Embed Size (px)
Citation preview

CLIN. CHEM. 41/8, 1109-1114 (1995) #{149}Molecular Pathology and Genetics
CLINICAL CHEMISTRY, Vol. 41, No. 8, 1995 1109
Inborn Errors of Metabolism Diagnosed in Sudden Death Cases by AcylcarnitineAnalysis of Postmortem BileMohamed S. Rashed,’ Pinar T. Ozand,’ Michael J. Bennett,2 Jeffrey J. Barnard,2 Diddahally R. Govindaraju,3and Piero Rinaldo3’4
Fatty acid oxidation (FAO) disorders represent a fre-quently misdiagnosed group of inborn errors of metabo-lism. Some patients die at the first episode of fastingintolerance and, if appropriate investigations are notundertaken, often meet the criteria of sudden infant deathsyndrome (SIDS). To expand existing protocols for thepostmortem diagnosis of FAQ and other metabolic dis-orders, we tested the hypothesis that analysis for acyl-carnitine in bile, a specimen readily available at autopsy,may be utilized for diagnostic purposes. Using electro-spray/tandem mass spectrometry, we analyzed for acyl-carnitine postmortem bile specimens from two infantswith long-chain 3-hydroxyacyl-C0A dehydrogenase defi-ciency, one infant with glutaryl-C0A dehydrogenase de-ficiency, and 17 uninformative SIDS cases as controls.The affected cases, and none of the controls, showedmarked accumulation of C10-C18 acylcarnitines or glu-tarylcarnitine (acyVfree carnitine ratio: 5.2, 2.7, and 1.9,respectively; controls 0.2 ± 0.1). In one patient, all otherdiagnostic methods were uninformative, suggesting thatbile acylcamitine profiling could lead to identification ofpreviously overlooked cases.
Indexing Terms: pediatric chemist,y/fatty acid oxidation/glutaryl-carnitine/postmortem diagnosis/sudden infant death syndrome
Inborn errors of metabolism often present early ininfancy with life-threatening episodes of metabolic de-compensation. In view of the high mortality rate that iscommon among these disorders, sudden infant deathsyndrome (SIDS) has been sporadically associated witha number of inborn errors of amino acid and energymetabolism (1-3), including glutaryl-CoA dehydroge-nase deficiency (4)#{149}5These isolated cases probablyresult from a delayed diagnosis combined with atypicaland (or) mild clinical phenotypes, and are unlikely torepresent a significant cause of sudden infant death.On the other hand, the number of cases found to havebeen affected with a disorder of fatty acid oxidation(FAO), either postmortem or retrospectively (after the
‘King Faisa! Specialist Hospitah and Research Center, MBC3,P.O. Box 3354, Riyadh 11211, Saudi Arabia.
2University of Texas Southwestern Medicah Center, Depart-
ment of Pathology, Dallas, TX 75235.Yale University School of Medicine, Department of Genetics,
333 Cedar St., P.O. Box 208005, New Haven, CT 06520-8005.for correspondence. Fax 203-785-3535; E-mail
[email protected] abbreviations: ES!JMS-MS, ehectrospray tan-
dem mass spectrometry; FAO, fatty acid oxidation; LCHAD,hong-chain 3-hydroxyacyl-CoA dehydrogenase; and SIDS, suddeninfant death syndrome.
Received April 11, 1995; accepted May 25, 1995.
diagnosis of an affected sibling), has soared in the last10 years (4-8). On the basis of these observations, weand others have postulated that FAO disorders may beresponsible for as many as 5% of SIDS cases (6-9),possibly even more if children who die suddenly andunexpectedly in early life are considered.
After the diagnosis a decade ago of medium chainacyl-CoA dehydrogenase deficiency in a SIDS victim(10), anecdotal reports have associated at least 13 FAOdisorders with sudden unexpected death in infancy (7).Among them, long-chain 3-hydroxyacyl-CoA dehydro-genase (LCHAD) deficiency has emerged as a commondisorder and has been linked to acute fatty liver ofpregnancy (11) and multiple cases of sudden infantdeath (12, 13).
Suspicion of a possible FAO disorder is usuallyraised by the finding at autopsy of diffuse microvesicu-lar steatosis (4). A final diagnosis can be reachedthrough various biochemical, enzymatic, and molecularmethods (4, 6-8, 14), but only if fluid and tissue spec-imens are collected during autopsy for this purpose. Inour experience, this is seldom done, which possiblycontributes to the underestimation of metabolic disor-ders among sudden death cases. To increase the gen-eral awareness of these disorders, we have soughtalternative biochemical methods that are based on theconstant availability of a suitable sample other thanblood or urine, require simple preparation procedures,and allow the diagnosis of as many disorders as possi-ble on the basis of multiple independent criteria (15).
Recently, we proposed a new method based on thesimultaneous quantitative determination of C8-C18fatty acids and glucose from the methanol wash of apellet obtained by ultracentriftigation of frozen liverhomogenate (7). Our current postmortem protocol in-cludes this method, liver histology, assay of liver car-nitine, and organic acid analysis of urine when avail-able. In our collective experience, we have thus fardiagnosed postmortem >40 patients with FAO disor-ders (6-8, 16, 17; and unpublished observations); inaddition, however, we encountered several suddendeath cases that remained without a precise diagnosisdespite one or more abnormal findings. We postulatedthat our current strategy could be improved by theanalysis of bile, a specimen easily collected at autopsy,for the postmortem diagnosis of FAO and other meta-bolic disorders associated with the accumulation ofcharacteristic acyhcarrntines in blood and urine. Wereport here the preliminary results obtained in threeconfirmed cases, two of which were diagnosed atautopsy.

Conc, pmol/g prot&n
Reference valueV
8 n = 100. Source: Boles et al. (7).
nd, not detectable.
1110 CLINICAL CHEMISTRY, Vol. 41, No. 8, 1995
Materials and Methods
Case Reports
Case 1. A Caucasian male presented shortly afterbirth with severe dilated cardioinyopathy and twolife-threatening episodes of hypoglycemia. Pregnancyand delivery were unremarkable. Urine organic acidanalysis showed massive amounts of C6-C14 saturatedand unsaturated 3-hydroxydicarboxylic acids withminimal ketonuria, a pattern suggestive of LCHADdeficiency. The diagnosis of a defect in the a-subunit ofthe mitochondrial trifunctional protein, which containsLCHAD and long-chain enoyl-CoA hydratase activity,was later confirmed by assay of enzyme activities incultured fibroblasts and molecular analysis (18). At age18 months, the patient became lethargic and vomited.In spite of prompt hospitalization and close monitoring,several hours later he died suddenly and unexpectedly.
Case 2. A Caucasian male born to unrelated parents.There was no significant obstetric history, and his twoolder half-siblings are reported healthy. His clinicalcourse consisted of poor feeding, frequent vomiting,and failure to thrive. He had multiple hospitalizations,but no metabolic investigations were undertaken. Atage 3 months, he was unexpectedly found dead.
Case 3. An 8-year-old Hispanic male was diagnosedwith cerebral palsy and seizure disorder. The clinicalhistories of this patient and of his three siblings, whoreportedly have similar manifestations, are not avail-able. The patient died suddenly and unexpectedlyshortly after being admitted to a hospital for evalua-tion of a non-life-threatening condition (persistent ab-dominal distension).
Controls
As part of a large-scale retrospective study, >450sudden death cases investigated by the Office of theMedical Examiner of the State of Maryland were testedfor a possible FAO disorder (7, 15, and RG Boles et al.,unpublished results). Seventeen SIDS cases who testednegative in all the investigations performed (review ofliver histology, metabolite profile of liver homogenate,and assay of liver carnitine) were randomly chosen onthe basis that a bile specimen was available. Theanalysis of postmortem liver, bile, and urine specimensfor diagnostic purposes was approved by the YaleUniversity human investigation committee (HIC no.05125).
Acylcarnitine Analysis
Bile specimens (-50-100 L) were spotted ontofilter paper (no. 903; Schheicher and Schuell, Dassel,Germany), allowed to dry overnight, and stored atroom temperature in polypropylene bags at room tem-perature until analysis. Two 3/16-in. (--5-mm)-diame-ter circles were punched out from the spot and ex-tracted as previously described (19). Qualitativeprofiles of acylcarnitine methyl or butyl esters wereobtained by electrospray tandem mass spectrometry(ESL’MS-MS) by monitoring precursor-ion scans of the
common fragment at m/z 99 (methyl-) or m/z 85 (n-butyl-) of acylcarnitine derivatives with a VG QuattroESJJMS-MS system (Fisons, Altrincham, UK) equippedwith a Jasco PU-980 HPLC pump and a Jasco AS-950autosampler (Jasco International, Tokyo, Japan) (20).
Other Methods
Total and free carnitine were measured in perfusate
and supernatant of liver homogenate samples by aradioenzymatic assay (21), with some modifications.Bile specimens (50 .iL) were incubated with 50 L ofcholestyramine (50 g/L, 30 min at room temperature)and subsequently diluted 10-fold with deionized waterto prevent bile acid inhibition of carnitine acetyltrans-ferase (22). The extremely high values of esterifiedcarnitine in patients’ bile samples were confirmed atseveral dilutions (up to 30-fold) and verified by adifferent method (23). C5-C18 fatty acids and glucosewere determined in liver homogenate as previouslydescribed (7). Activities of LCHAD and three othermitochondrial enzymes measured as controls in liverhomogenate were assayed by spectrophotometric meth-ods (24). Urine organic acids were separated by solventextraction and analyzed by gas chromatography/massspectrometry as trimethylsilyl derivatives (25). Glu-taric acid was determined by a gas chromatography!mass spectrometry stable isotope dilution method (26).
Results
In case 1, postmortem examination showed no fattyinfiltration of the liver, kidneys, or heart; the modestinflammatory infiltration of the myocardium was con-sistent with myocarditis. The metabolite profile of liverhomogenate was uninformative (Table 1), and totalliver carnitine was 0.89 moIJg wet weight (range ofcontrol values: 0.33-1.09, n = 18). A urine specimenrevealed only trace amounts of the metabolites charac-teristic of this disorder (18).
Table 1. Metabolite profile of liver homogenate In twocases with LCHAD deficiency.
Metabolite Case 1 Case 2 Range Mdian
Octanoic acid 0.2 nd 0.1-0.8 0.2cis-4-Decenoic acid nd nd ndDecanoic acid 1 nd nd-1.1 0.2Dodecenoic acid nd nd ndDodecanoic acid 1.8 3.2 nd-20.5 3.8Tetradecenoic acid nd nd nd-0.8Tetradecanoic acid 6.0 3.6 1.0-23.8 5.6Palmitoleic acid 11.6 18.3 nd-i 3.6 10.0Palmitic acid 176.9 56.8 20.6-142.5 54.9Linoleic acid 80.4 112.3 13.5-242.0 66.2Oleic acid 89.6 114.5 8.6-142.7 34.5Stearic acid 48.5 23.5 9.8-42.3 21.1Glucose 204.9 nd 2-85.0 22.7

Enzyme measured
LCHAD
SCHADLCHAD/SCHAD ratio
SKATLKAT
Case 2
132
2450.54
2183.98
Controls, mean
± SD (n)
268 ± 29 (8)249 ± 26 (6)1.04 ± 0.05(6)
127 ± 6(6)3.47, 4.10(2)
SCHAD, short-chain 3-hydroxyacyl-C0A dehydrogenase; SKAT, short-chain ketothiolase; LKAT, long-chain 3-ketoacyl-CoA thiolase.
12:1
Parents of 99ES+4.77e6
10:1.
p
I
41Parents of 99ES+
2.60e5
16.
MasWCharge (mlz)
380 390 400 410 420 430 440 450 480
CLINICAL CHEMISTRY, Vol. 41, No. 8, 1995 1111
The autopsy of case 2 revealed a pale, lipid-filledliver. The metabolite profile of homogenate livershowed undetectable glucose and an increased concen-tration of palmitoleic acid, findings consistent with apossible FAO disorder (Table 1) (7, 15). Total livercarnitine was 0.45 moVg wet weight. Urine organicacid analysis revealed hypoketotic C6-C10 dicarboxylicaciduria and C6-C14 3-hydroxydicarboxylic aciduria,suggesting possible LCHAD deficiency. This diagnosiswas confirmed by assay of LCHAD activity in liver thathad been collected at autopsy and stored without delayat -70 #{176}C(Table 2). Three other mitochondrial en-zymes (short-chain 3-hydroxyacyl-CoA dehydrogenase,short-chain 3-ketoacyl-CoA thiolase, and long-chain3-ketoacyl-CoA thiolase) were tested as controls.
The organic acid analysis of postmortem urine fromcase 3 showed massive excretion of glutaric acid (1593mmollmol creatiine; controls: 0.5-13), 3-hydroxyglu-taric acid, and glutaconic acid but no ketonuria ordicarboxylic aciduria, a pattern considered pathogno-monic for glutaryl-CoA dehydrogenase deficiency (glu-taric acidemia type I) (27). At autopsy, examination ofthe brain revealed bilateral widening of the operculum,spongy degeneration of the white matter, and localizedlesions of the putamen and caudate nuclei, findingsstrongly supportive of the biochemical diagnosis. Twoof the three siblings with a similar clinical history havesubsequently been investigated, and their urine or-ganic acid profiles have been pathognomonic for glu-
Table 2. Mitochondrlal enzyme activities in liver extractof one case with LCHAD deficiency diagnosed
as SIDS.Activity, imoVmin per g protein
taric acidemia type I-massive excretion in urine ofglutaric acid, 3-hydroxyghutaric acid, and glutaconicacid.
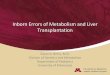
Figure 1 shows the acylcarnitine profiles (methylester derivatives) from case 1 and a control. Thepatient’s acylcarnitine profile was similar to thosepreviously described in plasma in cases with LCHADdeficiency (28), i.e., strong signals for saturated andunsaturated carnitine esters of C10-C18 fatty acids andless intense signals for the esters of C10-C18 3-hydroxyfatty acids. The acylcarrntine qualitative profile forcase 2 was essentially identical. These findings wereconfirmed by analysis involving a different derivatiza-tion (n-butyl-, data not shown). The marked increase of
Fig. 1. Acylcamitine profiles of postmortem bile obtained by precursor ion-scanning ESI/MS-MS: (top) case 1, LCHAD deficiency; (bottom)control.IS, Internal standard (d3-palmitoylcamitine, 72 pmol); n:8, 10 chain length of saturated acylcamitinespecies; n:1, chain length of monounsaturatedacylcamitlne species; n:2, chain length of diunsaturated acylcamitine species;#{149},fatty acylcamitinemethyl esters; *, fatty 3-hydroxyacylcamitine methyl esters.

Mean ± SD
472 ± 94
384 ± 8988 ± 24
0.2 ± 0.1
Range
323-566
158-469
49-1070.1-0.5
I
Mass/Charge (m/z)
1112 CLINICAL CHEMISTRY, Vol. 41, No. 8, 1995
Table 3. Camitine concentration in postmortem bile.Camitine, moI/L
Patients Controls (n = 8)
FractIon 1 2 3
Total 4139 907 148
Free 673 248 51
Acyl8 3466 659 97AcyVfree 5.2 2.7 1.9
ratio8 Calculated as total - free difference.
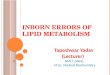
the acylcarnitine fraction in the postmortem bile spec-imens of these patients was confirmed by radioenzy-matic determination of total, free, and acylcarnitinefractions (Table 3). The acylcarnitine profile of the casewith ghutaryl-CoA dehydrogenase deficiency (Fig. 2)was characterized by a strong signal at m/z 304, corre-sponding to glutarylcarnitine (20). When analyzed un-der identical conditions, control bile samples fromSIDS cases that were uninformative by multiple anal-yses showed trace amounts of the C14-C16 fatty acylcar-nitines and no detectable accumulation of the otheracylcarnitine species described above.
DiscussionFormation of carnitine esters is involved in four
primary functions: (a) import of long-chain fatty acidsinto the mitochondria; (b) export of physiological short-chain acyl-CoA groups from mitochondria and peroxi-somes; (c) buffering of the free CoA/esterified CoA
ratio; and (d) enhancing urinary excretion of poten-tially toxic acyl-CoA groups accumulated as a conse-quence of a metabolic block (29). Because the latterfunction is limited when increasingly hydrophobiclong-chain fatty acids accumulate, carnitine-mediated
detoxification should theoretically not occur in long-chain FAO disorders (30). This conclusion, however,rests on the assumption that excretion in urine is theonly relevant mechanism of carnitine-mediated detox-ification in inherited metabolic diseases.
Gudjonsson et al. (31) reported that carnitine con-centrations in bile of rats receiving L-[3H]carnitineintraluminal injection approximated the concentra-tions found in the portal vein, suggesting passiverather than active transport into bile. Their conclusionwas that only a relatively small fraction of a radioac-tive carnitine dose is excreted in the bile, predomi-nantly in the esterified form. Several lines of experi-mental evidence otherwise suggest that the bifiaryexcretion of long-chain and possibly other acylcarnitinespecies may have been significantly underestimated.For instance, carnitine esters represented as much as83% of total carnitine in bile from rats fed a high-fatdiet for 72 h (32). In the fasted state, similar resultswere obtained not only in rats but in humans as well(33). In another study, the release of carnitine andisovalerylcarnitine was investigated in perfused ratliver after recirculating perfusion with 50 g.unol/L[3Hjcarnitine and infusion of 5 mmol/L a-ketoisocap-roate (34). a-Ketoisocaproate infusion produced accu-mulation of [3H]isovalerylcarnitine in the liver tissue
Fig. 2. Acyicamitine profiles of postmortem bile from case 3 (glutaryl-C0A dehydrogenase deficiency).5DC, glutarylcamitine; IS, internal standard (d3-palmitoylcamitine,72 pmol). Other symbols as in Fig. 1.

CLINICAL CHEMISTRY, Vol. 41, No. 8, 1995 1113
within 15 mm. Although no bile samples were exam-ined in this study, a rapid decrease of radioactivityin the liver tissue and the disappearance of[3Hlisovalerylcarnitine in the perfusate at 60 mm wereexplained by the authors as the consequence of rapidintrahepatic degradation of isovalerylcarnitine. How-ever, this carnitine ester is an end product ofisovaleryl-CoA catabolism that accumulates in bodyfluids of patients with isovaleryl-CoA dehydrogenase
deficiency (35) and is not a substrate for the microso-mal enzyme carnitine ester hydrolase (substrate spec-ificity: C6-C18) (36). A similar discrepancy is recogniz-able in a study of L-[CH3-3Hlcarnitine turnover in rats,in which unexplained cainitine losses were three timesthe amounts recovered in urine (37). Total carnitineexcretion in rat bile has been estimated as 0.4-1.4.tmol 24 h1 100 g body wt (31), which is in the sameorder of magnitude of urinary excretion (0.8-1.9 mol24 h’ 100 g body wt’) (37).
To our knowledge, our two patients with LCHAD
deficiency and the patient with glutaric acidemia typeI are the first cases of inborn errors of amino acid andfatty acid metabolism to have been assessed by metab-
olite profiling of bile. In all three cases, the qualitativeproffles were convincingly suggestive of the correctdiagnosis, as confirmed by a 10- to 25-fold increase ofthe respective acyl/free carnitine ratios. The detectionof glutarylcarnitine (C5), a compound readily excretedin urine, underlines the potential of bile analysis forthe biochemical diagnosis of a broad spectrum of dis-orders not limited to those with accumulation of long-chain acylcarnitines, the increasing hydrophobicity ofwhich precludes urinary excretion. In one LCHAD-
deficient patient, all other diagnostic methods includedin our current protocol (liver histology, metaboliteproffle and carnitine concentration of liver homoge-nate, and urine organic acids) were uninformative,suggesting that bile acylcarnitine profiling could leadto the identffication of an even greater proportion ofpreviously overlooked cases.
The finding of bile acylcarnitine concentrations inthe mmoJJL range was unexpected. Comparable con-centrations of carnitine have been reported in seminalfluid (1-3 mmol/L), but >90% of that is represented byfree carnitine excreted in the epididymal fluid underthe regulation of androgen hormones (29,38,39). Inbile, our results point instead to the existence of anactive primary transport of carnitine esters, with amechanism already demonstrated for the ATP-depen-dent glutathione S-conjugate carrier (40,41). Localiza-tion (basolateral or canalicular plasma membrane)(42), substrate specificity, and regulation of such aputative acylcarrntine carrier are unknown.
Comparison with postmortem plasma acylcarnitineprofiles was not possible in these cases, for the specificreason that collection and proper storage of bloodspecimens for metabolic testing is not routinely per-formed. However, published data consistently showthat plasma acylcarrntine concentrations in patientswith FAO disorders at the time of diagnosis are low
rather than high, being with few exceptions always<100 mo1.fL (43)-at least 10- to 40-fold lower thanthe acylcarnitine concentrations observed in postmor-tem bile.
Fasting intolerance is considered the main factorcausing life-threatening episodes in patients with FAOdisorders (44). In view of the fact that bile accumulatesin the gallbladder and is not released during fasting(45), acylcarnitines analysis of bile seems to be wellsuited for diagnostic purposes, especially in patientswith long-chain FAO disorders (30). Although testingof additional cases is needed to establish the specificityof this application, we propose the use of bile acylcar-nitine profiling for the postmortem diagnosis of meta-bolic disorders in infants and children who die sud-denly and unexpectedly.
This work was supported in part by a grant from the Saudi-USUniversities Project and by a Pilot Feasibility Project Grant fromthe Yale Liver Center (OK P3034989). Postmortem bile speci-mens used as controls were made available by Marvin Platt,Office of the Medical Examiner, Baltimore, MD.
References1. Johnson AR, Hood RL. Biotin and the sudden infant deathsyndrome. Nature 1980;285:159-60.2. Holton JB, Allen JT, Green CA, Partington RE, Gilbert RE,Berry PJ. Inherited metabolic diseases in the sudden infant deathsyndrome. Arch Dis Child 1991;66:1315-7.3. Smeitink JAM, Fischer JC, Ruitenbeek W, Duran M, HofkampM, Bentlage HA, Poll-The BT. Sudden infant death associatedwith defective oxidative phosphorylation [Letter]. Lancet 1993;341:1601.4. Bennett MJ, Allison F, Pollitt RJ, Variend S. Fatty acidoxidation defects as causes of unexpected death in infancy. ProgrChin Biol Res 1990;321:349-64.5. Anonymous. Sudden infant death and inherited disorders offat oxidation [Editorial]. Lancet 1986;ii:1073-5.6. Bennett MJ, Hale DE, Coates PM, Stanley CA. Postmortemrecognition of fatty acid oxidation disorders. Pediatr Pathol1991;11:365-70.7. Boles RG, Martin SK, Blitzer MG, Rinaldo P. Biochemicaldiagnosis of fatty acid oxidation disorders by metabolite analysisof post-mortem liver. Hum Pathol 1994;25:735-41.8. Bennett MJ, Powell S. Metabolic disease and sudden, unex-pected death in infancy. Hum Pathol 1994;25:742-6.9. Pollitt RJ. Defects in mitochondrial fatty acid oxidation: clin-ical presentations and their role in sudden infant death. PadiatrPadol 1993;28:13-7.10. Howat AJ, Bennett MJ, Shaw L, Variend S. Medium-chainacylcoenzyme A deficiency presenting as sudden infant deathsyndrome [Letter]. Br Med J 1984;288:397.11. Treem WR, Rinaldo P, Hale DE, Stanley CA, Millington DS,Hyams JS, et al. Acute fatty liver of pregnancy and long-chain3-hydroxyacyl-CoA dehydrogenase deficiency. Hepatology 1994;19:339-45.12. Wanders RJA, Duran M, Ijist L, de Jager JP, van Gennip AH,Jakobs C, et al. Sudden infant death and long-chain 3-hydroxy-acyl-CoA dehydrogenase [Letter). Lancet 1989;ii:52-3.13. Kainijo T, Wanders RJA, Saudubray JM, Aoyama T,Komiyama A, Hashimoto T. Mitochondrial trifunctional proteindeficiency. J Chin Invest 1994;93:1740-7.14. Tanaka K, Yokota I, Coates PM, Strauss AW, Kelly DP,Zhang Z, et al. Mutations in medium chain acyl-CoA dehydroge-nase (MCAD) gene. Hum Mutat 1992;1:271-9.15. Boles RG, Bhitzer MG, Platt M, Rinaldo P. Fatty acid oxida-tion and sudden death: analysis of 376 cases [Abstract]. PediatrRes 1994;35(Suppl):150A.16. Bennett MJ, Rinaldo P, Millington DS, Yokota I, Tanaka K,Coates PM. Medium chain acyl-CoA dehydrogenase deficiency:postmortem diagnosis in a case of sudden infant death and early

1114 CLINICAL CHEMISTRY, Vol. 41, No. 8, 1995
postnatal diagnosis of an affected sibling. Pediatr Pathol 1991;11:889-95.17. Brackett JC, Sims HF, Steiner RD, Nunge M, ZimmermanEM, deMartinville B, et al. A novel mutation in medium chainacyl-CoA dehydrogenase causes sudden neonatal death. J ChinInvest 1994;94: 1477- 83.18. Brackett JC, Sims HF, Rinaldo P, Shapiro 5, Powell CK,Bennett MJ, Strauss AW. Two a-subunit donor splice mutationscause human trifunctionah protein deficiency. J Clin Invest 1995;95:2076-82.19. Rashed MS, Ozand PT, Harrison ME, Watkins PJF, Evans S.Electrospray tandem mass spectrometry in the diagnosis oforganic acidemias. Rapid Commun Mass Spectrom 1994;8:129-33.20. Rashed MS, Little D, Ozand PT. Diagnosis of inborn errors ofmetabolism from blood spots by acylcarnitine and amino acidprofiling using automated electrospray tandem mass spectrome-try. Pediatr Res (in press).2L McGarry JD, Foster DW. An improved and simplified radio-isotopic assay for the determination of free and esterified can-tine. J Lipid Res 1976;17:277-81.22. Sekas G, Paul HS. Inhibition of carnitine acetyltransferaseby bile acids: implication for carrntine analysis. Anal Biochem1989;179:262-7.23. Cederblad G, Finnstrom 0, Martensson. Urinary excretion ofcarnitine and its derivatives in newborns. Biochem Med 1982;27:260-S.24. Weinberger MJ, Rinaldo P, Strauss AW, Bennett MJ. Intacta-subunit is required for membrane-binding of human mitochon-drial trifunctional p-oxidation protein, but is not necessary forconferring 3-ketoacyl-CoA thiolase activity to the p-subunit. Bio-chem Biophys Res Commun 1995;209:47-52.25. Bennett MJ, Ragni MC, Hood I, Hale DE. Comparison ofpost-mortem urinary and vitreous humor organic acids. Ann Chiniochem 1992;29:541-5.26. Shimuzu N, Yamaguchi 5, Onii T, Previs SF, Rinaldo P. Massspectrometric analysis of metabolite excretion in five Japanesepatients with the late onset form of glutanic aciduria type II. BiolMass Spectrom 1991:20:479-83.27. Goodman SI, Frerman FE. Organic acidemias due to defectsin lysine oxidation: 2-ketoadipic acidemia and glutaric acidemia.In: Scriver CR, Beaudet AL, Sly WS, Valle D, eds. The metabolicand molecular bases of inherited disease, 7th ed. New York:McGraw-Hill, 1995:1451-60.28. Millington DS, Terada N, Chace DH, Chen VT, Ding JH,Kodo N, Roe CR. The role of tandem mass spectrometry in thediagnosis of fatty acid oxidation disorders. Progr Chin Biol Res1992;375:339-54.29. Bremer J. Carnitine-metabolism, functions. Physiol Rev1983;63:1420-80.
30. Morrow RJ, Rose ME. Isolation of acylcarnitines from urine:a comparison of methods and application to long-chain acyl-CoAdehydrogenase deficiency. Chin Chim Acta 1992;211:73-81.31. Gudjonsson H, Li BIlK, Shug AL, Olsen WA. Studies ofcarnitine metabolism in relation to intestinal absorption. Am JPhysiol 1985;11:G313-9.32. Hamilton JJ, Hahn P. Carnitine in human and rat bile. In:Borum PR, ed. Clinical aspects of human carnitine deficiency.New York: Pergamon Press, 1986:38-9.33. Hamilton JJ, Hahn P. Carnitine and carnitine esters in ratbile and human duodenal fluid. Can J Physiol Pharmacol 1987;65:1816-20.34. Hokland BM. Uptake, metabolism and release of canrntineand acylcarnitine in the perfused rat liver. Biochim Biophys Acta1988;961:234-41.35. Roe CR, Millington DS, Mahtby DA, Kahier SG, Bohan TP.L-Carnitine therapy in isovaheric acidemia. J Chin Invest 1984;74:2290-5.36. Mahadevan 5, Sauer F. Carnitine hydnohase of rat liver. JBiol Chem 1969;244:4448-53.37. Brooks DE, McIntosh JEA. Turnover of carnitine by rattissue. Biochem J 1975;148:439-45.38. B#{248}hmerT, Hansson V. Androgen-dependent accumulation ofcarnitine by rat epididymis after injection of [3Hlbutyrobetaine invivo. Mol Cell Endocninol 1975;3:103-15.39. Lewin LM, Beer R, Lunenfehd B. Epididymis and seminalvesiche as sources of cannitine in human seminal fluid: the clinicalsignificance of the carrntine concentration in human seminalfluid. Fertil Steril 1976;27:9-13.40. Inoue M, Akerboom TPM, Sies H, Kinne R, Tran T, Arias IM.Biliary transport of glutathione S-conjugate by rat liver canalic-ular membrane vesicles. J Biol Chem 1984;259:4998-5002.41. Akerboom TPM, Nanayanaswann V. Kunet M, Sies H. ATP-dependent S-(2,4-dinitrophenyh) glutathione transport in canal-icular plasma membrane vesiches from rat liver. J Biol Chem1991;266:13147-52.42. Suchy FJ. The use of membrane vesiches to study hepatictransport. In: Tavohoni N, Berk PD, eds. Hepatic transport andbile secretion: physiology and pathophysiology. New York: RavenPress, 1993:211-23.43. Hoppel CL. Determination of cannitine. In: Hommes FA, ed.Techniques in diagnostic human biochemical genetics-a labora-tory manual. New York: Wiley-Liss, 1991:309-26.44. Treem WR. Inborn defects in mitochondrial fatty acid oxida-tion. In: Suchy FJ, ed. Liver disease in children. St. Louis: Mosby,1993:852-87. -
45. Vlahcevic ZR, Heuman DM, Hylemon PB. Physiology andpathophysiology of enterohepatic circulation of bile acids. In:Zakim D, Boyer JL, eds. Hepatohogy. Philadelphia: WB Saunders,1990:341-77.