Embed Size (px)
Citation preview

1
INHERITANCE: BASIC CONCEPTS IN RISK ASSESMENT John O. Thomas Objectives:
- Be able to construct a pedigree from a family history of a patient and evaluate the likelihood that there is a genetic component to a disorder that is seen in the family.
- Be able to estimate the likelihood that a patient who is related to an affected individual will develop the disorder.
Suggested reading: Gelehrter et al Ch. 1-4 Problem sets that you must to be able to solve: Molecular Basis of Medicine web site I. The Chromosomal basis of inheritance.
A. The human genome contains about 3 billion base pairs of DNA, packaged into 23 chromosomes. Most somatic cells are diploid, containing 23 pairs of chromosomes. Normal individuals have 22 pairs of autosomes and two sex chromosomes (XX-female; XY-male): An individual's chromosome constitution (number of autosomes and sex chromosomes and any abnormalities in number or morphology) is an individual's karyotype.
B. There are about 30,000 genes, located at specific loci. An up-to-date web-based compilation of genes, their known functions, and associated disorders can be found at OMIM (On Line Mendelian Inheritance in Man). This is a part of the Entrez medical data bases which can be reached at http://www3.ncbi.nlm.nih.gov/Entrez/.
C. Alternative forms of a gene are referred to as alleles. An individual's combination of alleles is the genotype. 1. Homozygous: two like alleles at a particular locus. 2. Heterozygous: two unlike alleles at a particular locus. 3. Compound heterozygous: two different mutant alleles at a particular locus. 4. Hemizygous: one allele at a locus (as in X linked loci in males or deletion of one copy of an autosomal locus).
D. Mitosis: production of somatic cells. 1. A rapidly dividing cell has a cell cycle of about 24 hr. divided into phases: G1, S (DNA
synthesis), G2, M (mitosis). Cells that are not rapidly dividing may stay in early G1 (also known as G0) for extended periods. Normal cells in G0 are haploid. That is, they have two copies of each autosome and two sex chromosomes.
2. Mutations in somatic cells are passed on to daughter cells. The accumulation of multiple mutations can result in the formation of a tumor.
3. Mutations in somatic cells are not passed on to future generations E. Meiosis: production of haploid gametes from diploid germ line cells.
1. Meiosis I. a. Following DNA replication, homologous chromosomes pair, and undergo recombination.
There are, on the average, about 1-3-recombination events per chromosome arm per meiosis. i. Genes that are far apart or on different chromosomes segregate randomly to gametes.
These lectures will focus on genes that segregate randomly. ii. Genes that are close together are likely to stay together during gametogenesis. Such genes
are said to be genetically linked. Closely linked genes will be discussed later in the course. b. Paired chromosomes disjoin and the sister chromatids, which remain together, move to
opposite poles of the cell. The chromosome number is reduced by half. This is the most error-prone step of cell division, and may give rise to chromosome disorders. These will be
2
discussed in the cytogenetics lectures. 2. Meiosis II.
a. Follows meiosis I without DNA synthesis. b. Sister chromatids separate as in mitosis. Errors may lead to chromosome disorders (discussed in the cytogenetics lectures)
II. Types of genetic disorders.
A. Effect of mutations on phenotype. DNA variations can: 1. Have no effect - the usual case since most of the DNA is non-coding and the genetic code is
redundant. 2. Lead to "healthy" but different people. 3. Lead to a predisposition to disease. 4. Produce phenotypes recognizable as diseases. 5. Produce defects that are incompatible with life. B. Single gene defects (nuclear genes). 1. Defects in one gene have a major role in causing the phenotype. 2. Other loci and environmental factors usually influence the phenotype. 3. Pattern of inheritance is Autosomal dominant, autosomal recessive or X-linked. C. Mitochondrial gene defects - maternally inherited. D. Chromosome disorders. 1. Abnormal number of chromosomes. 2. A microscopically visible chromosome or segment is aberrant. 3. Common:7/1000 live born infants and half of spontaneous first trimester abortions. 4. Often no family history. E. Polygenic and multifactorial disorders.
1. Polygenic refers to diseases caused by contributions from more than one gene and multifactorial implies both genetic and nongenetic causes.
2. Many congenital malformations. 3. Genetic predisposition to disease. 4. Environmental factors may play a role. 5. Recur in families but without the characteristic pedigree patterns of single gene traits. III. Hallmarks of a genetic disease.
A. Single gene defects show characteristic pedigrees. B. Disease occurs in related individuals and not in unrelated individuals in a pedigree, and the
incidence is related to the degree of relationship. This is expressed as the coefficient of relationship, r. 1. First degree relatives share 1/2 of their genome (r=1/2). This is the relationship between parent
and child or the relationship between siblings. 2. Second degree relatives share 1/4 of their genome (r=1/4). This is the relationship between
aunts/uncles and their nieces/nephews. 3. Third degree relatives share 1/8 of their genome (r=1/8). This is the relationship between first
cousins.

C. Concordance in studies of twins.
1. Mendelian: 100% in MZ twins and 50% in DZ twins. 2. Multifactorial: <100% in MZ twins but > than DZ twins.
3. Example: Cleft lip +/- Cleft Palate is a multifactorial disorder with a genetic component. It has an incidence of about 1/1000 in the general population, but the risk for a relative of an affected person is increased:
- Monozygotic twin: 400/1000; - First degree relative: 40/1000; - Dizygotic twin: 40/1000 - Second degree relative: 7/1000 IV. Inheritance of single gene defects.
A. Dominant and recessive as used in medical genetics. 1. A trait is considered to be dominant when there is a clinical phenotype in the heterozygote.
The phenotype is usually more severe in homozygotes. Example: aa is normal and Aa is affected.
2. A trait is considered to be recessive when there is a clinical phenotype only in individuals that are homozygous for the mutant allele. Example: AA and Aa are normal, aa is affected.
3. The presence and/or severity of "single gene disorders" may be modified by other genes and non-genetic factors.
4. Upper case letters are used for the dominant allele. a. In dominant disorders this is the variant allele (the aa genotype is normal). b. In recessive disorders this is the normal allele (the AA genotype is normal).
B. Symbols used in pedigrees.
3
C. Autosomal dominant traits (familial hypercholesterolemia, achondroplasia, Huntington disease,
A B
5 3 4
p
SB
3 2
Male Female Proband Unspecified sex Number of children Of indicated sex Pregnancy Spontaneous abortion Stillbirth Dizygotic twins Monozygotic twins
3 2
Deceased Affected individuals Heterozygotes for autosomal recessive Carrier of sex-linked trait Mating Consanquineous mating Parents & children (In B, the mother is not shown, indicating that she is not significant to the pedigree)

Marfan syndrome). 1. Pedigree patterns for autosomal dominant traits.
A. B. A family with a new mutation or a disorder showing incomplete penetrance
4
2. Typical mating: Parents: Aa x aa a a A Aa Aa a aa aa
Children Aa (50%), aa (50%) Aa - affected aa - normal
a. In a mating between normal and affected individuals, the probability of a child being affected is 50%.
b. Males and females have equal probability of being affected. c. Male to male inheritance is possible. d. A vertical pattern of inheritance: the trait appears in every generation (if 100% penetrant).
3. Example: interview with a patient with greatly elevated cholesterol as an overview of key counseling issues. This topic will be covered in greater detail later in the course and in the PPS course. a. Information gathering: Is a hereditary basis likely? Family and society are important. b. Therapeutic rapport: To be covered in the Physician/Patient/Society course c. Patient education: What does the patient need to know to know? Implications for other
family members. Patient autonomy and non-directive counseling. 4. New occurrences in unaffected pedigrees may be due to new mutations. 5. A trait may have less that 100% penetrance.
a. If a dominant trait is not expressed (to any degree) in some individuals that carry the mutant allele,it is said to show incomplete penetrance. Example: hereditary retinoblastoma (tumor of the retina) is about 90% penetrant. About 10% of people that have a mutant allele will not develop a tumor.
b. If penetrance is incomplete, a phenotypically normal individual may carry a mutant allele and produce affected offspring.
c. Penetrance and expressivity are different. 6. There may be varying degrees of expressivity. That is, the trait may range from mild to severe
in individuals with the same genotype. An example is neurofibromatosis I. 7. Modifying genes and environmental factors (such as diet, smoking, exercise) contribute to
variable penetrance and expressivity.

D. Autosomal recessive disorders (cystic fibrosis, Tay-Sachs disease, sickle cell disease, α1-antitrypsin deficiency, phenylketonuria). 1. Pedigree pattern for an autosomal recessive trait.
2. Typical mating: Parents: Aa x Aa
A a A AA Aa a AA aa
Children: AA (25%), Aa, aA (50%), aa (25%) AA - normal; Aa - normal (carrier); Aa - affected
a. In a mating between two carriers, 1/4 of all offspring are affected and 1/2 of all offspring are carriers. 3/4 have a normal phenotype.
b. In a mating between two carriers, 1/4 of sibs are affected and 2/3 of the normal offspring are carriers.
c. Males and females are affected equally. d. Horizontal transmission: disease may occur in sibs but is often not seen in other relatives. e. Heterozygotes (carriers) are very common compared to homozygotes.
3. Hardy Weinberg law is a very important relationship that can be used to estimate the frequency of carriers. a. It can be shown (Gelehrter et al p43) that:
q2 + 2pq + p2 = 1 where q is the frequency of the recessive allele p is the frequency of the dominant allele q2 is the frequency of homozygotes for the recessive allele 2pq is the frequency of heterozygotes p2 is the frequency of homozygotes for the dominant allele
b. Example: in the Caucasian population, about 1/2000 are homozygotes for cystic fibrosis. How many are carriers?
q2 = 1/2,000 = .0005 thus: q = .022 p = 1-q = .978 2pq = 2 X .978 X .022 = .043 or about 1/25 About 1 in 25 is a carrier for cystic fibrosis.
5

4. Consanguinity. Parents of children with rare autosomal recessive disorders are often related. a. Matings between closely related individuals are referred to as consanguineous matings. The
likelihood of a child being homozygous at any particular locus is dependent on the coefficient of relationship of the parents. For example, in a mating between two first degree relatives (r=1/2), 1/4 of the child's genes will be identical by descent. That is, for 1/4 of the child's genes, both copies will have come from the same grand-parental chromosome. Consider PKU, for which q=1/100. The chance of this child being affected is 1/4 X 1/100 = 1/400 as opposed to 1/10,000 in a random mating.
b. Consanguinity increases the chances of homozygosity and thus the expression of recessive disorders.
c. The less common a disorder, the more likely it is that the parents are related.
E. X-linked traits (hemophilia A, Duchenne muscular dystrophy, Lesch-Nyhan syndrome, Hunter disease). 1. Determined by genes on the X-chromosome.
2. Females are XX, males are XY: males are hemizygous for loci on the X-chromosome. 3. Trait occurs predominantly in males. 4. Pedigree pattern for an X-linked.
3 2 5 3
2. Typical mating: Parents: A x Aa
A a A AA Aa Y A a
Children: A (25%), a (25%), AA (25%), Aa (25%) A - normal male; a - affected male; AA - normal female; Aa - female carrier
a. Sons of carrier females have 50% risk of disease. b. Daughters of carrier females have 50% risk of carrier state. c. There is no carrier state in males (exception: fragile X syndrome, to be discussed later).
6. Other matings (e.g affected male with carrier female) should be considered when dealing with common traits such as color blindness and glucose-6-phosphate dehydrogenase deficiency.
7. Because of X inactivation, females are mosaics for all X-linked traits. Female carriers may be affected to some extent depending on the pattern of X-inactivation. For example, carriers of Duchenne Muscular dystrophy may show indications of muscle weakness, the extent being related to the pattern of X-inactivation in the muscle tissue.
8. New mutations are frequently seen in genetically lethal (no offspring) X-linked recessive
6

diseases. a. About 1/3 of the cases are new mutations. Since females have two X-chromosomes and
males have one, it follows that in a population, 1/3 of the alleles for a disorder are in males, and 2/3 are in females. For a disorder that is genetically lethal in males, 1/3 of the alleles will be lost in each generation. Therefore, for the frequency of a disorder to remain constant, the loss of alleles must be replaced by new mutations: 1/3 of the cases are due to new mutations.
b. The mother can not a priori be considered to be a carrier.
F. Y chromosome The Y chromosome contains about 150 transcription units and encodes about 30 distinct proteins. The genetics of the Y chromosome will be discussed in the lectures on Sex Determination
G. Mitochondrial inheritance. 1. Mitochondrial DNA (mtDNA)
a. Mitochondria contain a 16Kb circular DNA molecule, mtDNA. mtDNA encodes 13 peptides required for oxidative phosphorylation (the rest are encoded in the nucleus) and the rRNAs and tRNAs which are required for the mitochondrial expression of these peptides.
b. Cells contain many mitochondria, each with 4-10 mtDNA. A person may have both normal and affected mitochondria in any proportion (heteroplasmy).
c. mtDNA has a relatively high mutation rate. 2. Deleterious mtDNA mutations affect functions that depend heavily on oxidative
phoshorylation and therefore result in a broad spectrum of neurological and muscular diseases. 3. Pedigree of a family with a mitochondrially inherited disorder (DM is Diabetes Mellitus). From Reardon et al (1992) Lancet 240:1376-1379.
7

a. Pattern of inheritance differs from X-linked (1). Maternal inheritance; mitochondria are derived (by replication independent of nuclear
division) from those that are present in the ovum. (2). Male and female offspring have equal chances of being affected.
b. Severity of symptoms may be variable. (1) Each person receives a large number of mitochondria from the mother, only some of
which may carry a deleterious mutation. The severity of disease will depend on the proportion of normal versus abnormal mitochondria that are inherited.
(2) The presence of a mixed population of mitochondria is referred to as heteroplasmy (a single population is homoplasmy).
c. Age of onset and rate of progression may be variable. (1) This may be due to the high mutation rate of mtDNA. With a gradual accumulation of
somatic mtDNA mutations, symptoms may begin to appear when the normal mitochondrial function drops below a threshold. Some mtDNAs that contain large deletions may also replicate faster, resulting in a gradual increase in the proportion of defective mitochondria.
(2) The age of onset may also depend on the proportion of normal mitochondria that are inherited (heteroplasmy).
d. A wide range of symptoms may result from the same mtDNA mutation. (1) Depending on environmental and other genetic factors, some organ systems may be
more susceptible than others to a reduced level of oxidative phosphorylation. (2) During early development precursor cells for different organ systems may receive
different proportions of normal and abnormal mitochondria. V. Risk assessment in Mendelian inheritance.
A. Risk is dependent on pattern of inheritance: recessive or dominant, autosomal or X-linked. B. Risk is dependent on the penetrance of the disorder. C. There may be a delayed age of onset for the disorder (when taking a family history, young individuals may have not yet developed symptoms). A. The frequency of an allele being present in a population (given by the Hardy-Weinberg
equilibrium: q2 + 2pq + p2 = 1). B. Dependent on the penetrance of the disorder. C. Appearance of disorder in a pedigree may depend on the age of onset for the disorder. D. Severity is dependent on the expressivity.
VI. Examples of Risk assessment for single gene defects.
A. Examples of risk assessment for autosomal recessive disorders. 1. In this pedigree (cystic fibrosis, which occurs in 1/2000 live births), what is the risk of the
second child being affected? I
1 2 II 1 2
p
a. Both parents must be carriers (heterozygotes).
8

b. The fathers likelihood of transmitting the gene is 1/2. c. The Mothers likelihood of transmitting the gene is 1/2. d. The probability is therefore 1/2 x 1/2 = 1/4.
2. The mother in the previous pedigree (I-2) remarries. What is the risk of the child being affected?
I
1 2 3 II 1 2
p
a. The Mother must be a carrier. Her likelihood of transmitting the gene is 1/2. b. Using the Hardy-Weinberg law, calculate the likelihood that the father (I-3) is a carrier
(see above, under IV.D.6). This is about 1/25. c. The likelihood that the father will transmit the gene is 1/2. d. The probability is therefore 1 X 1/2 x 1/25 x 1/2 = 1/100.
3. What is the probability of the child, II-2, being affected in this pedigree, where the sister (I-2)
has an afflicted child?
9
a. The proband (I-3) has a 50% chance of being a carrier. b. Using the Hardy-Weinberg law, calculate the likelihood that the father (I-4) is a carrier
(see above, under IV.D.6). This is about 1/25. c. The probability is 1/2 x 1/2 x 1/2 x 1/25 = 1/200.
4. In this pedigree, the aunt (I-3) has cystic fibrosis. What is the risk for II-1?
I 1 2 3 4 II 1 2
p
I 1 2 3 II 1
p
a. The mother's (I-2) likelihood of being a carrier is 2/3. (3) Both her mother and father are carriers. (4) She does not have the trait.
b. The probability is 2/3 x 1/2 x 1/25 x 1/2 = 1/150.
5. Consanguinity - relationship by descent from a common ancestor. a. Increases the likelihood of being homozygous and therefore presents an increased risk of
autosomal recessive disorders, particularly those that are rare. b. The closer the relationship, the greater the likelihood of an offspring being homozygous.
Use this, and the next problem to discover why.
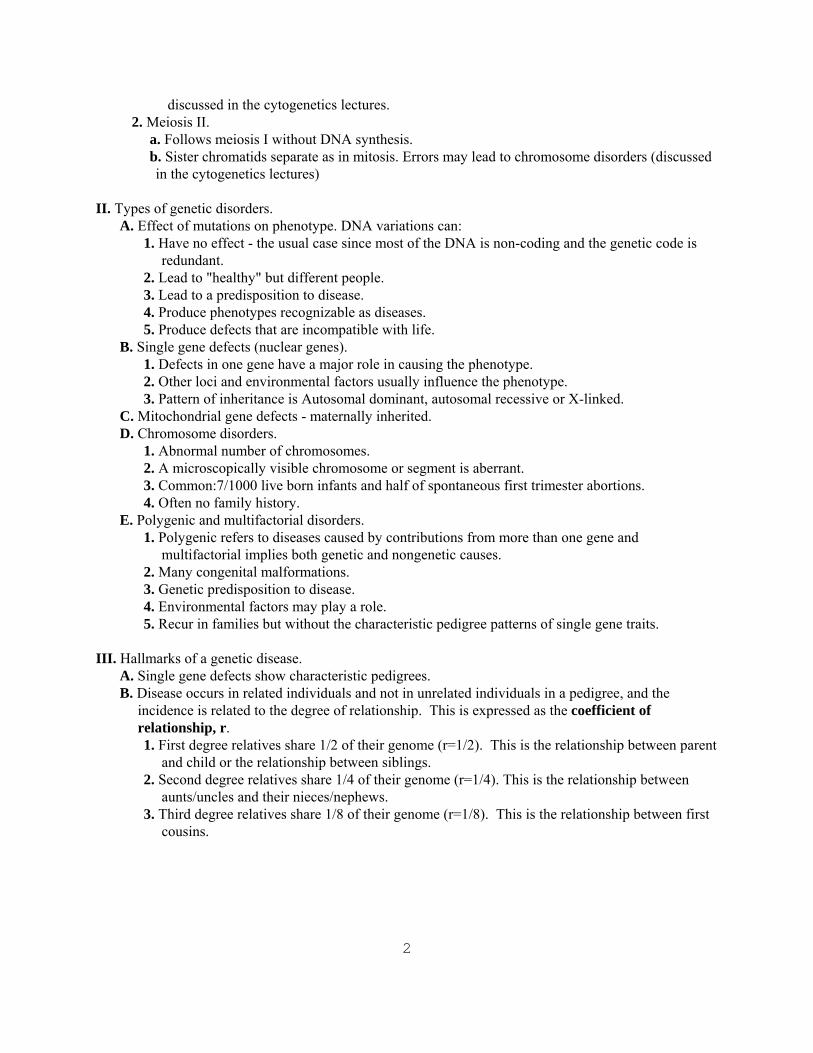
c. In this pedigree, what is the risk that the child, IV-1, will have the disease?
I 1 2 II 1 2 3 4 III 1 2 IV 1
p
d. II-2 and II-3 each have a 1/2 chance of being carriers. e. III-1 and III-2 each have a 1/4 chance of being carriers (actually the chance is slightly
greater than 1/4. If we use a disease frequency of 1/10,000 as in problem 6, there is a 1/50 chance that II-1 is a carrier and a 1/50 chance that II-4 is a carrier. However, for the purposes of counseling this doesn't make any difference since the quantity (1/4 + 1/2*1/50) should be expressed as 1/4, not 0.26).
f. The chance is therefore 1/2 X 1/4 X 1/2 X 1/4 = 1/64.
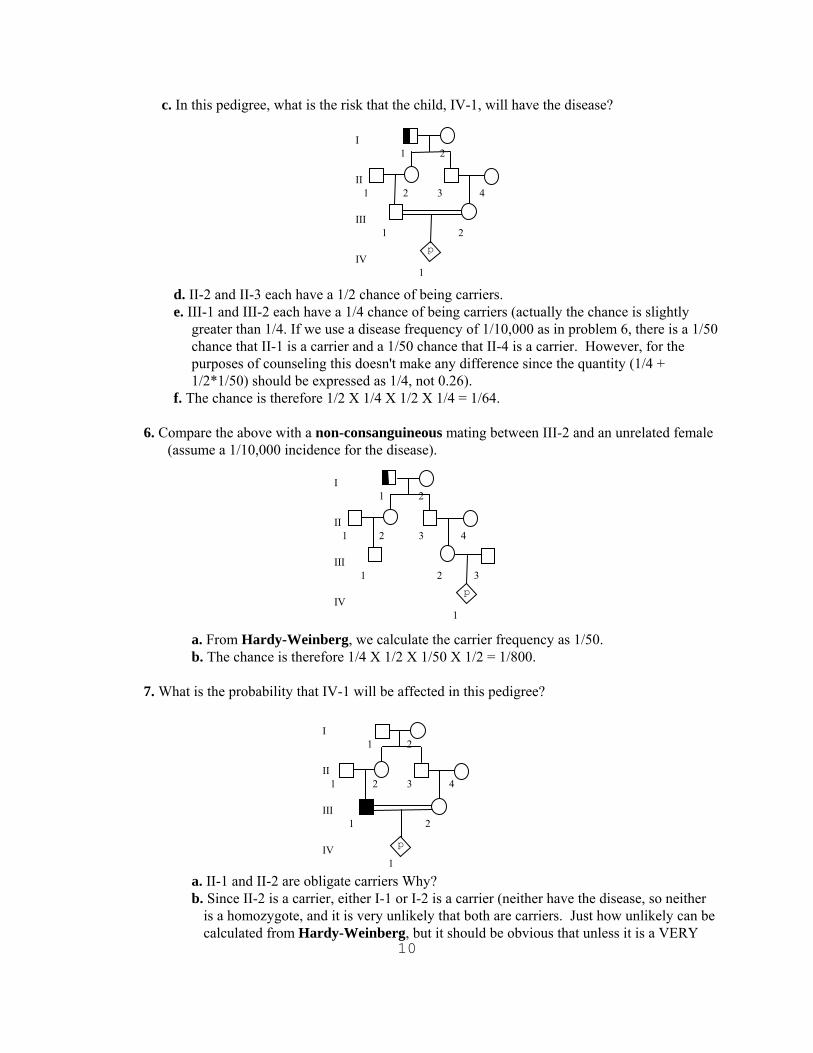
6. Compare the above with a non-consanguineous mating between III-2 and an unrelated female (assume a 1/10,000 incidence for the disease).
10
a. From Hardy-Weinberg, we calculate the carrier frequency as 1/50. b. The chance is therefore 1/4 X 1/2 X 1/50 X 1/2 = 1/800.
7. What is the probability that IV-1 will be affected in this pedigree?
a. II-1 and II-2 are obligate carriers Why?
I 1 2 II 1 2 3 4 III 1 2 3 IV 1
p
p
I 1 2 II 1 2 3 4 III 1 2 IV 1
b. Since II-2 is a carrier, either I-1 or I-2 is a carrier (neither have the disease, so neither is a homozygote, and it is very unlikely that both are carriers. Just how unlikely can be calculated from Hardy-Weinberg, but it should be obvious that unless it is a VERY
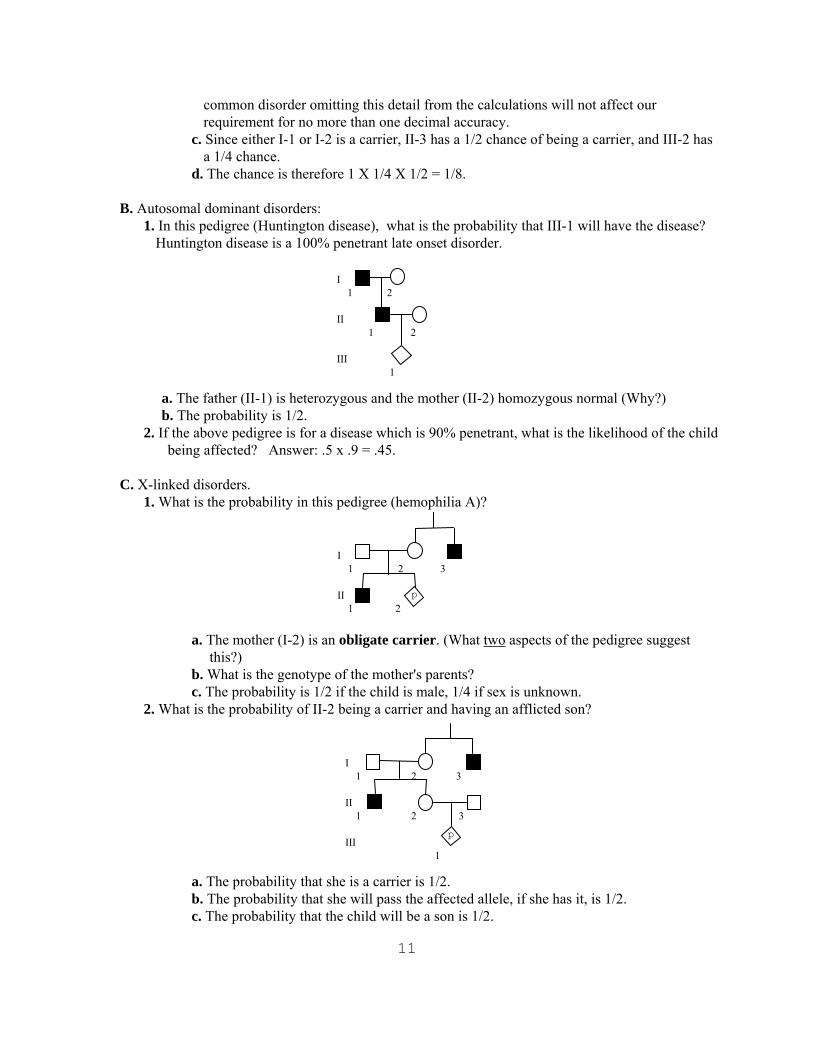
common disorder omitting this detail from the calculations will not affect our requirement for no more than one decimal accuracy.
c. Since either I-1 or I-2 is a carrier, II-3 has a 1/2 chance of being a carrier, and III-2 has a 1/4 chance.
d. The chance is therefore 1 X 1/4 X 1/2 = 1/8.
B. Autosomal dominant disorders: 1. In this pedigree (Huntington disease), what is the probability that III-1 will have the disease?
Huntington disease is a 100% penetrant late onset disorder.
a. The father (II-1) is heterozb. The probability is 1/2.
2. If the above pedigree is for a being affected? Answer: .5
C. X-linked disorders.
1. What is the probability in this
a. The mother (I-2) is anthis?)
b. What is the genotypec. The probability is 1/2
2. What is the probability of II-2
a. The probability that sb. The probability that sc. The probability that t
I 1 2 II 1 2 III 1
ygous and the mother (II-2) homozygous normal (Why?)
disease which is 90% penetrant, what is the likelihood of the child x .9 = .45.
pedigree (hemophilia A)?
I 1 2 3 II 1 2p
obligate carrier. (What two aspects of the pedigree suggest
of the mother's parents? if the child is male, 1/4 if sex is unknown. being a carrier and having an afflicted son?
hhh
I 1 2 3 II 1 2 3 III 1
p
e is a carrier is 1/2. e will pass the affected allele, if she has it, is 1/2. e child will be a son is 1/2.
11

d. The probability is 1/2 x 1/2 x 1/2 = 1/8.
3. In this pedigree for a genetically lethal disorder, what is the likelihood that II-2 will be affected?
a. The case in II-1 may bb. The mother has a 2/3
allele. The chance is D. Complex Pedigrees.
Many manI was ma
This widow hadMy father fell in
This made my daFor my daughter w
To complicate I soon beca
My little babAnd so becamFor if he was m
To the widow's grown
Father's wife tAnd he became mMy wife is now
Because although
Oh, if my wife'sAnd every tim
For now I haveAs the husband
I'm my oIt sounds funny, I k
"My Own Grandpa" lyrics by Dwight B. Lath
I 1 2 3 II 1 2
p
e due to a new mutation (1/3) or inherited from the mother (2/3). chance of being a carrier and, if so, a 1/2 chance of passing the 1/3 if the child is male, 1/6 if the sex is unknown.
y years ago, when I was twenty-three, rried to a widow as pretty as can be, a grown-up daughter who had hair of red, love with her and soon the two were wed.
d my son-in-law and changed my very life, as my mother, for she was my father's wife.
the matter, even though it brought me joy, me the father of a bouncing baby boy.
y thus became a brother-in-law to dad, e my uncle, though it made me very sad, y uncle then that also made him brother
-up daughter, who of course was my step-mother.
hen had a son who kept them on the run. y grandchild for he was my daughter's son.
my mother's mother and it makes me blue, she is my wife, she's my grandmother, too.
my grandmother then I am her grandchild.
e I think of it it nearly drives me wild. become the strangest case you ever saw -- of my grandmother, I am my own grandpa.
wn grandpa, I'm my own grandpa. now, but it really is so --I'm my own grandpa.
am and Moe Jaffee
12


























