Embed Size (px)
Citation preview

In¯uence of chronic alcohol abuseand ensuing forced abstinence onstatic subjective accommodation functionin humans
Hugh Campbell, Michael J. Doughty, Gordon Heron and RogerG. Ackerley
Department of Vision Sciences, Glasgow-Caledonian University, Glasgow G4 OBA, UK
Summary
Purpose. Acute alcohol ingestion can change accommodation, but the long term effects ofsustained alcohol consumption on accommodative function have not been studied in detail. Thisstudy was thus undertaken on individuals with a history of alcohol abuse.
Methods. Thirty-seven male individuals aged 25±56 years (average 40 years) from an alcoholrehabilitation centre in Inverness, Scotland, were assessed on admission and after a week offorced abstinence. The results were compared to a paired age-matched set of control malesubjects. The static amplitude of accommodation was measured by an RAF rule, and the pupilsize measured with a pupil gauge.
Results. On admission, the group mean measured amplitude of accommodation was 4:7 ^ 2:2 D(mean ^ SD). These values for the alcoholics were lower than age-matched controls (of 5:9 ^ 2:9 D�:The slope of the age-dependent decline in RAF rule accommodation measures was signi®cantlysmaller for the alcoholics compared to controls (at 0:215 ^ 0:027 D=year versus 0:332 ^0:015 D=year; respectively; p , 0:001�; with the younger alcoholics showing a greater impairment.Following abstinence, there was no measurable change in accommodation measured, indicatingthe lower amplitude in the alcoholics was not attributable to circulatory alcohol levels. The restingpupil diameter in the alcoholics was 4:37 ^ 0:63 mm compared to the controls of 3:97 ^ 0:75 mm;with a higher incidence of small pupils (#3 mm) in the controls.
Conclusions. The results indicate that chronic alcohol use can adversely affect subjective staticaccommodation, especially in younger alcoholics, as well as cause slight mydriasis. q 2001 TheCollege of Optometrists. Published by Elsevier Science Ltd. All rights reserved.
Introduction
A British Medical Association booklet for patients in the
late 1980s states that an average GP practice with 2000
patients aged between 15 and 75 would have 340 patients
who were drinking above sensible limits; 19 would be
classi®ed as dependent drinkers, i.e. alcoholics. Routine
optometric assessment of the near vision of such patients
referred from GPs indicated a precocious requirement
for reading additions in spectacles. For example, one emme-
tropic individual with complaints of photophobia, lacrima-
tion and blurred vision for close work, was found to require
a 11.50 DS reading addition despite his age of 35 years.
The consultant ophthalmologist, to whom he was referred,
concluded that his symptoms were probably related to
chronic alcohol consumption. A further investigation
seemed warranted for while there have been a number of
reports on the acute effects of alcohol consumption on
accommodation, the effects of chronic alcohol abuse of
the accommodation do not appear to have been established,
and such individuals are more likely to visit an optometric
practice.
The effect of alcohol consumption on vision has long
197
Ophthal. Physiol. Opt. Vol. 21, No. 3, pp. 197±205, 2001q 2001 The College of Optometrists. Published by Elsevier Science Ltd
All rights reserved. Printed in Great Britain0275-5408/01/$20.00
www.elsevier.com/locate/ophopt
PII: S0275-5408(00)00029-6
Received: 29 November 1999
Revised form: 10 April 2000
Accepted: 26 June 2000
Correspondence and reprint requests to: Michael J. Doughty. Tel.: 144-
141-3313393; fax: 144-141-3313387.
E-mail address: [email protected] (M. J. Doughty).

attracted attention (Goldberg, 1943; Watten and Lie, 1996;
Wegner and Fahle, 1999), especially since the adverse
effects of ethanol on visual function can have substantial
social and economic impacts including safety of the public
at large (Stapleton et al., 1986; Hindmarch et al., 1992). The
acute effects of alcohol consumption on accommodation
and related functions of the eye have been assessed
(Cohen and Alpern, 1969; Levett and Karras, 1977;
Hogan and Lin®eld 1983; Wilson and Mitchell, 1983;
Hogan and Gilmartin 1985; Miller et al., 1985, 1986; Hill
and Toffolon, 1990; Watten and Lie, 1996) and while the
outcomes from such studies have been rather mixed (see
Discussion), these types of investigations can be considered
as assessments of the impact of CNS depression on oculo-
motor function; ethanol is a potent CNS depressant drug
(Nutt and Peters, 1994). A neurological basis to the effects
of chronic excessive alcohol consumption (i.e. more than 21
units/week) has been explored by assessment of pupillary
function (Skogland, 1943; Schleyer and Wichmann, 1961;
Brown et al., 1977; Myers et al., 1979; Rubin et al., 1980;
Tan et al., 1984; Miralles et al., 1995) or corneal sensitivity
(Goldberg, 1943). The results of such studies have also been
inconclusive, perhaps as a result of the various control
groups not being well de®ned.
The present study was designed to compare accommodative
function and pupil status in a group of chronic alcoholics,
rehabilitating in a residential centre. The assessment of
possible dysfunction was made by comparison with a
de®ned group of age- and spectacle correction-matched
non-alcoholic individuals. A further part of this study was
to re-measure these aspects of visual function after one
week's supervised abstinence from alcohol consumption.
After this period of time it can be reasonably assumed that
all traces of alcohol in the body have been metabolised
(Lands, 1998). These latter measures therefore allow one
to determine what the effects of alcohol itself, rather than
alcohol per se, have on visual function.
Methods
Study subjects and study design
Two groups of individuals were recruited for this study,
namely 37 diagnosed male alcoholics and 37 age- and
spectacle-matched (paired) controls who consumed less
than 21 units of alcohol/week. The alcoholic subjects,
with a history of 5±15 years of alcohol abuse, were assessed
by clinical staff using the DSM-III-R (Diagnostic and
Statistical Manual of Mental Disorders) system. The
Highlands Psychiatric Research Group (HPRG; Highland
Health Board, Inverness) provided approval for the study
and facilitated access to the subjects to one of us (H.C.). Part
of the diagnosis of alcohol abuse was based on blood plasma
levels of the enzyme gamma-glutamyl transpeptidase
(GGT) and the red blood cell mean corpuscular volume
(MCV). These measures, when certain cut-off values are
applied, provide an indication of liver damage caused by
the alcohol abuse (Yersin et al., 1995). Blood samples were
taken by HPRG staff, analysed on site and also sent to
Scotia Pharmaceuticals (NS, Canada) for further analyses.
The mean GGT levels, an indicator of liver damage, were
113 ^ 96 Units/L (median 93 Units/L, range 17±366 Units/
L). With a cut off of 50 Units/L for alcoholic abuse (Yersin
et al., 1995), 31 (83.8%) of the individuals would be
classi®ed as positive for alcohol abuse. The MCV averaged
95:3 ^ 5:54 fentoL, median 96 fentoL, which with an upper
limit of normal of 95 fentoL, would mean that only 25
(67.6%) of the alcoholics would be classi®ed as positive
for alcohol abuse with this red blood cell test. The patients
were admitted on a voluntary basis with agreement to
monitored abstinence. They were assessed shortly after
admission to the centre and abstinence was enforced by
behaviour monitoring and random breathalyser checks,
e.g. after exercise breaks or visitation by family members.
The control male subjects were recruited from the opto-
metric practice of one of us (H.C.), after having the study
protocol explained to them and written consent forms were
signed. None of the control group were taking any medica-
tions, and had no ocular abnormality other than refractive
error and their VA was 6/9 or better. This group of control
subjects were age-matched to the alcoholics and with a
refractive error match to within ^0.5 DS, and usually to
within ^0.25 DS. The control subjects were provided with
an information lea¯et explaining what a unit of alcohol was
and were asked to keep a drinks diary of any alcohol
consumed (so as to conform with the upper-advised limit
of casual consumption of alcohol). All control subjects were
designated sober at the time of the assessments.
Measurements taken at the start of the study (designated
as admission for the alcoholics subjects) have been signi®ed
as T1 and a second assessment (T2) was made on the
alcoholics after a period of forced abstinence of seven
days. For practical reasons, these assessments and the
corresponding two measurements taken on the control
group were carried out at any time during the working
day. All subjects were identi®ed by a numerical code.
Clinical assessments
All subjects in the study had refractive error, amplitude of
accommodation and pupil size assessed. For measures of
static accommodation, a near-point rule (an RAF rule;
Clement Clarke, UK) and a modi®ed RAF rule utilising
the principle of the Badal-type optometer (Bennett, 1977)
were used monocularly. For the RAF rule, the distance for
clear resolution of the N5 type was assessed ®ve times for
both incoming (up measures to blur) and receding (back
measures to achieve clarity) presentation of the target
(which was manually moved along the 50 cm rule). The
Badal-type optometer had a 18.00 DS lens mounted on
198 Ophthal. Physiol. Opt. 2001 21: No 3

the RAF rule with the second focal point coincident with the
anterior focal point of the eye. The upper limit of measure-
ment with this device is limited to 8 D, but it was felt that
this would not be a signi®cant limitation, since the alcoholic
subjects were expected to have low amplitudes of accom-
modation. Pupil measures were taken to 0.5 mm accuracy
using an ophthalmic rule with black semicircles along its
edge, with the subjects ®xating on a distant Snellen acuity
chart. Room illumination was controlled for both measures,
so that the chart luminance was set at approximately 150±
250 cd/m2.
Statistical analyses
Graphic presentation and statistical analyses were carried
out on Systat Version 8.0 (Systat Inc., Evanston, IL, USA)
and were principally based upon the use of a paired Students
t-test (since the alcoholic subjects were age- and spectacle-
matched with a set of control subjects). Linear regression
analyses were used to assess age-dependent changes in the
clinical measures. Level of statistical signi®cance was set at
p , 0:05:
Results
The study subjects
The two groups of study subjects were age-matched by
pairing a control subject to each alcoholic. The average age
in both groups was thus 40:4 ^ 8:4 years �n � 37 each,
mean ^ SD), with a median value of 40 years for the age
range of 25±56 years. The pairing was also designed to
match refractive errors as reasonably as possible (Table 1),
and the difference between the groups was not signi®cantly
different. Astigmatism in the subjects was limited to
^2.0 D, and was mostly much less than this or non-existent.
The spectacle prescriptions for 18 of the alcoholics included
a near-point addition of 0.50±2.00 D (average 1.28 D),
while just 12 of the controls had a near-point addition of
0.50±2.25 D (average 1.21 D).
Measurement of accommodative function in alcoholics on
admission
The average RAF rule measures in the alcoholics at the
®rst assessment (T1) was 4.65 D from ®ve measures of the
response to an inwardly moving target (up or positive
measures), and averaged 4.60 D for the reverse response
(back or negative measures) (Table 2). The distribution of
all forward and back values was normally distributed about
the modal value of 4.5 D (e.g. Figure 1A), as assessed by a
Komologorov±Smirnov test �p , 0:05�; and the median
amplitudes were 4.8 D for both positive and negative
measures of accommodation (range 0±9 D). The variance
across the ®ve measures did not exceed 0.5 D (average 11%)
for any one subject for either response and the overall
variance between subjects, expressed as a standard
deviation, was 2.23 and 2.31 D, respectively, for the two
assessments. A similar result was obtained with a Badal-
type optometer, with average responses for the forward
and back tests being 4.0 ^ 2.6 D and 4.0 ^ 2.6 D,
respectively (mean ^ SD), with median values of 3.5 D
(Table 3).
There was the expected age-dependent decline in
amplitude of accommodation as assessed by the RAF rule
(Figure 2A), using forward or back response measures. Over
the age range of 25±56 years, linear regression analyses
(using the averaged RAF rule data from the forward and
back measures) showed the age-dependent decline in static
accommodation to be statistically signi®cant �p , 0:001; F
ratio 65.272, r2 � 0:651� and to have a magnitude of
20.215 ^ 0.027 D/decade (mean ^ SE of estimate).
In¯uence of chronic alcohol abuse on static subjective accommodation function: H. Campbell et al. 199
Table 1. Subject characteristics
Subject group Age (year) (mean ^ SD) Distance refractiveerror (DS)
(mean ^ SD)
Best correcteddistance refractive
error (D)(mean ^ SD)
Controls 40:4 ^ 8:4 0:10 ^ 1:03 0:21 ^ 0:94Alcoholics 40:4 ^ 8:4 0:07 ^ 1:08 0:19 ^ 0:96
Table 2. Static accommodative function measured by an RAF rule in normal subjects and alcoholics before and after forcedabstinence
RAF rule T1a upmeasures (D)
RAF rule T2 upmeasures (D)
RAF rule T1 backmeasures (D)
RAF rule T2 backmeasures (D)
Normal subjects 5:86 ^ 2:88 5:88 ^ 2:89 5:83 ^ 2:87 5:85 ^ 2:88Alcoholics 4:65 ^ 2:23 4:60 ^ 2:22 4:60 ^ 2:31 4:61 ^ 2:34
aT1 measures were made on admission and T2 measures after abstinence.

Measurement of accommodative function in age-matched
control group
For the controls, RAF rule measures produced average
values of 5:86 ^ 2:88 and 5:83 ^ 2:87 D (mean ^ SD) for
the forward and back responses, respectively, with median
values of 6.30 D in each case. A range of average values
from 1.2 to 10 D was encountered (Figure 1B). The variance
across measures did not exceed 0.5 D (average 7%) for
any individual subject. As assessed using a Badal-type
optometer, rather lower average values of 4:6 ^ 2:3 D
were obtained (Table 3), because of the upper limit to the
optometer measures of 8 D. The RAF rule and Badal-type
optometer thus produced statistically different measures for
the control subjects �p , 0:001; 36 DF, mean difference
1.23 D), while such a difference between measurement
techniques was not seen in the alcoholic group.
The measured amplitude of accommodation in the control
group decreased as a function of age (Figure 2B), with the
age-dependent decline being estimated with a simple linear
regression model to be 20.332 ^ 0.015 D/decade (mean ^
SE of estimate, p , 0:001; F ratio 477.461, r2 � 0:932�:
Re-assessments of accommodative function in alcoholics
and control subjects
All of the alcoholics were re-assessed after a 7-day period
of abstinence and the control subjects were also
re-assessed after a similar time period. There was no statistical
difference �p � 0:908; Student's t-test for paired samples) in
the measures for the alcoholics when the results at T1 and
T2 were compared from the RAF rule (Table 2) or Badal-
type optometer (Table 3).
A similar constancy was also found for the control
subjects at T1 and T2 (Tables 2 and 3) with, for example,
the measures with the RAF rule not being different �p �0:971; Student's t-test for paired samples).
Comparison of accommodative function in alcoholic to age-
matched control subjects
The age-dependent decline in static accommodative
function, as assessed with an RAF rule, was signi®cantly smal-
ler �p , 0:001� in the alcoholics compared to their age-
matched paired controls (Figure 3). Both the alcoholics and
controls had close to zero amplitudes at $50 years of age. The
overall difference between the entire group of alcoholics and
their age-matched controls is shown as a box plot in Figure
3A. The median values are clearly different (at 4.80 and
6.30 D for alcoholics and age-matched normals). While
the inter-quartile intervals do overlap substantially, the
two sets of data were signi®cantly different when compared
by the Mann±Whitney U test �U � 503:500; p � 0:050�and a Chi-square across measures analysis was also signi®-
cant �x � 3:833�: When the RAF rule accommodation
200 Ophthal. Physiol. Opt. 2001 21: No 3
Table 3. Static accommodative function measured by a Badal-type optometer in normal subjects and alcoholics before and afterforced abstinence
BADAL T1a upmeasures (D)
BADAL T2 upmeasures (D)
BADAL T1 backmeasures (D)
BADAL T2 backmeasures (D)
Normal subjects 4:63 ^ 2:32 4:64 ^ 2:32 4:63 ^ 2:32 4:64 ^ 2:32Alcoholics 4:02 ^ 2:59 4:16 ^ 2:53 3:97 ^ 2:63 4:15 ^ 2:55
aT1 measures were made on admission and T2 measures after abstinence.
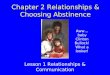
Figure 1. Distribution of measures of static amplitude of accommodation (up measures) in alcoholic subjects (A)and control subjects (B) at ®rst assessment (T1).

measures for the alcoholic and control group were compared
using a Student's t-test at either T1 or T2, a signi®cant
difference was also found �p , 0:025�; but the set of control
data was not as uniformly distributed as in the alcoholic
group (KS p . 0:1� and so less reliance can be placed on
this statistical test. Since the measured accommodation in
each group clearly declines to close to zero dioptres in the
®fth decade, this means that the younger alcoholics (#40
years of age) had a disproportionately lower amplitude of
accommodation than age-matched controls. This is shown in
the box plot in Figure 3B where the amplitude of accom-
modation for all the subjects in both groups #40 years �n �20� are compared. There is now essentially no overlap for
the inter-quartile intervals, and the difference is highly
statistically signi®cant �p , 0:001 Mann±Whitney U test,
p , 0:001 paired Students t-test). Within this smaller group
of 20 pairs of subjects aged #40 years, all of the pupil
diameters were $3.5 mm (see below and discussion).
Pupil diameter assessments and potential effect on RAF rule
accommodation measures
The average resting pupil diameter in the alcoholic
subjects was 4:37 ^ 0:63 mm (mean ^ SD, range 3±
5.5 mm, median 4.5 mm), while the comparative value for
the control group of subjects was 3:97 ^ 0:75 mm (range
2.5±5.5 mm, median 4.0 mm); this net difference of
0.39 mm (paired samples) was statistically signi®cant
(paired Student's t-test p 0.001, DF 36; signed rank test, p �0:003� (Table 4).
The measured resting pupil diameter values were depen-
dent on the age of the subjects for both the alcoholics
(Figure 4A) and the controls (Figure 4B). With more of
the control subjects showing small pupils (i.e. #3 mm),
the age-related decline was more substantial in the control
subjects. Regression analysis indicates an age-dependent
decline in resting pupil diameter of 0:057 ^
In¯uence of chronic alcohol abuse on static subjective accommodation function: H. Campbell et al. 201
Figure 3. Box plots to show differences between static amplitude of accommodation (up measures) in all alcoholicand control group subjects at ®rst assessment. (A) All 37 subjects, (B) subjects #40 years of age. The box showsthe median value and the 50% inter-quartile interval, while the bars show ^1.5 SD from the mean value. For thetwo plots, the abbreviations A and N indicate the alcoholic and normal control subjects, respectively.
Figure 2. Measures of static amplitude of accommodation (up measures) in alcoholic subjects (A) and controlsubjects (B) at ®rst assessment (T1) as a function of age. A very similar relationship was seen for back measuresand for both measures at second assessment (T2).

0:008 mm=year for the alcoholics, and 0:075 ^
0:008 mm=year for the controls. At T1, for example, one
of the alcoholics and six of the control group had pupil
diameters of 3 mm or less. An argument could be made
therefore that the very small pupil diameters adversely in¯u-
enced measures of static accommodation. However, exclu-
sion of those paired sets of data that included subjects with
pupil diameters of 3 mm or less, did not remove the overall
difference in RAF accommodation measures, e.g. at T1, the
amplitudes averaged 5:36 ^ 1:9 D for the alcoholics and
6:87 ^ 2:36 D for the controls. The average difference
was 21.50 D, which was statistically signi®cant (DF 28,
p , 0:001�: For those pairs of subjects aged #40 years,
all the pupil diameters were $3.5 mm, and averaged 4:73 ^
0:47 mm for the alcoholics and 4:48 ^ 0:55 mm for the
controls; the average difference of 0.25 mm was not statis-
tically signi®cant (19 DF, p � 0:116�: Similarly, if the data
from these seven pairs of individuals is excluded, the pupil
difference still exists, i.e. the pupil diameter in the alcoholic
group was marginally greater than in the controls �4:57 ^
0:53 mm vs. 4:24 ^ 0:59 mm�; the average difference
across the paired samples was 0.328 mm, which was statis-
tically signi®cant using a paired t-test (DF 28, p � 0:011�(Table 4).
Discussion
As mentioned in the introduction, the present study was
prompted by observations in optometric practice on the need
for near vision spectacle additions in alcoholic individuals.
The results do indicate that chronic alcoholics can indeed
suffer from a reduced static amplitude of accommodation.
This de®cit was reproducible in that it did not improve
following a week of abstinence from alcohol consumption.
It is acknowledged that individuals can have substantially
different alcohol clearance rates (Lands, 1998), but the time
elapsed between admission and assessment should have
been suf®cient to reduce blood alcohol to minimal levels.
For the alcoholic subjects, therefore, the impaired static
accommodation could not be obviously attributed to the
short term effects of ethanol and/or a high blood alcohol
level (BAL).
The measured amplitude of accommodation generally
starts to decline in early adolescence but various estimates
have been made to determine the rate of decline in accom-
modation with age after 25 years (Turner, 1958; Ayrshire
Study Circle, 1964; Hofstetter, 1965; Charman, 1989;
Koretz et al., 1989; Atchison, 1995; Mordi and Ciuffreda,
1998). Published data was extracted from the papers and
regression analyses performed (Table 5). A linear regression
analysis was used and although this is not considered
applicable beyond the age of about 48 years (Charman,
1989), it can be used as a way of comparing different reports
(Ramsdale and Charman, 1989). The results of these
analyses indicate that the control group in the present
study (with a rate of decline of 0.332 D/year) are generally
consistent with these previous ®ndings.
The measurements in the present study were all taken
202 Ophthal. Physiol. Opt. 2001 21: No 3
Figure 4. Measures of resting pupil diameter as a function of age in alcoholic subjects (A) and control subjects (B).
Table 4. Pupil diameters in normal subjects and alcoholics before and after forced abstinence
Subject group T1a measures(mm ^ SD)
Median T1(mm)
T1 range(mm)
T2 measures(mm ^ SD)
Median T2(mm)
T2 range(mm)
Normals 3.97 ^ 0.75 4.00 2.5±5.5 3:95 ^ 0:76 4.00 2.5±5.5Alcoholics 4.37 ^ 0.63 4.50 2.5±5.5 4:32 ^ 0:68 4.50 3.0±5.5
aT1 measures were made on admission and T2 measures after abstinence.

monocularly so as to remove the blurring effect of poor
convergence and extraocular muscle control when viewing
the target binocularly. This was done mainly because of
reports on the alteration of convergence and AC/A ratios
in relation to BAL following acute alcohol intake (Cohen
and Alpern, 1969; Hogan and Lin®eld, 1983; Wilson and
Mitchell, 1983; Hogan and Gilmartin, 1985; Miller et al.,
1986; Hill and Toffolon, 1990). Such alterations could have
an impact on binocular measures of accommodation (Miller
et al., 1985, 1986).
As noted in the introduction, a number of investigators
have considered whether chronic alcohol consumption
could cause a peripheral neuropathy, and have made studies
on the pupil or its re¯exes (Skogland, 1943; Schleyer and
Wichmann, 1961; Myers et al., 1979; Rubin et al., 1980;
Tan et al., 1984; Miralles et al., 1995). Schleyer and
Wichmann (1961) could ®nd no consistent effect of BAL
(0.6±2.4 mg/%) on pupil diameter, but do not provide
details (e.g. age) of the large group of individuals they
studied. An overall dose-dependent reduction in the overall
speed of the pupillary light re¯ex was, however, noted
(Schleyer and Wichmann, 1961). Rubin et al. (1980)
reported that the resting pupil diameter in darkness was
c.0.4 mm smaller in alcoholics compared to controls (of
6:23 ^ 0:37 mm�; and that the pupil diameter in bright
light for the alcoholics averaged 3.10 mm compared to
3.29 mm in the controls. The average age of the alcoholics
group was, however, 40 years (range 25±50 years) and the
average age in the controls was 28.5 years (range 21±40
years). Tan et al. (1984) reported that the resting pupil
diameter under ªstandard lighting conditionsº for alcoholics
(aged 40±69 years) with vagal neuropathy was 4:95 ^
0:97 mm; compared to 4:49 ^ 0:70 mm in an age-matched
group (aged 40±75 years). For another group of alcoholics
without evidence of vagal neuropathy, but some evidence of
peripheral neuropathy, the resting pupil size was smaller
than that found in controls, but this is likely due to larger
numbers of younger subjects in the control group used for
that comparison. Over the age interval of 40±50 years, the
age-related decline in pupil diameter was slightly more
pronounced in alcoholics with vagal neuropathy compared
to another group of alcoholics, but both alcoholic groups
showed similar age-dependent decline to control subjects
(that could not be statistically separated due to a rather
large variance in the data especially for the control group,
and those with vagal neuropathy). For a group of alcoholics
with evidence of peripheral neuropathy and aged 20±71
years (average 45.6 years), pupil cycling time was reported
to be signi®cantly slowed at 1286 ^ 297 ms; compared to
control values which were 1027 ^ 161 ms from a control
group aged 27±72 years (Miralles et al., 1995). The effect
was most pronounced in those alcoholics with advanced
vagal neuropathy (average 1500 ms), but in none of the
groups was resting pupil diameter provided. Such an effect
needs to be very much distinguished from the miosis and a
reduced, or totally absent pupil light re¯ex can be expected
in severe intoxication. In severely affected chronic
alcoholics Wernicke's encephalopathy may be present
(Jones et al., 1975), but the HPRG carried out interviews
with prospective subjects for the study, and eliminated all
those who may have reached this advanced stage of neural
damage. The pupil results obtained in the present study may
also be affected by the fact that most of the alcoholics
smoked very heavily during rehabilitation (Furuta and
Miyao, 1992). Notwithstanding, the ®nding of a slight
mydriasis in the alcoholics would be consistent with a slight
parasympathetic neuropathy.
Some of the resting pupil sizes encountered in the present
study were, as expected, rather small as a result of the age-
dependent decline in pupil diameter (Winn et al., 1994). The
resting pupil diameter for the subjects assessed in the present
study was found to be very slightly larger in the alcoholics,
although the pupil size during accommodation to the near
target could have been substantially different from this and
was not measured in the present studies. The age-related
change per year in pupil diameter was rather greater (at an
estimated 0.075 mm and 0.057 mm/year, for the controls
and alcoholics, respectively) compared to the 0.032 mm/
year for the age interval of 20±85 years reported by Winn
et al. (1994) at 220 cd/m2, but their regression plots do
In¯uence of chronic alcohol abuse on static subjective accommodation function: H. Campbell et al. 203
Table 5. Estimates of rate of decline in subjective amplitude of accommodation in humans between the age of 25 and 55 years:cross-sectional studies
Authors Year Amplitude at 25years of age
(D)a
Rate of decline D/year(25±55 years)b
Duane 1912 10.2 20.337 (25±50 y)Turner 1958 7.9 20.263Ayrshire Study Circle 1964 5.2 20.207 (37±52 y)Sun et al. 1988 6.6 20.17 (25±46 y)Koretz et al. 1989 8.0 20.307Mordi and Ciuffreda 1998 9.7 20.34Campbell et al. 2000 10.0 20.332
aAverage values are given for subjective (push-up) measures.bLinear regression analyses were performed for the 25±55 year age interval only, unless otherwise speci®ed.

suggest that there is a faster decline between 25 and 50
years. The size of the pupil under photopic conditions
should not affect the refraction greatly, but the depth of
®eld will alter depending on the pupil diameter (Hennessy
et al., 1976; Ward and Charman, 1985). It could be argued
that the depth of ®eld factor could have resulted in accen-
tuated amplitude of accommodation measures in those
subjects with pupil diameters of #3 mm. Comparative
analyses of just those pairs of individuals with resting
pupil diameters of $3.5 mm revealed the that the alcoholic
group still had an reduced amplitude of accommodation,
and the younger alcoholics (with larger pupils) had a greater
de®cit in accommodation.
Conclusions
The present studies indicate that chronic alcoholics,
especially if aged less than 40 years, could have a reduced
static accommodation and that this could precipitate a need
for an early near point spectacle correction, e.g. in recover-
ing alcoholics with an interest in reading or other close work
for example. While the mechanism underlying this change
cannot be de®ned from the present type of studies, the
results are consistent with alcohol abuse causing a form of
peripheral parasympathetic neuropathy.
Acknowledgements
Special thanks to the staff at the Highlands Psychiatric
Research Group (HPRG; Highland Health Board, Inverness)
for their invaluable assistance with the design and scheduling
of the present study, and to the subjects who gave of their
time to participate.
References
Atchison, D. A. (1995). Accommodation and presbyopia. Ophthal.Physiol. Opt. 15, 255±272.
Ayrshire Study Circle (1964). An investigation intoaccommodation. Br. J. Physiol. Opt. 21, 31±35.
Bennett, A. G. (1977). Methods of automated objective refraction.The Ophthalmic Optician 18 (1), 8±14.
Brown, B., Adams, A. J., Hegerstrom-Portnoy, G., Jones, R. T. andFlom, M. C. (1977). Pupil size after use of marijuahna andalcohol. Am. J. Ophthalmol. 83, 350±354.
Charman, W. N. (1989). The path to presbyopia: straight orcrooked?. Ophthalmic Physiol. Opt. 9, 424±430.
Cohen, M. M. and Alpern, M. (1969). Vergence andaccommodation. VI. The in¯uence of ethanol on the AC/A ratio.Arch. Ophthalmol. 81, 518±525.
Duane, A. (1912). Normal values of the accommodation at all ages.J. Am. Med. Assoc. 59, 1010±1013.
Furuta, M. and Miyao, M. (1992). Acute effects of tobaccosmoking on the autonomic nervous system in comparison withalcohol drinking. Jpn. J. Alcohol Drug Depend. 27, 647±656.
Goldberg, L. (1943). Quantitative studies on alcohol tolerance inman. Acta Physiol. Scand. 5 (Suppl. XVI), 5±128.
Hennessy, R. T., Iida, T., Shiina, K. and Leibowitz, H. W. (1976).
The effect of pupil size on accommodation. Vision Res. 16,587±589.
Hill, J. C. and Toffolon, G. (1990). Effect of alcohol on sensory andsensorimotor visual functions. J. Stud. Alcohol 51, 108±113.
Hindmarch, I., Bhatti, J. Z., Starmer, G. A., Mascord, D. J., Kerr, J.S. and Sherwood, N. (1992). The effects of alcohol on thecognitive function of males and females and on skills related tocar driving. Human Psychopharmacol. 7, 105±114.
Hofstetter, H. W. (1965). A longitudinal study of amplitudechanges in presbyopia. Am. J. Optom. Arch. Am. Acad. Optom.42, 3±8.
Hogan, R. E. and Lin®eld, P. B. (1983). The effects of moderatedoses of ethanol on heterophoria and other aspects of binocularvision. Ophthal. Physiol. Opt. 3, 21±31.
Hogan, R. E. and Gilmartin, B. (1985). The relationship betweentonic convergence and oculomotor stress induced by alcohol.Ophthal. Physiol. Opt. 5, 43±51.
Jones, B. P., Moskowitz, H. R., Butters, N. and Glosser, G. (1975).Psychophysical scaling of olfactory, visual, and auditorystimuli by alcoholic Korsakoff patients. Neuropsychologia 13,387±393.
Koretz, J. F., Kaufman, P. L., Neider, M. W. and Goeckner, P. A.(1989). Accommodation and presbyopia in the human eye Ðaging of the anterior segment. Vision Res. 29, 1685±1692.
Lands, W. E. M. (1998). A review of alcohol clearance in humans.Alcohol 15, 147±160.
Levett, J. and Karras, L. (1977). Effects of alcohol on humanaccommodation. Aviat. Space Environ. Med. 48, 434±437.
Miller, R. J., Pigion, R. G. and Martin, K. D. (1985). The effects ofingested alcohol on accommodation. Percept. Psychophys. 37,407±414.
Miller, R. J., Pigion, R. G. and Takahama, M. (1986). The effects ofingested alcohol on accommodative, fusional, and darkvergence. Percept. Psychophys. 39, 25±31.
Miralles, R., Espadaler, J. M., Navarro, X. and RubicËs-Prat, J.(1995). Autonomic neuropathy in chronic alcoholism:evaluation of cardiovascular, pupillary and sympathetic skinresponses. Eur. Neurol. 35, 287±292.
Mordi, J. A. and Ciuffreda, K. J. (1998). Static aspects ofaccommodation: age and presbyopia. Vision Res. 38, 1643±1653.
Myers, W., Willis, K. and Reeves, A. (1979). Absence ofparasympathetic denervation of the iris in alcoholics. J. Neurol.Neurosurg. Psychiatry 42, 1018±1019.
Nutt, D. J. and Peters, T. J. (1994). Alcohol: the drug. Br. Med.Bull. 50, 5±17.
Ramsdale, C. and Charman, W. N. (1989). A longitudinal study ofthe changes in the static accommodation response. Ophthal.Physiol. Opt. 9, 255±263.
Rubin, L. S., Gottheil, E., Roberts, A., Alterman, A. and Holstine,J. (1980). Effects of alcohol on autonomic reactivity inalcoholics. Pupillometric studies. III. J. Stud. Alcohol 41,611±622.
Schleyer, F. and Wichmann, D. (1961). StatistischeUntersuchungen uber die Beziehungen zwischenBlutalkoholgehalt und Pupillenweite und Lichtreaktion.Blutalkohol 1, 58±67.
Skogland, C. R. (1943). On the in¯uence of alcohol in the pupillarylight re¯ex in man. Acta Physiol. Scand. 6, 94±96.
Stapleton, J. M., Guthrie, S. and Linnoila, M. (1986). Effects ofalcohol and other psychotropic drugs on eye movements:relevance to traf®c safety. J. Stud. Alcohol 47, 426±432.
Sun, F., Stark, L., Nguyen, A., Wong, J., Lakshminarayanan, V.and Mueller, E. (1988). Changes in accommodation with age:static and dynamic. Am. J. Optom. Physiol. Opt. 65, 492±498.
204 Ophthal. Physiol. Opt. 2001 21: No 3

Tan, E. T. H., Lambie, D. G., Johnson, R. H. and Whiteside, E. A.(1984). Parasympathetic denervation of the iris in alcoholicswith vagal neuropathy. J. Neurol. Neurosurg. Psychiatry 47,61±64.
Turner, M. J. (1958). Observations on the normal subjectiveamplitude of accommodation. Br. J. Physiol. Opt. 15, 70±100.
Ward, P. A. and Charman, W. N. (1985). Effect of pupil size onsteady state accommodation. Vision Res. 25, 1317±1326.
Watten, R. G. and Lie, I. (1996). Visual functions and acuteingestion of alcohol. Ophthal. Physiol. Opt. 16, 460±466.
Wegner, A. J. and Fahle, M. (1999). Alcohol and visualperformance. Prog. Neuro-Psychopharmacol. Biol. Psychiatry23, 465±482.
Wilson, G. and Mitchell, R. (1983). The effect of alcohol onthe visual and ocular motor systems. Aus. J. Ophthalmol. 11,315±319.
Winn, B., Whitaker, D., Elliott, D. B. and Phillips, W. J. (1994).Factors affecting light-adapted pupil size in normal humansubjects. Investig. Ophthalmol. Vis. Sci. 35, 1132±1137.
Yersin, B., Nicolet, J-F., Decrey, H., Burnier, M., van Melle, G.and Pecoud, A. (1995). Screening for excessive alcoholdrinking. Comparative value of carbohydrate-de®cienttransferrin, gamma-glutamyl transferase, and mean corpuscularvolume. Arch. Intern. Med. 155, 1907±1911.
In¯uence of chronic alcohol abuse on static subjective accommodation function: H. Campbell et al. 205