Embed Size (px)
Citation preview

The Laryngoscope Lippincott-Raven Publishers, Philadelphia 0 1998 The American Larvnpoloeical. Rhinological and Otologicd goci&y, Inc.
Increased Risk of Salivary Gland Tumors After Low-Dose Irradiation Baruch Modan, MD; Angela Chetrit, BSc; Esther Alfandary, RN; Arnon Tamir, MD; Ayala Lusky, MSc; Michael Wolf, MD; Ofer Shpilberg, MD
Objectiue: To assess the risk of neoplastic devel- opment among persons exposed to scalp irradiation. Study Design: Historical cohort study initially; pros- pective follow-up subsequently. Method: Two control groups-population and siblings-matched for age, sex, ethnic origin, and year of immigration. Follow-up from time of irradiation (1950s) until the end of 1991. Linkage with nationwide cancer registry. Results: A 4.5-fold incidence of cancer (P c .01) and a 2.6-fold in- crease of benign tumors were noted. The mean length of latency period until tumor development was 11 years for malignant tumors and 21.5 years for benign. A clear dose response effect for both cancer and be- nign tumors was demonstrated. Conclusions: The study confirms the role of radiation in salivary gland carcinogenesis. It indicates a need for better aware- ness, a comprehensive examination, and long-term follow-up of patients who have been subjected to head and neck radiation. Key Words: Radiation; carcinogen- esis; salivary glands; screening.
Laryngoscope, 108:1095-1097,1998
INTRODUCTION Thus far only limited studies have demonstrated that
salivary glands are radiosensitive to carcinogenesis. Chil- dren who were treated for scalp irradiation for tinea capi- tis between 1949 and 1959 have had an increased risk of head and neck tumors in general,’ and provide a good model for the assessment of this issue. The long period of follow-up since exposure enables a more thorough ap- proach to the effect on the salivary glands and particu- larly the parotis.
From the Departments of Clinical Epidemiology (B.M., A.C., E.A., A.T., A.L., o.s.) and Otorhinolaryngology-Head and Neck Surgery (M.w.), Chaim Sheba Medical Center, and The Stanley Steyer Institute for Cancer Epi- demiology and Research (B.M.), Tel Aviv University School of Medicine, Tel Hashomer, Israel.
Editor’s Note: This Manuscript was accepted for publication January 2,1998.
Send Reprint Requests to Baruch Modan, MD, Department of Clini- cal Epidemiology, Chaim Sheba Medical Center, Tel Hashomer, Israel.
PATIENTS AND METHODS The irradiated cohort included 10,834 children, 10,834 age-,
sex-, ethnic origin-matched population controls, and 5392 sib- ling controls. The age at exposure ranged from 1 to 15 years; about half were 6 to 8 years old. The sex ratio was 1:l. Irradiation was given shortly after immigration to Israel. It followed the Adamson-Kienbok technique of a five-field treatment of the scalp. Patients were irradiated by 70- to 100-kVp superficial x-ray ma- chines with a 0.5-mm aluminum filter and 1-mm aluminum half- value layer; a typical course of therapy was about 3.5 Gy in air to each field. Dosimetry was estimated retrospectively on a specially designed phantom. Total computed radiation dose to the salivary glands was 78 cGy per treatment (range, 63-286 cGy).
The vital status of the population was determined through the Central Population Registry. The only subjects who might have been lost to follow-up were those who left the country (1.9% of both cases and controls). Patients with cancer from the com- bined cases and control groups were identified through the Na- tional Cancer Registry up to December 31,1991, without knowl- edge of their previous radiation exposure. Diagnosis was ultimately checked against hospital pathology records. Further details of the methodology were described previously.2J
RESULTS Most of the malignant tumors were located at the
parotid gland, as were all the benign neoplasms. Two thirds of the malignant tumors were of the mucoepider- moid variety whereas, with the exception of two Warthin’s-type tumors, all the benign lesions were of the mixed tumor variety.
Tables I and I1 present the number and rates of sali- vary neoplasms by major type and study category. A 4.5- fold incidence of cancer (P < .01) and 2.6-fold increase of benign tumors were noted. The significantly increased risk occurred in all age groups (Table 1111, but has very wide confidence intervals and is statistically significant only among those who had been irradiated between 5 and 9 years of age. The effect seems more evident in males than in females, but again the small numbers do not allow further breakdown (data not shown).
The mean latency period until tumor development was 11 years for the malignant tumors and 21.5 years for the benign. Three of the four tumors in the control group developed between 27 and 33 years after start of follow-
Laryngoscope 108: July 1 998 Modan et al.: Salivary Gland Tumors
1095
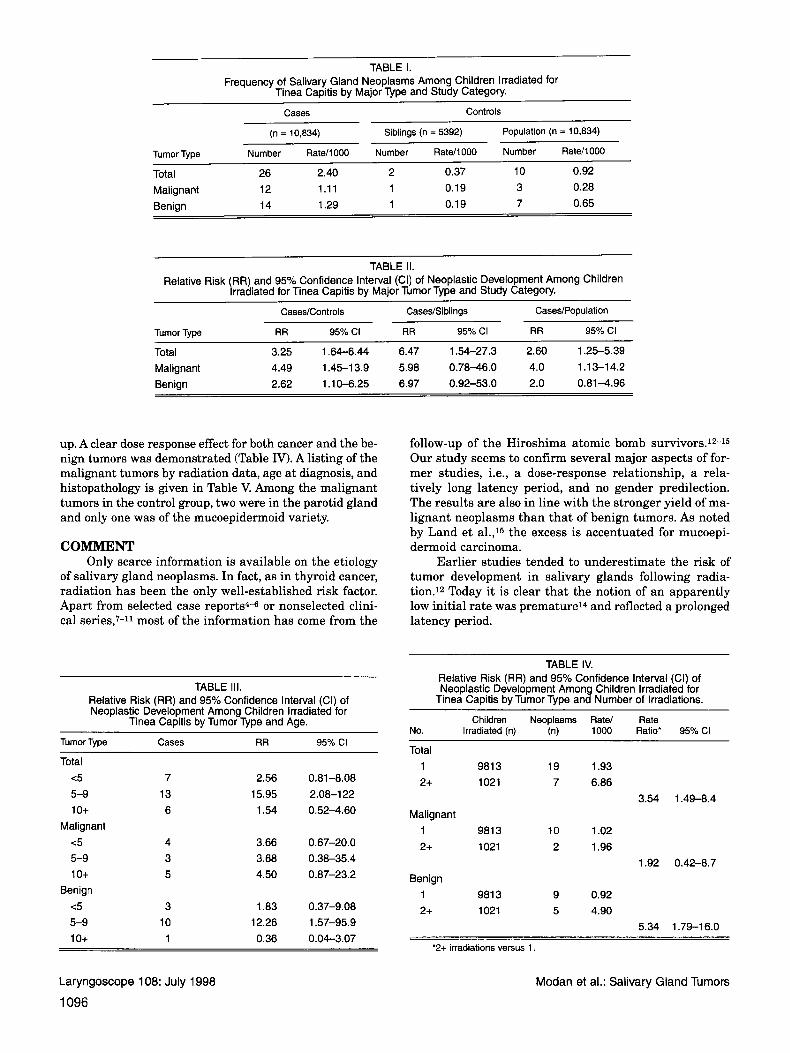
TABLE I. Frequency of Salivary Gland Neoplasms Among Children Irradiated for
Tinea Capitis by Major Type and Study Category. Cases Controls
(n = 10,834) Siblings (n = 5392) Population (n = 10,834)
Tumor Type Number Rate/1000 Number Rate/1000 Number Rate/l000
Total 26 2.40 2 0.37 10 0.92 Malignant 12 1.11 1 0.19 3 0.28 Benign 14 1.29 1 0.19 7 0.65
TABLE (I. Relative Risk (RR) and 95% Confidence Interval (CI) of Neoplastic Development Among Children
Irradiated for Tinea CaDitis bv Maior Tumor Type and Study Category. ~~
Cases/Controls CasesJSiblings Cases/Population
Tumor Type RR 95% CI RR 95% CI RR 95% CI
Total 3.25 1.64-6.44 6.47 1.54-27.3 2.60 1.25-5.39 Malignant 4.49 1.45-1 3.9 5.98 0.78-46.0 4.0 1.13-14.2 Benign 2.62 1.10-6.25 6.97 0.92-53.0 2.0 0.81-4.96
up. A clear dose response effect for both cancer and the be- nign tumors was demonstrated (Table IV). A listing of the malignant tumors by radiation data, age at diagnosis, and histopathology is given in Table V. Among the malignant tumors in the control group, two were in the parotid gland and only one was of the mucoepidermoid variety.
COMMENT Only scarce information is available on the etiology
of salivary gland neoplasms. In fact, as in thyroid cancer, radiation has been the only well-established risk factor. Apart from selected case reports4-6 or nonselected clini- cal series,7-11 most of the information has come from the
follow-up of the Hiroshima atomic bomb survivors.12-15 Our study seems to confirm several major aspects of for- mer studies, i.e., a dose-response relationship, a rela- tively long latency period, and no gender predilection. The results are also in line with the stronger yield of ma- lignant neoplasms than that of benign tumors. As noted by Land e t al.,15 the excess is accentuated for mucoepi- dermoid carcinoma.
Earlier studies tended to underestimate the risk of tumor development in salivary glands following radia- tion.12 Today it is clear that the notion of an apparently low initial rate was premature14 and reflected a prolonged latency period.
TABLE 111. Relative Risk (RR) and 95% Confidence Interval (CI) of Neoplastic Development Among Children Irradiated for
Tinea Capitis by Tumor Type and Age. Tumor Type Cases RR 95% CI
Total <5 7 2.56 0.81-8.08 5-9 13 15.95 2.08-122 1 o+ 6 1.54 0.52-4.60
Malignant <5 4 3.66 0.67-20.0 5-9 3 3.68 0.38-35.4 1 o+ 5 4.50 0.87-23.2
Benign <5 3 1.83 0.37-9.08 5-9 10 12.26 1.57-95.9 1 o+ 1 0.36 0.04-3.07
Laryngoscope 108: July 1998
1096
TABLE IV. Relative Risk (RR) and 95% Confidence Interval (CI) of Neoplastic Development Among Children Irradiated for
Tinea Capitis by Tumor Type and Number of Irradiations. Children Neoplasms Rate/ Rate
No. Irradiated (n) (n) 1000 Ratio' 95% CI
Total 1 981 3 2+ 1021
Malignant 1 9813 2+ 1021
Benign 1 981 3 2+ 1021
19 1.93 7 6.86
3.54 1.49-8.4
10 1.02 2 1.96
1.92 0.42-8.7
9 0.92 5 4.90
5.34 1.79-16.0
'2+ irradiations versus 1.
Modan et al.: Salivary Gland Tumors

TABLE V. Malignant Tumors That Developed in Individuals Subjected to Scalp Irradiation for Tinea Capitis.
Year of Irradiations Age at Age at Patient No. Sex Irradiation (n) irradiation (y) Diagnosis (y) Location Diagnosis
1 M 1955 1 6 20 Parotis Acinic cell carcinoma 2 M 1958 1 5 10 Parotis Mucoepidermoid carcinoma 3 M 1957 1 2 30 Parotis Acinic cell carcinoma 4 M 1956 1 1 1 15 Parotis Mucoepidermoid carcinoma 5 F 1958 1 4 1 1 Parotis Mucoepidermoid carcinoma 6 M 1957 2 2 23 Submandibular Mucoepidermoid carcinoma 7 M 1953 1 14 25 Minor gland Mucoepidermoid carcinoma 8 F 1959 1 4 34 Subrnandibular Mucoepidermoid carcinoma 9 M 1958 1 3 8 Parotis Mucoepidermoid carcinoma 10 M 1953 1 13 46 Parotis Adenocarcinoma 1 1 M 1955 2 13 18 Salivary gland Mucoepidermoid carcinoma 12 F 1956 1 10 27 Parotis Acinic cell carcinoma
The fact that salivary gland neoplasms may result from radiation is not surprising, because, with only minor exceptions, all body organs are susceptible. Malignant tu- mors, arising most probably from induced mutations and/or other DNA damage,l6 tend to develop earlier than the benign variety, but, needless to say, this perhaps could be just a reflection of an earlier diagnosis of a more ag- gressive disease. Alternatively, benign tumors may de- velop more insidiously. The higher yield of salivary gland cancer than that of benign lesions is also seen in other neoplastic sites, with the exception of meningiomas.3
The long latency period in the benign tumors may possibly explain the higher risk observed in this neoplas- tic category in the 5- to 9-year age group; i.e. a faster di- agnosis in persons in their mid-20s than in their teens. Yet we noticed a similar effect in the risk of breast cancer,l so that a higher susceptibility before puberty cannot be ruled out.
Finally, this report indicates once more the need for greater awareness, comprehensive examination and long- term follow-up of patients who have been subjected to head and neck radiation, in order to enable a n early diag- nosis of tumor development.17
BIBLIOGRAPHY 1. Modan B, Chetrit A, Alfandary E, Katz L. Increased risk of
breast cancer following low dose irradiation. Lancet 1989;l: 629-31.
2. Modan B, Baidatz D, Mart H, Steinitz R, Levin SG. Radiation induced head and neck tumors. Lancet 1974;1:277-9.
3. Ron E, Modan B, Boice J D Jr, et al. Tumors of the brain and nervous system after radiotherapy in childhood. N Engl J Med 1988;319:1033-9.
4. Rodriguez-Cuevas S, Ocampo LB. A case report of mucoepider- moid carcinoma of the parotid gland developing after ra- dioiodine therapy for thyroid carcinoma. Eur J Surg Oncol 1995;21:692.
5. Spraggs PD, Rose DS, Grant HR, Gallimore AP. Post-irradia- tion carcinosarcoma of the parotid gland. J Laryngol Otol
6. Warfield AT, Smallman LA. Simultaneous bilateral pleomor- phic adenomas of the parotid glands with unilateral tyro- sine rich crystalloids. J Clin Pathol 1994;47:362-4.
7. Saeger EL, Silverman FN, Sterling TD, Turner ME. Neopla- sia following therapeutic irradiation for benign conditions in childhood. Radiology 1960;74:889.
8. Shore-Freedman E, Abrahams C, Recant W, Schneider AB. Neurilemomas and salivary gland tumors of the head and neck following childhood irradiation. Cancer 1983;51: 2159-63.
9. Hempelmann LH, Pifer JW, Burke GH, Terry R, Ames WR. Neoplasms in persons treated with X-rays in infancy for thymic enlargement: a report of the third follow-up survey. J Natl Cancer Inst 1967;38:317-41.
10. Ju DMC. Salivary gland tumors occurring after radiation to the head and neck area. Am J Surg 1968;116:518-23.
11. Swelstad JA, Scanion EF, Ovledo MA, Hugo NE. Irradiation- induced polyglandular neoplasia of the head and neck. Am J Surg 1978;135:820-4.
12. Belsky JL, Tachikawa K, Cihak W, Yamamoto T. Salivary gland tumors in atomic bomb survivors. Hiroshima-Na- gasaki, 1957 to 1970. JAMA 1972;219:864-8.
13. Takeichi N, Hirose F,Yamamoto H, Ezaki H, Fujikura T. Sali- vary gland tumors in atomic bomb survivors. Hiroshima, Japan. 11. Pathologic study and supplementary epidemio- logic observations. Cancer 1983;52:377-85.
14. Saku T, Hayashi Y, Takahara 0, et al. Salivary gland tumors among atomic bomb survivors, 1950-1987. Cancer 1997;
15. Land CE, Saku T, Hayashi Y, et al. Incidence of salivary gland tumors among atomic bomb survivors, 1950-1987. Evalua- tion of radiation-related risk, Radiat Res 1996; 146:28-36.
16. Upton AC. Biological aspects of radiation carcinogenesis. In: Boice JD Jr, Fraumeni JF Jr, eds. Radiation Carcino- genesis: Epidemiology and Biological Significance. New York: Raven Press;1984:9-19.
17. Schneider AB, Favus MJ, Stachura ME, Arnold MJ, Frohman LA. Salivary gland neoplasms as a late conse- quence of head and neck irradiation. Ann Intern Med 1977;87:160-4.
1994; 108~443-5.
79:1465-75.
Laryngoscope 108: July 1998 Modan et al.: Salivary Gland Tumors
1097





























