Embed Size (px)
Citation preview

Malaria is a disease of poverty and has a major negative impact on political, social and economic stability, and thereby hampers the development of less prosperous human societies. In 2010, ~210 million people were infected with Plasmodium and 1.2 million people, primarily children, died of this devastating disease1. Although the exact num-bers are uncertain, Plasmodium falciparum is responsible for about two-thirds of all malaria infections and the vast majority (90–95%) of the infections that cause mortality in sub-Saharan Africa. The remaining malaria infections are due to Plasmodium vivax infection in individuals living in deprived areas of Latin America and Asia2 where the disease has an enormous economic cost, although mortality is not a substantial problem.
The Plasmodium genus belongs to the Apicomplexa phylum, and the parasite has a complex life cycle3 (FIG. 1). A female Anopheles mosquito injects Plasmodium into the skin, after which sporozoites enter the bloodstream, travel to the liver and undergo asexual replication. The merozoites derived from hepatocytes rapidly invade red blood cells (RBCs), and repeated cycles of invasion, replication and release from RBCs result in exponential growth of the parasite population. More than a century ago, Camillo Golgi proposed the ‘malaria toxin hypothesis’ on the basis that Plasmodium growth is synchronized and peaks of fever typically coincide with the rupture of infected RBCs during schizogeny, which indicates that a parasite ‘toxin’ is responsible for many of the symptoms and signs of disease4. It is now clear that the mechanism underly-ing the malaria toxin hypothesis involves a deleterious activation of innate immune cells by Plasmodium-derived components (known as pathogen-associated molecular patterns (PAMPs)) and host-derived components (known as damage-associated molecular patterns (DAMPs)).
The discovery of various families of innate immune receptors has enriched our understanding of how the host senses microbial infections and initiates immune responses5–8. Considerable progress has been made in identifying the malaria parasite molecules that elicit inflammation and the cognate host receptors that respond to these signals9. These Plasmodium components might be the long sought-after ‘malaria toxin’ that causes end-organ damage and potentially death. In this Review we briefly summarize malaria-associated syndromes, and then focus on recent studies that uncover the molecular and cellular mechanisms by which Plasmodium infection activates different innate immune receptors and related signalling pathways. In the second part of this Review, we discuss the biological relevance of these innate immune receptors for host resistance to infection and for the pathogenesis of malaria. Finally, we elaborate on how this knowledge could be exploited to treat systemic inflammation, avoid organ damage and prevent the most devastating forms of this disease.
Pathogenesis and malaria-associated syndromesMalaria is a multifactorial disease and its clinical out-come depends on many aspects, such as parasite and host genetics, previous exposure to infection, age, nutritional status, and geographic and socio-economic factors3,10,11. In non-immune individuals, the first symptoms of malaria — which include fever, headache, muscle pain, chills, vomit-ing and lethargy followed by malarial paroxysms — appear between 7–15 days post infection and are associated with high levels of circulating cytokines. The activa-tion of innate immune cells and consequent systemic inflammation lead to the initial signs and symptoms of malaria, and can also influence the development of
1Division of Infectious Diseases and Immunology, University of Massachusetts Medical School, 01605–02324 Worcester, Massachusetts, USA.2Laboratório de Imunopatologia, Centro de Pesquisa René Rachou, Fundação Oswaldo Cruz, 30190–002 Belo Horizonte, Minas Gerais, Brazil.3Departamento de Bioquímica e Imunologia, Instituto de Ciências Biológicas, Universidade Federal de Minas Gerais, 31270–901 Belo Horizonte, Minas Gerais, Brazil.Correspondence to R.T.G. e-mail: [email protected] doi:10.1038/nri3742Published online 17 October 2014
ApicomplexaA large group of protozoa that includes the Plasmodium genus. They possess an apical complex structure that is involved in penetrating host cells.
Innate sensing of malaria parasitesRicardo T. Gazzinelli1–3, Parisa Kalantari1, Katherine A. Fitzgerald1 and Douglas T. Golenbock1,2
Abstract | Innate immune receptors have a key role in immune surveillance by sensing microorganisms and initiating protective immune responses. However, the innate immune system is a classic ‘double-edged sword’ that can overreact to pathogens, which can have deleterious effects and lead to clinical manifestations. Recent studies have unveiled the complexity of innate immune receptors that function as sensors of Plasmodium spp. in the vertebrate host. This Review highlights the cellular and molecular mechanisms by which Plasmodium infection is sensed by different families of innate immune receptors. We also discuss how these events mediate both host resistance to infection and the pathogenesis of malaria.
R E V I E W S
744 | NOVEMBER 2014 | VOLUME 14 www.nature.com/reviews/immunol
© 2014 Macmillan Publishers Limited. All rights reserved

the more severe forms of the disease. If left untreated, the uncomplicated symptomatic malaria caused by P. falciparum can rapidly evolve into severe illness and lethality. Children with severe malaria may develop anae-mia, jaundice, respiratory distress in relation to metabolic acidosis, and/or cerebral disease. In adults, multi-organ involvement is also frequent, and impairment of kidney
function may contribute to the development of metabolic acidosis at later stages of infection. Importantly, individu-als who are infected with malaria multiple times develop natural acquired immunity; malaria parasitism is low in hyper-immune individuals and consequently, there is no deleterious activation of innate immune cells and the infection is asymptomatic.
Nature Reviews | Immunology
a Plasmodium life cycle
Low levels of RBCs
Cerebral malaria
Placental malaria
Acute respiratory distress
b Pathogenesis of malaria
Destructionof RBCs
Anaemia (bloodstream)Adhesion and rupture of infected and altered RBCsImpaired
erythropoiesis(bone marrow)
Parasite sequestration(brain and lungs)
Augmented expression of adhesion molecules and adherence of infected RBCs
Activation of vascularendothelial cells
Sepsis (spleen)Uptake of infected oraltered RBCs resultingin macrophage activationand cytokine production
Coagulation and disruption of vascular endothelial cells
Leukocyte infiltration into the tissue parenchyma
Endothelial dysfunction Tissue inflammation
Vascular leakage andperfusion abnormalities
Sexual stage (mosquito)Parasite development in the mosquito
Female gameteMale
gamete
Oocyst
Sporozoites
Salivary gland
Midget lumenZygote
Ookinete
Hypnozoite
P. vivax
Sporozoite infectshepatocyte
Merozoite
Asexual stage (bloodstream)Parasite cycle in RBCs
Asexual stage (liver)Infection and parasite replication in hepatocytes
GametocytesRing stage
Trophozoite
Schizont
Renal impairment andmetabolic acidosis• Increased glycolysis
and lactic acid accumulation
• Hypoxia• Hyperventilation
Pro-inflammatory cytokines
Pro-inflammatory cytokines
FeverMerozoite
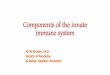
Figure 1 | Plasmodium life cycle and the pathogenesis of malaria. a | After a mosquito bite, sporozoites travel to the liver to infect hepatocytes and develop into approximately 30,000 merozoites that are released in the bloodstream. Repeated cycles of red blood cell (RBC) invasion, replication and merozoite release will result in the exponential growth of the parasite population and lead to disease. Plasmodium vivax sporozoites also differentiate into dormant hypnozoites that may cause disease relapses162. Infected RBCs will circulate containing ring-stage parasites, and a small proportion of merozoites will develop into male and female gametocytes that infect mosquitoes, completing the parasite life cycle. b | The removal of infected RBCs by splenic macrophages or the uptake of free haemozoin results in the activation of innate immune receptors and cytokine storm. The circulating cytokines will cause
paroxysms and induce the expression of adhesion molecules by endothelial cells, which mediate parasite sequestration. The sequestration of infected RBCs disrupts blood flow, promotes blood clots, injures endothelial cells and ruptures vascular walls, leading to the extravasation of vascular content and local tissue inflammation. These mechanisms contribute to acute respiratory distress, cerebral malaria or placental malaria. The sequestration of infected reticulocytes is less intense163, and these syndromes are not common in P. vivax malaria65. Haemolysis of infected and bystander (uninfected) RBCs, uptake of altered RBCs by splenic macrophages and cytokine-induced impairment of erythropoiesis cause anaemia. Free haemoglobin catalyses oxidative damage, hypoxia and lactic acidosis, promoting metabolic acidosis, which is aggravated by the altered renal function that is observed in patients with malaria.
R E V I E W S
NATURE REVIEWS | IMMUNOLOGY VOLUME 14 | NOVEMBER 2014 | 745
© 2014 Macmillan Publishers Limited. All rights reserved

SporozoitesThe Plasmodium stage that develops in the salivary glands of the mosquito and infects humans during the blood meal. When they are in the bloodstream, the sporozoites are transported to the liver where they invade hepatocytes for the first round of replication in the vertebrate host.
MerozoitesThe pathogenic Plasmodium stage that infects red blood cells (RBCs) and rapidly reproduces asexually, forming schizonts that contain multiple parasites. RBCs are destroyed by the end of this process, which releases many merozoites that will infect other host cells.
The three main pathophysiological events that occur during malaria infection are: the release of pro- inflammatory cytokines; adhesion of Plasmodium-infected RBCs to capillaries and venules; and the rup-ture and removal of parasitized and altered RBCs by splenic macro phages (FIG. 1). These three events are connected and are responsible for the main syndromes that are associated with malaria, which include systemic inflammation, anaemia, metabolic acidosis, as well as cerebral and placental malaria3,10,11 (TABLE 1).
Splenic macrophages and monocytes are main con-tributors to the cytokine storm that is observed during acute malaria episodes. As the microcirculatory beds filter out altered RBCs, innate immune cells in the spleen clear Plasmodium-infected RBCs12,13. Splenic macrophages have a central role in sensing and phago-cytosing altered RBCs, and they are exposed to a high number of parasites. As a consequence, at least in mice, these cells respond by producing large amounts of pro-inflammatory mediators14–16. However, the rupture and removal of infected RBCs by splenic macrophages is not sufficient to explain the pronounced decrease in the number of RBCs3,12,13,17. Instead, the suppressive effect of pro-inflammatory cytokines on erythropoiesis is thought to contribute to the severe anaemia that is observed in the advanced stages of malaria18,19.
As parasite growth may be synchronized, the release of pyrogenic cytokines — such as interleukin-1β (IL-1β) and tumour necrosis factor (TNF) — is cyclic20,21, and paroxysms occur every 48 hours in P. vivax and P. falciparum infections. Fever can aid host defence by delaying the growth of pathogens that have strict temperature preferences. Indeed, deliber-ate infection with P. vivax was used to induce high fever to eliminate Treponema pallidum infection in patients with neurosyphilis22. However, fever is also associated with signs of malaria illness, such as chills, rigours, low blood pressure, headache, excessive perspiration and hyperpyrexia11,17,23,24.
Another key event in malaria pathophysiology is the sequestration of parasitized RBCs into different organs including the lungs, brain, liver, kidneys and placenta25. Exposure to circulating cytokines — in particular TNF and interferon-γ (IFNγ) — or components released from Plasmodium-infected RBCs leads to enhanced expression of adhesion molecules by endothelial cells3,10,17. Also, members of the diverse family of mol-ecules related to P. falciparum erythrocyte membrane protein 1 (PfEMP1)26 are expressed on the surface of infected RBCs and bind to adhesion molecules that are distributed among different host organs and tissues, such as CD36, intercellular adhesion molecule 1 (ICAM1),
Table 1 | Malaria-associated syndromes
Syndrome Clinical features Mechanism Refs
Anaemia • Low haemoglobin levels and RBC counts
• Pallor• Lethargy often with jaundice
• Rupture of infected RBCs• Removal of infected and altered RBCs by splenic macrophages• Inhibition of erythropoiesis by cytokines
10–13,18,19
Systemic inflammation
• Alterations in body temperature• Tachycardia• Rapid breathing, often with
impaired gas exchange• Arterial hypotension• High levels of lactate in the blood• Altered mental status
• Parasite activation of splenic macrophages leads to a systemic inflammatory response (cytokine storm) that is associated with dysfunction of cardiovascular, respiratory, renal, neurological, hepatic, and/or coagulation systems
• Sepsis-like syndrome leads to acute respiratory distress syndrome• Parasitized RBC sequestration causes a disruption of the alveolar–capillary
interface, resulting in leukocyte infiltration, and oedema in the interstitium and alveoli, culminating in severe hypoxaemia
3,10,11,13, 17–19,23,
24,31
Metabolic acidosis
• Hyperventilation• Hypoxia• Headache• Altered mental status• Nausea• Vomiting• Abdominal pain• Muscle weakness
• Metabolic acidosis is due to increased glycolysis and the accumulation of lactic acid, in particular during hypoxia caused by anaemia and/or blood vessel obstruction by sequestering parasites
• Renal dysfunction and insufficient clearance of lactic acid. The lower blood pH stimulates the brainstem to increase the respiratory rate to expel more carbon dioxide, resulting in hypocapnia, which causes vasoconstriction and cerebral hypoxia, thus exacerbating cerebral disease
3,10,11,17, 23, 24,31
Cerebral malaria
• Lethargy• Unbalanced movements• Seizures• Impaired consciousness• Coma• Neurological sequelae
• Activation of endothelial cells by circulating pro-inflammatory mediators or by parasite components
• Enhanced expression of adhesion molecules in endothelial cells, parasite sequestration, obstruction of blood flow, intravascular coagulation, disruption of the endothelial barrier integrity, and local tissue inflammation
3,10,11,17, 25,28,29,31
Placental malaria
• Placental insufficiency• Fetal growth retardation• Low birth weight• Premature delivery• Stillbirth• Miscarriage• Neonatal and maternal morbidity
and mortality
Parasite sequestration and deposition of haemozoin in the intervillous space of the placenta results in the activation of placental macrophages, production of chemokines, recruitment of monocytes, intravascular macrophage differentiation, and production of pro-inflammatory cytokines that are deleterious to the fetus
10,25,30,31
RBC, red blood cell.
R E V I E W S
746 | NOVEMBER 2014 | VOLUME 14 www.nature.com/reviews/immunol
© 2014 Macmillan Publishers Limited. All rights reserved

SchizogenyThe replicative process of malaria parasites, either in hepatocytes or red blood cells, that involves nuclear division without cytoplasmic segmentation, followed by a cell budding to form the progeny called merozoites.
Pathogen-associated molecular patterns(PAMPs). Molecular structures that are normally abundant in certain pathogens and are detected by innate immune receptors known as pattern recognition receptors. PAMPs are often used as vaccine adjuvants.
Malaria-associated syndromesA collection of signs and symptoms that are characteristic of a specific manifestation of malaria, such as anaemia, respiratory distress or cerebral malaria.
ParoxysmsIn malaria, paroxysms refer to sudden attacks of disease that are characterized by high fever, chills and various other symptoms. This sudden worsening of malaria symptoms is cyclic and coincides with the synchronous rupture of Plasmodium-infected red blood cells.
Glycosylphosphatidylinositol anchors(GPI anchors). Glycolipid structures that link surface proteins to the surface membrane of eukaryotic cells. In protozoa, most surface proteins are linked via GPIs, and free GPIs are also expressed at the surface.
HaemozoinThe crystalline product resulting from the digestion of haemoglobin during different intraerythrocytic Plasmodium stages.
Toll-like receptors(TLRs). A family of pattern recognition receptors that sense pathogen-associated molecular patterns and initiate pro-inflammatory responses during microbial infection.
platelet endothelial cell adhesion molecule 1 (PECAM1), complement receptor 1, heparan sulphate and chon-droitin sulphate A. Hence, the expression of specific PfEMPs and adhesion molecules by host cells is the main determinant of parasite tissue tropism and pathogenicity27. For instance, CD36 and ICAM1 are important for parasite sequestration in the brain25,28,29, and heparan sulphate and chondroitin sulphate A are the main ligands for infected RBCs in the placenta30. Non-adherent parasitized RBCs are rapidly cleared in the spleen, whereas parasitized RBCs that are adhered to endothelial cells are protected12,13. However, adher-ence of infected RBCs triggers coagulation by activating thrombin — which catalyses fibrin deposition in blood vessels and amplifies inflammation — and thereby dis-rupts endothelial barrier integrity and favours local tissue inflammation31,32. The obstruction of capil-laries and venules, and local inflammation contrib-ute to the development of acute respiratory distress syndrome and metabolic acidosis, as well as cerebral and placental malaria. Of note, high levels of nitric oxide protect against vascular dysfunction and severe forms of malaria are associated with low availability of nitric oxide33,34.
In conclusion, systemic inflammation is a central event in the malaria-associated syndromes. Hence, defining the mechanism by which parasite components activate innate immune cells is crucial to understanding the pathophysiology of Plasmodium infection.
Sensors of Plasmodium PAMPsPAMPs are microbial structures that are detected by pattern recognition receptors (PRRs)8,35. Three P. falciparum PAMPs have been studied in detail — namely, glycosylphosphatidylinositol anchors (GPI anchors), haemozoin and immunostimulatory nucleic acid motifs (TABLE 2). The Toll-like receptors (TLRs)5 (FIG. 2)
detect PAMPs at the membrane of endosomes or at the cell surface, whereas RIG-I-like receptors (RLRs)6 and NOD-like receptors (NLRs)7 are cytosolic. Activated PRRs trigger distinct transcriptional programmes and induce multiple downstream pathways that are involved in pathogen clearance. However, excessive activation is deleterious as it can cause systemic inflammation and disease. The molecular structures of both PRRs and PAMPs are highly conserved among vertebrate hosts and certain categories of pathogens, respectively. In this section, we discuss experiments — carried out in mouse models or in vitro systems using human cells — that were instrumental in identifying the host PRRs that are activated by Plasmodium PAMPs.
GPI anchors. GPI anchors link most surface proteins to the protozoan plasma membrane and are therefore essential for parasite viability36. Importantly, protozoan GPI anchors are potent stimulators of cytokine syn-thesis by macrophages9. This activity is determined by their fine structure, which includes the number and variation of carbohydrate units; the lipid inositol por-tion (glycerol versus ceramide); and the number, length and degree of saturation of the hydrocarbon chains36.
GPI anchors from P. falciparum merozoites have either two or three fatty acyl chains and trigger the phosphory-lation of mitogen-activated protein kinases and inhibitor of nuclear factor-κB (NF-κB) family members through the activation of TLR2–TLR6 or TLR1–TLR2 hetero-dimers and, to a lesser extent, TLR4 homodimers37,38 (FIG. 2; TABLE 2). In mouse macrophages, the activation of TLRs induces the production of nitric oxide and the syn-thesis of pro-inflammatory cytokines, such as TNF and IL-1β39,40. In human umbilical vascular endothelial cells, TLR activation by GPI anchors induces the expression of ICAM1, vascular cell adhesion molecule 1 (VCAM1) and E-selectin, as well as the production of nitric oxide41.
Haemozoin. During the intraerythrocytic stage, parasites digest haemoglobin as a source of amino acids, which in turn leads to the generation of potentially toxic proto-porphyrin metabolites42,43. To survive, the parasite uses a detoxification enzyme that polymerizes haem and results in the formation of haemozoin crystals in the food vacuole of the parasite42. The parasitized RBCs are phagocytosed by macrophages, neutrophils and den-dritic cells (DCs) in various organs such as the spleen, liver and brain. The quantity of haemozoin that is depos-ited within phagocytes reflects the parasite burden, and coincides with periodic fevers and high circulating levels of IL-1β and TNF; therefore, haemozoin may be used as a biomarker of malaria severity43. Importantly, in vitro and in vivo studies have demonstrated that haemozoin activates both mouse and human monocytes and macro-phages to produce pro-inflammatory cytokines such as TNF and IL-1β, and certain chemokines44–49. By contrast, mouse but not human macrophages produce nitric oxide when stimulated with IFNγ and haemozoin50.
Although some studies indicate that β-haematin (syn-thetic haemozoin) crystals are pro-inflammatory, this matter becomes more complex when the strong adsorp-tive nature of haemozoin is taken into consideration. Natural haemozoin produced in P. falciparum cultures is normally bound to proteins, lipids and nucleic acids that may be of parasite or host origin45,51,52. The DNA binding seems to require certain proteins45,53. The identity of the crucial components of native haemozoin aggregates that trigger inflammation is still a matter of intense debate. It has been shown that synthetic haemozoin binds to, induces conformational changes in and activates TLR9 on mouse DCs and macrophages, and also on human B lym-phocytes48,54,55. In addition, purified synthetic haemozoin can induce NOD-, LRR- and pyrin domain-containing 3 (NLRP3)-dependent secretion of IL-1β by lipopoly-saccharide (LPS)-primed mouse macrophages and the human THP1 monocytic cell line46,47,56. In our view, however, haemozoin bound to P. falciparum nucleic acids traffics into phagolysosomes and the cytosol of host cells, where parasite DNA activates endosomal TLR9, inflamma-somes and other cytosolic sensors (FIG. 2). The activation of inflammasomes requires two signals: first, a priming sig-nal — which can result from TLR9 activation — leads to the transcription of the gene encoding pro-IL-1β, as well as those encoding inflammasome components; second, a signal — which can be provided by, for example, the
R E V I E W S
NATURE REVIEWS | IMMUNOLOGY VOLUME 14 | NOVEMBER 2014 | 747
© 2014 Macmillan Publishers Limited. All rights reserved

InflammasomesMolecular platforms formed by members of the NOD-like receptors family, which activate caspase 1 to cleave pro-IL-1β and pro-IL-18 and release the active form of these cytokines.
Cytosolic sensorsDifferent families of pattern recognition receptors located in the cytoplasm that are often activated by DNA and RNA, and that induce the production of type I interferons.
crystalline structure of haemozoin — that destabilizes the lysosomal membranes and causes the release of their con-tents into the cytosol46,47,53,56–58. Shio et al.46 also found that haemozoin-induced, NLRP3-dependent IL-1β production by mouse macrophages and the THP1 cell line is mediated by the tyrosine kinases SYK and LYN, as well as cathepsin B. Furthermore, this production is blocked by inhibiting phagocytosis, K+ efflux or the generation of reactive oxy-gen species46,47. Importantly, haemozoin that is carrying DNA can activate the DNA sensor absent in melanoma 2 (AIM2) to form inflammasome specks, and specks of NLRP3, AIM2 and NLRP12 inflammasomes are also found in circulating monocytes during malaria in humans16,53. Thus, haemozoin has emerged as a key component of innate immune activation by malaria parasites.
Plasmodial DNA. As is the case for other protozoa, DNA is an important activator of innate immune responses by Plasmodium parasites in both mice and humans45,59–64. Of particular interest, the P. falciparum
genome contains the highest AT content (82%) described in nature64. In silico analyses indicate that the P. falciparum genome contains approximately 300 CpG (cytosine and guanine separated by one phosphate)45 and 6,000 AT-rich64 immunostimulatory motifs. Despite the lower AT content (56%), the P. vivax genome has a similar number of AT-rich stimulatory motifs (~5,500) and has approximately 2,000 CpG motifs45,64. The higher CpG content may explain the lower pyrogenic threshold of P. vivax infection65.
When they are in the phagolysosomes, the immuno-stimulatory CpG motifs of Plasmodium DNA activate TLR9 (FIG. 2; TABLE 2). Phagocytosis of intact infected RBCs results in TLR9 engagement, presumably as a result of parasite degradation and the presence of parasite DNA in the phagolysosome. In addition, parasite DNA can be carried to the inner cellular compartments by haemo-zoin or protein aggregates45,53,63. If released in the host cell cytosol, in addition to activating AIM2 inflammasomes, DNA from schizonts also induces type I IFN release in
Table 2 | Malaria PAMPs and their role in pathogenesis
Parasite component
Properties Receptor activation Pathways Role in pathogenesis Refs
GPI anchors and GIPLs
• GPIs serve as a bridge between surface proteins and the protozoan plasma membrane
• The free forms of GPI anchors (GIPLs) are present in the protozoan surface membranes
• TLR1–TLR2 heterodimer (activated by GPI anchors containing three fatty acid chains)
• TLR4 homodimer• TLR2–TLR6 heterodimer
(activated by GPI anchors containing two fatty acid chains)
MYD88–NF-κB • Induces macrophage release of pro-inflammatory mediators (for example, TNF and nitric oxide)
• Induces the expression of adhesion molecules on endothelial cells
37–41
Haemozoin A detoxification crystal formed by haem released from haemoglobin, which is a main nutrient for the parasite during the erythrocytic stage
• TLR9 (induced by haemozoin bound to parasite DNA)
• NLRP3, AIM2 and other cytosolic sensors (owing to haemozoin-induced liberation of phagosome contents including DNA)
• MYD88–NF-κB• Assembly of
NLRP3 and AIM2 inflammasomes
• STING–IRF3
• Mediates induction of pro-inflammatory cytokine production by DCs and macrophages
• Promotes caspase 1 activation and cleavage of pro-IL-1β
• Mediates induction of type I IFN production
44–55
DNA
Immunostimulatory CpG motifs
• The P. falciparum genome contains ~300 CpG motifs
• The P. vivax genome contains ~2,500 CpG motifs
TLR9 MYD88–NF-κB Induces the release of pro-inflammatory cytokines by DCs and macrophages
45,62,63
AT-rich motif • P. falciparum DNA contains ~ 6,000 AT-rich motifs
• P. vivax DNA contains ~5,000 AT-rich motifs
Undefined STING–IRF3 Induces type I IFN production 64
Unknown motif DNA from different Plasmodium species
AIM2 Assembly of AIM2 inflammasomes
Promotes caspase 1 activation and cleavage of pro-IL-1β
53
RNA
Unknown motif Single-stranded RNA from different Plasmodium species
TLR7 MYD88–NF-κB Undefined 66,68
Unknown motif RNA from different Plasmodium species
MDA5–MAVS Type I IFN • Early activation of innate immune responses
• Induces type I IFN production in hepatocytes
66,67,69
AIM2, absent in melanoma 2; CpG, a cytosine and a guanine separated by one phosphate; DC, dendritic cell; GIPL, glycoinositol phospholipids; GPI, glycosylphos-phatidylinositol; IFN, interferon; IL, interleukin; IRF3, IFN-regulatory factor 3; MAVS, mitochondrial antiviral signalling protein; MDA5, melanoma differentiation-associated protein 5; MYD88, myeloid differentiation primary response protein 88; NF-κB, nuclear factor-κB; NLRP3, NOD-, LRR- and pyrin domain-containing 3; P. falciparum, Plasmodium falciparum; P. vivax, Plasmodium vivax; STING, stimulator of IFN genes protein; TLR, Toll-like receptor; TNF, tumour necrosis factor.
R E V I E W S
748 | NOVEMBER 2014 | VOLUME 14 www.nature.com/reviews/immunol
© 2014 Macmillan Publishers Limited. All rights reserved

Nature Reviews | Immunology
Mitochondrion
MAVS
TBK1
IRF3
Type IIFNsIL-1β
IL-18Pro IL-1βPro IL-18
IRF7
IRF3 IRF3 IRF3 IRF3
IRF7 IRF7
cGAS
IκB
?
? ?
?
MDA5
RNA
GTPATP
Haemozoin
dsDNA
Uratecrystals
dsDNA
TLR1 TLR2
GPI Haem
TLR4
Microvesicles
2′–3′ cGAMP
AT-rich DNA
Pro-inflammatorycytokines
Sporozoite
NucleusNucleus
ASC
NLRP3 NLRP12 AIM2
Pro-caspase 1 Pro-caspase 1
Active caspase 1
STING
ER
MYD88
MAL
IRAK1
IRAK1
TRAF6
TRAF3
TRAF6
MYD88
MAL
IRAK1
TRAF6
TRIF
TRAM
TBK1
TBK1
IKKε
IKKα
p65 p50
Type IIFNs
Type IIFNs
Phagolysosome
TLR7RNA
TLR9
MYD88
MYD88
IRAK4
Cytosol
Merozoite
Hepatocyte Macrophage or DC
NF-κB
Infected RBC
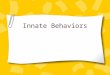
Figure 2 | Innate sensors of Plasmodium PAMPs and malaria DAMPs. RNA derived from merozoites translocates from the parasitophorous vacuole into the cytoplasm of hepatocytes (left panel) and activates melanoma differentiation-associated protein 5 (MDA5), which signals through mitochondrial antiviral signalling protein (MAVS) to induce the production of type I interferons (IFNs). Haemozoin traffics Plasmodium nucleic acids into the phagolysosomes (right panel). Toll-like receptor 7 (TLR7) and TLR9 are activated by parasite RNA and dsDNA, respectively, whereas parasite glycosylphosphatidylinositol (GPI) anchors activate TLR1–TLR2 heterodimers. Haem and host cell-derived microvesicles activate TLR4. TLRs signal through myeloid differentiation primary response protein 88 (MYD88), which eventually leads to the activation nuclear factor-κB (NF-κB) and the induction of pro-inflammatory cytokines. Haemozoin crystals destabilize phagolysosomes, which leads to the release of their contents into the host cell cytoplasm and the activation of NOD-, LRR- and pyrin domain-containing 3 (NLRP3) and NLRP12 that assemble into inflammasomes. The IFN-inducible protein absent in
melanoma 2 (AIM2), which is activated by parasite dsDNA, also forms inflammasomes. Inflammasomes recruit pro-caspase 1 either directly (NLRP12) or indirectly (NLRP3 and AIM2) via the adaptor molecule ASC. This leads to the activation of caspase 1, and the consequent cleavage and secretion of interleukin-1β (IL-1β). Cyclic GMP–AMP synthase (cGAS) generates the second messenger cyclic GMP–AMP (cGAMP), which binds and activates stimulator of IFN genes protein (STING) that in turn activates serine/threonine-protein kinase TBK1. TBK1-mediated phosphorylation of IFN-regulatory factor 3 (IRF3) leads to the expression of IFNβ. In addition, Plasmodium AT-rich motifs activate an unknown receptor that also converges on the STING–TBK1–IRF3 pathway. Question marks indicate that some components of these pathways remain to be characterized. DC, dendritic cell; ER, endoplasmic reticulum; IκB, inhibitor of NF-κB; IKK, IκB kinase; IRAK, IL-1 receptor-associated kinase; MAL, MYD88 adaptor-like protein; TRAF, TNF receptor-associated factor; TRAM, TRIF-related adaptor molecule; TRIF, TIR domain-containing adaptor protein inducing IFNβ.
R E V I E W S
NATURE REVIEWS | IMMUNOLOGY VOLUME 14 | NOVEMBER 2014 | 749
© 2014 Macmillan Publishers Limited. All rights reserved

MicrovesiclesVesicles derived from platelets, red blood cells, endothelial cells and leukocytes that serve as a communication system between host cells, and display important pro-inflammatory activity.
a TLR-independent manner in both human and mouse phagocytes64,66 (FIG. 2; TABLE 2). A potentially novel cyto-solic DNA sensor seems to detect Plasmodium DNA as TLR9, DNA-dependent activator of IFN-regulatory factors (DAI; also known as ZBP1), RNA polymer-ase III, IFNγ-inducible protein 16 (IFI16), retinoic acid- inducible gene I (RIG-I) and mitochondrial anti viral signalling protein (MAVS) could not recognize the P. falciparum AT-rich hairpin motifs64. Nevertheless, it was shown that the unidentified receptor for plasmodial AT-rich DNA signals through stimulator of IFN genes protein (STING; also known as TMEM173), serine/ threonine-protein kinase TBK1 and IFN-regulatory factor 3 (IRF3), which leads to type I IFN production. The role of cyclic GMP–AMP synthase (cGAS) in this pathway remains to be determined.
Plasmodial RNA. Recent studies indicate that RNA derived from either mouse parasites (such as Plasmodium berghei and Plasmodium yoelii) or human parasites (such as P. falciparum) activate PRRs66–68 (FIG. 2; TABLE 2). A pronounced signature of IFN-inducible genes is observed in hepatocytes soon after mice are infected with sporozoites67,69. The invasion of hepatocytes by sporozoites activates a type I IFN response via mela-noma differentiation-associated protein 5 (MDA5; also known as IFIH1) through MAVS and the transcription factors IRF3 and IRF7 (REF. 67). In addition, the erythro-cytic stage of P. yoelii induces the production of type I IFN in vivo, which is dependent on RNA polymerase III, MDA5 and MAVS, but not RIG-I66. In addition, the RNA sensor TLR7 has a role in the initial activation of innate immunity in a mouse model of malaria68. In all of these studies, the cytosolic sensors and the type I IFN response had a modest but significant role in controlling parasite growth and parasitaemia66,67,69.
Malaria DAMPsDAMPs are endogenous components released from stressed, damaged or dying cells that activate PRRs and inflammasomes, regardless of whether the cells are infected70. Uric acid, microvesicles and haem have been rec-ognized as important malaria DAMPs71–73 (FIG. 2; TABLE 3). In addition to the association with severe disease, malaria DAMPs possess intrinsic pro-inflammatory activity, which is in part mediated by the activation of PRRs71–73.
Nucleic acids and urate crystals. Circulating human DNA is found in physiological conditions and is thought to be derived from both active release from living cells and from the breakdown of dying cells74. However, DNA is found at elevated levels in both infec-tious and sterile inflammatory diseases74. In autoim-mune diseases, such as systemic lupus erythematosus and psoriasis, high levels of circulating RNA and DNA activate nucleic acid sensors and induce inflamma-tion6,75. Increased levels of circulating human DNA are also associated with symptomatic P. vivax infection in humans76. However, the relevance of this finding to the inflammatory response observed during malaria remains to be determined.
Nucleic acids are also pro-inflammatory owing to their degradation products. Uric acid — a byproduct of purine metabolism — is released in large quantities from dying cells and forms monosodium urate crystals when present at saturating concentrations in body flu-ids. Importantly, high levels of uric acid and the purine derivative hypoxanthine accumulate in infected RBCs during severe forms of human and mouse malaria, and they are released into the circulation when infected RBCs are ruptured72,77,78. Hypoxanthine is then converted into uric acid and urate crystals, and is internalized by phago-cytes, thereby contributing to NLRP3 activation and the inflammatory response during malaria58 (FIG. 2; TABLE 3).
Microvesicles. Host cell-derived microvesicles function as a communication system between host cells and they have immune-modulatory effects71. Pathogen-derived microvesicles contribute to inflammation by delivering components, such as antigens and TLR agonists, to antigen- presenting cells. Indeed, microvesicles derived from Plasmodium-infected human or mouse RBCs are internal-ized by macrophages and trigger a cytokine response via TLR4 activation79,164. However, the immunostimulatory components of these microvesicles have not been identi-fied71,79. Importantly, microvesicles derived from platelets, endothelial cells and leukocytes are also present at elevated levels during P. vivax and P. falciparum malaria, and their frequency correlates with the severity of disease80,81. Whether the circulating microvesicles are a cause or a consequence of systemic inflammation in human disease remains to be determined. Nevertheless, studies carried out both in cell lines and in mice suggest that these host-derived microvesicles contribute to the overall inflammatory response and the pathogenesis of malaria79,82.
Haem. Haemolysis and the release of haemoglobin is an important aspect of malaria pathophysiology. The oxida-tion of free haemoglobin leads to the release of the haem moiety that catalyses the formation of reactive oxygen species, which results in oxidative stress and, conse-quently, microvascular damage83. Haem also promotes inflammation by activating endothelial cells, which leads to the expression of adhesion molecules, increased vas-cular permeability and finally, tissue infiltration of leuko-cytes83. Although haem activates TLR4 in mice73, it is probably the excess of free haem that leads to inflamma-tion, primarily by inducing oxidative damage, cell death and tissue injury83. This toxic effect is prevented by haem oxygenase 1, which degrades haem and thereby attenuates the signs of severe malaria in mice84,85. However, a recent study suggests that carboxyhaemoglobin — a haem oxy-genase 1 byproduct — may exacerbate organ dysfunction in severe human disease86. Nevertheless, in both mice and humans, increased circulating levels of ferritin — which stores iron — seem to protect the host from malaria87.
Immunity to Plasmodium infectionAfter multiple malaria infections, most individuals liv-ing in hyperendemic areas develop natural acquired immunity and the main surrogate marker of protec-tion is the high level of circulating merozoite-specific
R E V I E W S
750 | NOVEMBER 2014 | VOLUME 14 www.nature.com/reviews/immunol
© 2014 Macmillan Publishers Limited. All rights reserved

antibodies3,10,88. When infected, hyper-immune indi-viduals will develop low parasitaemia and asymptomatic infection. The merozoite-specific antibodies are thought to mediate host resistance to infection by blocking para-site invasion of RBCs, or by opsonizing infected RBCs and promoting phagocytosis and parasite elimination by macrophages88,89. In addition, studies carried out in mice and humans indicate that both sporozoite-specific neutralizing antibodies and cytotoxic CD8+ T cells are important components of immune-mediated resistance to the hepatocytic stage of the Plasmodium life cycle88,89. However, it is not clear whether sporozoite-specific immune responses contribute to natural acquired immu-nity or whether they are only relevant to vaccine-induced protection88. Different studies have disclosed mechanisms by which innate immunity influences the development of acquired immunity, but the role of innate immune recep-tors in this process is still elusive89. The studies discussed above have unveiled the complexity of innate immune receptors that function as sensors of malaria parasites and we are beginning to understand how they mediate host resistance to Plasmodium infection. In this section, we discuss the known mechanisms of host defence that are triggered by the activation of PRRs.
Innate immunity. Sporozoites stimulate the expres-sion of type I IFN-inducible genes in hepatocytes dur-ing Plasmodium replication inside a parasitophorous vacuole67,69 (FIG. 3). Type I IFN-induced proteins medi-ate the recruitment of natural killer (NK) cells and NKT cells, which are important sources of IFNγ, and trigger the expression proteins that mediate control of parasite replication, such as those that are involved in the
production of nitric oxide and other toxic components that interfere with parasite schizogeny in the liver67,69. However, a single sporozoite will generate thousands of merozoites and type I IFN-mediated parasite control is inefficient67,69. The parasites that survive immunological control in hepatocytes are released into the bloodstream where they initiate the erythrocytic cycle and cause full-blown malaria in non-immune individuals.
TLRs, NF-κB-inducible pro-inflammatory cytokines and IFN-inducible genes are upregulated dur-ing the erythrocytic cycle in both human and mouse malaria15,64,90,91. IFNγ also has an important role in prim-ing innate immune cells and promoting pro-inflammatory responses, and in activating the effector functions of macrophages that mediate resistance to infection92–95,165. Of note, treatment with IL-12 during either the hepato-cytic or erythrocytic stages of malaria protects mice in a manner dependent on IFNγ, TNF and nitric oxide96,97. However, both antibody-mediated and T cell-mediated immunity are ultimately required for effective control of parasite burden and malaria89,98.
Bridging innate and acquired immunity. DCs have a cen-tral role as a bridge between innate and acquired immu-nity99. As mentioned above, parasite DNA activates DCs via TLR9 and cytosolic sensors to produce cytokines that mediate host resistance to infection14,62,66,100–104. An impor-tant mechanism of resistance to Plasmodium infection in mice is the myeloid differentiation primary response protein 88 (MYD88)-dependent production of IL-12 by DCs, and the subsequent release of IFNγ by NK cells100–104. This process results in the polarization of CD4+ T helper 1 (TH1) lymphocytes that produce IFNγ89,97, which activates
Table 3 | Malaria DAMPs
Host component
Properties Receptors Pathways Role in pathogenesis Refs
Uric acid Uric acid is released from dying cells and at high concentrations, forms monosodium urate crystals that incite inflammation
NLRP3 • Assembly of NLRP3 inflammasomes
• Caspase 1 activation and cleavage of pro-IL-1β
Release of active IL-1β 72,77,78
Microvesicles Microvesicles derived from platelets, endothelial cells, leukocytes and infected RBCs are pro-inflammatory
TLR4 MYD88–NF-κB • Induces the release of inflammatory mediators by macrophages
• Induces the expression of adhesion molecules on endothelial cells
71,79–82
Haem The oxidation of free haemoglobin released from infected RBCs produces haem
TLR4 MYD88–NF-κB Induces the release of inflammatory mediators by macrophages
73
TLR4-independent induction of oxidative stress
Catalyses the formation of reactive oxygen species
• Directly activates endothelial cells promoting the expression of adhesion molecules, increased vascular permeability and consequent tissue infiltration of leukocytes
• Causes membrane damage, cell death, tissue necrosis and inflammation
83–87
TLR4-independent induction of haem oxygenase 1
Degrades toxic haem
Haem oxygenase 1 exerts anti-inflammatory effects and promotes tissue repair
83–87
DAMP, damage-associated molecular pattern; IL, interleukin; MYD88, myeloid differentiation primary response protein 88; NF-κB, nuclear factor-κB; NLRP3, NOD-, LRR- and pyrin domain-containing 3; RBC, red blood cell; TLR4, Toll-like receptor 4.
R E V I E W S
NATURE REVIEWS | IMMUNOLOGY VOLUME 14 | NOVEMBER 2014 | 751
© 2014 Macmillan Publishers Limited. All rights reserved

effector functions, maintains the pool of effector memory T cells and promotes long-term resistance to Plasmodium infection105. The TH1 lymphocytes also direct the IgG2c isotype switch and the secretion of protective merozoite-specific antibodies98. However, the lack of a functional gene encoding MYD88 or IL-12 only partially affects the development of TH1 cell-mediated immune responses, which indicates that other PRRs and cytokines (such as IL-18) are also involved in the induction of IFNγ pro-duction by NK cells and T cells, and in promoting host resistance to mouse malaria106.
DCs are also sources of type I IFNs, but the role of these cytokines in host resistance to Plasmodium infec-tion is less well understood. On the one hand, IFNα mediates resistance to Plasmodium chabaudi infec-tion in mice by generating new DCs in a manner that is dependent on uric acid and FMS-related tyrosine kinase 3 ligand (FLT3L)107. On the other hand, type I IFNs modulate DC function and impair the devel-opment of protective T lymphocytes during mouse malaria108,109. These contrasting effects may be depend-ent on parasite strain. Importantly, in mice, virulent
Nature Reviews | Immunology
Active caspase 1
Pro-IL-1β
TNF
Blood vessel IL-1β
Fever
Bacteria
Disease
TLR9
TLR7
TLR1 TLR2 TLR4
MYD88
MYD88
MYD88
MALMYD88
MALTRIF
TRAM
Phagolysosome
Phagolysosome
TLR9
TLR7
IκBp65 p50
IκBp65 p50
InfectedRBC
Haemozoin
Merozoite
Pro-caspase 1
Type I IFNs
b Acquired immunity c
RNA
Type IIFNs
Hepatocytea Innate immunity
MDA5
MAVS
Immunologically silent (asymptomatic) Cytokine storm and local tissue inflammation (severe malaria)
Innate sensing TLR hyperresponsivenessIFNγ priming
STING
DNA and RNA sensors
Macrophage or DC
TNFreceptor
IFNγDysfunction ofendothelial wall
TH1 cell B cell
Antibodies
CD8+
T cellCD4+
T cell
MHC class I
MHC class II
IL-12
NK cellNKT cell
MYD88
MYD88
Chemokines and adhesion molecules
NF-κB
• Chemokines• Adhesion molecules• iNOS
Inflammasomeassembly
Leukocyte adhesionand infiltration
DNA
RNA
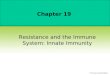
Figure 3 | Pattern recognition receptors and the pathophysiology of malaria. a | Plasmodium RNA translocates from the parasitophorous vacuole to the hepatocyte cytosol and activates melanoma differentiation-associated protein 5 (MDA5), which induces the production of type I interferons (IFNs). Macrophages and dendritic cells (DCs) phagocytose either free haemozoin or infected red blood cells (RBCs). In the phagolysosomes, nucleic acids are released from destroyed parasites or haemozoin and activate Toll-like receptors (TLRs). The release of the nuclear factor-κB (NF-κB) subunits p50 and p65 induces the expression of interleukin-12 (IL-12) that promotes production of IFNγ by CD4+ T cells, CD8+ T cells and natural killer (NK) cells. Haemozoin also destabilizes the membrane of phagolysosomes, which leads to the release of crystals and parasite DNA into host cell cytoplasm, and the activation of inflammasomes and DNA sensors. b | Type I IFN-inducible proteins promote the recruitment of leukocytes (such as NKT cells) and control parasite replication in the liver. Type I IFNs also interfere with DC function. IFNγ has multiple effects in phagocytic cells, including the induction of IL-12 production that favours the differentiation of T helper 1 (T
H1) lymphocytes. The IFNγ-inducible IgG isotypes opsonize infected RBCs
that are internalized and destroyed by activated macrophages. c | IFNγ priming makes macrophages prone to produce extreme levels of cytokines upon a secondary microbial challenge. Circulating cytokines lead to fever and promote parasite sequestration by inducing the expression of adhesion molecules on endothelial cells. The sequestration of infected RBCs results in an alteration in blood flow, rupture of the vascular wall, extravasation of vascular content and leukocyte migration into the parenchyma, leading to organ-specific syndromes such as cerebral malaria, respiratory distress and placental malaria. IκB, inhibitor of NF-κB; iNOS, inducible nitric oxide synthase; MAVS, mitochondrial antiviral signalling protein; MYD88, myeloid differentiation primary response protein 88; STING, stimulator of IFN genes protein; TRAM, TRIF-related adaptor molecule; TRIF, TIR domain-containing adaptor protein inducing IFNβ; TNF, tumour necrosis factor.
R E V I E W S
752 | NOVEMBER 2014 | VOLUME 14 www.nature.com/reviews/immunol
© 2014 Macmillan Publishers Limited. All rights reserved

AdjuvantAn agent that is mixed with an antigen to increase the immune response to that antigen following immunization.
ReticulocyteImmature red blood cells (RBCs) that correspond to 1% of total circulating RBCs in humans.
Plasmodium strains subvert the function of DCs, and thereby impair the production of IL-12 and the devel-opment of T cell-mediated immunity104,110. Consistent with this, the function of human DCs is impaired when they are exposed to infected RBCs or haemozoin111,112. Furthermore, patients with symptomatic P. falciparum or P. vivax malaria have decreased levels of circulating DCs113. Hence, modulation of DC function is an impor-tant mechanism of parasite escape from host immune responses.
Vaccine-induced immunity. After a mosquito bite, only a few sporozoites invade hepatocytes, thus a vaccine that blocks this obligatory step of the Plasmodium life cycle may induce sterile immunity. Indeed, experimental inoculation of irradiated sporozoites or intact sporo-zoites in healthy individuals receiving chloroquine is very effective as a vaccine against Plasmodium infec-tion in humans114,115. The potential of such a vaccine is currently being investigated further in clinical trials. Does the high level of protection that is observed in response to the administration of attenuated sporo-zoites reflect efficient activation of the innate immune system? The ability of sporozoite RNA to trigger a type I IFN gene signature in an MDA5-dependent and MAVS-dependent manner may help to answer this question. If this is important for the development of sporozoite- specific immunity, the use of poly I:C (a double-stranded RNA and potent inducer of type I IFN) may be a prefer-able adjuvant for a vaccine against the hepatocytic stage of malaria. In addition, RTS,S — the most advanced vaccine against malaria — uses the circumsporozoite protein, which is the dominant protein found on the sporozoite surface116. Although sterile immunity was not achieved in a Phase III trial of this vaccine, immu-nized children experienced a ~50% reduction in the incidence of clinical infections116. However, in another study with similar first year efficacy (43.6%), the level of protection dropped to 0.4% during the fourth year (with 32.1% overall across the four-year study), which indicates that the RTS,S vaccine needs considerable improvement117.
An alternative approach is an anti-malaria vaccine that targets the erythrocytic stage of the Plasmodium life cycle. For instance, vaccination with a synthetic segment of Plasmodium GPI anchor, which is a potent TLR2 activator, was shown to prevent inflammation-induced pathology and mortality in a mouse model of malaria118. Although it does not block transmission, natural acquired immunity controls the exponential parasite growth in RBCs, and prevents the excessive activation of innate immune cells, as well as clinical signs of disease. Consistent with this, vaccination with either merozoite surface protein 1 (MSP1) in combi-nation with MSP2 or the apical membrane antigen 1 induces a small, but significant reduction of clini-cal cases caused by parasite strains carrying the vac-cine alleles of the merozoite antigens119,120. The main candidate for a P. vivax-specific vaccine is the Duffy-binding protein, which is expressed by merozoites and is necessary for reticulocyte invasion121.
However, antigen variation among different parasite isolates and the induction of protective levels of parasite-specific antibodies are major obstacles to overcome88. The latter issue reflects the growing interest in innate immunity in the malaria field and the search of novel vaccine adjuvants that work through PRRs. For instance, the choice of adjuvant formulation substantially affected the efficacy of the RTS,S vaccine in a Phase II clinical trial122. In addition, the identification of func-tionally important malaria PAMPs may lead to the devel-opment of new immunological adjuvants. For example, Plasmodium-derived GPI anchors could be used as a vaccine adjuvant. Furthermore, highly pure synthetic haemozoin is an effective adjuvant in animal models54,123, and is a potential vaccine vehicle owing to its ability to bind proteins, DNA and lipids. Hence, haemozoin could be used to deliver antigen and adjuvants to lysosomes and the host cell cytoplasm to promote the activation of intracellular PRRs and antigen presentation via the exogenous and endogenous pathways53. Furthermore, both CpG motifs and AT-rich motifs that are found in the Plasmodium genome may be developed as adjuvants that induce DCs to express co-stimulatory molecules, such as IL-12 and type I IFNs45,64, which would favour the development of protective B cell-mediated and T cell-mediated immune responses.
Implications for malaria pathogenesisA hallmark of the innate immune response during both human and mouse malaria is pro-inflammatory prim-ing15,16,124–126; at very early stages of infection, Plasmodium parasites stimulate the production of IFNγ by NK cells and NKT cells15,69,127. IFNγ pre-activates the innate immune cells to respond to minute amounts of microbial products, and this enhanced ability to respond to micro-organisms during immunosurveillance protects against infectious insults. However, this pro-inflammatory prim-ing means that the innate immune system can overreact leading to a deleterious response (FIG. 3). In this section, we discuss the importance of different innate immune receptors and the cytokine storm in the pathogenesis of malaria. By reviewing immunogenetic and field studies conducted in patients with malaria, we provide evidence that these mechanisms are relevant to human disease.
MYD88 and TLRs. Bacterial superinfections in chil-dren with malaria have recently been recognized as important cofactors for severe disease65,128–130. The risk of developing severe P. falciparum malaria is estimated to increase 8.5-fold in children with bacteraemia131, and case–control and longitudinal studies indicate that children undergoing malaria episodes have an increased susceptibility to infection with non-typhoidal Salmonella species and other bacteria132,133. Consistent with this, Plasmodium-infected mice are highly suscep-tible to infection with non-typhoidal Salmonella species. It has been reported that malaria-induced immune-modulatory haem oxygenase 1 and IL-10 dampen the effector functions of neutrophils and macrophages134,135. Similarly, impaired neutrophil function has been described both in P. falciparum and P. vivax malaria126,136.
R E V I E W S
NATURE REVIEWS | IMMUNOLOGY VOLUME 14 | NOVEMBER 2014 | 753
© 2014 Macmillan Publishers Limited. All rights reserved

Plasmodium infection also lowers the threshold for bacteria-induced septic-shock. ‘Malaria loads the gun and bacteria pull the trigger’ is an expression that reflects the mechanism by which Plasmodium infec-tion enhances sensitivity to microbial infection. By pro-moting TLR hyperresponsiveness and the assembly of inflamma somes, IFNγ priming lowers the threshold for septic shock in mice by more than 100-fold15,16. Although IFNγ-deficient mice infected with P. chabaudi are highly resistant to LPS challenge, the role of TLR9 and IL-12 in pro-inflammatory priming is partial, which suggests that other PRRs and IFNγ-inducing cytokines also contribute to this response15,16.
In addition, MYD88-deficient mice infected with P. chabaudi are more resistant to systemic manifesta-tions, such as cytokinaemia, changes in body weight, temperature and liver damage14,137. Similarly, in the P. berghei model of placental malaria, mice lacking func-tional MYD88 had reduced levels of IL-6 and TNF, and unaltered fetal body weight, contrasting with the lower body weight of fetuses from infected wild-type mice138. Furthermore, inflammatory infiltrates and cytokinae-mia are reduced and pathology of experimental cerebral malaria is attenuated in MYD88-deficient mice103,139. Although the role of TLR2 and TLR4 in Plasmodium infection is controversial14,66,102,106,139,140, the data indicat-ing a role for TLR9 in experimental cerebral malaria are more consistent. Therapy with the TLR antagonist E6446, which binds both DNA and RNA within lyso-somes, is highly effective at protecting mice against experimental cerebral malaria127. Since protection against experimental cerebral malaria is only partial in TLR9-deficient mice, it is possible that the E6446 is also blocking the activation of TLR7, and other cytosolic DNA and RNA sensors53,64,68.
Hence, PRRs promote the development of cerebral malaria and sepsis-like syndrome by stimulating the production of extreme levels of the same cytokines that are involved in host resistance to Plasmodium infec-tion. For instance, the development of experimental cerebral malaria is attenuated in mice deficient for functional genes encoding IFNγ-inducible adhesion molecules, such as CXC-chemokine ligand 9 (CXCL9) and CXCL10, which are important for the recruitment of CD8+ T cells to the central nervous system141,142. Furthermore, treatment with TNF-specific monoclonal antibodies prevents the development of cerebral malaria in mice143. However, in small clinical trials, treatment with TNF-specific antibodies or the anti-inflammatory drug pentoxifylline was not shown to be effective in preventing human disease caused by P. falciparum144,145, and the role of cytokines and inflammation in cerebral malaria is still a matter of debate28,29.
Inflammasomes and IL-1β. Despite strong in vitro evidence that haemozoin triggers the formation of NLRP3 inflammasomes, different studies show that the lack of functional NLRP3, ASC, caspase 1, IL-18 or IL-1 receptor has only a minor impact (or no impact) on the control of parasitaemia and the devel-opment of mouse cerebral malaria16,46,140. Thus, the
role of inflammasomes, IL-1β and IL-18 in host resist-ance to Plasmodium infection is questionable16,46,140. Nevertheless, in both humans and mice, Plasmodium infection results in expression of an inflammasome gene signature, the formation of NLRP3, NLRP12 and AIM2 inflammasomes, and caspase 1 activation16. In addition, NLRP3, ASC and caspase 1 were shown to have an important role in mediating haemozoin-induced local inflammation, and may be involved in organ damage observed during malaria. During mouse malaria, inflammasomes and IL-1β are also key play-ers in enhanced sensitivity to bacteria-induced septic shock16. As a result, hypersensitivity to bacterial super-infection is prevented by treating mice with an IL-1R antagonist16. Furthermore, as IL-1β is highly pyrogenic, inflammasomes are probably important mediators of malaria paroxysms in humans10,11,65.
Cytosolic sensors and type I IFNs. The importance of nucleic acid sensors and type I IFN release is now being appreciated in the context of various infectious diseases, beyond their traditional roles in antiviral immunity. In a mouse model of cerebral malaria — using the ANKA strain of P. berghei — mice deficient for the type I IFN receptor, IRF3 or IRF7 exhibited less severe symptoms and delayed mortality compared with infected wild-type mice64,66,108,146,147. Type I IFNs dampen the development of TH1 cell responses that control of parasitaemia at a very early stage of infection and thereby cause a wors-ening the disease67,69,84,109. However, in another study, it was shown that therapy with IFNα protects mice from cerebral malaria, suggesting that the involvement type I IFNs in this process is more complex148.
Genetics and human disease. Various studies have associated single nucleotide polymorphisms (SNPs) in inflammatory genes with resistance or susceptibility to P. vivax or P. falciparum malaria. Although most of these studies are inconclusive because they used a small cohort of patients, protection against severe disease has been associated with SNPs in the genes encoding TNF149, IFNAR1 (a subunit of the type I IFN receptor)146,150, IL-12 (REF. 151), IFNγ152,153, IL1β154, CD40 ligand (CD40L; also known as TNFRSF5)155 and inducible nitric oxide syn-thase (also known as NOS2)156. Several SNPs identified in the genes encoding TLRs, such as TLR4 (REF. 157) and TLR9 (REF. 158), were associated with low birth weight and maternal anaemia. SNPs in TLR9 are also associated with increased levels of IFNγ in children with cerebral malaria159 and increased parasitaemia in patients with P. vivax malaria160. Furthermore, hemizygosity for a SNP in the gene encoding the TLR2 and TLR4 MYD88 adaptor-like protein (MAL; also known as TIRAP) may protect against death due to malaria161.
Concluding remarksMore than 150 years after the discovery of Plasmodium by Laveran in 1861, malaria remains a devastat-ing disease that accounts for ~1 million deaths every year. Although there are tools with which to elimi-nate the disease, the eradication of malaria will be
R E V I E W S
754 | NOVEMBER 2014 | VOLUME 14 www.nature.com/reviews/immunol
© 2014 Macmillan Publishers Limited. All rights reserved

extraordinarily expensive in the absence of an effective vaccine. Years of research on malaria pathogenesis have culminated in the consensus that the clinical manifes-tations are mostly owing to a deleterious activation of innate immune cells. It is now clear that Plasmodium infection activates innate immune cells through signal-ling pathways downstream of PRRs, but further inves-tigation is required to develop a better understanding of the biological role of specific receptors in malaria. We highlight studies indicating the crucial role of haemozoin in the activation of TLRs, inflammasomes
and other cytosolic sensors by Plasmodium DNA. We also emphasize the importance of IFNγ-mediated pro-inflammatory priming and TLR hyperresponsive-ness in promoting the cytokine storm and therefore, in each of the malaria-associated syndromes, as well as hypersensitivity to bacterial superinfection. Finally, the search for potent and better-tolerated adjuvants is a major goal for the development of an effective anti-malaria vaccine. Hence, any effort to eradicate malaria from the world requires a better understanding of the innate immune response to Plasmodium infection.
1. Murray, C. J. et al. Global malaria mortality between 1980 and 2010: a systematic analysis. Lancet 379, 413–431 (2012).
2. Gething, P. W. et al. A long neglected world malaria map: Plasmodium vivax endemicity in 2010. PLoS Negl. Trop. Dis. 6, e1814 (2012).
3. Miller, L. H., Ackerman, H. C., Su, X. Z. & Wellems, T. E. Malaria biology and disease pathogenesis: insights for new treatments. Nature Med. 19, 156–167 (2013).
4. Golgi, C. On the cycle of development of malarial parasites in tertian fever: differential diagnosis between the intracellular parasites of tertian and quartant fever. Archivio per le Scienza Mediche 13, 173–196 (Italian) (1889).
5. O’Neill, L. A., Golenbock, D. & Bowie, A. G. The history of Toll-like receptors — redefining innate immunity. Nature Rev. Immunol. 13, 453–460 (2013).
6. Barbalat, R., Ewald, S. E., Mouchess, M. L. & Barton, G. M. Nucleic acid recognition by the innate immune system. Annu. Rev. Immunol. 29, 185–214 (2011).
7. Schroder, K. & Tschopp, J. The inflammasomes. Cell 140, 821–832 (2010).
8. Takeuchi, O. & Akira, S. Pattern recognition receptors and inflammation. Cell 140, 805–820 (2010).
9. Gazzinelli, R. T. & Denkers, E. Y. Protozoan encounters with Toll-like receptor signalling pathways: implications for host parasitism. Nature Rev. Immunol. 6, 895–906 (2006).
10. Schofield, L. & Grau, G. E. Immunological processes in malaria pathogenesis. Nature Rev. Immunol. 5, 722–735 (2005).
11. Clark, I. A., Budd, A. C., Alleva, L. M. & Cowden, W. B. Human malarial disease: a consequence of inflammatory cytokine release. Malar. J. 5, 85 (2006).
12. Del Portillo, H. A. et al. The role of the spleen in malaria. Cell. Microbiol. 14, 343–355 (2012).
13. Buffet, P. A. et al. The pathogenesis of Plasmodium falciparum malaria in humans: insights from splenic physiology. Blood 117, 381–392 (2011).
14. Franklin, B. S. et al. MyD88-dependent activation of dendritic cells and CD4+ T lymphocytes mediates symptoms, but is not required for the immunological control of parasites during rodent malaria. Microbes Infect. 9, 881–890 (2007).
15. Franklin, B. S. et al. Malaria primes the innate immune response due to interferon-γ induced enhancement of Toll-like receptor expression and function. Proc. Natl Acad. Sci. USA 106, 5789–5794 (2009).This study describes the mechanism of pro-inflammatory priming during both mouse and human malaria.
16. Ataide, M. A. et al. Malaria-induced NLRP12/NLRP3-dependent caspase-1 activation mediates inflammation and hypersensitivity to bacterial superinfection. PLoS Pathog. 10, e1003885 (2014).This study describes the mechanism by which inflammasomes are induced in vivo and the relevance of this process to hypersensitivity to bacterial infection during malaria.
17. Cunnington, A. J., Riley, E. M. & Walther, M. Stuck in a rut? Reconsidering the role of parasite sequestration in severe malaria syndromes. Trends Parasitol. 29, 585–592 (2013).
18. Chang, K. H. & Stevenson, M. M. Malarial anaemia: mechanisms and implications of insufficient erythropoiesis during blood-stage malaria. Int. J. Parasitol. 34, 1501–1516 (2004).
19. Awandare, G. A. et al. Mechanisms of erythropoiesis inhibition by malarial pigment and malaria-induced proinflammatory mediators in an in vitro model. Am. J. Hematol. 86, 155–162 (2011).
20. Dinarello, C. A. Immunological and inflammatory functions of the interleukin-1 family. Annu. Rev. Immunol. 27, 519–550 (2009).
21. Tracey, K. J. & Cerami, A. Tumor necrosis factor: a pleiotropic cytokine and therapeutic target. Annu. Rev. Med. 45, 491–503 (1994).
22. Wagner-Jauregg, J. & Bruetsch, W. L. The history of the malaria treatment of general paralysis. Am. J. Psychiatry 102, 577–582 (1946).
23. Taylor, W. R., Hanson, J., Turner, G. D., White, N. J. & Dondorp, A. M. Respiratory manifestations of malaria. Chest 142, 492–505 (2012).
24. Van den Steen, P. E. et al. Pathogenesis of malaria-associated acute respiratory distress syndrome. Trends Parasitol. 29, 346–358 (2013).
25. White, N. J., Turner, G. D., Day, N. P. & Dondorp, A. M. Lethal malaria: Marchiafava and Bignami were right. J. Infect. Dis. 208, 192–198 (2013).
26. Scherf, A., Lopez-Rubio, J. J. & Riviere, L. Antigenic variation in Plasmodium falciparum. Annu. Rev. Microbiol. 62, 445–470 (2008).
27. Kraemer, S. M. & Smith, J. D. A family affair: var genes, PfEMP1 binding, and malaria disease. Curr. Opin. Microbiol. 9, 374–380 (2006).
28. Shikani, H. J. et al. Cerebral malaria: we have come a long way. Am. J. Pathol. 181, 1484–1492 (2012).
29. Idro, R., Jenkins, N. E. & Newton, C. R. Pathogenesis, clinical features, and neurological outcome of cerebral malaria. Lancet Neurol. 4, 827–840 (2005).
30. Rogerson, S. J., Hviid, L., Duffy, P. E., Leke, R. F. & Taylor, D. W. Malaria in pregnancy: pathogenesis and immunity. Lancet Infect. Dis. 7, 105–117 (2007).
31. Dondorp, A. M. et al. Direct in vivo assessment of microcirculatory dysfunction in severe falciparum malaria. J. Infect. Dis. 197, 79–84 (2008).
32. Francischetti, I. M. et al. Plasmodium falciparum-infected erythrocytes induce tissue factor expression in endothelial cells and support the assembly of multimolecular coagulation complexes. J. Thromb. Haemost. 5, 155–165 (2007).
33. Anstey, N. M. et al. Nitric oxide in Tanzanian children with malaria: inverse relationship between malaria severity and nitric oxide production/nitric oxide synthase type 2 expression. J. Exp. Med. 184, 557–567 (1996).
34. Ong, P. K. et al. Nitric oxide synthase dysfunction contributes to impaired cerebroarteriolar reactivity in experimental cerebral malaria. PLoS Pathog. 9, e1003444 (2013).
35. Janeway, C. A. Jr. Approaching the asymptote? Evolution and revolution in immunology. Cold Spring Harb. Symp. Quant. Biol. 54, 1–13 (1989).
36. Almeida, I. C. & Gazzinelli, R. T. Proinflammatory activity of glycosylphosphatidylinositol anchors derived from Trypanosoma cruzi: structural and functional analyses. J. Leukoc. Biol. 70, 467–477 (2001).
37. Krishnegowda, G. et al. Induction of proinflammatory responses in macrophages by the glycosylphosphatidylinositols of Plasmodium falciparum: cell signaling receptors, glycosylphosphatidylinositol (GPI) structural requirement, and regulation of GPI activity. J. Biol. Chem. 280, 8606–8616 (2005).This study demonstrates that malaria GPI anchors induce pro-inflammatory cytokines via TLR1–TLR2 heterodimers.
38. Durai, P., Govindaraj, R. G. & Choi, S. Structure and dynamic behavior of Toll-like receptor 2 subfamily triggered by malarial glycosylphosphatidylinositols of Plasmodium falciparum. FEBS J. 280, 6196–6212 (2013).
39. Schofield, L. & Hackett, F. Signal transduction in host cells by a glycosylphosphatidylinositol toxin of malaria parasites. J. Exp. Med. 177, 145–153 (1993).
40. Tachado, S. D. et al. Glycosylphosphatidylinositol toxin of Plasmodium induces nitric oxide synthase expression in macrophages and vascular endothelial cells by a protein tyrosine kinase-dependent and protein kinase C-dependent signaling pathway. J. Immunol. 156, 1897–1907 (1996).
41. Schofield, L. et al. Glycosylphosphatidylinositol toxin of Plasmodium up-regulates intercellular adhesion molecule-1, vascular cell adhesion molecule-1, and E-selectin expression in vascular endothelial cells and increases leukocyte and parasite cytoadherence via tyrosine kinase-dependent signal transduction. J. Immunol. 156, 1886–1896 (1996).
42. Jani, D. et al. HDP — a novel heme detoxification protein from the malaria parasite. PLoS Pathog. 4, e1000053 (2008).
43. Nguyen, P. H., Day, N., Pram, T. D., Ferguson, D. J. & White, N. J. Intraleucocytic malaria pigment and prognosis in severe malaria. Trans. R. Soc. Trop. Med. Hyg. 89, 200–204 (1995).
44. Jaramillo, M. et al. Synthetic Plasmodium-like hemozoin activates the immune response: a morphology - function study. PLoS ONE 4, e6957 (2009).
45. Parroche, P. et al. Malaria hemozoin is immunologically inert but radically enhances innate responses by presenting malaria DNA to Toll-like receptor 9. Proc. Natl Acad. Sci. USA 104, 1919–1924 (2007).This study demonstrates the importance of Plasmodium DNA in the activation of TLR9 by native haemozoin.
46. Shio, M. T. et al. Malarial hemozoin activates the NLRP3 inflammasome through Lyn and Syk kinases. PLoS Pathog. 5, e1000559 (2009).
47. Dostert, C. et al. Malarial hemozoin is a Nalp3 inflammasome activating danger signal. PLoS ONE 4, e6510 (2009).References 46 and 47 demonstrate that haemozoin crystals activate NLRP3 inflammasomes.
48. Coban, C. et al. Toll-like receptor 9 mediates innate immune activation by the malaria pigment hemozoin. J. Exp. Med. 201, 19–25 (2005).
49. Giribaldi, G. et al. Involvement of inflammatory chemokines in survival of human monocytes fed with malarial pigment. Infect. Immun. 78, 4912–4921 (2010).
50. Skorokhod, O. A., Schwarzer, E., Ceretto, M. & Arese, P. Malarial pigment haemozoin, IFN-γ, TNF-α, IL-1β and LPS do not stimulate expression of inducible nitric oxide synthase and production of nitric oxide in immuno-purified human monocytes. Malar. J. 6, 73 (2007).
51. Goldie, P., Roth, E. F. Jr., Oppenheim, J. & Vanderberg, J. P. Biochemical characterization of Plasmodium falciparum hemozoin. Am. J. Trop. Med. Hyg. 43, 584–596 (1990).
52. Barrera, V. et al. Host fibrinogen stably bound to hemozoin rapidly activates monocytes via TLR-4 and CD11b/CD18-integrin: a new paradigm of hemozoin action. Blood 117, 5674–5682 (2011).
R E V I E W S
NATURE REVIEWS | IMMUNOLOGY VOLUME 14 | NOVEMBER 2014 | 755
© 2014 Macmillan Publishers Limited. All rights reserved

53. Kalantari, P. et al. Dual engagement of the NLRP3 and AIM2 inflammasomes by Plasmodium-derived hemozoin and DNA during malaria. Cell Rep. 6, 196–210 (2014).This study describes the trafficking of haemozoin in phagocytic cells and the relevance of this process for activating endosomal and cytosolic innate immune receptors.
54. Coban, C. et al. Immunogenicity of whole-parasite vaccines against Plasmodium falciparum involves malarial hemozoin and host TLR9. Cell Host Microbe 7, 50–61 (2010).This study proposes the use of haemozoin as a vaccine adjuvant.
55. Torgbor, C. et al. A multifactorial role for P. falciparum malaria in endemic Burkitt’s lymphoma pathogenesis. PLoS Pathog. 10, e1004170 (2014).
56. Reimer, T. et al. Experimental cerebral malaria progresses independently of the Nlrp3 inflammasome. Eur. J. Immunol. 40, 764–769 (2010).
57. Rock, K. L., Latz, E., Ontiveros, F. & Kono, H. The sterile inflammatory response. Annu. Rev. Immunol. 28, 321–342 (2010).
58. Griffith, J. W., Sun, T., McIntosh, M. T. & Bucala, R. Pure hemozoin is inflammatory in vivo and activates the NALP3 inflammasome via release of uric acid. J. Immunol. 183, 5208–5220 (2009).
59. Caetano, B. C. et al. Requirement of UNC93B1 reveals a critical role for TLR7 in host resistance to primary infection with Trypanosoma cruzi. J. Immunol. 187, 1903–1911 (2011).
60. Schamber-Reis, B. L. et al. UNC93B1 and nucleic acid-sensing Toll-like receptors mediate host resistance to infection with Leishmania major. J. Biol. Chem. 288, 7127–7136 (2013).
61. Andrade, W. A. et al. Combined action of nucleic acid-sensing Toll-like receptors and TLR11/TLR12 heterodimers imparts resistance to Toxoplasma gondii in mice. Cell Host Microbe 13, 42–53 (2013).
62. Pichyangkul, S. et al. Malaria blood stage parasites activate human plasmacytoid dendritic cells and murine dendritic cells through a Toll-like receptor 9-dependent pathway. J. Immunol. 172, 4926–4933 (2004).
63. Wu, X., Gowda, N. M., Kumar, S. & Gowda, D. C. Protein–DNA complex is the exclusive malaria parasite component that activates dendritic cells and triggers innate immune responses. J. Immunol. 184, 4338–4348 (2010).
64. Sharma, S. et al. Innate immune recognition of an AT-rich stem-loop DNA motif in the Plasmodium falciparum genome. Immunity 35, 194–207 (2011).This study defines the importance of AT-rich DNA motifs from the P. falciparum genome in inducing type I IFN production via the STING pathway.
65. Anstey, N. M., Douglas, N. M., Poespoprodjo, J. R. & Price, R. N. Plasmodium vivax: clinical spectrum, risk factors and pathogenesis. Adv. Parasitol. 80, 151–201 (2012).
66. Wu, J. et al. Strain-specific innate immune signaling pathways determine malaria parasitemia dynamics and host mortality. Proc. Natl Acad. Sci. USA 111, E511–E520 (2014).This study demonstrates the importance of parasite strain on the activation of various innate immune receptors during Plasmodium infection.
67. Liehl, P. et al. Host-cell sensors for Plasmodium activate innate immunity against liver-stage infection. Nature Med. 20, 47–53 (2014).This study demonstrates the ability of sporozoite RNA to induce type I IFN in an MDA5-dependent manner.
68. Baccarella, A., Fontana, M. F., Chen, E. C. & Kim, C. C. Toll-like receptor 7 mediates early innate immune responses to malaria. Infect. Immun. 81, 4431–4442 (2013).
69. Miller, J. L., Sack, B. K., Baldwin, M., Vaughan, A. M. & Kappe, S. H. Interferon-mediated innate immune responses against malaria parasite liver stages. Cell Rep. 7, 436–447 (2014).This study describes the mechanism by which type I IFNs mediate control of Plasmodium replication in the liver.
70. Matzinger, P. Tolerance, danger, and the extended family. Annu. Rev. Immunol. 12, 991–1045 (1994).
71. Mantel, P. Y. & Marti, M. The role of extracellular vesicles in Plasmodium and other protozoan parasites. Cell. Microbiol. 16, 344–354 (2014).
72. Gallego-Delgado, J., Ty, M., Orengo, J. M., van de Hoef, D. & Rodriguez, A. A surprising role for uric acid: the inflammatory malaria response. Curr. Rheumatol Rep. 16, 401 (2014).
73. Figueiredo, R. T. et al. Characterization of heme as activator of Toll-like receptor 4. J. Biol. Chem. 282, 20221–20229 (2007).
74. Butt, A. N. & Swaminathan, R. Overview of circulating nucleic acids in plasma/serum. Ann. NY Acad. Sci. 1137, 236–242 (2008).
75. Barrat, F. J. & Coffman, R. L. Development of TLR inhibitors for the treatment of autoimmune diseases. Immunol. Rev. 223, 271–283 (2008).
76. Franklin, B. S. et al. Plasma circulating nucleic acids levels increase according to the morbidity of Plasmodium vivax malaria. PLoS ONE 6, e19842 (2011).
77. Orengo, J. M. et al. Plasmodium-induced inflammation by uric acid. PLoS Pathog. 4, e1000013 (2008).This study indicates the potential role of uric acid as a pro-inflammatory agent during malaria.
78. Lopera-Mesa, T. M. et al. Plasma uric acid levels correlate with inflammation and disease severity in Malian children with Plasmodium falciparum malaria. PLoS ONE 7, e46424 (2012).
79. Couper, K. N. et al. Parasite-derived plasma microparticles contribute significantly to malaria infection-induced inflammation through potent macrophage stimulation. PLoS Pathog. 6, e1000744 (2010).
80. Combes, V. et al. Circulating endothelial microparticles in malawian children with severe falciparum malaria complicated with coma. JAMA 291, 2542–2544 (2004).
81. Campos, F. M. et al. Augmented plasma microparticles during acute Plasmodium vivax infection. Malar. J. 9, 327 (2010).
82. Wassmer, S. C., Combes, V., Candal, F. J., Juhan-Vague, I. & Grau, G. E. Platelets potentiate brain endothelial alterations induced by Plasmodium falciparum. Infect. Immun. 74, 645–653 (2006).
83. Wagener, F. A. et al. Different faces of the heme-heme oxygenase system in inflammation. Pharmacol. Rev. 55, 551–571 (2003).
84. Pamplona, A. et al. Heme oxygenase-1 and carbon monoxide suppress the pathogenesis of experimental cerebral malaria. Nature Med. 13, 703–710 (2007).
85. Ferreira, A. et al. Sickle hemoglobin confers tolerance to Plasmodium infection. Cell 145, 398–409 (2011).References 84 and 85 demonstrate the importance of haem oxygenase 1 in protecting against the toxic effects of haem during malaria.
86. Yeo, T. W. et al. Increased carboxyhemoglobin in adult falciparum malaria is associated with disease severity and mortality. J. Infect. Dis. 208, 813–817 (2013).
87. Gozzelino, R. et al. Metabolic adaptation to tissue iron overload confers tolerance to malaria. Cell Host Microbe 12, 693–704 (2012).
88. Riley, E. M. & Stewart, V. A. Immune mechanisms in malaria: new insights in vaccine development. Nature Med. 19, 168–178 (2013).
89. Stevenson, M. M. & Riley, E. M. Innate immunity to malaria. Nature Rev. Immunol. 4, 169–180 (2004).
90. Sexton, A. C. et al. Transcriptional profiling reveals suppressed erythropoiesis, up-regulated glycolysis, and interferon-associated responses in murine malaria. J. Infect. Dis. 189, 1245–1256 (2004).
91. Ockenhouse, C. F. et al. Common and divergent immune response signaling pathways discovered in peripheral blood mononuclear cell gene expression patterns in presymptomatic and clinically apparent malaria. Infect. Immun. 74, 5561–5573 (2006).This study characterizes the expression of pro-inflammatory genes during human malaria.
92. Bastos, K. R. et al. Impaired macrophage responses may contribute to exacerbation of blood-stage Plasmodium chabaudi chabaudi malaria in interleukin-12-deficient mice. J. Interferon Cytokine Res. 22, 1191–1199 (2002).
93. Artavanis-Tsakonas, K. & Riley, E. M. Innate immune response to malaria: rapid induction of IFN-γ from human NK cells by live Plasmodium falciparum-infected erythrocytes. J. Immunol. 169, 2956–2963 (2002).
94. Walther, M. et al. Innate immune responses to human malaria: heterogeneous cytokine responses to blood-stage Plasmodium falciparum correlate with parasitological and clinical outcomes. J. Immunol. 177, 5736–5745 (2006).
95. Sponaas, A. M. et al. Migrating monocytes recruited to the spleen play an important role in control of blood stage malaria. Blood 114, 5522–5531 (2009).
96. Sedegah, M., Finkelman, F. & Hoffman, S. L. Interleukin 12 induction of interferon γ-dependent protection against malaria. Proc. Natl Acad. Sci. USA 91, 10700–10702 (1994).
97. Stevenson, M. M., Tam, M. F., Wolf, S. F. & Sher, A. IL-12-induced protection against blood-stage Plasmodium chabaudi AS requires IFN-γ and TNF-α and occurs via a nitric oxide-dependent mechanism. J. Immunol. 155, 2545–2556 (1995).
98. Su, Z. & Stevenson, M. M. IL-12 is required for antibody-mediated protective immunity against blood-stage Plasmodium chabaudi AS malaria infection in mice. J. Immunol. 168, 1348–1355 (2002).
99. Wykes, M. N. & Good, M. F. What really happens to dendritic cells during malaria? Nature Rev. Microbiol. 6, 864–870 (2008).
100. Ing, R., Segura, M., Thawani, N., Tam, M. & Stevenson, M. M. Interaction of mouse dendritic cells and malaria-infected erythrocytes: uptake, maturation, and antigen presentation. J. Immunol. 176, 441–450 (2006).This study demonstrates the activation of DCs by infected RBCs.
101. Torgler, R. et al. Sporozoite-mediated hepatocyte wounding limits Plasmodium parasite development via MyD88-mediated NF-κ B activation and inducible NO synthase expression. J. Immunol. 180, 3990–3999 (2008).
102. Gowda, N. M., Wu, X. & Gowda, D. C. TLR9 and MyD88 are crucial for the development of protective immunity to malaria. J. Immunol. 188, 5073–5085 (2012).
103. Griffith, J. W. et al. Toll-like receptor modulation of murine cerebral malaria is dependent on the genetic background of the host. J. Infect. Dis. 196, 1553–1564 (2007).
104. Wykes, M. N. et al. Plasmodium strain determines dendritic cell function essential for survival from malaria. PLoS Pathog. 3, e96 (2007).This study demonstrates that lethal strains of Plasmodium avoid activation of DCs to evade protective immune responses in mice.
105. da Silva, H. B. et al. IFN-γ-induced priming maintains long-term strain-transcending immunity against blood-stage Plasmodium chabaudi malaria. J. Immunol. 191, 5160–5169 (2013).This study defines the importance of IFNγ priming in maintaining long-term immunity to mouse malaria.
106. Cramer, J. P. et al. MyD88/IL-18-dependent pathways rather than TLRs control early parasitaemia in non-lethal Plasmodium yoelii infection. Microbes Infect. 10, 1259–1265 (2008).
107. Guermonprez, P. et al. Inflammatory Flt3l is essential to mobilize dendritic cells and for T cell responses during Plasmodium infection. Nature Med. 19, 730–738 (2013).
108. Haque, A. et al. Type I interferons suppress CD4+ T-cell-dependent parasite control during blood-stage Plasmodium infection. Eur. J. Immunol. 41, 2688–2698 (2011).
109. Haque, A. et al. Type I IFN signaling in CD8– DCs impairs Th1-dependent malaria immunity. J. Clin. Invest. 124, 2483–2496 (2014).References 108 and 109 demonstrate that signalling via the type I IFN receptor impairs DC function and the development of protective T cell responses in mouse malaria.
110. Perry, J. A., Olver, C. S., Burnett, R. C. & Avery, A. C. Cutting edge: the acquisition of TLR tolerance during malaria infection impacts T cell activation. J. Immunol. 174, 5921–5925 (2005).
111. Urban, B. C. et al. Plasmodium falciparum-infected erythrocytes modulate the maturation of dendritic cells. Nature 400, 73–77 (1999).
112. Schwarzer, E., Alessio, M., Ulliers, D. & Arese, P. Phagocytosis of the malarial pigment, hemozoin, impairs expression of major histocompatibility complex class II antigen, CD54, and CD11c in human monocytes. Infect. Immun. 66, 1601–1606 (1998).
113. Pinzon-Charry, A. et al. Apoptosis and dysfunction of blood dendritic cells in patients with falciparum and vivax malaria. J. Exp. Med. 210, 1635–1646 (2013).This study demonstrates that the frequency of circulating DCs is decreased during acute episodes of human malaria.
114. Roestenberg, M. et al. Protection against a malaria challenge by sporozoite inoculation. N. Engl. J. Med. 361, 468–477 (2009).
115. Seder, R. A. et al. Protection against malaria by intravenous immunization with a nonreplicating sporozoite vaccine. Science 341, 1359–1365 (2013).
R E V I E W S
756 | NOVEMBER 2014 | VOLUME 14 www.nature.com/reviews/immunol
© 2014 Macmillan Publishers Limited. All rights reserved

116. Agnandji, S. T. et al. First results of phase 3 trial of RTS,S/AS01 malaria vaccine in African children. N. Engl. J. Med. 365, 1863–1875 (2011).
117. Olotu, A. et al. Four-year efficacy of RTS,S/AS01E and its interaction with malaria exposure. N. Engl. J. Med. 368, 1111–1120 (2013).
118. Schofield, L., Hewitt, M. C., Evans, K., Siomos, M. A. & Seeberger, P. H. Synthetic GPI as a candidate anti-toxic vaccine in a model of malaria. Nature 418, 785–789 (2002).
119. Genton, B. et al. A recombinant blood-stage malaria vaccine reduces Plasmodium falciparum density and exerts selective pressure on parasite populations in a phase 1-2b trial in Papua New Guinea. J. Infect. Dis. 185, 820–827 (2002).
120. Thera, M. A. et al. A field trial to assess a blood-stage malaria vaccine. N. Engl. J. Med. 365, 1004–1013 (2011).
121. King, C. L. et al. Naturally acquired Duffy-binding protein-specific binding inhibitory antibodies confer protection from blood-stage Plasmodium vivax infection. Proc. Natl Acad. Sci. USA 105, 8363–8368 (2008).
122. Kester, K. E. et al. Randomized, double-blind, phase 2a trial of falciparum malaria vaccines RTS,S/AS01B and RTS,S/AS02A in malaria-naive adults: safety, efficacy, and immunologic associates of protection. J. Infect. Dis. 200, 337–346 (2009).
123. Onishi, M. et al. Hemozoin is a potent adjuvant for hemagglutinin split vaccine without pyrogenicity in ferrets. Vaccine 32, 3004–3009 (2014).
124. McCall, M. B. et al. Plasmodium falciparum infection causes proinflammatory priming of human TLR responses. J. Immunol. 179, 162–171 (2007).
125. Hartgers, F. C. et al. Enhanced Toll-like receptor responsiveness associated with mitogen-activated protein kinase activation in Plasmodium falciparum-infected children. Infect. Immun. 76, 5149–5157 (2008).
126. Leoratti, F. M. et al. Neutrophil paralysis in Plasmodium vivax malaria. PLoS Negl. Trop. Dis. 6, e1710 (2012).
127. Franklin, B. S. et al. Therapeutical targeting of nucleic acid-sensing Toll-like receptors prevents experimental cerebral malaria. Proc. Natl Acad. Sci. USA 108, 3689–3694 (2011).
128. Mabey, D. C., Brown, A. & Greenwood, B. M. Plasmodium falciparum malaria and Salmonella infections in Gambian children. J. Infect. Dis. 155, 1319–1321 (1987).
129. Berkley, J., Mwarumba, S., Bramham, K., Lowe, B. & Marsh, K. Bacteraemia complicating severe malaria in children. Trans. R. Soc. Trop. Med. Hyg. 93, 283–286 (1999).
130. Bronzan, R. N. et al. Bacteremia in Malawian children with severe malaria: prevalence, etiology, HIV coinfection, and outcome. J. Infect. Dis. 195, 895–904 (2007).
131. Were, T. et al. Bacteremia in Kenyan children presenting with malaria. J. Clin. Microbiol. 49, 671–676 (2011).This study reports an enhanced risk of developing severe malaria in patients with secondary bacterial infection.
132. Morpeth, S. C., Ramadhani, H. O. & Crump, J. A. Invasive non-Typhi Salmonella disease in Africa. Clin. Infect. Dis. 49, 606–611 (2009).
133. Scott, J. A. et al. Relation between falciparum malaria and bacteraemia in Kenyan children: a population-based, case-control study and a longitudinal study. Lancet 378, 1316–1323 (2011).This study reports an enhanced frequency of bacterial infections in children undergoing acute malaria episodes.
134. Cunnington, A. J., de Souza, J. B., Walther, M. & Riley, E. M. Malaria impairs resistance to Salmonella through heme- and heme oxygenase-dependent dysfunctional granulocyte mobilization. Nature Med. 18, 120–127 (2012).
135. Lokken, K. L. et al. Malaria parasite infection compromises control of concurrent systemic non-typhoidal Salmonella infection via IL-10-mediated alteration of myeloid cell function. PLoS Pathog. 10, e1004049 (2014).References 134 and 135 describe the mechanism of enhanced susceptibility to bacterial infection in mouse malaria.
136. Cunnington, A. J. et al. Prolonged neutrophil dysfunction after Plasmodium falciparum malaria is related to hemolysis and heme oxygenase-1 induction. J. Immunol. 189, 5336–5346 (2012).
137. Adachi, K. et al. Plasmodium berghei infection in mice induces liver injury by an IL-12- and toll-like receptor/myeloid differentiation factor 88-dependent mechanism. J. Immunol. 167, 5928–5934 (2001).
138. Barboza, R. et al. MyD88 signaling is directly involved in the development of murine placental malaria. Infect. Immun. 82, 830–838 (2014).
139. Coban, C. et al. Pathological role of Toll-like receptor signaling in cerebral malaria. Int. Immunol. 19, 67–79 (2007).References 137, 138 and 139 demonstrate the importance of MYD88 and TLRs in different aspects of the pathogenesis of mouse malaria.
140. Kordes, M., Matuschewski, K. & Hafalla, J. C. Caspase-1 activation of interleukin-1β (IL-1β) and IL-18 is dispensable for induction of experimental cerebral malaria. Infect. Immun. 79, 3633–3641 (2011).
141. Grau, G. E. et al. Monoclonal antibody against interferon-γ can prevent experimental cerebral malaria and its associated overproduction of tumor necrosis factor. Proc. Natl Acad. Sci. USA 86, 5572–5574 (1989).
142. Campanella, G. S. et al. Chemokine receptor CXCR3 and its ligands CXCL9 and CXCL10 are required for the development of murine cerebral malaria. Proc. Natl Acad. Sci. USA 105, 4814–4819 (2008).
143. Grau, G. E. et al. Tumor necrosis factor (cachectin) as an essential mediator in murine cerebral malaria. Science 237, 1210–1212 (1987).
144. Kwiatkowski, D. et al. Anti-TNF therapy inhibits fever in cerebral malaria. Q. J. Med. 86, 91–98 (1993).
145. Looareesuwan, S. et al. Pentoxifylline as an ancillary treatment for severe falciparum malaria in Thailand. Am. J. Trop. Med. Hyg. 58, 348–353 (1998).
146. Ball, E. A. et al. IFNAR1 controls progression to cerebral malaria in children and CD8+ T cell brain pathology in Plasmodium berghei-infected mice. J. Immunol. 190, 5118–5127 (2013).
147. Palomo, J. et al. Type I interferons contribute to experimental cerebral malaria development in response to sporozoite or blood-stage Plasmodium berghei ANKA. Eur. J. Immunol. 43, 2683–2695 (2013).
148. Vigario, A. M. et al. Recombinant human IFN-α inhibits cerebral malaria and reduces parasite burden in mice. J. Immunol. 178, 6416–6425 (2007).
149. McGuire, W., Hill, A. V., Allsopp, C. E., Greenwood, B. M. & Kwiatkowski, D. Variation in the TNF-α promoter region associated with susceptibility to cerebral malaria. Nature 371, 508–510 (1994).
150. Aucan, C. et al. Interferon-α receptor-1 (IFNAR1) variants are associated with protection against cerebral malaria in the Gambia. Genes Immun. 4, 275–282 (2003).
151. Phawong, C. et al. Haplotypes of IL12B promoter polymorphisms condition susceptibility to severe malaria and functional changes in cytokine levels in Thai adults. Immunogenetics 62, 345–356 (2010).
152. Koch, O. et al. IFNGR1 gene promoter polymorphisms and susceptibility to cerebral malaria. J. Infect. Dis. 185, 1684–1687 (2002).
153. Cabantous, S. et al. Evidence that interferon-γ plays a protective role during cerebral malaria. J. Infect. Dis. 192, 854–860 (2005).
154. Sortica, V. A. et al. IL1B, IL4R, IL12RB1 and TNF gene polymorphisms are associated with Plasmodium vivax malaria in Brazil. Malar. J. 11, 409 (2012).
155. Sabeti, P. et al. CD40L association with protection from severe malaria. Genes Immun. 3, 286–291 (2002).
156. Burgner, D. et al. Inducible nitric oxide synthase polymorphism and fatal cerebral malaria. Lancet 352, 1193–1194 (1998).
157. Mockenhaupt, F. P. et al. Toll-like receptor (TLR) polymorphisms in African children: common TLR-4 variants predispose to severe malaria. Proc. Natl Acad. Sci. USA 103, 177–182 (2006).
158. Mockenhaupt, F. P. et al. Common polymorphisms of toll-like receptors 4 and 9 are associated with the clinical manifestation of malaria during pregnancy. J. Infect. Dis. 194, 184–188 (2006).
159. Sam-Agudu, N. A. et al. TLR9 polymorphisms are associated with altered IFN-γ levels in children with cerebral malaria. Am. J. Trop. Med. Hyg. 82, 548–555 (2010).
160. Leoratti, F. M. et al. Variants in the toll-like receptor signaling pathway and clinical outcomes of malaria. J. Infect. Dis. 198, 772–780 (2008).
161. Khor, C. C. et al. A Mal functional variant is associated with protection against invasive pneumococcal disease, bacteremia, malaria and tuberculosis. Nature Genet. 39, 523–528 (2007).
162. Shanks, G. D. & White, N. J. The activation of vivax malaria hypnozoites by infectious diseases. Lancet Infect. Dis. 13, 900–906 (2013).
163. Lopes, S. C. et al. Paucity of Plasmodium vivax mature schizonts in peripheral blood is associated with their increased cytoadhesive potential. J. Infect. Dis. 209, 1403–1407 (2014).
164. Mantel, P. Y. et al. Malaria-infected erythrocyte-derived microvesicles mediate cellular communication within the parasite population and with the host immune system. Cell Host Microbe 13, 521–534 (2013).
165. Antonelli, L. R. et al. The CD14+CD16 + inflammatory monocyte subset displays increased mitochondrial activity and effector function during acute Plasmodium vivax malaria. PLoS Pathog. 10, e1004393 (2014).
AcknowledgementsThe authors thank M. Trombly for critically reviewing this manuscript. The authors are also grateful to all of the mem-bers and collaborators of the R.T.G., K.A.F. and D.T.G. labo-ratories for their invaluable contributions to the work that is reviewed here. R.T.G. is a recipient of a Scholar Fellowship from Coordenação de Aperfeiçoamento de Pessoal de Ensino Superior (CAPES), Brazil, and the David Rockefeller Center for Latin American Studies at Harvard School of Public Health, USA. The R.T.G. laboratory in Brazil is funded by the National Institute of Science and Technology for Vaccines, Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) and Fundação de Amparo a Pesquisa de Minas Gerai (Fapemig). D.T.G. is a recipient of a Visiting Scientists Fellowship from CNPq. K.A.F., D.T.G. and R.T.G. are funded by the US National Institutes of Health.
Competing interests statementThe authors declare no competing interests.
R E V I E W S
NATURE REVIEWS | IMMUNOLOGY VOLUME 14 | NOVEMBER 2014 | 757
© 2014 Macmillan Publishers Limited. All rights reserved

Reproduced with permission of the copyright owner. Further reproduction prohibited withoutpermission.