Embed Size (px)
Citation preview
In Vitro Hemocompatibility Testing: Continuing
Development of an Ovine Blood-Loop Assay
Yan Chen, PhDSr. Director, Biocompatibility
American Preclinical Services/NAMSA
SOT-MDCPSS Webinar, March 30, 2021
2CONFIDENTIAL2
DISCLAIMER
The material presented is for general information sharing only and is solely the opinion of the presenter.
3CONFIDENTIAL
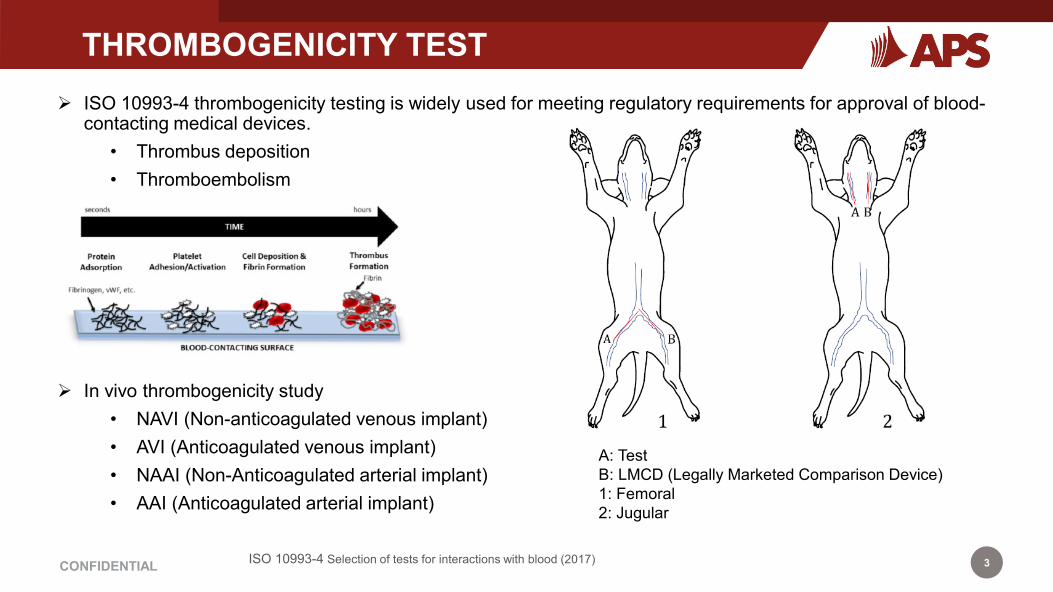
THROMBOGENICITY TESTTHROMBOGENICITY TEST ISO 10993-4 thrombogenicity testing is widely used for meeting regulatory requirements for approval of blood-
contacting medical devices.• Thrombus deposition• Thromboembolism
In vivo thrombogenicity study• NAVI (Non-anticoagulated venous implant)• AVI (Anticoagulated venous implant)• NAAI (Non-Anticoagulated arterial implant)• AAI (Anticoagulated arterial implant)
A: TestB: LMCD (Legally Marketed Comparison Device)1: Femoral2: Jugular
ISO 10993-4 Selection of tests for interactions with blood (2017)
4CONFIDENTIAL
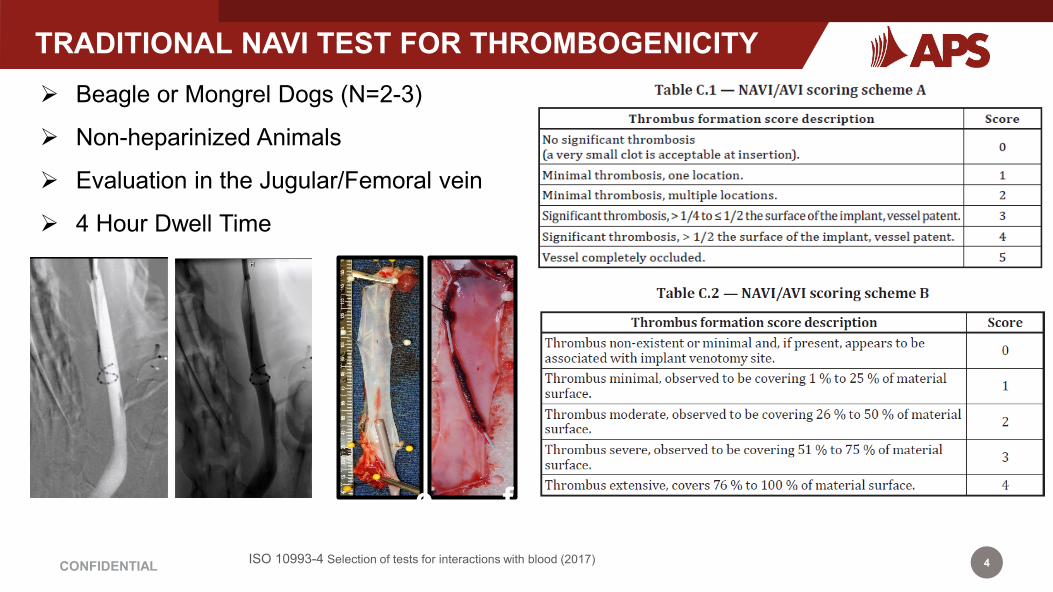
TRADITIONAL NAVI TEST FOR THROMBOGENICITY
ISO 10993-4 Selection of tests for interactions with blood (2017)
Beagle or Mongrel Dogs (N=2-3)
Non-heparinized Animals
Evaluation in the Jugular/Femoral vein
4 Hour Dwell Time
e f
5CONFIDENTIAL
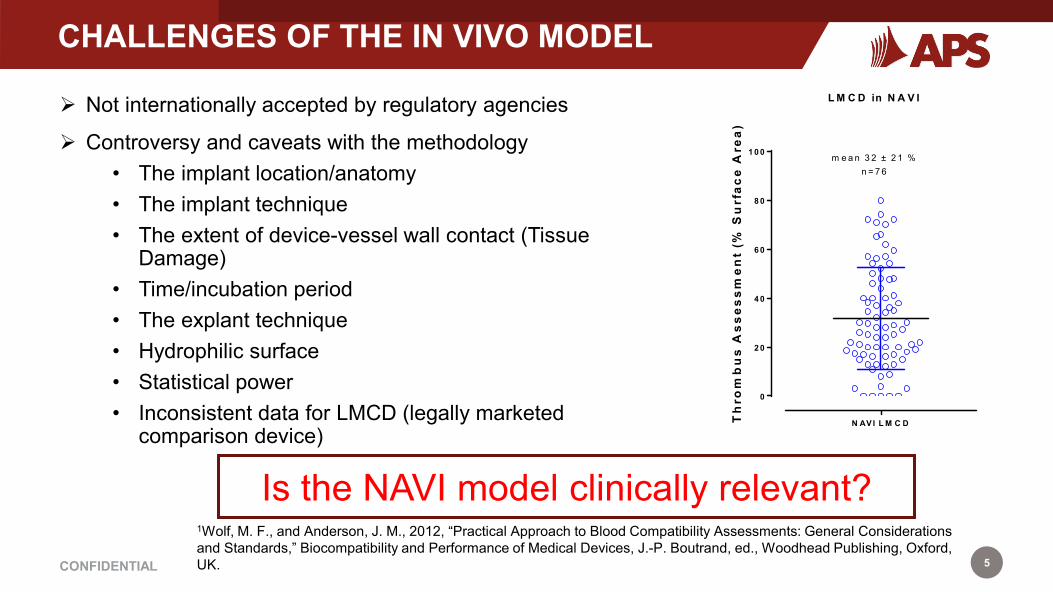
CHALLENGES OF THE IN VIVO MODEL
Not internationally accepted by regulatory agencies
Controversy and caveats with the methodology• The implant location/anatomy• The implant technique • The extent of device-vessel wall contact (Tissue
Damage)• Time/incubation period • The explant technique• Hydrophilic surface• Statistical power• Inconsistent data for LMCD (legally marketed
comparison device)
1Wolf, M. F., and Anderson, J. M., 2012, “Practical Approach to Blood Compatibility Assessments: General Considerations and Standards,” Biocompatibility and Performance of Medical Devices, J.-P. Boutrand, ed., Woodhead Publishing, Oxford, UK.
Is the NAVI model clinically relevant?
N AVI L M C D
0
2 0
4 0
6 0
8 0
1 0 0
L M C D in N A V I
Th
rom
bu
s A
sses
smen
t (%
Su
rfac
e A
rea)
m e a n 3 2 ± 2 1 %n = 7 6

6CONFIDENTIAL6
IN VITRO MODEL – BLOOD LOOPLoop Configuration Temperature Control
Positive Control: Latex Tubing (Manually Abraded)
Negative Control: PU Catheter (Hydromer Coated)
8CONFIDENTIAL8
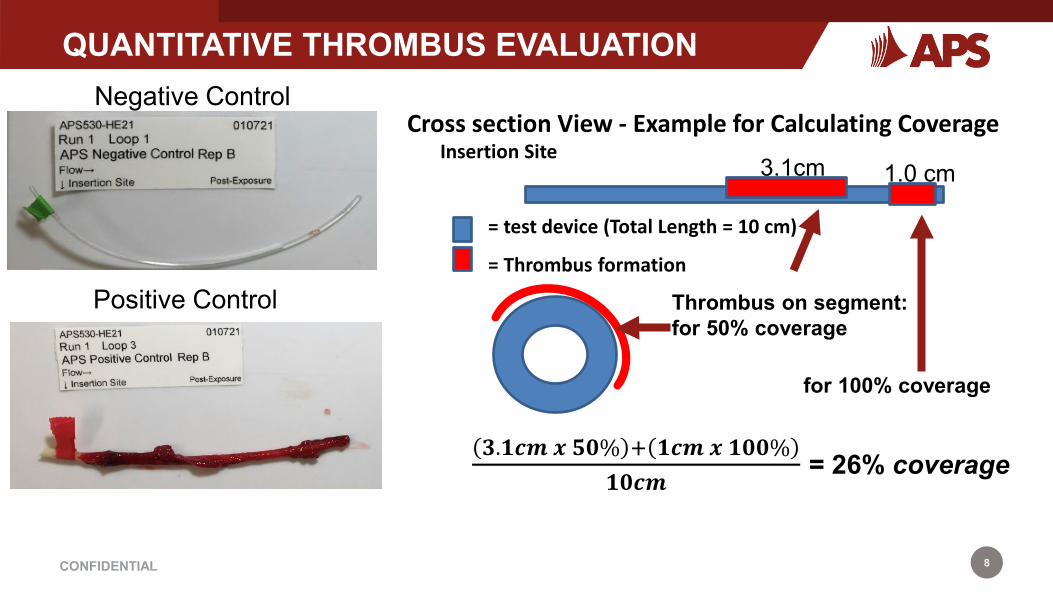
QUANTITATIVE THROMBUS EVALUATION
Insertion Site
= test device (Total Length = 10 cm)
= Thrombus formation
Thrombus on segment: for 50% coverage
for 100% coverage
Cross section View - Example for Calculating Coverage
𝟑𝟑.𝟏𝟏𝟏𝟏𝟏𝟏 𝒙𝒙 𝟓𝟓𝟓𝟓𝟓 + 𝟏𝟏𝟏𝟏𝟏𝟏 𝒙𝒙 𝟏𝟏𝟓𝟓𝟓𝟓𝟓𝟏𝟏𝟓𝟓𝟏𝟏𝟏𝟏
= 26% coverage
3.1cm 1.0 cm
Negative Control
Positive Control

9CONFIDENTIAL
STUDY ASSESSMENT
Thrombus formation • % surface area coverage
Non-adherent thrombus • Weights of non-adherent thrombus
Blood characterization• Complete blood counts (CBC)• Activated clotting time (ACT) • Platelet counts

10CONFIDENTIAL
IN VIVO – IN VITRO COMPARISON
NAVI (in vivo) Blood Loop (in vitro)
Implant positionand technique
• Animal anatomy variation• Experience based implant technique• Hard to check device deployment
• Uniform tubing diameter• Controlled deployment procedure
Device-vessel wall contact
• Tissue Factor • Minimal tubing wall contacting• No Tissue Factor components
Statistical power • N=2-3 • N= 3 – 9• Three donors
Controls • LMCD • LMCD• Positive Control• Negative Control
Risk for thromboembolism
• Downstream Organs (Heart and Lung)
• Unable to distinguish between test and LMCD
• Non-adherent thrombus quantification
• Separate loop to distinguish between test and LMCD

11CONFIDENTIAL
IN VITRO BLOOD LOOP - PUBLICATIONS
Journal of Medical Devices: Special Issue on Cardiovascular Device Development

12CONFIDENTIAL
3R’s AWARD FOR IN VITRO ALTERNATIVE ASSAY
13CONFIDENTIAL13
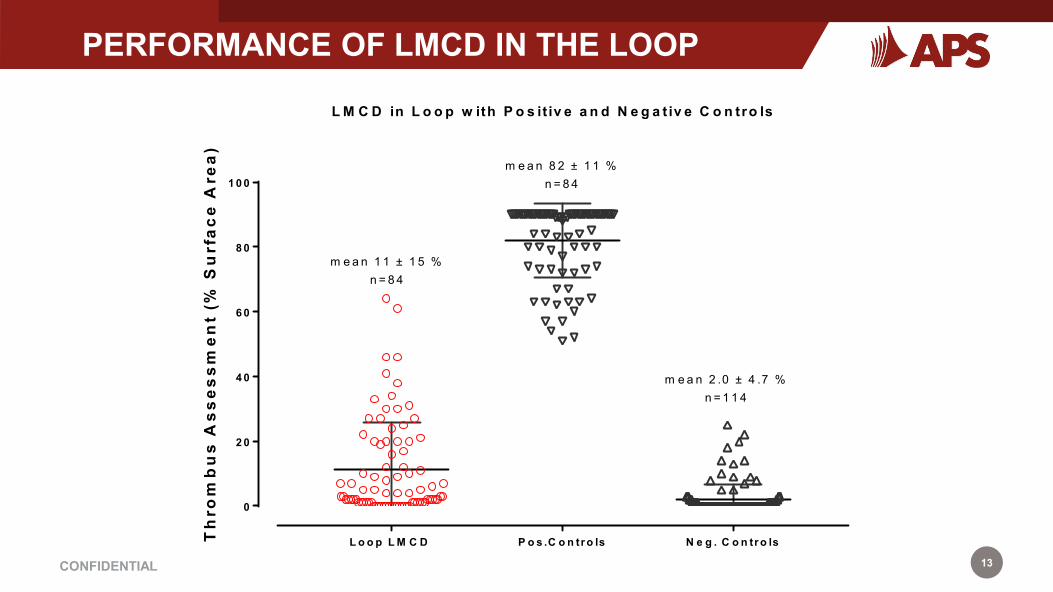
PERFORMANCE OF LMCD IN THE LOOP
L o o p L M C D P o s .C o n tr o ls N e g . C o n tr o ls
0
2 0
4 0
6 0
8 0
1 0 0
L M C D in L o o p w ith P o s it iv e a n d N e g a t iv e C o n tro ls
Th
rom
bu
s A
sses
smen
t (%
Su
rfac
e A
rea)
m e a n 1 1 ± 1 5 %n = 8 4
m e a n 2 .0 ± 4 .7 %n = 1 1 4
m e a n 8 2 ± 1 1 %n = 8 4
14CONFIDENTIAL14
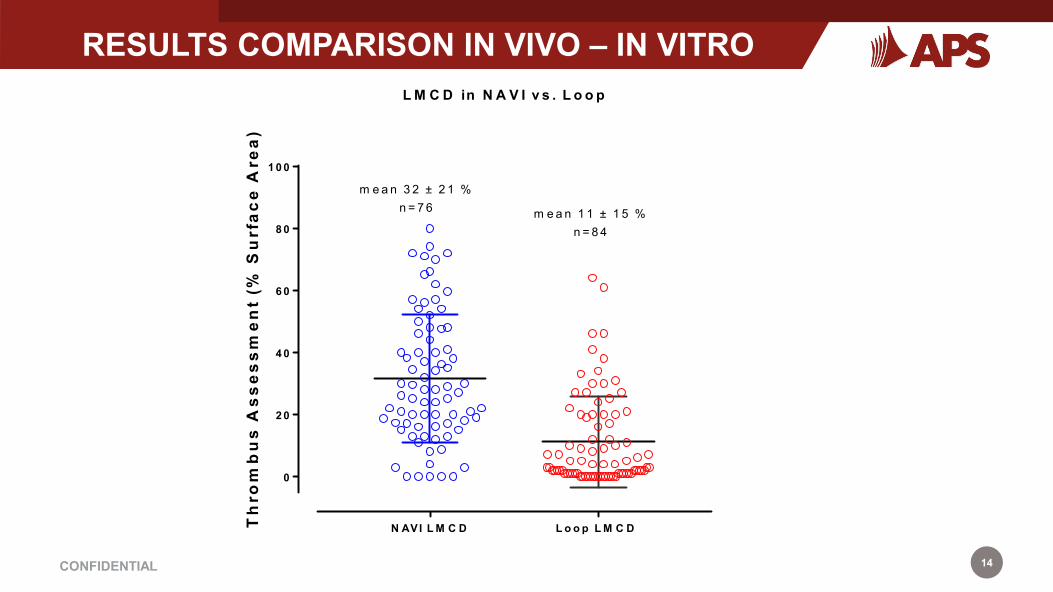
RESULTS COMPARISON IN VIVO – IN VITRO
N AVI L M C D L o o p L M C D
0
2 0
4 0
6 0
8 0
1 0 0
L M C D in N A V I v s . L o o p
Th
rom
bu
s A
sses
smen
t (%
Su
rfac
e A
rea)
m e a n 3 2 ± 2 1 %n = 7 6 m e a n 1 1 ± 1 5 %
n = 8 4
15CONFIDENTIAL15
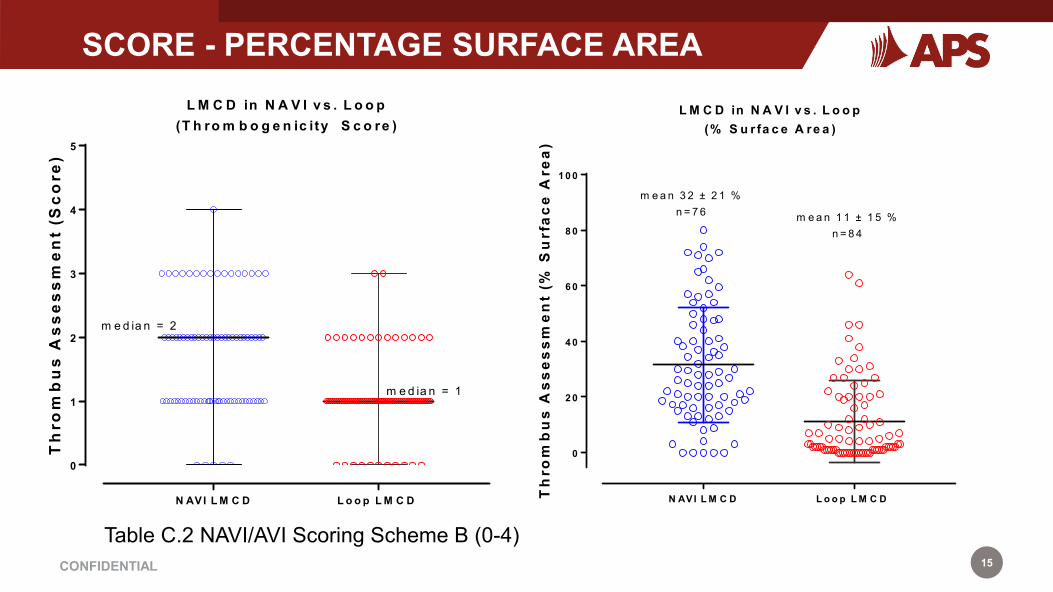
SCORE - PERCENTAGE SURFACE AREA
Table C.2 NAVI/AVI Scoring Scheme B (0-4)
N AVI L M C D L o o p L M C D
0
1
2
3
4
5
L M C D in N A V I v s . L o o p(T h ro m b o g e n ic ity S c o re )
Th
rom
bu
s A
sse
ss
me
nt
(Sc
ore
)
m e d ia n = 2
m e d ia n = 1
N AVI L M C D L o o p L M C D
0
2 0
4 0
6 0
8 0
1 0 0
L M C D in N A V I v s . L o o p(% S u r fa c e A re a )
Th
rom
bu
s A
sses
smen
t (%
Su
rfac
e A
rea)
m e a n 3 2 ± 2 1 %n = 7 6 m e a n 1 1 ± 1 5 %
n = 8 4
16CONFIDENTIAL16
CONCLUSIONS
The high frequency of thrombus formation leading to scores of ≥3 (≥ 51% surface areaoverage) for LMCDs highlights the deficiency in the performance of NAVI assay.
In comparison, the in vitro blood loop assay results where assay performance ofLMCDs was much more in line with their clinical performance and regulatory history.
In addition, the blood-loop assays also carries the enhanced support by concurrent useof well-behaved positive and negative controls to address the variability of the in vitroassay.
Overall, these results strongly supported the inability of the NAVI model to predictclinical risk. Alternative assays need to be developed and the regulatory acceptance isdesired.
17CONFIDENTIAL17
ACKNOWLEDGEMENT
Mark Smith, PhDChief Scientific Officer, Emeritus
APS
APS staff contributed to the blood loop projectAmber DargisSarah Howard
Heather AckersonTammy Fossum










![Bordetella Pertussis virulence factors in the continuing ... · Bordetella polysaccharides (Bps), and their significance in biofilm formation in vitro and in mice [26]. By func-tioning](https://img.dokumen.tips/doc/110x75/5ffe9ca82b08704ea77e4974/bordetella-pertussis-virulence-factors-in-the-continuing-bordetella-polysaccharides.jpg)