Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Influence of social support on health-related qualityof life in patients with systemic lupus erythematosus
Yuan Zheng & Dong-Qing Ye & Hai-Feng Pan &
Wen-Xian Li & Lian-Hong Li & Jing Li & Xiang-Pei Li &Jian-Hua Xu
Received: 4 August 2008 /Revised: 15 September 2008 /Accepted: 22 October 2008 /Published online: 11 November 2008# Clinical Rheumatology 2008
Abstract The objective of this study was to examinehealth-related quality of life (HRQOL) and social supportin patients with systemic lupus erythematosus (SLE) andcompare it with healthy people, to identify the relationshipbetween social support and HRQOL in SLE patients, and toassess the influence of age, SLE Disease Activity Index(SLEDAI) and disease duration on HRQOL. We adminis-tered The Medical Outcomes Study Short Form-36 (MOSSF-36) questionnaire and the Social Support Rate Scale(SSRS) to a group of 202 patients with SLE and a healthycontrol group of 207 individuals. Spearman correlation wasperformed to identify the relationship between socialsupport and HRQOL in SLE patients. The ordinal regres-sion analyses were used to identify independent variablesthat were associated with the PCS and MCS. Results showthat the physical (PCS) and mental (MCS) componentsummary scores of MOS SF-36 were lower in patientscompared with healthy controls. Patients with SLE have apoorer social support as compared with healthy controls insubjective support, objective support, and availability ofsupport. There was a positive correlation between social
support and PCS and MCS. MCS and PCS were negativelyassociated with age and SLEDAI. MCS were negativelyassociated with disease duration. Taken together, this datasuggested that patients with SLE have significant impair-ment of their HRQOL and less social support. HRQOLmay be affected by social support, age, and SLEDAI.
Keywords Health-related quality of life . Social support .
Systemic lupus erythematosus
Introduction
Systemic lupus erythematosus is a multisystem, autoim-mune, connective-tissue disorder with a broad range ofclinical presentations [1]. The course of SLE generallyinvolves periods of intense flares and periods of remission.[2]. Over the past years, there has been a remarkablesurvival improvement in SLE patients, probably related totechnological advances in therapeutics. Survival per se is nolonger perceived to be the only end point [3]. HRQOLassessment is nowadays considered as an importantcomponent of evaluation in chronic disease [4].
HRQOL is a multidimensional construct that typicallyincludes four broad categories: physical, functional, socialand emotional well-being [5]. QOL or HRQOL is definedas “individual’s perception of their position in life in thecontext of the culture and value systems in which they liveand in relation to their goals, expectations, standards, andconcerns” [6].
Social support has captured the attention of bothsociologist and medical scientists, which is a multiconstructwith multiple dimensions. Cobb primarily defined socialsupport as “information leading the subject to believe thathe or she is cared for and loved, that he/she is esteemed and
Clin Rheumatol (2009) 28:265–269DOI 10.1007/s10067-008-1033-7
Y. Zheng :D.-Q. Ye (*) :H.-F. Pan :W.-X. Li : L.-H. Li : J. LiDepartment of Epidemiology and Biostatistics,School of Public Health, Anhui Medical University,81 Meishan Road,Hefei, Anhui 230032, People’s Republic of Chinae-mail: [email protected]
X.-P. LiDepartment of Rheumatology, Anhui Provincial Hospital,Hefei, People’s Republic of China
J.-H. XuDepartment of Rheumatology, First Affiliated Hospital,Anhui Medical University,Hefei, People’s Republic of China

valued, and he/she belongs to a network of communicationand mutual obligation” [7].
Conceptualizations of social support have focused on thesources of support, the nature of what was available orprovided, and unidirectional versus reciprocal function [8].Social support is thought to affect health in two ways: byregulating psychological processes; by facilitating behav-ioral processes [9].
The studies on HRQOL in patients with SLE have beenwidely conducted in context of the developed countries[10–12]. However, there were very limited studies focusedon this in developing countries [13].
The present study was initiated to examine HRQOL andsocial support in SLE patients in China and compare themwith healthy people. We also identified the relationshipbetween social support and HRQOL in SLE patients andassessed the influence of age, SLEDAI, and diseaseduration on HRQOL.
Materials and methods
Patient selection
Consecutive patients with SLE were included in the study.All patients met the criteria for their diagnosis based onAmerican College of Rheumatology (ACR) criteria [14,15]. Two hundred and two patients were included in thiscase control study. Out of the 230 patients approached,twenty eight patients refused to consent. Response rate ofeffective questionnaires was 87.83%.
Control group
The control group was selected from community-basedhealthy person. They come from the same area as patients.They were matched to the SLE patients by gender, age,education level and marital status.
Information on subject age, gender, education andmarital status were collected from subject self-report.Disease duration was obtained from SLE patients. All thepatients and controls gave informed consent.
Quality of life assessment
Quality of life assessment HRQOL was assessed using theSF-36 questionnaire [16]. The SF-36 is a generic instrumentwith scores that are based on responses to individualquestions, which are summarized into eight scales, each ofwhich measures a health concept. These scales includefunction domains and aspects of well-being, as follows:physical function (PF), limitations in physical activitiesbecause of health problems; role—physical (RP), limita-
tions in usual role activities because of physical healthproblems; bodily pain (BP), limitations in social activitiesbecause of physical or emotional problems; general health(GH), influence of pain on daily activities; vitality (VT),energy level and fatigue; social function (SF), subjectiveperception of health status; role—emotional (RE), limita-tions in usual role activities because of emotional problems;mental health (MH), psychological distress and well-being.In addition, the scores of the eight subscales were computedinto two summary scores, physical component summary(PCS) and mental component summary score (MCS).
Social support assessment
The Social Support Rate Scale (SSRS) questionnaire hasten items. Each item represents one of three mainsubscales of the Social support. The ten items werecategorized under the three dimensions of Subjectivesupport (emotional support, four items); objective support(tangible support, three items) and availability of support(three items). Higher social support scores indicate abetter social support. The total score is determined by thesum of all the single scales. The validity and reliabilityof the SSRS have been validated. This instrumentevidenced a good internal consistency of alpha rangedfrom 0.89 to 0.94 [17].
Disease activity assessment
Disease activity was assessed using the SLE DiseaseActivity Index (SLEDAI) [18]. It is a validated diseaseactivity measure that includes clinical and laboratorymeasures of SLE activity. The total SLEDAI score canrange from 0 to 105.
Statistical analyses
Statistical analyses were carried out using the SPSS 10.01software (SPSS Inc., 2000). Statistical analysis included t-test for SSRS and SF-36 scales and Mann–Whitney U testfor variables not normally distributed. Spearman correlationwas performed to identify the relationship between socialsupport and health-related quality of life. Ordinal regressionwas carried out to assess the impact of related variables. Aprobability value of less than 0.05 was consideredsignificant.
Result
The patient group comprised 202 SLE patients with meanduration (4.38±3.96 year, range1 month to 20 year). Themean SLEDAI (score was 10.09±7.44, range0–24). The
266 Clin Rheumatol (2009) 28:265–269
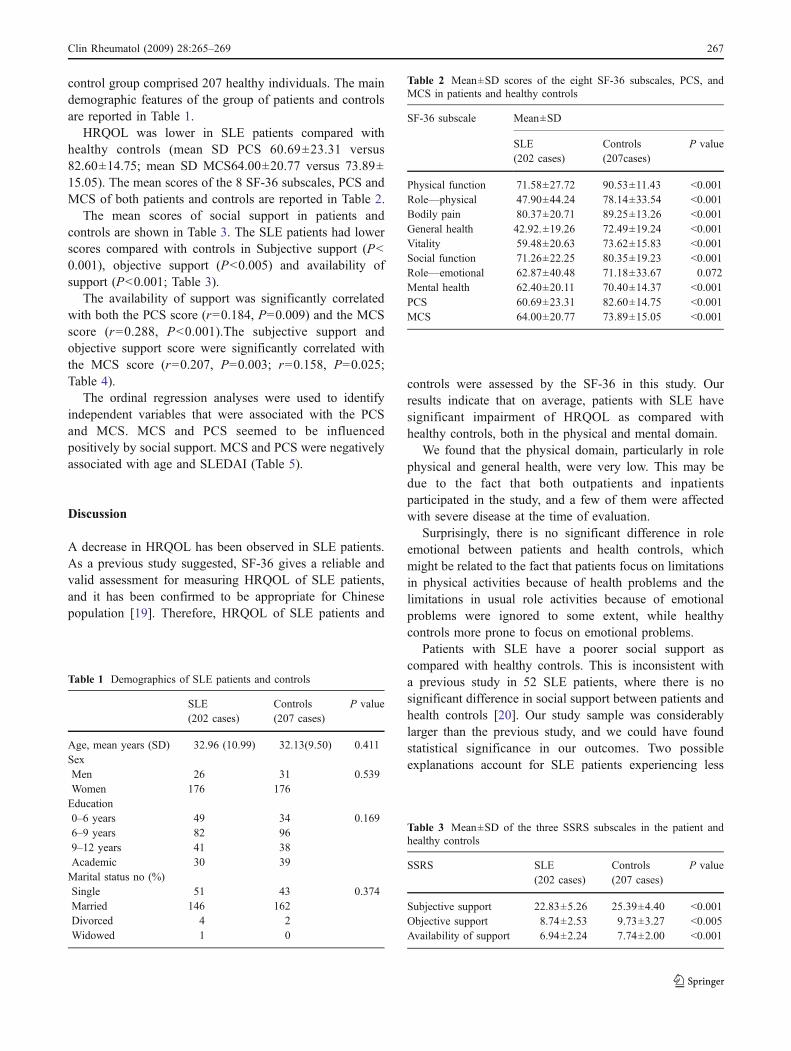
control group comprised 207 healthy individuals. The maindemographic features of the group of patients and controlsare reported in Table 1.
HRQOL was lower in SLE patients compared withhealthy controls (mean SD PCS 60.69±23.31 versus82.60±14.75; mean SD MCS64.00±20.77 versus 73.89±15.05). The mean scores of the 8 SF-36 subscales, PCS andMCS of both patients and controls are reported in Table 2.
The mean scores of social support in patients andcontrols are shown in Table 3. The SLE patients had lowerscores compared with controls in Subjective support (P<0.001), objective support (P<0.005) and availability ofsupport (P<0.001; Table 3).
The availability of support was significantly correlatedwith both the PCS score (r=0.184, P=0.009) and the MCSscore (r=0.288, P<0.001).The subjective support andobjective support score were significantly correlated withthe MCS score (r=0.207, P=0.003; r=0.158, P=0.025;Table 4).
The ordinal regression analyses were used to identifyindependent variables that were associated with the PCSand MCS. MCS and PCS seemed to be influencedpositively by social support. MCS and PCS were negativelyassociated with age and SLEDAI (Table 5).
Discussion
A decrease in HRQOL has been observed in SLE patients.As a previous study suggested, SF-36 gives a reliable andvalid assessment for measuring HRQOL of SLE patients,and it has been confirmed to be appropriate for Chinesepopulation [19]. Therefore, HRQOL of SLE patients and
controls were assessed by the SF-36 in this study. Ourresults indicate that on average, patients with SLE havesignificant impairment of HRQOL as compared withhealthy controls, both in the physical and mental domain.
We found that the physical domain, particularly in rolephysical and general health, were very low. This may bedue to the fact that both outpatients and inpatientsparticipated in the study, and a few of them were affectedwith severe disease at the time of evaluation.
Surprisingly, there is no significant difference in roleemotional between patients and health controls, whichmight be related to the fact that patients focus on limitationsin physical activities because of health problems and thelimitations in usual role activities because of emotionalproblems were ignored to some extent, while healthycontrols more prone to focus on emotional problems.
Patients with SLE have a poorer social support ascompared with healthy controls. This is inconsistent witha previous study in 52 SLE patients, where there is nosignificant difference in social support between patients andhealth controls [20]. Our study sample was considerablylarger than the previous study, and we could have foundstatistical significance in our outcomes. Two possibleexplanations account for SLE patients experiencing less
Table 1 Demographics of SLE patients and controls
SLE(202 cases)
Controls(207 cases)
P value
Age, mean years (SD) 32.96 (10.99) 32.13(9.50) 0.411SexMen 26 31 0.539Women 176 176Education0–6 years 49 34 0.1696–9 years 82 969–12 years 41 38Academic 30 39Marital status no (%)Single 51 43 0.374Married 146 162Divorced 4 2Widowed 1 0
Table 2 Mean±SD scores of the eight SF-36 subscales, PCS, andMCS in patients and healthy controls
SF-36 subscale Mean±SD
SLE(202 cases)
Controls(207cases)
P value
Physical function 71.58±27.72 90.53±11.43 <0.001Role—physical 47.90±44.24 78.14±33.54 <0.001Bodily pain 80.37±20.71 89.25±13.26 <0.001General health 42.92.±19.26 72.49±19.24 <0.001Vitality 59.48±20.63 73.62±15.83 <0.001Social function 71.26±22.25 80.35±19.23 <0.001Role—emotional 62.87±40.48 71.18±33.67 0.072Mental health 62.40±20.11 70.40±14.37 <0.001PCS 60.69±23.31 82.60±14.75 <0.001MCS 64.00±20.77 73.89±15.05 <0.001
Table 3 Mean±SD of the three SSRS subscales in the patient andhealthy controls
SSRS SLE(202 cases)
Controls(207 cases)
P value
Subjective support 22.83±5.26 25.39±4.40 <0.001Objective support 8.74±2.53 9.73±3.27 <0.005Availability of support 6.94±2.24 7.74±2.00 <0.001
Clin Rheumatol (2009) 28:265–269 267

social support. Firstly, because of knowing little about SLE,a few friends of patients stay away from them for worryingabout infection. Secondly, with the fear of a definitiveabandonment, a few patients isolate themselves fromothers.
It is necessary to improve the social support in SLEpatients. We can provide information on SLE to theirfriends. We can also develop a trusting relationship thatallows free communication between patient and therapistand family members.
The role of social support in chronic disease, such ascancer, has been widely researched. But its impact onsystemic lupus erythematosus has not been well confirmed.Karlson EW et al. [21] demonstrated less social support wasassociated with greater disease activity. Sutcliffe N et al.[22] reported a higher level of perceived social support wasassociated with better quality of life, except for role—emotional. Our results indicate social support is a contrib-utor of better HRQOL among SLE patients, especially inMCS. One potential mechanism is through the bufferingproperties of social support. Social support can buffer theeffects of stressful life events [7]. Therefore, it can help apatient adjust to life with a disease. Individuals who havehigher levels of perceived social support can manage thesituation effectively, even in the most difficult situation,while lower levels of perceived social support contribute topoor outcomes [23].
The result of this study also implied that the ability toutilize social support and emotional support seemed to playa more important role than tangible support in improvingHRQOL. As well as providing material aid or behavioralassistance, expressing love and affection, offering guidance,advice, and information may be helpful.
The ordinal regression analysis was used to identifysome associations in patients with SLE. The relationshipbetween age and SLEDAI and HRQOL of SLE patientremains controversial. Rinaldi S et al. [11] reported that agehas a negative effect on HRQOL. Khanna S et al. [13]demonstrated that no correlation between age and quality oflife. Wang C et al. [24] reported a negative correlationbetween HRQOL and SLEDAI, while Abu-Shakra M et al.[12] demonstrated no correlation between HRQOL andSLEDAI. In this study, age and SLEDAI were found to benegatively associated with PCS and MCS. More attentionshould be paid to older patients and patients with highdisease activity.
In interpreting these findings, a few limitationsdeserve comment. For one thing, we may underestimatethe impact on HRQOL in SLE patients caused by self-selection bias. Twenty eight SLE patients refused toattend the study. Individuals who refused to attend thestudy may be particularly vulnerable and highly de-pressed compared with participating group. For another,because of doubting about the timing of the relationship,it is also difficult to determine a casual relationship in across-sectional study. A follow-up study is needed tovalidate our findings.
Despite these limitations, our data suggested that SLEpatients experienced lower HRQOL as well as less socialsupport. Therapist and family members should not onlyfocus on disease-related factors but also recognize theimportance of social support and other variables in patientswith SLE. Our findings may improve patient care andbenefit disease management.
Acknowledgments This work was supported by grants from theNational Natural Science Foundation of China (30571608, 30771848)and the Specialized Research Fund for the Doctoral Program ofHigher Education of China (20070366002).
Disclosures None.
References
1. D’Cruz DP, Khamashta MA, Hughes GRV (2007) Systemic lupuserythematosus. Lancet 369:587–589
2. Bertoli AM, Alarcon GS, McGwin G Jr (2006) LUMINA StudyGroup. Systemic lupus erythematosus in a multiethnic U.S. cohort
Table 5 Variables independently associated with HRQOL by ordinalregression
Estimate Wald P value
Dependent variable: MCSIndependent variablesSocial support 0.121 21.149 <0.001Age −0.042 7.080 0.008SLEDAI −0.050 4.201 0.040
Dependent variable: PCSAge −0.038 10.008 0.002Social support 0.041 5.788 0.016SLEDAI −0.039 4.968 0.026
Model fitting: MCS P<0.001 PCS P<0.001MCS pseudo R2 =0.201 PCS Pseudo R2 =0.099
Table 4 Linear correlation between SSRS and HRQOL
SSRS PCS r(P value) MCS r(P value)
Subjective support 0.132(0.062) 0.207(0.003)Objective support 0.019(0.789) 0.158(0.025)Availability of support 0.184(0.009) 0.288(0.000)
268 Clin Rheumatol (2009) 28:265–269

(LUMINA) XXVII: factors predictive of a decline to low levels ofdisease activity. Lupus 15:13–18
3. Guyatt GH, Feeny DH, Patrick DL (1993) Measuring health-related quality of life. Ann Intern Med 118:622–629
4. Whoqol Group (The) (1993) Study protocol for the World HealthOrganisation project to develop a quality if life assessmentinstrument (Whoqol). Qual Life Res 2:153–159
5. Ware JE Jr, Sherbourne CD (1992) The MOS 36-item short formhealth survey (SF-36): I. Conceptual framework and itemselection. Med Care 30:473–483
6. The World Health Organization Quality of Life assessment(WHOQOL): position paper from the World Health Organization.Soc Sci Med 41:1403–1409
7. Cobb S (1976) Social support as a moderator of life stress.Psychosom Med 38:300–314
8. Decker CL (2007) Social support and adolescent cancer survivors:A review of the literature. Psycho-Oncol 16:1–11
9. Uchino BN (2006) Social support and health: a review ofphysiological processes potentially underlying links to diseaseoutcomes. J Behav Med 29:377–387
10. Alarcón GS, McGwin G Jr, Uribe A et al (2004) Systemic lupuserythematosus in a multiethnic lupus cohort (LUMINA). XVII.Predictors of self-reported health related quality of life early indisease course. Arthritis Care Res 51:465–474
11. Rinaldi S, Doria A, Salaffi F et al (2004) Health-related quality oflife in Italian patients with systemic lupus erythematosus. I.Relationship between physical and mental dimension and impactof age. Rheumatology 43:1574–1579
12. Abu-Shakra M, Keren A, Livshitz I et al (2006) Sense ofcoherence and its impact on quality of life of patients withsystemic lupus erythematosus. Lupus 15:32–37
13. Khanna S, Pal H, Pandey RM, Handa R (2004) The relationshipbetween disease activity and quality of life in systemic lupuserythematosus. Rheumatology 43:1536–1154
14. Hochberg MC (1997) Updating the American College ofRheumatology revised criteria for the classification of systemiclupus erythematosus. Arthritis Rheum 40:1725
15. Tan EM, Cohen AS, Fries JF et al (1982) The 1982 revisedcriteria for the classification of systemic lupus erythematosus.Arthritis Rheum 25:1271–1277
16. Ware JE, Snow KK, Kosonski M et al (1993) SF-36 Health surveymanual and interpretation guide. The Health Institute, NewEngland Medical Center, Boston
17. Xiao SY (1993) The social support rate scale. Chinese Journal ofPsychology 7(Suppl):42–46
18. Bombardier C, Gladman DD, Urowitz MB et al (1992) TheCommittee on Prognosis Studies in SLE. Derivation of theSLEDAI: a disease activity index for lupus patients. ArthritisRheum 35:630–640
19. Chaojie L, NingXiu L, Xiaohui R et al (2001) Feasibility of usingshort Form 36 in Chinese population. J West China Univ Med Sci32:39–42
20. Kozora E, EllisonMC, Waxmonsky JA et al (2005) Major life stress,coping styles, and social support in relation to psychological distressin patients with systemic lupus erythematosus. Lupus 14:363–372
21. Karlson EW, Daltroy LH, Lew RA et al (1997) The relationship ofsocioeconomic status, race, and modifiable risk factors to outcomes inpatients with systemic lupus erythematosus. Arthritis Rheum 40:47–56
22. Sutcliffe N, Clarke AE, Levinton C et al (1999) Associates ofhealth status in patients with systemic lupus erythematosus. JRheumatol 26:2352–2356
23. Vyavaharkar M, Moneyham L, Tavakoli A et al (2007) Socialsupport, coping, and medication adherence among HIV-positivewomen with depression living in rural areas of the southeasternUnited States. Aids Patient Care and STDs 21:667–680
24. Wang C, Mayo NE, Fortin PR (2001) The relationship betweenhealth related quality of life and disease activity and damage insystemic lupus erythematosus. J Rheumatol 28:525–532
Clin Rheumatol (2009) 28:265–269 269