setting Six of the 18 APD systems were being tested by users in the home environment (technologies 1-6). Five APD systems are being tested in outpatient settings (technologies 7-11). The remaining seven APD systems are being tested in inpatient settings (technologies 12-18).
3.1.3 Level of automation Twelve of the 18 APD systems were classified as second generation (technologies 3-6, 8-10 and 14-18). Of these, five systems were at stage 4 (technologies 4, 5, 10 and 17-18), one system was at stage 4/5 (technology 3), and six systems were at stage 5 (technologies 6, 8, 9 and 14-16). Three systems were classified as second/third generation, being at stage 5/6 (technologies 7, 12 and 13). Three systems were classified as third generation, being at stage 6 (technologies 1, 2 and 11), although for technology 11 this information was not confirmed by the developer.
3.1.4 Control algorithm Six of the 18 APD systems were based on a PID-type control algorithm (technologies 1, 6, 10, 11, 15 and 16). Five systems were based on an MPC control algorithm (technologies 4, 5, 7, 8 and 18). Three systems were based on a FL control algorithm (technologies 3, 14 and 17). One was based on both MPC and predictive derivative (PD) algorithms (technology 2), and one was based on a generalised predictive control (GPC) algorithm (technology 13). One system was based on PID, MPC and FL control algorithms (technology 9), and one system was based on a bio-inspired control algorithm (technology 12).
3.1.5 Glycaemic control strategy TTT or TTR Eleven of the 18 APD systems used a TTT strategy for glycaemic control (technologies 1, 2, 4, 6, 7, 10 and 12-16). Three systems used a TTR strategy (technologies 8, 17

23
and 18). Three systems used both of these strategies (technologies 3, 5 and 9). There was one system for which this information was not available (technology 11). Insulin only or bi-hormonal Twelve of the 18 APD systems used insulin only (technologies 3-6, 8-10 and 14-18). Six systems used the bi-hormonal approach (technologies 1, 2, 7 and 11-13).
3.2 HEALTHCARE PROFESSIONALS’ PERSPECTIVE None of the healthcare professionals notified us of any APD systems that had not already been identified by the Horizon Scanning Centre.
3.2.1 Clinical need All of the healthcare professionals agreed that there was a clinical need for APD systems. Comments included: ‘Our best efforts at diabetes control just now are failing to move more than a minority of patients into good glycaemic control.’ ‘Anything that helps reduce HbA1C and BG variability will reduce the risk of complications in the individual, and lead to improved health outcomes in the population.’ ‘Closed loop insulin delivery technology has the potential to improve glucose control by increasing the time in target and reducing glucose variability.’ ‘It is likely to be much longer [than it is for APD systems] before we have a cellular therapy.’
3.2.2 Potential benefits All of the healthcare professionals agreed that APD systems were likely to improve the health and quality of life for people with type 1 diabetes who wanted to use it. Potential benefits cited included: • Day-to-day benefits
‘Improvement of glycaemic control; less glucose variability.’ ‘Reducing the input required from the individual to maintain optimum BG control.’ ‘Prediction of control.’ ‘Less testing.’ ‘Reduction of insulin injections, preservation of injection sites.’ ‘Reduction in working days lost.’
• Psychological benefits ‘Reduce anxiety.’ ‘Less fear of hypoglycaemia for patients and parents/partners.’ ‘Peace of mind for family or carers.’ ‘Greater freedom.’ ‘Improved independence for some.’ ‘Flexibility of insulin doses matching to patients’ lifestyle, i.e. weight loss, less issues around food, managing exercise and social occasions.’ ‘For some it may also increase confidence.’

24
‘Starting the day with a BG within range often motivates young people to keep on top of things during the day.’
• Longer-term benefits ‘Reduction of long term complications and slow down of progression.’ ‘Reduction of complications or disability.’
3.2.3 Who might benefit? One of the healthcare professionals commented that for people with type 1 diabetes, APD technology could provide benefit ‘for all - better control and increased confidence overnight. If they are able to manage BG around food and exercise this will [provide] benefit across the population’. Another expert commented that ‘one of the challenges to overcome is defining which population will benefit, and in which circumstances the technology is most useful’. Several of the experts suggested specific groups that they thought might particularly benefit from this new form of technology: • Babies and very young children, and their parents. • Adolescents.
And those with: • Recurrent hypoglycaemia. • Issues in achieving optimum control despite intensified regimens. • Dawn rise. • Sensitivity to insulin. • Blunting of counter regulatory hormones. • Difficulties managing sport.
3.2.4 User-friendly features Comments from healthcare professionals about the practical features that they thought would be important in a commercial system included: ‘Discrete, integrated blood glucose monitor, bolus advisor, portable, linked to IT, ease of interpretation, readable screen and handset linked by technology such as Bluetooth, easy to operate, appropriate dose delivery, i.e. boluses and basal rate delivery. Manages hypoglycaemia with prediction CGM enabled.’ ’For young people anything that looks and behaves like an iPhone. For parents – if data regarding sensors and insulin delivery could be saved in the cloud, it could be accessed remotely (e.g. when child is on school trip, having a sleepover, etc). Facility to save apps to the device.’ ‘A significant problem to be overcome is alarm fatigue, so an interface that tells people what they need to know and can configure will be vital. Interface integration with their existing devices (smart phones, smart watches, etc).’

25
3.2.5 Perceived interest from potential users All of the healthcare professionals said that they were frequently asked about APD systems. Comments included: ‘It would be very enthusiastically adopted by many, providing they were convinced it was safe.’ ‘Most parents will bite our hands off. Teenagers will be more reticent.’ ‘This new technology will be well received by these groups: parents of young adults, [those] who find day-to-day self-injecting insulin difficult, [those with] hypo unawareness, and long-term poor control.’ ’The issues are very similar [to those about pumps and CGMs], and the evidence is clear that not everyone wishes [to use] the new technology or will be ready to use it. A lot of expensive kit is lying in cupboards around the world.’
3.2.6 Concerns The main issues that concerned the healthcare professionals were: ‘Device failure, their detection, and the action taken by the system and its user. The system needs a supervision layer which can detect a fault specifically and sensitively and can revert to a safe mode while notifying the user (or carer) clearly. In the case of sensor, controller or communication failure, the safe mode will be open loop control with default infusion rates. In the case of pump or infusion failure the default mode will be an alarm state. This safety layer has not yet been adequately described or developed.’ ‘A significant problem to be overcome will be alarm fatigue, so an interface that tells people what they need to know and can configure will be vital.’ ‘There are concerns for people with diabetes around relinquishing control to a machine, and the potential for anxiety and distress that this could bring.’ ‘My concerns would be that the patient does not question the decisions of the pump - it cannot be truly closed loop, as a piece of equipment cannot adapt to all eventualities’. ‘Over-dependence and de-skilling is a worry. Users must retain the knowledge and ability to manage system problems.’ ‘Aligned with the wearable technology will be much enhanced “traceability”, with data being ported to the cloud for surveillance and support - while I and parents will welcome this, there will be concerns about privacy.’
Several of the healthcare professionals expressed concerns about the use of glucagon, including:

26
‘Bi-hormonal systems are not feasible until we have stable, effective glucagon analogues. There are other significant concerns about bi-hormonal systems in terms of what might happen if one or other hormone delivery fails due to individual controller failure or individual infusion failure.’ There were ‘questions around the stability of glucagon, how well it is absorbed subcutaneously and how long it will last in the system. [Such systems are] unable to mix glucagon and insulin, therefore requiring 2 pumps and a sensor. [This raises concerns about] tolerability and effect on skin integrity, lipohypertrophy long-time use. Likely issues around user acceptability may include: a lot of technology, semi-invasive, 2 cannulas, [the need for] understanding time action profile, etc, maintaining continuous glucose monitoring, three needle lines, etc.’ ‘A two pump solution will be unacceptable to almost all users’ (comment on technology 1).
3.2.7 Potential barriers to adoption Several of the healthcare professionals raised the issues of safety and cost effectiveness. Comments included: ‘Adoption will depend less on patient demand than on reimbursement, availability, cost-effectiveness, NICE appraisal and usability, [which] will be significant hurdles. Service delivery is set up to support diabetes technology, but training will be a challenge.’ The key issues will be ‘safety and cost’. ‘‘Would need research to evidence cost effectiveness in the long run, e.g. reduction in admissions, complications, etc.’ ‘Not everyone wishes [to use] the new technology’.
3.2.8 Evidence base One of the healthcare professionals commented about the current evidence base, that so far there have been ‘only short duration studies. No long term outcomes. Do we know if it is truly safe to go closed loop?’ What is needed is ‘long term, real world studies randomised controlled studies with larger number of patients’. Another expert commented about ‘the usual tension of patient and advocate pester power versus a lack of good evidence base’.
Other experts have had experience of training and supporting people with type 1 diabetes using insulin pumps and CGMs, including a low glucose suspend device. One of these experts thought that ‘the advent of sensor-augmented pumps has improved certain patient’s diabetes management and has improved outcomes and quality of life. Next step is forward [is] hugely innovative. [The] pump is now making decisions, will be more accurate overnight when there are no variables, such as activity and food. [The] pump [is] not suspended but anticipating highs and lows and adjusting basal rate necessary. Still operator required to assess bolus requirements and override basal adjustments, not follow closed loop. Only as good as the algorithm programmed. Does not take into account variables. Better than what we currently have though.’

27
3.3 POTENTIAL USERS’ PERSPECTIVE The potential users’ questionnaire was sent to 40 members of the general public who had agreed to be involved in the review by providing their views on APD systems. Twenty-six people returned completed questionnaires, giving a response rate of 65%. Seventeen of the 26 respondents (65%) had been recruited via the ‘open call’ for involvement through the JDRF/Facebook advert route, and nine (35%) came via the ‘invited’ PPIE route. The ages of the people with type 1 diabetes in our sample ranged from 4 to 62 years of age. Seven of the respondents (27%) were children and their parents. The children were aged between four and thirteen years. The age ranges of the 19 adult respondents were: three people in their twenties, seven people in their thirties, four people in their forties, four people in their fifties, and one person in their sixties. All 26 respondents provided general comments about APD technology. In addition, 11 people also provided comments on some of the specific APD systems that had been identified. A summary of the views expressed, under each of the main thematic headings that emerged is below. Comments that related to specific APD systems (or types of APD systems) are summarised under the relevant thematic heading. Overall, positive comments were made about most of the APD systems that had been identified.
3.3.1 Physical properties of the controller device Wearability
It was very important to most of the potential users that the controller device needed to be easy to wear and carry. In terms of appearance, they wanted it to be as small, compact, and discrete as possible: ‘We don’t want lumps and bumps under tight clothes, or masses of tubing that cannot be hidden’. One person said that ‘weight is also important - it’s not comfortable to carry something heavy, especially for children’. Most people envisaged wearing the device under their clothes or in a pocket, while one said that they would like to have an option to ‘allow the machines to be worn off the body, e.g. in a handbag at social occasions’. Several people said they would like the controller device to look sleek and modern, and one said that it would be ‘nice if it was personalisable’.
Wireless connectivity
Several people thought that ‘wireless technology is a plus’, while ‘being connected via cable won’t be practical’. One person had had personal experience of using one of the APD systems (technology 4) while participating in a research study. They commented about the wireless connectivity aspect that they had been ‘initially worried if Bluetooth connection was lost what would happen? But the system just reverts back to open loop again’.
Battery power
A few people were concerned about the battery life of smartphones: ‘The battery life of the equipment and warning signs related to this.’ ‘Smartphones and iPhones in particular have a pretty poor battery life.’ Device-specific comments included one person who said that

28
they liked the fact that technology 1 ‘uses common batteries’, and another person wondered how large the battery pack would be for technology 11. Ease of use
Many people said they wanted the APD system to be quick and easy to programme, read and understand. ‘Being able to see the result frequently on an easy to use screen would be vital’. Some people said that they would prefer a ‘silent’ option for non-audible alerts (e.g. a vibrate-only setting). ‘It’d need to be as quiet as possible, so that I can sleep and it isn’t noticeable in a quiet room (e.g. in a meeting)’. 3.3.2 Controller functionality Data transmission and access
Several people said that frequent (e.g. minute-to-minute) transmission of blood glucose data and adjustment of insulin delivery would be essential in order to achieve good glycaemic control. Less frequent updating could be a concern, for example ‘if calculating insulin needs every 5 minutes and the blood glucose is changing quickly (as it can and does sometimes), I’d worry about the dose being wildly inaccurate.’
Several people said that it would be important to them to be able to monitor and review the activity of their devices frequently. ‘I would like to see what it is doing at all times to feel safe.’ ‘It would be very difficult to suddenly switch trust to a new system with no involvement whatsoever.’ Several people said that they would not want their data to be accessed remotely by healthcare professionals, and would want to ‘take responsibility to look after themselves’ without intervention or ‘remote assistance’. However, one person said that unsupervised use is not what they would be interested in. The parent of a four-year-old child said that they ‘would like to see a cloud in the sky system, so that I could see her blood levels on my smartphone’. One person commented that ‘I hope that any concerns over Bluetooth hacking have been addressed by the time any of these make it to market’.
Control algorithm Several people expressed general concerns about the whole concept of algorithmic control. For example: ‘I would be fearful that the algorithm might not have the self-knowledge and personal experience that I have.’ ‘I can’t see any artificial pancreas being anything like as clever as our own bodies. A piece of equipment can never know about unpredictable things like exercise, stress hormone fluctuations and alcohol consumption, which all affect one’s BG.’ Several people were concerned about whether APD systems would be able to respond quickly enough to fluctuations in glucose levels, and also to take account of the context behind those fluctuations. ‘A problem that might occur is that after a hypo, blood sugars

29
naturally shoot up in a “fake high”, but the pump tries to correct this when it doesn’t need correcting. A FL algorithm would be useful in telling the machine not to correct highs that come immediately after lows. Or at least not correct them at the same percentage.’
Many people thought that APD systems that used ‘intelligent’ and ‘learning’ algorithms were likely to cope better with their real-life needs. Device-specific comments about liking these features were made in relation to technologies 1, 3 and 10. General comments about this included: ‘The systems using fuzzy logic sound good because I would ideally want a system that would adjust itself to my specific physiology.’ ‘While any artificial pancreas must learn from each patient’s data and history … I appreciate from my own experience that doing the same every day does not give you the same results BG wise, so this is very challenging indeed!’ Device-specific comments about being able to individualise the control algorithm to better meet the needs of the user were made about technologies 13 and 17-18. Several people thought that an APD system capable of ‘predicting levels rather than just reacting to change would be beneficial’, and this comment was made in relation to technologies 14 and 17.
TTR or TTT
In terms of TTR versus TTT glycaemic control, one person commented. ‘I’d want a system that would work to a target range rather than a single number. I think this is more realistic’.
Bi-hormonal or insulin only
Many people liked the general principle of bi-hormonal control: ‘this is how a non-diabetic body works’. Device-specific comments in favour of the bi-hormonal approach were made in relation to technologies 1,2 and 7. However, several people were not keen on the fact that bi-hormonal systems could require them to use two pumps instead of one: ‘Prefer not to have another pump delivering glucagon. I feel this is too much to wear and would worry about overusing my injection sites.’ ‘I think glucagon would be a good thing to incorporate into a design that is more developed and reduced in size, but it’s not vital for these initial models.’ In terms of user acceptability, several people thought that the APD systems based on the more conventional insulin-only approach might be easier and quicker to learn how to use. Device-specific comments about one insulin-only system (technology 3) included: ‘The basal/bolus approach feels more familiar than the bi-hormonal approach.’ ‘I like the fact that conventional insulin regimes are used - changing to this system would likely involve less upheaval for most people as the regime would be more similar.’ Level of automation
Most of the people who were involved in providing views were excited by the idea of having an automated APD system. Some people wanted full automation: ‘no input from

30
the patient: freedom!’ Others thought that ‘anything that does not require too much input from the patient would be a bonus!’ Many people thought that ‘alleviating carb counting would be very beneficial.’
Opinion was split as to whether still needing (or having the option) to announce meals and/or manually bolus would be a good or a bad thing: ‘I love the fact that this allows you to bolus for meals.’ ‘The fact that no manual boluses or meal adjustments are needed is good.’ Device-specific comments about liking the fact that manual bolusing and making meal adjustments would no longer be needed were made in relation to technologies 8 and 15. Device-specific comments about wanting to keep the option to bolus for meals were made in relation to technologies 2 and 11. Safety
Issues around the safety and reliability of this new technology were raised by many people. ‘Sufficient support and back up mechanisms in case of equipment failure would be necessary to address my concerns.’ Several people said that sensitivity against sensor failure would be very important. Device-specific comments about liking safety alarm and warning features were made in relation to technologies 1, 3, 8, 13 and 16. One person said of technology 8 that they ‘like the fact that the “independent software layer”’ can send alerts not only to the user but also to remote caregivers’.
Some people had general concerns that the adoption of automated management systems could lead to the de-skilling of people affected by type 1 diabetes: ‘I worry about how some pump and CGM users rely so totally on their diabetes technology, as some people seem to forget how to manage without it!’
3.3.3 System configuration Overall amount of kit
Many people thought that it was very important to keep the overall number of devices and attachment sites to a minimum. Comments included: Would I need to wear a “utility belt” to carry everything?’ ‘You might feel overwhelmed with everything that needs to be plugged into you, hassle of rotating sites for insulin cannula and CGM.’ ‘After doing injections for 31 years, the idea of a ‘permanent’ fixture takes some getting used to.’ Another person commented that having many different body attachments would not be a good option for them and also ‘probably for young children, many of whom are allergic to the tapes used to secure CGM sensors’.

31
Compatibility with existing pumps/CGMs Many people liked the fact that several APD systems were compatible with various existing pumps and CGMs. One person commented that this would ’keep costs down’. Several commented that for people who already use pump and CGM technology, the addition of a third component - a controller device - might be a more easy and attractive proposition than for those who do not use such technology: ‘less training and change would be required for someone already using a pump’. Controller format Many people said that they would like the control function to be integrated into a smartphone. This view was expressed in relation to technologies 2-6, 11 and 18. Several people thought that this would have the benefit of making efficient use of familiar and readily available technology that many people have anyway, and it would also eliminate the need to use an additional controller device. However, several people had practical concerns about using a smartphone as the controller in an APD system: ‘What happens if the smartphone is lost or stolen?’ ‘The phone as a controller could cause friction at school’ if the use of mobile phones in school were not permitted. A few people commented on the controller being a separate device (as opposed to integrated). One person thought that the bespoke controller device used in technology 12 was ‘likely to be costly’, and someone else said that they would prefer to see a smartphone used. Another person suggested that if the readings from a separate controller device could be viewed on a smartphone or other wearable technology, then ‘that will possibly make the device smaller, by not needing a readable display’.
3.3.4 Use in real life Many people thought that being able to rely on an APD system at night would be very useful, both in terms of reducing worry and the extent to which their sleep is currently interrupted. Several people commented that they wanted an APD system that worked 24/7: ’only for 12 hours is no good for me, as I am alive 24 hours a day’. Other comments included ‘Can it be taken off for short periods of time?’ ‘Does the artificial pancreas expect a very consistent lifestyle? ‘Can it cope with a usual diet of fresh fruit and vegetables ruined by a night out with a bottle of wine and burger (with all the trimmings)?’ Many people wanted to know whether an APD system would be able to work during activities such as exercise, swimming and showering: ‘I’d like it to be totally waterproof.’

32
3.3.5 Potential impact on health and wellbeing The overall concept
Everyone who took part in the survey thought that APD technology had the potential to improve health and wellbeing, including the psychological aspects of living with type 1 diabetes. General comments included: ‘Exciting to think this could lead to a new kind of normal for me and fellow type 1 diabetics.’ ‘No need to set alarms to test in the night, etc. I think the psychological benefits would be as great as the improved BG control.’ ‘Although it is not a cure for T1, it comes pretty close in my eyes.’
Comments from young people and parents included: ‘My son could have as close to a ‘normal’ childhood as possible. It would also help eliminate anxiety about complications and management when not in our care. Perhaps even enable us to return to work full time too.’ ‘It would hugely improve the quality of life: dealing with BG levels due to anxiety, growth hormones and excitement.’ ‘Wouldn’t it be good if I could eat pizza?’ - the father of this young person adds ‘wouldn’t it be good to have a system that copes with situations where carb counting is difficult – at friends or eating out, or on school trips and activity weekends. Most of the people who took part in the survey said that they would be keen to try an APD system, if it became available on the NHS, and came with training and support. A few people expressed some reservations about using it, with comments including: ‘I would want to feel more confident about the reliability of a trial device.’ ‘I would be willing to give it a try, but I’m not too keen on having devices attached to my body.’ ‘Relying on technology and trusting it might be hard at first.’ Insulin regime
Many people thought that their insulin regime might be improved by using an APD system. Comments included: ‘Due to my irregularly active work environment, I often hypo during the day (mildly) or spend most of the time snacking to prevent hypos. A system that could manage good control within an irregular environment would be fantastic.’ Comments from young people and their parents included: A mother said that her daughter’s (aged 4) ‘instability is such that we test her every two hours. She will sleep through dangerously low blood sugars in the night, so it’s left to me to catch any lows or extreme highs. This breakthrough would mean not having to prop our sleepy daughter up at 3am whilst trying desperately to feed her high sugar drink and biscuit.’ A young person (aged 13) said: ‘you don’t have to carb count, so you can eat out without getting everything wrong. It would improve your control so that you could live a more happy life - because if you go high or low it can make you feel bad or sad or angry. It would make it easier for your parents at night time.’ One young person (aged 11) had already used an APD system (technology 4), as part of a clinical trial that they had been participating in since September 2014. Their mother said that it had been a ‘very positive experience. We do not want the trial to end. My child

33
says that he feels much safer overnight as he does not worry he may slip in to a nocturnal hypoglycaemic coma’. Most people thought that APD systems could offer them significant health benefits: ‘Less post meal spikes, less variance in BG due to illness/exercise, stress/growth; reduce issues around carb count miscalculations.’ Many people thought that using an APD system could also increase their sense of freedom and ability to live a more normal and spontaneous life. Comments included: ‘I think there will be great psychological benefits as well as ‘medical’. ‘Anything that wipes out the need to always be mindful of possible hypos would be life changing and liberating.’ ‘Take away a lot of stringent day to day planning.’ ‘Feel less dependent on healthcare professionals.’ ‘Not suffering hypos would enable many T1Ds to undertake lifestyle and work choices which are currently denied.’ Several people thought that APD systems could help them with overnight control and sleeping. Comments included: ‘I would love a system that would automatically adjust the insulin dose without waking me up.’ ‘No need to set alarms to test in the night.’
Many people thought that APD systems could be particularly beneficial to children and their parents and carers. Comments included: ‘Due to her young age I undertake night time testing, and it is very tiring.’ ‘I can see particular benefits to children going through puberty where good control of blood sugars can at times be very hard to achieve with current pumps.’
3.3.6 Adoption issues Cost
One person commented that the use of APD systems could ‘help to avoid raised glucose levels, which over time contribute to the development of complications; this will reduce cost to the NHS in the future.’ Several people thought that the use of existing digital technology (e.g. smartphones) and having a controller device that is compatible with currently used pumps and CGMs would keep costs down, require less training for those already using these technologies, and be a ‘big plus for the NHS and funding’.
Training
A few people commented on training issues. ‘Social media is great for this: quick, accurate advice from other users/peers!’ ‘One-size-fits-all tends to lead to protocols that work for the least knowledgeable and willing; however there is a gulf between low level plain English and the language of the medical literature - there are many of us who would love an intermediate level of information to help us understand better how to manage our condition.’

34
Access
Several people had concerns about how widely available this new technology would be as an NHS-funded option for those who wished to use it. ‘I just hope that they will be affordable for patients to have access to.’ ‘It is worrying, as NHS is not good at providing the existing technology (e.g. pumps) - especially for adults, plus CGMs are rarely funded.’

35
4. DISCUSSION We identified 18 APD systems, all of which were still being tested in clinical trials and were not yet available for routine use. The first fully automated APD systems are expected to appear on the market from late 2016 onwards. If and when they become available on the NHS will be a matter for future consideration by NICE and health service commissioners. In terms of the research evidence to support their use, APD systems have so far been shown to work safely in research settings when used during short periods of time51. During 2014, the first results were published on the use of such systems in outpatient settings including the home51. The research effort is now intensifying, with a focus on testing how well these systems work in real-life settings over longer periods of time, and what benefits they may offer. See appendices 7 and 8 for links to ongoing and published trials. The APD systems we identified differed in the way that they worked, including the type of control algorithm and the glycaemic control strategy used. In terms of practical look and feel, there are various design configurations that might be used in commercial systems, for example the control function could be housed in a bespoke controller device, or it might be integrated within an insulin pump or CGM, or a smartphone. Details about product design and functionality were limited, as many of the systems are at early stages of development. The involvement in the review of a small group of healthcare professionals and potential users revealed the general features that they would like to see in finished commercial products (Table 4): Table 4. Desirable features of APD systems identified through consultation with potential users and health professionals Dependability
• Safe (including giving warnings and alarms when user intervention is needed). • Reliable (including good battery life). • Accurate (including sensitive to glucose sensor inaccuracy).
Physical properties
• Small. • Lightweight. • Quiet. • Discrete (i.e. minimally noticeable to others). • Comfortable to wear. • Minimal number of devices/attachments. • Control function integrated into a regular smartphone. • Compatible with existing pumps and CGMs. • Wireless.

36
Functionality
• Easy to use. • Clear visual display that is easy to read and understand. • Overnight use, plus capable of working 24/7. • Usable during exercise, swimming and showering (waterproof). • Transmits and acts upon glucose data rapidly and frequently
(e.g. minute to minute). • Data accessible to the user at any time. • Alleviates carbohydrate counting. • Algorithm that can be individualised and can ‘learn’ about its user.
Some respondents commented on APD systems as being a new 3-part system, while others commented specifically on the addition of a closed-loop control function to insulin pumps and CGMs (which already exist and are used by some people). Some people were not keen on wearing any devices attached to their bodies. Others were already using pump/CGM technology, and saw the transition to using an APD system as less of a leap. Many people thought that closed-loop control was an attractive prospect, and that APD systems had the potential to improve their health and wellbeing. Many thought that APD systems that were compatible with existing pumps and CGMs would be more readily acceptable to users. People had differing views about the degree of automation they would like to see in an APD system. Some wanted it to be completely automatic whilst others wanted to keep the option of announcing meals and exercise, and bolusing. Many people thought that reducing the need to count carbohydrates would be a great advantage. Concerns included:
• Can an automated APD system cope with the complexity of the control task? • Trust issues around handing personal control over to a machine. • Might it lead to de-skilling and overreliance on technology which is fallible? • Would it be practical and comfortable enough to be worth using?
Cost and issues of access through the NHS were also highlighted, as this new technology is likely to be more expensive than current options. However, potential benefits in terms of improved health outcomes and wellbeing were also noted. In this report, we have sought to present an overview of APD technology and the systems that are in development. In addition, we wanted to find out about the healthcare professional and potential user’s perspective on this new technology. Quality of life is an important health outcome in type 1 diabetes, where the burden of self-management is demanding. Because people would literally have to live using the APD technology, psychosocial factors could affect rates of uptake and sustained usage21,59. So far the uptake of insulin pumps and CGMs has been associated with high rates of discontinuation of use21 - as one of our experts said: “a lot of expensive kit is lying in cupboards around the world’’. Research into APD systems has shown that expectations about the user experience, perceived burden of using the technology, and ability to trust it can all act as barriers to engagement60.

37
We found that although many people were interested in the idea of APD technology, there were many questions about the design and functionality of the device systems, and how they might fit into their everyday lives. Many of the answers to these practical questions are not yet available. In addition to demonstrating clinical and cost effectiveness, the concerns and expectations of users will need to be addressed by developers, if APD systems are to be widely acceptable to people with type 1 diabetes. Wider research horizons Both speed and accuracy are critical to achieving tight glycaemic control, and technologies that reduce time delays and sensory errors that occur within the control loop are needed. Areas of active research include the development of faster ways of delivering insulin (e.g. straight into the abdomen); insulin that works faster; rapid-acting analogues of insulin, and ways of speeding up absorption, e.g. by site-warming techniques and co-administration of hyalurinidase61; more stable (pumpable) forms of glucagon; and glucose sensors that are implanted into the abdomen. Other areas of research include the development of single-port systems62 (to replace the current two-port system for monitoring and treatment), and multi-array sensors to improve accuracy35. In addition to APD systems, other technological approaches are also being researched and these may be capable of curing and even preventing type 1 diabetes in the future32. Examples of these earlier-stage developments include:
• Insulin gene therapy, in which insulin secretory machinery is introduced into non beta cells.
• Transplantation - islet cell transplant, stem cell therapy. • Vaccination - immunological methods to prevent type 1 diabetes from happening
in the first place. In the meantime, people affected by type 1 diabetes, healthcare professionals and other stakeholders will continue to await developments in APD systems with interest.

38
APPENDICES Appendix 1. Glossary of terms Term Meaning
Algorithm A technical computing term that is used to mean a set of rules that precisely define a sequence of steps that leads to a decision about needs to be done, usually expressed as a series of complicated mathematical equations.
AP@home A European collaborative research project funded by the European Union. It includes 7 research centres and 5 industrial partners across Europe (including the UK). See website for further information: http://www.apathome.eu/
APD system Artificial Pancreas Device System (or AP, APDS) – see ‘Artificial Pancreas’.
App A common abbreviation for an ‘application’, meaning a computer program designed to run on smartphones, tablet computers and other mobile devices. Source: Wikipedia.
APP consortium See ‘Artificial Pancreas project Consortium’.
Artificial Pancreas An artificial pancreas is a technology in development to help people with diabetes automatically control their blood glucose level by providing the substitute endocrine functionality of a healthy pancreas. Other names used for an artificial pancreas include: glucose-sensor-controlled automated insulin delivery system, and bionic pancreas.
Artificial Pancreas project Consortium (APP)
An international collaborative research project funded by JDRF. It includes 28 research centres around the world (including the UK), and between them they are developing eight artificial pancreas systems.
See website for further information: http://jdrfconsortium.jaeb.org
Basal rate A low background amount of insulin that is delivered continuously for a specified period of time.
BG See ‘blood glucose’.
Bi-hormonal Aka dual-hormonal. Refers to a type of artificial pancreas device system that uses insulin to lower blood glucose and glucagon to raise blood glucose (rather than using insulin alone).
Blood glucose Blood glucose (BG) means the same as ‘blood sugar’. Blood sugar levels are literally the amount of glucose in the blood, sometimes called the serum glucose level. Usually, this amount

39
is expressed as millimoles per litre (mmol/l) and stays stable amongst people without diabetes at around 4-8mmol/L. See Diabetes UK website for further information: http://www.diabetes.co.uk/diabetes_care/Diabetes_and_blood_glucose.html
Blood sugar See ‘blood glucose’.
Bolus dose A dose of insulin taken to correct a rise in blood glucose (also called a correction bolus) or to deal with carbohydrates consumed in a meal or snack (also called a meal bolus).
CGM Continuous Glucose Monitor.
Clinical research stages Phase 1 trials aim to test the safety of the new medical technology in a small group of human subjects.
Phase 2 trials test it on a larger group of patients to get a better idea of whether it works and how well it works in the short-term.
Phase 3 trials test it in larger groups of patients, and compare it against existing treatment/s or a placebo, to see if it works better in practice and if it has important side effects. These phase 3 trials are often longer in duration, and may involve hundreds or even thousands of patients.
See: NHS Choices http://www.nhs.uk/Conditions/Clinical-trials/Pages/Phasesoftrials.aspx
Clinical research stages Phase 1 trials aim to test the safety of the new medical technology in a small group of human subjects.
Phase 2 trials test it on a larger group of patients to get a better idea of whether it works and how well it works in the short-term.
Phase 3 trials test it in larger groups of patients, and compare it against existing treatment/s or a placebo, to see if it works better in practice and if it has important side effects. These phase 3 trials are often longer in duration, and may involve hundreds or even thousands of patients.
See: NHS Choices http://www.nhs.uk/Conditions/Clinical-trials/Pages/Phasesoftrials.aspx
Clinical research stages Phase 1 trials aim to test the safety of the new medical technology in a small group of human subjects.
Phase 2 trials test it on a larger group of patients to get a better idea of whether it works and how well it works in the short-term.
Phase 3 trials test it in larger groups of patients, and compare it against existing treatment/s or a placebo, to see if it works better in practice and if it has important side effects. These phase 3 trials are often longer in duration, and may involve hundreds or even thousands of patients.

40
See: NHS Choices http://www.nhs.uk/Conditions/Clinical-trials/Pages/Phasesoftrials.aspx
Closed-loop control (CLC) Fully automated glycaemic control.
Cloud computing Cloud computing (aka the cloud) is computing in which large groups of remote servers are networked to allow centralised data storage and online access to computer services or resources. Clouds can be classified as public, private or hybrid. Source: Wikipedia http://en.wikipedia.org/wiki/Cloud_computing
Control algorithm See ‘algorithm’.
Control-to-Range (CTR) See ‘Treat-to-Range’.
Control-to-Target (CTT) See ‘Treat-to-Target’.
CSII Continuous Subcutaneous Insulin Infusion, also known as insulin pump therapy (see ‘insulin pump’).
Diabetes There are three main types of diabetes http://www.apathome.eu/project/glossar/diabetes-mellitus/ :
Type 1 diabetes: results from the body’s failure to produce insulin, and presently requires the person to inject insulin. (Also referred to as insulin-dependent diabetes mellitus, IDDM for short, and juvenile diabetes.)
Type 2 diabetes: results from insulin resistance, a condition in which cells fail to use insulin properly, sometimes combined with an absolute insulin deficiency. (Formerly referred to as non-insulin-dependent diabetes mellitus, NIDDM for short, and adult-onset diabetes.)
Gestational diabetes: is when pregnant women, who have never had diabetes before, have a high blood glucose level during pregnancy. It may precede development of type 2 DM.
Diabetes There are three main types of diabetes http://www.apathome.eu/project/glossar/diabetes-mellitus/ :
Type 1 diabetes: results from the body’s failure to produce insulin, and presently requires the person to inject insulin. (Also referred to as insulin-dependent diabetes mellitus, IDDM for short, and juvenile diabetes.)
Type 2 diabetes: results from insulin resistance, a condition in which cells fail to use insulin properly, sometimes combined with an absolute insulin deficiency. (Formerly referred to as non-insulin-dependent diabetes mellitus, NIDDM for short, and adult-onset diabetes.)
Gestational diabetes: is when pregnant women, who have never had diabetes before, have a high blood glucose level during

41
pregnancy. It may precede development of type 2 DM.
Diabetes There are three main types of diabetes http://www.apathome.eu/project/glossar/diabetes-mellitus/ :
Type 1 diabetes: results from the body’s failure to produce insulin, and presently requires the person to inject insulin. (Also referred to as insulin-dependent diabetes mellitus, IDDM for short, and juvenile diabetes.)
Type 2 diabetes: results from insulin resistance, a condition in which cells fail to use insulin properly, sometimes combined with an absolute insulin deficiency. (Formerly referred to as non-insulin-dependent diabetes mellitus, NIDDM for short, and adult-onset diabetes.)
Gestational diabetes: is when pregnant women, who have never had diabetes before, have a high blood glucose level during pregnancy. It may precede development of type 2 DM.
Diabetes UK A UK-based charity, and the operating name of The British Diabetic Association. See website for further information: http://www.diabetes.org.uk/
Dual-hormonal See ‘bi-hormonal’.
Fuzzy Logic (FL) A kind of control algorithm.
An approach to computing based on ‘degrees of truth’ rather than the usual ‘true or false’ (1 or 0) Boolean logic. It allows for fractions, partial data and imprecise data. FL control can be easily modified, and use multiple input and output sources.
Glucagon A hormone that is produced by alpha cells in the pancreas. It serves to keep blood glucose levels high enough for the body to function well. The effects of glucagon are the opposite of the effects induced by insulin. The two hormones need to work in partnership with each other to keep blood glucose levels balanced. Source: http://www.diabetes.co.uk/body/glucagon.html
Glucose A type of sugar that circulates in the bloodstream. See ‘blood glucose’.
HbA1c Glycated haemoglobin. By measuring HbA1c clinicians can get an overall picture of what our average blood sugar levels have been over a period of weeks/months. For people with diabetes the higher the HbA1c, the greater the risk of developing diabetes-related complications. Source: Diabetes UK http://www.diabetes.co.uk/what-is-hba1c.html
Hormone Chemical substances that act like messenger molecules in the body. After being made in one part of the body, they travel to other parts of the body where they help control how cells and

42
organs do their work. For example, insulin is a hormone that's made in the pancreas. When it's released into the blood, insulin helps regulate how the cells of the body use glucose to generate energy. Source: http://kidshealth.org/teen/diabetes_center/words_to_know/hormones.html
Hypoglycaemia (aka hypo) A short-term complication of diabetes, defined as a fall in blood glucose level that exposes the person to potential harm. The main initial symptoms include blurred vision, dizziness, fatigue, hunger and sweating. There is no single cut-off value that applies to all people and situations, although in clinical practice a glucose value of ≤3.9 mmol/L (70 mg/dL) is widely used as the threshold value for initiating treatment63. See also ‘severe hypoglycaemia’.
See: Diabetes UK website: http://www.diabetes.co.uk/Diabetes-and-Hypoglycaemia.html
Insulin A hormone that plays a key role in the regulation of blood glucose levels. It helps control them by signalling the liver and muscle and fat cells to take in glucose from the blood. Insulin therefore helps cells to take in glucose to be used to generate energy. The effects of insulin are the opposite of the effects induced by glucagon. The two hormones need to work in partnership with each other to keep blood glucose levels balanced. Source: http://www.diabetes.co.uk/body/glucagon.html
Insulin on board (IOB) The amount of insulin that is still active in the body from the previous bolus dose.
Insulin pump An externally-worn pump device for Continuous Subcutaneous Insulin Infusion (CSII)
JDRF A global type 1 diabetes charity which is a major research funder (formerly known as the Juvenile Diabetes Research Foundation). See website for further information: http://www.jdrf.org.uk
Meal bolus A dose of insulin administered as a top up before a meal or snack is consumed.
Model Predictive Control (MPC)
A kind of control algorithm.
Used to model the behaviour of complex dynamical systems. MPC models predict the change in the dependent variables of the modelled system that will be caused by changes in the independent variables.
Night time hypoglycaemia (aka night time hypo)
See ‘nocturnal hypoglycaemia’.
Nocturnal hypoglycaemia Hypoglycaemia that occurs during sleep. Symptoms include waking up with a headache, feeling unusually tired and

43
experiencing unprovoked sleep disturbance. See also ‘hypoglycaemia’.
Pancreas A small organ that sits behind the stomach and below the ribcage. It has two important functions: (1) it produces digestive chemicals (enzymes) that are used by the intestines to help digest food, and (2) it produces hormones, the most important being insulin, which regulates the level of sugar (glucose) in the blood. Source: http://www.nhs.uk/conditions/pancreatitis/pages/introduction.aspx
Phase 1, 2 or 3 clinical trial See ‘Clinical research stages’.
Proportional Integral Derivative (PID)
A kind of control algorithm.
A control loop feedback mechanism that calculates an error value as the difference between a measured process variable and a desired set point. The controller attempts to minimise the error by adjusting the process through use of a manipulated variable.
Severe hypoglycaemia
This is where blood glucose levels fall so low that the individual becomes semi-conscious or unconscious or in a coma with or without convulsions8. Urgent assistance from another person is required for recovery, and it is a diabetic emergency. Signs include confusion and disorientation, convulsions/fits/seizures, intense nightmares during sleep, loss of consciousness, and coma. (Note: alternative spelling: hypoglycemia). See Diabetes UK website: http://www.diabetes.co.uk/severe-hypoglycemia.html See also ‘hypoglycaemia’.
T1D Type 1 diabetes.
Treat-to-Range (TTR) A type of glycaemic control, in which the aim is to keep blood glucose levels inside a range (i.e. within an upper and lower limit). Same meaning as Control-to-Range (CTR).
Treat-to-Target (TTT) A type of glycaemic control, in which the aim is to keep blood glucose levels to a set figure. Same meaning as Control-to-Target (CTT).

44
Appendix 2. Identification sources and search terms Identification sources
Name of information source Website
General Google http://www.google.co.uk/ NICE (National Institute for Health and Care Excellence)
http://www.nice.org.uk
NHS Inform www.nhsinform.co.uk Yorkshire and Humber Public Health Observatory http://www.yhpho.org.uk Media and industry news Clinica Medtech Intelligence http://www.clinica.co.uk/ (full access
for members only) MedGadget http://www.medgadget.com Fierce Drug Delivery http://www.fiercedrugdelivery.com Fierce Medical Devices http://www.fiercemedicaldevices.com Medical News Today http://www.medicalnewstoday.com/ SmartBrief https://www2.smartbrief.com Primary research and online libraries Google Scholar http://scholar.google.com/ PubMed.gov http://www.elibrary.bham.ac.uk ZETOC – British Library Database http://zetoc.mimas.ac.uk/ Horizon scanning and health technology assessment sources
NIHR Horizon Scanning Centre - in-house technology database
http://hsc.nihr.ac.uk (database not publically available)
NIHR Health Technology Assessment (HTA) Programme
http://www.nets.nihr.ac.uk/programmes/hta
EuroScan International Network http://www.euroscan.org.uk (members’ only access to database)
ECRI Institute http://www.ecri.org (members’ only access to database)
AHRQ (Agency for Healthcare Research and Quality) Horizon Scanning System
http://www.effectivehealthcare.ahrq.gov
CADTH (Canadian Agency for Drugs and Technologies in Health)
http://www.cadth.ca
Trip database (a clinical search engine for research evidence)
www.tripdatabase.com
The Cochrane Library http://www.thecochranelibrary.com Regulatory authorities EMA (European Medicines Agency) http://www.ema.europa.eu FDA (US Food and Drug Administration) http://www.fda.gov Clinical trial databases ClinicalTrials.gov http://www.clinicaltrials.gov UKCRN Portfolio Database http://public.ukcrn.org.uk/search/ WHO International Clinical Trials Registry http://www.who.int/trialsearch/Default.a
spx NIHR Evaluation Trials and Studies Project http://www.nets.nihr.ac.uk/projects?coll

45
portfolio ection=netscc&meta_P_sand=Project Specialist sources for diabetes Diabetes UK http://www.diabetes.org.uk/ JDRF https://www.jdrf.org.uk/ JDRF/NIDDK Artificial Pancreas Project Consortium (APP consortium)
http://jdrfconsortium.jaeb.org
InDependent Diabetes Trust http://iddt.org/ AP@home project http://www.apathome.eu/ William Sansum Diabetes Center (formerly the Sansum Diabetes Research Institute)
http://www.sansum.org/
Diabetes Research In Children (DirecNet) - Jaeb Center for Health Research
http://direcnet.jaeb.org
Diabetes Forecast http://www.diabetesforecast.org Diabetes Mine http://www.diabetesmine.com diaTribe http://diatribe.org Royal College of Paediatrics and Child Health (RCPCH) National Paediatric Diabetes Audit reports
http://www.rcpch.ac.uk/child-health/standards-care/clinical-audit-and-quality-improvement/national-paediatric-diabetes-au-1
International Society for Pediatric and Adolescent Diabetes (ISPAD)
https://www.ispad.org/
American Diabetes Association (ADA) http://www.diabetes.org/ Advanced Technologies & treatment for in Diabetes (ATTD)
http://www2.kenes.com
European Association for the Study of Diabetes (EASD)
www.easd.org
Search terms The technology
• Pancreas, Artificial (MeSH term) NOT bioartificial • Artificial pancreas • Bionic pancreas • Medical device • Medical technology • Electromechanical device
The medical condition
• Diabetes Mellitus, Type 1 (MeSH term)
Both the technology and condition
• closed(-)loop AND (diabet* OR insulin OR glucose) • Infusion System, Insulin AND closed-loop system*
Clinical role
• Therapy OR Prevention and control
Current phase of research
• Clinical, human.

46
Appendix 3. List of developers identified Commercial developers Company website
Inreda Diabetic http://www.inredadiabetic.nl
DreaMed Diabetes Ltd www.dreamed-diabetes.com
Medtronic Diabetes http://www.medtronicdiabetes.com
Dose Safety Inc http://www.dosesafety.com
Non-commercial developers (research centres and collaborations)
University of Cambridge, UK
Imperial College London, UK
University of Yale, USA, and Kings College London, UK
University of Boston and Massachusetts General Hospital, USA
Sansum Research Institute, and the Universities of California at Santa Barbara, Stanford and Virginia in the USA, University of Montpellier in France, University of Amsterdam in the Netherlands, Schneider Children's Medical Center of Israel in Petah Tikva, Israel, and the Universities of Padova and Pavia in Italy
St Vincent’s Hospital Melbourne, Australia
University of Montreal, Institut de Recherches Cliniques de Montreal and McGill University, Canada
Sansum Diabetes Research Institute and Universities of California at Santa Barbara and Virginia, USA, and the University of Padova in Italy
Sansum Diabetes Research Institute and University of California at Santa Barbara, USA
Oregon Health & Science University, Rensselaer Polytechnic, and Legacy Health Systems, USA
Illinois Institute of Technology, University of Illinois at Chicago and the University of Chicago, USA, and York University in Toronto, Canada
Boston Children’s Hospital + Harvard Medical School, USA
Hospital Clinic of Barcelona, Hospital Clinic of Valencia, Universidad Politécnica de Valencia, Universidad de Girona, Spain
Autonomous University of Madrid and Hospital de Sabadell, Spain
CERITD (a non-profit clinical research centre) in Grenoble, France

47
Appendix 4. Technical questionnaire sent to developers The technology Name of AP system (+ known by any other names?)
Brief description of the system (in simple terms, that a user could
understand)
Commercial developer or funder (if any)
Type of algorithm: e.g. PID, MPC, FL, GPC
Glycaemic control objective: e.g. ‘treat-to-range’ or ‘treat-to-target’?
Which type (generation) of AP system are you developing?
• Automated basal/hybrid closed-loop with meal 47bolusing
• Fully automated insulin closed loop
• Fully automated bi-hormonal closed loop
Intended use: e.g. diurnal, nocturnal, during exercise, patient group?
Stage of development
Current research phase, e.g. Phase 2
Inpatient or Outpatient stage? If out: home, hotel or camp?
For your most recently published research, please state:
Age group, number of participants, care setting (e.g. home, hotel,
diabetes camp, inpatient, supervised/unsupervised), duration of use
Estimated timeframe for European launch (e.g. Q1/2 2016)
Research evidence
Published clinical trials
Unpublished but completed clinical trials
Ongoing clinical trials

48
Appendix 5. Healthcare professionals’ questionnaire The questionnaire was emailed to selected health professionals with an introduction that described what an APD system is, what our report was about, and why we wanted their input. We also provided a ‘further reading’ list with web links, and a glossary of terms. Part A. General comments
Suggested questions Comments
1. Do you think there is a clinical need for this new technology? If so, in what ways might it improve health outcomes?
2. Do you think it would improve quality of life for users? And if so, what issues might it help with?
3. Thinking about any potential benefits, might these be especially helpful for certain patient groups? (e.g. young children, adolescents, those with co-morbidities)
4. In practical terms, what features would make the technology really user-friendly? (e.g. size, visibility of the screen display).
5. Would you have any particular concerns about this kind of technology? If so, please explain your answer
6. Have any of your patients/carers asked you about this new technology, or expressed any views on it? Do you have any thoughts on how enthusiastically it might be adopted?
7. What potential barriers might there be to this technology coming into routine NHS use? (e.g. cost, training, service reorganisation, etc)
8. Do you have any experience of using this new technology? If so, please tell us about it
Any other thoughts or comments

49
Part B. Device-specific comments Device name Type, description and
research stage Comments
Inreda’s artificial pancreas Bionic pancreas Tech name …

50
Appendix 6. Potential users’ questionnaire
The questionnaire was emailed to the people with type 1 diabetes and/or their carers with an introduction that described what an APD system is, what our report was about, and why we wanted their input. We also provided a ‘further reading’ list with web links, and a glossary of terms. Part A. General comments
Suggested questions Your comments
1. Thinking about your quality of life in general, do you think that having a wearable artificial pancreas would improve things for you?
2. If you felt on Q1 that it would be a useful system, can you give some specific examples of how your insulin regime might be improved if you used it?
3. Would you be keen to give it a try? (if on the NHS, with training and support)
4. Would you have any particular concerns about using this kind of system? If so, what would the main issues be for you?
5. Thinking about the practicalities of your day-to-day life, what features would make the system user-friendly for you? e.g. visibility of the screen display.
6. Have you had any personal experience of using these systems? If so, please tell us about your experience.
7. Any other thoughts or comments Text here . . .

51
Part B. Device-specific comments Device name Type, description and
research stage Comments
Inreda’s artificial pancreas Bionic pancreas Tech name …

52
Appendix 7. Artificial pancreas device (APD) systems identified
This table is divided into 3 sections: Key to the developmental stages of APD systems:
Current research setting Total: 18 systems
Stage Generation What the APD system is capable of doing
Home use 6 Stage 4 Second generation Automated basal/hybrid closed-loop with meal bolusing Hotel or diabetes camp (‘outpatient’ setting) 5 Stage 5 Second generation Fully automated insulin closed loop Hospital or clinic (‘inpatient’ setting) 7 Stage 6 Third generation Fully automated bi-hormonal closed loop (insulin and glucagon)
Technology name & alternative name/s
Type Developer Technology description and research stage
Being tested in the home 1 Inreda’s artificial
pancreas Bi-hormonal artificial pancreas
PID algorithm Stage 6 system (3rd generation) Bi-hormonal TTT
Inreda Diabetic
http://www.inredadiabetic.nl/diabetes-product-ontwikkeling/
With the Inreda system (being developed by a Dutch company), insulin and glucagon delivery is fully automated and based on the continuous glucose reading of the sensors. The system includes two pump systems (one each for insulin and glucagon) that are connected to two separate infusion sets, and a CGM with two sensors. It uses an intelligent reactive control algorithm that works out when and how much insulin or glucagon needs to be administered. Insulin delivery is determined by the difference between current and target glucose levels, glucose rate of change, the insulin sensitivity of the patient, and two glucose thresholds, which triggers the delivery of a corrective insulin bolus.
The device runs on two AA batteries, transmits the data to a database every 24 hours. Audible alarms alert patients if they need to check something or to take action. The company say that their system will offer full diet and exercise freedom. Intended use: continuous use in daily life for adults. Currently being tested in the home setting (age

53
Technology name & alternative name/s
Type Developer Technology description and research stage
group 18-75 years; n=12, research setting: home; duration of use: 4 days).
Latest published research use46 Age group: adults (25-66 years), n=11, research setting: home (no meal and exercise instructions), duration of use: 48 hours.
Date for European launch: estimated for second half of 2016. 2 Bionic Pancreas
Bihormonal Artificial Pancreas, Closed-loop glucose-control system, Bihormonal closed-loop glucose-control system
MPC algorithm for insulin, and PD algorithm for glucagon (both customised) Stage 6 system (3rd generation) Bi-hormonal
TTT
USA research team (led by E Damiano, FH El-Khatib and SJ Russell)
Centres: Boston University + Massachusetts General Hospital
http://sites.bu.edu/bionicpancreas/ The Bionic Pancreas is being developed by an American research team for the automated control of blood glucose in people with type 1 diabetes. It automates the subcutaneous delivery of insulin and glucagon to provide consistent and safe blood glucose regulation, which is essential to prevent acute and chronic complications of diabetes. It is a fully automated bi-hormonal closed loop system. There is an option for the user to announce meals, which would trigger the system to calculate and deliver a meal bolus (bolus amount is automatically determined by system, not entered or specified the user). Intended use: 24/7, including exercise; all age groups. Currently being tested in the home setting. Latest published research use48 A publication that includes the findings of 2 studies:
) age group: adolescents (12-20 years), n=32, setting: supervised diabetes camp, duration of use: 5 days.
) age group: adults (21+ years), n=20, setting: supervised outpatient setting, duration of use: 5 days. Date for European launch: information not yet available (estimated launch in USA: first half of 2018).

54
Technology name & alternative name/s
Type Developer Technology description and research stage
3 GlucoSitter Based on the MD-Logic algorithm (MDLAP)
FL algorithm Can work as both stage 4 or stage 5 system (2nd generation) Combination of both TTR + TTT .
DreaMed Diabetes Ltd
http://www.dreamed-diabetes.com/
GlucoSitter is a wireless, fully automated closed-loop artificial pancreas. It uses input data from the glucose sensor, analyses it and commands the pump to deliver the correct dose of insulin at the right time. GlucoSitter is based on the MD-Logic algorithm, which is intended to integrate within an insulin pump or can operate on a dedicated handheld device. The algorithm is based on fuzzy-logic, a learning algorithm, and an alerts module and personalised system setting. The alerts module includes real-time alarms such as impending hypoglycaemia and long-standing hyperglycaemia. The system acts like the patient’s doctor in real-time, monitoring glucose levels around the clock, defining precisely when and how to adjust insulin levels. Intended use: daytime or just for overnight; all age groups. Currently in Phase 3 clinical trials.
According to the company, GlucoSitter is the only closed-loop system which uses conventional insulin treatment rules and automatically adjusts the basal treatment as well as delivering correction boluses (called a ‘basal/bolus’ approach).
Latest published research use47 Age group: children, adolescents and adults; n=24; research setting: 60 hours 24/7 use at home (with overnight remote supervision at night); duration of use: 6 weeks.
Date for European launch: marketing authorisation in Europe is pending (Source: company website).
4 Florence FlorenceD
MPC algorithm Stage 4 system (2nd generation)
UK research team (led by R Hovorka + H Thabit). Part of the JDRF APP Consortium + AP@home consortium.
Florence is being developed by a UK research team based at the University of Cambridge. The system is made up of an Android phone (Nexus 4) running the control algorithm and a translator (translating USB to Bluetooth data stream for Nav II; Triteq UK), a Dana R insulin pump (Sooil) and Nav II CGM (Abbott Diabetes Care). In addition to this portable Android phone version, a prototype version using a

55
Technology name & alternative name/s
Type Developer Technology description and research stage
TTT Centre: Cambridge University
Windows 8 tablet has been used in overnight closed-loop and inpatient studies. For picture see: https://www.dropbox.com/s/wdwc4zxem2z4lii/Florence%20D2A%20%5B2014_10_11%5D.ppt?dl=0
Latest published research use49,50 Age group: adolescents (12-18 years) and adults (18+); n=16 adolescents and n=23 adults; research setting: home, unsupervised; duration of use: 3 to 4 weeks.
Date for European launch: information not yet available. 5 DiAs
Diabetes Assistant
MPC algorithm Stage 4 system (2nd generation) Switchable between both TTT + TTR Called ‘enhanced Treat-to-range’ (eCTR)
International research collaboration (led by B Kovatchev, C Cobelli, E Renard, J DeVries, F Doyle, B Buckingham). Part of the JDRF APP Consortium. Centres: USA (Sansum Research Institute, Santa Barbara, California, the Universities of Stanford and Virginia), France (Montpellier), Netherlands (Amsterdam), Israel (Petah Tikva), and Italy (Padova)
DiAs is being developed by an international team of researchers. It is a modular artificial pancreas platform based on an Android smartphone. The smartphone app contains the computer program that controls blood glucose. It wirelessly receives data from the CGM and gives commands via Bluetooth to an insulin pump.
According to the researchers, one advantage of DiAs is that it can be compatible with any CGM or insulin pump. In their latest research, DiAs received CGM data from one of 2 Dexcom G4 platinum sensors (Dexcom Inc) via a communication box converting the USB signal of the G4 receiver into wireless Bluetooth. DiAs controlled a t: slim insulin pump (Tandem Diabetes Care) via the wireless Bluetooth low-energy signal. Intended use: daytime, night time, during exercise; children and adult. Currently in long-term (1-3 months use) clinical trials in the home setting.
Latest published research use55 Age group: adults; n=20; research setting: supervised outpatient; duration of use: two 40-hour sessions.
Date for European launch: information not yet available. 6 Closed Loop PID algorithm Australian research team The controller for this Australian artificial pancreas system is a

56
Technology name & alternative name/s
Type Developer Technology description and research stage
Glucose-Sensing Insulin-Delivery System bionic pancreas
Stage 5 system (2nd generation) TTT
(led by D O’Neal and A Sharifi). Part of the JDRF APP Consortium. Centre: St Vincent’s Hospital Melbourne
modified smartphone. The Android device processes information coming in from the CGM, and uses it to control the delivery of insulin. Intended use: can be used overnight or as a hybrid closed-loop system 24/24 hours. Currently being tested in the home setting (n=24, aged 14+, duration of use: overnight for 12 hours, for 4 nights in a row). No research has been published yet.
Date for European launch: information not yet available.
Being tested in a camp/hotel setting (outpatient) 7 CLASS
Closed-Loop Assessment
Adaptive MPC algorithm Both stage 5 and stage 6 system (2nd + 3rd generation) Bi-hormonal TTT
Canadian research team (led by A Haidar and R Rabasa-Lhoret). Part of the JDRF APP Consortium. Centres: Montreal University, Institut de Recherches Cliniques de Montreal and McGill University
This Canadian system regulates glucose levels automatically, changing its basal insulin delivery every 10 minutes and sometimes giving glucagon mini-boluses in response to falling glucose levels. The glucagon boluses are small in size, leading to a total daily glucagon dose of (in most cases) less than 20% of that used to treat severe hypoglycaemia.
According to the researchers, users (more than 250 tests so far) did not report any symptoms from the small amount of glucagon delivery, which was also effective in preventing hypoglycaemia. For meals, the system gives meal boluses. The company say that they have shown that the system has the potential to alleviate carbohydrate counting without loss of glucose control. The user only has to describe the meal as small, medium or large. Intended use: day and night, exercise; adults and children. Currently in Phase 2 and Phase 3 clinical research. Being tested in a diabetes camp setting: age group 8-17 years, n=33, duration of use: 3 nights in a row.
Latest published research use64 Age group: 12+ years, n=30, setting: inpatient, duration of use: 24 hours.
Date for European launch: information not yet available.

57
Technology name & alternative name/s
Type Developer Technology description and research stage
8 ZMPC Zone-MPC
MPC algorithm Stage 5 system (2nd generation) TTR
USA and Italian collaboration (led by FJ Doyle and E Dassau). Part of the JDRF APP Consortium. Centres: USA: Sansum Diabetes Research Institute (USA), and Universities of California Santa Barbara and Virginia. Italy: University of Padova
The researchers describe the ZMPC algorithm as being the next generation of MPC-type control models. They say that their TTR strategy is a more natural control strategy than TTT. ZMPC uses a dynamic model that relates the effect of subcutaneously injected insulin on blood glucose concentration, and uses this to make predictions into the near future. For a given desired glucose target zone, the model can be used to calculate how much insulin needs to be delivered in the future in order to keep to this glucose target value or zone. The first of these insulin amounts is commanded to the insulin pump and delivered to the patient, and the calculations are repeated when new information becomes available (i.e. a new CGM measurement comes in). Intended use: 24+ hours (including exercise), all age groups. Currently in Phase 2 clinical trials. Currently being tested in a hotel setting (age group 21-65 years; n=36; duration of use: 2 x 24-27.5 hours).
Latest published research use65 Age group: adults, n= 12, setting: inpatient, duration of use: 24 hours.
Date for European launch: information not yet available. 9 pAPS
portable Artificial Pancreas System
MPC, PID and FL algorithms Stage 5 system (2nd generation) TTR + TTT
USA research team (led by FJ Doyle and E Dassau). Part of the JDRF APP Consortium. Centres: Sansum Diabetes Research Institute (USA) and University of California at Santa Barbara
This is a closed-loop system is being developed by a USA-led research team. It is composed of the Artificial Pancreas System platform (APS) inside a portable computer. The system connects a subcutaneous CGM and a subcutaneous insulin delivery pump for automated adjustment of insulin dosing. The researchers say that their APS has been safely used in over 500 individual clinical sessions at 12 leading clinical research centres around the world. Intended use: 24+ hours (including exercise), adults. Currently in Phase 2 clinical research.

58
Technology name & alternative name/s
Type Developer Technology description and research stage
Latest published research use66,67 Age group: 12-65 years, n=53, setting: inpatient, duration of use: 22 hours.
Date for European launch: information not yet available. 10 Medtronic
artificial pancreas system (product name not yet available). In research studies, versions of this system have been known by the following names: OCL Overnight Closed Loop System and ePID MiniMed external physiological insulin delivery system
PID algorithm with insulin feedback (IFB) Stage 4 system (2nd generation) TTT
Medtronic Diabetes Prototypes of the system are being tested by USA and UK research teams (led by S Weinzimer and B Buckingham in the USA + P Choudhary in the UK). Part of the JDRF APP Consortium. Centres: USA University of Yale, UK Kings College London.
This automated basal/hybrid closed-loop system, which operates with meal bolusing, is being developed by Medtronic Diabetes. Versions of the technology are being tested by research teams in both the USA and the UK (at Kings College London). The system is based on a PID controller that includes an insulin feedback (IFB) element in the algorithm. This functions rather like an ‘insulin-on-board’, subtracting from insulin delivery based on previous insulin delivery. Further technical details are not yet publically available. Currently being tested in a diabetes camp setting: age group: 10-35 years, n=46, duration of use: 12 hours overnight.
Date for European launch: information not yet available.
11 APC Artificial Pancreas Control software Oregon bi-hormonal closed-loop system
A PID-like controller:
‘Adaptive Proportional Derivative’ (APD) algorithm
Legacy Health Systems/ USA research team (led by K Ward, W Bequette + J Castle). Centres: Oregon Health & Science University,
APC is being developed by an American research team who are testing it with two CGMs and two pumps. The APC controller software runs on a smartphone device, which connects wirelessly with the other components. The system uses a custom made battery pack. It is capable of delivering both a pre-meal insulin bolus and automated insulin or glucagon infusion. According to the researchers, the unique thing about their system is that it uses its PID-like controller working in

59
Technology name & alternative name/s
Type Developer Technology description and research stage
Stage 6 system (3rd generation). Note: this has not yet been confirmed by developer Bi-hormonal Not known if TTT and/or TTR
Rensselaer Polytechnic and Legacy Health Systems
concert with a mathematical model of glucose regulation, and this enables it to adjust for changes in insulin sensitivity. Currently in Phase 2 clinical research in outpatient settings (hotel).
Latest published research use34 Age group: 21-65 years, n=13, setting: inpatient, duration of use: 28 hours.
Date for European launch: information not yet available.
Being tested in an inpatient setting (clinic/hospital) 12 BiAP
Bio-inspired Artificial Pancreas
A ‘bio-inspired’ algorithm Stage 5 system with capability to work in stage 6 mode (2nd/3rd generation) Bi-hormonal TTT
UK research team (led by D Johnston, P Georgiou and N Oliver). Centre: Imperial College London
http://www3.imperial.ac.uk/bioinspiredtechnology/research/bionicpancreas
The BiAP system uses a control algorithm based on a mathematical model of the way that pancreatic beta-cells (β-cells) work. The algorithm runs on a low-power miniature silicon microchip within a portable handheld device which interfaces the other components of the artificial pancreas. The researchers are currently using the Enlite sensor (Medtronic) and Accu-Chek insulin pump (Roche), however the BiAP handheld unit can be integrated with any of the commercially available sensors and pumps.
Intended use: throughout the day (including exercise and other activities of daily living) for adults. Currently in Phase 2 clinical research. The researchers aim to start unsupervised home studies in August 2015.

60
Technology name & alternative name/s
Type Developer Technology description and research stage
Latest published research use68 Age group: 18-75 years, n=20, research setting: supervised in a clinical research facility (inpatient), duration of use: 24 hours.
Date for European launch: information not yet available. 13 MAAP
Integrated Multivariable Adaptive Artificial Pancreas
Generalised Predictive Control (GPC) algorithm Stage 5 system with capability to work in stage 6 mode (2nd/3rd generation). Bi-hormonal TTT
USA and Canadian research team (led by A Cinar + K Turksoy). Part of the JDRF APP Consortium. Centres: Illinois Institute of Technology, University of Illinois at Chicago, University of Chicago, and York University (Toronto)
Research team’s web page: http://www.iit.edu/ecdre/research/new_awards.shtml
This American/Canadian system uses GPC, plus a hypoglycaemia early alarm system. Both systems use recursive models updated at each sampling time. Subcutaneous glucose concentrations and several physiological signals from a sports armband are collected and used in glucose prediction models and control algorithms. Intended use: day and night, 24/7.
Latest published research use69 Age group: 18-35 years, n=9, research setting: inpatient, duration of use: 32-60 hours.
Date for European launch: information not yet available.
14 DSC Dose Safety Controller
FL algorithm (and ‘Dynamic Bayesian Network’) Stage 5 system (2nd generation) TTT
Dose Safety Inc http://www.dosesafety.com/
This American system is designed to provide fully automated closed loop glucose control 24/7. The DSC software runs in the background and requires minimal user interaction. The system has 3 modes of operation: (a) auto-dosing (the default mode), (b) suspended, and (c) disabled. In auto-dosing mode, the insulin pump only infuses dose amounts calculated by the Fuzzy Logic Dosing Module (FLDM). Auto-dosing provides all of the user’s insulin needs: after meals, during fasting periods.
The DSC automatically switches from the auto-dosing mode to the suspended mode whenever:

61
Technology name & alternative name/s
Type Developer Technology description and research stage
(1) The user manually boluses insulin using insulin pump. Auto-dosing
resumes after user-selected time delay. Note that when the user manually boluses, they are interacting directly with the insulin pump. No user interaction with the DSC system is necessary.
(2) Hypoglycaemia is predicted. The system reverts to auto-dosing after actual blood glucose values begin rising. No basal insulin is delivered in the suspend mode.
(3) The DSC automatically switches to the disabled mode when the insulin pump or the CGM subsystems become inoperable or when the user disables the auto-dosing. When auto-dosing is disabled, the insulin pump reverts to the user’s basal schedule.
Intended use: daytime, night time, during exercise. Currently in later stage feasibility studies (no publications yet). Date for European launch: information not yet available.
15 PIDAB Physiologic Insulin Delivery with Adaptive Basal
Modified version of a PID algorithm Stage 5 system (2nd generation) TTT
USA research team (led by GM Steil + A Dauber). Part of JDRF APP Consortium. Centres: Boston Children’s Hospital + Harvard Medical School
This American system is fully automated, and does not require meal announcement or manual insulin delivery. It includes a meal identification algorithm which is designed to allow the insulin normally used to cover a meal to be delivered within the first 15-30 minutes of meal, with somewhat more insulin delivered between 30-45 minutes of the meal and approximately the same amount delivered by 60 minutes. It includes an adaptive basal adjustment which allows changes in basal rate, similar to those observed in most pump users to be affected over a ~30 minute interval with limited hypo or hyperglycaemic excursions (target ±15 mg/dL). Intended use: 24 hour, all ages.
Date for European launch: information not yet available. 16 CL4M
PID algorithm (modified by
Spanish research team (led by FJ Ampudia-
Research team’s website about CL4M: http://closedloop4meal.org/

62
Technology name & alternative name/s
Type Developer Technology description and research stage
ClosedLoop 4Meal Controls
SMRC-based external loop adjustments) Stage 5 system (2nd generation) TTT
Blasco, I Conget, J Bondia and J. Vehí). Centres: Hospital Clinic of Barcelona, Hospital Clinic of Valencia, Universidad Politécnica de Valencia, Universidad de Girona
According to the Spanish research team developing this system, the innovative element of this closed-loop controller is a safety auxiliary feedback based on sliding mode reference conditioning (SMRC), which they say has been demonstrated (in simulation studies) to limit over-dosing on insulin and the resulting hypoglycaemia, reducing glycaemic variability. The system follows a two-Stage approximation to constrained control, and is claimed to be sensitive against sensor failures. The algorithm, called ‘SAFE’, is a security loop to be added to the main control loop. Currently in Phase 1 clinical research. Date for European launch: information not yet available.
17 pRBA Predictive Rule-Based Algorithm
FL algorithm Stage 4 system (2nd generation) TTR
Spanish research team (led by M Rigla). Centres: Autonomous University of Madrid and Hospital de Sabadell.
pRBA is hybrid artificial pancreas system being developed by a Spanish research team. The algorithm is based on the knowledge of medical experts and its ability to predict glucose levels over the next 30 minutes. It calculates the amount of insulin needed every 5 minutes, using CGM values, information on daily events such as carbohydrate intake, and its prediction of glucose levels. Each system is also individualised to its user based on their body weight and sensitivity to insulin. Intended use: 24 hours (including exercise). Currently in Phase 1 clinical research.
Latest published research use70 Age group: adults 18+ years, n=10, research setting: clinical research facility (i.e. inpatient); duration of use: 12 hours.
Date for European launch: information not yet available. 18 DIABELOOP MPC algorithm
Stage 4 system (2nd generation)
French research team (led by PY Benhamou). Centre: CERITD (a non-profit clinical research centre), Grenoble
This semi-closed loop system is being developed by a French research team. It consists of an MPC algorithm and controller uploaded onto an android smartphone, which receives information from a CGM (Dexcom) and drives a patch pump (Debiotech) under continuous telemonitoring (i.e. remotely). It has the potential for user information input (e.g. meals, physical activity). Intended use: 24 hour.

63
Technology name & alternative name/s
Type Developer Technology description and research stage
TTR
Currently in Phase 2 clinical research. A study is planned for 2015 in which participants will sleep in an inpatient setting but go out to restaurants during the day time (n=36, monitored throughout, duration of use: 72 hours).
Latest published research use71 Age group: adults over 18 years, n=12, research setting: inpatient, duration of use 5 hours.
Date for European launch: information not yet available.

64
Appendix 8. Further information on the APD systems identified 1. Inreda’s artificial pancreas General information
• Company website product pages: http://www.inredadiabetic.nl/diabetes-product-ontwikkeling/ and http://www.inredadiabetic.nl/news/
Published research • van Bon A, Luijf YM, Koebrugge R et al. Feasibility of a portable bihormonal closed-loop system to control glucose excursions
at home under free-living conditions for 48 hours. Diabetes Technology & Therapeutics 2014;16(3):131-136. http://www.ncbi.nlm.nih.gov/pubmed/24224750
Ongoing research • A Dutch study is looking at home use with no meal and exercise instruction (2 centres in the Netherlands: Arnhem and
Amsterdam) (n=12, aged 18-75, refs: APPEL 4 NCT02160275) running last quarter of 2014. Study title: ‘Algorithm to Control Postprandial, Post Exercise and Night Glucose Excursions in a Portable Closed Loop Format, APPEL 4’. http://www.clinicaltrials.gov/ct2/show/NCT02160275
2. Bionic Pancreas General information
• Research team’s webpage about Bionic Pancreas: http://bionicpancreas.org/ • Cardiometabolic Health Congress. The bionic pancreas. Presentation by Edward Damiano, 29 January 2015.
http://cardiometabolichealth.org/2014/General_Sessions/Friday/Bionic-Pancreas.pdf • MedPage Today. Look back at 2014: the artificial pancreas. News article, 29 December 2014.
http://www.medpagetoday.com/Endocrinology/GeneralEndocrinology/49342 • Time Magazine. The next best thing to a cure for diabetes, 29 Jan 2015. http://time.com/3687291/the-next-best-thing-to-a-
cure-for-diabetes/ • BBC News. Bionic pancreas: a new dawn for diabetics? News article, 31 Aug 2014. http://www.bbc.co.uk/news/health-
28810813 • National Institutes for Health. Bionic pancreas outperforms insulin pump in adults, youth. Press release, 15 June 2014.
http://www.nih.gov/news/health/jun2014/niddk-15.htm • Fierce Medical Devices. Artificial pancreas beats out insulin pump in Type 1 diabetes study. News article, 16 June 2014.
http://www.fiercemedicaldevices.com/story/artificial-pancreas-beats-out-insulin-pump-type-1-diabetes-study/2014-06-16 and http://www.medicalnewstoday.com/articles/278307.php
Published research • Russell SJ, El-Khatib FH, Sinha M et al. Outpatient glycemic control with a bionic pancreas in type 1 diabetes. New England
Journal Medicine 2014;371:313-325. Trial refs: NCT01833988 and NCT01762059. http://www.nejm.org/doi/full/10.1056/NEJMoa1314474#t=articleTop
• El-Khatib FH, Russell SJ, Magyar KL et al. Autonomous and continuous adaptation of a bihormonal bionic pancreas in adults and adolescents with type 1 diabetes. Clinical Endocrinology Metabolism 2014;99(5):1701-1711. http://sites.bu.edu/bionicpancreas/files/2014/07/El-Khatib_etal_2014.pdf
• Completed research, but not yet published • A USA Phase 2 study (n=24, aged 6-11 years, ref: NCT02105324). Study title: ‘The Summer Camp Study 2: Outpatient
Automated Blood Glucose Control With a Bi-Hormonal Bionic Endocrine Pancreas in a Pediatric Population Ages 6-11 at the Clara Barton Diabetes Camps’. http://clinicaltrials.gov/show/NCT02105324
Ongoing research • A USA Phase 2 study (n=48, aged 18+, outpatient setting, ref: NCT02092220) started Apr 2014, and due to complete June
2015. Study title: ‘A Multicenter Study of Outpatient Automated Blood Glucose Control With a Bihormonal Bionic Pancreas’. http://www.clinicaltrials.gov/ct2/show/NCT02092220
• A USA study using glucagon only (n=40, aged 21+, ref: NCT02181127) started July 2014, and was due to complete Dec 2014. Study title: ‘Closed-loop glucagon administration for the automated prevention and treatment of hypoglycemia’. http://www.clinicaltrials.gov/ct2/show/NCT02181127

65
3. GlucoSitter General information
• Company website product page: http://www.dreamed-diabetes.com/ • Mor Research Applications Ltd company website product page: http://www.mor-research.com/project/artificial-pancreas-
algorithm/?tid=58 • YouTube. Bi-hormonal artificial endocrine pancreas. Video clip, 20 January 2015.
https://www.youtube.com/watch?v=CzVAHtleISk • YouTube. The GlucoSitter. Video clip, 6 July 2014. http://www.youtube.com/watch?v=ENrrICib_rk • YouTube. 24/7 first study of DreaMed's GlucoSitter artificial pancreas system. Video clip, 6 June 2014.
https://www.youtube.com/watch?v=VzPmLnzGdFA Published research
• Nimri R, Muller I, Atlas E et al. MD-Logic overnight control for 6 weeks of home use in patients with type 1 diabetes: randomized crossover trial. Diabetes Care 2014;37(11):3025-3032. http://www.ncbi.nlm.nih.gov/pubmed/25078901
• Nimri R and Phillip M. Artificial pancreas: fuzzy logic and control of glycemia. Current Opinions Endocrinology Diabetes Obesity 2014;21(4):251-256. http://www.ncbi.nlm.nih.gov/pubmed/24937038
• Nimri R, Muller I, Atlas E et al. Night glucose control with MD-Logic artificial pancreas in home setting: a single blind, randomized crossover trial – interim analysis. Pediatric Diabetes 2014;15:91-99. Trial ref: NCT01726829. http://onlinelibrary.wiley.com/doi/10.1111/pedi.12071/pdf
• Oron T, Farfel A, Muller I et al. A remote monitoring system for artificial pancreas support is safe, reliable, and user friendly. Diabetes Technology & Therapeutics 2014;16(11):699-705. http://www.ncbi.nlm.nih.gov/pubmed/25211216
Ongoing research • An international study (Germany, Israel and Slovenia) (n=223, aged 10-65, ref: NCT01238406) started Mar 2011, and due to
complete Dec 2015. Study title: ‘Multicenter, Prospective, Open Label, Cross Over, Pilot Trial to Evaluate Blood Glucose Control Overnight Under Closed-loop Insulin Delivery with MD Logic Artificial Pancreas (MDLAP) System in Patients With Type 1 Diabetes’. http://www.clinicaltrials.gov/ct2/show/NCT01238406
• An Israeli study (n=40, aged 14-25, ref: NCT01901913) started Oct 2013 and was due to complete Oct 2014. Study title: ‘MD-Logic Artificial Pancreas for Automatic Type 1 Diabetes Meals Management’. http://www.clinicaltrials.gov/ct2/show/NCT01901913
• An international study (Germany, Israel and Slovenia) (n=72, aged 10-65, ref: NCT01726829) started Nov 2012, and was due to complete Dec 2014. Study title: ‘Overnight Type 1 Diabetes Control Under MD-Logic Closed Loop System at the Patient's Home, Pilot Study’. http://clinicaltrials.gov/ct2/show/NCT01726829
• An Israeli Phase 1 study (n=25, aged 12-65, inpatient setting 3x 12-24 hour visits, ref: NCT01501032) started Oct 2013 and was due to complete Dec 2014. Study title: ‘Inpatient Evaluation of the MD-Logic Artificial Pancreas System in Patients’. http://www.clinicaltrials.gov/ct2/show/NCT01501032
• An international study (Israel and Slovenia) (n=80, aged 10-18, ref: NCT01308164) started Mar 2011, and was due to complete Dec 2014. Study title: ‘Evaluation of Automated-Insulin Pump Setting Using the MD-Logic Pump Advisor - Minors Sub Study’. http://www.clinicaltrials.gov/ct2/show/NCT01308164
• An international study (Israel and Slovenia) (n=135, aged 18-65, ref: NCT01157923) started Jul 2010 and was due to complete Dec 2014. Study title: ‘Evaluation of Automated Insulin Pump Settings Using the MD-Logic Pump Advisor-Adults Sub Study’. http://www.clinicaltrials.gov/ct2/show/NCT01157923
4. Florence General information
• Medscape Medical News. Artificial pancreas 'impressive' in 4-week, nightly home use studies. News article, 19 September 2014. http://search.medscape.com/news-search?newSearchHeader=1&queryText=artificial+pancreas
• NHS Choices. 'Bionic' pancreas could be used to treat diabetes. News article, 16 June 2014. http://www.nhs.uk/news/2014/06June/Pages/Bionic-pancreas-could-be-used-to-treat-diabetes.aspx
• Medical New Today. Breakthrough artificial pancreas study. News article, 24 April 2014. http://www.medicalnewstoday.com/releases/275830.php
Published research • Thabit H, Lubina-Soloman A, Stadler M et al. Home use of closed-loop insulin delivery for overnight glucose control in adults
with type 1 diabetes: a 4-week, multicentre, randomised crossover study. Lancet Diabetes & Endocrinology 2014;2(9):701-709. Trial ref: NCT01440140. http://www.thelancet.com/journals/landia/article/PIIS2213-8587(14)70114-7/fulltext?_eventId=login
• Hovorka R, Elleri D, Thabit H et al. Overnight closed-loop insulin delivery in young people with type 1 diabetes: a free-living, randomized clinical trial. Diabetes Care 2014;37(5):1204-1211. Trial ref. NCT01221467. http://care.diabetesjournals.org/content/37/5/1204.short

66
• Leelarathna L, Dellweg S, Mader JK et al. Day and night home closed-loop insulin delivery in adults with type 1 diabetes: three-center randomized crossover study. Diabetes Care 2014;37(7):1931-1937. http://care.diabetesjournals.org/content/37/7/1931.abstract
• Leelarathna L, Dellweg S, Mader JK et al. Assessing the effectiveness of 3 months day and night home closed-loop insulin delivery in adults with suboptimally controlled type 1 diabetes: a randomised crossover study protocol. British Medical Journal Open 2014; doi.org/10.1136/bmjopen-2014-006075. Trial refs: AP@home04 and NCT01961622. http://bmjopen.bmj.com/content/4/9/e006075.full.pdf+html
• Elleri D. Safety of closed-loop therapy during reduction or omission of meal boluses in adolescents with type 1 diabetes: a randomized clinical trial. Trial ref. NCT01629277. Diabetes, Obesity & Metabolism 2014;16:1174-1178. http://onlinelibrary.wiley.com/doi/10.1111/dom.12324/pdf
• Completed research, but not yet published • A Luxembourg/UK (Luxembourg and Cambridge) study (n=15, aged 6-12, ref: NCT02099409). Study title: ‘Open Label Single
Center Randomized Cross Over Study to Validate Current Algorithms and Evaluate Safety and Efficacy of Closed Loop Insulin Delivery (FlorenceD2 System) in Children With Type 1 Diabetes Between 6 - 12 Years of Age’. http://clinicaltrials.gov/show/NCT02099409
Ongoing research • An international study (UK [Cambridge], Austria and Germany) (n=30, aged 18+, refs: AP@home04, NCT01961622) started Apr
2014, and due to complete Dec 2015. Study title: ‘An Open-label, Multi-centre, Randomised, Two-period, Crossover Study to Assess the Efficacy, Safety and Utility of 12 Week Day and Night Automated Closed-loop Glucose Control Under Free Living Conditions Compared to Conventional Insulin Pump Therapy Combined With Continuous Glucose Monitoring in Adults With Type 1 Diabetes With Sub-optimal Glucose Control’. http://www.clinicaltrials.gov/ct2/show/NCT01961622
• UK Phase 2 study (n=24, aged 6-18, overnight use for 3 months in the home setting, refs: NCT01778348 APCam08) started Dec 2013 and due to complete May 2015. Study title: ‘An Open-label, Three-centre, Randomised, Two-period, Crossover Study to Assess the Efficacy, Safety and Utility of Overnight Closed-loop in Comparison With CGM Alone in the Home Setting in Children and Adolescents With Type 1 Diabetes’. http://www.clinicaltrials.gov/ct2/show/NCT01778348
• UK study (n=12, aged 10-18, refs: NCT01873066, DAN04) started July 2014 and due to complete Dec 2014. Title: ‘An Open-label, Single-centre, Randomised, Two-period Crossover Study to Assess the Efficacy, Safety and Utility of Closed-loop Day and Night Over 7 Days, in Comparison With CGM in the Home Setting in Children and Adolescents With T1D’. http://www.clinicaltrials.gov/ct2/show/NCT01873066
• UK Phase 2 study (n=40, aged 18+, ref. NCT01774565, ANGI202) due to run Oct 214 to Oct 2015. Study title: ‘An Open-label, Single-centre, Randomised, Parallel Design Study to Assess the Efficacy and Safety of 72-hour Automated Closed-loop Glucose Control in Comparison With Conventional Treatment in Insulin Treated Type 2 Diabetes’. https://clinicaltrials.gov/ct2/show/NCT01774565?term=hovorka&rank=4
• UK study (n=12, aged 6-18, refs: NCT02129868, APCAM09) started Apr 2014 and due to complete Oct 2014. Study title: ‘An Open-label, Single-centre, Randomised, 2-period Cross-over Study to Assess the Efficacy and Safety of a Novel Automated Overnight Closed-loop Glucose Control System on Day 1 of Continuous Glucose Monitoring Sensor Insertion in Comparison to Day 3 to 4 After Sensor Insertion in Children and Adolescents With Type 1 Diabetes’. http://www.clinicaltrials.gov/ct2/show/NCT02129868
• UK study (Cambridge) (n=12, aged 10-18, ref: UKCRN ID 15077) currently open, and due to close in Feb 2015. Study title: ‘Home testing of 24/7 closed-loop in young people with type 1 diabetes’. http://public.ukcrn.org.uk/Search/StudyDetail.aspx?StudyID=15077
• Phase 3 international study (including Cambridge) (n=30, aged 18+, ref: UKCRN ID16082). Study title: ‘DRN 830 Closing the loop in adults with type 1 diabetes’. http://public.ukcrn.org.uk/Search/StudyDetail.aspx?StudyID=16082
• UK multicentre study (including Cambridge) (n=24, aged 6-18, refs: UKCRN ID 15892, ISRCTN 24960600, MREC N° 13/EE/0120) closed Aug 2014, and reported to be in follow-up stage. Study title: ‘Multicentre closed-loop home study in young people with type1 diabetes’. http://public.ukcrn.org.uk/Search/StudyDetail.aspx?StudyID=15892
• Phase 2-3 UK study (Cambridge) (n=12, aged 12-18, ref: UKCRN ID 11447) study closed Apr 2012, reported to be in follow-up stage. Study title: ‘Closing the loop in adolescents during non-compliance behaviours’. http://public.ukcrn.org.uk/Search/StudyDetail.aspx?StudyID=11447
• Phase 1-2 UK study (Cambridge) (n=12, aged 2-6, ref: UKCRN ID 12884) study closed Nov 2013, now reported to be in follow-up stage. Study title: ‘Closing the loop in young children with type 1 diabetes’. http://public.ukcrn.org.uk/Search/StudyDetail.aspx?StudyID=12884
• Phase 2-3 UK multicentre study (including Cambridge) (n=27, aged 18+, ref: UKCRN ID 12254) study closed Sept 2013 and reported to be in follow-up stage. Study title: ‘DRN 694 (Closing the loop in adults with type 1 diabetes in the home setting’. http://public.ukcrn.org.uk/Search/StudyDetail.aspx?StudyID=12254
• UK pilot study (n=18, aged 18+, ref: UKCRN ID 13814) closed Jan 2013, and reported to be in follow-up stage. Study title: ‘DRN 761 (Short-term closed-loop glucose control in adults with Type 1 Diabetes)’. http://public.ukcrn.org.uk/Search/StudyDetail.aspx?StudyID=13814

67
5. DiAs General information
• DiaTribe. FDA approved three-month at-home trial of artificial pancreas. News article, 7 August 2014. http://diatribe.org/issues/67/new-now-next/4
• carbDM. T1 topics recap: progress towards an artificial pancreas. News article, 23 January 2015. http://carbdm.org/2015/01/23/t1-topics-recap-progress-towards-an-artificial-pancreas/
• MedPage Today. Look back at 2014: the artificial pancreas. News article, 29 December 2014. http://www.medpagetoday.com/Endocrinology/GeneralEndocrinology/49342
• Diabetes Forecast. The artificial pancreas aces new tests, News article, March 2014. http://www.diabetesforecast.org/2014/mar/the-artificial-pancreas-aces.html
• Picture of the device: http://www.diabetesmine.com/2014/02/tom-brobson-and-the-artificial-pancreas-road-show.html • MedGadget. UVA's continuous closed-loop artificial pancreas powered by Android Smartphone. News article, 15 August 2013
http://www.medgadget.com/2013/08/uvas-continuous-closed-loop-artificial-pancreas-powered-by-android-smartphone.html Published research
• Kovatchev BP, Renard E, Cobelli C et al. Safety of outpatient closed-loop control: first randomized crossover trials of a wearable artificial pancreas. Diabetes Care 2014;37(7):1789-1796. Trial refs: NCT01714505, NCT01727817 and NCT01742741. http://care.diabetesjournals.org/content/37/7/1789.long
• Del Favero S, Place J, Kropff J et al. Multicenter outpatient dinner-overnight reduction of hypoglycemia and increased time if glucose in target with a wearable artificial pancreas using modular model predictive control in adults with type 1 diabetes. Diabetes, Obesity and Metabolism. Accepted manuscript online: 20 January 2015. http://onlinelibrary.wiley.com/doi/10.1111/dom.12440/pdf
• Ly TT, Breton MD, Keith-Hynes P et al. Overnight glucose control with an automated, unified safety system in children and adolescents with type 1 diabetes at diabetes camp. Diabetes Care 2014;37(8):2310-2316. http://care.diabetesjournals.org/content/37/8/2310.full.
• Breton MD, Brown SA, Karvetski CH et al. Adding heart rate signal to a control-to-range artificial pancreas system improves the protection against hypoglycemia during exercise in type 1 diabetes. Diabetes Technology & Therapeutics 2014;16(8):506-511. Trial ref: NCT01582139. http://online.liebertpub.com/doi/abs/10.1089/dia.2013.0333
• Del Favero S, Bruttomesso D, Di Palma F et al. First use of Model Predictive Control in outpatient wearable artificial pancreas. Diabetes Care 2014;37(5):1212-1215. Trial ref: NCT1447992. http://care.diabetesjournals.org/content/37/5/1212.long
• DeSalvo DJ Keith-Hynes P, Peyser T et al. Remote glucose monitoring in camp setting reduces the risk of prolonged nocturnal hypoglycemia. Diabetes Technology & Therapeutics 2014;16(1):1-7. http://www.ncbi.nlm.nih.gov/pubmed/24168317
• Patek SD, Breton MD, Vereshchetin P et al. Model-based control of type I diabetes in risk space. 19th World Congress of the International Federation of Automatic Control. August 2014. Paper MoA07.3. https://ifac.papercept.net/conferences/conferences/IFAC14/program/IFAC14_ContentListWeb_1.html#moa07
• Del Favero S, Magni L, Kovatchev B et al. From in- to out-patient artificial pancreas studies: results and new developments. of the 19th World Congress The International Federation of Automatic Control. August 2014. IFAC-PapersOnLine 2014;19(1):255-262. http://www.ifac-papersonline.net/Detailed/65285.html https://ifac.papercept.net/conferences/conferences/IFAC14/program/IFAC14_ContentListWeb_1.html#moa07
• Chernavvsky DR, DeBoer MD, Keith-Hynes K et al. Use of an artificial pancreas among adolescents for a missed snack bolus and an underestimated meal bolus. Pediatric Diabetes. Published online first: 27 October 2014. http://onlinelibrary.wiley.com/doi/10.1111/pedi.12230/pdf
• DeBoer MD, Chernavvsky DR, Breton MD et al. Use of an artificial pancreas among adolescents to minimize extreme hyperglycemia in the setting of insulin omission for food. Endocrine Society's 96th Annual Meeting and Expo. June 2014. Oral presentation OR26-2. http://press.endocrine.org/doi/abs/10.1210/endo-meetings.2014.DGM.18.OR26-2
Completed research studies • http://clinicaltrials.gov/ct2/show/NCT01447979; http://clinicaltrials.gov/ct2/show/NCT01578980;
http://clinicaltrials.gov/ct2/show/NCT01680653; http://clinicaltrials.gov/ct2/show/NCT01973413 Ongoing research
• USA study (n=15, aged 13-18, ref: NCT01890954) was due to run Aug-Dec 2013. Study title: ‘Optimizing Closed-Loop Control of Type 1 Diabetes Mellitus in Adolescents’. http://www.clinicaltrials.gov/ct2/show/NCT01890954
• USA study (n=36, aged 21-64, ref: NCT01939834) started Dec 2013, and was due to complete Sept 2014. Study title: ‘Early Feasibility Study of Adaptive Advisory/Automated (AAA) Control of Type 1 Diabetes’. http://www.clinicaltrials.gov/ct2/show/NCT01939834
• USA study (n=12, aged 21-64, ref: NCT02008188) started Dec 2013 and was due to complete Sept 2014. Study title: ‘Early Feasibility Study of Adaptive Advisory/Automated (AAA) Control of Type 1 Diabetes’. http://www.clinicaltrials.gov/ct2/show/NCT02008188

68
• Phase 3 international study (n=24, aged 18-69, ref: NCT02137512). Study title: ‘Pilot Study 3 of Outpatient Control-to-Range: Safety and Efficacy With Day-and-Night In-Home Use (CTR3)’. http://www.clinicaltrials.gov/ct2/show/NCT02137512
• Phase 2 international study (n=36, aged 18-70, 2 months in home setting, ref: NCT02153190) started May 2014, and due to complete Jan 2015. Study title: ‘Assessment of Hybrid Use of an Artificial Pancreas in a Home Setting for Two Months in Patients With Type 1 Diabetes’. http://www.clinicaltrials.gov/ct2/show/NCT02153190 According to ClinicalTrials.gov, there are some further trials ongoing:
• USA study (n=5, aged 21-65, ref: NCT01697150) started Apr 2012 and was due to complete Dec 2013. Study title: ‘Systems Approach to Closed-Loop Control of Type 1 Diabetes at Home’. http://www.clinicaltrials.gov/ct2/show/NCT01697150
• USA study (n=48, aged 10-55, ref: NCT02147860) started May 2014, and was due to complete Dec 2014. Study title: ‘Full Day and Night Closed-Loop With DiAs Platform’. http://www.clinicaltrials.gov/ct2/show/NCT02147860
• USA study (n=30, aged 21-65, ref: NCT02131766) started May 2013 and was due to complete May 2014. Study title: ‘Unified Safety System (USS) Virginia Closed-Loop Versus Sensor Augmented Pump Therapy for Oversight Control in Type 1 Diabetes’. http://www.clinicaltrials.gov/ct2/show/NCT02131766
• USA study (n=20, aged 12-17, ref: NCT01945060) started Sept 2013 and was due to complete Sept 2014. Study title: ‘Closed Loop Control in Adolescents Using Heart Rate as Exercise Indicator’. http://www.clinicaltrials.gov/ct2/show/NCT01945060
6. Closed Loop Glucose-Sensing Delivery system General information
• ABS News. Bionic pancreas gives insulin hope to those with Type 1 diabetes. News article, 17 June 2014. http://www.abc.net.au/pm/content/2014/s4027193.htm?site=sunshine
Ongoing research • An Australian study (n=24, aged 14+, ref: NCT02040571) started Jan 2014 and due to complete Jan 2015. Study title: ‘The
Impact of the Overnight Closed Loop System on Glycemia, Subsequent Day-time Metabolic Control, Insulin Delivery, Counter Regulatory Hormones, Sleep Quality, Cognition and Satisfaction with Treatment, Compared to Open Loop System (Sensor Augmented Pump Therapy) in Both the Clinical Trial Centre and in the Home Setting in Type 1 Diabetes’. http://www.clinicaltrials.gov/ct2/show/NCT02040571
7. CLASS Published research
• Haidar A, Legault L, Messier V et al. Comparison of dual-hormone artificial pancreas, single-hormone artificial pancreas, and conventional insulin pump therapy for glycaemic control in patients with type 1 diabetes: an open-label randomised controlled crossover trial. Lancet Diabetes & Endocrinology 2015 3(1):17-26. Trial refs: CLASS-03 and NCT01754337. http://www.thelancet.com/journals/landia/article/PIIS2213-8587(14)70226-8/fulltext
• Haidar A, Farid D, St Yves A et al. Post-breakfast closed-loop glucose control is improved when accompanied with carbohydrate-matching bolus compared to weight-dependent bolus. Diabetes & Metabolism 2014;40(3):211-214. Trial ref: NCT01519102. http://www.ncbi.nlm.nih.gov/pubmed/24656963?dopt=Abstract http://www.clinicaltrials.gov/ct2/show/NCT01519102
• Haidar A, Legault L, Dallaire M et al. Glucose-responsive insulin and glucagon delivery (dual-hormone artificial pancreas) in adults with type 1 diabetes: a randomized crossover controlled trial’. Canadian Medical Association Journal 2013;185(4):297-305. Trial ref: NCT01297946. http://www.cmaj.ca/content/185/4/297.full.pdf+html
• http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/200/CN-00864200/frame.html Completed research, not yet published
• http://clinicaltrials.gov/ct2/show/NCT01905020 • http://clinicaltrials.gov/ct2/show/NCT01930097 • http://clinicaltrials.gov/ct2/show/NCT02189694
Ongoing research • Phase 2 in-patient study of 60 minutes’ exercise (n=15, aged 18+, refs: CLASS-06, NCT01930110) due to run April 2014 to April
2015. Study title: ‘An Open-label, Randomized, Cross-over Study to Compare the Efficacy of Single-hormone Closed-loop Strategy and Dual-hormone Closed-loop Strategy at Regulating Glucose Levels During Continuous Exercise and Interval Exercise in Adults With Type-1 Diabetes’. http://clinicaltrials.gov/ct2/show/NCT01930110;
• Phase 2 in-patient study of 60 minutes exercise (n=20, aged 18+, refs: CLASS07, NCT01966393) due to run April 2014 to Sept 2015. Study title: ‘An Open-label, Randomized, Three-way, Cross-over Study to Assess the Efficacy of Single-hormone Closed-loop Strategy, Dual-hormone Closed-loop Strategy and Conventional Insulin Pump Therapy in Regulating Glucose Levels During 60 Hours in Free-living Conditions in Patients With Type 1 Diabetes’. http://clinicaltrials.gov/ct2/show/NCT01966393.
• Another trial (ref: CLASS09) was due to begin in November 2014 (details not available at the time to writing).

69
8. ZMPC General information
• The UC Santa Barbara Current. A pediatric diabetes game-changer. News article, 9 February 2015. http://www.news.ucsb.edu/2015/014982/pediatric-diabetes-gamechanger
Published research • Harvey RA, Dassau E, Bevier WC et al. Clinical evaluation of an automated artificial pancreas using Zone-Model Predictive
control and health monitoring system. Diabetes Technology & Therapeutics 2014;16(6):348-357. Trial ref: NCT01472406. http://www.clinicaltrials.gov/ct2/show/NCT01472406 http://www.ncbi.nlm.nih.gov/pubmed/24471561?dopt=Abstract
Completed research, but not yet published • USA study (n=36, aged 21-65, ref: NCT01929798, 2 x 24-27.5 hours sessions in an outpatient hotel setting). Study title:
‘Randomized Crossover Feasibility Study of Artificial Pancreas Device (AP) Using Zone-MPC Controller (Zone-Model Predictive Control) and Health Monitoring System (HMS) With and Without Basal and Insulin-to-Carbohydrate Bolus Initialization’. http://clinicaltrials.gov/ct2/show/NCT01929798
Ongoing research • USA study (n=20, aged 21-65, ref: NCT01987206, 2 x 27.5 hour sessions in a clinic setting). Study title: ‘Feasibility Study of
Using a PID (Proportional-Integral-Derivative) Controller Versus an MPC (Model Predictive Control) Controller Algorithm and Health Monitoring System (HMS)’. http://clinicaltrials.gov/show/NCT01987206
• French study (n=10, aged 18-65, ref: NCT01555788) started Mar 2013 and was due to complete 2014. Study title: ‘Closed Loop Artificial Pancreas Using Intraperitoneal (IP) Insulin Via DiaPort®’. http://www.clinicaltrials.gov/ct2/show/NCT01555788
• USA study (Sansum Diabetes Research Institute, California) (n=20, aged 21-65, ref: NCT01874392) started Oct 2012 and was due to complete Dec 2013. Study title: ‘Feasibility Study Using Zone-MPC Controller (Zone-Model Predictive Control) and Health Monitoring System (HMS) and Technosphere® Insulin Inhalation System From MannKind Corp’. http://clinicaltrials.gov/ct2/show/NCT01874392
9. pAPS Published research
• Zisser H, Renard E, Kovatchev B et al. Multicenter closed-loop insulin delivery study points to challenges for keeping blood glucose in a safe range by a control algorithm in adults and adolescents with type 1 diabetes from various sites. Diabetes Technology & Therapeutics 2014;16(10):613-622. Trial ref: NCT01271023. http://www.ncbi.nlm.nih.gov/pubmed/25003311
• Chase HP, Doyle FJ, Zisser H et al. Multicenter closed-loop/hybrid meal bolus insulin delivery with type 1 diabetes. Diabetes Technology & Therapeutics 2014;16(10):623-632. Trial ref: NCT01271023. http://www.ncbi.nlm.nih.gov/pubmed/25188375?dopt=Abstract
Completed research, but not yet published • USA study (n=36, aged 21-65, ref: NCT01929798, 2 x 24-27.5 hours sessions in hotel setting). Study title: ‘Randomized
Crossover Feasibility Study of Artificial Pancreas Device (AP) Using Zone-MPC Controller (Zone-Model Predictive Control) and Health Monitoring System (HMS) With and Without Basal and Insulin-to-Carbohydrate Bolus Initialization’. http://clinicaltrials.gov/ct2/show/NCT01929798
Ongoing research • USA study (n=20, aged 21-65, ref: NCT01987206, 2 x 27.5 hour sessions in a clinic setting). Study title: ‘Feasibility Study of
Using a PID (Proportional-Integral-Derivative) Controller Versus an MPC (Model Predictive Control) Controller Algorithm and Health Monitoring System (HMS)’. http://clinicaltrials.gov/show/NCT01987206
10. Medtronic device (research versions called OCL/ePID) Completed research, but not yet published
• USA study (1 centre: Boston, Massachusetts) (n=12, aged 18-75, ref: NCT02065895). Study title: ‘Effect of Gain on Closed-Loop Insulin’. http://www.clinicaltrials.gov/ct2/show/NCT02065895
Ongoing research • Phase 2 multicentre USA (California, Colorado, Connecticut (Yale), Massachusetts, Virginia, Washington) in-clinic feasibility
study of overnight use (n=85, aged 22-75, ref: NCT01857973) started June 2013, and was due to complete Oct 2014. Study title: ‘In-Clinic Feasibility Study to Observe the Overnight Closed Loop System’. http://www.clinicaltrials.gov/ct2/show/NCT01857973
• Phase 3 UK study (n=18, aged 18-70, ref: NCT01712594) started May 2013 and due to complete April 2015. Study title: ‘Feasibility and Safety of a Closed Loop Insulin Delivery System (aka AAGC) With an Artificially Induced Calibration Error During the Overnight Period’. http://www.clinicaltrials.gov/ct2/show/NCT01712594

70
• USA study (1 centre: Stanford, California) (n=46, aged 10-35, ref: NCT01881009) started June 2013 and was due to complete Sept 2014. Study title: ‘Nocturnal Closed-Loop Control Using An ePID Algorithm On An Android Platform With Remote Monitoring In A Closely Monitored Camp Setting: The OCL Camp Study’. http://www.clinicaltrials.gov/ct2/show/NCT01881009
• Phase 1 USA study (1 centre: New York) (n=17, aged 18-40, ref: NCT01755416) started Jan 2013, and due to complete Jan 2015. Study title: ‘Phase 1 Study of Medtronic Diabetes Closed Loop Device With ePID Algorithm and Enlite Sensors on Adjuvant Therapy With Insulin and Liraglutide to Minimize Post-prandial Hyperglycemia’. http://www.clinicaltrials.gov/ct2/show/NCT01755416
• Phase 0 USA study (1 centre: Yale, Connecticut) (n=20, aged12-40, ref: NCT01787318) started Jan 2013 and due to complete Dec 2014. Study title: ‘Effect of the Insupatch on Automated Closed-loop Glucose Control in Type 1 Diabetes’. http://www.clinicaltrials.gov/ct2/show/NCT01787318
11. APC General information
• Oregon Live. Artificial pancreas for diabetics could eliminate need to manually check blood sugar. News article, 16 July 2012. http://www.oregonlive.com/health/index.ssf/2012/07/artificial_pancreas_for_diabet.html
Published research • Jacobs PG, El Youssef J, Castle J et al. Automated control of an adaptive bi-hormonal, dual-sensor artificial pancreas and
evaluation during inpatient studies. IEEE Transactions on Biomedical Engineering 2014;61(10):2569-2581. http://www.ncbi.nlm.nih.gov/pubmed/24835122
• Bakhtiania PA, El Youssef A, Duella AK et al. Factors affecting the success of glucagon delivered during an automated closed-loop system in type 1 diabetes. Journal of Diabetes and its Complications 2015;29(1):93-98. http://www.sciencedirect.com/science/article/pii/S105687271400258X
Completed research, but not yet published • Phase 2 single-centre USA (Oregon) hotel-setting study (n=25, aged 21-65, ref: NCT01871870) began in May 2013 (and was
due to end Sept 2013) has been completed. No publications were identified. Study title: ‘Sensor-controlled Insulin- and Glucagon Delivery in Subjects With Type 1 Diabetes: Testing of an Automated System in an Outpatient (Hotel) Setting.’ http://www.clinicaltrials.gov/ct2/show/NCT01871870 and http://www.clinicaltrials.gov/ct2/show/NCT01261052
12. BiAP General information
• Imperial College London. Bio inspired Silicon Pancreas. Video clip. http://wwwf.imperial.ac.uk/imedia/videos/view/440/bio-inspired-silicon-pancreas/
• Imperial College London. The bio-inspired artificial pancreas for type I diabetes. Project overview, including photo of the device system. http://www3.imperial.ac.uk/bioinspiredtechnology/research/bionicpancreas
• Twitter page: Bionic Pancreas@Imperial_BiAP: https://twitter.com/Imperial_BiAP Published research
• Reddy M, Herrero P, Sharkawy, M et al. Feasibility study of a bio-inspired artificial pancreas in adults with type 1 diabetes. Diabetes Technology & Therapeutics 2014;16(8):550-557. Trial ref: NCT01534013. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4135321/pdf/dia.2014.0009.pdf
• Pagkalos I, Herrero P, Toumazou C et al. Bio-Inspired glucose control in diabetes based on an analogue implementation of a β-cell model. IEEE Transactions on Biomedical Circuits and Systems 2014;8(2):186-95. This modelling paper compares BiAP with ePID. http://ieeexplore.ieee.org/xpls/icp.jsp?arnumber=6778812
• Older publication (2012) with details about the bio-inspired algorithm: http://www.ncbi.nlm.nih.gov/pubmed/22768892 Completed research, but not yet published
• A prospective 24-hour in-patient study (n=12 adults) and a 24-hour in-patent sub-study without meal announcement (n=8 adults).
Ongoing research • UK study (n=20, aged 18+, refs: NCT01534013, UKCRN ID 11505) started Aug 2011 and was due to complete Aug 2014. Study
title: ‘Clinical Assessment of a Closed-loop Insulin Delivery System’ http://www.clinicaltrials.gov/ct2/show/NCT01534013 • A study of the BiAP over 24-hours with glucagon, during exercise and mixed meals, assessing BiAP in 3 separate sub-studies:
(a) in a bi-hormonal configuration (n=10), (b) during and after exercise (n=20), and (c) during and after meals of mixed composition (n=20).

71
13. MAAP General information
• Illinois Institute of Technology. Artificial pancreas for use during and after exercise (NIH). Press release, 29 April 2014. http://www.iit.edu/ecdre/research/new_awards.shtml
• American Pharmaceutical review. Modeling and control of biological systems: applications in tissue engineering and artificial pancreas. Article, 1 December 2014. http://www.americanpharmaceuticalreview.com/Featured-Articles/170903-Modeling-and-Control-of-Biological-Systems-Applications-in-Tissue-Engineering-and-Artificial-Pancreas/
• Medical News Today. Illinois institute of technology works to develop artificial pancreas systems for use during and after exercise. News article, 16 Dec 2013. http://www.medicalnewstoday.com/releases/270162.php
Published research • Turksoy K, Quinn L, Littlejohn E et al. An integrated multivariable artificial pancreas control system. Journal of Diabetes
Science and Technology 2014;8:498-507. http://www.ncbi.nlm.nih.gov/pubmed/24876613 • Turksoy K, Quinn L, Littlejohn E et al. Multivariable adaptive identification and control for artificial pancreas systems. IEEE
Transactions on Biomedical Engineering 2014;61(3):883-891. http://www.ncbi.nlm.nih.gov/pubmed/24557689
14. DSC General information
• Company website: http://www.dosesafety.com Announced (6 December 2014) that a study is planned: n=20, home setting, to evaluate the ability of the Dose Safety fuzzy logic controller to reverse hypoglycemic unawareness. http://www.dosesafety.com/styled-9/index.html
Completed research, but not yet published • Kircher R, Matheson D and Mauseth R. Improved prediction accuracy and Dynamic Bayesian Network (DBN) glucoregulatory
system model and smart low glucose suspend capabilities of the Dose Safety Fuzzy Logic Dosing Controller. Diabetes Technology Conference. November 2014. Poster presentation. http://www.dosesafety.com/styled-7/index.html
• Greenbaum C, Hirsch I, Kircher R et al. Testing a fuzzy logic artificial pancreas controller. Advanced Technologies & Treatments for Diabetes Conference. February 2014. Poster presentation. http://www.dosesafety.com/styled-7/index.html
• Kircher R, Lee, J, Matheson D et al. Procedure for creating the baseline Dynamic Bayesian Network (DBN) glucoregulatory system statistical model for artificial pancreas safety monitor. Advanced Technologies & Treatments for Diabetes Conference. February 2014. Poster presentation. http://www.dosesafety.com/styled-7/index.html
15. PIDAB Completed research, but not yet published
• USA study (n=12, aged 18-75, ref: NCT02065895). Study title: ‘Effect of Gain on Closed-Loop Insulin’. http://clinicaltrials.gov/show/NCT02065895
16. CL4M General information
• Research project’s website: http://closedloop4meal.org/ Announced (9 Sept 2014) funding for new project entitled: SAFE-AP ‘New methods for an efficient and safe domiciliary artificial pancreas in type 1 diabetes’. http://www.insulaid2.org/?page_id=27&?open_id=15935
Ongoing research • Spanish study (n=20, aged 18-70, 2x meal tests 1-2 weeks apart, refs: CL4M Controls, NCT02100488) started Mar 2014 and
due to complete Mar 2015. Study title: ‘Improving Postprandial Glycaemia by a New Developed Closed-loop Control System (Closedloop4meals). An Interdisciplinary, Investigator's Initiated Project for Optimization of Glucose Control in Type1 Diabetic Subjects’. http://clinicaltrials.gov/show/NCT02100488
17. pRBA Published research
• Capel I, Rigla M, Garcıa-Saez G et al. Artificial pancreas using a personalized rule-based controller achieves overnight normoglycemia in patients with type 1 diabetes. Diabetes Technology & Therapeutics 2014;16(3):172-179. Trial ref: NCT01614496. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3934437/
Ongoing research • Spanish study (Barcelona) (n=12, aged 18-70, ref: NCT02160184) not yet recruiting according to ClinicalTrials.gov. Study title:
‘Nocturnal Insulin-Glucose in Hospital: Tight Control (NIGHT CONTROL)’. http://clinicaltrials.gov/ct2/show/NCT02160184

72
18. DIABELOOP Published research
• Quemerais MA, Doron M, Dutrech F et al. Preliminary evaluation of a new semi-closed-loop insulin therapy system over the prandial period in adult patients with type 1 diabetes: the WP6.0 Diabeloop Study. Journal of Diabetes Science and Technology 2014;8(6):1177-1184. http://www.ncbi.nlm.nih.gov/pubmed/25097057
• Borot S, Franc S, Cristante J et al. Accuracy of a new patch pump based on a microelectromechanical system (MEMS) compared to other commercially available insulin pumps: results of the first in vitro and in vivo studies. Journal of Diabetes Science and Technology 2014;8(6):1133-1141. http://www.ncbi.nlm.nih.gov/pubmed/25079676
Completed clinical trials • NCT01640210 (Technical Evaluation Of JewelPUMP In Type 1 Diabetic Patients Treated With Extern Insulin Pump)
http://clinicaltrials.gov/show/NCT01640210 • NCT01640223 (Diabeloop WP.3) http://clinicaltrials.gov/show/NCT01640223; • NCTO1754181 (Diabeloop WP6.0) http://clinicaltrials.gov/show/NCT01754181; • NCT02097316 (Feasibility Study of the JewelPUMP Version 3) http://clinicaltrials.gov/show/NCT02097316
Ongoing research • French Phase 3 study (n=15, aged 18+, ref: NCT02101229) was due to run May 2014 to Jan 2015. Study title: ‘Diabeloop
WP6.1: Validation of the Artificial Pancreas Diabeloop Algorithm in the Hospital’. https://clinicaltrials.gov/ct2/show/NCT02101229

73
REFERENCES
1 JDRF. Artificial Pancreas. http://jdrf.org/artificialpancreas/ Accessed 9 February 2015. 2 JDRF: Artificial Pancreas. YouTube video, 31 July 2013. https://www.youtube.com/watch?v=bOMtXCp_MCU 3 NHS Choices. Diabetes. http://www.nhs.uk/conditions/diabetes/pages/diabetes.aspx Accessed 9 February 2015. 4 InDependent Diabetes Trust. Newsletter Issue 81, June 2014. http://www.iddt.org/wp-
content/uploads/2014/06/IDDTNewsletter-Jun2014.pdf 5 JDRF. Behind the headlines: the causes of type 1, 6 July 2012. http://www.jdrf.org.uk/news/latest-news/behind-the-
headlines-the-causes-of-type-1?gclid=CKO_0oj6mcECFU1wvAodV6QAeQ 6 JDRF. Artificial pancreas trial reduces weekly hypo rates in type 1 diabetes patients, 23 April 2014.
http://www.diabetes.co.uk/news/2014/apr/artificial-pancreas-trial-reduces-weekly-hypo-rates-in-type-1-diabetes-patients-93706519.html
7 Newcastle University. ‘Hypo’ attacks in type 1 diabetes could be managed more effectively, 23 May 2014. http://www.ncl.ac.uk/press.office/press.release/item/hypo-attacks-in-type-1-diabetes-could-be-managed-more-effectively
8 National Institute for Health and Care Excellence. Type 1 diabetes in adults: type 1 diabetes: diagnosis and management of type 1 diabetes in adults. Clinical guideline CG15 update in development. Expected August 2015. Draft for consultation, December 2014. https://www.nice.org.uk/guidance/gid-cgwaver122/resources/type-1-diabetes-update-draft-guideline2
9 Diabetes UK. Diabetes prevalence. http://www.diabetes.co.uk/diabetes-prevalence.html Accessed 18 February 2014. 10 NHS Choices. Type 2 diabetes. http://www.nhs.uk/conditions/diabetes-type2/Pages/Introduction.aspx Accessed 9
February 2015. 11 Diabetes UK. Annual Report and Financial Statements 2013.
http://www.diabetes.org.uk/Documents/About%20Us/annual-reports/diabetes-uk-annual-report-financial-statement-2013-0614.pdf
12 National Institute for Health and Care Excellence. Clinical Knowledge Summaries. Diabetes - type 1, December 2014. http://cks.nice.org.uk/diabetes-type-1#!backgroundsub:4
13 NHS Choices. Type 1 diabetes - introduction. http://www.nhs.uk/Conditions/Diabetes-type1/Pages/Introduction.aspx Accessed 18 February 2015.
14 UK Parliamentary business. Type 1 diabetes (young people), 30 April 2014. http://www.publications.parliament.uk/pa/cm201314/cmhansrd/cm140430/halltext/140430h0001.htm
15 National Institute for Health and Care Excellence. Type 1 diabetes: integrated sensor-augmented pump therapy systems for managing blood glucose levels. Diagnostics guidance in development. Expected October 2015. Final scope document, September 2014. http://www.nice.org.uk/guidance/gid-dt22/documents/type-1-diabetes-integrated-sensoraugmented-pump-therapy-systems-for-managing-blood-glucose-levels-the-minimed-paradigm-veo-system-and-the-vibe-and-g4-platinum-cgm-system-final-scope2
16 Diabetes UK. Diabetes in the UK 2011-2012: key statistics on diabetes, December 2011. http://www.diabetes.org.uk/documents/reports/diabetes-in-the-uk-2011-12.pdf
17 Diabetes UK. 1 in 5 cases of Type 1 diabetes diagnosed in the over-40s, 6 March 2014. http://www.diabetes.org.uk/About_us/News/1-in-5-cases-of-diabetes-diagnosed-in-the-over-40s/
18 Diabetes UK. Diabetes: facts and stats. Version 3, March 2014. https://www.diabetes.org.uk/Documents/About%20Us/Statistics/Diabetes-key-stats-guidelines-April2014.pdf
19 Diabetes UK. The cost of diabetes report, January 2014. http://www.diabetes.org.uk/Documents/Diabetes%20UK%20Cost%20of%20Diabetes%20Report.pdf
20 Diabetes UK. How to test your blood glucose. http://www.diabetes.co.uk/blood-glucose/how-to-test-blood-glucose-levels.html Accessed 15 October 2014.
21 Barnard KD, Hood KK, Weissberg-Benchell J et al. Psychosocial assessment of artificial pancreas (AP): commentary and review of existing measures and their applicability in AP research. Diabetes Technology & Therapeutics. Published online first, 30 December 2014. http://www.ncbi.nlm.nih.gov/pubmed/25549042
22 Wong JC, Foster NC, Maahs DM et al. Real-time continuous glucose monitoring among participants in the T1D Exchange Clinic Registry. Diabetes Care 2014;37:2702-2709. http://www.ncbi.nlm.nih.gov/pubmed/25011947
23 Diabetes UK. Pump pros and cons http://www.diabetes.org.uk/Information-for-parents/Diabetes-care/Insulin-pumps/Pump-pros-and-cons/ Accessed 8 October 2014.
24 National Institute for Health and Care Excellence. Continuous subcutaneous insulin infusion for the treatment of diabetes mellitus. Technology appraisal TA151. London: NICE; July 2008. http://www.nice.org.uk/guidance/TA151
25 Diabetes UK. Insulin pumps. http://www.diabetes.co.uk/insulin/Insulin-pumps.html Accessed 15 October 2014. 26 JDRF, ABCD, Diabetes UK. The United Kingdom Insulin Pump Audit - Service Level Data. http://www.diabetologists-
abcd.org.uk/Audits/UK_Pump_Audit_data.pdf Accessed 18 February 2015.

74
27 Babar GS, Parton EA, Hoffman RG et al. Factors associated with adherence to continuous subcutaneous insulin
infusion in pediatric diabetes. Diabetes Technology & Therapeutics 2009;11(3):131-137. http://www.ncbi.nlm.nih.gov/pubmed/19216689
28 White HD, Goenka N, Furlong NJ et al. The UK service level audit of insulin pump therapy in adults. Diabetic Medicine. 2014;31(4):412-418. http://onlinelibrary.wiley.com/doi/10.1111/dme.12325/abstract;jsessionid=0AFB96E62537EA343545E8FEC90040EA.f02t03
29 Mobihealthnews. Prediction: 24 million will use diabetes apps by 2018, 24 March 2014. http://mobihealthnews.com/31313/prediction-24-million-will-use-diabetes-apps-by-2018/
30 Diabetes in Control. Updated bolus calculators for diabetes management, 20 March 2014. http://www.diabetesincontrol.com/articles/diabetes-news/16063-updated-bolus-calculators-for-diabetes-management
31 Cobelli C, Renard E and Kovatchev B. The artificial pancreas: a digital-age treatment for diabetes. Lancet Diabetes & Endocrinology 2014;2(9):679-681. http://www.sciencedirect.com/science/article/pii/S2213858714701263
32 Aathira R and Jain V. Advances in management of type 1 diabetes mellitus. World Journal of Diabetes 2014;5(5):689-696. http://www.wjgnet.com/1948-9358/full/v5/i5/689.htm
33 Turksoy K and Cinar A. Adaptive control of artificial pancreas systems - a review. Journal of Health Engineering 2014;5(1):1-22. http://www.ncbi.nlm.nih.gov/pubmed/24691384
34 Jacobs PG, El Youssef J, Castle J et al. Automated control of an adaptive bi-hormonal, dual-sensor artificial pancreas and evaluation during inpatient studies. IEEE Transactions on Biomedical Engineering 2014;61(10):2569-2581. http://www.ncbi.nlm.nih.gov/pubmed/24835122
35 Doyle FJ, Huyett LM, Lee JB et al. Closed-loop artificial pancreas systems: Engineering the Algorithms. Diabetes Care 2014;37:1191-1197. http://care.diabetesjournals.org/content/37/5/1191.full.pdf
36 JDRF. Artificial Pancreas Project Research. http://jdrf.org/research/treat/artificial-pancreas-project/ Accessed 10 March 2015.
37 JDRF. JDRF celebrates another artificial pancreas breakthrough, 23 January 2015. http://www.jdrf.org.uk/news/latest-news/jdrf-celebrates-another-artificial-pancreas-breakthrough
38 JDRF. JDRF congratulates Medtronic Inc - next generation AP system launches. http://jdrf.org/press-releases/jdrf-congratulates-metronic-inc-next-generation-ap-system-launches/
39 Health News From NPR. Diabetes technology inches closer to an artificial pancreas. 30 January 2015. http://www.npr.org/blogs/health/2015/01/30/382172052/diabetes-technology-inches-closer-to-an-artificial-pancreas
40 Insulin Nation. Is Medtronic’s MiniMed 640G an artificial pancreas? 22 January 2015. http://insulinnation.com/treatment2/artificial-pancreas/is-medtronics-minimed-640g-an-artificial-pancreas/
41 Peyser T, Dassau E, Breton M et al. The artificial pancreas: current status and future prospects in the management of diabetes. Annals of the New York Academy of Science 2014;1311:102-123. http://www.ncbi.nlm.nih.gov/pubmed/24725149
42 Hampton T. Fully automated artificial pancreas finally within reach. Journal of the American Medical Association 2014;311(22):2260-2261. http://jama.jamanetwork.com/article.aspx?articleID=1877064&utm_source=Silverchair+Information+Systems&utm_medium=email&utm_campaign=JAMA%3AOnlineFirst05%2F28%2F2014
43 Celafu W and Tamborlane WV. The artificial pancreas: are we there yet? Diabetes Care 2014;37:1182-1183. http://care.diabetesjournals.org/content/37/5/1182.full.pdf+html
44 Del Favero S, Magni L, Kovatchev B et al. From in- to out-patient artificial pancreas studies: results and new developments. of the 19th World Congress The International Federation of Automatic Control. August 2014. IFAC-PapersOnLine 2014;19(1):255-262. http://www.ifac-papersonline.net/Detailed/65285.html
45 American Diabetes Association: Diabetes Forecast. The artificial pancreas aces new test, March 2014. http://www.diabetesforecast.org/2014/mar/the-artificial-pancreas-aces.html
46 van Bon A, Luijf YM, Koebrugge R et al. Feasibility of a portable bihormonal closed-loop system to control glucose excursions at home under free-living conditions for 48 hours. Diabetes Technology & Therapeutics 2014;16(3):131-136. http://www.ncbi.nlm.nih.gov/pubmed/24224750
47 Nimri R, Muller I, Atlas E et al. MD-Logic overnight control for 6 weeks of home use in patients with type 1 diabetes: randomized crossover trial. Diabetes Care 2014;37(11):3025-3032. http://www.ncbi.nlm.nih.gov/pubmed/25078901
48 Russell SJ, El-Khatib FH, Sinha M et al. Outpatient glycemic control with a bionic pancreas in type 1 diabetes. New England Journal Medicine 2014;371:313-325. http://www.nejm.org/doi/full/10.1056/NEJMoa1314474#t=articleTop
49 Thabit H, Lubina-Soloman A, Stadler M et al. Home use of closed-loop insulin delivery for overnight glucose control in adults with type 1 diabetes: a 4-week, multicentre, randomised crossover study. Lancet Diabetes & Endocrinology 2014;2(9):701-709. http://www.thelancet.com/journals/landia/article/PIIS2213-8587(14)70114-7/fulltext?_eventId=login
50 Hovorka R, Elleri D, Thabit H et al. Overnight closed-loop insulin delivery in young people with type 1 diabetes: a free-living, randomized clinical trial. Diabetes Care 2014;37(5):1204-1211. http://care.diabetesjournals.org/content/37/5/1204.short

75
51 Skyler JS. T1DM in 2014: progress towards a bionic pancreas. Nature Reviews Endocrinology 2015;11:75-76.
http://www.nature.com/nrendo/journal/v11/n2/full/nrendo.2014.228.html 52 Medscape. Artificial Pancreas ‘impressive’ in 4-week, nightly home use studies, 19 September 2014.
http://search.medscape.com/news-search?newSearchHeader=1&queryText=artificial+pancreas 53 Nimri R and Phillip M. Artificial pancreas: fuzzy logic and control of glycemia. Current Opinion in Endocrinology,
Diabetes & Obesity: 2014;21(4):251-256. http://journals.lww.com/co-endocrinology/Abstract/2014/08000/Artificial_pancreas__fuzzy_logic_and_control_of.2.aspx
54 Oliver NS, Evans ML, Hovorka R et al. Comment on Doyle et al. Closed-loop artificial pancreas systems: engineering the algorithms. Diabetes Care 2014;37:1191-1197. http://care.diabetesjournals.org/content/37/10/e226.full
55 Kovatchev BP, Renard E, Cobelli C et al. Safety of outpatient closed-loop control: first randomized crossover trials of a wearable artificial pancreas. Diabetes Care 2014;37:1789-1796. http://care.diabetesjournals.org/content/37/7/1789.full.pdf+html
56 Bevier WC, Fuller SM, Fuller RP et al. Artificial pancreas (AP) clinical trial participants’ acceptance of future AP technology. Diabetes Technology & Therapeutics 2014;16(9):590-595. http://www.ncbi.nlm.nih.gov/pubmed/24811147
57 Wikipedia. Artificial pancreas. http://en.wikipedia.org/wiki/Artificial_pancreas Accessed 28 January 2015 58 Gale NK, Heath G, Cameron E et al. Using the framework method for the analysis of qualitative data in multi-disciplinary
health research. BMC Biomedical Research Methodology 2013;13:117-124. http://www.biomedcentral.com/content/pdf/1471-2288-13-117.pdf
59 Barnard KD, Pinkser JE, Oliver N et al. Future artificial pancreas technology for type 1 diabetes: what do users want? Diabetes Technology & Therapeutics. Published online first: 28 January 2015. http://www.ncbi.nlm.nih.gov/pubmed/25629627
60 Barnard KD, Wysocki T, Allen JM et al. Closing the loop overnight at home setting: psychosocial impact for adolescents with type 1 diabetes and their parents. British Medical Journal Open Diabetes Research Care 2014: doi:10.1136/bmjdrc-2014-000025. http://drc.bmj.com/content/2/1/e000025.full.pdf+html
61 Bakhtiani PA, Zhao LM, J. El Youssef J et al. A review of artificial pancreas technologies with an emphasis on bi-hormonal therapy. Diabetes, Obesity and Metabolism 2013;15:1065-1070. http://onlinelibrary.wiley.com/doi/10.1111/dom.12107/pdf
62 AP@home. http://www.apathome.eu/project/technical-approach/ Accessed 12 January 2015. 63 International Society for Pediatric and Adolescent Diabetes (ISPAD) - clinical practice consensus guidelines 2014.
https://www.ispad.org/content/ispad-clinical-practice-consensus-guidelines-2014 64 Haidar A, Legault L, Messier V et al. Comparison of dual-hormone artificial pancreas, single-hormone artificial pancreas,
and conventional insulin pump therapy for glycaemic control in patients with type 1 diabetes: an open-label randomised controlled crossover trial. Lancet Diabetes & Endocrinology 2015 3(1):17-26. http://www.thelancet.com/journals/landia/article/PIIS2213-8587(14)70226-8/fulltext
65 Harvey RA, Dassau E, Bevier WC et al. Clinical evaluation of an automated artificial pancreas using Zone-Model Predictive control and health monitoring system. Diabetes Technology & Therapeutics 2014;16(6):348-357. http://www.ncbi.nlm.nih.gov/pubmed/24471561?dopt=Abstract
66 Zisser H, Renard E, Kovatchev B et al. Multicenter closed-loop insulin delivery study points to challenges for keeping blood glucose in a safe range by a control algorithm in adults and adolescents with type 1 diabetes from various sites. Diabetes Technology & Therapeutics 2014;16(10):613-622. http://www.ncbi.nlm.nih.gov/pubmed/25003311
67 Chase HP, Doyle FJ, Zisser H et al. Multicenter closed-loop/hybrid meal bolus insulin delivery with type 1 diabetes. Diabetes Technology & Therapeutics 2014;16(10):623-632. http://www.ncbi.nlm.nih.gov/pubmed/25188375?dopt=Abstract
68 Reddy M, Herrero P, Sharkawy, M et al. Feasibility study of a bio-inspired artificial pancreas in adults with type 1 diabetes. Diabetes Technology & Therapeutics 2014;16(8):550-557. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4135321/pdf/dia.2014.0009.pdf
69 Turksoy K, Quinn L, Littlejohn E et al. An integrated multivariable artificial pancreas control system. Journal of Diabetes Science & Technology 2014;8:498-507. http://www.ncbi.nlm.nih.gov/pubmed/24876613
70 Capel I, Rigla M, Garcıa-Saez G et al. Artificial pancreas using a personalized rule-based controller achieves overnight normoglycemia in patients with type 1 diabetes. Diabetes Technology & Therapeutics 2014;16(3):172-179. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3934437/
71 Quemerais MA, Doron M, Dutrech F et al. Preliminary evaluation of a new semi-closed-loop insulin therapy system over the prandial period in adult patients with type 1 diabetes: the WP6.0 Diabeloop Study. Journal of Diabetes Science and Technology 2014;8(6):1177-1184. http://www.ncbi.nlm.nih.gov/pubmed/25097057