Embed Size (px)
Citation preview

In situ antimicrobial activity of chlorhexidine in the oral cavity
Tomás I1, Rubido S1, Donos N2
1-Special Needs Unit. School of Medicine and Dentistry. Santiago de Compostela University. Spain. 2-Periodontology Unit. UCL Eastman Dental Institute. London. United Kingdom.
Chlorhexidine (CHX) is the oral antiseptic par excellence. One of its principal advantages, in addition to its powerful antimicrobial action, is its ability to bind to a variety of substrates while maintaining its antibacterial activity; it is then slowly released, leading to the persistence of effective concentrations. This property is called substantivity. The purpose of this chapter is to review the findings published in the literature on the in situ antimicrobial activity of CHX in different oral ecosystems and to report our own results in this field.
Numerous authors have demonstrated the immediate antibacterial effect of CHX and its substantivity in saliva for a minimum of 7 hours after a single mouthrinse. However, few authors have studied the in situ antibacterial activity of CHX on the salivary flora, analysing the influence of intrinsic factors associated with the antiseptic and extrinsic factors, all of which can affect its antibacterial activity. Nor have many studies been published using confocal laser scanning microscopy (CLSM) in association with bacterial viability techniques to determine the effects of CHX on in situ undisturbed plaque-like biofilm, and the results have not been uniform.
Consequently, a more extensive application of advanced microbiological and/or microscopy techniques in combination with CLSM is required in future research in order to increase our understanding of the antibacterial effects of CHX and other antimicrobial agents on plaque-like biofilm structure. These effects should then be compared with the effects observed in other oral ecosystems (such as salivary flora) and the influence of intrinsic and extrinsic factors on the effectiveness of the antiseptic should be analysed.
Keywords: chlorhexidine; substantivity; salivary flora; biofilm; bacterial viability; epifluorescence microscopy; confocal laser scanning microscopy.
1. Introduction
In 1947, a complex study to synthesize new antimalarial agents led to the development of the polybiguanides [1]. These compounds showed significant antimicrobial potential, particularly compound 10,040, a cationic detergent later called chlorhexidine (CHX) [2]. Although two salts with similar antibacterial activity, the diacetate and the dihydrochloride, were initially selected, the diacetate was more soluble and was therefore more suitable for laboratory work. Davies et al [2] demonstrated that this compound had bacteriostatic activity, especially against Gram-positive bacteria (linked to the central hexamethylene unit and the terminal benzene ring) and bactericidal activity (depending on the concentration of 10,040, inoculum size and pH). Compound 10,040 did not modify the action of penicillin, streptomycin, chloramphenicol, oxytetracyline or aureomycin. Experimental studies in albino mice revealed a low degree of toxicity at 10 days after the subcutaneous, intraperitoneal, intravenous or oral administration of a single dose of CHX, as well as after a year of continuous oral administration. The first salt derived from compound 10,040 that reached the market was CHX gluconate, which was registered in 1954 by Imperial Chemical Industries Co. Ltd of Macclesfield (United Kingdom) as Hibitane®, the first internationally accepted antiseptic for cleansing wounds and the skin [3,4]. In 1957, only 3 years after coming onto the market, the broad antimicrobial spectrum of CHX led to an extension of its indications to include not only skin disinfection but also use in the fields of ophthalmology, urology, gynaecology and otorhinolaryngology. Although CHX started to be used to control bacterial plaque in 1959, it was not until publication of the studies by Löe and Schiött in the 1970s that the use of CHX became widespread in dentistry [5,6]. Nowadays, CHX is considered to be the oral antiseptic par excellence. The most commonly used concentrations in commercially available CHX mouthrinses are 0.2% and 0.12%. Besides its effects on plaque and gingivitis, CHX is effective in the prevention and treatment of caries, infections secondary to oral surgical procedures, and in the maintenance of implants. CHX reduces the bacterial load of aerosols and reduces bacteraemia after dental manipulation. It is also employed in the treatment of recurrent aphthous and denture-related stomatitis. CHX is particularly indicated in certain population groups, such as individuals with orthodontic appliances, disabled people, and immunologically compromised patients [7]. One of the main advantages of CHX, besides being a powerful antimicrobial, is its ability to bind to a wide variety of substrates while maintaining its antibacterial activity. It is then slowly released, leading to persistence of effective concentrations; this property is known as substantivity [8]. The purpose of this chapter is to review the findings
530 ©FORMATEX 2011
Science against microbial pathogens: communicating current research and technological advances A. Méndez-Vilas (Ed.)______________________________________________________________________________

published in the literature on the in situ antimicrobial activity of CHX in different oral ecosystems, and to report our own results in this field.
2. General characteristics of chlorhexidine
CHX is the most extensively studied and effective anti-plaque and anti-gingivitis agent and it is the most widely used antimicrobial among the available agents. It is one of the second generation oral antiseptics with the greatest antibacterial activity and substantivity [4].
2.1 Chemical structure
CHX is an amphipathic molecule with hydrophilic and hydrophobic groups and is cationic at physiological pH. This molecule was synthesized from proguanil and belongs to the biguanide family, a group of compounds with antimalarial activity [9]. Structurally, it consists of two symmetrical chlorophenol rings (4-chlorophenyl) and two biguanide groups, united by a central hydrophobic hexamethylene chain. The result, as shown in Figure 1, is a symmetrical bicationic molecule called 1,6-di(4’-chlorophenyldiguanido)hexane [10].
Fig 1. Chemical structure of chlorhexidine (C22H30Cl2N10).
Normally, CHX is used in salt form, principally as diacetate, digluconate or dihydrochloride, as the base molecule is relatively insoluble in water [4,11,12]. Digluconate salt is the most soluble in water and alcohols [12] and is therefore the form employed in the majority of mouthrinsees, gels and varnishes. In addition, this CHX salt has the added advantage that, at physiological pH, it releases the active component with a positive ionic charge [13].
2.2. Mechanism and spectrum of antibacterial action
The concept of "target" used to explain the mechanism of action of antibiotics may also be applicable to CHX; however, unlike the antibiotics, it does not break down the bacterial wall [14]. CHX, like other cationic antimicrobials known for decades as "membrane-active agents" [10], acts on the cell membrane to increase its permeability and facilitate the release of intracytoplasmic material [15]. The outermost layer of the bacterial cell wall carries a negative charge, usually stabilised by the presence of cations such as Mg2+ and Ca2+; for this reason, the majority of antiseptics are cationic agents that have a high affinity with the bacterial cell wall [10,16]. The first phase of action of CHX is its adsorption onto the wall of the microorganism [13]. This is a very rapid process that is explained by the presence of two basic and symmetrical clorophenylguanide groups attached to a lipophilic chain of hexamethylene and which form the bicationic molecule that readily interacts with the bacterial surface [17]. Conditions for binding are favourable when the pH is neutral or slightly alkaline; the amount of CHX adsorbed is dependent on the concentration of the agent. Although the mechanism of action of the bisbiguanides is very similar to that of the quaternary ammonium compounds, their binding to phospholipids and proteins from the bacterial cell wall and membrane is stronger; in addition, the length of the hydrophobic region of the bisbiguanides prevents their interdigitation within the lipid bilayer. CHX thus establishes a bridge between pairs of adjacent phospholipids and displaces the associated divalent cations. The cationic CHX molecule will bind principally to anionic compounds such as free sulphates, lipopolysaccharide phosphate groups and protein carboxyl groups [18]. At low concentrations, CHX decreases the permeability of the cytoplasmic membrane, altering its metabolic osmoregulatory capacity and its enzyme content [9,19]. Some indirect indicators of these effects are the escape of potassium ions, phosphorus and protons, and an inhibition of respiration and of solute transport. This alteration of membrane integrity is responsible for the bacteriostatic effect of CHX and is reversible [11,15,20]. At higher
531©FORMATEX 2011
Science against microbial pathogens: communicating current research and technological advances A. Méndez-Vilas (Ed.)_______________________________________________________________________________
concentrations of CHX, the interactions are stronger, with crystallization of the membrane that causes loss of its structural integrity, leading to a catastrophic release of intracellular material. This is the basis of the bactericidal effect of CHX, which causes precipitation or coagulation of the bacterial cytoplasm, with a paradoxical decrease in the outflow of components through the membrane. This process eventually leads to cell death [21-23] . CHX is a broad-spectrum antiseptic, bactericide and fungicide [20]. Although it is not considered to be virucidal, CHX show some activity on the lipid envelopes of viruses such as HIV, Herpes 1 and 2 and Influenza A [12,24]. CHX is not sporicidal, nor does it eliminate acid-fast bacteria [13,25], though it can inhibit the growth of spores and has a bacteriostatic effect on some mycobacteria [12]. CHX is more effective against Gram-positive than against Gram-negative bacteria due to differences in the structural characteristics of the outer membrane [3].
3. In situ antimicrobial activity of chlorhexidine on different oral ecosystems
Study of the in situ antibacterial activity of an antiseptic involves an analysis of its immediate effect and of its substantivity. Substantivity is defined as the prolonged adherence of the antiseptic to the oral surfaces (teeth and mucosas) and its slow release in effective doses that guarantee the persistence of its antimicrobial activity [8]. This property, together with the antimicrobial activity, is essential for an antiseptic to be clinically effective. It has been shown that CHX has a greater immediate in situ antibacterial effect and substantivity than other antiseptics used in the oral cavity [26-29]. For this reason, the majority of recent microbiological studies have used 0.12% or 0.2% CHX as the positive control in the analysis of results obtained with other active substances on specific oral ecosystems [30-32]. However, there still remain certain aspects of the antibacterial activity of CHX that have not been studied in sufficient depth. It has been shown that the retention of CHX in the oral cavity depends not only on the nature of the product, but also on intrinsic factors associated with the antiseptic (such as concentration, duration of mouthrinse, and temperature) and extrinsic factors (such as the presence or absence of teeth, dental prostheses or organic material, the pH of the saliva and the intake of food or drink) [33-35]; the retention of CHX in the oral cavity could affect its antibacterial activity.
3.1 In situ antimicrobial activity of chlorhexidine on salivary flora
Since the first results reported by Schiött et al in 1970 [36], many studies evaluating the antimicrobial activity of CHX on the salivary flora have been published in the literature [26-29]. It has been recognised that analysis of the salivary flora provides information on CHX antimicrobial activity and is considered to be predictive of its substantivity [37,38]. This is probably because the saliva acts as a "means of dissemination" of oral microorganisms from one ecological niche to another [39]. On this subject, Weiger et al [40] suggested that the first phenomena of microbial colonisation after contact with a clean tooth surface occur mainly due to the adhesion of salivary bacteria. However, other authors argued that a single determination of the reduction in the bacterial load in saliva does not demonstrate any correlation with effects on plaque inhibition [41]. In 2003, Sekino et al [42] showed that the number of bacteria in the saliva after different CHX regimens may influence the amount of plaque that forms early during a phase of no oral hygiene.
Methodological approach
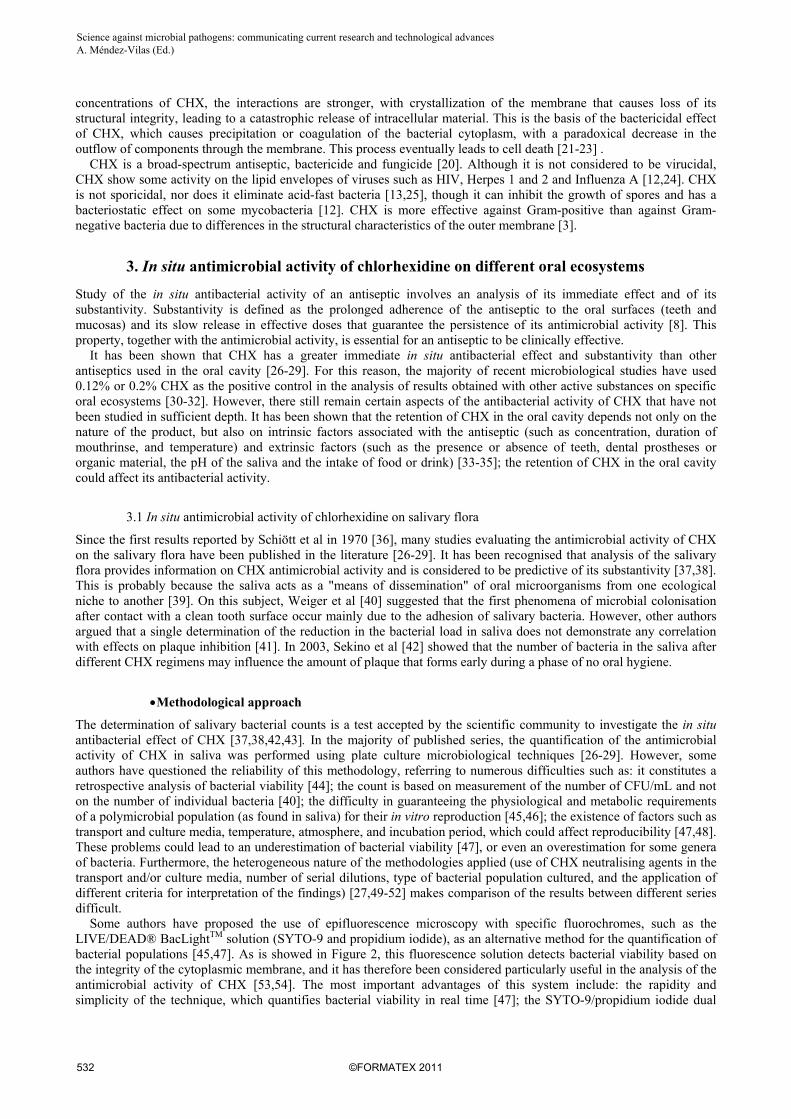
The determination of salivary bacterial counts is a test accepted by the scientific community to investigate the in situ antibacterial effect of CHX [37,38,42,43]. In the majority of published series, the quantification of the antimicrobial activity of CHX in saliva was performed using plate culture microbiological techniques [26-29]. However, some authors have questioned the reliability of this methodology, referring to numerous difficulties such as: it constitutes a retrospective analysis of bacterial viability [44]; the count is based on measurement of the number of CFU/mL and not on the number of individual bacteria [40]; the difficulty in guaranteeing the physiological and metabolic requirements of a polymicrobial population (as found in saliva) for their in vitro reproduction [45,46]; the existence of factors such as transport and culture media, temperature, atmosphere, and incubation period, which could affect reproducibility [47,48]. These problems could lead to an underestimation of bacterial viability [47], or even an overestimation for some genera of bacteria. Furthermore, the heterogeneous nature of the methodologies applied (use of CHX neutralising agents in the transport and/or culture media, number of serial dilutions, type of bacterial population cultured, and the application of different criteria for interpretation of the findings) [27,49-52] makes comparison of the results between different series difficult. Some authors have proposed the use of epifluorescence microscopy with specific fluorochromes, such as the LIVE/DEAD® BacLightTM solution (SYTO-9 and propidium iodide), as an alternative method for the quantification of bacterial populations [45,47]. As is showed in Figure 2, this fluorescence solution detects bacterial viability based on the integrity of the cytoplasmic membrane, and it has therefore been considered particularly useful in the analysis of the antimicrobial activity of CHX [53,54]. The most important advantages of this system include: the rapidity and simplicity of the technique, which quantifies bacterial viability in real time [47]; the SYTO-9/propidium iodide dual
532 ©FORMATEX 2011
Science against microbial pathogens: communicating current research and technological advances A. Méndez-Vilas (Ed.)______________________________________________________________________________
staining allows viable and non-viable bacteria to be counted simultaneously [47]; and the possibility of detecting bacteria that cannot be cultured using plate culture techniques [44,55].
Fig 2. Salivary bacteria with intact membranes (emitting green fluorescence) and with damaged membranes (emitting red fluorescence) on epithelial cells (100x objective).
Recently, Tomás et al [56] showed that epifluorescence microscopy with the SYTO-9/propidium iodide dual staining permits evaluation of the antimicrobial activity of CHX on the salivary flora in real time. On the other hand, the quantification of bacteria by epifluorescence microscopy may also have some associated problems such as bacterial coaggregation (even after homogenisation) and the staining of cellular elements or contaminating material [45]. There are even authors who considered the microscopic examination of the staining bacteria tedious, time consuming and unsuitable for testing a large number of samples [57].
Immediate effect and substantivity of chlorhexidine
Using plate culture techniques, many authors have detected the immediate antibacterial effect and the persistence of its substantivity for a minimum of 7 hours after a mouthrinse with 0.12% CHX (15 mL/30 seconds), although the immediate decrease in bacterial viability in this case did not exceed 72%-87% (<1 log10) [30,50,58], and was 58%-88% (<1 log10) at 7 hours after the mouth rinse [28,30,58]. In contrast, Cousido et al [59], using epifluorescence microscopy with SYTO 9/propidium iodide dual staining, observed that the mouthrinse with 0.12% CHX produced an immediate decrease in the percentage of live bacteria less than 90% compared to baseline values. This antimicrobial activity was only detectable up to 3 hours after the mouthrinse, at which point the reduction in bacterial viability was of 20%. Other authors have demonstrated that the application of a mouthrinse with 0.2% CHX (10 mL/1 minute) was associated with an immediate antibacterial effect, with a reduction of ≥90% (≥ 1 log10) in the bacterial concentration with respect to the baseline values [26,60-63], and its substantivity persisted for a minimum of up to 7 hours after the mouth rinse, with a reduction ≥90% [26,60,61,63]. Cousido et al [59] detected that the mouthrinse with 0.2% CHX resulted in an immediate decrease in the percentage of live bacteria (≥90%), and this antimicrobial activity was still detectable 7 hours after the mouthrinse, with a significant reduction in bacterial viability of 14% compared to baseline values. Many authors have observed that the immediate antibacterial effect of a single application of 0.12% or 0.2% CHX remained constant for a minimum of up to 7 hours after the mouth rinse [26,49,60,61,63,64]. However, other authors have detected a continued fall in bacterial viability up to 3-5 hours after the mouthrinse, with a subsequent recovery of the salivary flora at 7 hours after the mouthrinse [27,65]. In accordance with the results reported in some in vitro studies [66], the paper published by Cousido et al [59] showed a significant recovery in bacterial viability in the saliva samples collected at 1 hour after the different CHX mouthrinses in comparison with the viability at 30 seconds after mouthrinsing. These differences could be due to methodological variations and they highlight the need to clarify the influence of CHX substantivity on the recovery of the salivary flora after its application. The scientific community has assumed that the substantivity of CHX persists for 12 to 14 hours after its application. However, there are few studies published in which the in situ substantivity of CHX on the salivary flora has been determined more than 7 hours after the application of the antiseptic, and the majority of those studies analysed samples collected at 24 hours after the mouthrinse [64,67]. Recently, Tomás et al (unpublished data) observed that the antimicrobial activity of 0.2% CHX persisted up to 12 hours after the mouthrinse, with a reduction in bacterial viability of 20%.
533©FORMATEX 2011
Science against microbial pathogens: communicating current research and technological advances A. Méndez-Vilas (Ed.)_______________________________________________________________________________

Influence of intrinsic and extrinsic factors
Some authors have investigated the in situ antibacterial activity on the salivary flora of a single mouthrinse of 0.2% CHX versus 0.12% CHX, mainly analysing the influence of the dose administered (applying different volumes of both CHX concentrations) [49,68]. Addy et al [49] studied the substantivity in saliva of CHX mouthrinses at various concentrations and volumes (10 mL of 0.2% CHX, 15 mL of 0.12% CHX, and 15 mL of 0.1% CHX for 1 minute). At 30 minutes after the mouthrinse, the 0.2% and 0.12% CHX solutions showed significant reductions in bacterial concentrations (decrease ≥1 log10 CFU/mL) which persisted up to 7 hours after the mouthrinse. Harper et al [68] also evaluated the substantivity of a number of mouthrinses of different volumes and CHX concentrations applied for 1 minute (10 mL of 0.2% CHX, 15 mL of 0.12% CHX from 2 different manufacturers, and 15 mL of 0.1% CHX dissolved in 30 mL of water). The greatest antibacterial activity at 30 minutes was found after the mouthrinse with the 0.2% and 0.12% CHX. Significant differences in the bacterial concentrations persisted up to 5 hours after the application of the 3 CHX mouthrinses, but at 7 hours the effect was only observed with the 0.2% CHX and one of the 0.12% CHX mouthrinses (Prexidine®). Thus both Addy et al [49] and Harper et al [68] agree that the antibacterial activity of CHX is dose-dependent. In the majority of in situ studies on the 0.12% CHX substantivity in saliva the authors have evaluated the antibacterial effect after the application of a 30 second mouthrinse [30,65,69], whereas a period of 1 minute was used with the 0.2% CHX mouthrinse [61-63]. In the series published by Tomás et al [70], the increase in the duration of application (from 30 seconds to 1 minute) led to greater substantivity with both concentrations of CHX (up to 5 hours after the 0.12% CHX mouthrinse and up to 7 hours after the 0.2% CHX mouthrinse). Despite the importance given to the concentration of CHX with respect to its antimicrobial activity [71], few authors have studied in situ the influence of CHX concentration (0.2% versus 0.12%) on its antibacterial activity on the salivary flora. Recently, using plate culture techniques, Tomás et al [72] observed that a mouthrinse with 0.2% CHX (10 mL/30 seconds) was associated with an immediate antimicrobial activity that was maintained for 1 hour after its application and that this was significantly greater than the effect of a mouthrinse with 0.12% CHX (10 mL/30 seconds). In another study published later by this research group [59], 0.2% CHX produced a significantly greater antibacterial effect than 0.12% CHX in all the saliva samples obtained after the mouthrinse. These results confirmed that the antibacterial effect of CHX and its substantivity are concentration-dependent, as previously reported by other authors who compared different concentrations of CHX (0.12% versus 0.06%, 0.06% versus 0.03%, and 0.12% versus 0.1%) [49,52]. However, when the same volume of different CHX concentrations is used (10 mL of 0.12% and 0.2% CHX), we are analysing not only the influence of concentration, but also the dose administered (12 mg versus 20 mg). Recently, it has been demonstrated that, on comparing both concentrations, the mouthrinse with 15 mL of 0.12% CHX had a lower substantivity on the salivary flora than 10 mL of the 0.2% solution. This supports the greater importance of concentration rather than dose with regard to CHX substantivity on the salivary flora [70]. On comparing both concentrations, the mouthrinse with 0.12% CHX for 1 minute had a lower substantivity on the salivary flora than the mouthrinse with 0.2% CHX for 30 seconds. This confirms that the concentration is also more important than the time of application with regard to CHX substantivity on the salivary flora [70]. These results could be explained by the findings previously reported by Bonesvoll et al [73], who showed that the amount of CHX retained in the oral cavity increased nearly proportionally with the CHX concentration of the mouthrinse. After reviewing the literature, we have observed that the impact of the intrinsic factors of the CHX mouthrinse on the microbiological results obtained in the present series does not correlate with those described in clinical models of de novo plaque regrowth with the application of CHX over 3 or 4 days [74-76]. This lack of concordance could be due to the fact that these microbiological findings had no repercussion on the short-term antiplaque effect and/or the limitations inherent in the use of plaque indices that give only a rough impression of the amount of plaque [77]. Although the clinical efficacy of other forms of presentation of CHX, such as the gel and spray, has also been demonstrated [78,79], the substantivity of this antiseptic in its different forms of application has not been investigated after a single dose. García-Caballero et al [80] evaluated the in situ antimicrobial activity of CHX digluconate up to 7 hours after its application in solution, gel, spray and swab on the salivary flora. In this series, the solution was the form that presented the greatest antimicrobial activity. This finding may probably be explained by the fact that the CHX mouthrinse has “direct contact”with the salivary flora in contrast to other forms of application of CHX, and this favours an immediate antimicrobial action in saliva. Vianna et al [81] observed that the CHX gel is more difficult to mix with the bacterial suspension, although it could show the highest activity at the site of application [82]. In accordance with previous studies [83,84], it has recently been demonstrated that the salivary CHX concentrations at 1 and 2 hours after application of the gel decrease faster than when the mouthrinse is used. These findings could explain the results of salivary bacterial viability reported by García-Caballero et al [80] after the application of CHX in the form of a gel (at 3 hours, the percentage of live bacteria achieved basal figures). These authors also detected a lower antimicrobial activity of the sprays and of the swab application compared with the use of the CHX solution. This was probably due to the low doses of CHX used and because the solution provided a significantly higher salivary CHX concentration than the spray formulation [84]. In accordance with these findings, Stoeken et al [85], in a 3-day de novo plaque formation study,
534 ©FORMATEX 2011
Science against microbial pathogens: communicating current research and technological advances A. Méndez-Vilas (Ed.)______________________________________________________________________________
demonstrated that CHX applied in spray (0.2% and 0.12%) was not as effective as a 0.2% CHX mouthrinse in plaque inhibition. Despite the repercussions attributed to extrinsic factors of CHX on its retention in the oral cavity [34], we have not found any in situ study that has evaluated the influence of these factors on the antibacterial activity of a CHX single mouthrinse on the salivary flora. However, in our opinion, analysis of these factors is essential in order to establish the “true substantivity” of CHX in clinical situations in which patients carry out daily living activities in the periods between mouthrinses. Tomás et al [70] found that the practice of eating, chewing, and drinking significantly decreased the substantivity of 0.2% CHX, with complete recovery of the salivary flora at 3 to 7 hours after the mouthrinse. These results allow us to question the traditional regimen for the administration of CHX every 12 hours (twice a day), and reconsider the suitability of increasing the number of applications per day in order to guarantee a maximum antiseptic cover in those clinical situations in which infectious complications of oral origin must be prevented.
3.2 In situ antimicrobial activity of chlorhexidine on plaque-like biofilm
In vitro research has demonstrated that bacteria growing in structured communities on a surface differ phenotypically from their counterparts growing in planktonic phase [86,87], behaving like cells in a multicellular organism [88]. In fact, bacteria in biofilms can be 10–1,000 times more resistant to antimicrobial treatment than those grown in planktonic phase [89]. Pratten and Wilson [90] observed that oral microorganisms grown in vitro biofilms are shown to be up to 250 times more resistant to CHX than their planktonic counterparts. Even after a 60-minute exposure to 0.2% CHX, substantial numbers of bacteria in the biofilm remained vital [91]. This condition might be related to the slower growth rate of biofilm, to problems of antimicrobial agent penetration into the biofilm, or to inactivation of the agent in the biofilm [92]. An ideal prerequisite for a successful antimicrobial agent is that all bacteria within the biofilm should be exposed at an adequate concentration for an adequate time in order to achieve a clinically relevant reduction in pathogenesis [93]. The rate and extent of antimicrobial agent penetration depends on factors including the biofilm structure and composition [92,94], and perhaps most importantly, biofilm thickness [95], as well as the physicochemical properties of the solute [92,94]. In this sense, Von Ohle et al [93] used a simple diffusion model to calculate CHX concentration as a function of depth and time of application on in situ 3-day PL-biofilm, assuming that a concentration of 0.1% CHX would be a clinically relevant concentration. The calculated concentration profiles showed that when using a 0.2% CHX solution with an exposure time of 1 minute, a concentration of 0.1% or greater was achieved only to a depth of 70 µm. The model predicts that it would take 17.5 minutes to achieve 0.1% CHX at the base of a 300 µm-thick biofilm (e.g., interproximal or at other retention sites). However, if the thickness of the biofilm were reduced to 100 µm the time would be reduced to <2 minutes; if it were reduced to 30 µm, then it would only take 12 seconds [93] . On the other hand, although another very interesting aspect is based on solute penetration during brief exposure periods (<2 minutes), it is relatively unexplored. Up to now, it has been evaluated that exposure periods of antimicrobial agents in vitro biofilm models ranged from several minutes [96] to hours [97], which has little relevance to the oral cavity, where biofilm exposure to antimicrobial agents may be 30 seconds-1 minute.
Methodological approach
The in vitro development of biofilm models have led to significant advances in the study of oral biofilms [98,99]. However, in vitro oral biofilm models tend to involve limited numbers of species and, in addition, they are created under conditions that still cannot adequately reflect the physiological situation in the mouth [94,100,101]. Factors related to the oral cavity, such as the turnover rate of saliva, the ability of antibacterial substances to adhere to the pellicle of the tooth or the surface of soft tissues in order to achieve their effects, and the interaction with unculturable bacteria, cannot be modelled in in vitro experiments [102]. Consequently, at the present time, the scientific community recognises that in vitro models cannot guarantee the creation of oral biofilms whose composition and structure is comparable with those that form in situ [94,100,101,103]. For this reason, there is a need to develop in situ biofilm models that can subsequently be analysed intact ex vivo [100,104,105]. Studies have been published in the literature in which the in situ antimicrobial activity of CHX on the plaque-like biofilm (PL-biofilm) has been evaluated using microbiological plate culture techniques [31,106,107]. However, the numerous disadvantages associated with the use of culture-dependent methods are well known [56,102]. Since Netuschil first used fluorescence techniques to investigate the dental plaque in 1983 [108], numerous authors have applied fluorescence methods to study the in situ antibacterial effect of CHX on PL-biofilm [32,109,110]. A common methodological characteristic of all these studies is that evaluation of the supragingival bacterial plaque was performed on material previously removed from the surface of the tooth [32,109,110], whereas the subgingival bacterial plaque was obtained by paper point sampling or by mechanical debridement [106,111]. This is likely to disturb the delicate three-dimensional relationship of the cells, matrix, space, and substrate [92,112,113]. Another disadvantage of this type of research, in which the dental plaque is disturbed, is that the level of penetration of an antimicrobial agent into the PL-biofilm cannot be evaluated as the samples are dispersed for analysis [32]. This methodology therefore provides an
535©FORMATEX 2011
Science against microbial pathogens: communicating current research and technological advances A. Méndez-Vilas (Ed.)_______________________________________________________________________________

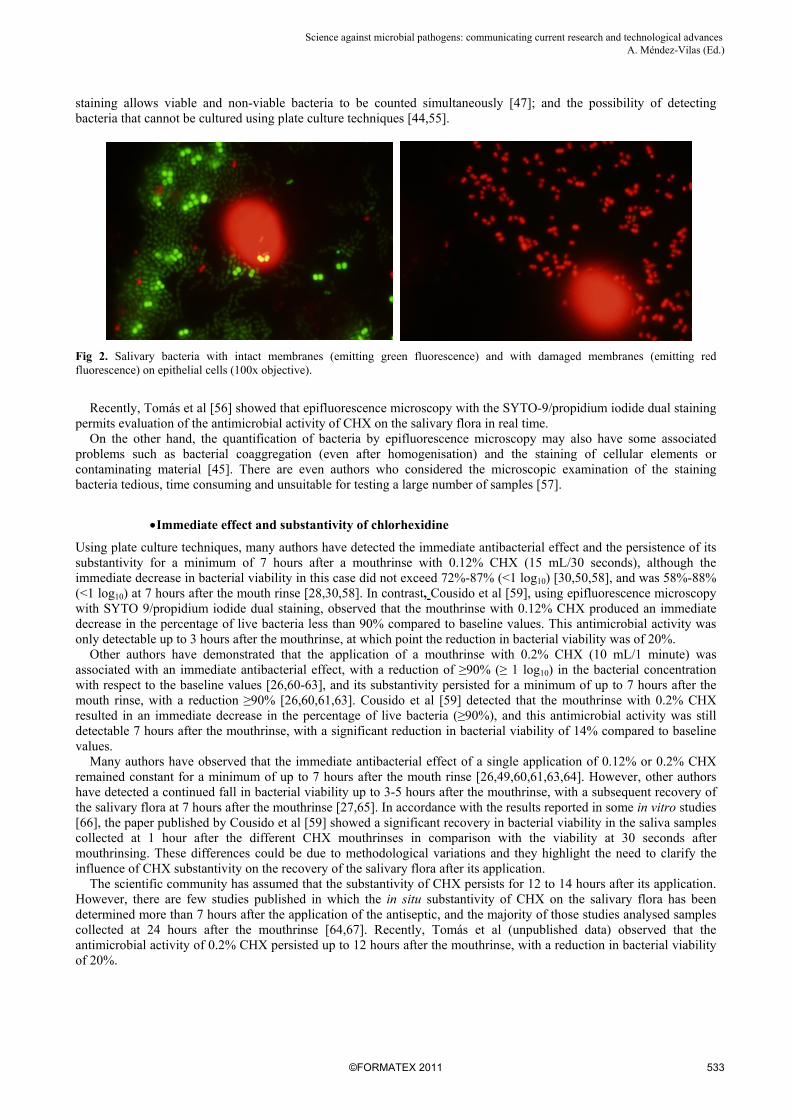
inadequate study of the architecture and organization of in situ PL-biofilm, as well as of the action of antimicrobial agents on its structure [94,114]. As a result, and in order to improve the methodology of such studies, some authors designed special removable appliances that included a number of disks on which growth of the PL-biofilm took place [101,114-116]. Subsequently, as is shown in Figure 3, this undisturbed PL-biofilm was analysed using confocal laser scanning microscopy (CLSM) and fluorescence solutions that permitted the simultaneous study of the three-dimensional structure of the biofilm and the evaluation of bacterial viability [101,114-116]. Other techniques such as fluorescence-labelled antibodies and fluorescence hybridization (FISH) have been frequently used in combination with CLSM to analyse bacterial topography of in situ undisturbed PL-biofilm [112,113,117,118].
Fig. 3. Bacteria with intact membranes (emitting green fluorescence) and with damaged membranes (emitting red fluorescence) in the de novo plaque-like biofilm (63x water-immersion objective). With CLSM, biofilms can be studied in their natural hydrated state, with no need for dehydration, fixation, or staining [77,100,114]. In addition, the optical sectioning properties of CLSM mean that very thin optical sections in the horizontal plane (X-Y axes) can be taken at 0.5 to 2 µm intervals, at increasing depths through the biofilm (from the surface of the biofilm to its base), and they will be free from out-of-focus blurring [77,102,112,119,120]. Consequently, at present, the scientific community considers that the methodological design based on use of special removable appliances (including disks) to obtain biofilm samples and its analysis by CLSM (in combination with other microscopic and microbiological techniques) is the most suitable approach for studying the in situ architecture and physiology of undisturbed PL-biofilm formed on surfaces, as well as the antibacterial effect of antimicrobials on this microbial structure [92,104,114].
Immediate effect and substantivity of chlorhexidine
Despite the in-depth knowledge about antimicrobial activity of different agents on in vitro biofilm [96,97], there are few studies published in the literature in which the effects of antimicrobial agents on in situ PL-biofilm at defined time points have been investigated applying CLSM together with bacterial viability techniques. To the best of the author’s knowledge, there are only two in situ studies in which the antimicrobial effect of CHX on PL-biofilm derived from a single application has been studied and in both the treatment was practised exvivo [93,121]. In 2001, Zaura-Arite et al [121] were the first authors to visualise the antimicrobial effect of a single exvivo CHX treatment on PL-biofilm remaining on bovine dentin disks. These disks were removed at 6 hours, 1 and 2 days and then broken into halves along the middle groove. One of the halves was covered with 50 µl of 0.2% CHX digluconate and treated for 1 minute; the other half served as a control covered with 50 µl of saline. The mean bacterial viability values of control and CHX-treated biofilms were at 6 hours (35% versus 18%), at 1 day (outer layer, 49% versus 34%; middle layer, 67% versus 42%; inner layer, 50% versus 48%) and at 2 days (outer layer, 52% versus 33%; middle layer, 63% versus 42%; inner layer 54% versus 48%). Consequently, these authors concluded that only minor and superficial bactericidal effects of CHX were obtained on PL-biofilm, with a thickness less than 65 µm. However, it’s very interesting to note that the subjects brushed their teeth twice a day (without the presence of intraoral appliances) with a NaF toothpaste [121], which could have conditioned the results obtained. Recently, von Ohle et al [93] examined the CHX antimicrobial effect on the physiology of the PL-biofilms during exposure to sucrose, using a 0.2% CHX formulation and biofilms were exvivo exposed to 10 mL of the CHX solution for either 1 or 10 minutes. In contrast to the results reported by Zaura-Arite et al [121], CHX treatment significantly
536 ©FORMATEX 2011
Science against microbial pathogens: communicating current research and technological advances A. Méndez-Vilas (Ed.)______________________________________________________________________________

reduced the bacterial viability (67% in control biofilm compared to 2% and 0.7% in CHX-treated biofilms at 1 and 10 minutes, respectively). However, CHX treatment did not significantly reduce the overall oxygen metabolism since even after a 10 minute exposure the biofilm was still physiologically active, demonstrating incomplete killing, and there was a relocation of activities deeper in the biofilm. CHX inactivated bacteria from the top down and layer by layer of PL-biofilms were killed with the highest efficacy in the outer regions. For these authors, this is presumably caused by a combination of several mechanisms: (i) the deeper penetration of oxygen, reducing the appearance of anaerobic processes; (ii) the higher CHX concentrations and increased toxicity effects in deeper layers strongly affecting the fermentative processes; and (iii) a differing susceptibility to CHX of the functional group of organisms (i.e., aerobic heterotrophs versus anaerobic fermentative bacteria). CHX had a more pronounced effect on acidification than respiration, thereby creating a more aerated and less acidogenic environment and consequently the microecology might have been changed to one that was less pathogenic [93].
3.3 In situ antimicrobial activity of chlorhexidine on salivary flora versus plaque-like biofilm
It has been stated that fluorescence techniques could be particularly useful in a simultaneous analysis of the effects of antimicrobials that alter the cytoplasmic membrane integrity on different oral ecosystems [56]. Despite the interrelationship between the two ecosystems and the importance of their study, there are no papers published in the literature in which CHX substantivity on saliva and PL-biofilm was compared. Tomás et al (unpublished data) detected that bacteria growing in situ 2-day PL-biofilm were 5 times more resistant (at 30 seconds) to a 0.2% CHX mouthrinse than those present in salivary flora (viability of 5% and 1% respectively). However, a 0.2% CHX mouthrinse showed higher substantivity (sustained antibacterial activity) on de novo PL-biofilm than on salivary flora at 5 and 7 hours after CHX application (viability of 25% and 32% versus 55% and 77% respectively). This condition might be related to the slower growth rate of PL-biofilm or the presence of an open architecture with such channels and voids in situ PL-biofilm, which would presumably provide direct communication between the oral environment and the enamel surface [92]. These “circulatory” channels and voids could have important implications for the movement of tooth damaging organic acids, bacterial toxins, and other antigens, as well as for the delivery of antimicrobial agents to the desired targets within the PL-biofilm [92]. In this sense, although it has been assumed that dead bacteria and exopolymeric substances produce impede fast penetration of the antimicrobials through the biofilm, in contrast, other authors have stated that PL-biofilm may also contribute to a reservoir function for antimicrobial agents [32]. Subsequently, this same research group evaluated the in situ substantivity at 8, 10, and 12 hours after performing a single mouthrinse with 0.2% CHX on the salivary flora and on undisturbed 2-day PL-biofilm, differentiating between two times of application (daytime mouthrinse versus nocturnal mouthrinse)(unpublished data). The application of a single mouthrinse with 0.2% CHX had a lower substantivity on the salivary flora between 8 and 12 hours after its application than was found with PL-biofilm. In the saliva, the bacterial viability recovered progressively and was affected by the time of application of the mouthrinse (day or night); being more effective when performed at night. In the PL-biofilm, bacterial viability remained stable for up to 12 hours after the mouthrinse and was not affected by the time of day the mouthrinse was performed. These results support the greater physiological dynamics of the salivary flora and the slower growth rate and/or the possible reservoir function associated with the structure of undisturbed de novo PL-biofilm.
4. Conclusions
Numerous authors have demonstrated the immediate antibacterial effect of CHX, and its substantivity in saliva for a minimum of 7 hours after a single mouthrinse. However, few authors have studied the in situ antibacterial activity of CHX on the salivary flora, analysing the influence of intrinsic factors associated with the antiseptic and extrinsic factors, all of which can affect its antibacterial activity. Nor have many papers been published using CLSM in association with bacterial viability techniques to determine the effects of CHX on in situ undisturbed PL-biofilm, and in the studies carried out the results have not been uniform. Consequently, a more extensive application of advanced microbiological and/or microscopy techniques in combination with CLSM is required in future research in order to increase our understanding of the antibacterial effects of CHX and other antimicrobial agents on PL-biofilm structure. These effects should then be compared with the effects observed in other oral ecosystems (such as salivary flora) and the influence of intrinsic and extrinsic factors on the effectiveness of the antiseptic should be analysed.
References
[1] Lang NP, Brecx M. Chlorhexidine digluconate: an agent for chemical plaque control and prevention of gingival inflammation. Journal of Periodontal Research. 1986;21:74-89.
537©FORMATEX 2011
Science against microbial pathogens: communicating current research and technological advances A. Méndez-Vilas (Ed.)_______________________________________________________________________________

[2] Davies GE, Francis J, Martin AR, Rose FL, Swain G. 1:6-Di-4'-chlorophenyldiguanidohexane (hibitane): laboratory investigation of a new antibacterial agent of high potency. British Journal of Pharmacology and Chemotherapy. 1954;9:192-196.
[3] Bascones A, Manso FJ. Clorhexidina en Odontoestomatología: Conceptos actuales y revisión de la literatura. Avances en Odontoestomatología. 1994;10:685-708.
[4] Ruppert M, Schlagenhauf U. La clorhexidina en Odontología. Aspectos generales. Quintessence (Ed. Española). 2005;18:12-23. [5] Löe H, Schiött CR. The effect of mouthrinses and topical application of chlorhexidine on the development of dental plaque and
gingivitis in man. Journal of Periodontal Research. 1970;5:79-83. [6] Löe H, Schiött CR, Karring G, Karring T. Two years oral use of chlorhexidine in man. I. General design and clinical effects.
Journal of Periodontal Research. 1976;11:135-144. [7] Enrile de Rojas FJ, Alemany AS, Burguera AC, Dios PD. Aplicaciones clínicas adicionales de colutorios antisépticos.
Periodoncia. 2006;16:95-104. [8] Manau-Navarro C, Guasch-Serra S. Métodos de control de placa bacteriana. In: Cuenca E, Manau C, Serra LL. Odontología
Preventiva y Comunitaria. Principios Métodos y Aplicaciones. Barcelona: Masson; 2003:69-88. [9] Al-Tannir MA, Goodman HS. A review of clorhexidine and its use in special populations. Special Care in Dentistry.
1994;14:116-122. [10] Gilbert P, Moore LE. Cationic antiseptics: diversity of action under a common epithet. Journal of Applied Microbiology.
2005;99:703–715. [11] Franch M, Pascual A, Santos A. Colutorios en periodoncia. Parte II. Archivos de Odontoestomatología. 2005;21:471-487. [12] Arévalo JM, Arribas JL, Calbo L, Hernández MJ, Lizán M, Herruzco R. Guía del grupo de trabajo sobre desinfectantes y
antisépticos. Revisión 1998. Medicina Preventiva. 1998;4:38-43. [13] Albertos JM, Junquera LM, Albertos MT, Olay S, López-Arranz E. La clorhexidina. Perspectiva actual. Anales de
Odontoestomatología. 1996;5:217-223. [14] Maris P. Modes of action of disinfectants. Revue Scentifique et Technique (International Office of Epizootics). 1995;14:47-55. [15] Hugo WB. Disinfection mechanisms. In: Russell AD, Hugo WB, Ayliffe GAJ, eds. Principles and Practice of Disinfection,
Preservation and Sterilization. Oxford: Blackwell; 1992:187-210. [16] Maillard JY. Bacterial target sites for biocide action. Journal of Applied Microbiology. 2002;92:16-27. [17] Musteata FM, Pawliszyn J. Assay of stability, free and total concentration of chlorhexidine in saliva by solid phase
microextraction. Journal of Pharmaceutical and Biomedical Analysis. 2005;37:1015-1024. [18] Rölla G, Melsen B. On the mechanism of the plaque inhibition by chlorhexidine. Journal of Dental Research. 1975;54:57-62. [19] Hugo WB, Longworth AR. The effect of chlorhexidine on the electrophoretic mobility, cytoplasmic constituents, dehydrogenase
activity and cell walls of Escherichia coli and Staphylococcus aureus. Journal of Pharmacy and Pharmacology. 1966;18:569-578.
[20] Fardal O, Turnbull RS. A review of the literature on use of chlorhexidine in dentistry. Journal of the American Dental Association. 1986;112:863-869.
[21] Longworth, AR. Chlorhexidine. In: Hugo WB, ed. Inhibition and destruction of the bacterial cell. New York, N.Y: Academic Press; 1971:95-106.
[22] Chawner JA, Gilbert P. A comparative study of the bactericidal and growth inhibitory activities of the bisbiguanides alexidine and chlorhexidine. Journal of Applied Bacteriology. 1989;66:243-252.
[23] Chawner JA, Gilbert P. Interaction of the bisbiguanides chlorhexidine and alexidine with phospholipid-vesicles: evidence for separate modes of action. Journal of Applied Bacteriology. 1989;66:253–258.
[24] Bernimoulin JP. Recent concepts in plaque formation. Journal of Clinical Periodontology. 2003;30:7-9. [25] Junco-Lafuente MP, Baca-García P, Mesa-Aguado FL. Utilización de la clorhexidina en la prevención oral de pacientes de la
tercera edad. Revista del Ilustre Consejo General de Colegios de Odontólogos y Estomatólogos de España. 2001;6:81-89. [26] Moran J, Addy M, Wade WG, Maynard JH, Roberts SE, Aström M, Movert R. A comparison of delmopinol and chlorhexidine
on plaque regrowth over a 4-day period and salivary bacterial counts. Journal of Clinical Periodontology. 1992;19:749-753. [27] Jenkins S, Addy M, Wade W, Newcombe RG. The magnitude and duration of the effects of some mouthrinse products on
salivary bacterial counts. Journal of Clinical Periodontology. 1994;21:397-401. [28] Elworthy A, Greenman J, Doherty FM, Newcombe RG, Addy M. The substantivity of a number of oral hygiene products
determined by the duration of effects on salivary bacteria. Journal of Periodontology. 1996;67:572-576. [29] Balbuena L, Stambaugh KI, Ramirez SG, Yeager C. Effects of topical oral antiseptic rinses on bacterial counts of saliva in
healthy human subjects. Otolaryngology and Head and Neck Surgery. 1998;118:625-629. [30] Fernandes-Naglik L, Downes J, Shirlaw P, Wilson R, Challacombe SJ, Kemp GK, Wade WG. The clinical and microbiological
effects of a novel acidified sodium chlorite mouthrinse on oral bacterial mucosal infections. Oral Disease. 2001;7:276-280. [31] Rosin M, Welk A, Kocher T, Majic-Todt A, Kramer A, Pitten FA. The effect of a polyhexamethylene biguanide mouthrinse
compared to an essential oil rinse and a chlorhexidine rinse on bacterial counts and 4-day plaque regrowth. Journal of Clinical Periodontology. 2002;29:392-399.
[32] van der Mei HC, White DJ, Atema-Smit J, van de Belt-Gritter E, Busscher HJ. A method to study sustained antimicrobial activity of rinse and dentifrice components on biofilm viability in vivo. Journal of Clinical Periodontology. 2006;33:14-20.
[33] Bonesvoll P, Lökken P, Rölla G. Influence of concentration, time, temperature, and pH on the retention of chlorhexidine in the human oral cavity after mouthrinses. Archives of Oral Biology. 1974;19:1025-1029.
[34] Bonesvoll P, Olsen I. Influence of teeth, pla que and dentures on the retention of chlorhexidine in the human oral cavity. Journal of Clinical Periodontology. 1974;1:214-221. [35] Tsuchiya H, Miyazaki T, Ohmoto S. High-performance liquid chromatographic analysis of chlorhexidine in saliva after
mouthrinsing. Caries Research. 1999;33:156-163. [36] Schiött CR, Löe H, Jensen SB, Kilian M, Davies RM, Glavind K. The effect of chlorhexidine mouthrinses on the human oral
flora. Journal of Periodontal Research. 1970;5:84-89.
538 ©FORMATEX 2011
Science against microbial pathogens: communicating current research and technological advances A. Méndez-Vilas (Ed.)______________________________________________________________________________

[37] Roberts WR, Addy M. Comparison of the in vivo and in vitro antibacterial properties of antiseptic mouthrinses containing chlorhexidine, alexidine, cetyl pyridinium chloride and hexetidine. Relevance to mode of action. Journal of Clinical Periodontology. 1981;8:295-310.
[38] Addy M, Jenkins S, Newcombe R. Toothpastes containing 0.3% and 0.5% triclosan. II. Effects of single brushings on salivary bacterial counts. American Journal of Dentistry. 1989;2:215-219.
[39] Collaert B, Edwardsson S, Attström R, Hase JC, Aström M, Movert R. Rinsing with delmopinol 0.2% and chlorhexidine 0.2%: short-term effect on salivary microbiology, plaque, and gingivitis. Journal of Periodontology. 1992;63:618-625.
[40] Weiger R, Netuschil L, Wester-Ebbinghaus T, Brecx M. An approach to differentiate between antibacterial and antiadhesive effects of mouthrinses in vivo. Archives of Oral Biology. 1998;43:559-565.
[41] Rosin M, Welk A, Bernhardt O, Ruhnau M, Pitten FA, Kocher T, Kramer A. Effect of a polyhexamethylene biguanide mouthrinse on bacterial counts and plaque. Journal of Clinical Periodontology. 2001;28:1121-1126.
[42] Sekino S, Ramberg P, Uzel NG, Socransky S, Lindhe J. Effect of various chlorhexidine regimens on salivary bacteria and de novo plaque formation. Journal of Clinical Periodontology. 2003;30:919-925.
[43] Addy M, Moran JM. Evaluation of oral hygiene products: science is true; don’t be misled by the facts. Periodontology 2000. 1997;15:40-51.
[44] Berney M, Hammes F, Bosshard F, Weilenmann HU, Egli T. Assessment and interpretation of bacterial viability by using the LIVE/DEAD Baclight Kit in combination with flow cytometry. Applied Environmental Microbiology. 2007;73:3283-3290.
[45] Nadkarni MA, Martin FE, Jacques NA, Hunter N. Determination of bacterial load by real-time PCR using a broad-range (universal) probe and primers set. Microbiology. 2002;148:257-266.
[46] Biggerstaff JP, Le Puil M, Weidow BL, Prater J, Glass K, Radosevich M, White DC. New methodology for viability testing in environmental samples. Molecular and Cellular Probes. 2006;20:141-146.
[47] Boulos L, Prévost M, Barbeau B, Coallier J, Desjardins R. LIVE/DEAD BacLight: application of a new rapid staining method for direct enumeration of viable and total bacteria in drinking water. Journal of Microbiological Methods. 1999;37:77-86.
[48] Lehtinen J, Nuutila J, Lilius EM. Green fluorescent protein-propidium iodide (GFP-PI) based assay for flow cytometric measurement of bacterial viability. Cytometry. Part A: Journal of International Society for Analytical Cytology. 2004;60:165-172.
[49] Addy M, Jenkins S, Newcombe R. The effect of some chlorhexidine-containing mouthrinses on salivary bacterial counts. Journal of Clinical Periodontology. 1991;18:90-93.
[50] Buckner RY, Kayrouz GA, Briner WW. Reduction of oral microbes by a single chlorhexidine rinse. Compendium. 1994;15:512-520.
[51] Pitten FA, Kramer A. Antimicrobial efficacy of antiseptic mouthrinse solutions. European Journal of Clinical Pharmacology. 1999;55:95-100.
[52] Sreenivasan PK, Gittins E. Effects of low dose chlorhexidine mouthrinses on oral bacteria and salivary microflora including those producing hydrogen sulfide. Oral Microbiology and Immunology. 2004;19:309-313.
[53] Hope CK, Wilson M. Analysis of the effects of chlorhexidine on oral biofilm vitality and structure based on viability profiling and an indicator of membrane integrity. Antimicrobial Agents and Chemotherapy. 2004;48:1461-1468.
[54] Filoche SK, Coleman MJ, Angker L, Sissons CH. A fluorescence assay to determine the viable biomass of microcosm dental plaque biofilms. Journal of Microbiological Methods. 2007;69:489-496.
[55] Joux F, Lebaron P. Use of fluorescent probes to assess physiological functions of bacteria at single-cell level. Microbes and Infection/Institut Pasteur. 2000;2:1523-1535.
[56] Tomás I, García-Caballero L, Cousido MC, Limeres J, Álvarez M, Diz P. Evaluation of chlorhexidine substantivity on salivary flora by epifluorescence microscopy. Oral Disease. 2009;15:428-433.
[57] Singh MP. Rapid test for distinguishing membrane-active antibacterial agents. Journal of Microbiological Methods. 2006;67:125-130.
[58] Jenkins S, Addy M, Newcombe R. The effect of triclosan, stannous fluoride and chlorhexidine products on: (II) Salivary bacterial counts. Journal of Clinical Periodontology. 1990;17:698-701.
[59] Cousido MC, Tomás I, García-Caballero L, Limeres J, Álvarez M, Diz P. In vivo substantivity of 0.12% and 0.2% chlorhexidine mouthrinses on salivary bacteria. Clinical Oral Investigations. 2010;14:397-402.
[60] Jenkins S, Addy M, Newcombe R. Triclosan and sodium lauryl sulphate mouthrinsees (I). Effects on salivary bacterial counts. Journal of Clinical Periodontology. 1991;18:140-144.
[61] Reynolds S, Moran J, Addy M, Wade WG, Newcombe R. Taurolin as an oral rinse. I. Antimicrobial effects in vitro and in vivo. Clinical Preventive Dentistry. 1991;13:13-17.
[62] Simonsson T, Hvid EB, Rundegren J, Edwardsson S. Effect of delmopinol on in vitro dental plaque formation, bacterial acid production and the number of microorganisms in saliva. Oral Microbiology and Immunology. 1991;6:305-309.
[63] Moran J, Addy M, Wade W, Milson S, McAndrew R, Newcombe RG. The effect of oxidising mouthrinses compared with chlorhexidine on salivary bacterial counts and plaque regrowth. Journal of Clinical Periodontology. 1995;22:750-755.
[64] Addy M, Wright R. Comparison of the in vivo and in vitro antibacterial properties of povidone iodine and chlorhexidine gluconate mouthrinses. Journal of Clinical Periodontology. 1978;5:198-205.
[65] Yates R, Moran J, Addy M, Mullan PJ, Wade WG, Newcombe R. The comparative effect of acidified sodium chlorite and chlorhexidine mouthrinses on plaque regrowth and salivary bacterial counts. Journal of Clinical Periodontology. 1997;24:603-609.
[66]Toljanic JA, Hagen JC, Takahashi Y, Shapiro RD. Evaluation of the substantivity of a chlorhexidine oral rinse in irradiated head and neck cancer patients. Journal of Oral and Maxillofacial Surgery. 1992;50:1055-1059.
[67] Dahlen G. Effect of antimicrobial mouthrinses on salivary microflora in healthy subjects. Scandinavian Journal of Dental Research. 1984;92:38-42.
539©FORMATEX 2011
Science against microbial pathogens: communicating current research and technological advances A. Méndez-Vilas (Ed.)_______________________________________________________________________________
[68] Harper PR, Milsom S, Wade W, Addy M, Moran J, Newcombe RG. An approach to efficacy screening of mouthrinses: studies on a group of French products (II). Inhibition of salivary bacteria and plaque in vivo. Journal of Clinical Periodontology. 1995;22:723-727.
[69] Herrera D, Roldan S, Santacruz I, Santos S, Masdevall M, Sanz M. Differences in antimicrobial activity of four commercial 0.12% chlorhexidine mouthrinse formulations: an in vitro contact test and salivary bacterial counts study. Journal of Clinical Periodontology. 2003;30:307-314.
[70] Tomás I, Cousido MC, García-Caballero L, Rubido S, Limeres J, Diz P. Substantivity of a single chlorhexidine mouthrinse on salivary flora: influence of intrinsic and extrinsic factors. Journal of Dentistry. 2010;38:541-546.
[71] Milstone AM, Passaretti CL, Perl TM. Chlorhexidine: Expanding the armamentarium for infection control and prevention. Clinical Infectious Disease. 2008;46:274-281.
[72] Tomás I, Cousido MC, Tomás M, Limeres J, García-Caballero L, Diz P. In vivo bactericidal effect of 0.2% chlorhexidine but not 0.12% on salivary obligate anaerobes. Archives of Oral Biology. 2008;53:1186-1191.
[73] Bonesvoll P, Lökken P, Rölla G. Influence of concentration, time, temperature and pH on the retention of chlorhexidine in the human oral cavity after mouthrinses. Archives of Oral Biology. 1974;19:1025-1029.
[74] Smith RG, Moran J, Addy M, Doherty F, Newcombe RG. Comparative staining in vitro and plaque inhibitory properties in vivo of 0.12% and 0,2% chlorhexidine mouthrinses. Journal of Clinical Periodontology. 1995;22:613-617.
[75] Keijser JA, Verkade H, Timmerman MF, van der Weijden FA. Comparison of 2 commercially available chlorhexidine mouthrinses. Journal of Periodontology. 2003;74:214-218.
[76] van der Weijden GA, Timmerman MF, Novotny AG, Rosema NA, Verkerk AA. Three different rinsing times and inhibition of plaque accumulation with chlorhexidine. Journal of Clinical Periodontology. 2005;32:89-92.
[77] Arweiler NB, Lenz R, Sculean A, Al-Ahmad A, Hellwig E, Auschill TM. Effect of food preservatives on in situ biofilm formation. Clinical Oral Investigations. 2008;12:203-208.
[78] Francis JR, Addy M, Hunter B. A comparison of three delivery methods of chlorhexidine in handicapped children. II. Parent and house-parent preferences. Journal of Periodontology. 1987;58:456-459.
[79] Kalaga A, Addy M, Hunter B. Comparison of chlorhexidine delivery by mouthrinse and spray on plaque accumulation. Journal of Periodontology. 1989;60:127-130.
[80] García-Caballero L, Carmona IT, González MC, Posse JL, Taboada JL, Dios PD. Evaluation of the substantivity in saliva of different forms of application of chlorhexidine. Quintessence International. 2009;40:141-144.
[81] Vianna ME, Gomes BP, Berber VB, Zaia AA, Ferraz CC, de Souza-Filho FJ. In vitro evaluation of the antimicrobial activity of chlorhexidine and sodium hypochlorite. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontics. 2004;97:79-84.
[82] Benigni A, Paolantonio M, Di Murro C, Cattabriga M. Efficacy of chlorhexidine as a gel and as a mouthrinse. Prevenzione & Assistenza Dentale. 1989;15:9-15.
[83] Borer G, Schait A, Muhlemann HR. The oral clearance of chlorhexidine solutions and gels. Schweizerische Monatsschrift für Zahnheilkunde. 1978;88:619-621.
[84] Legaz Mellado AB, Sánchez A, García-Teresa G, Alcázar M. Comparative study of salivary chlorhexidine concentrations after oral application of different pharmaceutical forms. Journal of Clinical Periodontology. 2006;33 (Supplement 7):106-107.
[85] Stoeken JE, Versteeg PA, Rosema NA, Timmerman MF, van der Velden U, van der Weijden GA. Inhibition of de novo plaque formation with 0.12% chlorhexidine spray compared to 0.2% spray and 0.2% chlorhexidine mouthrinse. Journal of Periodontology. 2007;78:899-904.
[86] Costerton JW, Lewandowski Z, Caldwell DE, Korber DR, Lappin-Scott HM. Microbial biofilms. Annual Review of Microbiology. 1995;49:711-745.
[87] Costerton JW, Cook G, Lamont R. The community architecture of biofilms: dynamic structures and mechanisms. In: Newman HN, Wilson M, eds. Dental plaque revisited. Oral biofilms in health and disease. Cardiff, UK: Bioline; 1999:5-14.
[88] Pratten J, Andrews CS, Craig DQ, Wilson M. Structural studies of microcosm dental plaques grown under different nutritional conditions. FEMS Microbiology Letters. 2000;189:215-218.
[89] Davies D. Understanding biofilm resistance to antibacterial agents. Nature Reviews. Drug Discovery. 2003;2:114-122. [90] Pratten J, Wilson M. Antimicrobial susceptibility and composition of microcosm dental plaques supplemented with sucrose.
Antimicrobial Agents and Chemotherapy. 1999;43:1595-1599. [91] Wilson M, Patel H, Noar JH. Effect of chlorhexidine on multispecies biofilms. Current Microbiology. 1998;36:13-18. [92] Wood SR, Kirkham J, Marsh PD, Shore RC, Nattress B, Robinson C. Architecture of intact natural human plaque biofilms
studied by confocal laser scanning microscopy. Journal of Dental Research. 2000;79:21-27. [93] von Ohle C, Gieseke A, Nistico L, Decker EM, DeBeer D, Stoodley P. Real-time microsensor measurement of local metabolic
activities in ex vivo dental biofilms exposed to sucrose and treated with chlorhexidine. Applied and Environmental Microbiology. 2010;76:2326-2334.
[94] Watson PS, Pontefract HA, Devine DA, Shore RC, Nattres BR, Kirkham J, Robinson C. Penetration of fluoride into natural plaque biofilms. Journal of Dental Research. 2005;84:451-455.
[95] Stewart PS. Diffusion in biofilms. Journal of Bacteriology. 2003;185:1485-1491. [96] Shen Y, Stojicic S, Qian W, Olsen I, Haapasalo M. The synergistic antimicrobial effect by mechanical agitation and two
chlorhexidine preparations on biofilm bacteria. Journal of Endodontics. 2010;36:100-104. [97] Corbin A, Pitts B, Parker A, Stewart PS. Antimicrobial penetration and efficacy in an in vitro oral biofilm model. Antimicrobial
Agents and Chemotherapy. 2011;55:3338-3344. [98] McBain AJ. Chapter 4: In vitro biofilm models: An overview. Advances in Applied Microbiology. 2009;69:99-132. [99]Palmer RJ Jr. Supragingival and subgingival plaque: Paradigm of biofilms. Compendium of Continuing Education in Dentistry.
2010;31:104-138. [100] Auschill TM, Hellwig E, Sculean A, Hein N, Arweiller NB. Impact of the intraoral location on the rate of biofilm growth.
Clinical Oral Investigations. 2004;8:97-101.
540 ©FORMATEX 2011
Science against microbial pathogens: communicating current research and technological advances A. Méndez-Vilas (Ed.)______________________________________________________________________________

[101]Auschill TM, Hein N, Hellwig E, Follo M, Sculean A, Arweiler N.B. Effect of two antimicrobial agents on early in situ biofilm formation. Journal of Clinical Periodontology. 2005;32:147-152.
[102] Al-Ahmad A, Wunder A, Auschill TM, Follo M, Braun G, Hellwig E, Arweiler NB. The in vivo dynamics of Streptococcus spp., Actinomyces naeslundii, Fusobacterium nucleatum and Veillonella spp. in dental plaque biofilm as analysed by five-colour multiplex fluorescence in situ hybridization. Journal of Medical Microbiology. 2007;56:681-687.
[103] Al-Ahmad A, Wiedmann-Al-Ahmad M, Faust J, Bächle M, Follo M, Wolkewitz M, Hannig C, Hellwig E, Carvalho C, Kohal R. Biofilm formation and composition on different implant materials in vivo. Journal of Biomedical Materials Research. Part B, Applied Biomaterials. 2010;95:101-109.
[104] Hannig C, Hannig M. The oral cavity--a key system to understand substratum-dependent bioadhesion on solid surfaces in man. Clinical Oral Investigations. 2009;13:123-139.
[105] Palmer RJ Jr, Wu R, Gordon S, Bloomquist CG, Liljemark WF, Kilian M, Kolenbrander PE. Retrieval of biofilms from the oral cavity. Methods in Enzymology. 2001;337:393-403.
[106] Daneshmand N, Jorgensen MG, Nowzari H, Morrison JL, Slots J. Initial effect of controlled release chlorhexidine on subgingival microorganisms. Journal of Periodontal Research. 2002;37:375-379.
[107]Sreenivasan PK, Mattai J, Nabi N, Xu T, Gaffar A. A simple approach to examine early oral microbial biofilm formation and the effects of treatments. Oral Microbiology and Immunology. 2004;19:297-302.
[108] Netuschil L. Vitalfärbung von plaque-mikroorganismen mit fluoresceindiacetat und ethidium-bromid. Deutsche Zahnärztliche Zeitschrift. 1983;38:914-917.
[109] Arweiler NB, Boehnke N, Sculean A, Hellwig E, Auschill TM. Differences in efficacy of two commercial 0.2% chlorhexidine mouthrinse solutions: A 4-day plaque regrowth study. Journal of Clinical Periodontology. 2006;33:334-339.
[110] Al-Ahmad A, Roth D, Wolkewitz M, Wiedmann-Al-Ahmad M, Follo M, Ratka-Krüger P, Deimling D, Hellwig E, Hannig C. Change in diet and oral hygiene over an 8-week period: effects on oral health and oral biofilm. Clinical Oral Investigations. 2010;14:391-396.
[111] Loivukene K, Pahkla ER, Koppel T, Saag M, Naaber P. The microbiological status of patients with periodontitis in southern Estonia after non-surgical periodontal therapy. Stomatologija. 2005;7:45-47.
[112] Dige I, Nyengaard JR, Kilian M, Nyvad B. Application of stereological principles for quantification of bacteria in intact dental biofilms. Oral Microbiology and Immunology. 2009;24:69-75.
[113] Wecke J, Kersten T, Madela K, Moter A, Gobel UB, Friedmann A, Bernimoulin J. A novel technique for monitoring the development of bacterial biofilms in human periodontal pockets. FEMS Microbiology Letters. 2000;191:95-101.
[114] Arweiler NB, Hellwig E, Sculean A, Hein N, Auschill TM. Individual vitality pattern of in situ dental biofilms at different locations in the oral cavity. Caries Research. 2004;38:442-447.
[115] Netuschil L, Reich E, Unteregger G, Sculean A, Brecx M. A pilot study of confocal laser scanning microscopy for the assessment of undisturbed dental plaque vitality and topography. Archives of Oral Biology. 1998;43:277-285.
[116] Auschill TM, Arweiler NB, Netuschil L, Brecx M, Reich E, Sculean A. Spatial distribution of vital and dead microorganisms in dental biofilms. Archives of Oral Biology. 2001;46:471-476.
[117] Palmer RJ Jr, Diaz PI, Kolenbrander PE. Rapid succession within the Veillonella population of a developing human oral biofilm in situ. Journal of Bacteriology. 2006;188:4117-4124.
[118] Gu F, Lux R, Du-Thumm L, Stokes I, Kreth J, Anderson MH, Wong DT, Wolinsky L, Sullivan R, Shi W. In situ and non-invasive detection of specific bacterial species in oral biofilms using fluorescently labelled monoclonal antibodies. Journal of Microbiological Methods. 2005;62:145-160.
[119] Dige I, Nilsson H, Kilian M, Nyvad B. In situ identification of streptococci and other bacteria in initial dental biofilm by confocal laser scanning microscopy and fluorescence in situ hybridization. European Journal of Oral Sciences. 2007;115:459-467.
[120] Konishi N, Torii Y, Kurosaki A, Takatsuka T, Itota T, Yoshiyama M. Confocal laser scanning microscopic analysis of early plaque formed on resin composite and human enamel. Journal of Oral Rehabilitation. 2003;30:790-795.
[121] Zaura-Arite E, van Marle J, ten Cate JM. Confocal microscopy study of undisturbed and chlorhexidine-treated dental biofilm. Journal of Dental Research. 2001;80:1436-1440.
541©FORMATEX 2011
Science against microbial pathogens: communicating current research and technological advances A. Méndez-Vilas (Ed.)_______________________________________________________________________________