Embed Size (px)
Citation preview

Christopher J. Colburn, MEng, CSP, CHMM
Manager, Environmental, Health and Safety – North America
Incident Investigation using Incident Trisection Techniques / Lean / Six Sigma Tools
1
Session Objectives
Define and Discuss Safety I versus Safety II thinking and its application to Incident Investigations
Define and Discuss Incident Trisection, Causal and Contributing Factors
Demonstrate the application of Ishikawa Diagrams, Root Cause Analysis, Countermeasure Identification and Implementation
Discuss the concept of organizational drift and methods to Manage to Smart, Sustainable Solutions

2
Safety – What it is really?
What is the definition of “Safety?”
– “Freedom from Unacceptable Levels of Risk” – ISO Guide 51:1999E / ANSI Z10-2012
– “Safety is not the absence of events; safety is the presence of defenses” – Todd Conklin, Pre-Accident Investigation

3
Hazards – Have the potential to cause harm
Swiss Cheese Model James Reason
Swiss Cheese Model

4
Accident Pyramid
Hazardous Energy
Threat/Target Initiating Mechanism
“If you wish to understand the Universe, think of energy, frequency and vibration”
~ Nikola Tesla
“Energy can be neither created nor destroyed. However, energy can change forms, and energy can flow from one place to another.” – First Law of Thermodynamics

5
Accident Pyramid
Hazardous Energy
Threat/Target Initiating Mechanism

6
Accident Pyramid
Hazardous Energy
Threat/Target Initiating Mechanism

7
Accident Pyramid
Hazardous Energy
Threat/Target Initiating Mechanism

8
…safety is not something you have, it’s something you do.
Change Adaptation

9
Safety I Vs. Safety II 9
Intervene by changing people
Safety is best measured by its absence
Safety is a bureaucratic accountability
up
People are a problem to
control
Safety I Safety II
Versus

10
Operational Mismatch
Blunt End – MGT/ Support
Sharp End – Operations
Work Imagined Work Completed
VP/GM Director Manager Supervisor Crew Chief Line Worker
Resource Availability
Resource Effect

11
Incident Trisection
What is an Incident? – Simply Stated and Incident is a “Unexpected Outcome” as
the result of an event or sequence of events
What is Incident Trisection – Breaking the incident down into three distinctive and
digestible portions in order to learn and grow 1. Context 2. Consequence 3. Retrospect

12
Incident Trisection
Context Consequence Retrospect
Incident
13
Context
All the “Stuff” that occurred leading up to the incident – Consider everything that occurred up to 72 hours before the
incident – Identify and categorize these things as either:
– Causal Factors – Contributing Factors
Context

14
Key Definitions
Causal Factor: “A condition or an event that results in an effect (anything that shapes or influences the outcome).”
Causal Factor Chain: “A cause and effect sequence in which a specific action creates a condition that contributes to or results in an event. Earlier events in a sequence are called “upstream” factors”
Direct Cause: “The cause that directly resulted in the occurrence.”
Contributing Cause: “A cause that contributed to an occurrence but, by itself, would not have caused the occurrence.”
Root Cause: “The cause that, if corrected, would prevent recurrence of this and similar occurrences. It is the most fundamental aspect of the cause that can logically be identified and corrected.”
Source: DOE-NE-STD-1004-92

15
Consequence
Rarely that interesting
Consequence
16
Retrospect
There is rarely the opportunity that a good worker made a bad decision that led to error. In retrospect, every error appears to be a choice but that is often incorrect. The outcome is agnostic to the cause when variability
manifests itself in the system Confirmation Bias
Retrospect

17
Accident Investigation
1.Focus on understanding the context of the incident • Understand how things normally work
to understand how it didn’t work this time
• Why do the decisions make sense in context? (local rationality)
2.Remove blame from the process • Accountability should be forward-
looking 3. Learning Teams
22

18
Learn and Grow
“Once you begin to Blame and Punish, you forfeit the opportunity to Learn and Grow.”
~ Todd Conklin

19 19
Step 1 - Clarify the Problem

20 20
Step 2 – Short Term Containment
Need to identify if there are any short term containment actions that need to be put in place to protect employees. When creating the short term containment plan, be sure to clearly identify who, will do what, and when.
Short Term Containment:

21 21
Steps 3 & 4 – POC & CS Determine the Point of Cause & State the Current Situation

22 22
Steps 3 & 4 – POC & CS Determine the Point of Cause & State the Current Situation

23 23
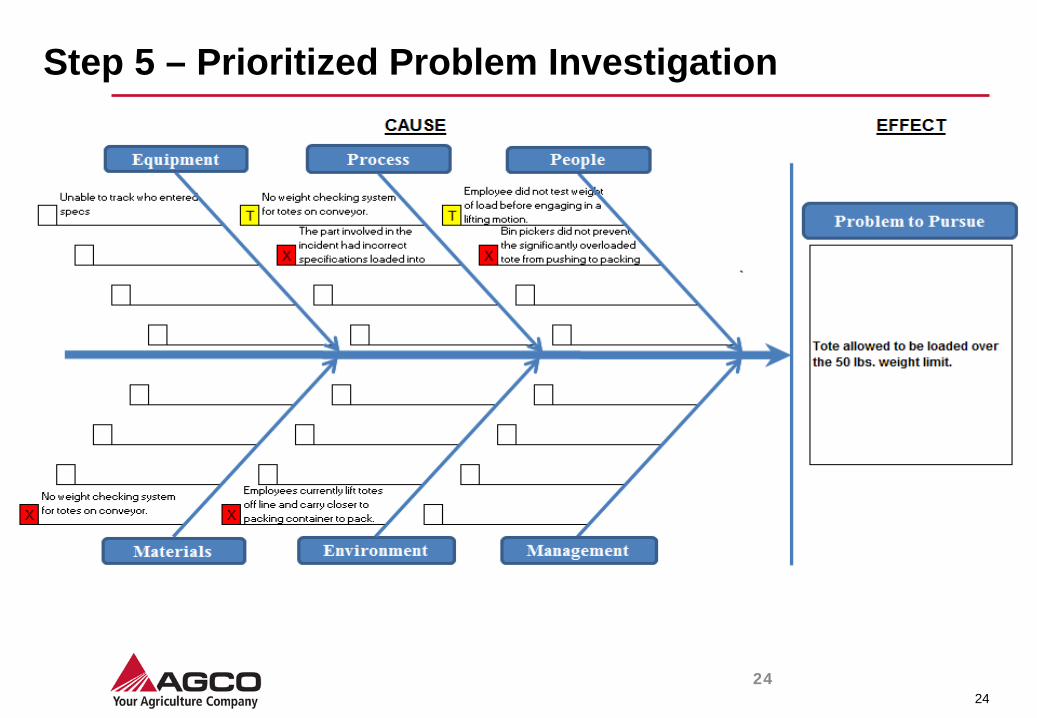
Step 5 – Prioritized Problem Investigation
Without any prejudice:
Examine the Point of Cause and determine possible causes without prejudice
• Utilize your experiences and intuition as a reference when you make considerations.
• Make determinations based on facts. • While listening to others clarify whether you are hearing an opinion or actual facts
How to Perform this Step: • Do the exercise twice, once on your own, and another at the Gemba w/
the Experts. • Avoid “Leading Questions”
24 24
Step 5 – Prioritized Problem Investigation

25 25
Step 5 – Prioritized Problem Investigation Examine the Point of Cause and determine possible causes without prejudice
Go and See to Confirm
Possible Causes
Problem to Pursue
26 26
WHY
Potential Cause
Potential Cause
Actual Cause
Potential Cause
Actual Cause
Potential Cause
Potential Cause
Potential Cause
Actual Cause
Potential Cause
Root Cause
WHY
WHY
WHY
Possible Cause
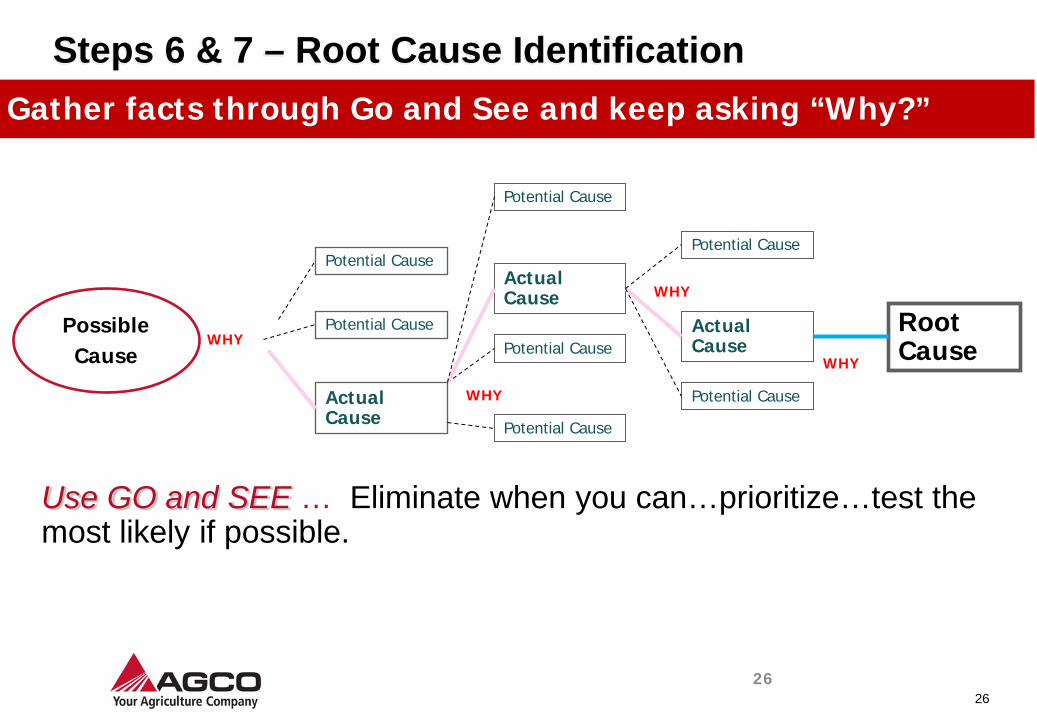
Steps 6 & 7 – Root Cause Identification Gather facts through Go and See and keep asking “Why?”
Use GO and SEE … Eliminate when you can…prioritize…test the most likely if possible.

27 27
Step 6 & 7 – Root Cause Identification
Maintenance team member did not properly secure Why?
Example : Bolts are loose
Why?
: Supervisor does not have good understanding : Supervisor lacks power of concentration
Specify the root cause
Team member did not follow standard work
Team member had not been trained on standard work
Why?
Why?
Why?
Maintenance supervisor forgot to train
No standard training checklist to follow

28 28
Step 6 & 7 – Root Cause Identification
Check if it truly IS the root cause
Specify the root cause
• If Countermeasure is taken for the cause, we can expect the Problem to Pursue at the Point of Cause to be solved and the same result to be achieved consistently.
• The Possible Root Cause can be connected to the previous cause with the word “Therefore” eventually reaching the Prioritized Problem at the Point of Occurrence.

29 29
Root Cause Identification
Problem
Possible Cause
Cause
Cause
Cause
Root Cause?
Why? Why?
Why?
Why?
Cause >> Effect Relationships
Therefore Test
Problem to Pursue @ the Point of
Cause
30 30
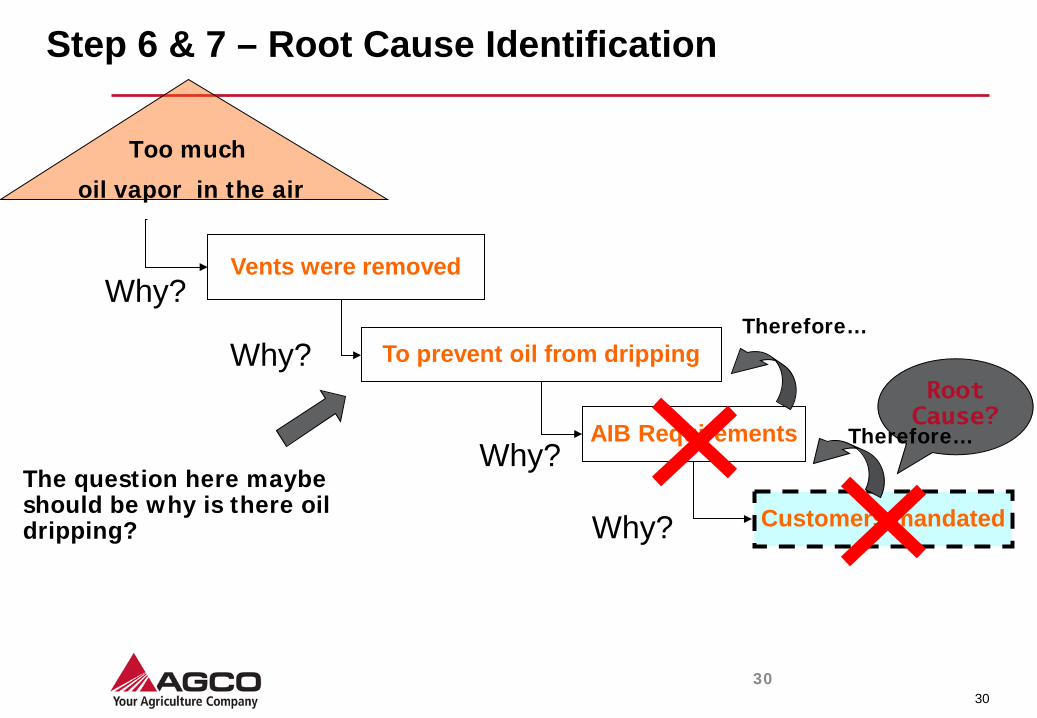
Step 6 & 7 – Root Cause Identification
Too much
oil vapor in the air
Vents were removed
To prevent oil from dripping
AIB Requirements
Customers mandated
Root Cause?
Why?
Why?
Why?
Why? Therefore…
Therefore…
The question here maybe should be why is there oil dripping?

31 31
Step 6 & 7 – Root Cause Identification

32 32
Step 8 – Countermeasure Evaluation
Temporary Countermeasure Reverse a negative situation, establish containment
or temporarily return to normal or standard
Countermeasure By addressing Root Cause, prevents problem from
recurring

33 3/4/2010
Step 8 – Counter Measure - Hierarchy of Controls
1. Elimination 2. Substitution 3. Engineering Controls 4. Warnings 5. Administrative Controls 6. Personal Protective Equipment
• Design to eliminate hazards, such as falls, hazardous materials, noise, confined spaces, and manual material handling
• Substitute for less hazardous material • Reduce energy. For example: Lower speed, force,
amperage, pressure, temperature, and noise.
• Ventilation systems • Machine guarding • Sound enclosures • Circuit breakers • Platforms and guard railing • Interlocks • Lift tables, conveyors, and balancers
• Signs • Backup alarms • Beepers • Horns • Labels
Procedures
• Safe job procedures • Rotation of workers • Safety equipment inspections • Changing work schedule
Training • Hazard Communication Training • Confined Space Entry
• Safety glasses • Hearing protection • Face shields • Safety harnesses and lanyards • Gloves • Respirators
CONTROLS EXAMPLES
Most Effective
Least Effective

34 34
Step 8 – Countermeasure Evaluation Build consensus with others
Build consensus with related people and departments to achieve an increased level of speed and smoothness. Share your findings and your problem solving report including target.
•Explain and discuss plans with all relevant people at the planning stage.
•Set up a committee for planning purpose.
•Hold the meeting to collect opinions.
•Always share latest status/information.
Build consensus with others
35 35
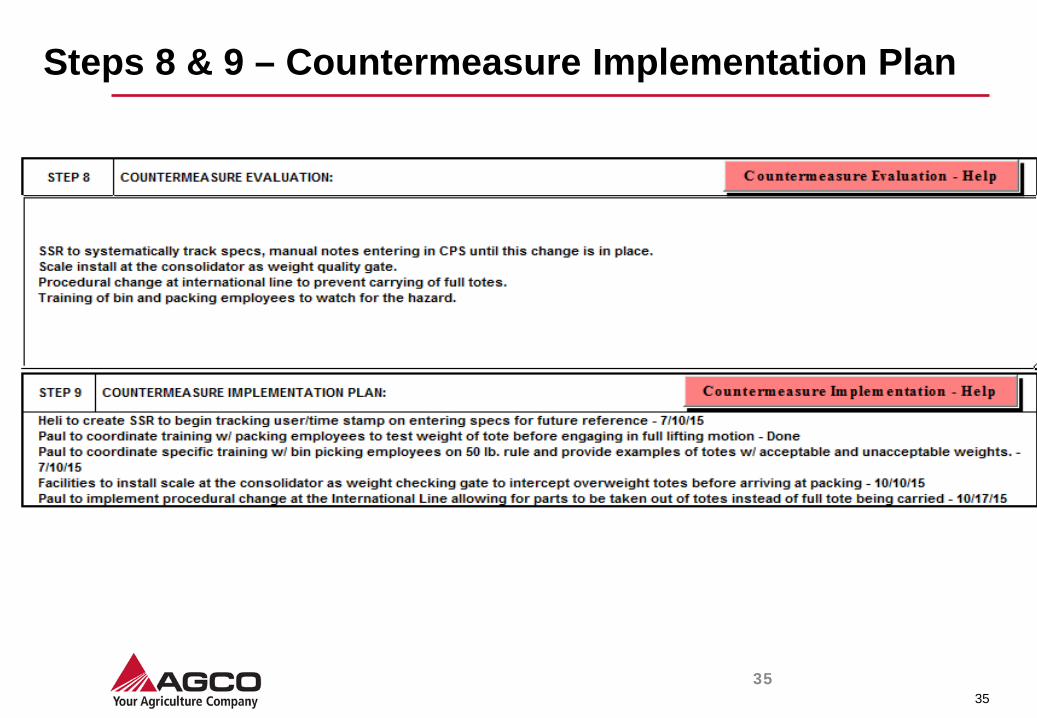
Steps 8 & 9 – Countermeasure Implementation Plan

36 36
Step 10 – Check Countermeasures
Evaluate whether or not the target was achieved
Evaluate the results
Was the target achieved?
Evaluate the process
Did we follow the 11 steps?
Did we follow the process outlined in our countermeasure?
Confirm positive and negative effects incidental to results
Evaluate results and processes, and share it with members involved

37 37
Step 11 - Standardize and Share
Examples of standardization
Forms Manual Checklists Flow-chart
If possible, the standard should clarify all relevant factors so that anyone, at anytime, without waste can implement the standard
Set successful processes as new standards
42
In Conclusion….
“No question is so difficult to answer as that to which the answer is obvious.”
~ George Bernard Shaw 1856-1950

43
Christopher J. Colburn, MEng, CSP, CHMM
AGCO Corporation Manager, EHS – North America
Region IV VPPPA Board of Directors – Treasurer Elect [email protected]
Cell: 404-353-4626





























