Embed Size (px)
Citation preview

Infectious Crystalline Keratopathy Caused by Gram-negative Bacteria
TIMOTHY T. KHATER, MD, PHD, DAN B. JONES, MD, AND KIRK R. WILHELMUS, MD
• PURPOSE: To identify the characteristics and outcomes of infectious crystalline keratopathy caused by gram-negative bacteria. • METHODS: We reviewed all patients treated at a university eye center for infectious crystalline keratopathy from 1978 through 1995 and performed a nested case-comparison study by comparing patients with keratitis caused by gram-negative rods and those with keratitis caused by gram-positive cocci. • RESULTS: Eighteen patients (mean age ± SD, 59 ± 17 years) displayed unilateral culture-positive infectious crystalline keratopathy. Among 18 eyes with crystalline keratopathy, five occurrences (28%) were caused by gram-negative rods (Acine-tobacter Iwoffi, Citrobacter koseri, Enterobacter aerogenes, Pseudomonas aeruginosa, and Steno-trophomonas maltophilia), 10 (55%) were caused primarily by gram-positive cocci, and three (17%) were caused primarily by yeasts. Four cases grew two different isolates. No significant difference in predisposing factors, clinical appearance, or visual outcome was found between infections caused by gram-negative bacteria and those caused by gram-positive bacteria. • CONCLUSIONS: Gram-negative bacteria can cause infectious crystalline keratopathy but have no distinguishing features from infectious crystal-
Accepted for publication Jan 24, 1997. From the Cullen Eye Institute and the Sid W. Richardson Ocular
Microbiology Laboratory, Department of Ophthalmology, Baylor College of Medicine, Houston, Texas. This study was supported in part by Research to Prevent Blindness, Inc, New York, New York. Dr Wilhelmus is a Research to Prevent Blindness Senior Scientific Investigator.
Reprint requests to Kirk R. Wilhelmus, MD, Cullen Eye Institute, 6501 Fannin St, Houston, TX 77030; fax: (713) 798-4142; e-mail: kirkw® bcm.tmc.edu or [email protected]
line keratopathy caused by streptococci and other gram-positive bacteria. Appropriate laboratory evaluation is therefore necessary to guide specific antimicrobial therapy.
NFECTIOUS CRYSTALLINE KERATOPATHY IS A MINIMAL-
ly inflammatory infection in which colonies of microorganisms produce branching crystalline
opacities within the corneal stroma.1 Bacterial corne-al infections are commonly associated with an acute suppurative reaction, but most eyes with infectious crystalline keratopathy are minimally inflamed. Reasons for an altered inflammatory response include topical corticosteroid use and penetrating keratoplas-ty.2'5 Viridans streptococci are the most common cause of infectious crystalline keratopathy; other bacteria and fungi have been occasionally reported, although only three previous reports identified gram-negative bacteria.6'8 We studied a series of patients with infectious crystalline keratopathy caused by various gram-negative rods and assessed the predisposing risk factors, clinical appearances, and outcomes.
PATIENTS AND METHODS
THE CHARTS OF ALL PATIENTS EXAMINED AT THE CUL-
len Eye Institute with the diagnosis of infectious crystalline keratopathy between January 1, 1978, and December 31, 1995, were reviewed. Data concerning demographics, clinical presentation, previous ocular surgery or trauma, medications, causative organisms, management, and visual outcome were recorded. Final visual acuity was measured when the patient
VOL.124, No. 1 © AMERICAN JOURNAL OF OPHTHALMOLOGY 1997;124:19-23 19
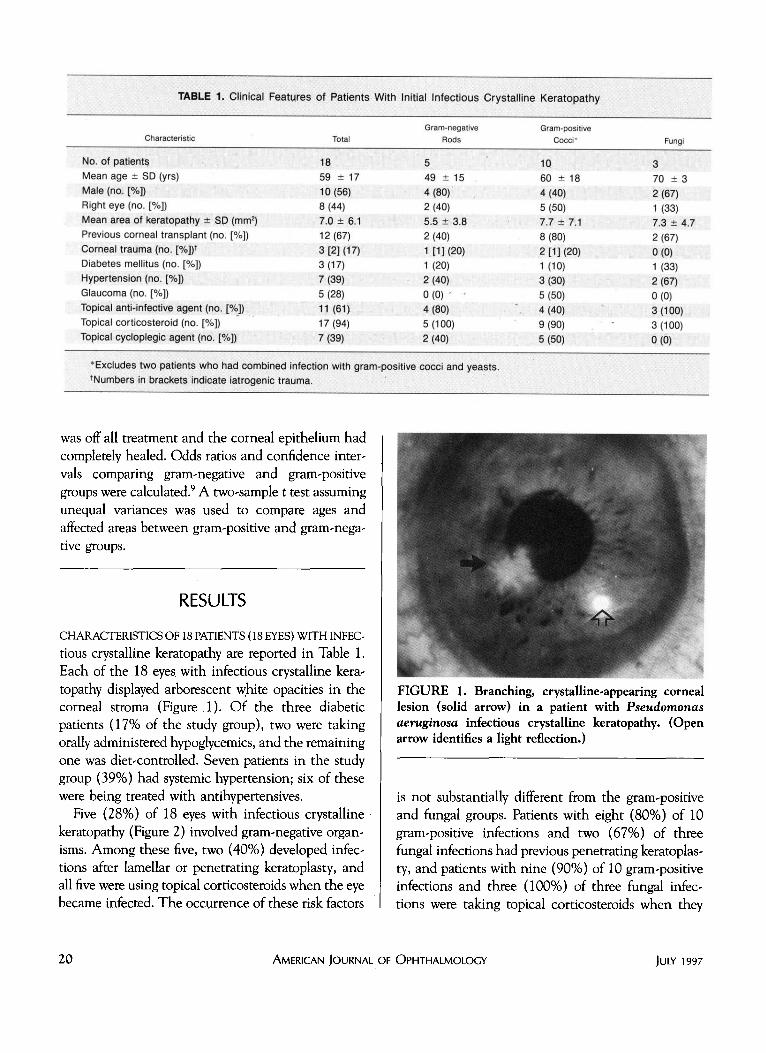
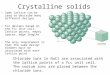
TABLE 1. Clinical Features of Patients With Initial Infectious Crystalline Keratopattiy
Characteristic Total Gram-negative
Rods Gram-positive
Cocci* Fungi
No. of patient? Mean age ± SD (yrs) Male (no. [%]) Right eye (no. [%]) Mean area of keratopathy ± SP (mm2) Previous corneal transplant (no. [%]) Corneal trauma (no. [%])* Diabetes mellitus (no. [%]) Hypertension (no. [%]) Glaucoma (no. [%]) Topical anti-infective agent (no. [%]) Topical corticosteroid (no. [%]) Topical cycloplegic agent (no. [%])
18 59 ± 17 10 (56) 8(44) 7.0 ± 6.1 12 (67) 3 [2] (17) 3(17) 7(39) 5(28) 11 (61) 17(94) 7(39)
5 49 ± 15 4 (80) 2(40) 5.5 ± 3.8 2(40) 1[1](20) 1(20) 2(40) 0 (0) " ■ 4(80) 5(100) 2(40)
1Q 60 ± 18 4(40) 5(50) 7.7 ± 7.1 8(80) 2 [1] (20) 1(10) 3(30) 5(50)
". 4(40) 9 (90) 5(50)
3 70 ± 3 2(67) 1(33) 7.3 ± 4.7 2(67) 0(0) 1(33) 2(67) 0(0) 3(100) 3(100) 0(0)
'Excludes two patients who had combined infection with gram-positive cocci and yeasts. ♦Numbers in brackets Indicate iatrogenic trauma.
was off all treatment and the corneal epithelium had completely healed. Odds ratios and confidence inter-vals comparing gram-negative and gram-positive groups were calculated.9 A two-sample t test assuming unequal variances was used to compare ages and affected areas between gram-positive and gram-negative groups.
RESULTS
CHARACTERISTICS OF 18 PATIENTS (18 EYES) WITH INFEC-tious crystalline keratopathy are reported in Table 1. Each of the 18 eyes with infectious crystalline keratopathy displayed arborescent white opacities in the corneal stroma (Figure 1). Of the three diabetic patients (17% of the study group), two were taking orally administered hypoglycemics, and the remaining one was diet-controlled. Seven patients in the study group (39%) had systemic hypertension; six of these were being treated with antihypertensives.
Five (28%) of 18 eyes with infectious crystalline keratopathy (Figure 2) involved gram-negative organisms. Among these five, two (40%) developed infections after lamellar or penetrating keratoplasty, and all five were using topical corticosteroids when the eye became infected. The occurrence of these risk factors
FIGURE 1. Branching, crystalline-appearing corneal lesion (solid arrow) in a patient with Pseudomonas aeruginosa infectious crystalline keratopathy. (Open arrow identifies a light reflection.)
is not substantially different from the gram-positive and fungal groups. Patients with eight (80%) of 10 gram-positive infections and two (67%) of three fungal infections had previous penetrating keratoplasty, and patients with nine (90%) of 10 gram-positive infections and three (100%) of three fungal infections were taking topical corticosteroids when they
20 AMERICAN JOURNAL OF OPHTHALMOLOGY JULY 1997
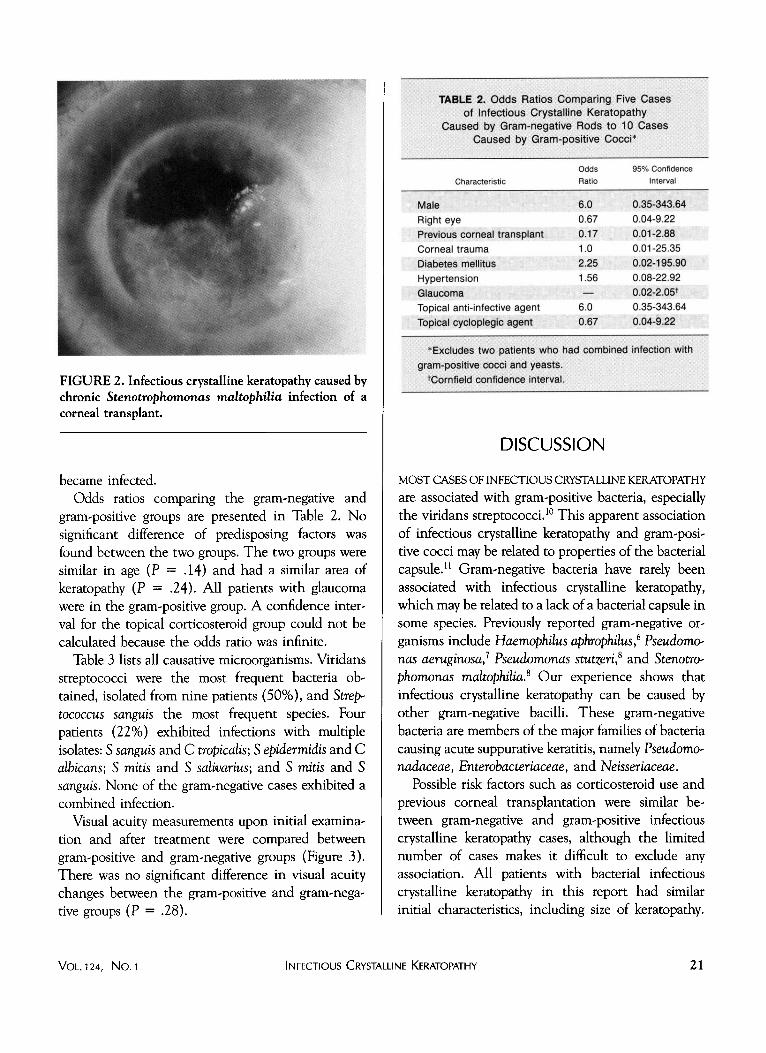
FIGURE 2. Infectious crystalline keratopathy caused by chronic Stenotrophomonas maltophilia infection of a corneal transplant.
became infected. Odds ratios comparing the gram-negative and
gram-positive groups are presented in Table 2. No significant difference of predisposing factors was found between the two groups. The two groups were similar in age (P = .14) and had a similar area of keratopathy (P = .24). All patients with glaucoma were in the gram-positive group. A confidence interval for the topical corticosteroid group could not be calculated because the odds ratio was infinite.
Table 3 lists all causative microorganisms. Viridans streptococci were the most frequent bacteria obtained, isolated from nine patients (50%), and Strep' tococcus sanguis the most frequent species. Four patients (22%) exhibited infections with multiple isolates: S sanguis and C tropicalis; S epidermidis and C albicans; S mitis and S salivarius; and S mitis and S sanguis. None of the gram-negative cases exhibited a combined infection.
Visual acuity measurements upon initial examination and after treatment were compared between gram-positive and gram-negative groups (Figure 3). There was no significant difference in visual acuity changes between the gram-positive and gram-negative groups (P = .28).
VOL.124, No. 1 INFECTIOUS CRY<
TABLE 2. Odds Ratios Comparing Five Cases of Infectious Crystalline Keratopathy
Caused by Gram-negative Rods to 10 Cases Caused by Gram-positive Cocci*
Characteristic
Male Right eye Previous corneal transplant Corneal trauma Diabetes mellitus Hypertension Glaucoma Topical anti-infective agent Topical cycioplegic agent
Odds Ratio
6.0 0.67 0.17 1.0 2.25 1.56 —
6.0 0.67
95% Confidence Interval
0.35-343.64 0.04-9.22 0.01-2.88 0.01-25.35 0.02-195.90 0.08-22.92 0.02-2.05* 0.35-343.64 0.04-9.22
* Excludes two patients who had combined infection with gram-positive cocci and yeasts.
♦Cornfield confidence Interval.
DISCUSSION
MOST CASES OF INFECTIOUS CRYSTALLINE KERATOPATHY are associated with gram-positive bacteria, especially the viridans streptococci.10 This apparent association of infectious crystalline keratopathy and gram-positive cocci may be related to properties of the bacterial capsule.11 Gram-negative bacteria have rarely been associated with infectious crystalline keratopathy, which may be related to a lack of a bacterial capsule in some species. Previously reported gram-negative organisms include Haemophilus aphrophilus,6 Pseudomcy nas aeruginosa,1 Pseudomonas stutzeri? and StenotrO' phomonas maltophilia.8 Our experience shows that infectious crystalline keratopathy can be caused by other gram-negative bacilli. These gram-negative bacteria are members of the major families of bacteria causing acute suppurative keratitis, namely PseudomO' nadaceae, Enterobacteriaceae, and Neisseriaceae.
Possible risk factors such as corticosteroid use and previous corneal transplantation were similar between gram-negative and gram-positive infectious crystalline keratopathy cases, although the limited number of cases makes it difficult to exclude any association. All patients with bacterial infectious crystalline keratopathy in this report had similar initial characteristics, including size of keratopathy.
KERATOPATHY 21
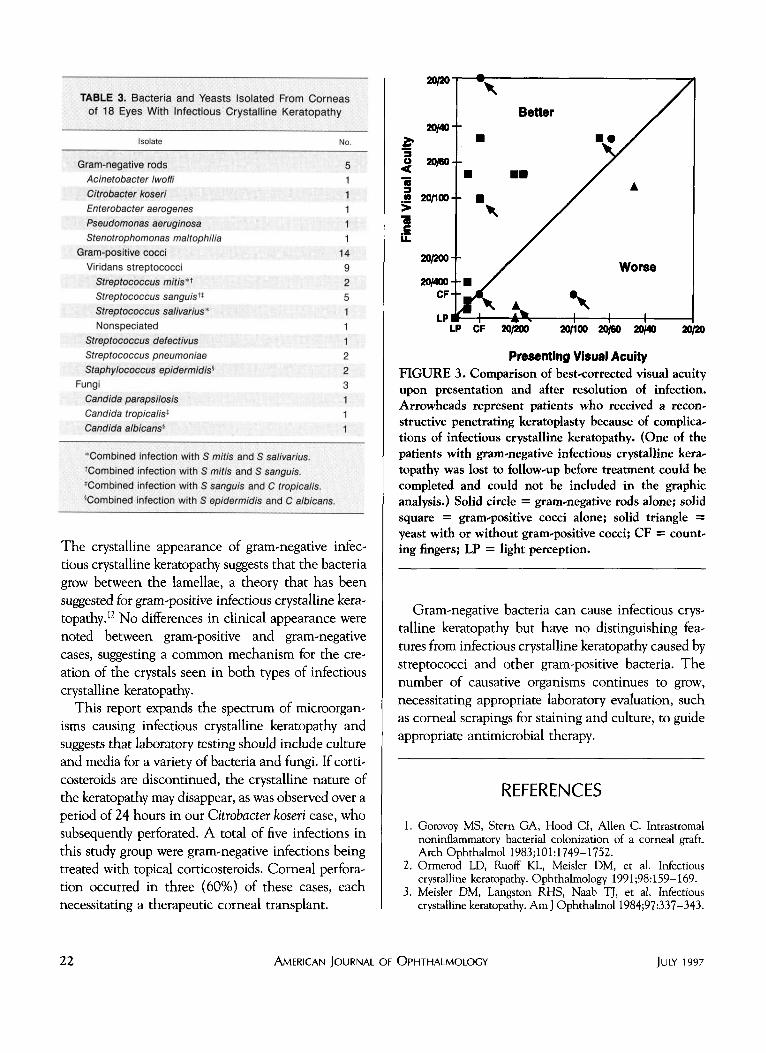
TABLE 3. Bacteria and Yeasts Isolated From Corneas of 18 Eyes With Infectious Crystalline Keratopathy
Isolate No.
Gram-negative rods Acinetobacter Iwoffi Citrobacter koseri Enterobacter aerogenes Pseudomonas aeruginosa Stenotrophomonas maltophilia
Gram-positive cocci Viridans streptococci
Streptococcus mitis** Streptococcus sanguis1* Streptococcus salivarius* Nonspeciated
Streptococcus defectivus Streptococcus pneumoniae Staphylococcus epidermidis*
Fungi Candida parapsilosis Candida tropicalis* Candida albicansi
5 1 1 1 1 1
14 9 2 5 1 1 1 2 2 3 1 1 1
'Combined infection with S mitis and S salivarius. ♦Combined infection with S mitis and S sanguis. ♦Combined infection with S sanguis and C tropicalis. 'Combined infection with S epidermidis and C albicans.
The crystalline appearance of gram-negative infectious crystalline keratopathy suggests that the bacteria grow between the lamellae, a theory that has been suggested for gram-positive infectious crystalline keratopathy.12 No differences in clinical appearance were noted between gram-positive and gram-negative cases, suggesting a common mechanism for the creation of the crystals seen in both types of infectious crystalline keratopathy.
This report expands the spectrum of microorganisms causing infectious crystalline keratopathy and suggests that laboratory testing should include culture and media for a variety of bacteria and fungi. If corti-costeroids are discontinued, the crystalline nature of the keratopathy may disappear, as was observed over a period of 24 hours in our Citrobacter koseri case, who subsequently perforated. A total of five infections in this study group were gram-negative infections being treated with topical corticosteroids. Corneal perforation occurred in three (60%) of these cases, each necessitating a therapeutic corneal transplant.
20/20"
20/40-£ 3 U 20/60-
75 3 .2 20/100-> a c i l
20/200-
20/400-CF-
LPI
V -
■ -■
- ■ X
y my d l
Better
■■
/ / /
/ /
W-
/ /
■ • / ^^v /
/ / ▲
/ r
Worse
H 1 1 LP CF 20/200 20/100 20/60 20/40 20/20
Presenting Visual Acuity FIGURE 3. Comparison of best-corrected visual acuity upon presentation and after resolution of infection. Arrowheads represent patients who received a reconstructive penetrating keratoplasty because of complications of infectious crystalline keratopathy. (One of the patients with gram-negative infectious crystalline keratopathy was lost to follow-up before treatment could be completed and could not be included in the graphic analysis.) Solid circle = gram-negative rods alone; solid square = gram-positive cocci alonej solid triangle = yeast with or without gram-positive cocci; CF = counting fingers; LP = light perception.
Gram-negative bacteria can cause infectious crystalline keratopathy but have no distinguishing features from infectious crystalline keratopathy caused by streptococci and other gram-positive bacteria. The number of causative organisms continues to grow, necessitating appropriate laboratory evaluation, such as corneal scrapings for staining and culture, to guide appropriate antimicrobial therapy.
REFERENCES
1. Gorovoy MS, Stem GA, Hood CI, Allen C. Intrastromal noninflammatory bacterial colonization of a corneal graft. Arch Ophthalmol 1983;101:1749-1752.
2. Ormerod LD, Ruoff KL, Meisler DM, et al. Infectious crystalline keratopathy. Ophthalmology 1991;98:159-169.
3. Meisler DM, Langston RHS, Naab TJ, et al. Infectious crystalline keratopathy. Am J Ophthalmol 1984;97:337-343.
22 AMERICAN JouRNAt OF OPHTHALMOLOGY JULY 1997

4. Remeijer L, van Rij G, Mooij CM, et al. Infectious crystalline keratopathy. Doc Ophthalmol 1987;67:95-103.
5. Zabel RW, Mintsioulis G, MacDonald I, Tuft S. Infectious crystalline keratopathy. Can ] Ophthalmol 1988;23: 311-314-
6. Groden LR, Pascucci SE, Brinser JH. Haemophilus aphroph.il-us as a cause of crystalline keratopathy. Am ] Ophthalmol 1987;104:89-90.
7. Hu FR. Infectious crystalline keratopathy caused by Mycobac-terium fortuitum and Pseudomonas aeruginosa. Am J Ophthalmol 1990;109:738-739.
8. Rabinowitz SM, Alfonso E, Culbertson WW, et al. Infectious crystalline keratopathy: a report of ten cases and presentation of new clinical observations. ARVO abstracts. Invest Ophthalmol Vis Sci 1989;30(3,suppl):276.
9. Herrera CR. Epidemiology analysis software programs, 3rd ed. Bethesda, Maryland: Food and Drug Administration Center for Drug Evaluation and Research, Office of Epidemiology and Biostatistics, 1989.
10. Stern GA. Infectious crystalline keratopathy. Int Ophthalmol Clin 1993;33:1-7. Matoba AY, O'Brien TP, Wilhelmus KR, Jones DB. Infectious crystalline keratopathy due to Streptococcus pneumo niae: possible association with serotype. Ophthalmology 1994;101:1000-1004. Reiss GR, Campbell RJ, Bourne WM. Infectious crystalline keratopathy. Surv Ophthalmol 1986;31:69-72.
11
12
Authors Interactive™ Comments and questions regarding this article may be addressed to authors via THE JOURNAL'S Web Site. Selected comments, questions, and author responses are posted on Authors Interactive™ at http://www.ajo.com/
VOL.124, No. 1 INFECTIOUS CRYSTALLINE KERATOPATHY 23